
The Effectiveness of Multi-Component Interventions on the Positive and Negative Aspects of Well-Being among Informal Caregivers of People with Dementia: A Systematic Review and Meta-Analysis



{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
:1. Introduction
2. Materials and Methods
2.1. Design
2.2. Search Methods
2.3. Inclusion and Exclusion Criteria
2.4. Types of Outcome Measures
2.5. Study Selection
2.6. Quality Appraisal
2.7. Data Extraction
2.8. Synthesis
3. Results
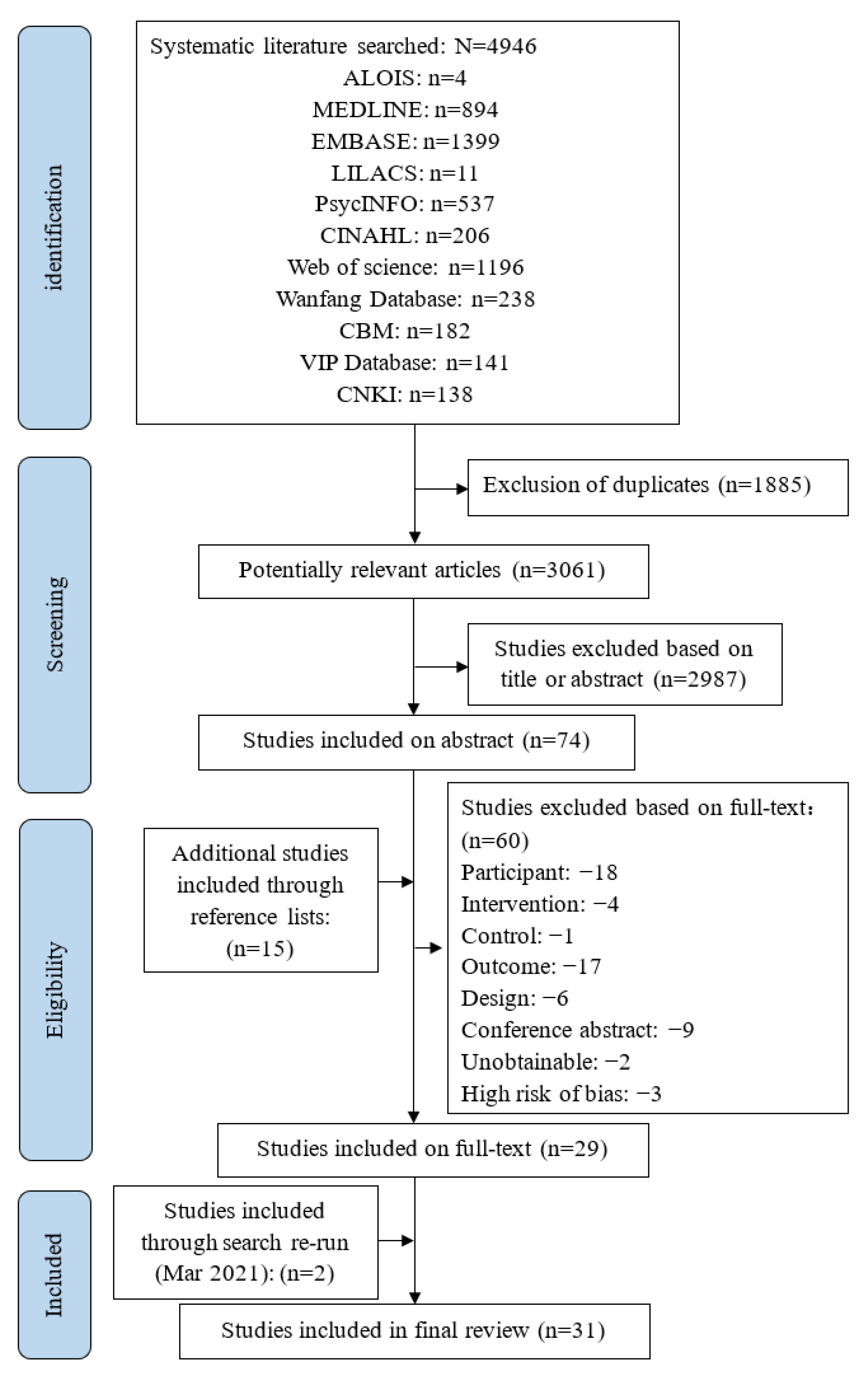
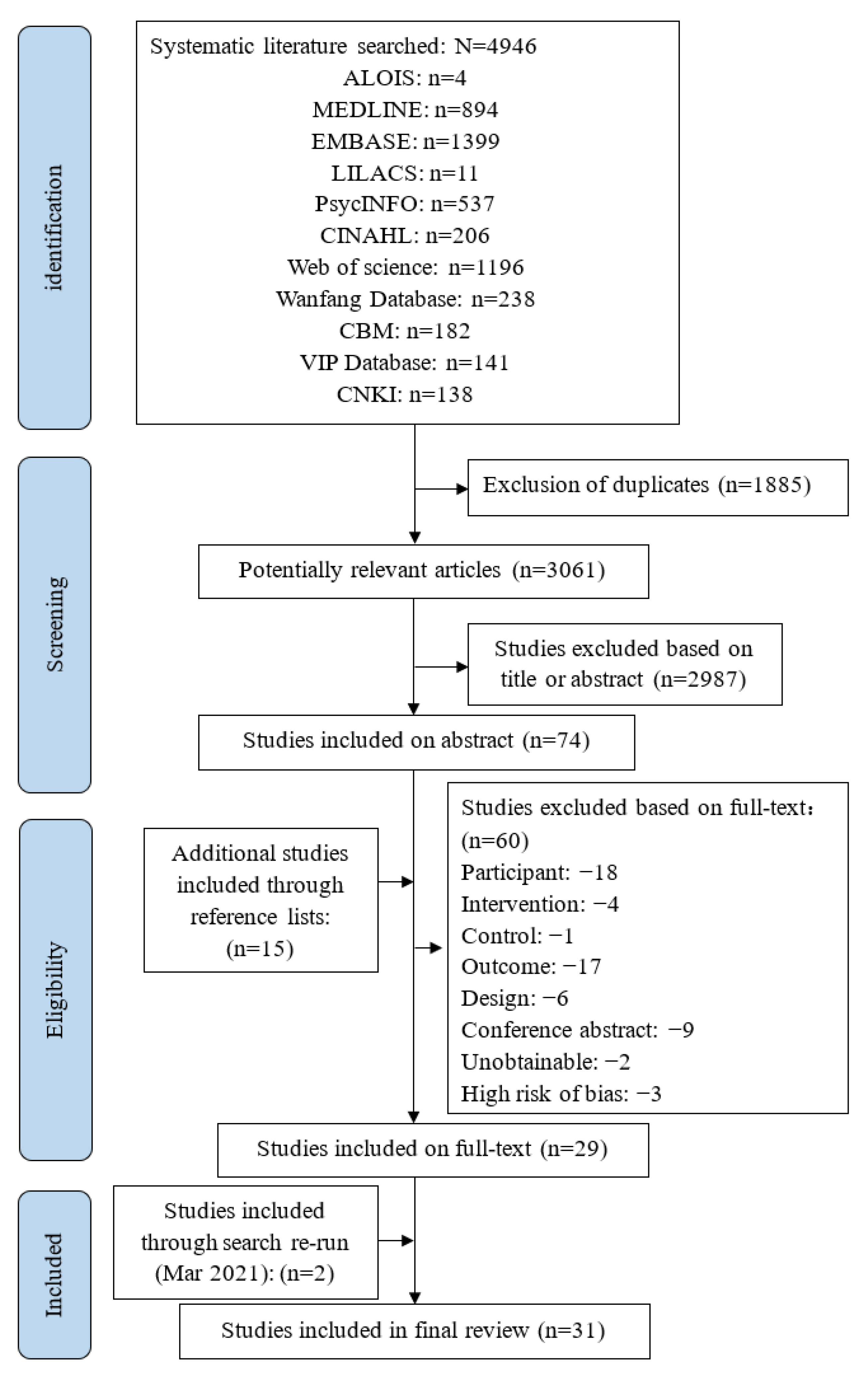
3.1. Study Selection
3.2. Study Characteristics
3.3. Risk of Bias
3.4. Impact on the Positive Aspects of Caregiver Well-Being
3.4.1. Impact on the Caregiver’s Subjective Well-Being
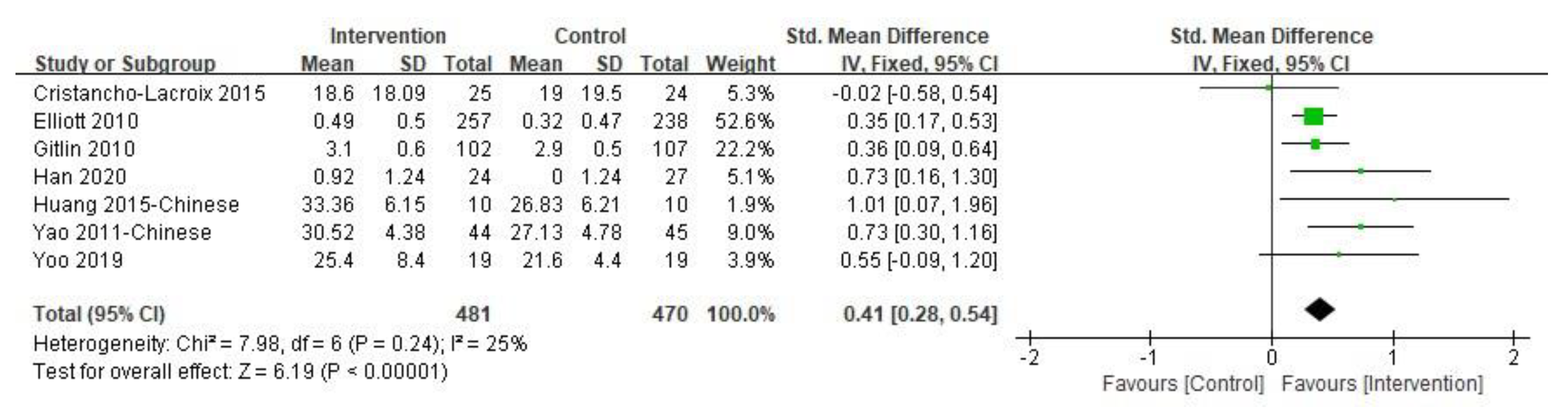
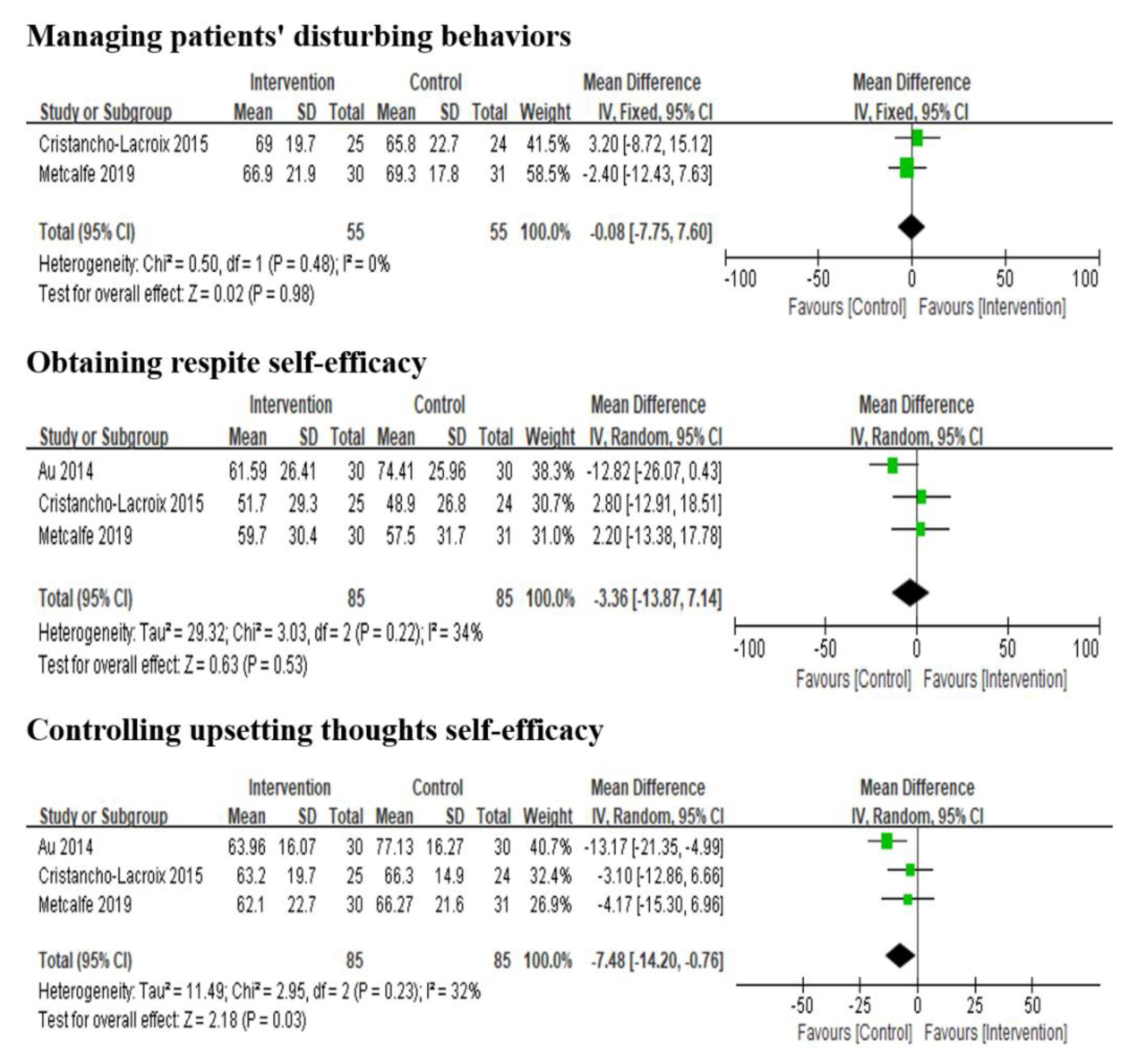
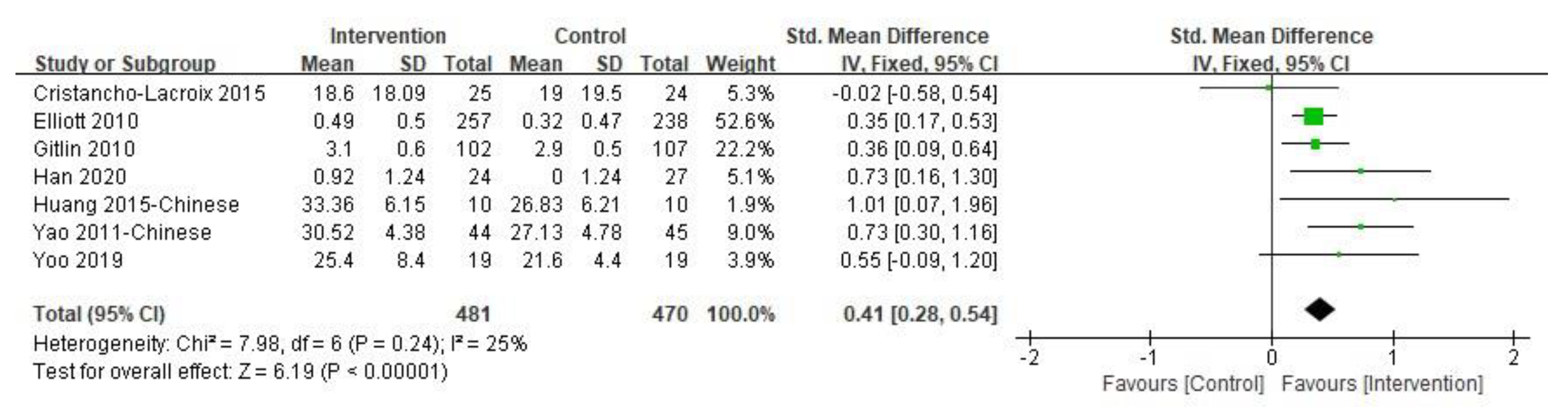
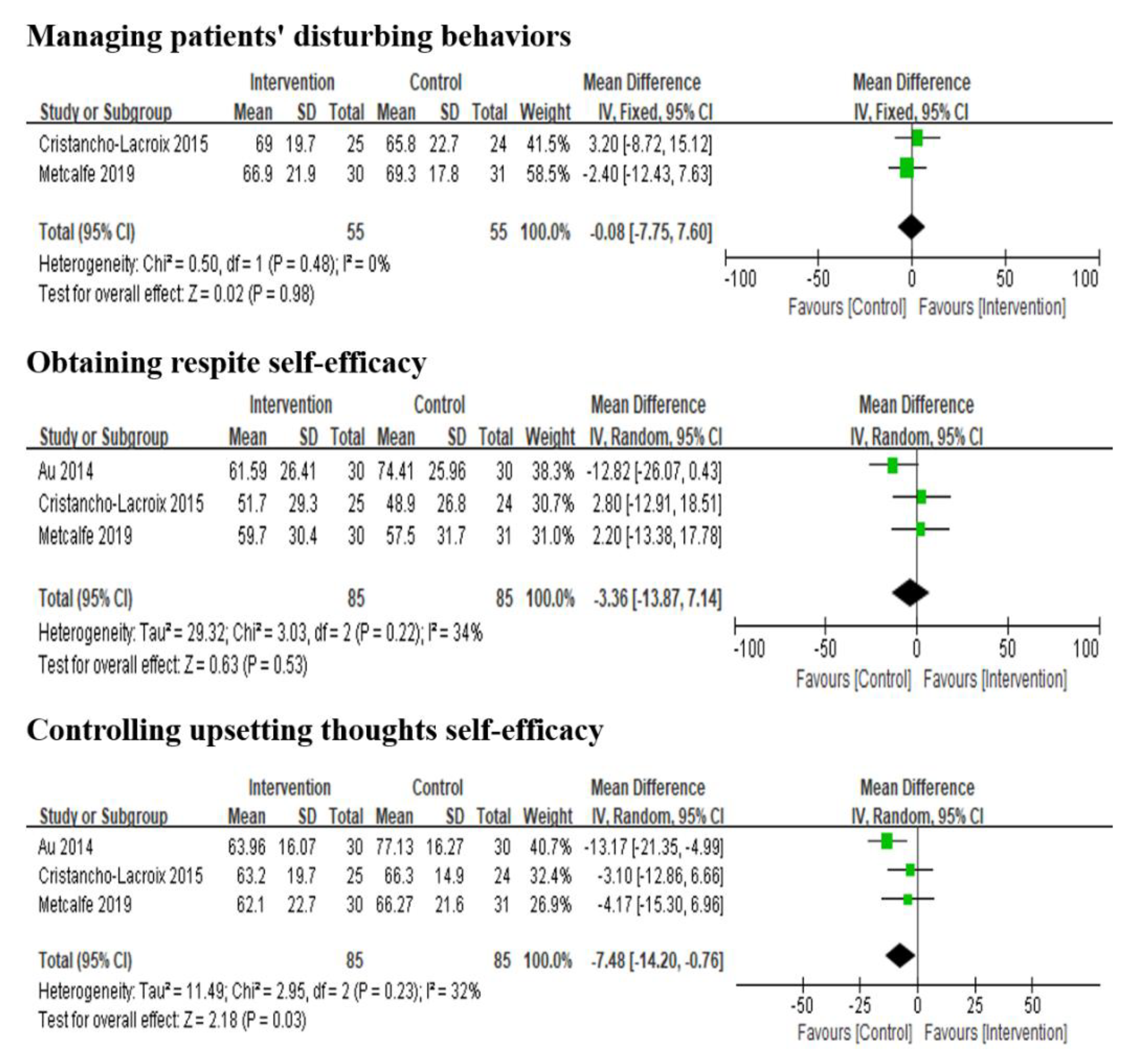
3.4.2. Impact on the Caregiver’s Self-Efficacy
3.4.3. Impact on Other Positive Outcomes
3.5. Impact on the Negative Aspects of Caregiver Well-Being
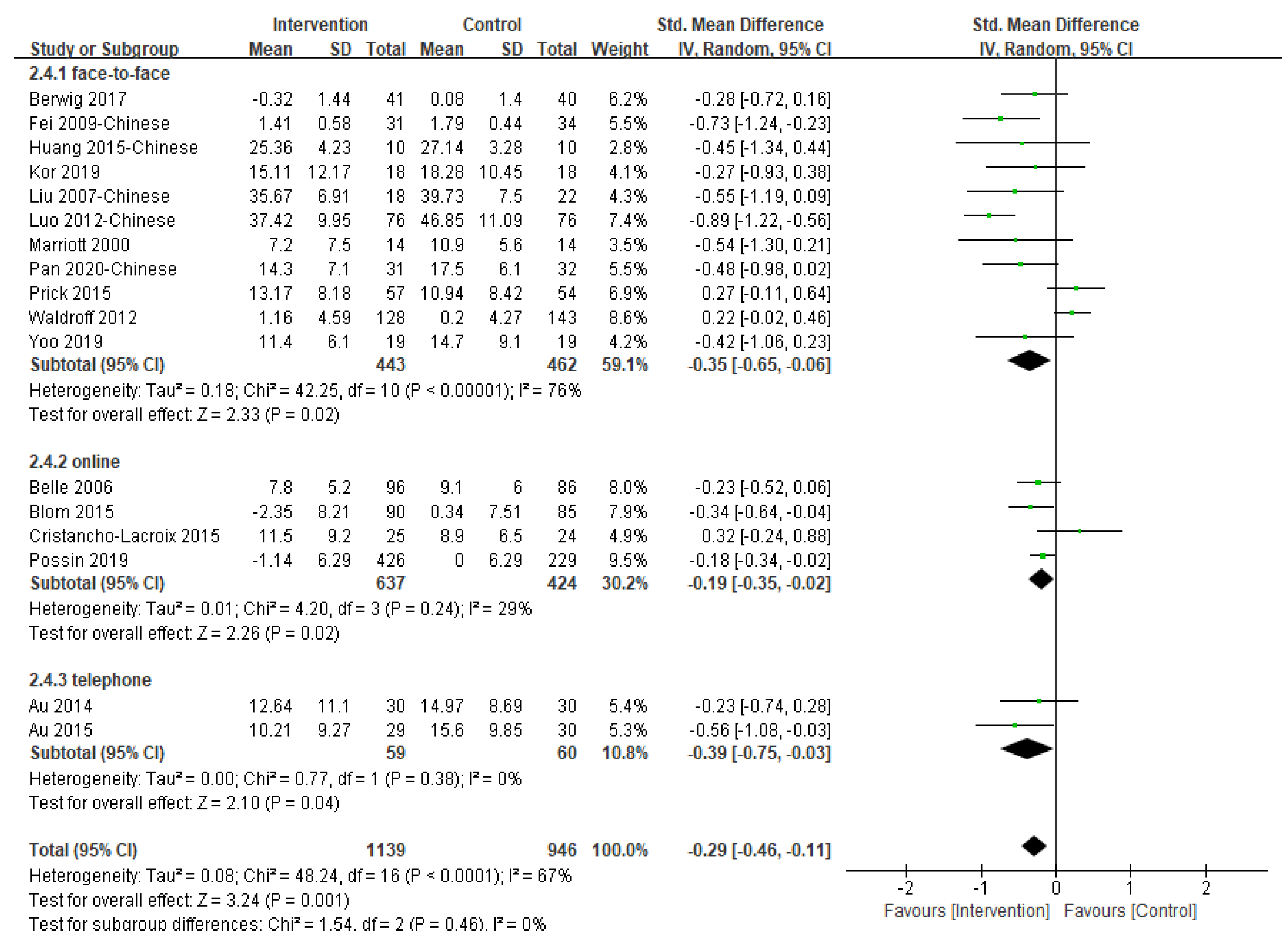
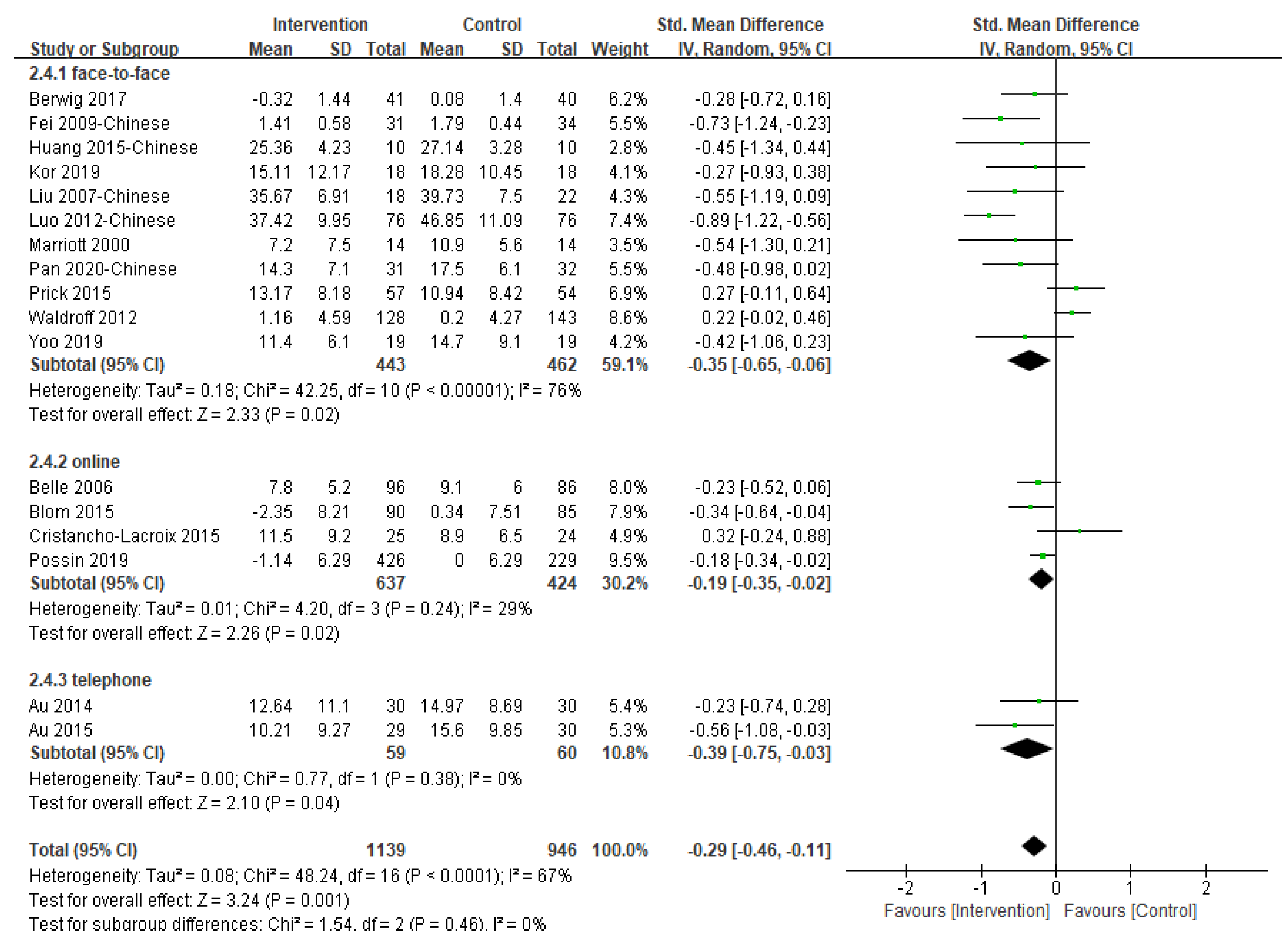
3.5.1. Impact on the Caregiver’s Depression
3.5.2. Impact on the Caregiver’s Burden
3.5.3. Impact on the Caregiver’s Anxiety
3.5.4. Impact on the Caregiver’s Stress
3.5.5. Publication Bias
4. Discussion
5. Limitations and Implications for Future Research
6. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- World Health Organization (WHO). Dementia: A Public Health Priority; World Health Organization: Geneva, Switzerland, 2012.
- Alzheimer’s Disease International. World Alzheimer Report 2018: The State of the Art of Dementia Research; Alzheimer’s Disease International: London, UK, 2018; pp. 1–46. [Google Scholar]
- Wang, H.; Xie, H.; Qu, Q.; Chen, W.; Sun, Y.; Zhang, N.; Liu, Y.; Li, T.; Chan, K.Y.; Gauthier, S.; et al. The Continuum of Care for Dementia: Needs, Resources and Practice in China. J. Glob. Health 2019, 9, 020321. [Google Scholar] [CrossRef]
