
Investigating Strategies of Emotion Regulation As Mediators of Occupational Stressors and Mental Health Outcomes in First Responders

 ,
,
Abstract
:1. Introduction
2. Methods
Participants and Procedures
3. Measures
3.1. First Responder Demographics
3.2. Occupational Stressors
3.3. Emotion Regulation
3.4. PTSD Symptoms
3.5. MD Symptoms
3.6. GAD Symptoms
4. Data Analyses
5. Results
5.1. Descriptive Statistics
5.2. Inferential Statistics
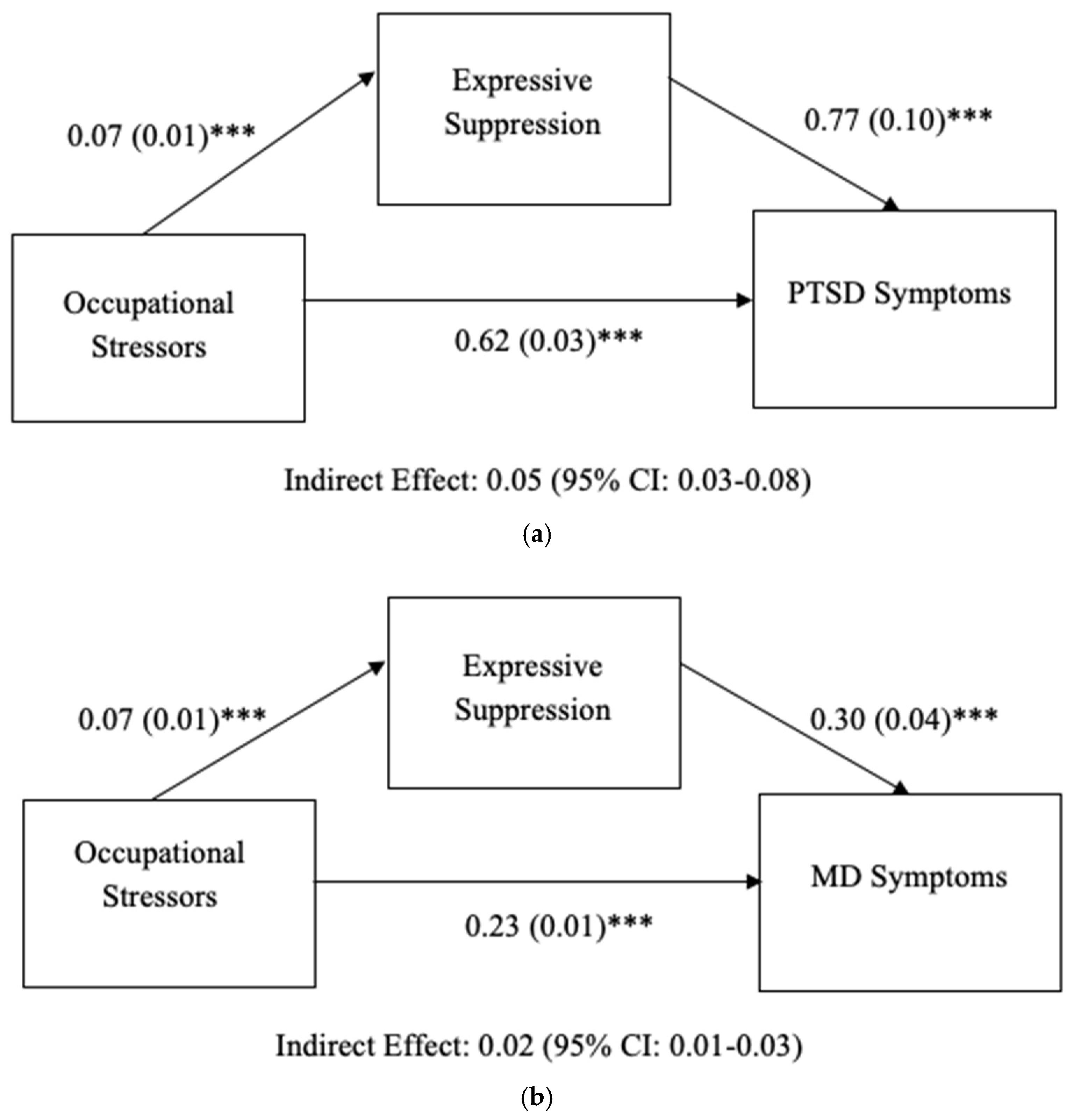
Expressive Suppression as a Mediator
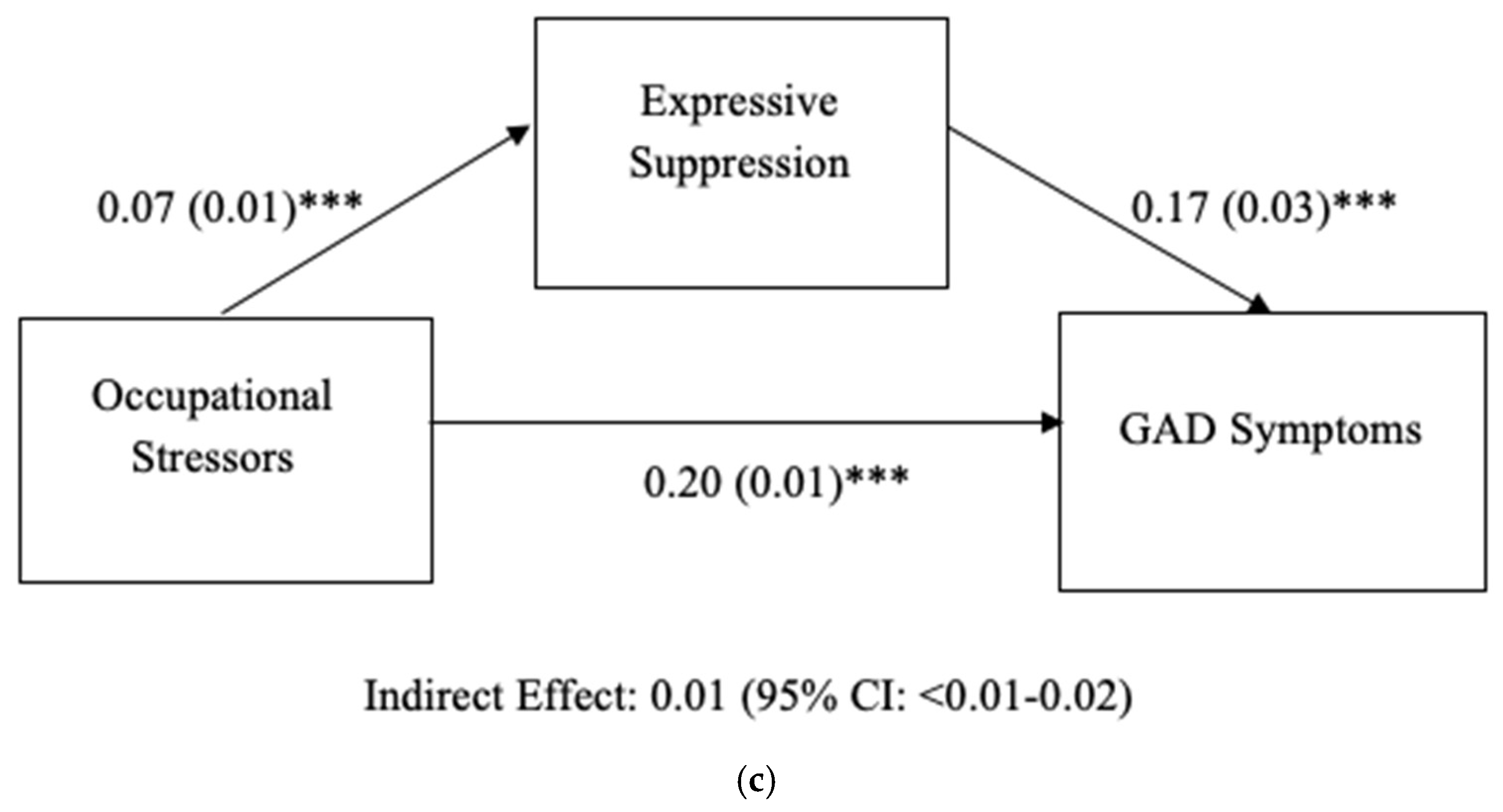
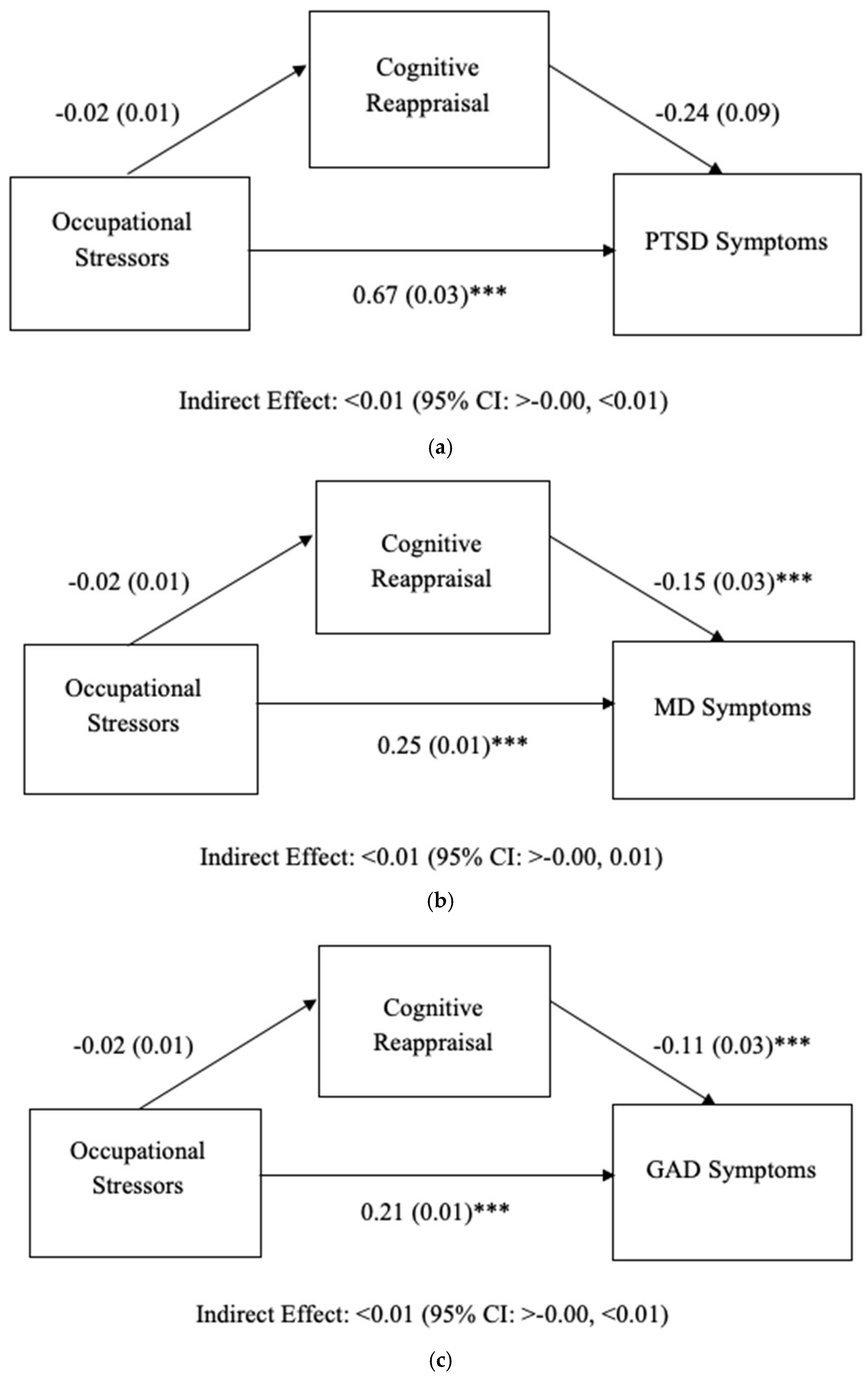
5.3. Cognitive Reappraisal as a Mediator
6. Discussion
7. Implications
8. Limitations
9. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Gärtner, A.; Behnke, A.; Conrad, D.; Kolassa, I.T.; Rojas, R. Emotion regulation in rescue workers: Differential relationship with perceived work-related stress and stress-related symptoms. Front. Psychol. 2019, 9, 2744. [Google Scholar] [CrossRef] [PubMed]
- Prati, G.; Pietrantoni, L. The relation of perceived and received social support to mental health among first responders: A meta-analytic review. J. Community Psychol. 2010, 38, 403–417. [Google Scholar] [CrossRef]
- Setti, I.; Lourel, M.; Argentero, P. The role of affective commitment and perceived social support in protecting emergency workers against burnout and vicarious traumatization. Traumatology 2016, 22, 261–270. [Google Scholar] [CrossRef] [Green Version]
