
Harmful Alcohol and Drug Use Is Associated with Syndemic Risk Factors among Female Sex Workers in Nairobi, Kenya

 ,
,  , , , , , ,
, , , , , ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design and Setting
2.2. Data Collection and Study Procedures
2.2.1. Quantitative Data
2.2.2. Laboratory Methods
2.2.3. Qualitative Data
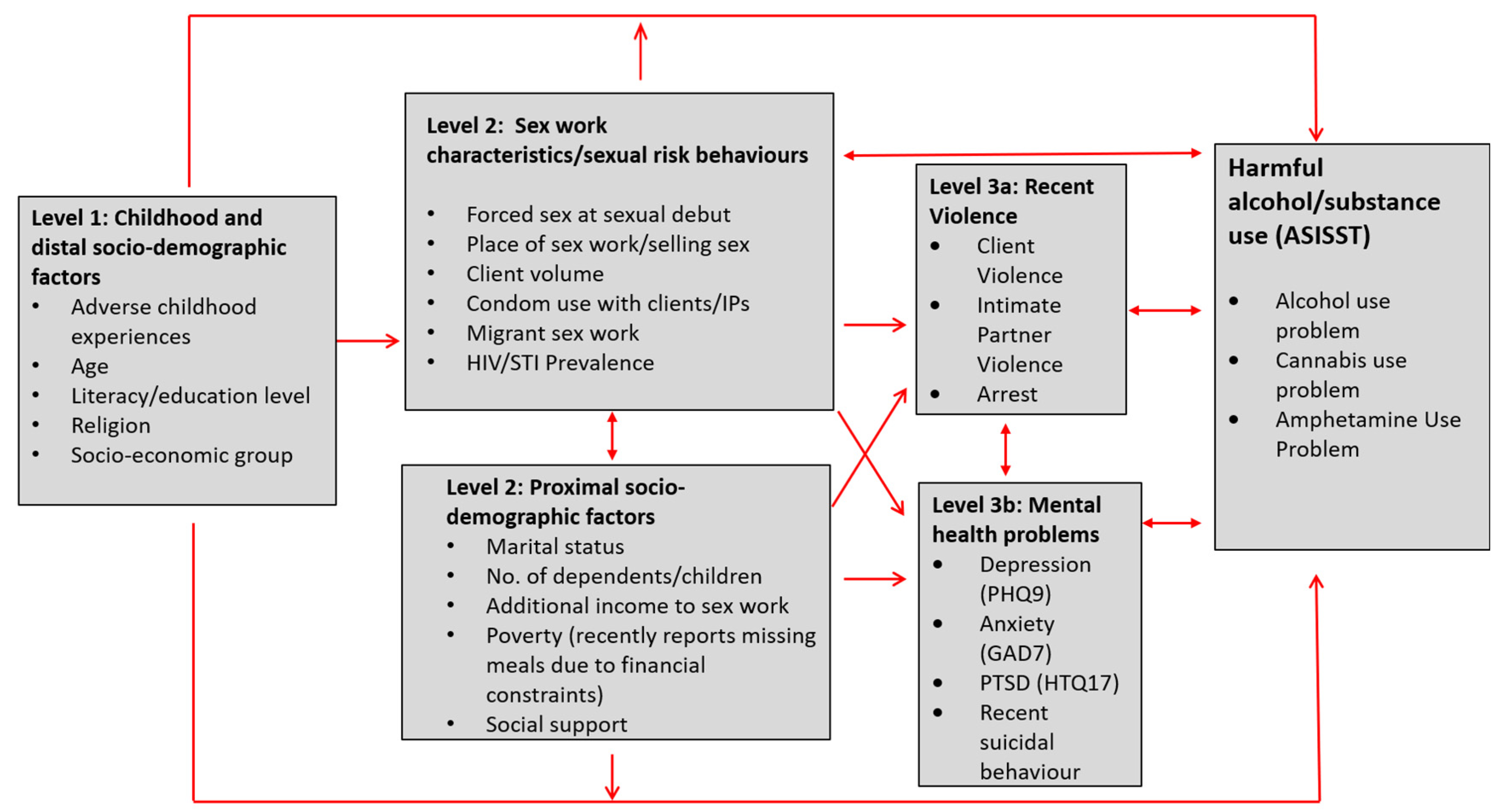
2.3. Integration of Mixed Methods and Conceptual Framework
2.4. Analyses
2.4.1. Quantitative Analyses
2.4.2. Qualitative Analyses
2.4.3. Ethical Considerations
3. Results
3.1. Sample Demographics
3.2. Adverse Childhood Experiences
“I therefore decided to move out of my grandmother’s and I moved in with this man but he was not a peaceful man he was violent …… He loved fighting and verbal abuse lots of insults…. He used to hold the knife on me and point it towards me and I would just watch.”(MF 033)
3.3. Age and Socio-Demographic Differences in Alcohol and Substance Use
“Mine it does not affect me. You know I drink controllably and I will not drink to the extent that I am so drunk, and it is not every day.”(MF 282)
I: So…how much do you drink in a given day? R: If it is beer because me I love beer so much; I will take… ten. I: You take ten bottles? R: Yes, that is for the whole night… You are bought by a client there because if you dance well they tell you sit down and be given [a drink], will you refuse?(MF 240)
“I: So khat helps. R: It helps. I: And what side effects does it have? R: And again when you chew khat you can’t get drunk.”(MF282)
“Muguka (khat) is very cheap.”(MF0569)
3.4. Alcohol and Other Drug Use during Sex Work
“I don’t drink daily, I take when am going to work because of that fear… to remove that fear.”(MF024)
“Sometimes it [bhang] calms me. Because in this job you face so many challenges… So me when I smoke I feel good, relaxed, and if I don’t smoke when going to the streets I will not work.”(MF0569)
“There is a time I used to drink that is when I was at risk. Because you would find that you go to work drunk and to negotiate with a client about the condom will be a bit tough because yourself you are drunk, you find that you just had sex without the condom. So those days I was on PEP a lot but I was advised that it is either I reduce alcohol or I stop [drinking] completely.”(MF 012)
“I… another one his drunkenness is showing him [in] fights. So you see instead of fighting just do what brought you there [sex work], and the next day you know what to do. Me that is when I go [to] SWOP to pick PEPs….”(MF 255)
“I used to get so drunk… I had to tell even the people from SWOP and they told me to reduce. Because…the drugs [ARVs] will not work you will even forget to take.”(MF497)
3.5. Family Relationships, Mental and Physical Health
R: “I used to get so drunk that even when my children see me they would start crying.... I had to tell even the people from SWOP and they told me to reduce. Because these children of yours first you will give them stress, second they will join that behaviour you are showing them… Now that is where I started because I was like at times when I get to the house and you ask me a question I will respond with a kick.”(MF 497)
I: “Is there a possibility that one can become an addict? R: I literally smoke bhang everyday whether I am going to work or not even while in the house I have to smoke bhang.”(MF132)
4. Discussion
Strengths and Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- James, S.L.; Abate, D.; Abate, K.H.; Abay, S.M.; Abbafati, C.; Abbasi, N.; Abbastabar, H.; Abd-Allah, F.; Abdela, J.; Abdelalim, A.; et al. Global, regional, and national incidence, prevalence, and years lived with disability for 354 diseases and injuries for 195 countries and territories, 1990–2017: A systematic analysis for the Global Burden of Disease Study 2017. Lancet 2018, 392, 1789–1858. [Google Scholar] [CrossRef] [Green Version]
- Global Burden of Disease Collaborative Network. In Global Burden of Disease Study 2017: Incidence, Prevalence, and Years Lived with Disability 1990—2017; Institute for Health Metrics and Evaluation: Seattle, DA, USA; Available online: http://ghdx.healthdata.org/record/ihme-data/gbd-2017-incidence-prevalence-and-ylds-1990–2017 (accessed on 1 April 2022).
