
Pesticide Exposure in Relation to the Incidence of Abnormal Glucose Regulation: A Retrospective Cohort Study



Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Population
2.2. Covariates
2.3. Data Collection
2.4. Exposure Assessment
2.5. Statistical Analysis
3. Results
3.1. Descriptive Statistics of Variables
3.2. Incidence of AGR According to Pesticide Exposure
3.3. RRs of the Incidence of AGR by Variables Related to Pesticide Exposure
3.4. RRs of AGR Incidence by Variables Related to Pesticide Exposure in Male Participants
3.5. RRs of AGR Incidence by Variables Related to Pesticide Exposure in Female Participants
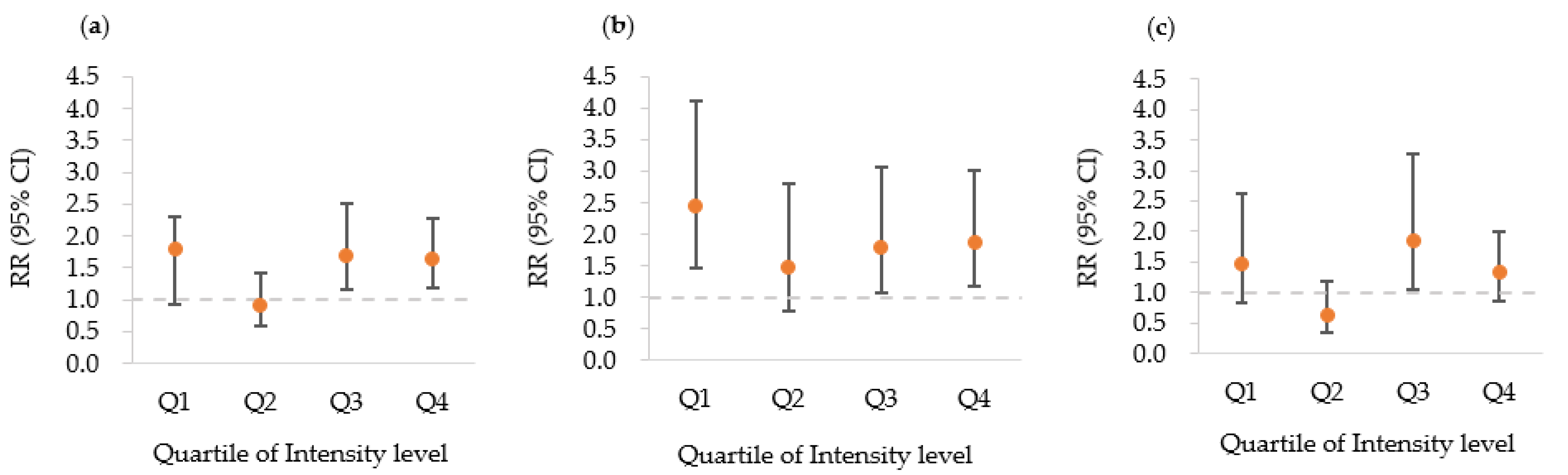
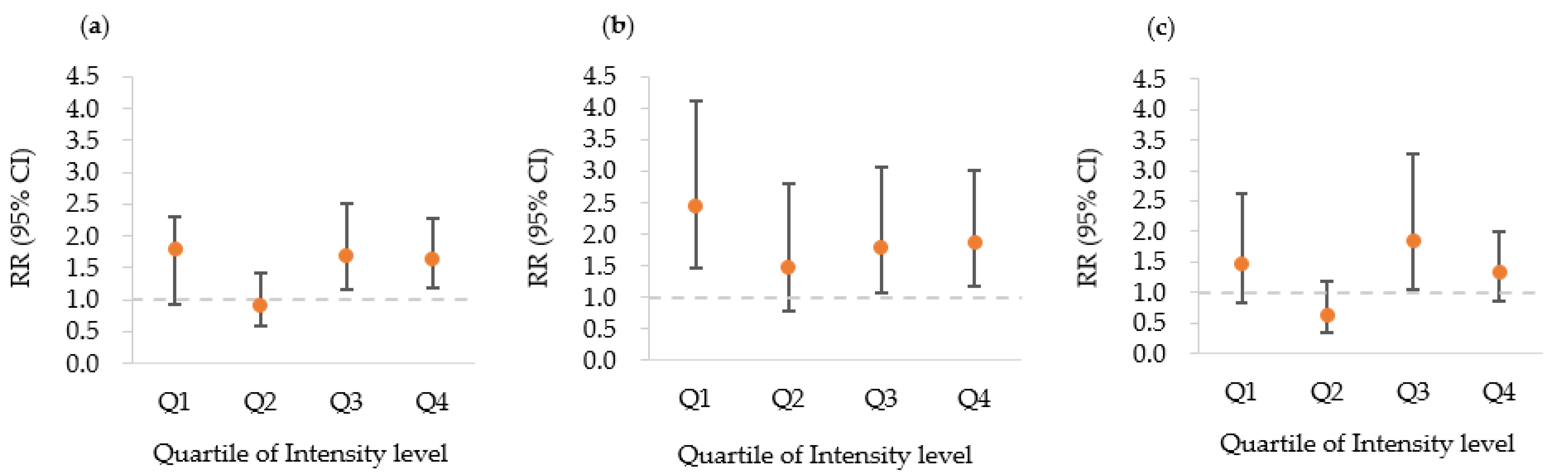
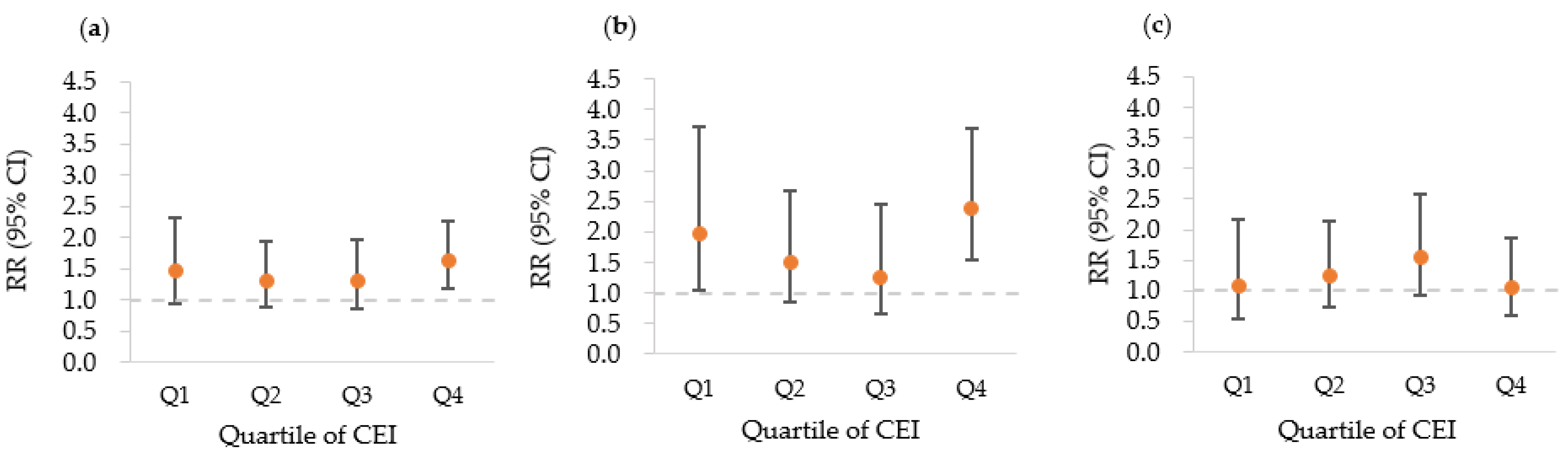
3.6. Dose–Response Patterns between Pesticide Exposure and Incidence of AGR
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Jeyaratnam, J. Acute pesticide poisoning: A major global health problem. World Health Stat. Q. 1990, 43, 139–144. [Google Scholar] [PubMed]
- Gilden, R.C.; Huffling, K.; Sattler, B. Pesticides and health risks. J Obstet. Gynecol. Neonatal Nurs. 2010, 39, 103–110. [Google Scholar] [CrossRef] [PubMed]
- Guerrero, S.; Muñoz, A. Agri-Environmental Indicators: Land Use, Pesticides and Biodiversity in Farmland; OECD: Paris, France, 2019; pp. 1–31. [Google Scholar]
- Firbank, L.G.; Petit, S.; Smart, S.; Blain, A.; Fuller, R.J. Assessing the impacts of agricultural intensification on biodiversity: A British perspective. Philos. Trans. R. Soc. B Biol. Sci. 2008, 363, 777–787. [Google Scholar] [CrossRef] [PubMed]
- Carmichael, S.L.; Yang, W.; Ma, C.; Roberts, E.; Kegley, S.; English, P.; Lammer, E.J.; Witte, J.S.; Shaw, G. Joint effects of genetic variants and residential proximity to pesticide applications on hypospadias risk. Birth Defects Res. Part A Clin. Mol. Teratol. 2016, 106, 653–658. [Google Scholar] [CrossRef] [Green Version]
- Mabuchi, K.; Lilienfeld, A.M.; Snell, L.M. Lung cancer among pesticide workers exposed to inorganic arsenicals. Arch. Environ. Health 1979, 34, 312–320. [Google Scholar] [CrossRef]
- Hancock, D.B.; Martin, E.R.; Mayhew, G.M.; Stajich, J.M.; Jewett, R.; Stacy, M.A.; Scott, B.L.; Vance, J.M.; Scott, W.K. Pesticide exposure and risk of Parkinson’s disease: A family-based case-control study. BMC Neurol. 2008, 8, 6. [Google Scholar] [CrossRef] [Green Version]
- Rasoul, G.M.A.; Salem, M.E.A.; Mechael, A.A.; Hendy, O.M.; Rohlman, D.S.; Ismail, A.A. Effects of occupational pesticide exposure on children applying pesticides. Neurotoxicology 2008, 29, 833–838. [Google Scholar] [CrossRef]
- Band, P.R.; Abanto, Z.; Bert, J.; Lang, B.; Fang, R.; Gallagher, R.P.; Le, N.D. Prostate cancer risk and exposure to pesticides in British Columbia farmers. Prostate 2011, 71, 168–183. [Google Scholar] [CrossRef]
- Colosio, C.; Corsini, E.; Barcellini, W.; Maroni, M. Immune parameters in biological monitoring of pesticide exposure: Current knowledge and perspectives. Toxicol. Lett. 1999, 108, 285–295. [Google Scholar] [CrossRef]