- Alzheimer’s Disease International (ADI). World Alzheimer Report 2015: The Global Impact of Dementia; Alzheimer’s Disease International: London, UK, 2015. [Google Scholar]
- Collins, R.N.; Kishita, N. Prevalence of Depression and Burden among Informal Caregivers of People with Dementia: A Meta-Analysis. Ageing Soc. 2020, 40, 2355–2392. [Google Scholar] [CrossRef] [Green Version]
- Lindert, J.; Bain, P.A.; Kubzansky, L.D.; Stein, C. Well-Being Measurement and the WHO Health Policy Health 2010: Systematic Review of Measurement Scales. Eur. J. Public Health 2015, 25, 731–740. [Google Scholar] [CrossRef] [Green Version]
- Huber, M.; Knottnerus, J.A.; Green, L.; Van der Horst, H.; Jadad, A.R.; Kromhout, D.; Leonard, B.; Lorig, K.; Loureiro, M.I.; Van der Meer, J.W.; et al. How Should We Define Health? BMJ 2011, 343, d4163. [Google Scholar] [CrossRef] [Green Version]
- Cunningham, N.A.; Cunningham, T.R.; Roberston, J.M. Understanding and Measuring the Wellbeing of Carers of People with Dementia. Gerontologist 2019, 59, e552–e564. [Google Scholar] [CrossRef]
- Farhadi, A.; Foroughan, M.; Mohammadi, F.; Rassouli, M.; Moghadam, L.S.; Nazari, S.; Sadeghi, N. Caregiving Appraisal in Family Caregivers of Older Adults. Salmand-Iran. J. Ageing 2016, 11, 8–18. [Google Scholar] [CrossRef] [Green Version]
- Stansfeld, J.; Stoner, C.R.; Wenborn, J.; Vernooij-Dassen, M.; Moniz-Cook, E.; Orrell, M. Positive Psychology Outcome Measures for Family Caregivers of People Living with Dementia: A Systematic Review. Int. Psychogeriatr. 2017, 29, 1281–1296. [Google Scholar] [CrossRef] [Green Version]
- Yu, D.S.F.; Cheng, S.-T.; Wang, J. Unravelling Positive Aspects of Caregiving in Dementia: An Integrative Review of Research Literature. Int. J. Nurs. Stud. 2018, 79, 1–26. [Google Scholar] [CrossRef]
- Kajiwara, K.; Noto, H.; Yamanaka, M. Changes in Caregiving Appraisal among Family Caregivers of Persons with Dementia: A Longitudinal Study Over 12 Months. Psychogeriatrics 2018, 18, 460–467. [Google Scholar] [CrossRef]
