
Differences in Immunological Evasion of the Delta (B.1.617.2) and Omicron (B.1.1.529) SARS-CoV-2 Variants: A Retrospective Study on the Veneto Region’s Population

 , , , , and
, , , , and 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Data Source
2.2. Study Design
2.3. Statistical Analysis
3. Results
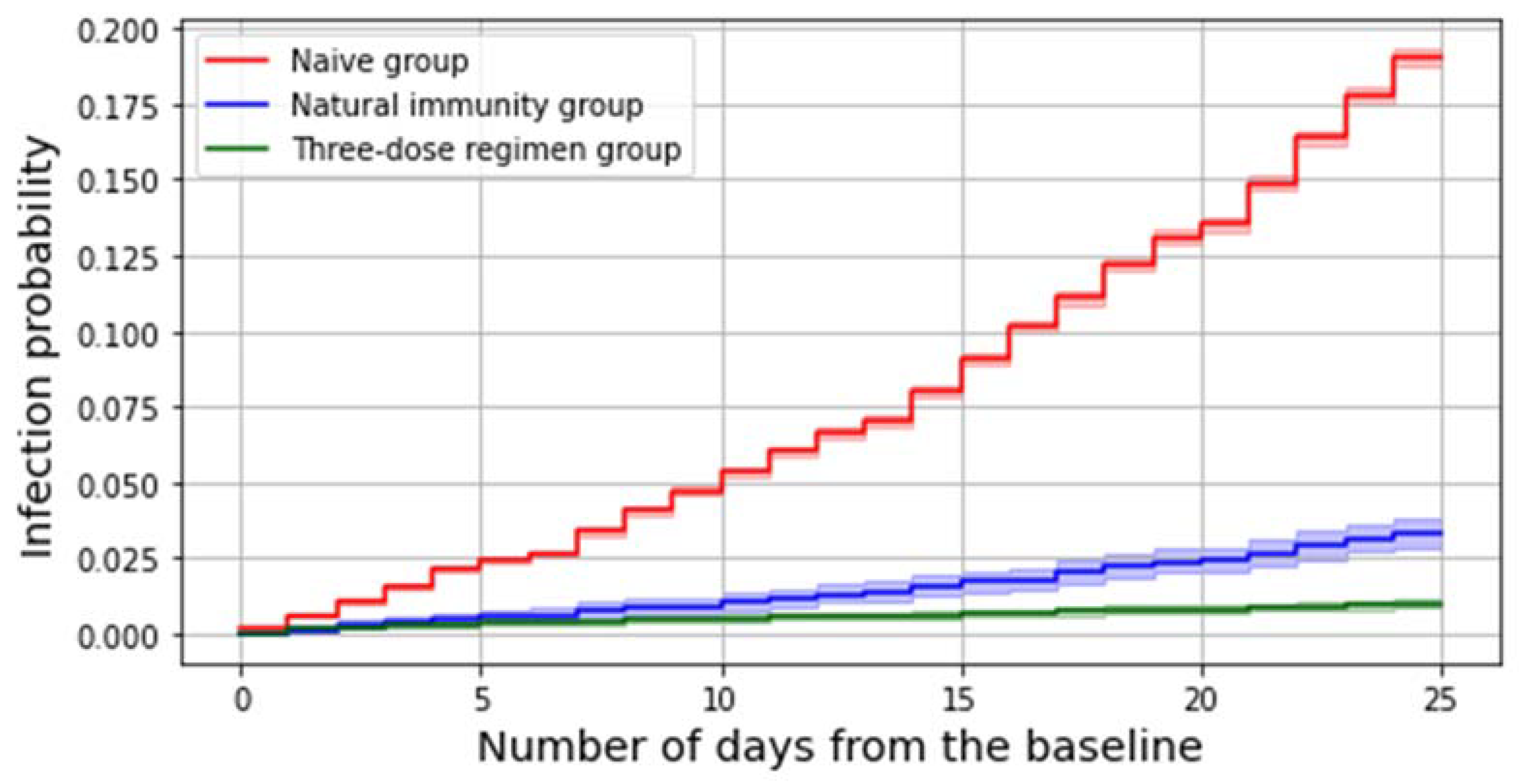
3.1. Delta Period
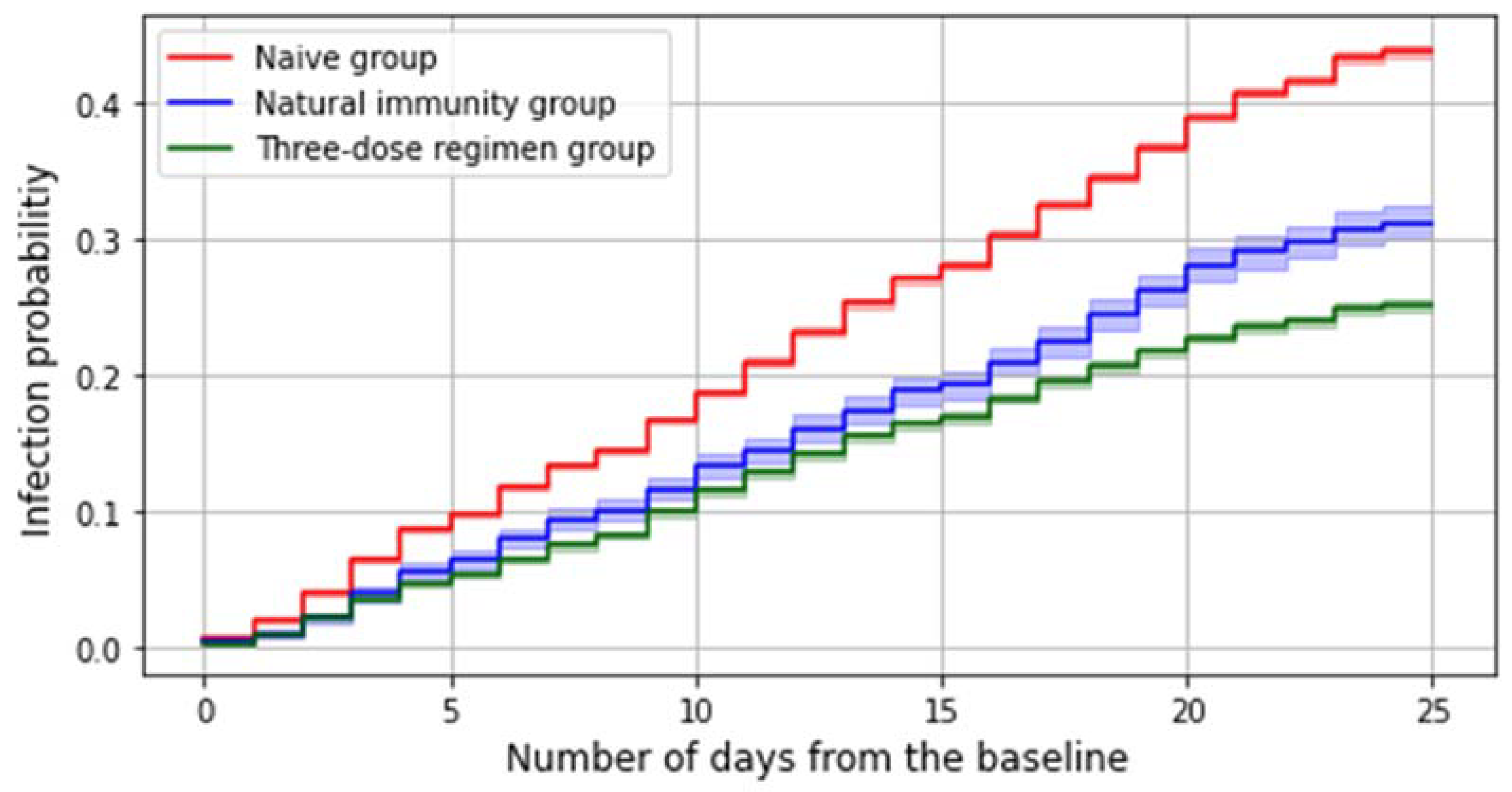
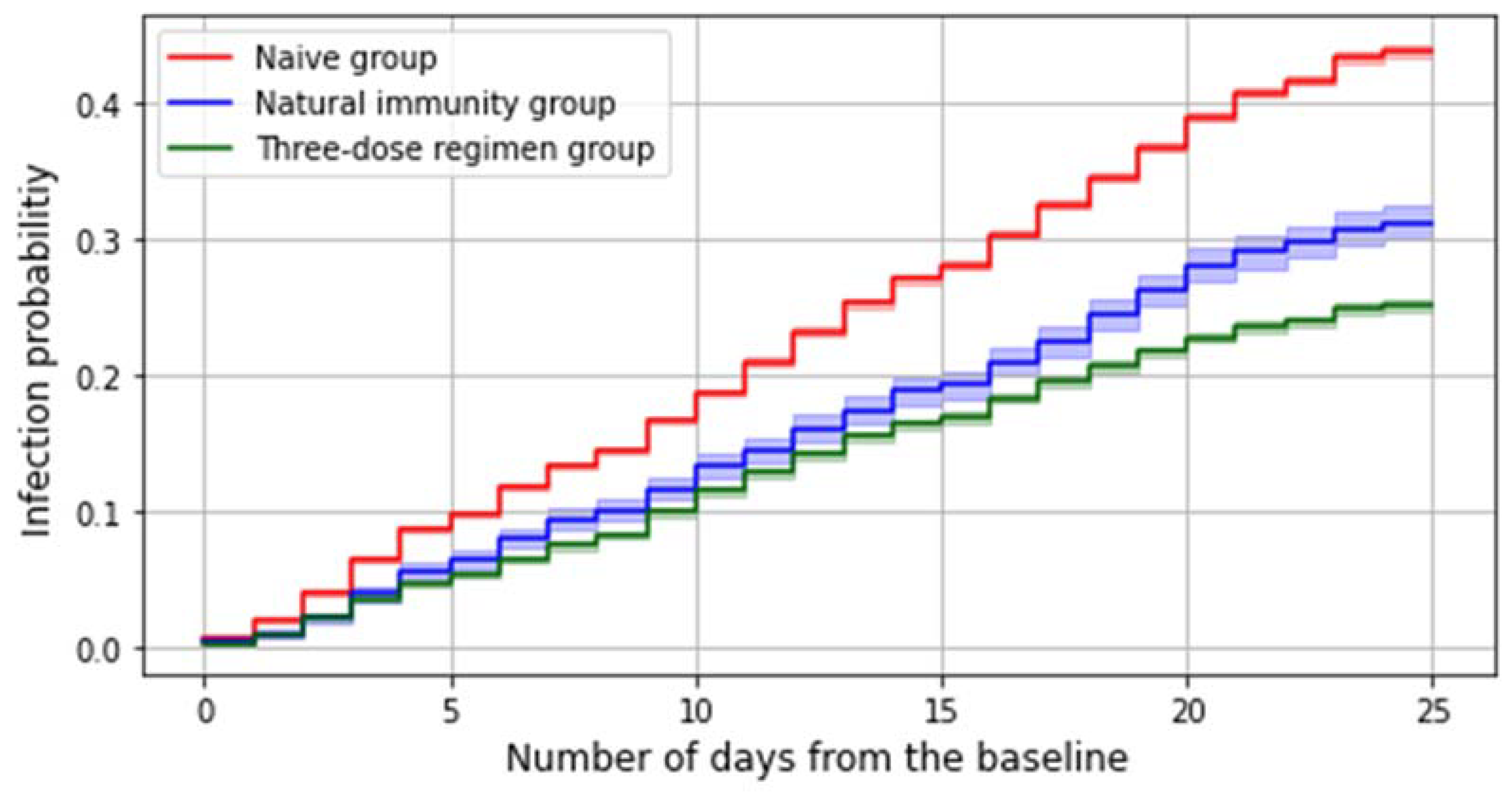
3.2. Omicron Period
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Worldometer. Information on COVID-19 Coronavirus Pandemic. Available online: https://www.worldometers.info/coronavirus/ (accessed on 14 March 2022).