- Cha, E.S.; Lee, Y.K.; Moon, E.K.; Kim, Y.B.; Lee, Y.-J.; Jeong, W.C.; Cho, E.Y.; Lee, I.J.; Hur, J.; Ha, M.J. Paraquat application and respiratory health effects among South Korean farmers. Occup. Environ. Med. 2012, 69, 398–403. [Google Scholar] [CrossRef]
- World Health Organization. Global Health Risks: Mortality and Burden of Disease Attributable to Selected Major Risks; World Health Organization: Geneva, Switzerland, 2009. [Google Scholar]
- Baena-Díez, J.M.; Peñafiel, J.; Subirana, I.; Ramos, R.; Elosua, R.; Marín-Ibañez, A.; Guembe, M.J.; Rigo, F.; Tormo-Díaz, M.J.; Moreno-Iribas, C. Risk of cause-specific death in individuals with diabetes: A competing risks analysis. Diabetes Care 2016, 39, 1987–1995. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bartnik, M.; Malmberg, K.; Norhammar, A.; Tenerz, A.; Ohrvik, J.; Ryden, L. Newly detected abnormal glucose tolerance: An important predictor of long-term outcome after myocardial infarction. Eur. Heart J. 2004, 25, 1990–1997. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Di Pino, A.; Scicali, R.; Calanna, S.; Urbano, F.; Mantegna, C.; Rabuazzo, A.M.; Purrello, F.; Piro, S. Cardiovascular risk profile in subjects with prediabetes and new-onset type 2 diabetes identified by HbA1c according to American diabetes association criteria. Diabetes Care 2014, 37, 1447–1453. [Google Scholar] [CrossRef] [Green Version]
- Bartnik, M.; Rydén, L.; Ferrari, R.; Malmberg, K.; Pyörälä, K.; Simoons, M.; Standl, E.; Soler-Soler, J.; Öhrvik, J.; EHS Investigators. The prevalence of abnormal glucose regulation in patients with coronary artery disease across Europe: The Euro Heart Survey on diabetes and the heart. Eur. Heart J. 2004, 25, 1880–1890. [Google Scholar] [CrossRef] [PubMed]
- Zhu, Z.; Yang, J.; Zhong, C.; Xu, T.; Wang, A.; Bu, X.; Peng, Y.; Peng, H.; Xu, T.; Chen, C.-S.; et al. Abnormal glucose regulation, hypoglycemic treatment during hospitalization and prognosis of acute ischemic stroke. J. Neurol. Sci. 2017, 379, 177–182. [Google Scholar] [CrossRef]
- Jia, Q.; Zheng, H.; Zhao, X.; Wang, C.; Liu, G.; Wang, Y.; Liu, L.; Li, H.; Zhong, L.; Wang, Y. Abnormal glucose regulation in patients with acute stroke across China: Prevalence and baseline patient characteristics. Stroke 2012, 43, 650–657. [Google Scholar] [CrossRef] [Green Version]
- World Health Organization. Package of Essential Noncommunicable (PEN) Disease Interventions for Primary Health Care in Low-Resource Settings; World Health Organization: Geneva, Switzerland, 2010. [Google Scholar]
- Waugh, N.; Scotland, G.; McNamee, P.; Gillett, M.; Brennan, A.; Goyder, E.; Williams, R.; John, A. Screening for type 2 diabetes: Literature review and economic modelling. Health Technol. Assess. 2007, 11. [Google Scholar] [CrossRef] [Green Version]
- Blas, E.; Kurup, A.S. Equity, Social Determinants and Public Health Programmes; World Health Organization: Geneva, Switzerland, 2010. [Google Scholar]
- Lasram, M.M.; Dhouib, I.B.; Bouzid, K.; Lamine, A.J.; Annabi, A.; Belhadjhmida, N.; Ahmed, M.B.; El Fazaa, S.; Abdelmoula, J.; Gharbi, N. Association of inflammatory response and oxidative injury in the pathogenesis of liver steatosis and insulin resistance following subchronic exposure to malathion in rats. Environ. Toxicol. Pharmacol. 2014, 38, 542–553. [Google Scholar] [CrossRef]
