
Determinants of Survival of HIV Patients Receiving Dolutegravir: A Prospective Cohort Study in Conflict-Affected Bunia, Democratic Republic of Congo


 , ,
, ,
Abstract
1. Introduction
2. Methods
2.1. Study Design and Participants
2.2. Procedures, Data Collection, and Outcome
2.3. Statistical Analysis
2.4. Ethical Statement
3. Results
3.1. Patient Characteristics at Enrollment and Follow-Up Status
3.2. LTFU and Mortality Rate
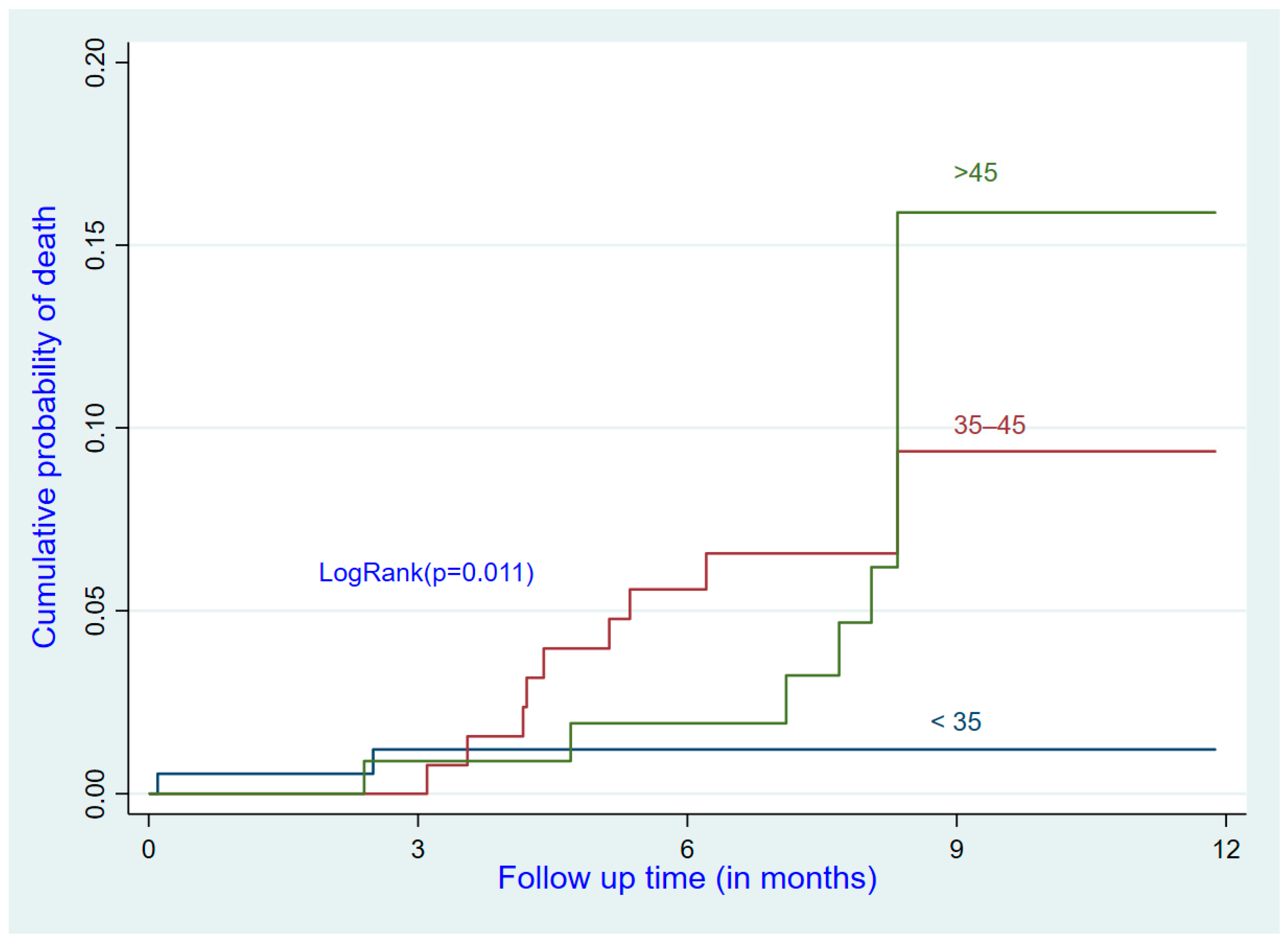
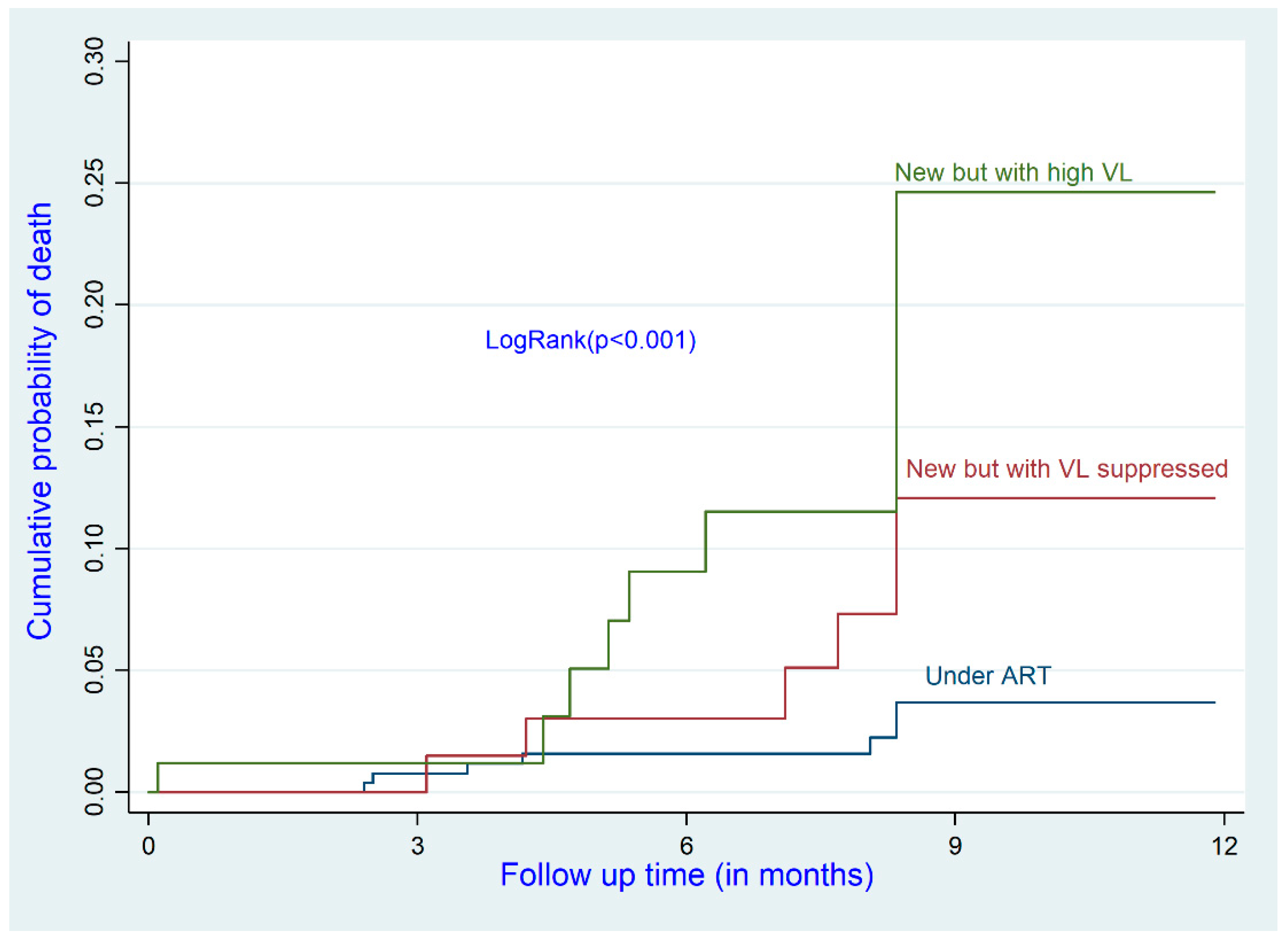
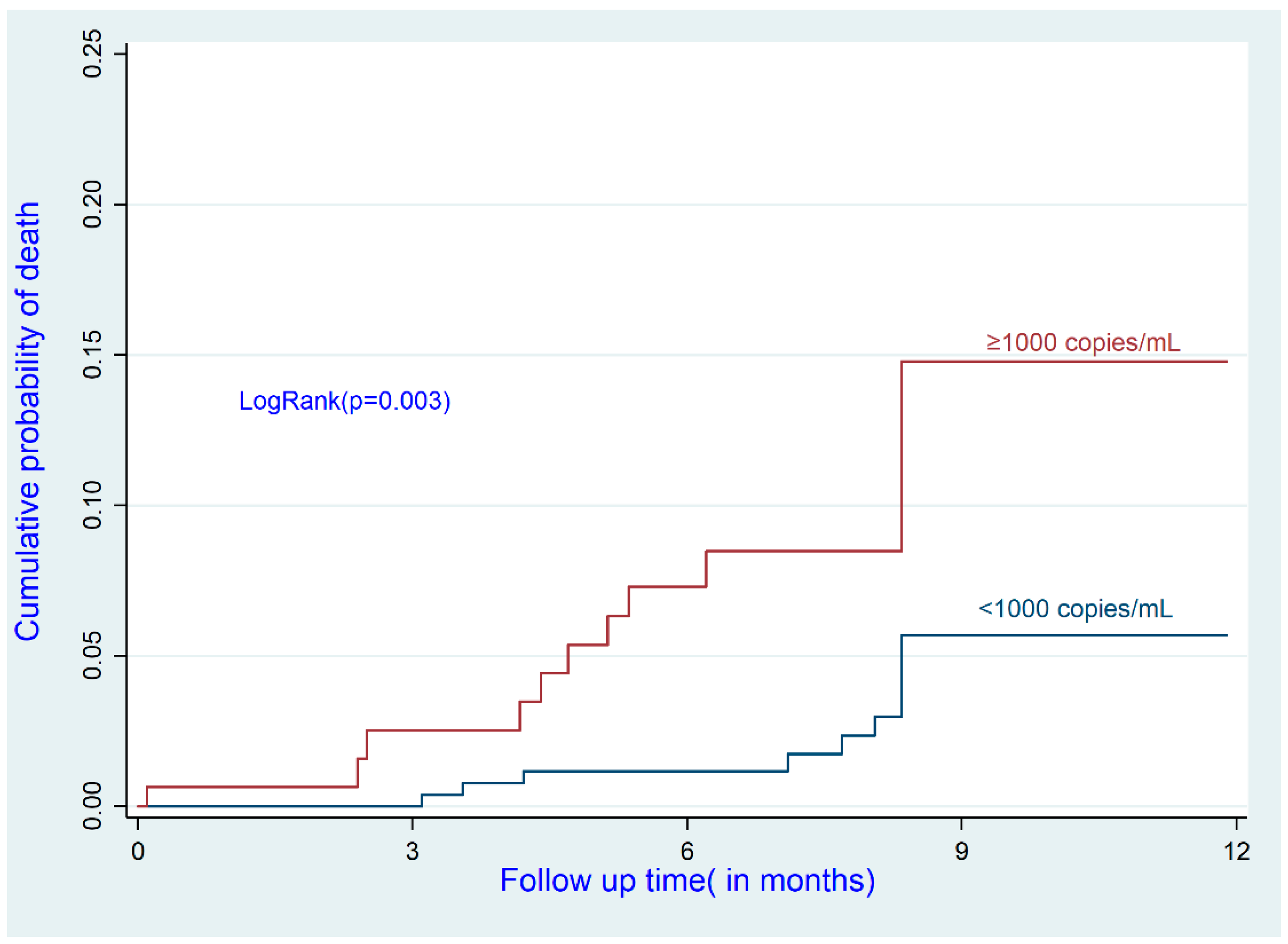
3.3. Predictors of Death among Patients with HIV on ART
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- ONUSIDA. Mettre Fin à L’épidémie du VIH-SIDA: Fiche D’information—Journée Mondiale de Lutte Contre le Sida; ONUSIDA: Geneva, Switzerland, 2021. [Google Scholar]
- Nishijima, T.; Inaba, Y.; Kawasaki, Y.; Tsukada, K.; Teruya, K.; Kikuchi, Y.; Gatanaga, H.; Oka, S. Mortality and causes of death in people living with HIV in the era of combination antiretroviral therapy compared with the general population in Japan. AIDS 2020, 34, 913–921. [Google Scholar] [CrossRef] [PubMed]
- UNAIDS DRC: HIV and AIDS Estimates. Available online: https://www.unaids.org/fr/regionscountries/countries/democraticrepublicofthecongo (accessed on 6 January 2022).
