
A Psychoeducational Intervention in Prenatal Classes: Positive Effects on Anxiety, Self-Efficacy, and Temporal Focus in Birth Attendants

 ,
,  ,
,  , ,
, , 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Sample
2.3. Procedures
2.4. Instruments
2.5. Statistical Analysis
3. Results
4. Discussion
5. Limitations and Suggestions
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Kessler, R.C.; McConagle, K.A.; Zhao, S.; Nelson, C.B.; Hughes, M.; Eshleman, S.; Wittchen, H.U.; Kendler, K.S. Lifetime and 12-month prevalence of DSM-III-R psychiatric disorders in the United States. Results from the National Comorbidity Survey. Arch. Gen. Psychiatry 1994, 51, 8–19. [Google Scholar] [CrossRef] [PubMed]
- Rapee, R.M. The development of generalized anxiety. In The Developmental Psychopathology of Anxiety; Dadds, M.R., Vasey, M.W., Eds.; Oxford University Press: London, UK, 2001. [Google Scholar]
- Martini, J.; Knappe, S.; Beesdo-Baum, K.; Lieb, R.; Wittchen, H.U. Anxiety disorders before birth and self-perceived distress during pregnancy: Associations with maternal depression and obstetric, neonatal and early childhood outcomes. Early Hum. Dev. 2010, 86, 305–310. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Reck, C.; Struben, K.; Backenstrass, M.; Stefenelli, U.; Reinig, K.; Fuchs, T.; Sohn, C.; Mundt, C. Prevalence, onset and comorbidity of post-partum anxiety and depressive disorders. Acta Psychiatr. Scand. 2008, 118, 459–468. [Google Scholar] [CrossRef] [PubMed]
- Biaggi, A.; Conroy, S.; Pawlby, S.; Pariante, C.M. Identifying the women at risk of antenatal anxiety and depression: A systematic review. J. Affect. Disord. 2016, 191, 62–77. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dennis, C.L.; Falah-Hassani, K.; Shiri, R. Prevalence of antenatal and postnatal anxiety: Systematic review and meta-analysis. Br. J. Psychiatry 2017, 210, 315–323. [Google Scholar] [CrossRef]
- Fawcett, E.J.; Fairbrother, N.; Cox, M.L.; White, I.R.; Fawcett, J.M. The prevalence of anxiety disorders during pregnancy and the postpartum period: A multivariate Bayesian meta-analysis. J. Clin. Psychiatry 2019, 80, 1181. [Google Scholar] [CrossRef]
- Gelaye, B.; Rondon, M.B.; Araya, R.; Williams, M.A. Epidemiology of maternal depression, risk factors, and child outcomes in low-income and middle-income countries. Lancet Psychiatry 2016, 3, 973–982. [Google Scholar] [CrossRef] [Green Version]
- Jomeen, J.; Martin, C.R. A mixed-methods approach to understanding women’s worries during early pregnancy. Health Psychol. Update 2005, 14, 17–27. [Google Scholar]
- Barimani, M.; Vikstrom, A.; Rosander, M.; Forslund Frykedal, K.; Berlin, A. Facilitating and inhibiting factors in transition to parenthood—Ways in which health professionals can support parents. Scand. J. Caring Sci. 2017, 31, 537–546. [Google Scholar] [CrossRef]
- Krysa, J.; Iwanowicz-Palus, G.; Bien, A.; Rzońca, E.; Zarajczyk, M. Antenatal classes as a form of preparation for parenthood: Analysis of benefits of participating in prenatal education. Pol. J. Public Health 2016, 126, 192–196. [Google Scholar] [CrossRef] [Green Version]
- Deave, T.; Johnson, D. The transition to parenthood: What does it mean for fathers? J. Adv. Nurs. 2008, 63, 626–633. [Google Scholar] [CrossRef] [PubMed]
- Fagerskiold, A. A change in life as experienced by first-time fathers. Scand. J. Caring Sci. 2008, 22, 64–71. [Google Scholar] [CrossRef]
- Premberg, A.; Hellstrom, A.L.; Berg, M. Experiences of the first year as father. Scand. J. Caring Sci. 2008, 22, 56–63. [Google Scholar] [CrossRef] [PubMed]
- Leahy Warren, P. First-time mothers: Social support and confidence in infant care. J. Adv. Nurs. 2005, 50, 479–488. [Google Scholar] [CrossRef] [PubMed]
- Nystrom, K.; Ohrling, K. Parenthood experiences during the child’s first year: Literature review. J. Adv. Nurs. 2004, 46, 319–330. [Google Scholar] [CrossRef]
- Ammaniti, M. La Gravidanza tra Fantasia e Realtà; Il Pensiero Scientifico: Roma, Italy, 1992. [Google Scholar]
- Brunton, R.J.; Dryer, R.; Saliba, A.; Kohlhoff, J. Pregnancy anxiety: A systematic review of current scales. J. Affect. Disord. 2015, 176, 24–34. [Google Scholar] [CrossRef]
- Miloyan, B.; Pachana, N.A.; Suddendorf, T. The future is here: A review of foresight systems in anxiety and depression. Cogn. Emot. 2014, 28, 795–810. [Google Scholar] [CrossRef]
- Bluedorn, A.C. The Human Organization of Time: Temporal Realities and Experience; Stanford Business Books: Stanford, CA, USA, 2002. [Google Scholar]
- Rappaport, H. Marking Time; Simon & Schuster: New York, NY, USA, 1990. [Google Scholar]
- Nuttin, J.; Lens, W. Future Time Perspective and Motivation; Leuven University Press and Lawrence Erlbaum Associates: Leuven & Hillsdale, NJ, USA, 1985. [Google Scholar]
- Wheeler, M.A.; Stuss, D.T.; Tulving, E. Toward a theory of episodic memory: The frontal lobes and autonoetic consciousness. Psychol. Bull. 1997, 121, 331–354. [Google Scholar] [CrossRef]
- Murray, H.A. Explorations in Personality: A Clinical and Experimental Study of Fifty Men of College Age; Oxford University Press: New York, NY, USA; London, UK, 1938. [Google Scholar]
- Heron, J.; O’Connor, T.G.; Evans, J.; Golding, J.; Glover, V. The course of anxiety and depression through pregnancy and the postpartum in a community sample. J. Affect. Disord. 2004, 80, 65–73. [Google Scholar] [CrossRef]
- Brandt, R.; da Silveira Viana, M.; Crocetta, T.B.; Andrade, A. Association between mood states and performance of Brazilian elite sailors: Winners vs. non-winners. Cult. Cienc. Deporte 2016, 11, 119–125. [Google Scholar] [CrossRef] [Green Version]
- Rondung, E.; Ekdahl, J.; Hildingsson, I.; Rubertsson, C.; Sundin, Ö. Heterogeneity in childbirth related fear or anxiety. Scand. J. Psychol. 2018, 59, 634–643. [Google Scholar] [CrossRef] [PubMed]
- Bandura, A. Social cognitive theory: An agentic perspective. Annu. Rev. Psychol. 2001, 52, 1–26. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cottle, T.J. Perceiving Time: A Psychological Investigation with Men and Women; Wiley: New York, NY, USA, 1976. [Google Scholar]
- Fried, Y.; Slowik, L.H. Enriching goal-setting theory with time: An integrated approach. Acad. Manag. Rev. 2004, 29, 404–442. [Google Scholar] [CrossRef]
- Yuliana, A.; Murti, B.; Prasetya, H. The Effect of Antenatal Class on Birth and Parenting Preparedness: A Path Analysis Evidence from Salatiga, Central Java. In Proceedings of the 4th International Conference on Public Health 2018. Masters Program in Public Health, Universitas Sebelas Maret, Solo, Indonesia, 29–30 August 2018. [Google Scholar] [CrossRef]
- Sanna, L.J.; Stocker, S.L.; Clarke, J.A. Rumination, imagination, and personality: Specters of the past and future in the present. In Virtue, Vice, and Personality: The Complexity of Behavior; Chang, E.C., Sanna, L.J., Eds.; American Psychological Association: Washington, DC, USA, 2003; pp. 105–124. [Google Scholar]
- Carver, C.S.; Scheier, M.F. Control theory: A useful conceptual framework for personality-social, clinical, and health psychology. Psychol. Bull. 1982, 92, 111–135. [Google Scholar] [CrossRef]
- Weick, K.E. The Social Psychology of Organizing, 2nd ed.; McGraw-Hill: New York, NY, USA, 1979. [Google Scholar]
- Wilson, A.E.; Ross, M. The identity function of autobiographical memory: Time Is Our Side. Memory 2003, 11, 137–149. [Google Scholar] [CrossRef]
- Bird, B. Implementing entrepreneurial ideas: The case for intention. Acad. Manag. Rev. 1988, 13, 442–453. [Google Scholar] [CrossRef]
- Das, T.K. Strategic planning and individual temporal orientation. Strateg. Manag. J. 1987, 8, 203–209. [Google Scholar] [CrossRef]
- Li, H.; Cao, Y. The hope of the future: The experience of pregnancy influences women’s implicit space-time mappings. J. Soc. Psychol. 2018, 158, 152–156. [Google Scholar] [CrossRef]
- Bolotova, K.A.; Hachaturova, R.M. The role of time perspective in coping behaviour. Psychol. Russ. State Art 2013, 6, 120–131. [Google Scholar] [CrossRef] [Green Version]
- Oyanadel, C.; Buela-Casal, G. Time perception and psychopathology: Influence of time perspective on quality of life of severe mental illness. Actas Españolas Psiquiatr. 2014, 42, 99–107. [Google Scholar]
- Åström, E.; Wiberg, B.; Sircova, A.; Wiberg, M.; Carelli, M.G. Insights into features of anxiety through multiple aspects of psychological time. J. Integr. Psychol. Ther. 2014, 2, 3. [Google Scholar] [CrossRef]
- Papastamatelou, J.; Unger, A.; Giotakos, O.; Athanasiadou, F. Is Time Perspective a Predictor of Anxiety and Perceived Stress? Some Preliminary Results from Greece. Psychol. Stud. 2015, 60, 468–477. [Google Scholar] [CrossRef]
- Zimbardo, P.G.; Sword, R.M.; Sword, R.K.M. The Time Cure: Overcoming PTSD with the New Psychology of Time Perspective Therapy; Jossey-Bass: San Francisco, CA, USA, 2012. [Google Scholar]
- Yuksel, F.; Akin, S.; Durna, Z. Prenatal distress in Turkish pregnant women and factors associated with maternal prenatal distress. J. Nurs. Clinic. 2014, 23, 54–64. [Google Scholar] [CrossRef] [PubMed]
- Horvath Marques, A.; O’Connor, T.G.; Roth, C.; Susser, E.; Bjørke-Monsen, A.L. The influence of maternal prenatal and early childhood nutrition and maternal prenatal stress on offspring immune system development and neurodevelopmental disorders. Front. Neurosci. 2013, 7, 120. [Google Scholar]
- Qiao, Y.; Wang, J.; Li, J.; Wang, J. Effects of depressive and anxiety symptoms during pregnancy o pregnant, obstetric and neonatal outcomes: A follow-up study. J. Obstet. Gynaecol. 2012, 32, 237–240. [Google Scholar] [CrossRef] [PubMed]
- Fishell, A. Depression and Anxiety in Pregnancy. J. Popul. Ther. Clin. Pharmachology 2010, 17. Available online: https://www.jptcp.com/index.php/jptcp/article/view/513 (accessed on 24 May 2022).
