
Higher Levels of Postnatal Depressive Symptomatology, Post-Traumatic Growth, and Life Satisfaction among Gay Fathers through Surrogacy in Comparison to Heterosexual Fathers: A Study in Israel in Times of COVID-19




Abstract
:1. Introduction
1.1. The Israeli Sociocultural Context
1.2. Research Hypotheses
2. Materials and Methods
2.1. Participants
2.2. Measures
2.2.1. Demographics
2.2.2. Edinburgh Postnatal Depression Scale (EPDS)
2.2.3. Satisfaction with Life Scale (SWLS)
2.2.4. Post-Traumatic Growth Inventory (PTGI-SF)
2.3. Procedure
2.4. Data Analysis
3. Results
3.1. Group Differences
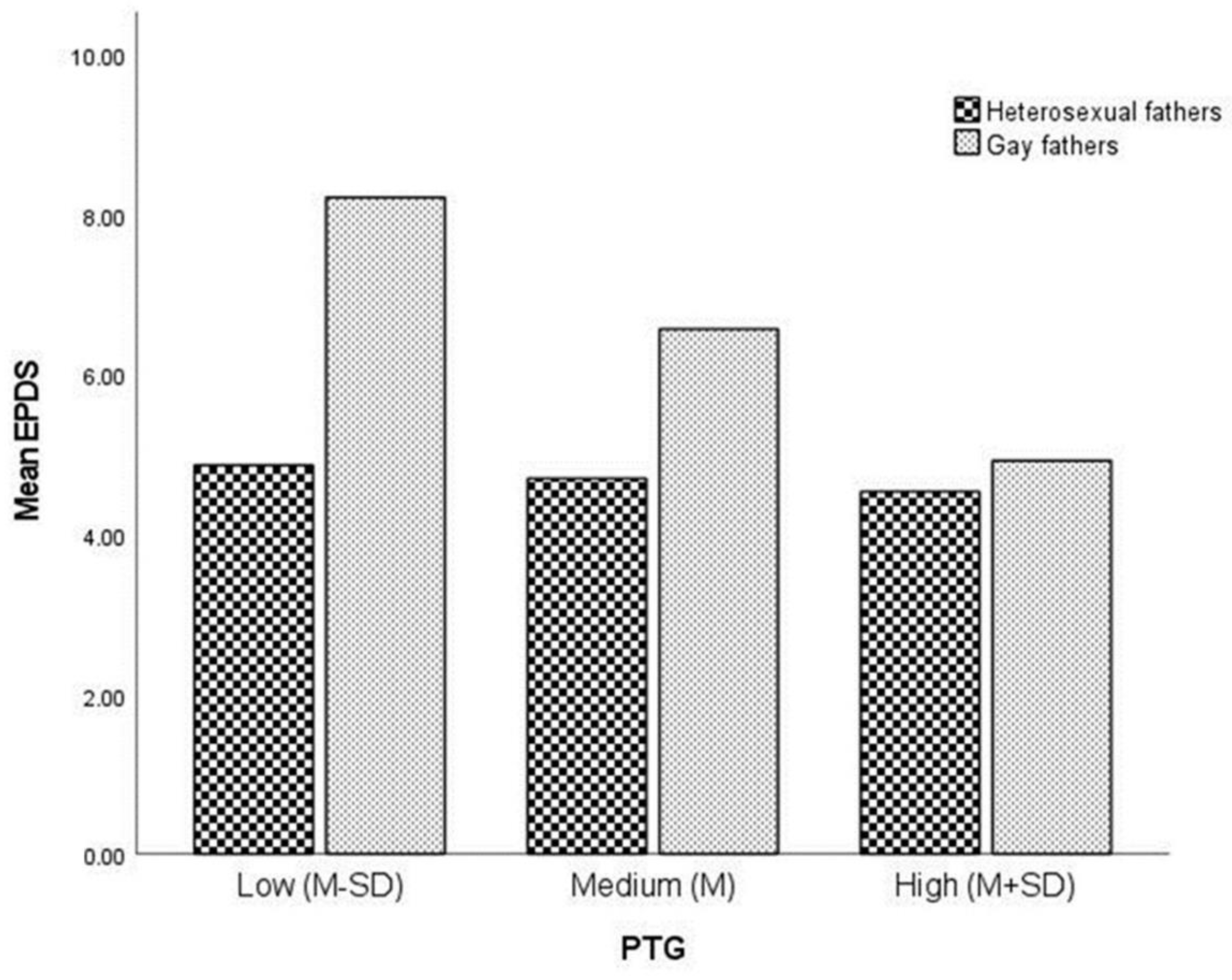
3.2. Moderating the Association between Sexual Orientation and Postnatal Depressive Symptomatology by Posttraumatic Growth
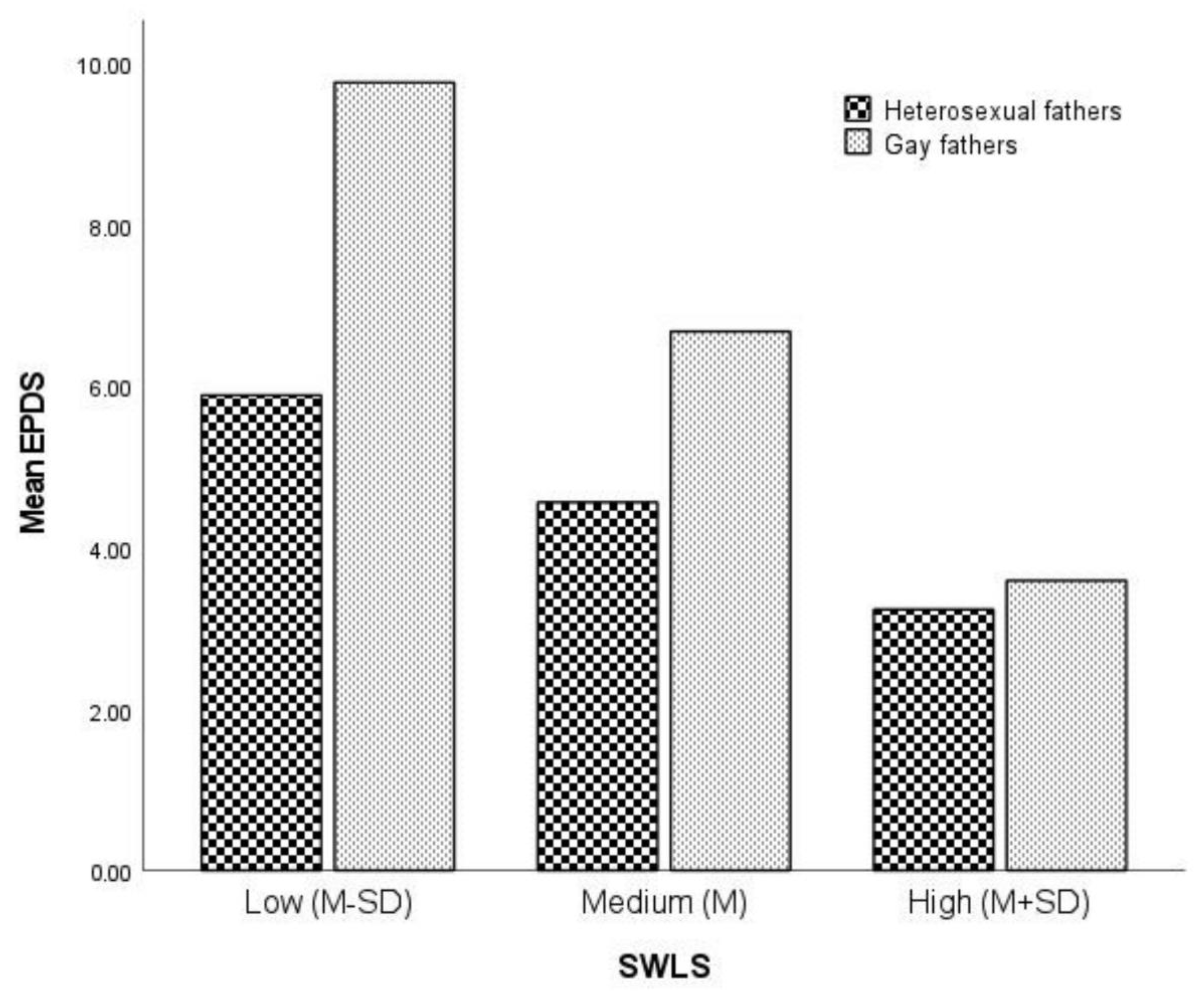
3.3. Moderating the Association between Sexual Orientation and Postnatal Depressive Symptomatology by Life Satisfaction
4. Discussion
Strengths and Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Tasker, F.; Patterson, C.J. Research on gay and lesbian parenting: Retrospect and prospect. J. GLBT Fam. Stud. 2008, 3, 9–34. [Google Scholar] [CrossRef]
- Bos, H.M.W.; Gartrell, N.K. Lesbian-mother families formed through donor insemination. In LGBTQ-Parent Families: Innovations in Research and Implications for Practice, 2nd ed.; Goldberg, A.E., Allen, K.R., Eds.; Springer: New York, NY, USA, 2020; pp. 25–44. [Google Scholar]
- Carone, N.; Bos, H.M.W.; Shenkman, G.; Tasker, F. Editorial: LGBTQ parents and their children during the family life cycle. Front. Psychol. 2021, 12, 643647. [Google Scholar] [CrossRef]
- Berkowitz, D. Gay men and surrogacy. In LGBTQ-Parent Families: Innovations in Research and Implications for Practice, 2nd ed.; Goldberg, A.E., Allen, K.R., Eds.; Springer: New York, NY, USA, 2020; pp. 143–160. [Google Scholar]
- Carone, N.; Baiocco, R.; Manzi, D.; Antoniucci, C.; Caricato, V.; Pagliarulo, E.; Lingiardi, V. Surrogacy families headed by gay men: Relationships with surrogates and egg donors, fathers’ decisions over disclosure and children’s views on their surrogacy origins. Hum. Reprod. 2018, 33, 248–257. [Google Scholar] [CrossRef]
- Shenkman, G.; Siboni, O.; Taker, F.; Costa, P. Pathways to fatherhood: Psychological welfare among Israeli gay fathers through surrogacy, gay fathers through previous heterosexual relationships, and heterosexual fathers. Front. Psychol. 2020, 11, 91. [Google Scholar] [CrossRef] [Green Version]