- Ramirez, J.A.B.; Franco, H.D. The Effect of Conflict and Displacement on the Health of Internally Displaced People: The Co-lombian Crisis. Univ. Ott. J. Med. 2016, 6, 26. [Google Scholar] [CrossRef]
- Buju, R.T.; Akilimali, P.Z.; Kamangu, E.N.; Mesia, G.K.; Kayembe, J.M.N.; Situakibanza, H.N. Predictors of Viral Non-Suppression among Patients Living with HIV under Dolutegravir in Bunia, Democratic Republic of Congo: A Prospective Cohort Study. Int. J. Environ. Res. Public Health 2022, 19, 1085. [Google Scholar] [CrossRef]
- Katherine, H.F.; Leonard, S.R. La santé dans les conflits armés: Une approche sous l’angle des droits de l’homme. Rev. Int. La Croix-Rouge 2013, 95, 93–116. [Google Scholar]
- Ferreyra, C.; O’Brien, D.; Alonso, B.; Al-Zomour, A.; Ford, N. Provision and continuation of antiretroviral therapy during acute conflict: The experience of MSF in Central African Republic and Yemen. Confl. Health 2018, 12, 30. [Google Scholar] [CrossRef]
- Inzaule, S.C.; Hamers, R.L.; Doherty, M.; Shafer, R.W.; Bertagnolio, S.; de Wit, T.F.R. Curbing the rise of HIV drug resistance in low-income and middle-income countries: The role of dolutegravir-containing regimens. Lancet Infect. Dis. 2019, 19, e246–e252. [Google Scholar] [CrossRef]
- Akilimali, P.Z.; Mutombo, P.B.; Kayembe, P.K.; Kaba, D.K.; Mapatano, M.A. Les déterminants de la survie des patients vivant avec le VIH sous thérapie antirétrovirale dans la ville de Goma, RD-Congo. Rev. Epidemiol. Sante Publique 2014, 62, 201–206. [Google Scholar] [CrossRef]
- Nigussie, F.; Alamer, A.; Mengistu, Z.; Tachbele, E. Survival and Predictors of Mortality Among Adult HIV/AIDS Patients Initiating Highly Active Antiretroviral Therapy in Debre-Berhan Referral Hospital, Amhara, Ethiopia: A Retrospective Study. HIV/AIDS Res. Palliat. Care 2020, 12, 757–768. [Google Scholar] [CrossRef]
- Damtew, B.; Mengistie, B.; Alemayehu, T. Survival and determinants of mortality in adult HIV/Aids patients initiating antiretroviral therapy in Somali Region, Eastern Ethiopia. Pan. Afr. Med. J. 2015, 22, 138. [Google Scholar] [CrossRef]
- Workie, K.L.; Birhan, T.Y.; Angaw, D.A. Predictors of mortality rate among adult HIV-positive patients on antiretroviral thera-py in Metema Hospital, Northwest Ethiopia: A retrospective follow-up study. AIDS Res. Ther. 2021, 18, 27. [Google Scholar] [CrossRef]
- Same, D.A.K.Y.; Billong, S.C.; Fokam, J.; Momo, P.T.; Amadou, S.; Nemb, M.N.; Ekali, G.L.; Lontchi, E.F.; Ngufor, R.; Nkomom, F.M.; et al. Survival Analysis among Patients receiving An-tiretroviral Therapy in Urban and Rural Settings of the Centre Region of Cameroon. Health Sci. Dis. 2016, 17, 2–7. [Google Scholar]
- Buju, R.T.; Akilimali, P.Z.; Kamangu, E.N.; Mesia, G.K.; Kayembe, J.M.N.; Situakibanza, H.N. Incidence and Predictors of Loss to Follow Up among Patients Living with HIV under Dolutegravir in Bunia, Democratic Republic of Congo: A Prospective Cohort Study. Int. J. Environ. Res. Public Health 2022, 19, 4631. [Google Scholar] [CrossRef]