- Montgomery, M.; Kamel, F.; Saldana, T.M.; Alavanja, M.; Sandler, D.P. Incident diabetes and pesticide exposure among licensed pesticide applicators: Agricultural Health Study, 1993–2003. Am. J. Epidemiol. 2008, 167, 1235–1246. [Google Scholar] [CrossRef]
- Evangelou, E.; Ntritsos, G.; Chondrogiorgi, M.; Kavvoura, F.K.; Hernández, A.F.; Ntzani, E.E.; Tzoulaki, I. Exposure to pesticides and diabetes: A systematic review and meta-analysis. Environ. Int. 2016, 91, 60–68. [Google Scholar] [CrossRef]
- Kim, S.-K.; Park, S.; Chang, S.-J.; Kim, S.-K.; Song, J.S.; Kim, H.-R.; Oh, S.-S.; Koh, S.-B. Pesticides as a risk factor for metabolic syndrome: Population-based longitudinal study in Korea. Mol. Cell. Toxicol. 2019, 15, 431–441. [Google Scholar] [CrossRef]
- Dosemeci, M.; Alavanja, M.C.; Rowland, A.S.; Mage, D.; Zahm, S.H.; Rothman, N.; Lubin, J.H.; Hoppin, J.A.; Sandler, D.P.; Blair, A. A quantitative approach for estimating exposure to pesticides in the Agricultural Health Study. Ann. Occup. Hyg. 2002, 46, 245–260. [Google Scholar] [PubMed] [Green Version]
- Coble, J.; Arbuckle, T.; Lee, W.; Alavanja, M.; Dosemeci, M. The validation of a pesticide exposure algorithm using biological monitoring results. J. Occup. Environ. Hyg. 2005, 2, 194–201. [Google Scholar] [CrossRef] [PubMed]
- Lee, W.J.; Cha, E.S. Overview of pesticide poisoning in South Korea. J. Rural Med. 2009, 4, 53–58. [Google Scholar] [CrossRef] [Green Version]
- Cha, E.S.; Jeong, M.; Lee, W.J. Agricultural pesticide usage and prioritization in South Korea. J. Agromedicine 2014, 19, 281–293. [Google Scholar] [CrossRef]
- Lee, K.M.; Park, S.-Y.; Lee, K.; Oh, S.-S.; Ko, S.B. Pesticide metabolite and oxidative stress in male farmers exposed to pesticide. Ann. Occup. Environ. Med. 2017, 29, 5. [Google Scholar] [CrossRef] [Green Version]
- American Diabetes Association. 2. Classification and diagnosis of diabetes: Standards of medical care in diabetes-2020. Diabetes Care 2020, 43 (Suppl. S1), S14. [Google Scholar]
- Mayega, R.W.; Guwatudde, D.; Makumbi, F.E.; Nakwagala, F.N.; Peterson, S.; Tomson, G.; Östenson, C.-G. Comparison of fasting plasma glucose and haemoglobin A1c point-of-care tests in screening for diabetes and abnormal glucose regulation in a rural low income setting. Diabetes Res. Clin. Pract. 2014, 104, 112–120. [Google Scholar] [CrossRef] [Green Version]
- Greenland, S. Interpretation and choice of effect measures in epidemiologic analyses. Am. J. Epidemiol. 1987, 125, 761–768. [Google Scholar] [CrossRef]
- Arbuckle, T.E. Are there sex and gender differences in acute exposure to chemicals in the same setting? Environ. Res. 2006, 101, 195–204. [Google Scholar] [CrossRef]
- Henry, R.M.; Kostense, P.J.; Spijkerman, A.M.; Dekker, J.M.; Nijpels, G.; Heine, R.J.; Kamp, O.; Westerhof, N.; Bouter, L.M.; Stehouwer, C.D. Arterial stiffness increases with deteriorating glucose tolerance status: The Hoorn Study. Circulation 2003, 107, 2089–2095. [Google Scholar] [CrossRef] [PubMed]