- Shenkman, G.; Carone, N.; Mouton, B.; d’Amore, D.; Bos, H.M.W. Assisted conception socialization self-efficacy among Israeli lesbian, gay, and heterosexual parent families and its association with child externalizing problems. J. Child Fam. Stud. 2022. [Google Scholar] [CrossRef]
- Lamb, M.E.; Lewis, C. The development and significance of father–child relationships in two-parent families. In The Role of the Father in Child Development, 5th ed.; Lamb, M.E., Ed.; Wiley: Hoboken, NJ, USA, 2010; pp. 94–153. [Google Scholar]
- Disabato, D.J.; Goodman, F.R.; Kashdan, T.B.; Short, J.L.; Jarden, A. Different types of well-being? A cross-cultural examination of hedonic and eudaimonic well-being. Psychol. Assess. 2016, 28, 471–482. [Google Scholar] [CrossRef] [Green Version]
- Shenkman, G.; Shmotkin, D. “Kids are joy”: Psychological welfare among Israeli gay fathers. J. Fam. Issues 2014, 35, 1926–1939. [Google Scholar] [CrossRef]
- Shenkman, G.; Shmotkin, D. Self-perceived parental role and mental health concomitants among Israeli gay and heterosexual fathers. J. Homosex. 2020, 67, 712–732. [Google Scholar] [CrossRef]
- Nomaguchi, K.; Milkie, M.A. Parenthood and well-being: A decade in review. J. Marriage Fam. 2020, 82, 198–223. [Google Scholar] [CrossRef]
- Lévesque, S.; Bisson, V.; Charton, L.; Fernet, M. Parenting and relational well-being during the transition to parenthood: Challenges for first-time parents. J. Child Fam. Stud. 2020, 29, 1938–1956. [Google Scholar] [CrossRef]
- Vigod, S.N.; Villegas, L.; Dennis, C.L.; Ross, L.E. Prevalence and risk factors for postpartum depression among women with preterm and low-birth-weight infants: A systematic review. BJOG Int. J. Obstet. Gynaecol. 2010, 117, 540–550. [Google Scholar] [CrossRef]
- Eddy, B.; Poll, V.; Whiting, J.; Clevesy, M. Forgotten fathers: Postpartum depression in men. J. Fam. Issues 2019, 40, 1001–1017. [Google Scholar] [CrossRef]
- Hahn-Holbrook, J.; Cornwell-Hinrichs, T.; Anaya, I. Economic and health predictors of national postpartum depression prevalence: A systematic review, meta-analysis, and meta-regression of 291 studies from 56 countries. Front. Psychiatry 2018, 8, 248. [Google Scholar] [CrossRef] [Green Version]