- Talge, N.M.; Neal, C.; Glover, V. The Early Stress, Translational Research and Prevention Science Network: Fetal and neonatal experience on child and adolescent mental health. Antenatal maternal stressand long-term effects on child neurodevelopment: How and why? J. Child Psychol. Psychiatry 2007, 48, 245–261. [Google Scholar] [CrossRef]
- Edhborg, M.; Nasreen, H.E.; Kabir, Z.N. Impact of postpartum depressive and anxiety symptoms on mothers’ emotional tie to their infants 2–3 months postpartum: A population-based study from rural Bangladesh. Arch. Women’s Ment. Health 2011, 14, 307–316. [Google Scholar] [CrossRef]
- Cantwell, R.; Cox, J.L. Psychiatric disorders in pregnancy and the puerperium. Curr. Obstet. Gynaecol. 2003, 13, 7–13. [Google Scholar] [CrossRef]
- Clark, A.; Skouteris, H.; Wertheim, E.H.; Paxton, S.J.; Milgrom, J. My baby body: A qualitative insight into women’s body related experiences and mood during pregnancy and the postpartum. J. Reprod. Infant Psychol. 2009, 27, 330–345. [Google Scholar] [CrossRef] [Green Version]
- Wijma, K. Why focus on fear of childbirth? J. Psychosom. Obstet. Gynecol. 2003, 24, 141–143. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bewley, S.; Cockburn, J. Responding to fear of childbirth. Lancet 2002, 359, 2128–2129. [Google Scholar] [CrossRef]
- Kacperczyk-Bartnik, J.; Bartnik, P.; Symonides, A.; Sroka-Ostrowska, N.; Dobrowolska-Redo, A.; Romejko-Wolniewicz, E. Association between antenatal classes attendance and perceived fear and pain during labour. Taiwan J. Obstet. Gynecol. 2019, 58, 492–496. [Google Scholar] [CrossRef] [PubMed]
- Gregory, E. Do antenatal classes do enough to prepare parents for when things go wrong? J. Paediatr. Child Health 2012, 48, 717–720. [Google Scholar] [CrossRef] [Green Version]
- Andrade, A.; Bevilacqua, G.G.; Coimbra, D.R.; Pereira, F.S.; Brandt, R. Sleep quality, mood and performance: A study of elite Brazilian volleyball athletes. J. Sports Sci. Med. 2016, 15, 601. [Google Scholar]
- Brixval, C.S.; Axelsen, S.F.; Andersen, S.K.; Due, P.; Koushede, V. The effect of antenatal education in small classes on obstetric and psycho-social outcomes: A systematic review and meta-analysis protocol. Syst. Rev. 2014, 4, 20. [Google Scholar] [CrossRef] [Green Version]
- World Health Organization (WHO) Regional Office for Europe’s Health Evidence Network (HEN). Programmes and Projects, What Is the Effectiveness of Antenatal Care? (Supplement). 2005. Available online: http://www.euro.who.int/Document/E87997.pdf (accessed on 22 April 2022).