- Yoon, H.K.; Kim, G.S. An Empowerment Program for Family Caregivers of People with Dementia. Public Health Nurs. 2020, 37, 222–233. [Google Scholar] [CrossRef]
- Elvish, R.; Lever, S.-J.; Johnstone, J.; Cawley, R.; Keady, J. Psychological Interventions for Carers of People with Dementia: A Systematic Review of Quantitative and Qualitative Evidence. Couns. Psychother. Res. 2013, 13, 106–125. [Google Scholar] [CrossRef]
- National Institute for Health and Care Excellence (UK). Dementia: Assessment, Management and Support for People Living with Dementia and Their Carers; National Institute for Health and Care Excellence: London, UK, 2018. [Google Scholar]
- Cheung, K.S.-L.; Lau, B.H.-P.; Wong, P.W.-C.; Leung, A.Y.-M.; Lou, V.W.Q.; Chan, G.M.-Y.; Schulz, R. Multicomponent Intervention on Enhancing Dementia Caregiver Well-Being and Reducing Behavioral Problems among Hong Kong Chinese: A Translational Study Based on REACH II. Int. J. Geriatr. Psychiatry 2015, 30, 460–469. [Google Scholar] [CrossRef] [PubMed]
- Dickinson, C.; Dow, J.; Gibson, G.; Hayes, L.; Robalino, S.; Robinson, L. Psychosocial Intervention for Carers of People with Dementia: What Components are Most Effective and When? A Systematic Review of Systematic Reviews. Int. Psychogeriatr. 2017, 29, 31–43. [Google Scholar] [CrossRef]
- Waldorff, F.B.; Buss, D.V.; Eckermann, A.; Rasmussen, M.L.H.; Keiding, N.; Rishøj, S.; Siersma, V.; Sørensen, J.; Sørensen, L.V.; Vogel, A.; et al. Efficacy of Psychosocial Intervention in Patients with Mild Alzheimer’s Disease: The Multicentre, Rater Blinded, Randomised Danish Alzheimer Intervention Study (DAISY). BMJ Br. Med. J. 2012, 345, e4693. [Google Scholar] [CrossRef] [Green Version]
- Possin, K.L.; Merrilees, J.J.; Dulaney, S.; Bonasera, S.J.; Chiong, W.; Lee, K.; Hooper, S.M.; Allen, I.E.; Braley, T.; Bernstein, A.; et al. Effect of Collaborative Dementia Care via Telephone and Internet on Quality of Life, Caregiver Well-being, and Health Care Use: The Care Ecosystem Randomized Clinical Trial. JAMA Intern. Med. 2019, 179, 1658–1667. [Google Scholar] [CrossRef]