- Rao, W.W.; Zhu, X.M.; Zong, Q.Q.; Zhang, Q.; Hall, B.J.; Ungvari, G.S.; Xiang, Y.T. Prevalence of prenatal and postpartum depression in fathers: A comprehensive meta-analysis of observational surveys. J. Affect. Disord. 2020, 263, 491–499. [Google Scholar] [CrossRef]
- Goodman, J.H. Postpartum depression beyond the early postpartum period. J. Obstet. Gynecol. Neonatal. Nurs. 2004, 33, 410–420. [Google Scholar] [CrossRef]
- Ramchandani, P.G.; Stein, A.; O’Connor, T.G.; Heron, J.O.N.; Murray, L.; Evans, J. Depression in men in the postnatal period and later child psychopathology: A population cohort study. J. Am. Acad. Child. Adolesc. Psychiatry 2008, 47, 390–398. [Google Scholar] [CrossRef] [Green Version]
- Erez, C.; Shenkman, G. Gay dads are happier: Subjective well-being among gay and heterosexual fathers. J. GLBT Fam. Stud. 2016, 12, 451–467. [Google Scholar] [CrossRef]
- Shenkman, G.; Ifrah, K.; Shmotkin, D. Meaning in life among middle-aged and older gay and heterosexual fathers. J. Fam. Issues 2018, 39, 2155–2173. [Google Scholar] [CrossRef]
- Shenkman, G.; Segal-Engelchin, D.; Taubman-Ben-Ari, O. What we know and what remains to be explored about LGBTQ parent families in Israel: A sociocultural perspective. Int. J. Environ. Res. Public Health 2022, 19, 4355. [Google Scholar] [CrossRef]
- Shenkman, G.; Shmotkin, D. The association between self-perceived parental role and meaning in life among gay and heterosexual fathers. J. Fam. Psychol. 2016, 30, 552–561. [Google Scholar] [CrossRef]
- Tsfati, M.; Ben-Ari, A. Between the social and the personal: Israeli male gay parents, surrogacy and socio-political concepts of parenthood and gender. J. GLBT Fam. Stud. 2019, 15, 42–57. [Google Scholar] [CrossRef]
- Van Rijn-van Gelderen, L.; Bos, H.M.W.; Jorgensen, T.D.; Ellis-Davies, K.; Winstanley, A.; Golombok, S.; Rubio, B.; Gross, M.; Vecho, O.; Lamb, M.E. Well-being of gay fathers with children born through surrogacy: A comparison with lesbian-mother families and heterosexual IVF parent families. Hum. Reprod. 2018, 33, 101–108. [Google Scholar] [CrossRef] [Green Version]
- Frost, D.M. Social stigma and its consequences for the socially stigmatized. Soc. Personal. Psychol. Compass 2011, 5, 824–839. [Google Scholar] [CrossRef]
- King, M.; Semlyen, J.; Tai, S.; Killaspy, H.; Osborn, D.; Popelyuk, D.; Nazareth, I. A systematic review of mental disorder, suicide, and deliberate self-harm in lesbian, gay and bisexual people. BMC Psychiatry 2008, 8, 70. [Google Scholar] [CrossRef] [Green Version]