- Forslund Frykedal, K.; Rosander, M.; Berlin, A.; Barimani, M. With or without the group: Swedish midwives’ and child healthcare nurses’ experiences in leading parent education groups. Health Promot. Int. 2015, 31, 899–907. [Google Scholar] [CrossRef] [Green Version]
- Lima-Pereira, P.; Bermudez-Tamayo, C.; Jasienska, G. Use of the Internet as a source of health information amongst participants of antenatal classes. J. Clin. Nurs. 2012, 21, 322–330. [Google Scholar] [CrossRef]
- Toohill, J.; Fenwick, J.; Gamble, J.; Creedy, D.K.; Buist, A.; Turkstra, E.; Ryding, E.L. A randomized controlled trial of a psycho-education intervention by midwives in reducing childbirth fear in pregnant women. Birth 2014, 41, 384–394. [Google Scholar] [CrossRef]
- Byrne, J.; Hauck, Y.; Fisher, C.; Bayes, S.; Schutze, R. Effectiveness of a mindfulness based childbirth education pilot study on maternal self-efficacy and fear of childbirth. J. Midwifery Women’s Health 2014, 59, 192–197. [Google Scholar] [CrossRef]
- Malata, A.; Hauck, Y.; Monterosso, L.; McCaul, K. Development and evaluation of a childbirth education programme for Malawian women. J. Adv. Nurs. 2007, 60, 67–78. [Google Scholar] [CrossRef] [PubMed]
- Spinelli, A.; Baglio, G.; Donati, S.; Grandolfo, M.E.; Osborn, J. Do antenatal classes benefit the mother and her baby? J. Matern.-Fetal Neonatal Med. 2003, 13, 94–101. [Google Scholar] [CrossRef] [PubMed]
- Szymański, S.; Aniołkowska, P.; Fryc, D.; Kurkiewicz, V. The impact of antenatal classes on the newborn state. Nurs. Public Health 2019, 9, 279–283. [Google Scholar] [CrossRef]
- Gagnon, A.J.; Sandall, J. Individual or group antenatal education for childbirth or parenthood, or both. Cochrane Database Syst. Rev. 2007, 3, CD002869. [Google Scholar] [CrossRef]
- Fabian, H.M.; Radestad, I.J.; Waldenstrom, U. Childbirth and parenthood education classes in Sweden. Women’s opinion and possible outcomes. Acta Obstet. Gynecol. Scandinivia 2005, 84, 436–443. [Google Scholar] [CrossRef]
- Musthofa, S.; Raharjo, T.; Sugiharto, D.; Achmad, R.C. The Portrait of Implementation of Antenatal Classes. In Proceedings of the 5th International Conference on Science, Education and Technology, ISET 2019, Semarang, Indonesia, 29 June 2019. [Google Scholar] [CrossRef] [Green Version]