- Italian Institute of Statistics (ISTAT). Population with Permanent Address in Veneto Region on 1 January 2021. Available online: http://dati.istat.it/Index.aspx?QueryId=18549 (accessed on 4 March 2022).
- Italian Department of Civil Protection. COVID-19 Italy—Monitoring of the Situation. Available online: https://opendatadpc.maps.arcgis.com/apps/dashboards/b0c68bce2cce478eaac82fe38d4138b1 (accessed on 14 March 2022).
- Italian Agency of Drugs (AIFA). Annual Report on the Safety of Anti-COVID-19 Vaccines, 27/12/2020–26/12/2021. Available online: https://www.aifa.gov.it/documents/20142/1315190/Rapporto_annuale_su_sicurezza_vaccini%20anti-COVID-19.pdf (accessed on 14 March 2022).
- Italian Ministry of Health. Vaccinations Web Portal. Legislative Archive. Available online: https://www.salute.gov.it/portale/vaccinazioni/archivioNormativaVaccinazioni.jsp (accessed on 14 March 2022).
- Veneto Region. Veneto Region Web Portal. Anti-COVID-19 Vaccination Campaign. Available online: https://regione.veneto.it/dati-vaccinazioni/ (accessed on 7 March 2022).
- Goldberg, Y.; Mandel, M.; Bar-On, Y.M.; Bodenheimer, O.; Freedman, L.; Haas, E.J.; Milo, R.; Alroy-Preis, S.; Ash, N.; Huppert, A. Waning Immunity after the BNT162b2 Vaccine in Israel. N. Engl. J. Med. 2021, 385, e85. [Google Scholar] [CrossRef] [PubMed]
- Bar-On, Y.M.; Goldberg, Y.; Mandel, M.; Bodenheimer, O.; Freedman, L.; Kalkstein, N.; Mizrahi, B.; Alroy-Preis, S.; Ash, N.; Milo, R.; et al. Protection of BNT162b2 Vaccine Booster against Covid-19 in Israel. N. Engl. J. Med. 2021, 385, 1393–1400. [Google Scholar] [CrossRef] [PubMed]
- Italian Ministry of Health. General Direction of Health Prevention. Preliminary Indications for the Administration of Additional and “Booster” Doses during the Anti-SARS-CoV-2/COVID-19 Vaccination Campaign. Available online: https://www.trovanorme.salute.gov.it/norme/renderNormsanPdf?anno=2021&codLeg=82776&parte=1%20&serie=null (accessed on 14 March 2022).
- Italian Ministry of Health. Vaccinations Web Portal. Anti-COVID-19 Vaccination Strategy. Available online: https://www.salute.gov.it/portale/nuovocoronavirus/dettaglioContenutiNuovoCoronavirus.jsp?lingua=italiano&id=5452&area=nuovoCoronavirus&menu=vuoto (accessed on 4 March 2022).
- COVID-19 on the Veneto Region: Report. Coronavirus: Cases and Vaccines, 8 March 2022. Veronasera. Available online: https://www.veronasera.it/attualita/coronavirus-covid19-Veneto-Verona-dati-bollettino-casi-vaccino-8-marzo-2022.html (accessed on 23 June 2021).
- Coronavirus Statistics. Coronavirus Statistics on the Veneto Region. Available online: https://statistichecoronavirus.it/coronavirus-italia/coronavirus-veneto/ (accessed on 4 March 2022).