- Meyer, I.H. Prejudice, social stress, and mental health in lesbian, gay, and bisexual populations: Conceptual issues and research evidence. Psychol. Bull. 2003, 129, 674–697. [Google Scholar] [CrossRef]
- Radloff, L.S. The CES-D Scale: A self-report depression scale for research in the general population. Appl. Psychol. Meas. 1977, 1, 385–401. [Google Scholar] [CrossRef]
- Rizzo, R.; Piccinelli, M.; Mazzi, M.A.; Bellantuono, C.; Tansella, M. The Personal Health Questionnaire: A new screening instrument for detection of ICD-10 depressive disorders in primary care. Psychol. Med. 2000, 30, 831–840. [Google Scholar] [CrossRef]
- Carone, N.; Manzi, D.; Barone, L.; Lingiardi, V.; Baiocco, R.; Bos, H.M. Father–child bonding and mental health in gay fathers using cross-border surrogacy during the COVID-19 pandemic. Reprod. Biomed. Online 2021, 43, 756–764. [Google Scholar] [CrossRef]
- Edmondson, O.J.; Psychogiou, L.; Vlachos, H.; Netsi, E.; Ramchandani, P.G. Depression in fathers in the postnatal period: Assessment of the Edinburgh Postnatal Depression Scale as a screening measure. J. Affect. Disord. 2010, 125, 365–368. [Google Scholar] [CrossRef] [Green Version]
- Cox, J.L.; Holden, J.M.; Sagovsky, R. Detection of postnatal depression: Development of the 10-item Edinburgh Postnatal Depression Scale. Br. J. Psychiatry 1987, 150, 782–786. [Google Scholar] [CrossRef] [Green Version]
- Ryff, C.D.; Singer, B.H. Know thyself and become what you are: A eudaimonic approach to psychological well-being. J. Happiness Stud. 2008, 9, 13–39. [Google Scholar] [CrossRef]
- Porat-Zyman, G.; Taubman-Ben-Ari, O.; Spielman, V. Dyadic transition to parenthood: A longitudinal assessment of personal growth among parents of pre- and full-term infants. Stress Health 2017, 33, 24–34. [Google Scholar] [CrossRef] [Green Version]
- Sawyer, A.; Ayers, S.; Young, D.; Bradley, R.; Smith, H. Posttraumatic growth after childbirth: A prospective study. Psychol. Health 2012, 27, 362–377. [Google Scholar] [CrossRef]
- Taubman-Ben-Ari, O. First-time parents’ personal growth: Role of parental separation anxiety. Health Soc. Care Community 2022. [Google Scholar] [CrossRef]
- Taubman-Ben-Ari, O.; Spielman, V. Personal growth following the first child’s birth: A comparison of parents of pre- and full-term babies. Soc. Work Res. 2014, 38, 91–106. [Google Scholar] [CrossRef]