- World Health Organization. Haemoglobin concentrations for the diagnosis of anaemia and assessment of severity. In Vitamin and Mineral Nutrition Information System; WHO: Geneva, Switzerland, 2011. [Google Scholar]
- Friedman, S.R.; Rossi, D.; Braine, N. Theorizing “big events” as a potential risk environment for drug use, drug-related harm and HIV epidemic outbreaks. Int. J. Drug Policy 2009, 20, 283–291. [Google Scholar] [CrossRef] [PubMed]
- Braitstein, P.; Brinkhof, M.W.; Dabis, F.; Schechter, M. Mortality of HIV-1-infected patients in the first year of antiretroviral the-rapy: Comparison between low-income and high-income countries. Lancet 2006, 367, 817. [Google Scholar] [PubMed]
- Zhou, C.; Zhang, W.; Lu, R.; Ouyang, L.; Xing, H.; Shao, Y.; Wu, G.; Ruan, Y. Higher Risk of Mortality and Virologic Failure in HIV-Infected Patients With High Viral Load at Antiretroviral Therapy Initiation: An Observational Cohort Study in Chongqing, China. Front. Public Health 2022, 10, 800839. [Google Scholar] [CrossRef]
- Eduardo, E.; Lamb, M.R.; Kandula, S.; Howard, A.; Mugisha, V.; Kimanga, D.; Kilama, B.; El-Sadr, W.; Elul, B. Characteristics and Outcomes among Older HIV-Positive Adults Enrolled in HIV Programs in Four Sub-Saharan African Countries. PLoS ONE 2014, 9, e103864. [Google Scholar] [CrossRef] [PubMed]
- Dawood, H.; Hassan-Moosa, R.; Zuma, N.-Y.; Naidoo, K. Mortality and treatment response amongst HIV-infected patients 50 years and older accessing antiretroviral services in South Africa. BMC Infect. Dis. 2018, 18, 168. [Google Scholar] [CrossRef]
- Guaraldi, G.; Orlando, G.; Zona, S.; Menozzi, M.; Carli, F.; Garlassi, E.; Berti, A.; Rossi, E.; Roverato, A.; Palella, F. Premature Age-Related Comorbidities Among HIV-Infected Persons Compared With the General Population. Clin. Infect. Dis. 2011, 53, 1120–1126. [Google Scholar] [CrossRef]
- Mesic, A.; Spina, A.; Mar, H.T.; Thit, P.; Decroo, T.; Lenglet, A.; Thandar, M.P.; Thwe, T.T.; Kyaw, A.A.; Homan, T.; et al. Predictors of virological failure among people living with HIV receiving first line antiretroviral treatment in Myanmar: Retrospective cohort analysis. AIDS Res. Ther. 2021, 18, 16. [Google Scholar] [CrossRef]
- Cao, W.; Hsieh, E.; Li, T. Optimizing Treatment for Adults with HIV/AIDS in China: Successes over Two Decades and Remaining Challenges. Curr. HIV/AIDS Rep. 2020, 17, 26–34. [Google Scholar] [CrossRef]
- Klugman, J.; Li, L.; Barker, K.M.; Parsons, J.; Dale, K. How are the domains of women’s inclusion, justice, and security associated with maternal and infant mortality across countries? Insights from the Women, Peace, and Security Index. SSM-Popul. Health 2019, 9, 100486. [Google Scholar] [CrossRef] [PubMed]