- Kaur, N.; Starling, A.P.; Calafat, A.M.; Sjodin, A.; Clouet-Foraison, N.; Dolan, L.M.; Imperatore, G.; Jensen, E.T.; Lawrence, J.M.; Ospina, M. Longitudinal association of biomarkers of pesticide exposure with cardiovascular disease risk factors in youth with diabetes. Environ. Res. 2020, 181, 108916. [Google Scholar] [CrossRef] [PubMed]
- Lee, D.-H.; Steffes, M.W.; Sjödin, A.; Jones, R.S.; Needham, L.L.; Jacobs, D.R., Jr. Low dose of some persistent organic pollutants predicts type 2 diabetes: A nested case–control study. Environ. Health Perspect. 2010, 118, 1235–1242. [Google Scholar] [CrossRef]
- Rohlman, D.S.; Anger, W.K.; Lein, P.J. Correlating neurobehavioral performance with biomarkers of organophosphorouspesticide exposure. Neurotoxicology 2011, 32, 268–276. [Google Scholar] [CrossRef] [Green Version]
- Albasher, G.; Albrahim, T.; Alsultan, N.; Alfaraj, S.; Alharthi, M.S.; Kassab, R.B.; Moneim, A.E.A. Red beetroot extract mitigates chlorpyrifos-induced reprotoxicity associated with oxidative stress, inflammation, and apoptosis in rats. Environ. Sci. Pollut. Res. Int. 2020, 27, 3979–3991. [Google Scholar] [CrossRef]
- Aouey, B.; Derbali, M.; Chtourou, Y.; Bouchard, M.; Khabir, A.; Fetoui, H. Pyrethroid insecticide lambda-cyhalothrin and its metabolites induce liver injury through the activation of oxidative stress and proinflammatory gene expression in rats following acute and subchronic exposure. Environ. Sci. Pollut. Res. Int. 2017, 24, 5841–5856. [Google Scholar] [CrossRef]
- Duzguner, V.; Erdogan, S. Acute oxidant and inflammatory effects of imidacloprid on the mammalian central nervous system and liver in rats. Pestic. Biochem. Phys. 2010, 97, 13–18. [Google Scholar] [CrossRef]
- Lee, D.-H.; Jacobs, D.R.; Steffes, M. Association of organochlorine pesticides with peripheral neuropathy in patients with diabetes or impaired fasting glucose. Diabetes. 2008, 57, 3108–3111. [Google Scholar] [CrossRef] [Green Version]
- Song, Y.; Chou, E.L.; Baecker, A.; You, N.C.Y.; Song, Y.; Sun, Q.; Liu, S. Endocrine-disrupting chemicals, risk of type 2 diabetes, and diabetes-related metabolic traits: A systematic review and meta-analysis. J. Diabetes. 2016, 8, 516–532. [Google Scholar] [CrossRef]
- Alberti, K.G.M.M.; Zimmet, P.; Shaw, J. Metabolic syndrome—A new world-wide definition. A consensus statement from the international diabetes federation. Diabet. Med. 2006, 23, 469–480. [Google Scholar] [CrossRef]
- Ben Khadda, Z.; Fagroud, M.; El Karmoudi, Y.; Ezrari, S.; Berni, I.; De Broe, M.; Behl, T.; Bungau, S.G.; Sqalli Houssaini, T. Farmers’ knowledge, attitudes, and perceptions regarding carcinogenic pesticides in Fez Meknes region (Morocco). Int. J. Environ. Res. 2021, 18, 10879. [Google Scholar] [CrossRef] [PubMed]
- Lily, M.; Godwin, M. Treating prediabetes with metformin: Systematic review and meta-analysis. Can. Fam. Physician 2009, 55, 363–369. [Google Scholar] [PubMed]