- Cox, M.J.; Paley, B. Families as systems. Annu. Rev. Psychol. 1997, 48, 243–267. [Google Scholar] [CrossRef]
- Birenbaum-Carmeli, D.; Dirnfeld, M. The more the better? IVF policy in Israel and women’s views. Reprod. Health Matters 2008, 16, 182–191. [Google Scholar] [CrossRef]
- OECD. Society at a Glance 2019: OECD Social Indicators; OECD Publishing: Paris, France, 2019. [Google Scholar] [CrossRef]
- Birenbaum-Carmeli, D. Thirty-five years of assisted reproductive technologies in Israel. Reprod. Biomed. Soc. Online 2016, 2, 16–23. [Google Scholar] [CrossRef] [Green Version]
- Costa, P.A.; Shenkman, G. LGBT parent families in non-Western contexts. In LGBTQ-Parent Families: Innovations in Research and Implications for Practice, 2nd ed.; Goldberg, A.E., Allen, K.R., Eds.; Springer: New York, NY, USA, 2020; pp. 319–336. [Google Scholar]
- Tsfati, M.; Nadan, Y.; Biton, N.; Serdtse, Y. Fatherhood as a spatial-contextual phenomenon: Israeli gay fathers through surrogacy. Men Masc. 2021, 24, 590–610. [Google Scholar] [CrossRef]
- Gross, A. The politics of LGBT rights in Israel and beyond: Nationality, normativity & queer politics. Colomb. Hum. Rights Law Rev. 2014, 46, 82–151. [Google Scholar]
- Shenkman, G.; Ifrah, K.; Shmotkin, D. Interpersonal vulnerability and its association with depressive symptoms among gay and heterosexual men. Sex. Res. Social Policy 2020, 17, 199–208. [Google Scholar] [CrossRef]
- Shenkman, G.; Shmotkin, D. The hostile-world scenario among Israeli homosexual adolescents and young adults. J. Appl. Soc. Psychol. 2013, 43, 1408–1417. [Google Scholar] [CrossRef]
- Shenkman, G. Anticipation of stigma upon parenthood impacts parenting aspirations in the LGB community in Israel. Sex. Res. Social Policy 2021, 18, 753–764. [Google Scholar] [CrossRef]
- Thartori, E.; Pastorelli, C.; Cirimele, F.; Remondi, C.; Gerbino, M.; Basili, E.; Favini, E.; Lunetti, C.; Fiasconaro, I.; Caprara, G.V. Exploring the protective function of positivity and regulatory emotional self-efficacy in time of pandemic COVID-19. Int. J. Environ. Res. Public Health 2021, 18, 13171. [Google Scholar] [CrossRef]
- Kinsey, A.C.; Pomeroy, W.B.; Martin, C.E. Sexual Behavior in the Human Male; Saunders: Oxford, UK, 1948. [Google Scholar]