- World Health Organisation. Global Status Report on Alcohol and Health 2018. WHO: Geneva, Switzerland; Available online: https://www.who.int/publications/i/item/9789241565639 (accessed on 1 April 2022).
- Walls, H.; Cook, S.; Matzopoulos, R.; London, L. Advancing alcohol research in low-income and middle-income countries: A global alcohol environment framework. BMJ Glob. Health 2020, 5, e001958. [Google Scholar] [CrossRef]
- Ferreira-Borges, C.; Parry, C.D.H.; Babor, T.F. Harmful Use of Alcohol: A Shadow over Sub-Saharan Africa in Need of Workable Solutions. Int. J. Environ. Res. Public Health 2017, 14, 346. [Google Scholar] [CrossRef] [Green Version]
- UNAIDS. Sex Work and HIV/AIDS: Technical Update; UNAIDS: Geneva, Switzerland, 2002; Available online: https://data.unaids.org/publications/irc-pub02/jc705-sexwork-tu_en.pdf (accessed on 1 April 2022).
- Platt, L.; Grenfell, P.; Meiksin, R.; Elmes, J.; Sherman, S.G.; Sanders, T.; Mwamgi, P.; Crago, A.-L. Associations between sex work laws and sex workers’ health: A systematic review and meta-analysis of quantitative and qualitative studies. PLoS Med. 2018, 15, e1002680. [Google Scholar] [CrossRef]
- Mbonye, M.; Nakamanya, S.; Nalukenge, W.; King, R.; Vandepitte, J.; Seeley, J. ‘It is like a tomato stall where someone can pick what he likes’: Structure and practices of female sex work in Kampala, Uganda. BMC Public Health 2013, 13, 741. [Google Scholar] [CrossRef] [Green Version]
- Li, Q.; Li, X.; Stanton, B. Alcohol use among female sex workers and male clients: An integrative review of global literature. Alcohol Alcohol. 2010, 45, 188–199. [Google Scholar] [CrossRef] [Green Version]
- Karlsen, O. Alcohol and Substance Use among Female Sex Workers in Low- and Middle- Income Countries: A Systematic Review and Meta-Analysis. 2019; unpublished. [Google Scholar]
- Mbonye, M.; Nalukenge, W.; Nakamanya, S.; Nalusiba, B.; King, R.; Vandepitte, J.; Seeley, J. Gender inequity in the lives of women involved in sex work in Kampala, Uganda. J. Int. AIDS Soc. 2012, 15 (Suppl. S1), 1–9. [Google Scholar] [CrossRef]
- Bukenya, J.; Vandepitte, J.; Kwikiriza, M.; Weiss, H.A.; Hayes, R.; Grosskurth, H. Condom use among female sex workers in Uganda. AIDS Care. 2013, 25, 767–774. [Google Scholar] [CrossRef]
- Norris, A.H.; Kitali, A.J.; Worby, E. Alcohol and transactional sex: How risky is the mix? Soc. Sci. Med. 2009, 69, 1167–1176. [Google Scholar] [CrossRef]
- Woolf-King, S.E.; Maisto, S.A. Alcohol use and high-risk sexual behavior in Sub-Saharan Africa: A narrative review. Arch. Sex Behav. 2011, 40, 17–42. [Google Scholar] [CrossRef]
- Chen, Y.Y.; Li, X.M.; Zhang, C.; Hong, Y.; Zhou, Y.J.; Liu, W. Alcohol Use and Sexual Risks: Use of the Alcohol Use Disorders Identification Test (AUDIT) Among Female Sex Workers in China. Health Care Women Int. 2013, 34, 122–138. [Google Scholar] [CrossRef] [Green Version]
- Chersich, M.F.; Bosire, W.; King’ola, N.; Temmerman, M.; Luchters, S. Effects of hazardous and harmful alcohol use on HIV incidence and sexual behaviour: A cohort study of Kenyan female sex workers. Glob. Health 2014, 10, 22. [Google Scholar] [CrossRef] [Green Version]
- Lancaster, K.E.; MacLean, S.A.; Lungu, T.; Mmodzi, P.; Hosseinipour, M.C.; Hershow, R.B.; Powers, K.A.; Pence, B.W.; Hoffman, I.F.; Miller, W.C.; et al. Socioecological Factors Related to Hazardous Alcohol use among Female Sex Workers in Lilongwe, Malawi: A Mixed Methods Study. Subst. Use Misuse 2018, 53, 782–791. [Google Scholar] [CrossRef] [Green Version]
- Bazzi, A.R.; Yotebieng, K.; Otticha, S.; Rota, G.; Agot, K.; Ohaga, S.; Syvertsen, J.L. PrEP and the syndemic of substance use, violence, and HIV among female and male sex workers: A qualitative study in Kisumu, Kenya. J. Int. AIDS Soc. 2019, 22, e25266. [Google Scholar] [CrossRef]
- Evens, E.; Lanham, M.; Santi, K.; Cooke, J.; Ridgeway, K.; Morales, G.; Parker, C.; Brennan, C.; de Bruin, M.; Desrosiers, P.C.; et al. Experiences of gender-based violence among female sex workers, men who have sex with men, and transgender women in Latin America and the Caribbean: A qualitative study to inform HIV programming. BMC Int. Health Hum. Rights 2019, 19, 9. [Google Scholar] [CrossRef]