- Benedek, D.M.; Fullerton, C.; Ursano, R.J. First responders: Mental health consequences of natural and human-made disasters for public health and public safety workers. Annu. Rev. Public Health 2007, 28, 55–68. [Google Scholar] [CrossRef]
- Eftekhari, A.; Zoellner, L.A.; Vigil, S.A. Patterns of emotion regulation and psychopathology. Anxiety Stress Coping 2009, 22, 571–586. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gross, J.J. Emotion and Emotion Regulation. In Handbook of Personality: Theory and Research, 2nd ed.; Pervin, L.A., John, O.P., Eds.; Guilford: New York, NY, USA, 1999; pp. 525–552. [Google Scholar]
- Gross, J.J. The emerging field of emotion regulation: An integrative review. Rev. Gen. Psychol. 1998, 2, 271–299. [Google Scholar] [CrossRef]
- Moore, S.A.; Zoellner, L.A.; Mollenholt, N. Are expressive suppression and cognitive reappraisal associated with stress-related symptoms? Behav. Res. Ther. 2008, 46, 993–1000. [Google Scholar] [CrossRef] [Green Version]
- Kimbrel, N.A.; Steffen, L.E.; Meyer, E.C.; Kruse, M.I.; Knight, J.A.; Zimering, R.T.; Gulliver, S.B. A revised measure of occupational stress for firefighters: Psychometric properties and relationship to posttraumatic stress disorder, depression, and substance abuse. Psychol. Serv. 2011, 8, 294–306. [Google Scholar] [CrossRef]
- Cutuli, D. Cognitive reappraisal and expressive suppression strategies role in the emotion regulation: An overview on their modulatory effects and neural correlates. Front. Syst. Neurosci. 2014, 8, 175. [Google Scholar] [CrossRef] [Green Version]