- Bina, R.; Harrington, D. Differential predictors of postpartum depression and anxiety: The Edinburgh postnatal depression scale Hebrew version two factor structure construct validity. Matern. Child Health J. 2017, 21, 2237–2244. [Google Scholar] [CrossRef]
- Matthey, S.; Barnett, B.; Kavanagh, D.J.; Howie, P. Validation of the Edinburgh Postnatal Depression Scale for men, and comparison of item endorsement with their partners. J. Affect. Disord. 2001, 64, 175–184. [Google Scholar] [CrossRef]
- Diener, E.; Emmons, R.A.; Larsen, R.J.; Griffin, G. The satisfaction with life scale. J. Pers. Assess. 1985, 49, 71–75. [Google Scholar] [CrossRef]
- Shenkman, G.; Shmotkin, D. Mental health among Israeli homosexual adolescents and young adults. J. Homosex. 2010, 58, 97–116. [Google Scholar] [CrossRef]
- Shenkman, G.; Stein, Y.; Bos, H. The mediating role of attachment avoidance in the association between sexual orientation and mental Health. J. Homosex. 2021, 68, 461–475. [Google Scholar] [CrossRef]
- Cann, A.; Calhoun, L.G.; Tedeschi, R.G.; Taku, K.; Vishnevsky, T.; Triplett, K.N.; Danhauer, S.C. A short form of the Posttraumatic Growth Inventory. Anxiety Stress Coping 2010, 23, 127–137. [Google Scholar] [CrossRef]
- Taubman–Ben-Ari, O.; Findler, L.; Sharon, N. Personal growth in mothers: Examination of the suitability of the posttraumatic growth inventory as a measurement tool. Women Health 2011, 51, 604–622. [Google Scholar] [CrossRef]
- Faul, F.; Erdfelder, E.; Buchner, A.; Lang, A.G. Statistical power analyses using G* Power 3.1: Tests for correlation and regression analyses. Behav. Res. Methods 2009, 41, 1149–1160. [Google Scholar] [CrossRef] [Green Version]
- Altman, D.G. Statistics in medical journals. Stat. Med. 1982, 1, 59–71. [Google Scholar] [CrossRef]
- Hayes, A.F. An Introduction to Mediation, Moderation, and Conditional Process Analysis: A Regression-Based Approach, 2nd ed.; Guilford: New York, NY, USA, 2018. [Google Scholar]
- Aiken, L.S.; West, S.G. Multiple Regression: Testing and Interpreting Interactions; Sage Publications: Thousand Oaks, CA, USA, 1991. [Google Scholar]
- Ziv, I.; Freund-Eschar, Y. The pregnancy experience of gay couples expecting a child through overseas surrogacy. Fam. J. 2015, 23, 158–166. [Google Scholar] [CrossRef]
- Lustenberger, S. “We are citizens”—Vulnerability and privilege in the experiences of Israeli gay men with surrogacy in India. J. Comp. Fam. Stud. 2017, 48, 393–403. [Google Scholar] [CrossRef]