- Patriajati, S.; Sriatmi, A. Determinants of mothers’ participation in antenatal classes. J. Adm. Kesehat. Indones. 2019, 7, 139–146. [Google Scholar] [CrossRef] [Green Version]
- Wigert, H.; Nilsson, C.; Dencker, A.; Begley, C.; Jangsten, E.; Sparud-Lundin, C.; Mollberg, M.; Patel, H. Women’s experiences of fear of childbirth: A metasynthesis of qualitative studies. Int. J. Qual. Stud. Health Well-Being 2020, 15, 1704484. [Google Scholar] [CrossRef] [Green Version]
- Renkert, S.; Nutbeam, D. Opportunities to improve maternal health literacy through antenatal education: An exploratory study. Health Promot. Int. 2001, 16, 381–388. [Google Scholar] [CrossRef] [Green Version]
- Jacobson, E. Progressive Relaxation; University of Chicago Press: Chicago, IL, USA, 1929. [Google Scholar]
- Beck, A.T. Depression: Clinical, Experimental and Theoretical Aspects; Harper and Row: New York, NY, USA, 1967. [Google Scholar]
- Linden, W. The Autogenic Training Method of J.H. Schultz. In Principles and Practice of Stress Management; Lehrer, P.M., Woolfolk, R.L., Sime, W.E., Eds.; The Guilford Press: New York, NY, USA, 2007; pp. 151–174. [Google Scholar]
- Diotaiuti, P.; Corrado, S.; Mancone, S.; Falese, L.; Rodio, A.; Siqueira, T.C.; Andrade, A. Influence of Cognitive Orientation and Attentional Focus on Pain Perception. Int. J. Environ. Res. Public Health 2021, 18, 7176. [Google Scholar] [CrossRef]
- Piscitelli, U. Respiratory Autogenic Training and Obstetric Psychoprophylaxix; Piccin: Padova, Italy, 1987. [Google Scholar]
- Schultz, J.H. Il Training Autogeno. Metodo di Autodistensione da Concentrazione Psichica, [Autogenic Training. Method of Self-Distention by Psychic Concentration]; Feltrinelli: Milano, Italy, 1984. [Google Scholar]
- Endler, N.S.; Edwards, J.M.; Vitelli, R. EMAS Endler Multidimensional Anxiety Scales; Western Psychological Services: Los Angeles, CA, USA, 1991. [Google Scholar]
- Diotaiuti, P.; Valente, G.; Mancone, S. Validation study of the Italian version of Temporal Focus Scale: Psychometric properties and convergent validity. BMC Psychol. 2021, 9, 19. [Google Scholar] [CrossRef]
- Lu, Y.; Zhang, Z.; Min, K.; Luo, X.; He, Z. Pregnancy-Related Information Seeking in Online Health Communities: A Qualitative Study. In Diversity, Divergence, Dialogue. iConference 2021. Lecture Notes in Computer Science; Toeppe, K., Yan, H., Chu, S.K.W., Eds.; Springer: Cham, Switzerland, 2021; pp. 18–36. [Google Scholar]