- Gross, J.J.; John, O.P. Individual differences in two emotion regulation processes: Implications for affect, relationships and well-being. J. Pers. Soc. Psychol. 2003, 85, 348–362. [Google Scholar] [CrossRef]
- Richards, J.M.; Gross, J.J. Emotion regulation and memory: The cognitive costs of keeping one’s cool. J. Pers. Soc. Psychol. 2000, 79, 410–424. [Google Scholar] [CrossRef] [PubMed]
- Troy, A.S.; Shallcross, A.J.; Mauss, I.B. Corrigendum: A person-by-situation approach to emotion regulation: Cognitive reappraisal can either help or hurt, depending on the context. Psychol. Sci. 2013, 24, 2505–2514. [Google Scholar] [CrossRef] [PubMed]
- Gross, J.J.; John, O.P. Mapping the domain of emotional expressivity: Multi-method evidence for a hierarchical model. J. Pers. Soc. Psychol. 1998, 74, 170–191. [Google Scholar] [CrossRef] [PubMed]
- Naragon-Gainey, K.; McMahon, T.P.; Chacko, T.P. The structure of common emotion regulation strategies: A meta-analytic examination. Psychol. Bull. 2017, 143, 384. [Google Scholar] [CrossRef]
- Sun, J.W.; Lin, P.Z.; Zhang, H.H.; Li, J.H.; Cao, F.L. A non-linear relationship between the cumulative exposure to occupational stressors and nurses’ burnout and the potentially emotion regulation factors. J. Ment. Health 2018, 27, 409–415. [Google Scholar] [CrossRef]
- Leitão, J.; Pereira, D.; Gonçalves, Â. Quality of work life and contribution to productivity: Assessing the moderator effects of burnout syndrome. Int. J. Environ. Res. Public Health 2021, 18, 2425. [Google Scholar] [CrossRef]