- Shenkman, G.; Shrira, A.; Ifrah, K.; Shmotkin, D. Interpersonal vulnerability among offspring of Holocaust survivors gay men and its association with depressive symptoms and life satisfaction. Psychiatry Res. 2018, 259, 89–94. [Google Scholar] [CrossRef]
- Shmotkin, D. Happiness in face of adversity: Reformulating the dynamic and modular bases of subjective well-being. Rev. Gen. Psychol. 2005, 9, 291–325. [Google Scholar] [CrossRef]
- Shmotkin, D.; Shrira, A. On the distinction between subjective well-being and meaning in life: Regulatory versus reconstructive functions in the face of a hostile world. In The Human Quest for Meaning: A Handbook of Psychological Research and Clinical Applications, 2nd ed.; Wong, T.P., Ed.; Routledge: New York, NY, USA, 2021; pp. 143–163. [Google Scholar]
- Fish, J.N.; Russell, S.T. Queering methodologies to understand queer families. Fam. Relat. 2018, 67, 12–25. [Google Scholar] [CrossRef]
- Hatzenbuehler, M.L.; McLaughlin, K.A.; Keyes, K.M.; Hasin, D.S. The impact of institutional discrimination on psychiatric disorders in lesbian, gay, and bisexual populations: A prospective study. Am. J. Public Health. 2010, 100, 452–459. [Google Scholar] [CrossRef]
- Shenkman, G. Winds of change: Will current amendments to Israeli laws discriminating against LGBTQ+ individuals positively affect their mental health? Psychiatry Res. 2022, 313, 114607. [Google Scholar] [CrossRef]

{kind=link}
{kind=link}
| Sociodemographic Variables | Gay Fathers (N = 47) | Heterosexual Fathers (N = 70) | F/Chi-Square | p | ||
|---|---|---|---|---|---|---|
| M (SD), Range | N (%) | M (SD), Range | N (%) | |||
| Age | 37.2 (4.2), 29–46 | 34.5 (4.2), 23–47 | 10.8 | 0.001 | ||
| Age of youngest child (in months) | 10.2 (8.2), 0–36 | 11.2 (8.8), 0–36 | 0.5 | 0.462 | ||
| Academic education a | 42 (89) | 62 (89) | 0.0 | 0.894 | ||
| Above average income b | 36 (77) | 46 (66) | 1.6 | 0.208 | ||
| Number of children | 1.6 (1.0), 1–8 | 1.7 (1.0), 1–8 | 0.1 | 0.771 | ||
| In a romantic relationship c | 67 (98.5) | 98 (99) | FET | 1.000 | ||
| Study Variables | Gay Fathers (N = 68) | Heterosexual Fathers (N = 99) | F | |||
| EPDS | 6.1 (5.0), 0–21 | 4.7 (3.8), 0–18 | 4.1 | 0.044 | ||
| SWLS | 5.4 (1.0), 2.4–7.0 | 5.2 (0.9), 2.4–7.0 | 3.8 | 0.053 | ||