- Rondung, E.; Thomtén, J.; Sundin, Ö. Psychological perspectives on fear of childbirth. J. Anxiety Disord. 2016, 44, 80–91. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gunning, M.D.; Denison, F.C.; Stockley, C.J.; Ho, S.P.; Sandhu, H.K.; Reynolds, R.M. Assessing maternal anxiety in pregnancy with the State-Trait Anxiety Inventory (STAI): Issues of validity, location and participation. J. Reprod. Infant Psychol. 2010, 28, 266–273. [Google Scholar] [CrossRef]
- Cena, L.; Palumbo, G.; Mirabella, F.; Gigantesco, A.; Stefana, A.; Trainini, A.; Tralli, N.; Imbasciati, A. Perspectives on Early Screening and Prompt Intervention to Identify and Treat Maternal Perinatal Mental Health. Protocol for a Prospective Multicenter Study in Italy. Front. Psychol. 2020, 11, 365. [Google Scholar] [CrossRef] [PubMed]
- Cohen, J. Statistical Power Analysis for the Behavioural Sciences, 2nd ed.; Erlbaum: Hillside, NJ, USA, 1988. [Google Scholar]
- Wiener, A.; Rogers, C. Antenatal classes: Women can’t think beyond labour. Br. J. Midwifery 2008, 16, 121–124. [Google Scholar] [CrossRef]
- McCourt, C. (Ed.) Childbirth, Midwifery and Concepts of Time, 1st ed.; Berghahn Books: New York, NY, USA, 2010; Volume 17. [Google Scholar]
- McKay, M.T.; Cole, J.C.; Percy, A. Temporal focus clusters differ meaningfully in terms of anxiety and depressive symptomatology. Psychiatry Res. 2017, 256, 283–285. [Google Scholar] [CrossRef] [PubMed]
- Runjati, R.; Susanto, H.; Sawitri, D.; Thaufik, S. The effect of antenatal class plus coping skill training on the level of stress and childbirth self-efficacy. Adv. Sci. Lett. 2017, 23, 3329–3333. [Google Scholar] [CrossRef]
- Aryastuti, S.A.; Juwita, D.A.P.R.; Cahyawati, P.N.; Witari, N.P.D.; Pradnyawati, L.G. Empowerment of Health Cadre in Managing Antenatal Class in Tulikup Village, Gianyar-Bali. Int. J. Community Serv. Learn. 2020, 4, 393–400. [Google Scholar] [CrossRef]
- Schwartz, L.; Toohill, J.; Creedy, D.K.; Baird, K.; Gamble, J.; Fenwick, J. Factors associated with childbirth self-efficacy in Australian childbearing women. BMC Pregnancy Childbirth 2015, 15, 29. [Google Scholar] [CrossRef] [Green Version]
- Timmermans, E.; Timmermans, O.; Mestdagh, E.; Bogaerts, A. The Effect of Prenatal Interventions on Self-Efficacy in Women During Childbirth—A Systematic Review. J. Gynecol. Women’s Health 2019, 16, 555946. [Google Scholar] [CrossRef]