- Haga, S.M.; Kraft, P.; Corby, E.K. Emotion regulation: Antecedents and well-being outcomes of cognitive reappraisal and expressive suppression in cross-cultural samples. J. Happiness Stud. 2009, 10, 271–291. [Google Scholar] [CrossRef]
- Boden, M.T.; Westermann, S.; McRae, K.; Kuo, J.; Alvarez, J.; Kulkarni, M.R.; Gross, J.J.; Bonn-Miller, M.O. Emotion regulation and posttraumatic stress disorder: A prospective investigation. J. Soc. Clin. Psychol. 2013, 32, 296–314. [Google Scholar] [CrossRef]
- Salters-Pedneault, K.; Roemer, L.; Tull, M.T.; Rucker, L.; Mennin, D.S. Evidence of broad deficits in emotion regulation associated with chronic worry and generalized anxiety disorder. Cogn. Ther. Res. 2006, 30, 469–480. [Google Scholar] [CrossRef]
- Abravanel, B.T.; Sinha, R. Emotion dysregulation mediates the relationship between lifetime cumulative adversity and depressive symptomatology. J. Psychiatr. Res. 2015, 61, 89–96. [Google Scholar] [CrossRef] [Green Version]
- Cloitre, M.; Khan, C.; Mackintosh, M.A.; Garvert, D.W.; Henn-Haase, C.M.; Falvey, E.C.; Saito, J. Emotion regulation mediates the relationship between ACES and physical and mental health. Psychol. Trauma Theory Res. Pract. Policy 2019, 11, 82. [Google Scholar] [CrossRef] [PubMed]
- John, S.G.; Cisler, J.M.; Sigel, B.A. Emotion regulation mediates the relationship between a history of child abuse and current PTSD/depression severity in adolescent females. J. Fam. Violence 2017, 32, 565–575. [Google Scholar] [CrossRef]