- Griffiths, K.; Ford, N. Provision of antiretroviral care to displaced populations in humanitarian settings: A systematic review. Med. Confl. Surviv. 2013, 29, 198–215. [Google Scholar] [CrossRef] [PubMed]
- Pyne-Mercier, L.D.; John-Stewart, G.C.; Richardson, B.A.; Kagondu, N.L.; Thiga, J.; Noshy, H.; Kist, N.; Chung, M.H. The consequences of post-election violence on antiretroviral HIV therapy in Kenya. AIDS Care 2011, 23, 562–568. [Google Scholar] [CrossRef] [PubMed][Green Version]




{kind=link}
{kind=link}
{kind=link}
| n | % | |
|---|---|---|
| Mean age (SD) | 38.97 (11.94) | |
| Age (years) | ||
| <35 | 183 | 39.1 |
| 35–45 | 161 | 34.4 |
| >45 | 124 | 25.5 |
| Sex | ||
| Female | 325 | 69.4 |
| Male | 143 | 30.6 |
| Education | ||
| None/primary | 307 | 65.6 |
| Secondary/tertiary | 161 | 34.4 |
| Marital status | ||
| Living alone | 263 | 56.2 |
| In union | 205 | 43.8 |
| Ethnic group | ||
| Nilotic | 224 | 47.9 |
| Bantou | 114 | 24.4 |
| Semi-Bantou | 93 | 19.9 |
| Sudanese | 37 | 7.9 |
| Tobacco consumption | ||
| No | 357 | 76.3 |
| Yes | 111 | 23.7 |
| Alcohol consumption | ||
| No | 265 | 56.6 |
| Yes | 203 | 43.4 |
| Total | 468 | 100.0 |
| Baseline Characteristics | n | % |
|---|---|---|
| HIV stage | ||
| I and II | 219 | 46.8 |
| III and IV | 249 | 53.2 |
| Status of treatment at baseline | ||
| Receiving ART | 291 | 62.2 |
| New but with VL suppressed | 93 | 19.9 |
| New but with high VL | 84 | 17.9 |
| Viral load at baseline | ||
| <1000 copies/mL | 313 | 66.9 |
| ≥1000 copies/mL | 155 | 33.1 |
| AgHBs | ||
| Negative | 449 | 95.9 |
| Positive | 19 | 4.1 |
| RPR | ||
| Negative | 397 | 84.8 |
| Positive | 71 | 15.2 |
| Hemoglobin mean (SD) | 13.84 (2.77) | |
| Anemia | ||
| No | 339 | 72.4 |
| Yes | 129 | 27.6 |
| Creatinine | ||
| Normal | 310 | 66.2 |
| Abnormal | 158 | 33.8 |
| ALAT | ||
| Normal | 431 | 92.1 |
| Abnormal | 37 | 7.9 |
| Loss to follow-up | ||
| No | 333 | 71.2 |
| Yes | 135 | 28.8 |
| Deceased | ||
| No | 445 | 95.1 |
| Yes | 23 | 4.9 |
| Total | 468 | 100.0 |
| n | Events (Death) | Person-Months | Incidence Rate of Death | Adjusted HR | 95%CI | p-Value (1) | |
|---|---|---|---|---|---|---|---|
| Age (years) | |||||||
| <35 | 183 | 2 | 1310.9 | 1.53 | 1 | ||
| 35–45 | 161 | 10 | 1177.23 | 8.49 | 5.14 | 1.09–24.18 | 0.038 |
| >45 | 124 | 11 | 947.09 | 11.61 | 5.47 | 1.13–26.38 | 0.034 |
| Gender | |||||||
| Female | 325 | 11 | 2428.58 | 4.53 | 1 | ||
| Male | 143 | 12 | 1006.64 | 11.92 | 1.27 | 0.50–3.18 | 0.610 |
| WHO HIV stage | |||||||
| Stage I and II | 219 | 8 | 1795 | 4.46 | 1 | ||
| Stage III and IV | 249 | 15 | 1640.22 | 9.15 | 1.38 | 0.57–3.35 | 0.469 |
| Creatinine | |||||||
| Normal | 310 | 12 | 2421.23 | 4.96 | 1 | ||
| Abnormal | 158 | 11 | 1013.99 | 10.85 | 1.84 | 0.79–4.25 | 0.153 |
| Status of treatment before enrollment | |||||||
| Under ART | 291 | 7 | 2288.08 | 3.06 | 1 | ||
| Naïve but suppressed VL | 93 | 6 | 676.68 | 8.87 | 5.43 | 1.59–18.48 | 0.007 |