| PTGI | 3.9 (0.7), 1.5–5.5 | 3.5 (0.9), 1.1–5.8 | 8.9 | 0.003 | ||
| Predictor | B | t | p |
|---|---|---|---|
| Group a | 8.1 | 2.5 | 0.014 |
| PTGI | −0.2 | −0.4 | 0.692 |
| Group by PTGI | −1.7 | −2.0 | 0.047 |
| Estimated at PTGI | Effect | t | p |
|---|---|---|---|
| Low level 2.8 | 3.3 | 3.1 | 0.002 |
| Medium level 3.7 | 1.9 | 2.7 | 0.008 |
| High level 4.6 | 0.4 | 0.4 | 0.684 |
| Predictor | B | t | p |
|---|---|---|---|
| Group a | 12.0 | 5.3 | <0.001 |
| SWLS | −1.4 | −3.3 | 0.001 |
| Group by SWLS | −1.9 | −3.0 | 0.003 |
| Estimated at SWLS | Effect | t | p |
|---|---|---|---|
| Low level 4.3 | 3.9 | 4.6 | <0.001 |
| Medium level 5.3 | 2.1 | 3.6 | <0.001 |
| High level 6.2 | 0.3 | 0.4 | 0.664 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Shenkman, G.; Levy, S.; Winkler, Z.B.-D.; Bass, D.; Geller, S. Higher Levels of Postnatal Depressive Symptomatology, Post-Traumatic Growth, and Life Satisfaction among Gay Fathers through Surrogacy in Comparison to Heterosexual Fathers: A Study in Israel in Times of COVID-19. Int. J. Environ. Res. Public Health 2022, 19, 7946. https://doi.org/10.3390/ijerph19137946
Shenkman G, Levy S, Winkler ZB-D, Bass D, Geller S. Higher Levels of Postnatal Depressive Symptomatology, Post-Traumatic Growth, and Life Satisfaction among Gay Fathers through Surrogacy in Comparison to Heterosexual Fathers: A Study in Israel in Times of COVID-19. International Journal of Environmental Research and Public Health. 2022; 19(13):7946. https://doi.org/10.3390/ijerph19137946
Chicago/Turabian StyleShenkman, Geva, Sigal Levy, Ziv Ben-Dor Winkler, Doriel Bass, and Shulamit Geller. 2022. "Higher Levels of Postnatal Depressive Symptomatology, Post-Traumatic Growth, and Life Satisfaction among Gay Fathers through Surrogacy in Comparison to Heterosexual Fathers: A Study in Israel in Times of COVID-19" International Journal of Environmental Research and Public Health 19, no. 13: 7946. https://doi.org/10.3390/ijerph19137946
APA StyleShenkman, G., Levy, S., Winkler, Z. B.-D., Bass, D., & Geller, S. (2022). Higher Levels of Postnatal Depressive Symptomatology, Post-Traumatic Growth, and Life Satisfaction among Gay Fathers through Surrogacy in Comparison to Heterosexual Fathers: A Study in Israel in Times of COVID-19. International Journal of Environmental Research and Public Health, 19(13), 7946. https://doi.org/10.3390/ijerph19137946