- Raio, C.M.; Orederu, T.A.; Palazzolo, L.; Shurick, A.A.; Phelps, E.A. Cognitive emotion regulation fails the stress test. Proc. Natl. Acad. Sci. USA 2013, 110, 15139–15144. [Google Scholar] [CrossRef] [Green Version]
- Essex, B.; Scott, L.B. Chronic stress and associated coping strategies among volunteer EMS personnel. Prehospital Emerg. Care 2008, 12, 69–75. [Google Scholar] [CrossRef]
- Kleim, B.; Westphal, M. Mental health in first responders: A review and recommendation for prevention and intervention strategies. Traumatology 2011, 17, 17–24. [Google Scholar] [CrossRef]
- Williams, E.S.; Konrad, T.R.; Linzer, M.; McMurray, J.; Pathman, D.E.; Gerrity, M.; Schwartz, W.E.; Van Kirk, J.; Rhodes, E.; Douglas, J. Refining the measurement of physician job satisfaction: Results from the Physician Worklife Survey. Med. Care 1999, 11, 1140–1154. [Google Scholar] [CrossRef] [PubMed]
- Beaton, R.D.; Murphy, S.A. Sources of occupational stress among firefighter/EMTs and firefighter/paramedics and correlations with job-related outcomes. Prehospital Disaster Med. 1993, 8, 140–150. [Google Scholar] [CrossRef]
- Preece, D.A.; Becerra, R.; Robinson, K.; Gross, J.J. The emotion regulation questionnaire: Psychometric properties in general community samples. J. Personal. Assess. 2019, 102, 348–356. [Google Scholar] [CrossRef]
- Weathers, F.W.; Litz, B.T.; Keane, T.M.; Palmieri, P.A.; Marx, B.P.; Schnurr, P.P. The PTSD Checklist for DSM-5 (pcl-5). 2013. Available online: www.ptsd.va.gov (accessed on 1 October 2018).