- Beattie, T.; Smilenova, B.; Krishnaratne, S.; Mazzuca, A. Mental Health Problems among Female Sex Workers in Low- and Middle-Income Countries: A Systematic Review and Meta-Analysis. PLoS Med. 2020, 17, e1003297. [Google Scholar] [CrossRef]
- Hughes, K.; Bellis, M.A.; Hardcastle, K.A.; Sethi, D.; Butchart, A.; Mikton, C.; Jones, L.; Dunne, M.P. The effect of multiple adverse childhood experiences on health: A systematic review and meta-analysis. Lancet Public Health 2017, 2, e356–e366. [Google Scholar] [CrossRef] [Green Version]
- Singer, M.; Clair, S. Syndemics and public health: Reconceptualizing disease in bio-social context. Med. Anthropol. Q. 2003, 17, 423–441. [Google Scholar] [CrossRef]
- White, D.; Wilson, K.S.; Masese, L.N.; Wanje, G.; Jaoko, W.; Mandaliya, K.; Richardson, B.A.; Kinuthia, J.; Simoni, J.M.; McClelland, S. Alcohol Use and Associations With Biological Markers and Self-Reported Indicators of Unprotected Sex in Human Immunodeficiency Virus-Positive Female Sex Workers in Mombasa, Kenya. Sex Transm. Dis. 2016, 43, 642–647. [Google Scholar] [CrossRef] [Green Version]
- Wilson, K.S.; Deya, R.; Yuhas, K.; Simoni, J.; Vander Stoep, A.; Shafi, J.; Jaoko, W.; Hughes, J.P.; Richardson, B.A.; McClelland, R.S. A Prospective Cohort Study of Intimate Partner Violence and Unprotected Sex in HIV-Positive Female Sex Workers in Mombasa, Kenya. AIDS Behav. 2016, 20, 2054–2064. [Google Scholar] [CrossRef] [Green Version]
- Pack, A.P.; L’engle, K.; Mwarogo, P.; Kingola, N. Intimate partner violence against female sex workers in Mombasa, Kenya. Cult. Health Sex 2014, 16, 217–230. [Google Scholar] [CrossRef] [PubMed]
- Parcesepe, A.M.; Engle, L.K.L.; Martin, S.L.; Green, S.; Sinkele, W.; Suchindran, C.; Speizer, I.S.; Mwarogo, P.; Kingola, N. The impact of an alcohol harm reduction intervention on interpersonal violence and engagement in sex work among female sex workers in Mombasa, Kenya: Results from a randomized controlled trial. Drug Alcohol Depend. 2016, 161, 21–28. [Google Scholar] [CrossRef] [Green Version]
- van der Elst, E.M.; Okuku, H.S.; Nakamya, P.; Muhaari, A.; Davies, A.; McClelland, R.S.; Price, M.A.; Smith, A.D.; Graham, S.M.; Sanders, E.J. Is audio computer-assisted self-interview (ACASI) useful in risk behaviour assessment of female and male sex workers, Mombasa, Kenya? PLoS ONE 2009, 4, e5340. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Beckerleg, S.; Telfer, M.; Hundt, G.L. The rise of injecting drug use in east Africa: A case study from Kenya. Harm. Reduct. J. 2005, 2, 12. [Google Scholar] [CrossRef] [Green Version]
- Syvertsen, J.L.; Agot, K.; Ohaga, S.; Bazzi, A.R. You can’t do this job when you are sober: Heroin use among female sex workers and the need for comprehensive drug treatment programming in Kenya. Drug Alcohol Depend. 2019, 194, 495–499. [Google Scholar] [CrossRef]
- Semple, S.J.; Pitpitan, E.V.; Chavarin, C.V.; Strathdee, S.A.; Zavala, R.I.; Aarons, G.A.; Patterson, T. Prevalence and Correlates of Hazardous Drinking among Female Sex Workers in 13 Mexican Cities. Alcohol Alcohol. 2016, 51, 450–456. [Google Scholar] [CrossRef] [Green Version]
- Bhattacharjee, P.; Musyoki, H.; Prakash, R.; Malaba, S.; Dallabetta, G.; Wheeler, T.; Moses, S.; Isac, S.; Steen, R. Micro-planning at scale with key populations in Kenya: Optimising peer educator ratios for programme outreach and HIV/STI service utilisation. PLoS ONE 2018, 13, e0205056. [Google Scholar] [CrossRef]
- Beksinska, A.; Jama, Z.; Kabuti, R.; Kungu, M.; Babu, H.; Nyariki, E.; Shah, P.; Nyabuto, C.; Okumu, M.; Mahero, A.; et al. Prevalence and correlates of common mental health problems and recent suicidal thoughts and behaviours among female sex workers in Nairobi, Kenya. BMC Psychiatry 2021, 21, 503. [Google Scholar] [CrossRef]
- Masson, L.; Passmore, J.-A.S.; Liebenberg, L.J.; Werner, L.; Baxter, C.; Arnold, K.B.; Williamson, C.; Little, F.; Mansoor, L.E.; Naranbhai, V.; et al. Genital inflammation and the risk of HIV acquisition in women. Clin. Infect. Dis. 2015, 61, 260–269. [Google Scholar] [CrossRef] [Green Version]
- NACC and NASCOP. Kenya AIDS Epidemic Update 2012. National Aids Control Council. 2012. Available online: http://guidelines.health.go.ke:8000/media/FINAL_Kenya_Update_2012_30_May.pdf (accessed on 13 June 2022).