- Kor, P.P.K.; Liu, J.Y.W.; Chien, W.T. Effects of a Modified Mindfulness-Based Cognitive Therapy for Family Caregivers of People with Dementia: A Pilot Randomized Controlled Trial. Int. J. Nurs. Stud. 2019, 98, 107–117. [Google Scholar] [CrossRef]
- Blom, M.M.; Zarit, S.H.; Groot Zwaaftink, R.B.; Cuijpers, P.; Pot, A.M. Effectiveness of an Internet Intervention for Family Caregivers of People with Dementia: Results of a Randomized Controlled Trial. PLoS ONE 2015, 10, e0116622. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Metcalfe, A.; Jones, B.; Mayer, J.; Gage, H.; Oyebode, J.; Boucault, S.; Aloui, S.; Schwertel, U.; Böhm, M.; Tezenas du Montcel, S.; et al. Online Information and Support for Carers of People with Young-Onset Dementia: A Multi-Site Randomised Controlled Pilot Study. Int. J. Geriatr. Psychiatry 2019, 34, 1455–1464. [Google Scholar] [CrossRef] [PubMed]
- Pan, Y.X.; Zhang, H.Y. Study of the Effect of Psychosocial Intervention on Depressive Psychology and Care Burden of Family Caregivers of Dementia Patients. Shanghai Med. Pharm. J. 2020, 41, 13–15, 49. (In Chinese) [Google Scholar]
- Berwig, M.; Heinrich, S.; Spahlholz, J.; Hallensleben, N.; Brahler, E.; Gertz, H.-J. Individualized Support for Informal Caregivers of People with Dementia-Effectiveness of the German Adaptation of REACH II. BMC Geriatr. 2017, 17, 286. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Liew, T.M.; Lee, C.S. Reappraising the Efficacy and Acceptability of Multicomponent Interventions for Caregiver Depression in Dementia: The Utility of Network Meta-Analysis. Gerontologist 2019, 59, e380–e392. [Google Scholar] [CrossRef]
- Ying, J.; Wang, Y.; Zhang, M.; Wang, S.; Shi, Y.; Li, H.; Li, Y.; Xing, Z.; Sun, J. Effect of Multicomponent Interventions on Competence of Family Caregivers of People with Dementia: A Systematic Review. J. Clin. Nurs. 2018, 27, 1744–1758. [Google Scholar] [CrossRef] [PubMed]