- Hostalek, U.; Gwilt, M.; Hildemann, S. Therapeutic use of metformin in prediabetes and diabetes prevention. Drugs 2015, 75, 1071–1094. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Davidson, M.B. Metformin Should Not Be Used to Treat Prediabetes. Diabetes Care 2020, 43, 1983–1987. [Google Scholar] [CrossRef] [PubMed]
- Behl, T.; Kaur, I.; Sehgal, A.; Singh, S.; Sharma, N.; Bhatia, S.; Al-Harrasi, A.; Bungau, S. The dichotomy of nanotechnology as the cutting edge of agriculture: Nano-farming as an asset versus nanotoxicity. Chemosphere 2022, 288, 132533. [Google Scholar] [CrossRef]
- Mamane, A.; Baldi, I.; Tessier, J.-F.; Raherison, C.; Bouvier, G. Occupational exposure to pesticides and respiratory health. Eur. Respir. Rev. 2015, 24, 306–319. [Google Scholar] [CrossRef] [Green Version]
- Knudsen, E.C.; Seljeflot, I.; Abdelnoor, M.; Eritsland, J.; Mangschau, A.; Arnesen, H.; Andersen, G.Ø. Abnormal glucose regulation in patients with acute ST-elevation myocardial infarction-a cohort study on 224 patients. Cardiovasc. Diabetol. 2009, 8, 6. [Google Scholar] [CrossRef] [Green Version]


{kind=link}
{kind=link}
| Demographic Characteristics | Pesticide Use | p-Value | |
|---|---|---|---|
| No (n = 660) | Yes (n = 502) | ||
| Mean (±SD) * or Frequency (%) ** | |||
| Sex | |||
| Male | 159 (27.0%) | 236 (48.4%) | <0.0001 |
| Female | 429 (73.0%) | 252 (51.6%) | |
| Age (years) | 52.8 (±8.1) | 54.7 (±8.0) | <0.0001 |
| Fasting glucose (mg/dL) | 87.1 (±6.2) | 87.5 (±6.0) | 0.32 |
| HbA1c (%) | 5.21 (±0.01) | 5.28 (±0.10) | <0.0001 |
| BMI (kg/m2) | 23.9 (±2.9) | 24.3 (±3.1) | 0.02 |
| Smoking status | |||
| Non-smoker | 485 (82.8%) | 338 (69.8%) | <0.0001 |
| Ex-smoker | 41 (7.0%) | 65 (13.4%) | |
| Current smoker | 60 (10.2%) | 81 (16.8%) | |
| Alcohol use | |||
| No | 377 (64.4%) | 256 (52.6%) | <0.0001 |
| Yes | 208 (35.6%) | 231 (47.4%) | |
| Regular exercise | |||
| No | 354 (60.7%) | 416 (86.0%) | <0.0001 |
| Yes | 229 (39.3%) | 68 (14.0%) | |
| Monthly income (Korean won) | |||
| <1,500,000 | 255 (47.2%) | 312 (74.6%) | <0.0001 |
| ≥1,500,000 | 285 (52.8%) | 106 (25.4%) | |
| Education | |||
| Elementary school or below | 207 (35.3%) | 318 (65.3%) | <0.0001 |
| Middle school or higher | 379 (64.7%) | 169 (34.7%) | |
| Marital status | |||
| Married | 511 (87.4%) | 450 (93.6%) | <0.001 |
| Others | 74 (12.6%) | 31 (6.4%) | |
| Pesticide-Related Variables | Incidence of AGR, n (%) | p-Value * |
|---|---|---|
| Pesticide use | 0.026 | |
| No | 136 (23.1%) | |
| Yes | 142 (29.1%) | |
| Pesticide mixing status | 0.238 | |
| No | 176 (24.3%) | |
| <50% of the instances | 38 (30.7%) | |
| >50% of the instances | 64 (28.0%) | |
| Application method | 0.062 | |
| No | 136 (23.1%) | |
| Seed treatment or tablet distribution | 30 (25.2%) | |
| Backpack | 18 (37.5%) | |
| Hand spray | 58 (31.7%) | |
| Mist blower/fogger or air-blast | 36 (26.1%) | |
| Years of pesticide use | 0.104 | |
| 0 | 136 (23.1%) | |
| ≤15 | 28 (27.5%) | |
| ≤25 | 34 (25.0%) | |
| ≤30 | 29 (27.9%) | |
| >30 | 39 (35.1%) | |
| Frequency of pesticide use (per year) | 0.092 | |
| 0 | 136 (23.1%) | |
| ≤7 | 39 (35.5%) | |
| ≤15 | 28 (27.5%) | |