- Wanjiru, R.; Nyariki, E.; Babu, H.; Lwingi, I.; Liku, J.; Jama, Z.; Kung’u, M.; Ngurukiri, P.; The Maisha Fiti Study Champions; Nyamwaya, C.; et al. Beaten but not down! Exploring resilience among female sex workers (FSWs) in Nairobi, Kenya. BMC Public Health 2022, 22, 965. [Google Scholar] [CrossRef]
- World Health Organisation (WHO). The Alcohol, Smoking and Substance Involvement Screening Test (ASSIST): Manual for use in Primary Care Geneva: WHO; 2010. Available online: https://www.who.int/publications/i/item/978924159938-2 (accessed on 13 June 2022).
- McNeely, J.; Strauss, S.M.; Wright, S.; Rotrosen, J.; Khan, R.; Lee, J.D.; Gourevitch, M.N. Test-retest reliability of a self-administered Alcohol, Smoking and Substance Involvement Screening Test (ASSIST) in primary care patients. J. Subst. Abuse Treat. 2014, 47, 93–101. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- World Health Organisation. Adverse Childhood Experiences International Questionnaire; WHO: Geneva, Switzerland, 2018; Available online: https://www.who.int/publications/m/item/adverse-childhood-experiences-international-questionnaire-(ace-iq) (accessed on 13 June 2022).
- Christoforou, R.; Ferreira, N. Psychometric Assessment of Adverse Childhood Experiences International Questionnaire (ACE-IQ) with Adults Engaging in Non-Suicidal Self-Injury. Mediter. J. Clin. Psychol. 2020, 8. [Google Scholar] [CrossRef]
- Kroenke, K.; Spitzer, R.L.; Williams, J.B. The PHQ-9: Validity of a brief depression severity measure. J. Gen. Intern Med. 2001, 16, 606–613. [Google Scholar] [CrossRef]
- Spitzer, R.L.; Kroenke, K.; Williams, J.B.; Löwe, B. A brief measure for assessing generalized anxiety disorder: The GAD-7. Arch. Intern Med. 2006, 166, 1092–1097. [Google Scholar] [CrossRef] [Green Version]
- Kleijn, W.C.; Hovens, J.E.; Rodenburg, J.J. Posttraumatic stress symptoms in refugees: Assessments with the Harvard Trauma Questionnaire and the Hopkins symptom Checklist-25 in different languages. Psychol. Rep. 2001, 88, 527–532. [Google Scholar] [CrossRef]
- World Health Organisation. WHO multi-country study on women’s health and domestic violence against women: Initial results on prevalence, health outcomes and women’s responses. Geneva. 2005. Available online: https://apps.who.int/iris/handle/10665/43309 (accessed on 13 June 2022).
- Krieger, N. Methods for the scientific study of discrimination and health: An ecosocial approach. Am. J. Public Health 2012, 102, 936–944. [Google Scholar] [CrossRef]
- Shannon, K.; Goldenberg, S.M.; Deering, K.N.; Strathdee, S.A. HIV infection among female sex workers in concentrated and high prevalence epidemics: Why a structural determinants framework is needed. Curr. Opin. HIV AIDS 2014, 9, 174–182. [Google Scholar] [CrossRef] [Green Version]
- Shannon, K.; Strathdee, S.A.; Goldenberg, S.M.; Duff, P.; Mwangi, P.; Rusakova, M.; Reza-Paul, S.; Lau, J.; Deering, K.; Pickles, M.R.; et al. Global epidemiology of HIV among female sex workers: Influence of structural determinants. Lancet 2015, 385, 55–71. [Google Scholar] [CrossRef] [Green Version]
- Victora, C.G.; Huttly, S.R.; Fuchs, S.C.; Olinto, M.T. The role of conceptual frameworks in epidemiological analysis: A hierarchical approach. Int. J. Epidemiol. 1997, 26, 224–227. [Google Scholar] [CrossRef] [Green Version]
- Rutakumwa, R.; Mugisha, J.O.; Bernays, S.; Kabunga, E.; Tumwekwase, G.; Mbonye, M.; Seeley, J. Conducting in-depth interviews with and without voice recorders: A comparative analysis. Qual. Res. 2019, 20, 565–581. [Google Scholar] [CrossRef] [Green Version]
- Kendagor, A.; Gathecha, G.; Ntakuka, M.W.; Nyakundi, P.; Gathere, S.; Kiptui, D.; Akbubakar, H.; Ombiro, O.; Juma, P.; Ngaruiya, C. Prevalence and determinants of heavy episodic drinking among adults in Kenya: Analysis of the STEPwise survey, 2015. BMC Public Health 2018, 18 (Suppl. S3), 1216. [Google Scholar] [CrossRef] [PubMed]
- National Authority for the Campaign Against Alcohol and Drug Abuse. Rapid Situation Assessment of the Status of Drug and Substance Abuse in Kenya, 2012; NACA: Nairobi, Kenya, 2012; Available online: https://www.nacada.go.ke/sites/default/files/2019-10/National%20ADA%20Survey%20Report%202017_2_2.pdf (accessed on 13 June 2022).