- Zhao, Y.; Wu, J.; Yang, H.; Yin, X.; Li, D.; Qiu, L.; Sun, N.; Gong, Y. Factors associated with childbirth self-efficacy: A multicenter cross-sectional study in China. Midwifery 2021, 93, 102883. [Google Scholar] [CrossRef]
- Carlsson, I.M.; Ziegert, K.; Nissen, E. The relationship between childbirth self-efficacy and aspects of well-being, birth interventions and birth outcomes. Midwifery 2015, 31, 1000–1007. [Google Scholar] [CrossRef] [PubMed]
- Tilden, E.L.; Caughey, A.B.; Lee, C.S.; Emeis, C. The effect of childbirth self-efficacy on perinatal outcomes. J. Obstet. Gynecol. Neonatal Nurs. 2016, 45, 465–480. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Liying, B.; Xin, L.; Yanjiao, L. Effects of Psychological Intervention on Childbirth Self-efficacy, Prenatal Fear, Outcome and Postpartum Depression in Primiparas. Investig. Clínica 2020, 61, 2. [Google Scholar]
- Rowe, R.E.; Garcia, J.; Macfarlane, A.J.; Davidson, L.L. Improving communication between health professionals and women in maternity care: A structured review. Health Expect. 2002, 5, 63–83. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Diotaiuti, P.; Valente, G.; Mancone, S.; Grambone, A. Psychometric Properties and a Preliminary Validation Study of the Italian Brief Version of the Communication Styles Inventory (CSI-B/I). Front. Psychol. 2020, 11, 1421. [Google Scholar] [CrossRef]
- Cutajar, L.; Miu, M.; Fleet, J.A.; Cyna, A.M.; Steen, M. Antenatal education for childbirth: Labour and birth. Eur. J. Midwifery 2020, 4, 11. [Google Scholar] [CrossRef]
- Diotaiuti, P.; Valente, G.; Mancone, S.; Grambone, A.; Chirico, A. Metric goodness and measurement invariance of the italian brief version of interpersonal reactivity index: A study with young adults. Front. Psychol. 2021, 12, 773363. [Google Scholar] [CrossRef]
- Ho, I.; Holroyd, E. Chinese women’s perceptions of the effectiveness of antenatal education in the preparation for motherhood. J. Adv. Nurs. 2002, 38, 74–85. [Google Scholar] [CrossRef]
- Nolan, M.L. Information giving and education in pregnancy: A review of qualitative studies. J. Perinat. Educ. 2009, 18, 21–30. [Google Scholar] [CrossRef] [Green Version]
- Andrade, A.; Vilarino, G.T.; Bevilacqua, G.G. What is the effect of strength training on pain and sleep in patients with fibromyalgia? Am. J. Phys. Med. Rehabil. 2017, 96, 889–893. [Google Scholar] [CrossRef]