- Laver, K.; Milte, R.; Dyer, S.; Crotty, M. A Systematic Review and Meta-Analysis Comparing Carer Focused and Dyadic Multicomponent Interventions for Carers of People with Dementia. J. Aging Health 2017, 29, 1308–1349. [Google Scholar] [CrossRef] [Green Version]
- Walter, E.; Pinquart, M. How Effective Are Dementia Caregiver Interventions? An Updated Comprehensive Meta-Analysis. Gerontologist 2020, 60, e609–e619. [Google Scholar] [CrossRef] [PubMed]
- Higgins, J.P.T.; Thomas, J.; Chandler, J.; Cumpston, M.; Li, T.; Page, M.J.; Welch, V.A. (Eds.) Cochrane Handbook for Systematic Reviews of Interventions Version 6.3; Cochrane: London, UK, 2022. [Google Scholar]
- Lomas, T.; Medina, J.C.; Ivtzan, I.; Rupprecht, S.; Eiroa-Orosa, F.J. A Systematic Review and Meta-Analysis of the Impact of Mindfulness-Based Interventions on the Well-Being of Healthcare Professionals. Mindfulness 2019, 10, 1193–1216. [Google Scholar] [CrossRef] [Green Version]
- Higgins, J.P.T.; Green, S. (Eds.) Cochrane Handbook for Systematic Reviews of Interventions Version 5.1.0; Cochrane: London, UK, 2011. [Google Scholar]
- Jang, Y.; Clay, O.J.; Roth, D.L.; Haley, W.E.; Mittelman, M.S. Neuroticism and Longitudinal Change in Caregiver Depression: Impact of a Spouse-Caregiver Intervention Program. Gerontologist 2004, 44, 311–317. [Google Scholar] [CrossRef] [Green Version]
- Shang, S.M.; Wang, Z.W.; Deng, S.H.; Liu, Q.S.; Fu, Y.; Yue, P.; Zhang, H. Effects of the Nursing Intervention on Caregivers’ Burden for Dementia Patients in Community. J. Nurs. Adm. 2011, 11, 88–90, 101. (In Chinese) [Google Scholar]
- Mittelman, M.S.; Ferris, S.H.; Shulman, E.; Steinberg, G.; Ambinder, A.; Mackell, J.A.; Cohen, J. A Comprehensive Support Program: Effect on Depression in Spouse-Caregivers of AD Patients. Gerontologist 1995, 35, 792–802. [Google Scholar] [CrossRef] [PubMed]
- Belle, S.H.; Burgio, L.; Burns, R.; Coon, D.; Czaja, S.J.; Gallagher-Thompson, D.; Gitlin, L.N.; Klinger, J.; Koepke, K.M.; Lee, C.C.; et al. Enhancing the Quality of Life of Dementia Caregivers from Different Ethnic or Racial Groups—A Randomized, Controlled Trial. Ann. Intern. Med. 2006, 145, 727–738. [Google Scholar] [CrossRef]