- Ongeri, L.; Kirui, F.; Muniu, E.; Manduku, V.; Kirumbi, L.; Atwoli, L.; Agure, S.; Wanzala, P.; Kaduka, L.; Karimi, M.; et al. Khat use and psychotic symptoms in a rural Khat growing population in Kenya: A household survey. BMC Psychiatry 2019, 19, 137. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Young, J.T.; Butt, J.; Hersi, A.; Tohow, A.; Mohamed, D.H. Khat Dependence, Use Patterns, and Health Consequences in Australia: An Exploratory Study. J. Stud. Alcohol. Drugs 2016, 77, 343–348. [Google Scholar] [CrossRef]
- Odenwald, M.; Neuner, F.; Schauer, M.; Elbert, T.; Catani, C.; Lingenfelder, B.; Hinkel, H.; Häfner, H.; Rockstroh, B. Khat use as risk factor for psychotic disorders: A cross-sectional and case-control study in Somalia. BMC Med. 2005, 3, 5. [Google Scholar] [CrossRef] [Green Version]
- Jewkes, R.K.; Dunkle, K.; Nduna, M.; Jama, P.N.; Puren, A. Associations between childhood adversity and depression, substance abuse and HIV and HSV2 incident infections in rural South African youth. Child Abuse Negl. 2010, 34, 833–841. [Google Scholar] [CrossRef] [Green Version]
- Dunkle, K.L.; Jewkes, R.K.; Brown, H.C.; Yoshihama, M.; Gray, G.E.; McIntyre, J.A.; Harlow, S.D. Prevalence and patterns of gender-based violence and revictimization among women attending antenatal clinics in Soweto, South Africa. Am. J. Epidemiol. 2004, 160, 230–239. [Google Scholar] [CrossRef] [Green Version]
- Gatuguta, A.; Colombini, M.; Seeley, J.; Soremekun, S.; Devries, K. Supporting children and adolescents who have experienced sexual abuse to access services: Community health workers’ experiences in Kenya. Child Abuse Negl. 2021, 116, 104244. [Google Scholar] [CrossRef]
- Scorgie, F.; Chersich, M.F.; Ntaganira, I.; Gerbase, A.; Lule, F.; Lo, Y.R. Socio-demographic characteristics and behavioral risk factors of female sex workers in sub-saharan Africa: A systematic review. AIDS Behav. 2012, 16, 920–933. [Google Scholar] [CrossRef]
- Abramsky, T.; Devries, K.; Kiss, L.; Nakuti, J.; Kyegombe, N.; Starmann, E.; Cundill, B.; Francisco, L.; Kaye, D.; Musuya, T.; et al. Findings from the SASA! Study: A cluster randomized controlled trial to assess the impact of a community mobilization intervention to prevent violence against women and reduce HIV risk in Kampala, Uganda. BMC Med. 2014, 12, 122. [Google Scholar] [CrossRef] [Green Version]
- Kapiga, S.; Harvey, S.; Mshana, G.; Hansen, C.H.; Mtolela, G.J.; Madaha, F.; Hashim, R.; Kapinga, I.; Mosha, N.; Abramsky, T.; et al. A social empowerment intervention to prevent intimate partner violence against women in a microfinance scheme in Tanzania: Findings from the MAISHA cluster randomised controlled trial. Lancet Glob. Health 2019, 7, e1423–e1434. [Google Scholar] [CrossRef] [Green Version]
- Beattie, T.S.; Bhattacharjee, P.; Isac, S.; Mohan, H.L.; Simic-Lawson, M.; Ramesh, B.M.; Blanchard, F.; Moses, S.; Watts, C.H.; Heise, L. Declines in violence and police arrest among female sex workers in Karnataka state, south India, following a comprehensive HIV prevention programme. J. Int. Aids Soc. 2015, 18, 20079. [Google Scholar] [CrossRef]
- Boden, J.M.; Fergusson, D.M. Alcohol and depression. Addiction 2011, 106, 906–914. [Google Scholar] [CrossRef]
- Gilman, S.E.; Abraham, H.D. A longitudinal study of the order of onset of alcohol dependence and major depression. Drug Alcohol Depend. 2001, 63, 277–286. [Google Scholar] [CrossRef]
- L’Engle, K.L.; Mwarogo, P.; Kingola, N.; Sinkele, W.; Weiner, D.H. A Randomized Controlled Trial of a Brief Intervention to Reduce Alcohol Use Among Female Sex Workers in Mombasa, Kenya. Jaids-J. Acquir. Immune Defic. Syndr. 2014, 67, 446–453. [Google Scholar] [CrossRef]
- Witte, S.S.; Altantsetseg, B.; Aira, T.; Riedel, M.; Chen, J.; Potocnik, K.; El-Bassel, N.; Wu, E.; Gilbert, L.; Carlson, C.; et al. Reducing sexual HIV/STI risk and harmful alcohol use among female sex workers in Mongolia: A randomized clinical trial. AIDS Behav. 2011, 15, 1785–1794. [Google Scholar] [CrossRef] [Green Version]