- Blevins, C.A.; Weathers, F.W.; Davis, M.T.; Witte, T.K.; Domino, J.L. The Posttraumatic Stress Disorder Checklist for DSM-5 (PCL-5): Development and initial psychometric evaluation. J. Trauma. Stress 2015, 28, 489–498. [Google Scholar] [CrossRef]
- Bovin, M.J.; Marx, B.P.; Weathers, F.W.; Gallagher, M.W.; Rodriguez, P.; Schnurr, P.P.; Keane, T.M. Psychometric properties of the PTSD Checklist for Diagnostic and Statistical Manual of Mental Disorders-Fifth Edition (PCL-5) in Veterans. Psychol. Assess. 2015, 28, 1379–1391. [Google Scholar] [CrossRef]
- Kroenke, K.; Spitzer, R. The PHQ-9: A new depression diagnostic and severity measure. Psychiatr. Ann. 2002, 32, 509–515. [Google Scholar] [CrossRef] [Green Version]
- Ganguly, S.; Samanta, M.; Roy, P.; Chatterjee, S.; Kaplan, D.W.; Basu, B. Patient health questionnaire-9 as an effective tool for screening of depression among Indian adolescents. J. Adolesc. Health 2013, 52, 546–551. [Google Scholar] [CrossRef] [PubMed]
- Liu, S.I.; Yeh, Z.T.; Huang, H.C.; Sun, F.J.; Tjung, J.J.; Hwang, L.C.; Shih, Y.; Yeh, A.W.C. Validation of Patient Health Questionnaire for depression screening among primary care patients in Taiwan. Compr. Psychiatry 2011, 52, 96–101. [Google Scholar] [CrossRef] [PubMed]
- Spitzer, R.L.; Kroenke, K.; Williams, J.B.; Löwe, B. A brief measure for assessing generalized anxiety disorder: The GAD-7. Arch. Intern. Med. 2006, 166, 1092–1097. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jordan, P.; Shedden-Mora, M.C.; Löwe, B. Psychometric analysis of the Generalized Anxiety Disorder scale (GAD-7) in primary care using modern item response theory. PLoS ONE 2017, 12, 1–14. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hayes, A.F. Introduction to Mediation, Moderation, and Conditional Process Analysis: A Regression-Based Approach, 2nd ed.; Guilford: New York, NY, USA, 2017. [Google Scholar]
- IBM Corp. IBM SPSS Statistics for Windows; IBM Corp.: Armonk, NY, USA, 2017. [Google Scholar]
- Miklósi, M.; Martos, T.; Szabó, M.; Kocsis-Bogár, K.; Forintos, D.P. Cognitive emotion regulation and stress: A multiple mediation approach. Transl. Neurosci. 2014, 5, 64–71. [Google Scholar] [CrossRef] [Green Version]
- Alexander, J.K.; Hillier, A.; Smith, R.M.; Tivarus, M.E.; Beversdorf, D.Q. Beta-adrenergic modulation of cognitive flexibility during stress. J. Cogn. Neurosci. 2007, 19, 468–478. [Google Scholar] [CrossRef] [Green Version]
- Carter, L. First Responders Deserve Better. EMS1. Available online: https://www.ems1.com/health-and-wellness/articles/first-responders-deserve-better-3MtIEZhHIGoeTQhl/ (accessed on 10 March 2015).