- Birkenhäger-Gillesse, E.G.; Achterberg, W.P.; Janus, S.I.M.; Kollen, B.J.; Zuidema, S.U. Effects of Caregiver Dementia Training in Caregiver-Patient Dyads: A Randomized Controlled Study. Int. J. Geriatr. Psychiatry 2020, 35, 1376–1384. [Google Scholar] [CrossRef]
- Elliott, A.F.; Burgio, L.D.; Decoster, J. Enhancing Caregiver Health: Findings from the Resources for Enhancing Alzheimer’s Caregiver Health II Intervention. J. Am. Geriatr. Soc. 2010, 58, 30–37. [Google Scholar] [CrossRef]
- Gitlin, L.N.; Winter, L.; Dennis, M.P.; Hodgson, N.; Hauck, W.W. A Biobehavioral Home-Based Intervention and the Well-Being of Patients with Dementia and Their Caregivers: The COPE Randomized Trial. JAMA 2010, 304, 983–991. [Google Scholar] [CrossRef]
- Laakkonen, M.-L.; Kautiainen, H.; Holtta, E.; Savikko, N.; Tilvis, R.S.; Strandberg, T.E.; Pitkala, K.H. Effects of Self-Management Groups for People with Dementia and Their Spouses-Randomized Controlled Trial. J. Am. Geriatr. Soc. 2016, 64, 752–760. [Google Scholar] [CrossRef] [PubMed]
- Marriott, A.; Donaldson, C.; Tarrier, N.; Burns, A. Effectiveness of Cognitive-Behavioural Family Intervention in Reducing the Burden of Care in Carers of Patients with Alzheimer’s Disease. Br. J. Psychiatry 2000, 176, 557–562. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Prick, A.-E.; De Lange, J.; Twisk, J.; Pot, A.M. The Effects of a Multi-Component Dyadic Intervention on the Psychological Distress of Family Caregivers Providing Care to People with Dementia: A Randomized Controlled Trial. Int. Psychogeriatr. 2015, 27, 2031–2044. [Google Scholar] [CrossRef] [Green Version]
- Cristancho-Lacroix, V.; Wrobel, J.; Cantegreil-Kallen, I.; Dub, T.; Rouquette, A.; Rigaud, A.-S. A Web-Based Psychoeducational Program for Informal Caregivers of Patients with Alzheimer’s Disease: A Pilot Randomized Controlled Trial. J. Med. Internet Res. 2015, 17, e117. [Google Scholar] [CrossRef] [PubMed]