| ≤20 | 29 (25.4%) | |
| >20 | 30 (28.0%) | |
| Scores for PPE | 0.140 | |
| 0 | 136 (23.1%) | |
| ≤0.6 | 37 (28.0%) | |
| <1 | 16 (26.2%) | |
| 1 | 89 (30.2%) | |
| Intensity level of pesticide exposure | <0.001 | |
| 0 | 136 (23.1%) | |
| ≤4 | 25 (39.7%) | |
| ≤9 | 27 (20.3%) | |
| ≤12 | 29 (34.5%) | |
| >12 | 61 (29.3%) | |
| CEI of pesticide exposure | 0.201 | |
| 0 | 136 (23.1%) | |
| ≤448 | 16 (34.0%) | |
| ≤2160 | 32 (28.3%) | |
| ≤5000 | 28 (25.9%) | |
| >5000 | 48 (30.4%) |
| Pesticide-Related Variables | Crude RR (95% CI) | RR (95% CI) * | RR (95% CI) ** |
|---|---|---|---|
| Pesticide use | |||
| No | 1 (reference) | 1 (reference) | 1 (reference) |
| Yes | 1.26 (1.03–1.54) | 1.25 (1.02–1.53) | 1.32 (1.03–1.69) |
| Pesticide mixing status | |||
| No | 1 (reference) | 1 (reference) | 1 (reference) |
| <50% of the instances | 1.35 (1.00–1.83) | 1.35 (0.99–1.84) | 1.33 (0.92–1.91) |
| >50% of the instances | 1.16 (0.91–1.48) | 1.20 (0.93–1.56) | 1.30 (0.98–1.74) |
| Application method | |||
| No | 1 (reference) | 1 (reference) | 1 (reference) |
| Seed treatment or tablet distribution | 1.08 (0.77–1.52) | 1.03 (0.73–1.47) | 1.14 (0.75–1.73) |
| Backpack | 1.61 (1.09–2.39) | 1.72 (1.14–2.58) | 1.74 (1.13–2.66) |
| Hand spray | 1.41 (1.08–1.83) | 1.46 (1.10–1.92) | 1.55 (1.12–2.15) |
| Mist blower/fogger or air-blast | 1.59 (1.08–2.34) | 1.20 (0.86–1.67) | 1.36 (0.94–1.95) |
| Years of pesticide use | |||
| 0 | 1 (reference) | 1 (reference) | 1 (reference) |
| ≤15 | 1.22 (0.86–1.74) | 1.24 (0.87–1.77) | 1.26 (0.85–1.87) |
| ≤25 | 1.10 (0.79–1.54) | 1.17 (0.84 –1.64) | 1.35 (0.93–1.97) |
| ≤30 | 1.24 (0.87–1.75) | 1.23 (0.87–1.76) | 1.40 (0.92–2.12) |
| >30 | 1.55 (1.15–2.08) | 1.45 (1.07–1.98) | 1.69 (1.17–2.45) |
| Frequency of pesticide use (per year) | |||
| 0 | 1 (reference) | 1 (reference) | 1 (reference) |
| ≤7 | 1.60 (1.19–2.16) | 1.51 (1.11–2.06) | 1.57 (1.10–2.26) |
| ≤15 | 1.18 (0.83–1.67) | 1.18 (0.83–1.68) | 1.35 (0.92–1.97) |
| ≤20 | 1.17 (0.82–1.67) | 1.16 (0.81–1.65) | 1.31 (0.86–1.98) |
| >20 | 1.20 (0.86–1.69) | 1.27 (0.90–1.81) | 1.41 (0.97–2.06) |
| Scores for PPE | |||
| 0 | 1 (reference) | 1 (reference) | 1 (reference) |
| 0.1–0.8 | 1.22 (0.93–1.61) | 1.24 (0.93–1.65) | 1.41 (1.02–1.93) |
| 1 | 1.32 (1.05–1.67) | 1.30 (1.03–1.64) | 1.39 (1.06–1.84) |
| Intensity level of pesticide exposure | |||
| 0 | 1 (reference) | 1 (reference) | 1 (reference) |
| ≤4 | 1.70 (1.21–2.39) | 1.72 (1.22–2.43) | 1.80 (1.24–2.60) |
| ≤9 | 0.90 (0.62–1.31) | 0.90 (0.62–1.31) | 0.92 (0.59–1.42) |
| ≤12 | 1.53 (1.10–2.14) | 1.58 (1.13–2.23) | 1.69 (1.15–2.50) |
| >12 | 1.30 (1.00–1.69) | 1.28 (0.98–1.67) | 1.48 (1.08–2.02) |
| CEI of pesticide exposure | |||
| 0 | 1 (reference) | 1 (reference) | 1 (reference) |
| ≤448 | 1.46 (0.96–2.23) | 1.42 (0.91–2.20) | 1.46 (0.93–2.31) |
| ≤2160 | 1.29 (0.92–1.81) | 1.29 (0.92–1.81) | 1.31 (0.89–1.94) |
| ≤5000 | 1.11 (0.78–1.58) | 1.14 (0.80–1.64) | 1.29 (0.85–1.95) |
| >5000 | 1.36 (1.02–1.80) | 1.36 (1.02–1.82) | 1.63 (1.18–2.27) |
| Pesticide-Related Variables | Crude RR (95% CI) | RR (95% CI) * | RR (95% CI) ** |