- Carney, T.; Petersen Williams, P.M.; Parry, C.D. Ithubalethu-Intervention to Address Drug Use and Sexual HIV Risk Patterns among Female Commercial Sex Workers in Durban, South Africa. J. Psychoact. Drugs 2016, 48, 303–309. [Google Scholar] [CrossRef]
- Nadkarni, A.; Velleman, R.; Dabholkar, H.; Shinde, S.; Bhat, B.; McCambridge, J.; Murthy, P.; Wilson, T.; Weobong, B.; Patel, V. The systematic development and pilot randomized evaluation of counselling for alcohol problems, a lay counselor-delivered psychological treatment for harmful drinking in primary care in India: The PREMIUM study. Alcohol. Clin. Exp. Res. 2015, 39, 522–531. [Google Scholar] [CrossRef] [Green Version]
- Cook, W.K.; Bond, J.; Greenfield, T.K. Are alcohol policies associated with alcohol consumption in low- and middle-income countries? Addiction 2014, 109, 1081–1090. [Google Scholar] [CrossRef] [Green Version]
- Hawkins, B.; Holden, C.; Eckhardt, J.; Lee, K. Reassessing policy paradigms: A comparison of the global tobacco and alcohol industries. Glob. Public Health 2018, 13, 1–19. [Google Scholar] [CrossRef]
- Bryden, A.; Roberts, B.; McKee, M.; Petticrew, M. A systematic review of the influence on alcohol use of community level availability and marketing of alcohol. Health Place 2012, 18, 349–357. [Google Scholar] [CrossRef]
- Sharma, A.; Sinha, K.; Vandenberg, B. Pricing as a means of controlling alcohol consumption. Br. Med. Bull. 2017, 123, 149–158. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kuteesa, M.O.; Seeley, J.; Weiss, H.A.; Cook, S.; Kamali, A.; Webb, E.L. Alcohol Misuse and Illicit Drug Use Among Occupational Groups at High Risk of HIV in Sub-Saharan Africa: A Systematic Review. AIDS Behav. 2019, 23, 3199–3225. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
{kind=link}
| N (%) (N = 1003) | Harmful Alcohol Use % (N = 304) | Harmful Cannabis Use % (N = 186) | Harmful Amphetamine Use % (N = 220) | |||
|---|---|---|---|---|---|---|
| Level 1: Adverse Childhood Experiences and distal socio-demographic characteristics | ||||||
| Age (years) | <25 | 212 (11.7%) | 34.1 | 33.5 | 26.9 | |
| 25–34 | 353 (39.4%) | 35.9 | 21.0 | 25.3 | ||
| 35+ | 438 (48.9%) | 23.8 | 9.5 | 17.1 | ||
| Adverse childhood experiences | Ever lived on the streets | no | 878 (88.0%) | 27.5 | 14.2 | 19.3 |
| yes | 125 (12.0%) | 46.5 | 36.1 | 37.5 | ||
| Experienced physical/sexual violence | no | 212 (20.7%) | 14.0 | 8.6 | 15.9 | |
| yes | 791 (79.3%) | 33.9 | 19.0 | 22.9 | ||
| Total number of ACEs reported | <4 | 281 (28.7%) | 17.7 | 9.1 | 16.9 | |
| 5–8 | 540 (54.1%) | 31.5 | 17.9 | 21.3 | ||
| 9–12 | 170 (17.2%) | 44.9 | 25.6 | 28.4 | ||
| Literacy | Illiterate | 166 (17.6%) | 25.1 | 13.6 | 17.2 | |
| Literate | 837 (82.4%) | 30.8 | 17.5 | 22.4 | ||
| Religion | Catholic | 375 (36.9%) | 35.0 | 17.7 | 23.8 | |
| Protestant | 534 (54.4%) | 25.7 | 14.2 | 17.2 | ||
| Muslim | 46 (4.6%) | 34.2 | 20.8 | 41.5 | ||
| Other/none | 46 (4.6%) | 31.0 | 37.8 | 35.1 | ||
| Socio-economic Status (SES) | Low/low-middle | 401 (39.3%) | 33.8 | 18.2 | 25.6 | |
| middle | 200 (19.9%) | 23.9 | 19.6 | 26.1 | ||
| Upper middle/upper | 400 (40.8%) | 29.0 | 14.2 | 15.2 | ||
| Level 2: Proximal socio-demographic characteristics, sex work characteristics, sexual risk behaviours, HIV and STI prevalence | ||||||
| Marital status | Ever married | No | 216 (18.8%) | 28.4 | 19.6 | 17.0 |
| Yes | 787 (81.2%) | 30.1 | 16.2 | 22.5 | ||
| No. of children 1 | None | 40 (3.4%) | 41.3 | 32.7 | 18.9 | |
| 1–2 | 644 (66.1%) | 30.1 | 16.6 | 20.9 | ||
| 3+ | 264 (30.5%) | 28.2 | 16.3 | 24.2 | ||
| Income | No additional income | 571 (56.4%) | 28.9 | 18.1 | 24.0 | |
| Income other than sex work | 432 (43.7%) | 30.9 | 15.2 | 18.1 | ||
| Hunger | Skipped a meal in the last 7 days due to financial constraints | No | 670 (66.1%) | 25.4 | 14.2 | 18.8 |
| yes | 331 (33.9%) | 38.5 | 22.0 | 26.7 | ||
| Social support | Someone to talk to about your problems | No | 278 (27.5%) | 31.8 | 18.2 | 23.3 |
| yes | 725 (72.5%) | 29.0 | 16.3 | 20.8 | ||
| Age first sex | Mean (years) | 16.3 | 16.1 | 15.6 | 15.9 | |
| Age first sex work | Mean (years) | 24.4 | 23.3 | 21.5 | 22.8 | |
| Forced sexual debut | Tricked, pressured or forced into sex | No | 695 (68.7%) | 24.2 | 15.6 | 21.6 |