- Andrade, A.; Steffens, R.D.A.K.; Vilarino, G.T.; Sieczkowska, S.M.; Coimbra, D.R. Does volume of physical exercise have an effect on depression in patients with fibromyalgia? J. Affect. Disord. 2017, 208, 214–217. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| MA | GA | IN | RN | SN | PSE | Past | Pres | Fut | PT | SA | |
|---|---|---|---|---|---|---|---|---|---|---|---|
| MA | 1 | ||||||||||
| GA | −0.105 | 1 | |||||||||
| IN | 0.026 | 0.147 | 1 | ||||||||
| RN | −0.001 | 0.246 ** | 0.685 ** | 1 | |||||||
| SN | −0.028 | −0.074 | 0.431 ** | 0.468 ** | 1 | ||||||
| PSE | −0.045 | 0.097 | −0.220 ** | −0.254 ** | −0.185 ** | 1 | |||||
| Past | 0.032 | 0.021 | −0.066 | 0.012 | 0.062 | −0.078 | 1 | ||||
| Pre | 0.124 | −0.052 | 0.281 ** | 0.303 ** | 0.292 ** | 0.024 | −0.078 | 1 | |||
| Fut | 0.142 | −0.226 ** | 0.206 ** | 0.252 ** | 0.341 ** | −0.045 | 0.340 ** | 0.370 ** | 1 | ||
| TA | −0.106 | −0.001 | 0.106 | 0.281 ** | 0.207 ** | −0.315 ** | 0.063 | −0.068 | 0.252 ** | 1 | |
| SA | −0.003 | 0.082 | 0.135 | 0.211 ** | 0.144 * | −0.122 | 0.046 | 0.324 ** | 0.288 ** | −0.003 | 1 |
| Psychoeducational Intervention Group (n = 80) | Traditional Antenatal Course Group (n = 80) | No Course Group (n = 80) | |||||
|---|---|---|---|---|---|---|---|
| Variables | Time | (Mean ± SD) | (Mean ± SD) | (Mean ± SD) | F | p-Value | η2 |
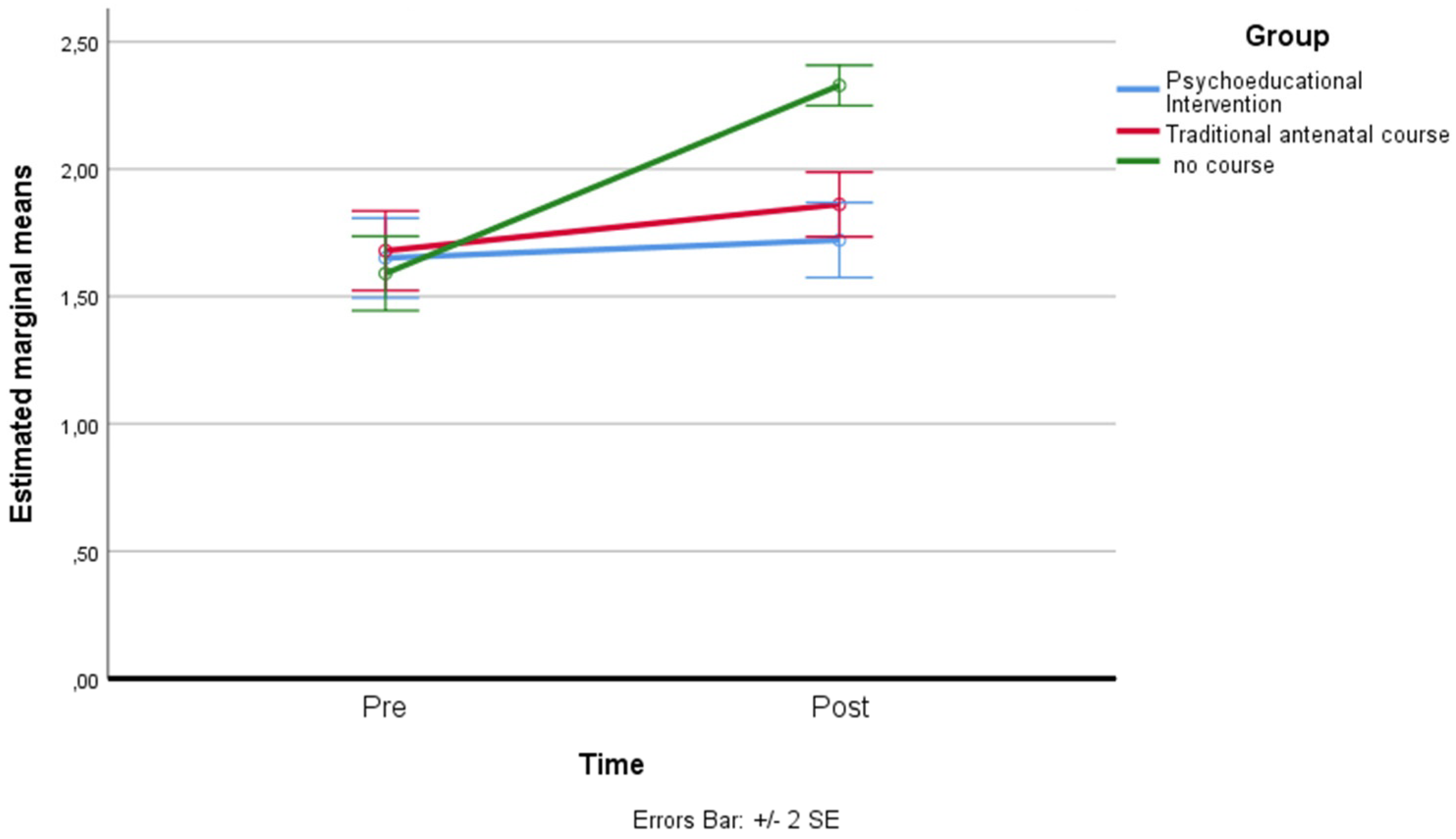
| Threat Anxiety | PRE | 1.65 ± 0.70 | 1.67 ± 0.69 | 1.59 ± 0.65 | 0.356 | >0.05 | 0.003 |
| POST | 1.72 ± 0.65 | 1.86 ± 0.56 | 2.32 ± 0.35 | 27.592 | <0.001 | 0.189 | |
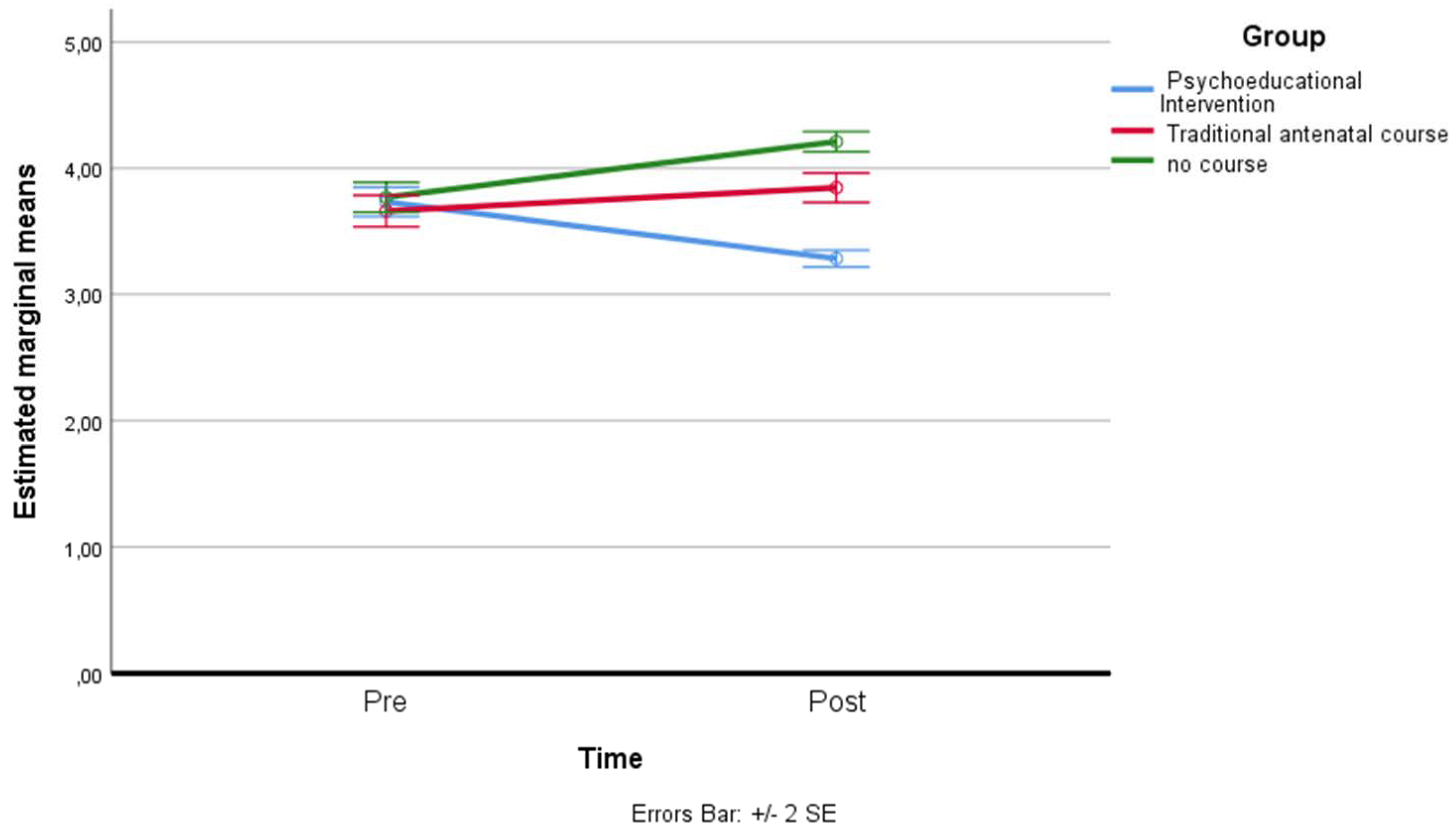
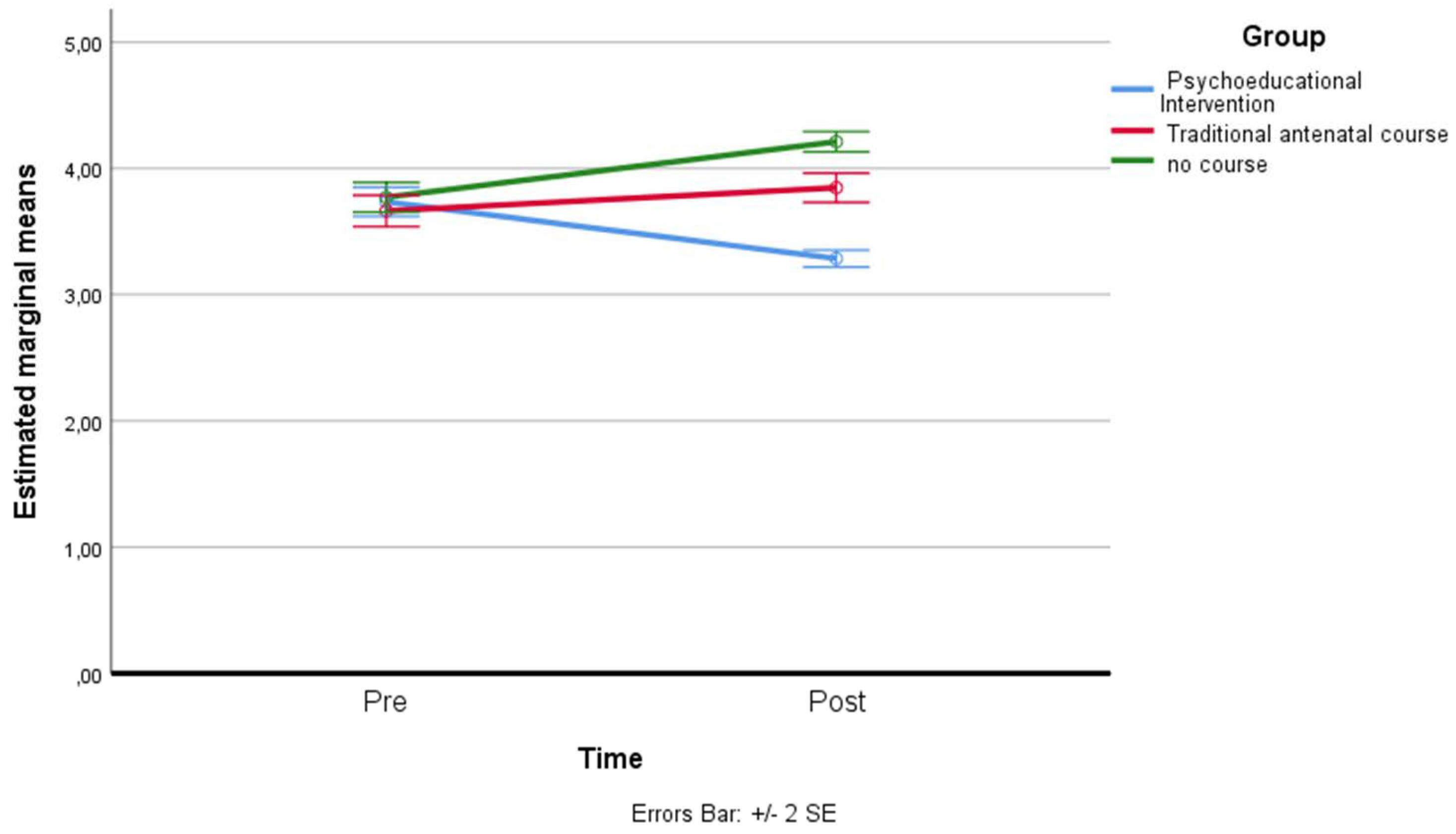
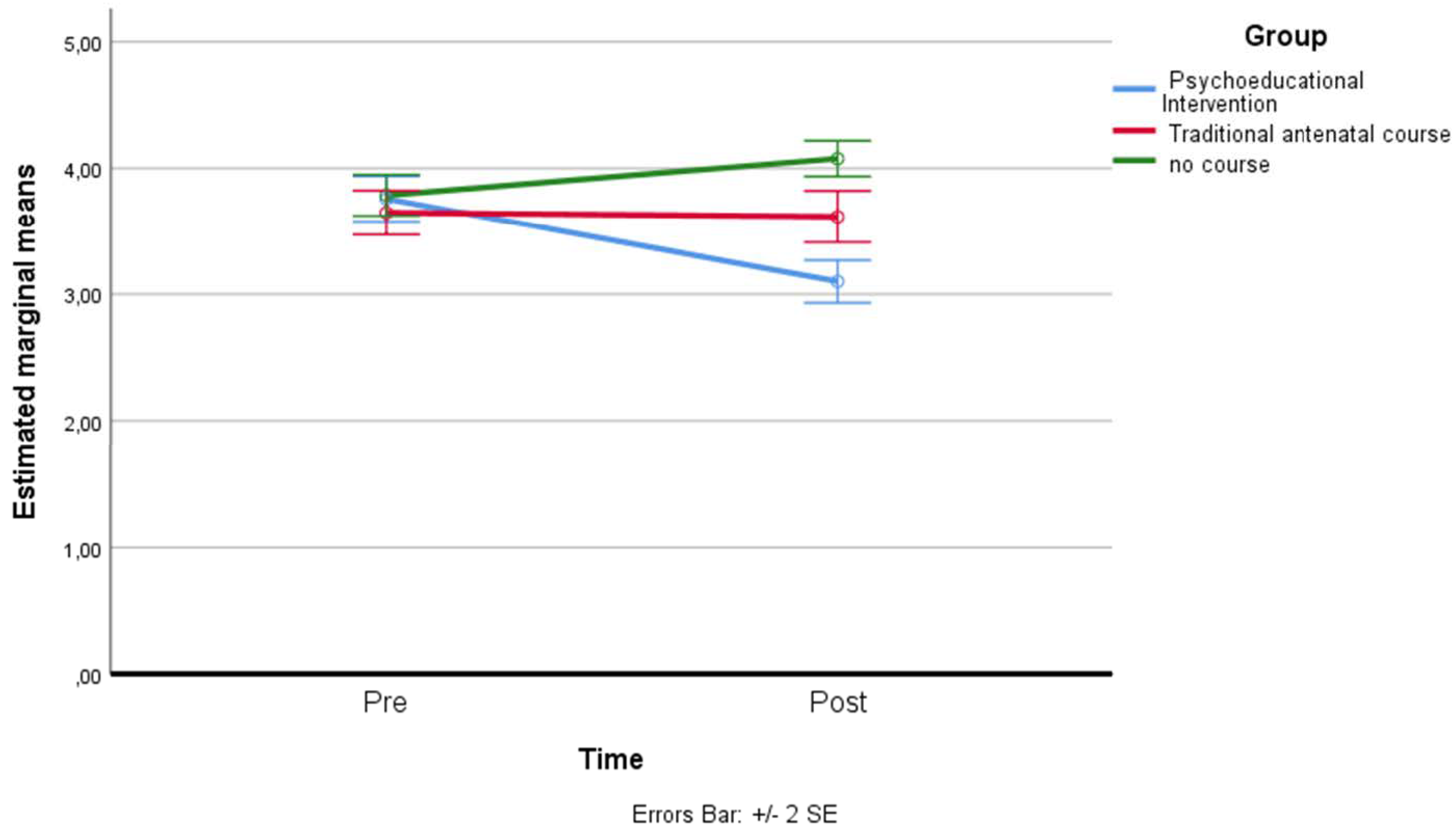
| State Anxiety | PRE | 3.73 ± 0.52 | 3.66 ± 0.56 | 3.77 ± 0.53 | 0.858 | >0.05 | 0.007 |
| POST | 3.29 ± 0.30 | 3.85 ± 0.52 | 4.21 ± 0.36 | 107.038 | <0.001 | 0.475 | |
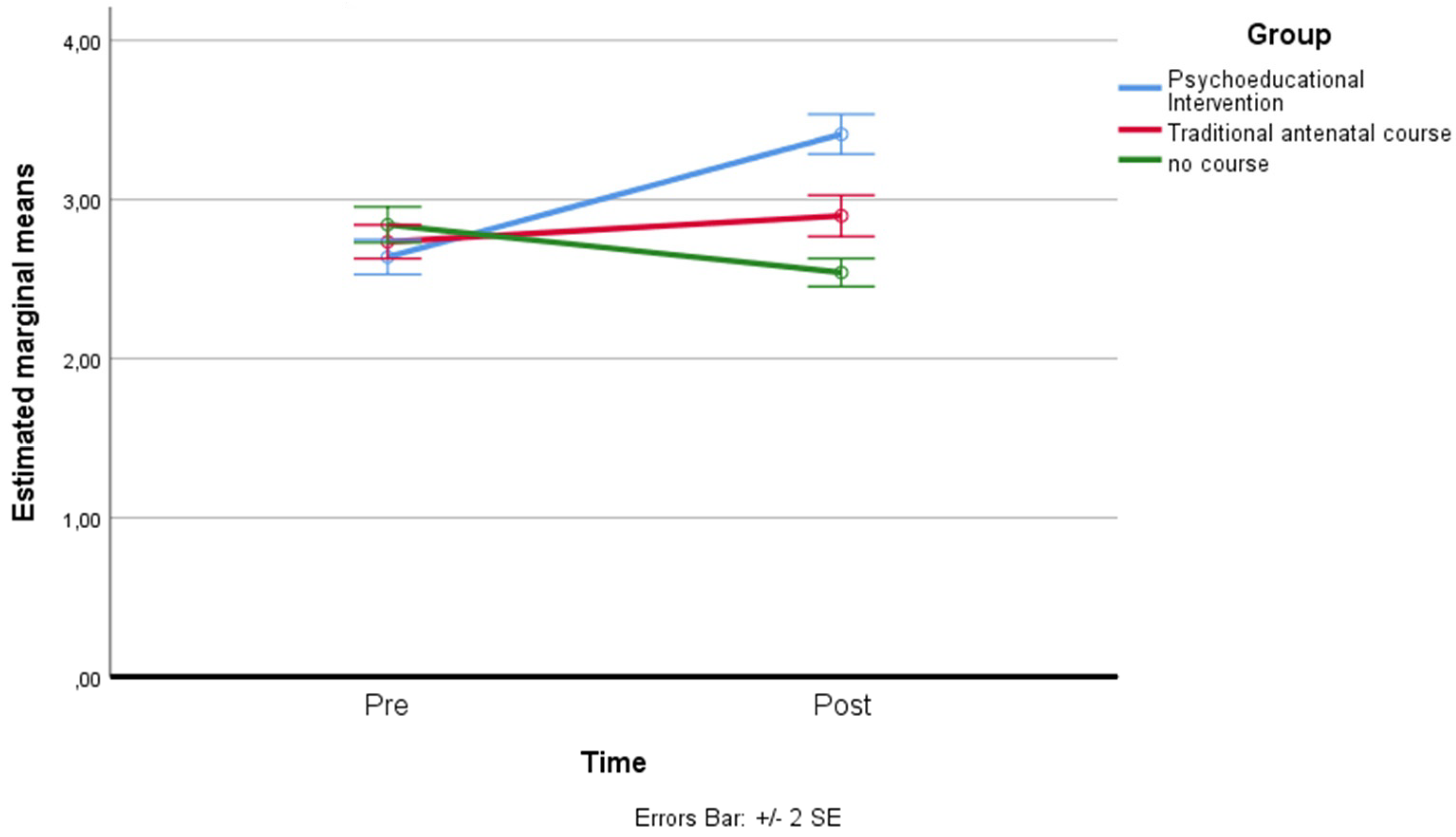
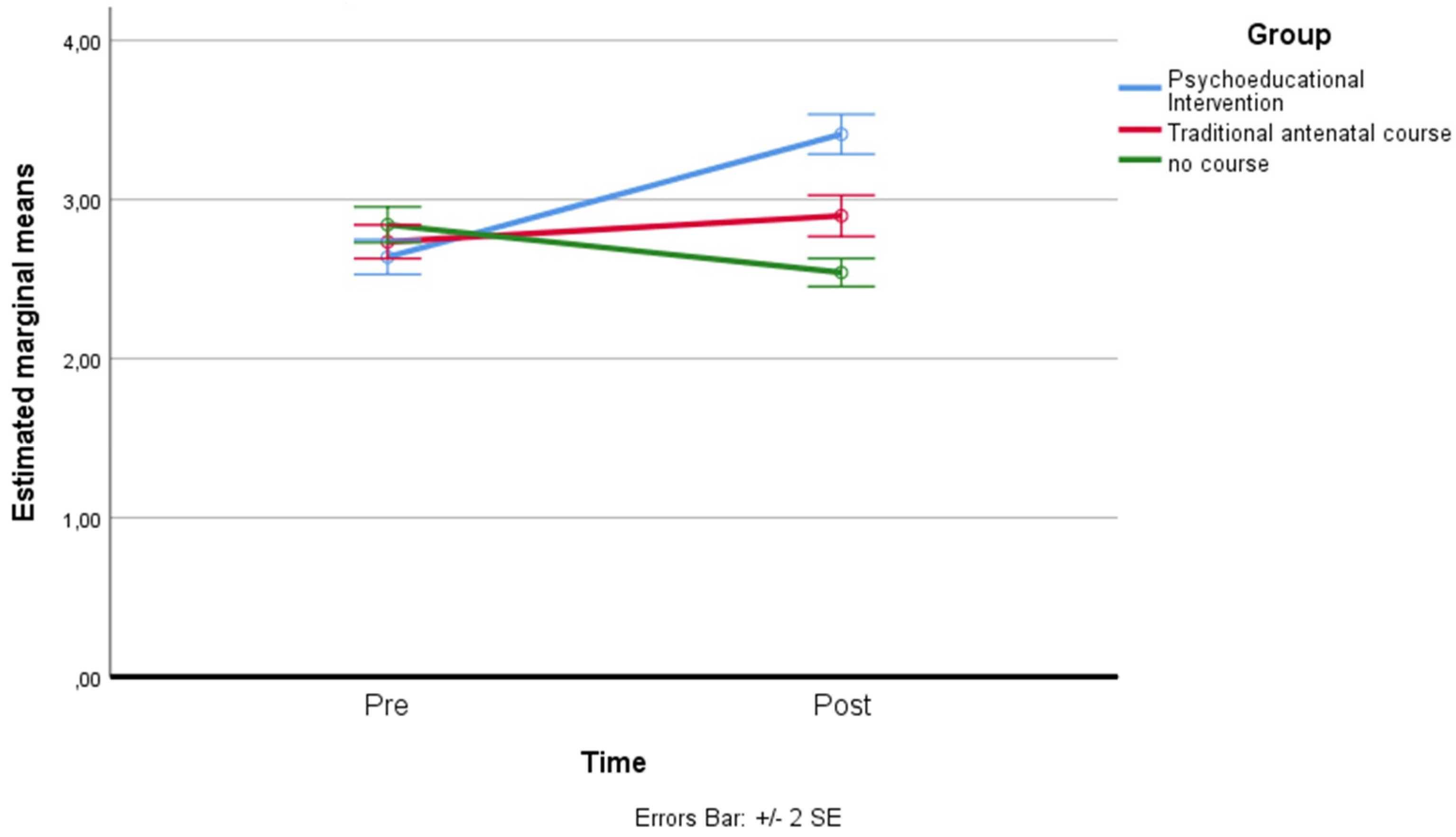
| Self-Efficacy | PRE | 2.64 ± 0.49 | 2.74 ± 0.47 | 2.84 ± 0.50 | 3.450 | >0.05 | 0.028 |
| POST | 3.41 ± 0.56 | 2.90 ± 0.58 | 2.54 ± 0.39 | 57.157 | <0.001 | 0.325 | |
| Information Need | PRE | 3.92 ± 0.81 | 3.87 ± 0.92 | 3.51 ± 0.75 | 5.728 | >0.05 | 0.046 |
| POST | 2.96 ± 0.63 | 3.11 ± 0.61 | 3.91 ± 0.59 | 56.707 | <0.001 | 0.324 | |
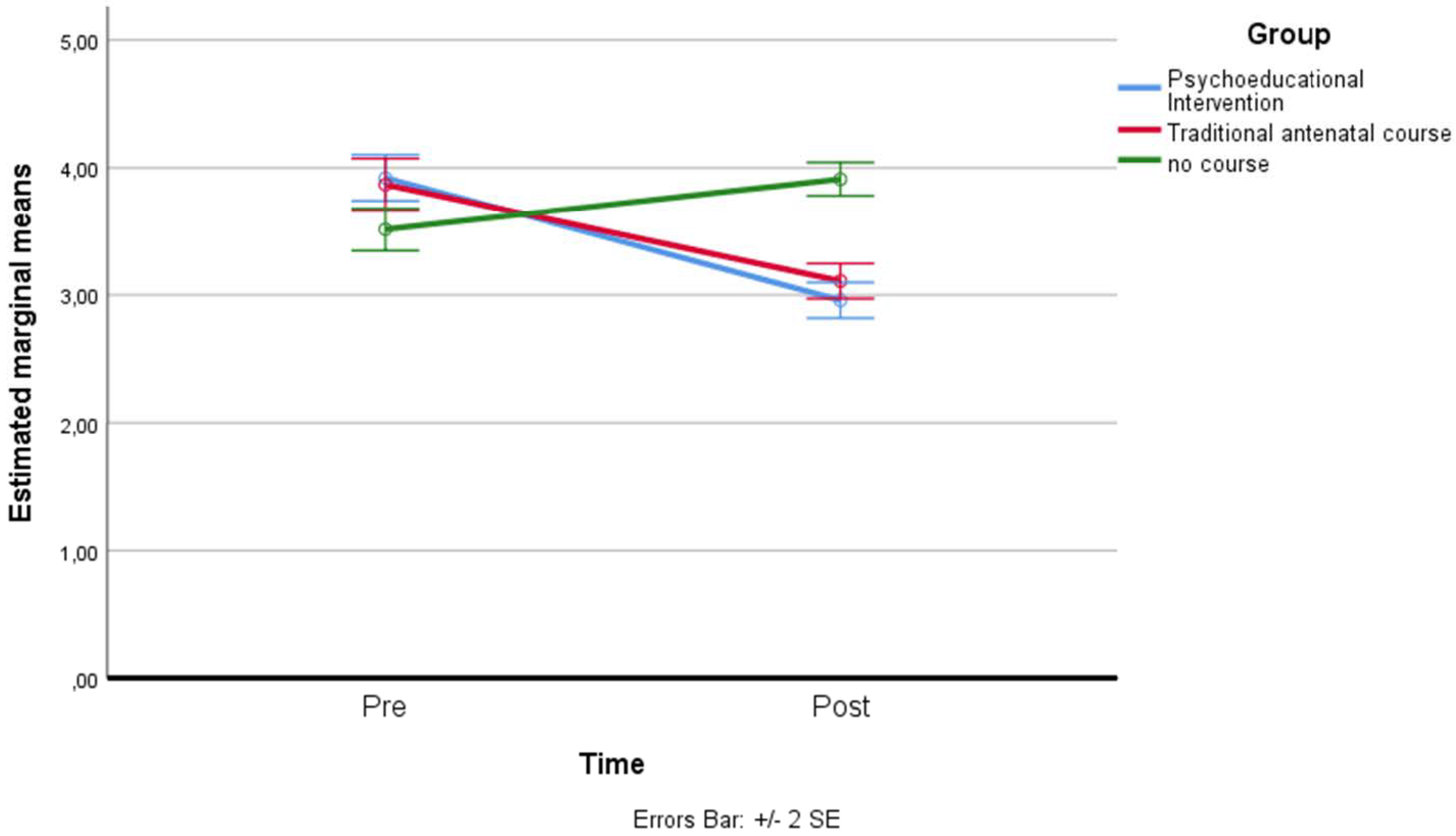
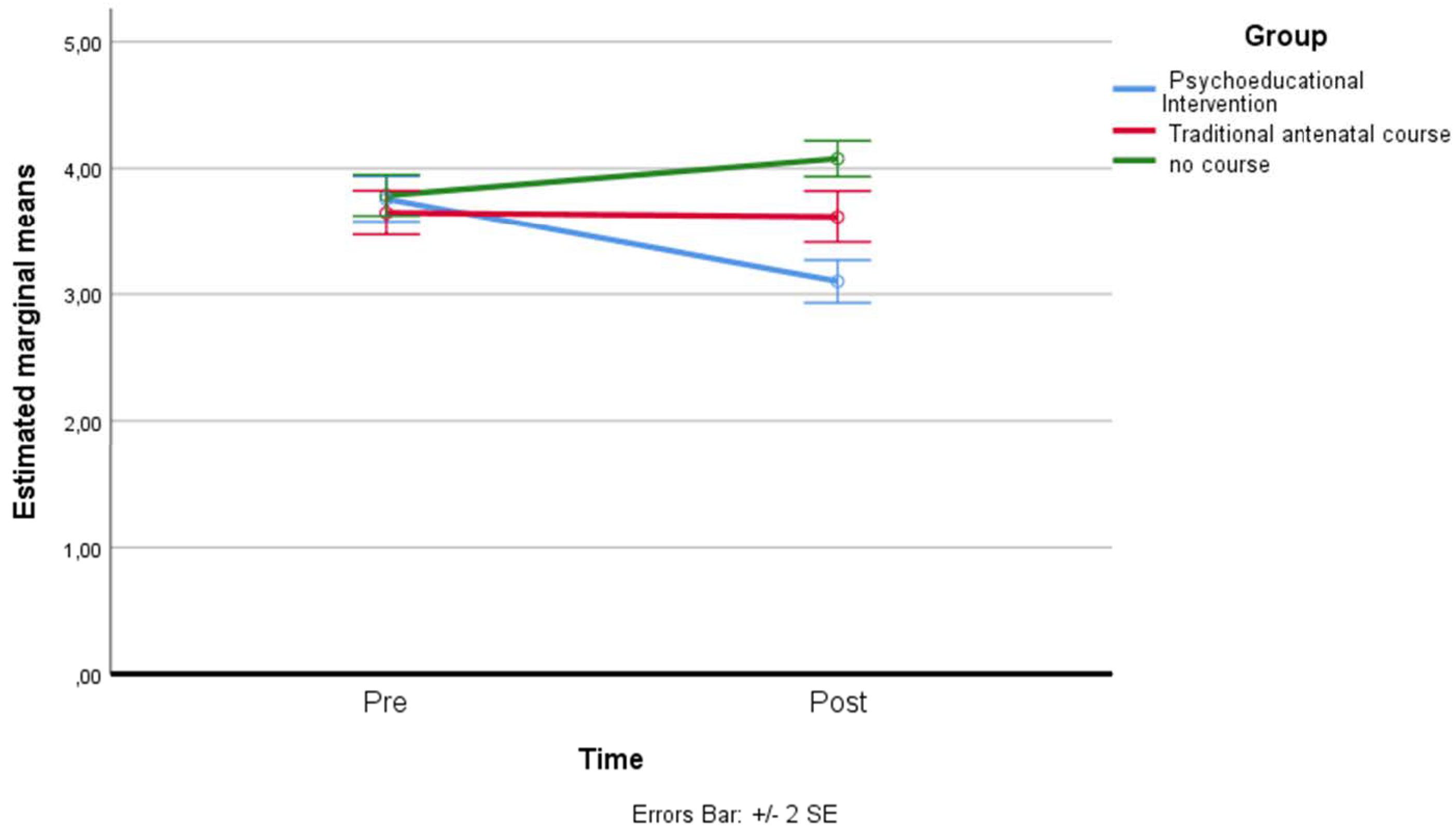
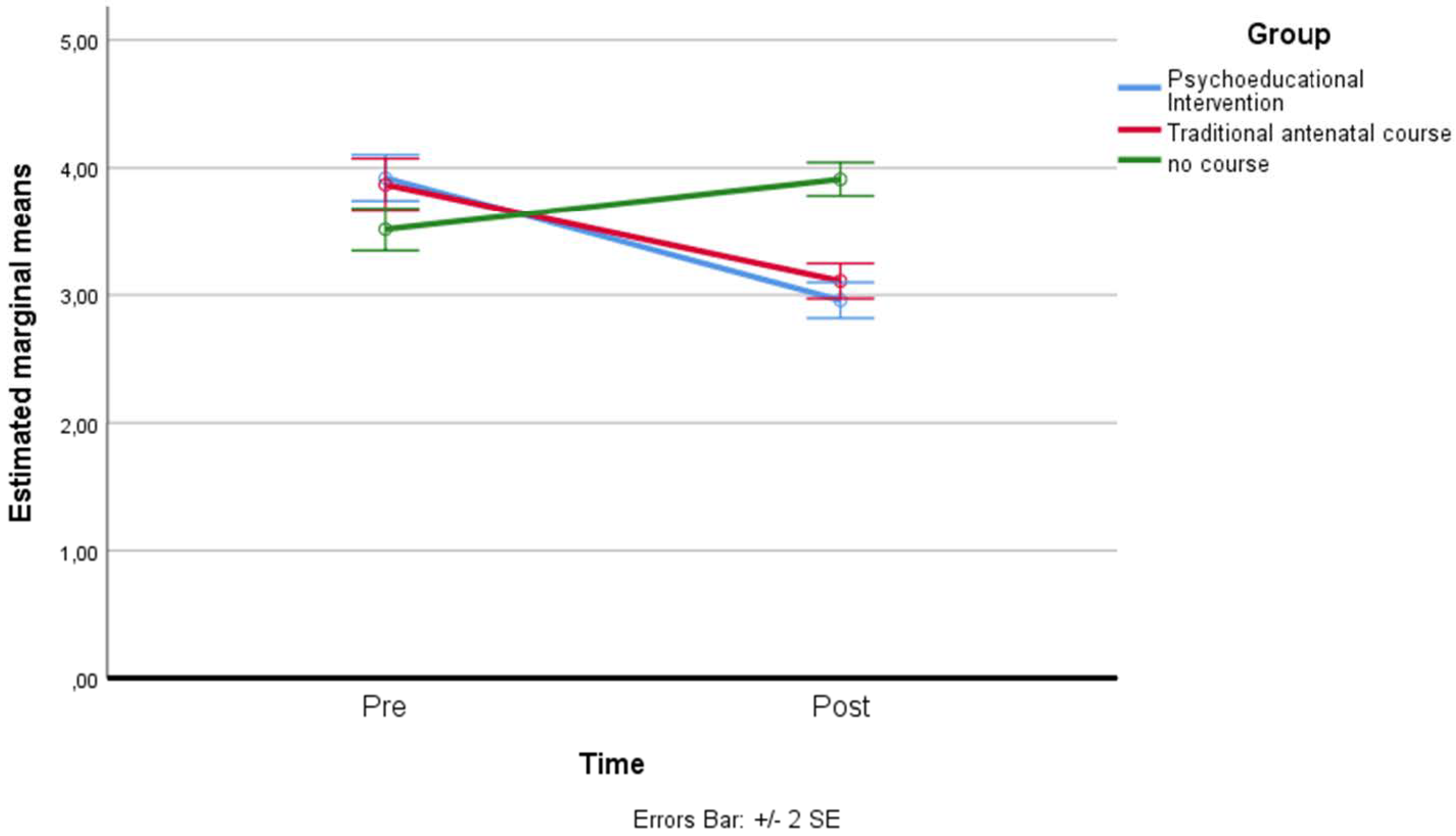
| Reassurance Need | PRE | 3.76 ± 0.80 | 3.65 ± 0.78 | 3.79 ± 0.73 | 0.712 | >0.05 | 0.006 |
| POST | 3.10 ± 0.75 | 3.62 ± 0.92 | 4.08 ± 0.63 | 31.666 | <0.001 | 0.211 | |
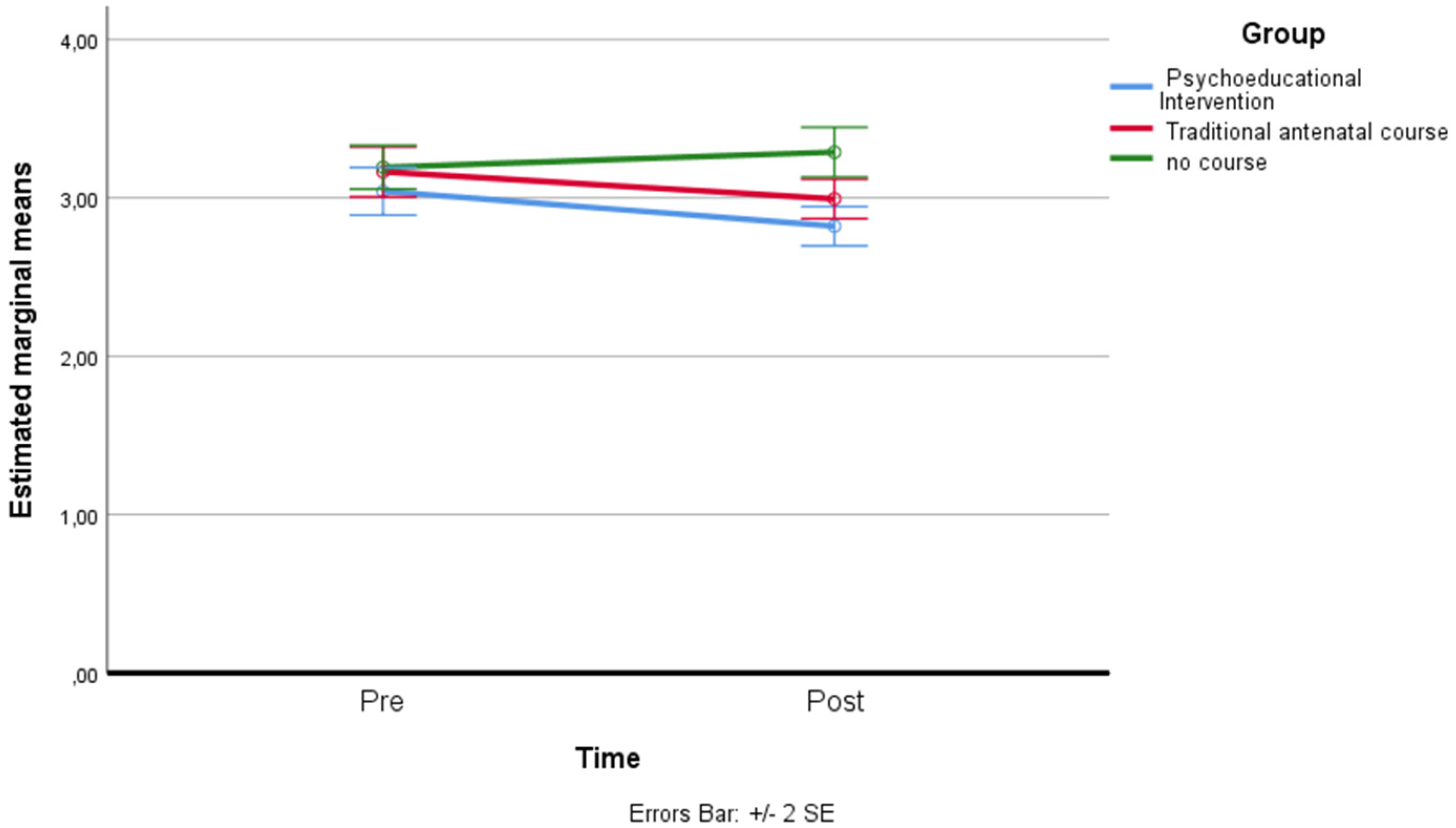