|---|---|---|---|
| Pesticide use | |||
| No | 1 (reference) | 1 (reference) | 1 (reference) |
| Yes | 1.45 (1.01–2.1) | 1.44 (1.00–2.08) | 1.81 (1.22–2.67) |
| Mixing status of pesticide | |||
| No | 1 (reference) | 1 (reference) | 1 (reference) |
| <50% of the instances | 1.39 (0.88–2.20) | 1.37 (0.87–2.16) | 1.69 (1.04–2.76) |
| >50% of the instances | 1.31 (0.90–1.91) | 1.30 (0.89–1.90) | 1.66 (1.11–2.47) |
| Application method | |||
| No | 1 (reference) | 1 (reference) | 1 (reference) |
| Seed treatment or tablet distribution | 2.48 (1.16–5.31) | 2.48 (1.15–5.34) | 2.77 (1.48–5.20) |
| Backpack | 1.86 (1.12–3.09) | 1.83 (1.11–3.01) | 2.26 (1.35–3.78) |
| Hand spray | 1.44 (0.93–2.21) | 1.42 (0.92–2.19) | 1.75 (1.10–2.78) |
| Mist blower/fogger or air-blaster | 1.21 (0.73–2.01) | 1.21 (0.73–2.00) | 1.61 (0.93–2.79) |
| Years of pesticide use | |||
| 0 | 1 (reference) | 1 (reference) | 1 (reference) |
| ≤15 | 1.09 (0.60–2.01) | 1.10 (0.60–2.02) | 1.19 (0.63–2.25) |
| ≤25 | 1.04 (0.59–1.85) | 1.05 (0.59–1.86) | 1.64 (0.95–2.81) |
| ≤30 | 1.63 (1.01–2.63) | 1.62 (1.00–2.62) | 2.45 (1.46–4.12) |
| >30 | 2.02 (1.30–3.14) | 1.97 (1.26–3.09) | 3.03 (1.74–5.27) |
| Frequency of pesticide use (per year) | |||
| 0 | 1 (reference) | 1 (reference) | 1 (reference) |
| ≤7 | 1.93 (1.21–3.08) | 1.88 (1.17–3.02) | 2.14 (1.28–3.55) |
| ≤15 | 1.18 (0.68–2.05) | 1.16 (0.67–2.02) | 1.52 (0.86–2.67) |
| ≤20 | 1.50 (0.87–2.58) | 1.48 (0.86–2.54) | 2.01 (1.09–3.71) |
| >20 | 1.44 (0.89–2.33) | 1.45 (0.90–2.35) | 1.86 (1.15–3.02) |
| Scores for PPE | |||
| 0 | 1 (reference) | 1 (reference) | 1 (reference) |
| 0.1–0.8 | 2.14 (1.29–3.55) | 2.01 (1.09–3.71) | 1.54 (0.98–2.44) |
| 1 | 1.52 (0.86–2.67) | 1.87 (1.15–3.02) | 1.30 (0.70–2.41) |
| Intensity level of pesticide exposure | |||
| 0 | 1 (reference) | 1 (reference) | 1 (reference) |
| ≤4 | 1.96 (1.19–3.24) | 1.94 (1.17–3.20) | 2.45 (1.45–4.12) |
| ≤9 | 1.20 (0.67–2.15) | 1.18 (0.66–2.11) | 1.47 (0.77–2.80) |
| ≤12 | 1.52 (0.90–2.57) | 1.52 (0.91–2.56) | 1.80 (1.06–3.07) |
| >12 | 1.42 (0.91–2.22) | 1.40 (0.89–2.20) | 1.88 (1.18–3.01) |
| CEI of pesticide exposure | |||
| 0 | 1 (reference) | 1 (reference) | 1 (reference) |
| ≤448 | 1.72 (0.93–3.17) | 1.73 (0.93–3.19) | 1.96 (1.04–3.71) |
| ≤2160 | 1.51 (0.91–2.50) | 1.48 (0.89–2.45) | 1.50 (0.85–2.63) |
| ≤5000 | 0.83 (0.44–1.54) | 0.83 (0.44–1.54) | 1.26 (0.65–2.44) |
| >5000 | 1.90 (1.24–2.91) | 1.88 (1.23–2.88) | 2.39 (1.54–3.70) |
| Pesticide-Related Variables | Crude RR (95% CI) | RR (95% CI) * | RR (95% CI) ** |
|---|---|---|---|
| Pesticide use | |||
| No | 1 (reference) | 1 (reference) | 1 (reference) |
| Yes | 1.19 (0.93–1.54) | 1.16 (0.89–1.49) | 1.10 (0.80–1.51) |
| Mixing status of pesticide | |||
| No | 1 (reference) | 1 (reference) | 1 (reference) |
| <50% of the instances | 1.44 (0.93–2.23) | 1.37 (0.89–2.12) | 1.11 (0.63–1.95) |
| >50% of the instances | 1.10 (0.76–1.60) | 1.12 (0.77–1.62) | 1.17 (0.75–1.81) |
| Application method | |||
| No | 1 (reference) | 1 (reference) | 1 (reference) |