- Duggleby, W.; Ploeg, J.; McAiney, C.; Peacock, S.; Fisher, K.; Ghosh, S.; Markle-Reid, M.; Swindle, J.; Williams, A.; Triscott, J.A.; et al. Web-Based Intervention for Family Carers of Persons with Dementia and Multiple Chronic Conditions (My Tools 4 Care): Pragmatic Randomized Controlled Trial. J. Med. Internet Res. 2018, 20, e10484. [Google Scholar] [CrossRef]
- Au, A.; Wong, M.K.; Leung, L.M.; Leung, P.; Wong, A. Telephone-Assisted Pleasant-Event Scheduling to Enhance Well-Being of Caregivers of People with Dementia: A Randomised Controlled Trial. Hong Kong Med. J. 2014, 20, 30–33. [Google Scholar]
- Hattink, B.; Meiland, F.; Van der Roest, H.; Kevern, P.; Abiuso, F.; Bengtsson, J.; Giuliano, A.; Duca, A.; Sanders, J.; Basnett, F.; et al. Web-Based STAR E-Learning Course Increases Empathy and Understanding in Dementia Caregivers: Results from a Randomized Controlled Trial in the Netherlands and the United Kingdom. J. Med. Internet Res. 2015, 17, 15. [Google Scholar] [CrossRef] [PubMed]
- Shata, Z.N.; Amin, M.R.; El-Kady, H.M.; Abu-Nazel, M.W. Efficacy of a Multi-Component Psychosocial Intervention Program for Caregivers of Persons Living with Neurocognitive Disorders, Alexandria, Egypt: A randomized Controlled Trial. Avicenna J. Med. 2017, 7, 54–63. [Google Scholar] [CrossRef]
- Hepburn, K.W.; Tornatore, J.; Center, B.; Ostwald, S.W. Dementia Family Caregiver Training: Affecting Beliefs about Caregiving and Caregiver Outcomes. J. Am. Geriatr. Soc. 2001, 49, 450–457. [Google Scholar] [CrossRef]
- Chiao, C.Y.; Wu, H.S.; Hsiao, C.Y. Caregiver Burden for Informal Caregivers of Patients with Dementia: A Systematic Review. Int. Nurs. Rev. 2015, 62, 340–350. [Google Scholar] [CrossRef]
- World Health Organization. Global Action Plan on the Public Health Response to Dementia 2017–2025. Available online: https://www.who.int/mental_health/neurology/dementia/action_plan_2017_2025/en/ (accessed on 31 March 2017).