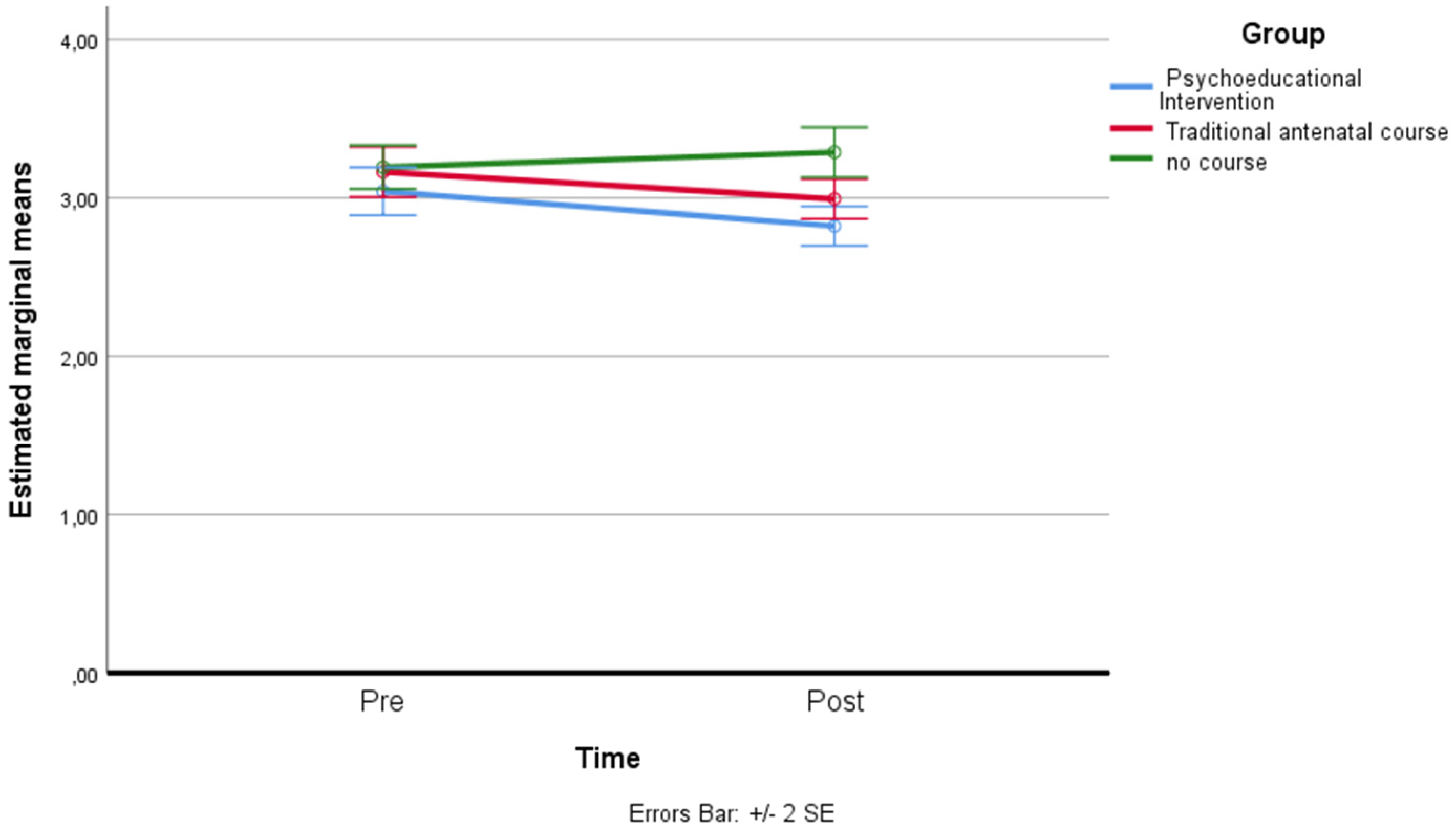
| Sharing Need | PRE | 3.04 ± 0.67 | 3.16 ± 0.71 | 3.19 ± 0.61 | 1.169 | >0.05 | 0.010 |
| POST | 2.82 ± 0.55 | 2.99 ± 0.56 | 3.29 ± 0.67 | 12.620 | <0.001 | 0.096 | |
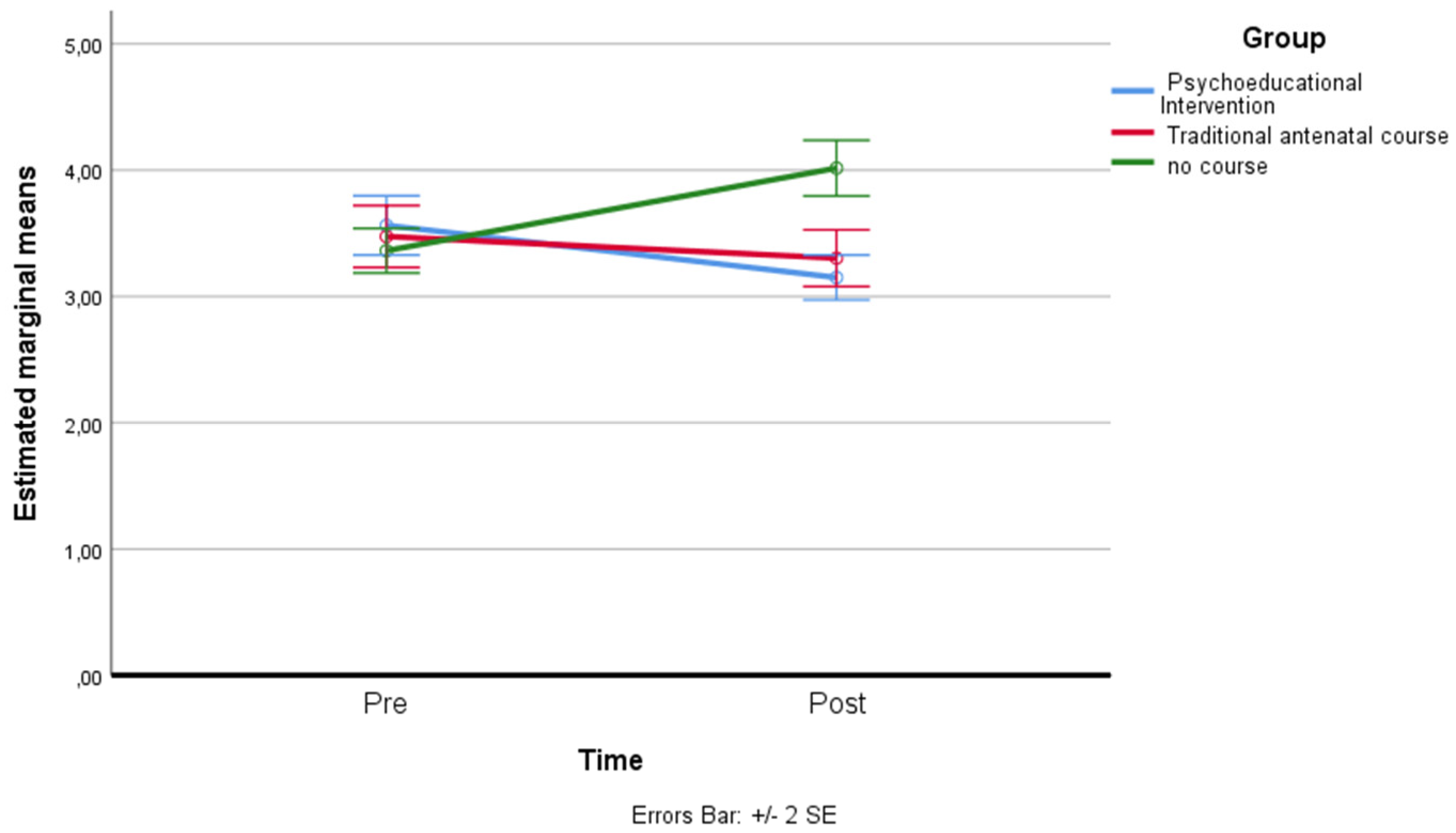
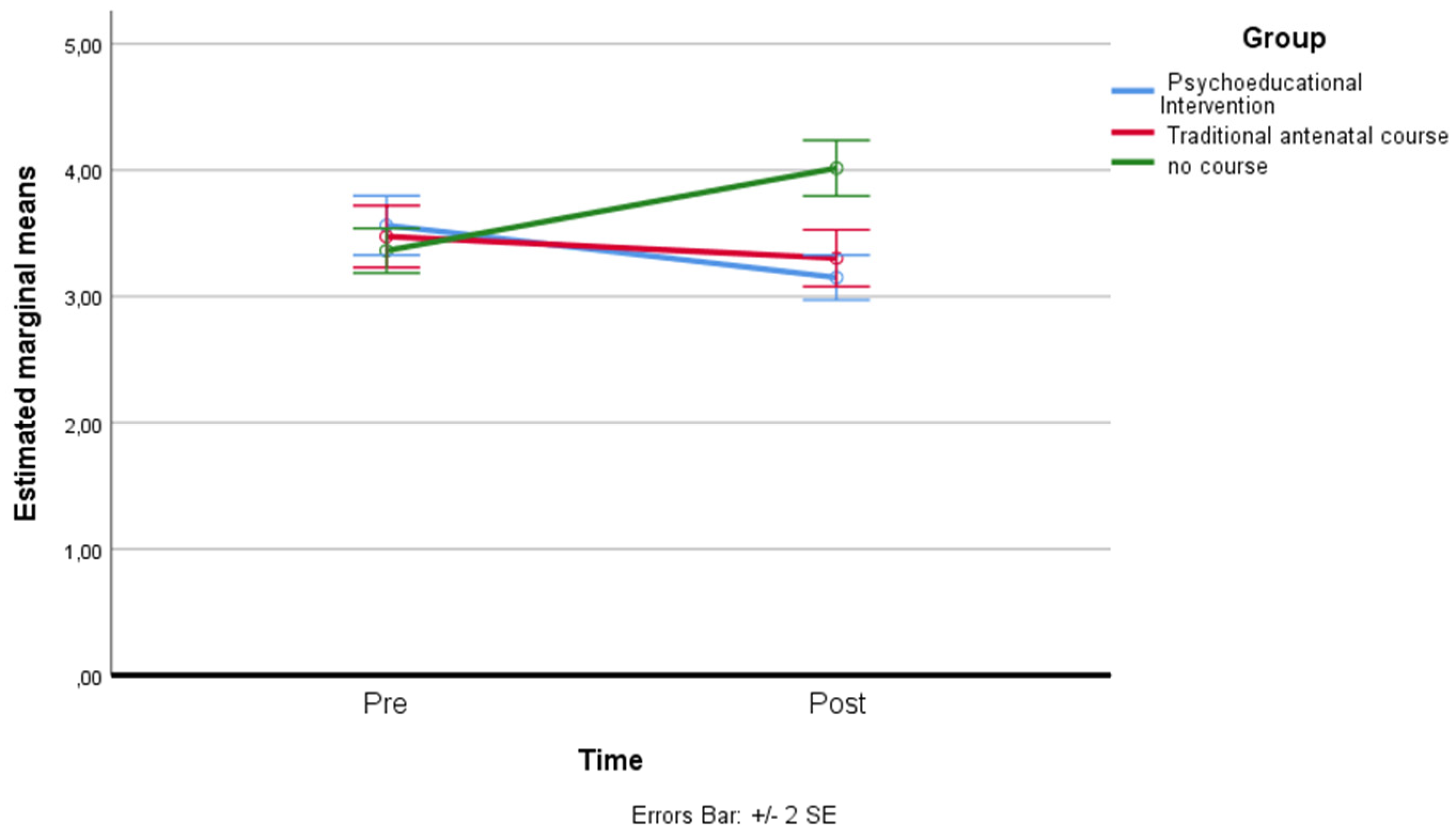
| Past Focus | PRE | 3.56 ± 1.05 | 3.47 ± 1.09 | 3.36 ± 0.79 | 0.825 | >0.05 | 0.007 |
| POST | 3.15 ± 0.79 | 3.30 ± 1.00 | 4.01 ± 0.98 | 19.610 | <0.001 | 0.142 | |
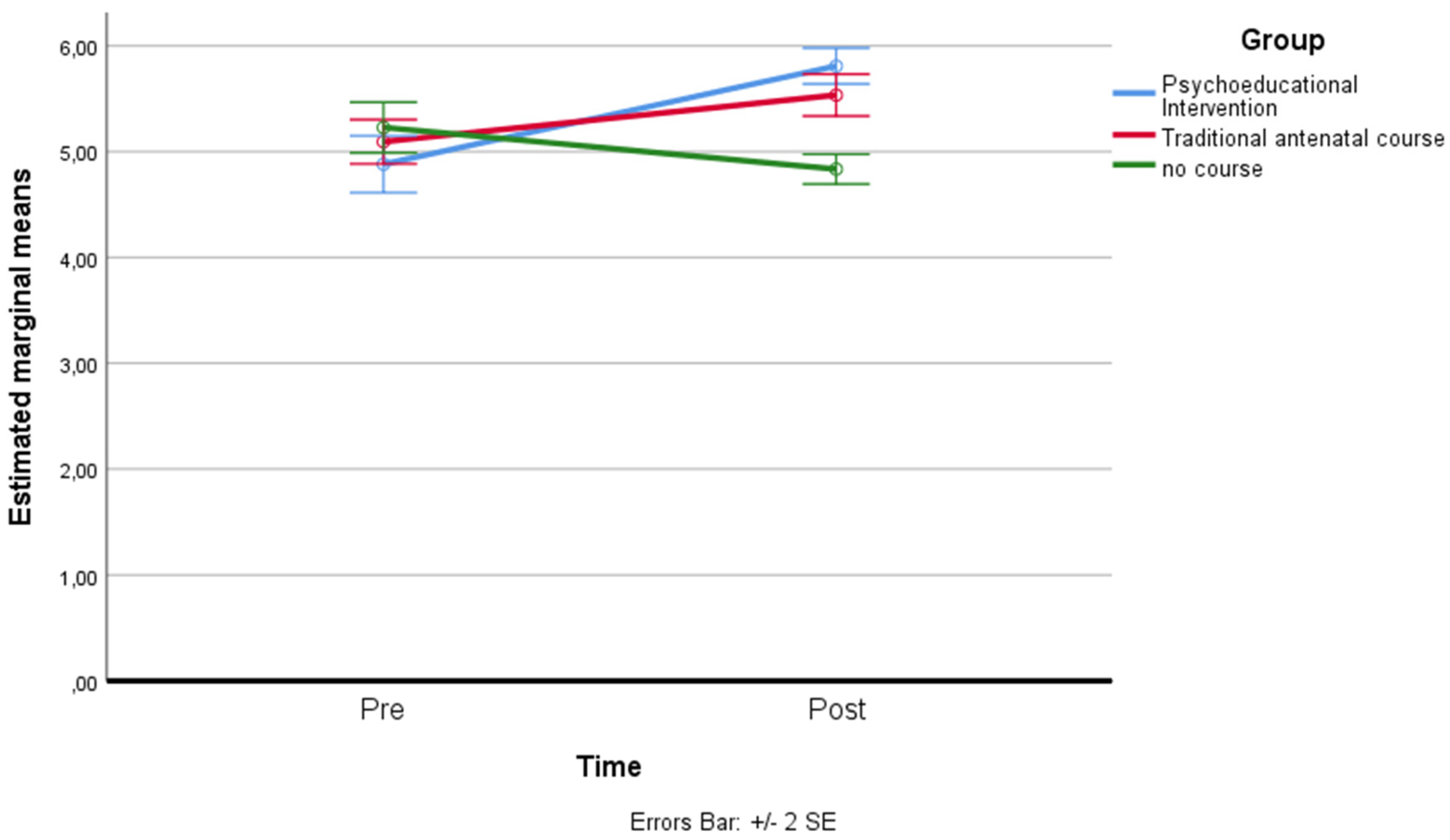
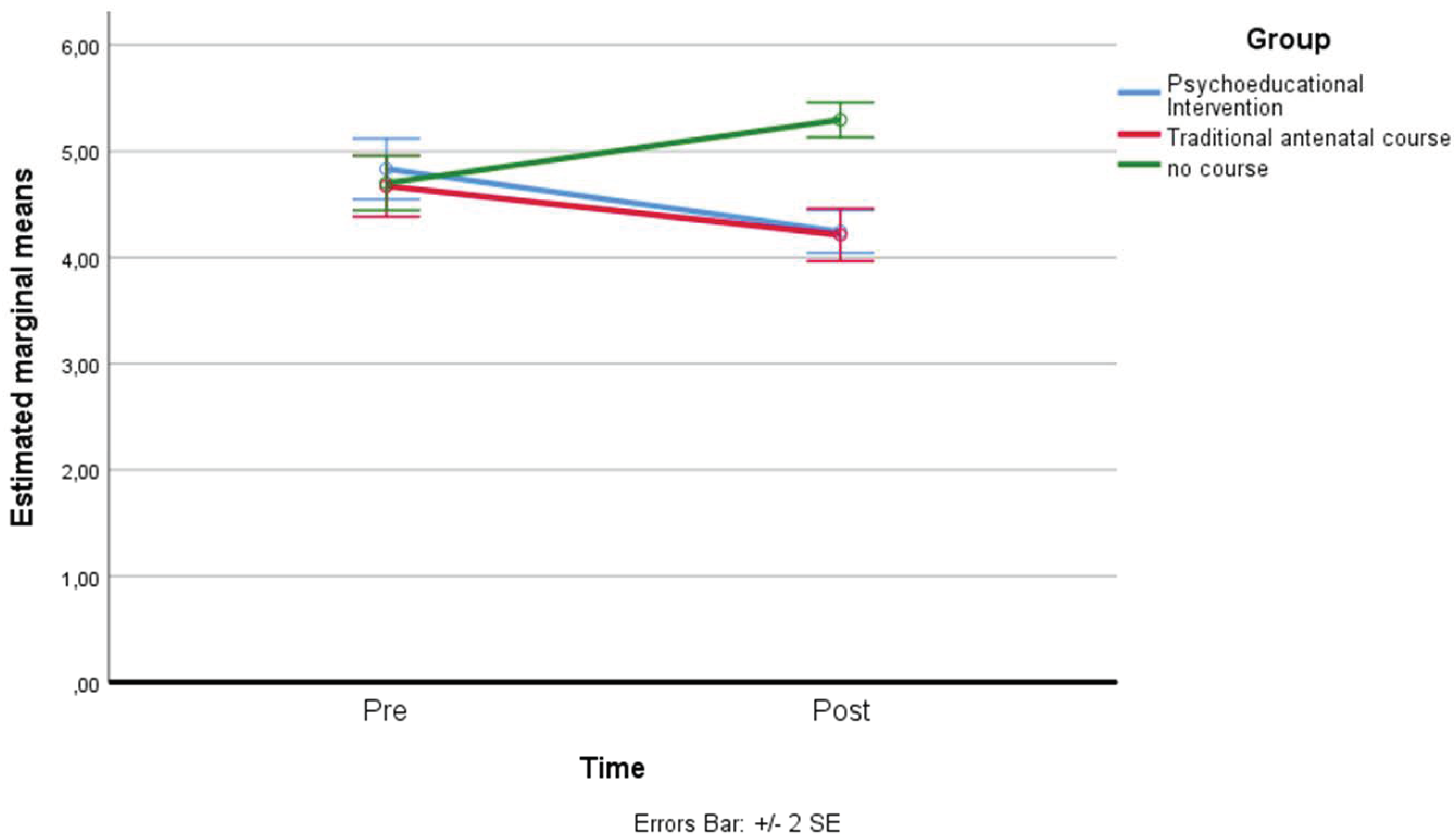
| Present Focus | PRE | 4.88 ± 1.20 | 5.09 ± 0.93 | 5.23 ± 1.07 | 2.119 | >0.05 | 0.018 |
| POST | 5.81 ± 0.76 | 5.53 ± 0.88 | 4.83 ± 0.63 | 34.534 | <0.001 | 0.226 | |
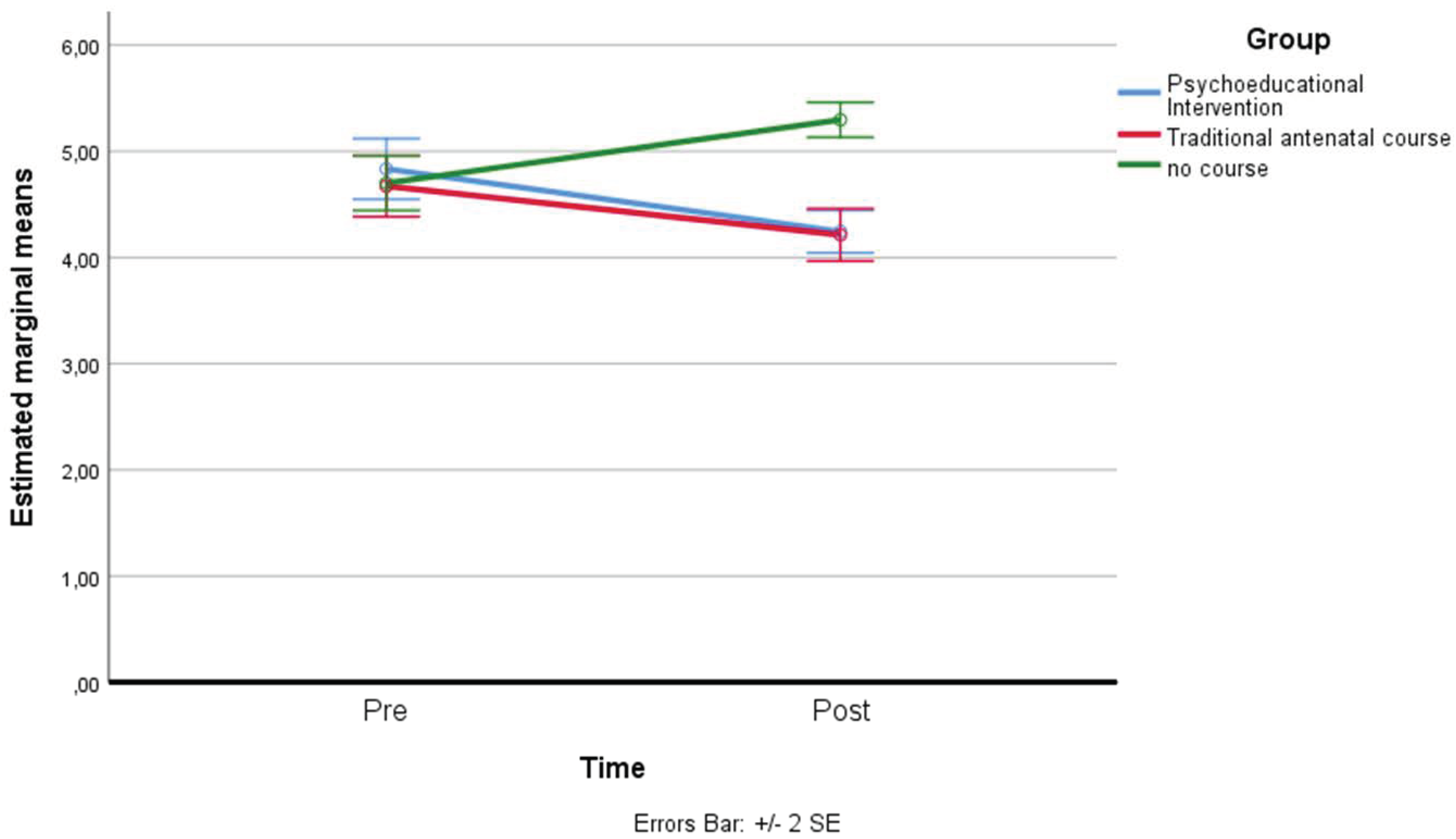
| Future Focus | PRE | 4.83 ± 1.28 | 4.67 ± 1.29 | 4.70 ± 1.15 | 0.392 | >0.05 | 0.003 |
| POST | 4.24 ± 0.89 | 4.21 ± 1.10 | 5.30 ± 0.74 | 35.689 | <0.001 | 0.231 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Diotaiuti, P.; Valente, G.; Mancone, S.; Falese, L.; Corrado, S.; Siqueira, T.C.; Andrade, A. A Psychoeducational Intervention in Prenatal Classes: Positive Effects on Anxiety, Self-Efficacy, and Temporal Focus in Birth Attendants. Int. J. Environ. Res. Public Health 2022, 19, 7904. https://doi.org/10.3390/ijerph19137904
Diotaiuti P, Valente G, Mancone S, Falese L, Corrado S, Siqueira TC, Andrade A. A Psychoeducational Intervention in Prenatal Classes: Positive Effects on Anxiety, Self-Efficacy, and Temporal Focus in Birth Attendants. International Journal of Environmental Research and Public Health. 2022; 19(13):7904. https://doi.org/10.3390/ijerph19137904
Chicago/Turabian StyleDiotaiuti, Pierluigi, Giuseppe Valente, Stefania Mancone, Lavinia Falese, Stefano Corrado, Thais Cristina Siqueira, and Alexandro Andrade. 2022. "A Psychoeducational Intervention in Prenatal Classes: Positive Effects on Anxiety, Self-Efficacy, and Temporal Focus in Birth Attendants" International Journal of Environmental Research and Public Health 19, no. 13: 7904. https://doi.org/10.3390/ijerph19137904
APA StyleDiotaiuti, P., Valente, G., Mancone, S., Falese, L., Corrado, S., Siqueira, T. C., & Andrade, A. (2022). A Psychoeducational Intervention in Prenatal Classes: Positive Effects on Anxiety, Self-Efficacy, and Temporal Focus in Birth Attendants. International Journal of Environmental Research and Public Health, 19(13), 7904. https://doi.org/10.3390/ijerph19137904