- Ren, S.Y.; Wang, W.B.; Gao, R.D.; Zhou, A.M. Omicron variant (B.1.1.529) of SARS-CoV-2: Mutation, infectivity, transmission, and vaccine resistance. World J. Clin. Cases 2022, 10, 1255–1256. [Google Scholar] [CrossRef] [PubMed]
- Gowrisankar, A.; Priyanka, T.M.C.; Banerjee, S. Omicron: A mysterious variant of concern. Eur. Phys. J. Plus 2022, 137, 100. [Google Scholar] [CrossRef] [PubMed]
- Andrews, N.; Stowe, J.; Kirsebom, F.; Toffa, S.; Rickeard, T.; Gallagher, E.; Gower, C.; Kall, M.; Groves, N.; O’Connell, A.-M.; et al. COVID-19 Vaccine Effectiveness against the Omicron (B.1.1.529) Variant. N. Engl. J. Med. 2022, 386, 1532–1546. [Google Scholar] [CrossRef] [PubMed]
- Nemet, I.; Kliker, L.; Lustig, Y.; Zuckerman, N.; Erster, O.; Cohen, C.; Kreiss, Y.; Alroy-Preis, S.; Regev-Yochay, G.; Mendelson, E.; et al. Third BNT162b2 Vaccination Neutralization of SARS-CoV-2 Omicron Infection. N. Engl. J. Med. 2022, 386, 492–494. [Google Scholar] [CrossRef] [PubMed]
- Tseng, H.F.; Ackerson, B.K.; Luo, Y.; Sy, L.S.; Talarico, C.A.; Tian, Y.; Bruxvoort, K.J.; Tubert, J.E.; Florea, A.; Ku, J.H.; et al. Effectiveness of mRNA-1273 against SARS-CoV-2 Omicron and Delta variants. Nat. Med. 2022, 28, 1063–1071. [Google Scholar] [CrossRef] [PubMed]
- Italian Superior Institute of Health (ISS). Extended Report on COVID-19. COVID-19: Surveillance, Infections Impact and Vaccine Efficacy, 11/03/2022. Available online: https://www.epicentro.iss.it/coronavirus/bollettino/Bollettino-sorveglianza-integrata-COVID-19_9-marzo-2022.pdf (accessed on 14 March 2022).
- World Health Organization (WHO). Tracking SARS-CoV-2 Variants. Available online: https://www.who.int/en/activities/tracking-SARS-CoV-2-variants (accessed on 16 March 2022).
- Collie, S.; Champion, J.; Moultrie, H.; Bekker, L.G.; Gray, G. Effectiveness of BNT162b2 Vaccine against Omicron Variant in South Africa. N. Engl. J. Med. 2022, 386, 494–496. [Google Scholar] [CrossRef] [PubMed]
- Altarawneh, H.N.; Chemaitelly, H.; Ayoub, H.H.; Tang, P.; Hasan, M.R.; Yassine, H.M.; Al-Khatib, H.A.; Smatti, M.K.; Coyle, P.; Al-Kanaani, Z.; et al. Effects of Previous Infection and Vaccination on Symptomatic Omicron Infections. N. Engl. J. Med. 2022. [Google Scholar] [CrossRef] [PubMed]
- Karim, S.S.A.; Karim, Q.A. Omicron SARS-CoV-2 variant: A new chapter in the COVID-19 pandemic. Lancet 2021, 398, 2126–2128, Erratum in Lancet 2022, 399, 142. [Google Scholar] [CrossRef]
- Wang, J.; Kaperak, C.; Sato, T.; Sakuraba, A. COVID-19 reinfection: A rapid systematic review of case reports and case series. J. Investig. Med. 2021, 69, 1253–1255. [Google Scholar] [CrossRef] [PubMed]
- Cocchio, S.; Zabeo, F.; Facchin, G.; Piva, N.; Furlan, P.; Nicoletti, M.; Saia, M.; Tonon, M.; Mongillo, M.; Russo, F.; et al. The Effectiveness of a Diverse COVID-19 Vaccine Portfolio and Its Impact on the Persistence of Positivity and Length of Hospital Stays: The Veneto Region’s Experience. Vaccines 2022, 10, 107. [Google Scholar] [CrossRef] [PubMed]
- Yahav, D.; Yelin, D.; Eckerle, I.; Eberhardt, C.S.; Wang, J.; Cao, B.; Kaiser, L. Definitions for coronavirus disease 2019 reinfection, relapse and PCR re-positivity. Clin. Microbiol. Infect. 2021, 27, 315–318. [Google Scholar] [CrossRef] [PubMed]
- Experimental Zooprophylactic Institute of Venices. Diseases and Pathogens: COVID-19. Available online: https://www.izsvenezie.it/categoria/covid-19/ (accessed on 16 March 2022).