- Arble, E.; Arnetz, B.B. A model of first-responder coping: An approach/avoidance bifurcation. Stress Health 2017, 33, 223–232. [Google Scholar] [CrossRef]
- Saedpanah, D.; Salehi, S.; Moghaddam, L.F. The effect of emotion regulation training on occupational stress of critical care nurses. J. Clin. Diagn. Res. JCDR 2016, 10, 1–4. [Google Scholar] [CrossRef]

{kind=link}
{kind=link}
{kind=link}
| N | % | M (SD) | |
|---|---|---|---|
| Demographics: | |||
| Age (years) | 37.32 (12.09) | ||
| Male gender | |||
| Yes | 530 | 59.2 | |
| No | 365 | 40.8 | |
| FR work-related characteristics: | |||
| Age at start of FR (years) | 21.22 (6.91) | ||
| FR work type: | |||
| Fire only | 52 | 5.8 | |
| EMS only | 534 | 59.7 | |
| Both—combined | 175 | 19.6 | |
| Both—separate agencies | 134 | 15.0 | |
| FR department type: | |||
| Volunteer | 146 | 16.3 | |
| Career | 525 | 58.7 | |
| Combined | 224 | 25.0 | |
| Response area type: | |||
| Rural | 219 | 24.5 | |
| Suburban | 337 | 37.7 | |
| Urban | 339 | 37.9 | |
| Employment status: | |||
| Full time | 611 | 68.3 | |
| Part-time | 79 | 8.8 | |
| Per diem | 62 | 6.9 | |
| Volunteer | 143 | 16.0 | |
| Time as a FR: | |||
| Less than 1 year | 11 | 1.2 | |
| 1–5 years | 179 | 20.0 | |
| 6–10 years | 187 | 20.9 | |
| 11–15 years | 163 | 18.2 | |
| 16–20 years | 112 | 12.5 | |
| 21–25 years | 78 | 8.7 | |
| More than 25 years | 165 | 18.4 | |
| FR agency type: | |||
| Federal | 10 | 1.1 | |
| State | 30 | 3.4 | |
| County | 161 | 18.0 | |
| Local | 358 | 40.0 | |
| Private | 284 | 31.7 | |
| Other | 52 | 5.8 |
| 1 | 2 | 3 | 4 | 5 | 6 | |
|---|---|---|---|---|---|---|
| 1. Occupational stressors | — | |||||
| 2. Expressive suppression | 0.22 *** | — | ||||
| 3. Cognitive reappraisal | −0.06 | 0.03 | — | |||
| 4. PTSD symptoms | 0.60 *** | 0.33 *** | −0.11 ** | — | ||
| 5. MD symptoms | 0.59 *** | 0.31 *** | −0.15 *** | 0.79 *** | — | |
| 6. GAD symptoms | 0.58 *** | 0.24 *** | −0.13 *** | 0.77 *** | 0.83 *** | — |
| M | 37.50 | 17.78 | 29.96 | 25.86 | 9.56 | 8.57 |
| SD | 15.85 | 5.12 | 5.73 | 18.59 | 7.20 | 6.34 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kshtriya, S.; Lawrence, J.; Kobezak, H.M.; Popok, P.J.; Lowe, S. Investigating Strategies of Emotion Regulation As Mediators of Occupational Stressors and Mental Health Outcomes in First Responders. Int. J. Environ. Res. Public Health 2022, 19, 7009. https://doi.org/10.3390/ijerph19127009
Kshtriya S, Lawrence J, Kobezak HM, Popok PJ, Lowe S. Investigating Strategies of Emotion Regulation As Mediators of Occupational Stressors and Mental Health Outcomes in First Responders. International Journal of Environmental Research and Public Health. 2022; 19(12):7009. https://doi.org/10.3390/ijerph19127009
Chicago/Turabian StyleKshtriya, Sowmya, Jacqueline Lawrence, Holly M. Kobezak, Paula J. Popok, and Sarah Lowe. 2022. "Investigating Strategies of Emotion Regulation As Mediators of Occupational Stressors and Mental Health Outcomes in First Responders" International Journal of Environmental Research and Public Health 19, no. 12: 7009. https://doi.org/10.3390/ijerph19127009
APA StyleKshtriya, S., Lawrence, J., Kobezak, H. M., Popok, P. J., & Lowe, S. (2022). Investigating Strategies of Emotion Regulation As Mediators of Occupational Stressors and Mental Health Outcomes in First Responders. International Journal of Environmental Research and Public Health, 19(12), 7009. https://doi.org/10.3390/ijerph19127009