| yes | 306 (31.3%) | 42.1 | 19.6 | 21.2 | ||
| Place of selling sex | Phone/internet/friends | 54 (5.4%) | 25.5 | 8.2 | 19.0 | |
| Home/middle men/markets | 15 (1.6%) | 21.5 | 3.5 | 32.1 | ||
| Brothel/escort service/massage parlour | 14 (1.5%) | 7.7 | 7.7 | 30.8 | ||
| Bar/club/lodge/social gatherings | 620 (61.5%) | 30.3 | 15.9 | 18.8 | ||
| Street/bus/taxis | 294 (30.0%) | 30.3 | 21.5 | 26.8 | ||
| Place of sex work | Lodge/hotel/rented room | 907 (91.4%) | 29.0 | 16.5 | 21.6 | |
| Other public place | 28 (2.8%) | 50.0 | 41.9 | 30.0 | ||
| Home | 60 (5.8%) | 30.1 | 10.5 | 17.3 | ||
| Client volume/week | Median | 3 | 4 | 4 | 4 | |
| Condom use last sex with intimate partner | Last sex with IP | No | 411 (65.8%) | 31.5 | 16.2 | 22.4 |
| yes | 199 (34.2%) | 25.6 | 13.4 | 15.7 | ||
| Condom use at last sex with client | No | 200 (19.8%) | 41.0 | 20.3 | 26.1 | |
| Yes | 784 (80.2%) | 27.2 | 16.3 | 20.8 | ||
| Migrant sex work | Sold sex outside Nairobi in last 6 months | No | 730 (73.0%) | 28.0 | 14.3 | 21.5 |
| yes | 264 (27.0%) | 34.2 | 24.0 | 22.0 | ||
| HIV status | Negative | 746 (72.0%) | 34.4 | 19.4 | 24.1 | |
| Positive | 257 (28.0%) | 17.9 | 10.2 | 14.7 | ||
| Chlamydia Trachomatis | Negative | 932 (94.3%) | 29.2 | 15.7 | 21.2 | |
| Positive | 67 (5.7%) | 38.0 | 34.3 | 27.0 | ||
| Neisseria Gonorrhoea | Negative | 975 (97.4%) | 29.9 | 16.7 | 21.5 | |
| Positive | 67 (2.6%) | 23.4 | 21.3 | 21.3 | ||
| Syphilis (Treponema pallidum) | Negative | 979 (97.9%) | 30.0 | 16.9 | 21.6 | |
| Positive | 20 (2.1%) | 26.3 | 15.8 | 10.5 | ||
| Bacterial vaginosis | Negative | 428 (42.1%) | 32.8 | 17.5 | 21.5 | |
| Positive | 199 (20.0%) | 30.2 | 15.9 | 19.9 | ||
| Intermediate | 371 (37.9%) | 26.4 | 16.5 | 22.2 | ||
| Trichomonas vaginalis | Negative | 969 (97.0%) | 29.7 | 16.6 | 21.6 | |
| Positive | 31 (3.0%) | 31.5 | 24.0 | 14.8 | ||
| Level 3a: Recent violence/arrest (last 6 months) | ||||||
| Any recent sexual and/or physical non-IP violence | no | 456 (45.0%) | 20.3 | 9.8 | 16.0 | |
| yes | 547 (55.0%) | 37.6 | 22.7 | 26.0 | ||
| Any recent sexual and/or physical IP violence | no | 693 (69.1%) | 24.7 | 15.5 | 19.9 | |
| yes | 310 (30.9%) | 41.1 | 19.8 | 24.9 | ||
| Recent arrest | No | 701 (69.3%) | 24.4 | 13.0 | 16.6 | |
| yes | 302 (30.7%) | 42.0 | 25.5 | 32.7 | ||
| Level 3b: Mental health problems | ||||||
| Depression | PHQ9 score ≥ 15 | No | 778 (76.8%) | 23.0 | 14.0 | 18.1 |
| yes | 222 (23.2%) | 52.5 | 26.4 | 32.9 | ||
| Anxiety | GAD-7 score ≥ 10 | No | 894 (89.9%) | 26.3 | 15.8 | 20.2 |
| yes | 109 (11.0%) | 57.6 | 25.2 | 31.3 | ||
| PTSD | HTQ17 score ≥ 2.5 | no | 856 (85.8%) | 24.8 | 15.5 | 20.2 |
| yes | 138 (14.2%) | 60.2 | 25.4 | 28.6 | ||
| Recent suicidal behaviour | suicidal ideation or attempt last 30 days | No | 902 (89.8%) | 27.3 | 15.4 | 20.2 |
| yes | 101 (10.2%) | 51.6 | 29.8 | 32.6 | ||
| Model 1 | Crude OR (95%CI) | Adjusted OR * (95%CI) | p-Value | ||
|---|---|---|---|---|---|
| Alcohol | Number of reported ACEs | ≤4 | 1.0 | 1.0 | |
| 5–8 | 2.14 (1.50–3.04) | 2.06 (1.43–2.97) | |||
| 9–12 | 3.78 (2.47–5.79) | 3.66 (2.34–5.72) | <0.001 | ||
| Experienced sexual or physical violence in childhood | 3.16 (2.09–4.77) | 3.27 (2.13–5.02) | <0.001 | ||
| Street homelessness as a child | 2.29 (1.57–3.36) | 1.95 (1.31–2.92) | 0.001 | ||
| Age | <25 | 1.0 | 1.0 | ||
| 25–34 | 1.08 (0.76–1.54) | 1.18 (0.82–1.71) | |||
| 35+ | 0.60 (0.42–0.86) | 0.67 (0.46–0.99) | 0.05 | ||
| Literacy | Literate | 1.33 (0.93–1.33) | 1.48 (1.00–2.20) | 0.05 | |
| Cannabis | Number of ACEs | ≤4 | 1.0 | 1.0 | |
| 5–8 | 2.20 (1.40–3.45) | 1.99 (1.23–3.21) | |||
| 9–12 | 3.45 (1.05–5.80) | 2.99 (1.72–5.21) | <0.001 | ||
| Experienced sexual or physical violence in childhood | 2.50 (1.54–4.05) | 2.58 (1.52–4.37) | <0.001 | ||
| Street homelessness as a child | 3.41 (2.27–5.12) | 2.61 (1.66–4.10) | <0.001 | ||
| Age | <25 | 1.0 | 1.0 | ||
| 25–34 | 0.53 (0.36–0.77) | 0.61 (0.41–0.92) | |||
| 35+ | 0.21 (0.14–0.32) | 0.27 (0.17–0.43) | <0.001 | ||
| Amphetamines | Ever lived on the streets in childhood | 2.52 (1.69–3.74) | 1.92 (1.27–2.91) | 0.002 | |