- Centers for Disease Control and Prevention. COVID Data Tracker. Available online: https://covid.cdc.gov/covid-data-tracker/#demographicsovertime (accessed on 4 March 2022).
- Saciuk, Y.; Kertes, J.; Shamir Stein, N.; Ekka Zohar, A. Effectiveness of a Third Dose of BNT162b2 mRNA Vaccine. J. Infect. Dis. 2022, 225, 30–33. [Google Scholar] [CrossRef] [PubMed]
- Altarawneh, H.N.; Chemaitelly, H.; Hasan, M.R.; Ayoub, H.H.; Qassim, S.; AlMukdad, S.; Coyle, P.; Yassine, H.M.; Al-Khatib, H.A.; Benslimane, F.M.; et al. Protection against the Omicron Variant from Previous SARS-CoV-2 Infection. N. Engl. J. Med. 2022, 386, 1288–1290. [Google Scholar] [CrossRef] [PubMed]
- Mallapaty, S. COVID reinfections surge during Omicron onslaught. Nature 2022, 10. [Google Scholar] [CrossRef] [PubMed]
- Veneto Region. Decision of the Regional Council (DGR) n. 1511, 11/11/2021. Available online: https://www.aulss3.veneto.it/index.cfm?action=mys.apridoc&iddoc=30075 (accessed on 20 March 2022).
- Veneto Region Council. Temporary Indications for the Priority Use of SARS-CoV-2 Molecular Tests, 29/12/2021. Available online: https://citynews-veronasera.stgy.ovh/~media/7262534639411/nota-tamponi-1-2.pdf (accessed on 20 March 2022).
- Pray, I.W.; Ford, L.; Cole, D.; Lee, C.; Bigouette, J.P.; Abedi, G.R.; Bushman, D.; Delahoy, M.J.; Currie, D.; Cherney, B.; et al. Performance of an Antigen-Based Test for Asymptomatic and Symptomatic SARS-CoV-2 Testing at Two University Campuses—Wisconsin, September–October 2020. MMWR Morb. Mortal Wkly. Rep. 2021, 69, 1642–1647. [Google Scholar] [CrossRef] [PubMed]
- Crotty, S. Hybrid immunity. Science 2021, 372, 1392–1393. [Google Scholar] [CrossRef]

{kind=link}
{kind=link}
| Immunity Status | Subjects (n) | Swabs (n) | Person-Days (n) | Infections (n) | Positivity Rate (%) | Incidence Rate (×10,000 Person-Days) | adjOR (95% C.I.) |
|---|---|---|---|---|---|---|---|
| No previous infection | 80,238 | 11,381 | 1,836,179 | 15,133 | 13.3 | 82.4 | Ref. |
| Infected 3+ months before baseline | 5,552 | 8,461 | 133,972 | 190 | 2.2 | 14.2 | 0.15 (0.13–0.17) |
| Infected 12+ months before baseline | 600 | 947 | 14,509 | 33 | 3.5 | 22.7 | 0.24 (0.17–0.34) |
| Infected 9 to 12 months before baseline | 3,014 | 4,789 | 72,886 | 87 | 1.8 | 11.9 | 0.13 (0.10–0.16) |
| Infected 6 to 9 months before baseline | 1,438 | 2,042 | 34,843 | 45 | 2.2 | 12.9 | 0.15 (0.11–0.20) |
| Infected 3 to 6 months before baseline | 500 | 683 | 11,734 | 15 | 2.2 | 12.8 | 0.16 (0.09–0.26) |
| Third dose within 120 days from the baseline | 16,886 | 31,911 | 419,765 | 170 | 0.5 | 4 | 0.03 (0.03–0.04) |
| Total | 102,676 | 15,418 | 2,389,916 | 15,483 | 10 | 64.8 | − |