| Seed treatment or tablet distribution | 0.96 (0.66–1.39) | 0.94 (0.65–1.37) | 0.92 (0.57–1.46) |
| Backpack | 1.53 (0.62–3.81) | 1.52 (0.61–3.77) | 1.11 (0.36–3.41) |
| Hand spray | 1.60 (1.12–2.28) | 1.54 (1.07–2.22) | 1.50 (0.94–2.40) |
| Mist blower/fogger or air-blaster | 1.28 (0.82–1.99) | 1.19 (0.77–1.85) | 1.25 (0.76–2.04) |
| Years of pesticide use | |||
| 0 | 1 (reference) | 1 (reference) | 1 (reference) |
| ≤15 | 1.41 (0.91–2.19) | 1.36 (0.89–2.07) | 1.31 (0.83–2.07) |
| ≤25 | 1.21 (0.81–1.83) | 1.31 (0.87–1.97) | 1.34 (0.82–2.18) |
| ≤30 | 0.98 (0.54–1.78) | 0.91 (0.50–1.66) | 0.79 (0.35–1.80) |
| >30 | 1.22 (0.76–1.95) | 1.08 (0.66–1.77) | 1.10 (0.60–2.02) |
| Frequency of pesticide use (per year) | |||
| 0 | 1 (reference) | 1 (reference) | 1 (reference) |
| ≤7 | 1.47 (0.97–2.23) | 1.32 (0.86–2.02) | 1.26 (0.77–2.08) |
| ≤15 | 1.33 (0.84–2.11) | 1.31 (0.82–2.09) | 1.40 (0.83–2.35) |
| ≤20 | 1.00 (0.61–1.67) | 0.98 (0.60–1.60) | 0.93 (0.49–1.77) |
| >20 | 1.08 (0.62–1.88) | 1.15 (0.65–2.02) | 1.09 (0.54–2.17) |
| Scores for PPE | |||
| 0 | 1 (reference) | 1 (reference) | 1 (reference) |
| 0.1–0.8 | 0.99 (0.61–1.60) | 0.99 (0.61–1.61) | 1.23 (0.73–2.05) |
| 1 | 1.63 (0.74–3.61) | 1.54 (0.74–3.22) | 1.40 (0.59–3.31) |
| Intensity level of pesticide exposure | |||
| 0 | 1 (reference) | 1 (reference) | 1 (reference) |
| ≤4 | 1.63 (0.98–2.72) | 1.56 (0.94–2.59) | 1.46 (0.82–2.61) |
| ≤9 | 0.76 (0.46–1.26) | 0.75 (0.45–1.24) | 0.63 (0.33–1.19) |
| ≤12 | 1.75 (1.11–2.77) | 1.74 (1.10–2.75) | 1.85 (1.05–3.27) |
| >12 | 1.29 (0.93–1.80) | 1.22 (0.88–1.71) | 1.32 (0.87–1.99) |
| CEI of pesticide exposure | |||
| 0 | 1 (reference) | 1 (reference) | 1 (reference) |
| ≤448 | 1.36 (0.73–2.55) | 1.14 (0.59–2.23) | 1.09 (0.55–2.17) |
| ≤2160 | 1.22 (0.75–1.99) | 1.23 (0.76–1.98) | 1.25 (0.73–2.14) |
| ≤5000 | 1.65 (1.10–2.48) | 1.63 (1.09–2.43) | 1.54 (0.93–2.57) |
| >5000 | 1.01 (0.64–1.58) | 0.99 (0.63–1.55) | 1.06 (0.60–1.85) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kim, S.-K.; Oh, H.-J.; Oh, S.-S.; Koh, S.-B. Pesticide Exposure in Relation to the Incidence of Abnormal Glucose Regulation: A Retrospective Cohort Study. Int. J. Environ. Res. Public Health 2022, 19, 7550. https://doi.org/10.3390/ijerph19127550
Kim S-K, Oh H-J, Oh S-S, Koh S-B. Pesticide Exposure in Relation to the Incidence of Abnormal Glucose Regulation: A Retrospective Cohort Study. International Journal of Environmental Research and Public Health. 2022; 19(12):7550. https://doi.org/10.3390/ijerph19127550
Chicago/Turabian StyleKim, Sung-Kyung, Hyun-Jung Oh, Sung-Soo Oh, and Sang-Baek Koh. 2022. "Pesticide Exposure in Relation to the Incidence of Abnormal Glucose Regulation: A Retrospective Cohort Study" International Journal of Environmental Research and Public Health 19, no. 12: 7550. https://doi.org/10.3390/ijerph19127550
APA StyleKim, S.-K., Oh, H.-J., Oh, S.-S., & Koh, S.-B. (2022). Pesticide Exposure in Relation to the Incidence of Abnormal Glucose Regulation: A Retrospective Cohort Study. International Journal of Environmental Research and Public Health, 19(12), 7550. https://doi.org/10.3390/ijerph19127550