| SES group | Low/lower middle | 1.0 | 1.0 | ||
| Middle | 1.02 (0.70–1.50) | 1.15 (0.76–1.74) | |||
| Upper middle/upper | 0.52 (0.37–0.74) | 0.65 (0.43–0.98) | 0.04 | ||
| Literacy | literate | 1.39 (0.91–2.14) | 1.74 (1.14–2.65) | 0.01 | |
| Religion | Catholic | 1.0 | 1.0 | ||
| Protestant | 0.66 (0.48–0.91) | 0.73 (0.52–1.02) | |||
| Muslim | 2.27 (1.21–4.26) | 2.39 (1.17–4.87) | |||
| Other/none | 1.73 (0.90–3.32) | 1.87 (0.94–3.73) | 0.0008 | ||
| Model 2 | Crude OR (95%CI) | Adjusted OR * (95%CI) | p-Value | ||
|---|---|---|---|---|---|
| Alcohol | Hunger (skipped a meal in the last week due to low income) | 1.84 (1.40–2.43) | 1.82 (1.29–2.57) | 0.001 | |
| Forced sexual debut | 2.27 (1.72–3.01) | 2.25 (1.62–3.13) | <0.001 | ||
| Condom use last sex with client | 0.54 (0.39–0.74) | 0.61 (0.42–0.87) | 0.006 | ||
| HIV positive | 0.42 (0.30–0.59) | 0.41 (0.27–0.62) | <0.001 | ||
| Cannabis | Hunger (skipped a meal in the last week due to low income) | 1.70 (1.23–2.37) | 1.48 (0.98–2.24) | 0.07 | |
| Place of sex work | Lodge/hotel/rented room | 1.0 | 1.0 | ||
| Public place | 3.65 (1.71–7.77) | 3.26 (1.23–8.65) | |||
| home | 0.58 (0.27–1.30) | 0.62 (0.29–1.34) | 0.03 | ||
| Migrated for sex work | 1.90 (1.35–2.67) | 1.80 (1.20–2.72) | 0.005 | ||
| Amphetamines | Ever married | 1.42 (0.96–2.11) | 1.68 (1.05–2.67) | 0.03 | |
| HIV positive | 0.54 (0.37–0.79) | 0.52 (0.34–0.79) | 0.003 | ||
| Model 3b * | Crude OR (95%CI) | Adjusted OR * (95%CI) | p-Value | |
| Alcohol | Recent sexual/physical violence non-IP | 2.37 (1.78–3.15) | 1.60 (1.13–2.27) | 0.008 |
| Recent sexual/physical violence IP | 2.13 (1.61–2.82) | 1.56 (1.12–2.19) | 0.009 | |
| Recent arrest (6 months) | 2.24 (1.69–2.97) | 1.93 (1.37–2.72) | 0.001 | |
| Cannabis | Recent sexual/physical violence non-IP | 2.71 (1.91–3.86) | 2.03 (1.31–3.15) | 0.001 |
| Recent arrest (6 months) | 2.29 (1.65–3.18) | 1.60 (1.08 -2.35) | 0.02 | |
| Amphetamines | Recent arrest (6 months) | 2.44 (1.79–3.32) | 2.06 (1.43–2.97) | <0.001 |
| Model 3b ** | Crude OR (95%CI) | Adjusted OR ** (95%CI) | p-Value | |
| Alcohol | Moderate/severe depression and/or anxiety | 3.79 (2.80–5.12) | 2.36 (1.58–3.52) | <0.001 |
| PTSD | 4.54 (3.14–6.56) | 3.20 (2.00–5.12) | <0.001 | |
| CannabisAmphetamines | Depression and/or anxiety | 2.36 (1.68–3.32) | 2.08 (1.32–3.28) | 0.002 |
| Depression and/or anxiety | 2.15 (1.55–2.96) | 1.95 (1.29–2.96) | 0.002 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Beksinska, A.; Nyariki, E.; Kabuti, R.; Kungu, M.; Babu, H.; Shah, P.; The Maisha Fiti Study Champions; Nyabuto, C.; Okumu, M.; Mahero, A.; et al. Harmful Alcohol and Drug Use Is Associated with Syndemic Risk Factors among Female Sex Workers in Nairobi, Kenya. Int. J. Environ. Res. Public Health 2022, 19, 7294. https://doi.org/10.3390/ijerph19127294
Beksinska A, Nyariki E, Kabuti R, Kungu M, Babu H, Shah P, The Maisha Fiti Study Champions, Nyabuto C, Okumu M, Mahero A, et al. Harmful Alcohol and Drug Use Is Associated with Syndemic Risk Factors among Female Sex Workers in Nairobi, Kenya. International Journal of Environmental Research and Public Health. 2022; 19(12):7294. https://doi.org/10.3390/ijerph19127294
Chicago/Turabian StyleBeksinska, Alicja, Emily Nyariki, Rhoda Kabuti, Mary Kungu, Hellen Babu, Pooja Shah, The Maisha Fiti Study Champions, Chrispo Nyabuto, Monica Okumu, Anne Mahero, and et al. 2022. "Harmful Alcohol and Drug Use Is Associated with Syndemic Risk Factors among Female Sex Workers in Nairobi, Kenya" International Journal of Environmental Research and Public Health 19, no. 12: 7294. https://doi.org/10.3390/ijerph19127294
APA StyleBeksinska, A., Nyariki, E., Kabuti, R., Kungu, M., Babu, H., Shah, P., The Maisha Fiti Study Champions, Nyabuto, C., Okumu, M., Mahero, A., Ngurukiri, P., Jama, Z., Irungu, E., Adhiambo, W., Muthoga, P., Kaul, R., Seeley, J., Weiss, H. A., Kimani, J., & Beattie, T. S. (2022). Harmful Alcohol and Drug Use Is Associated with Syndemic Risk Factors among Female Sex Workers in Nairobi, Kenya. International Journal of Environmental Research and Public Health, 19(12), 7294. https://doi.org/10.3390/ijerph19127294