| Immunity Status | Subjects (n) | Swabs (n) | Person-Days (n) | Infections (n) | Positivity Rate (%) | Incidence Rate (×10,000 Person-Days) | adjOR (95% C.I.) |
|---|---|---|---|---|---|---|---|
| No previous infection | 67,721 | 90,819 | 1,266,730 | 28,715 | 31.6 | 226.7 | Ref. |
| Infected 3+ months before baseline | 5,771 | 8,694 | 117,473 | 1,741 | 20 | 148.2 | 0.64 (0.61–0.67) |
| Infected 12+ months before baseline | 2,857 | 4,757 | 58,686 | 873 | 18.4 | 148.8 | 0.64 (0.59–0.68) |
| Infected 9 to 12 months before baseline | 1,424 | 1,984 | 28,742 | 436 | 22 | 151.7 | 0.67 (0.61–0.73) |
| Infected 6 to 9 months before baseline | 447 | 599 | 9,311 | 132 | 22 | 141.8 | 0.62 (0.52–0.74) |
| Infected 3 to 6 months before baseline | 1,043 | 1,354 | 20,734 | 300 | 22.2 | 144.7 | 0.64 (0.57–0.71) |
| Third dose within 120 days from the baseline | 4,253 | 7,243 | 919,823 | 1,069 | 14.8 | 116.2 | 0.53 (0.52–0.55) |
| Total | 116,022 | 17,194 | 2,304,026 | 41,146 | 23.9 | 178.6 | − |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Cocchio, S.; Zabeo, F.; Facchin, G.; Piva, N.; Venturato, G.; Marcon, T.; Saia, M.; Tonon, M.; Mongillo, M.; Da Re, F.; et al. Differences in Immunological Evasion of the Delta (B.1.617.2) and Omicron (B.1.1.529) SARS-CoV-2 Variants: A Retrospective Study on the Veneto Region’s Population. Int. J. Environ. Res. Public Health 2022, 19, 8179. https://doi.org/10.3390/ijerph19138179
Cocchio S, Zabeo F, Facchin G, Piva N, Venturato G, Marcon T, Saia M, Tonon M, Mongillo M, Da Re F, et al. Differences in Immunological Evasion of the Delta (B.1.617.2) and Omicron (B.1.1.529) SARS-CoV-2 Variants: A Retrospective Study on the Veneto Region’s Population. International Journal of Environmental Research and Public Health. 2022; 19(13):8179. https://doi.org/10.3390/ijerph19138179
Chicago/Turabian StyleCocchio, Silvia, Federico Zabeo, Giacomo Facchin, Nicolò Piva, Giovanni Venturato, Thomas Marcon, Mario Saia, Michele Tonon, Michele Mongillo, Filippo Da Re, and et al. 2022. "Differences in Immunological Evasion of the Delta (B.1.617.2) and Omicron (B.1.1.529) SARS-CoV-2 Variants: A Retrospective Study on the Veneto Region’s Population" International Journal of Environmental Research and Public Health 19, no. 13: 8179. https://doi.org/10.3390/ijerph19138179
APA StyleCocchio, S., Zabeo, F., Facchin, G., Piva, N., Venturato, G., Marcon, T., Saia, M., Tonon, M., Mongillo, M., Da Re, F., Russo, F., & Baldo, V. (2022). Differences in Immunological Evasion of the Delta (B.1.617.2) and Omicron (B.1.1.529) SARS-CoV-2 Variants: A Retrospective Study on the Veneto Region’s Population. International Journal of Environmental Research and Public Health, 19(13), 8179. https://doi.org/10.3390/ijerph19138179