| Naïve but high VL | 84 | 10 | 470.46 | 21.26 | 2.29 | 0.78–6.74 | 0.131 |
| Viral load at baseline | |||||||
| <1000 copies/mL | 313 | 10 | 2458.52 | 4.07 | 1 | ||
| ≥1000 copies/mL | 155 | 13 | 976.7 | 13.31 | 6.04 | 1.78–20.43 | 0.004 |
| Overall | 468 | 23 | 3435.22 | 6.70 |
| Baseline Characteristics | Related to Armed Conflict | p-Value * | |||
|---|---|---|---|---|---|
| Yes | No | ||||
| n | % | n | % | ||
| Age, mean | 44.83 ± 15.39 | 47.76 ± 12.27 | ns | ||
| Age (years) | ns | ||||
| <35 | 1 | 16.7 | 1 | 5.9 | |
| 35–45 | 1 | 16.7 | 9 | 52.9 | |
| >45 | 4 | 66.6 | 7 | 41.2 | |
| Sex | ns | ||||
| Female | 4 | 66.7 | 7 | 41.2 | |
| Male | 2 | 33.3 | 10 | 58.8 | |
| WHO HIV stage | ns | ||||
| Stage I or II | 4 | 66.7 | 4 | 23.5 | |
| Stage III or IV | 2 | 33.3 | 13 | 76.5 | |
| Creatinine | ns | ||||
| Normal | 2 | 33.3 | 10 | 58.8 | |
| Abnormal | 4 | 66.7 | 7 | 41.2 | |
| Status of treatment before enrollment | ns | ||||
| Receiving ART | 2 | 33.3 | 5 | 29.4 | |
| New but with VL suppressed | 2 | 33.3 | 4 | 23.5 | |
| New but with high VL | 2 | 33.3 | 8 | 47.1 | |
| Viral load at baseline | ns | ||||
| <1000 copies/mL | 3 | 50.0 | 7 | 41.2 | |
| ≥1000 copies/mL | 3 | 50.0 | 10 | 58.8 | |
| Total | 6 | 26.1 | 17 | 73.9 | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Buju, R.T.; Akilimali, P.Z.; Tran, N.-T.; Kamangu, E.N.; Mesia, G.K.; Kayembe, J.M.N.; Situakibanza, H.N. Determinants of Survival of HIV Patients Receiving Dolutegravir: A Prospective Cohort Study in Conflict-Affected Bunia, Democratic Republic of Congo. Int. J. Environ. Res. Public Health 2022, 19, 10220. https://doi.org/10.3390/ijerph191610220
Buju RT, Akilimali PZ, Tran N-T, Kamangu EN, Mesia GK, Kayembe JMN, Situakibanza HN. Determinants of Survival of HIV Patients Receiving Dolutegravir: A Prospective Cohort Study in Conflict-Affected Bunia, Democratic Republic of Congo. International Journal of Environmental Research and Public Health. 2022; 19(16):10220. https://doi.org/10.3390/ijerph191610220
Chicago/Turabian StyleBuju, Roger T., Pierre Z. Akilimali, Nguyen-Toan Tran, Erick N. Kamangu, Gauthier K. Mesia, Jean Marie N. Kayembe, and Hippolyte N. Situakibanza. 2022. "Determinants of Survival of HIV Patients Receiving Dolutegravir: A Prospective Cohort Study in Conflict-Affected Bunia, Democratic Republic of Congo" International Journal of Environmental Research and Public Health 19, no. 16: 10220. https://doi.org/10.3390/ijerph191610220
APA StyleBuju, R. T., Akilimali, P. Z., Tran, N.-T., Kamangu, E. N., Mesia, G. K., Kayembe, J. M. N., & Situakibanza, H. N. (2022). Determinants of Survival of HIV Patients Receiving Dolutegravir: A Prospective Cohort Study in Conflict-Affected Bunia, Democratic Republic of Congo. International Journal of Environmental Research and Public Health, 19(16), 10220. https://doi.org/10.3390/ijerph191610220