- Moreno-Camara, S.; Palomino-Moral, P.A.; Moral-Fernandez, L.; Frias-Osuna, A.; Parra-Anguita, L.; Del-Pino-Casado, R. Perceived Needs of the Family Caregivers of People with Dementia in a Mediterranean Setting: A Qualitative Study. Int. J. Environ. Res. Public Health 2019, 16, 993. [Google Scholar] [CrossRef] [Green Version]
- Abrahams, R.; Liu, K.P.Y.; Bissett, M.; Fahey, P.; Cheung, K.S.L.; Bye, R.; Chaudhary, K.; Chu, L.W. Effectiveness of Interventions for Co-residing Family Caregivers of People with Dementia: Systematic Review and Meta-analysis. Aust. Occup. Ther. J. 2018, 65, 208–224. [Google Scholar] [CrossRef] [PubMed]
- Wasilewski, M.B.; Stinson, J.N.; Cameron, J.I. Web-based Health Interventions for Family Caregivers of Elderly Individuals: A Scoping Review. Int. J. Med. Inform. 2017, 103, 109–138. [Google Scholar] [CrossRef] [PubMed]
- Pink, J.; O’Brien, J.; Robinson, L.; Longson, D. Dementia: Assessment, Management and Support: Summary of Updated NICE Guidance. BMJ 2018, 361, k2438. [Google Scholar] [CrossRef] [PubMed]
- Kishita, N.; Hammond, L.; Dietrich, C.M.; Mioshi, E. Which Interventions Work for Dementia Family Carers?: An Updated Systematic Review of Randomized Controlled Trials of Carer Interventions. Int. Psychogeriatr. 2018, 30, 1679–1696. [Google Scholar] [CrossRef]
- Levinson, A.J.; Ayers, S.; Butler, L.; Papaioannou, A.; Marr, S.; Sztramko, R. Barriers and Facilitators to Implementing Web-Based Dementia Caregiver Education from the Clinician’s Perspective: Qualitative Study. JMIR Aging 2020, 3, e21264. [Google Scholar] [CrossRef] [PubMed]
- Deeken, F.; Rezo, A.; Hinz, M.; Discher, R.; Rapp, M.A. Evaluation of Technology-Based Interventions for Informal Caregivers of Patients with Dementia-A Meta-Analysis of Randomized Controlled Trials. Am. J. Geriatr. Psychiatry 2019, 27, 426–445. [Google Scholar] [CrossRef] [PubMed]
- Bayly, M.; Morgan, D.; Elliot, V.; Kosteniuk, J.; Froehlich Chow, A.; Peacock, S.; O’Connell, M.E. Does Early-Stage Intervention Improve Caregiver Well-Being or Their Ability to Provide Care to Persons with Mild Dementia or Mild Cognitive impairment? A systematic review and meta-analysis. Psychol. Aging 2021, 36, 834–854. [Google Scholar] [CrossRef]
- Tang, W.K.; Chan, C.Y.J. Effects of Psychosocial Interventions on Self-Efficacy of Dementia Caregivers: A Literature Review. Int. J. Geriatr. Psychiatry 2016, 31, 475–493. [Google Scholar] [CrossRef]
- Cheung, D.S.K.; Tang, S.K.; Ho, K.H.M.; Jones, C.; Tse, M.M.Y.; Kwan, R.Y.C.; Chan, K.Y.; Chiang, V.C.L. Strategies to Engage People with Dementia and Their Informal Caregivers in Dyadic Intervention: A Scoping Review. Geriatr. Nurs. 2021, 42, 412–420. [Google Scholar] [CrossRef] [PubMed]
- Evripidou, M.; Charalambous, A.; Middleton, N.; Papastavrou, E. Nurses’ Knowledge and Attitudes about Dementia Care: Systematic Literature Review. Perspect. Psychiatr. Care 2019, 55, 48–60. [Google Scholar] [CrossRef] [Green Version]
- Dening, K.; Hibberd, P. Exploring the Community Nurse Role in Family-Centred Care for Patients with Dementia. Br. J. Community Nurs. 2016, 21, 198–202. [Google Scholar] [CrossRef]
- Wang, Y.; Xiao, L.D.; Ullah, S.; He, G.-P.; De Bellis, A. Evaluation of a Nurse-Led Dementia Education and Knowledge Translation Programme in Primary Care: A Cluster Randomized Controlled Trial. Nurse Educ. Today 2017, 49, 1–7. [Google Scholar] [CrossRef] [PubMed]
- Van’t Leven, N.; Van der Ploeg, E.; De Lange, J.; Pot, A.M. Indicators to Estimate the Appropriateness of Activating Interventions for People Living with Dementia and for Their Informal Caregivers. Aging Ment. Health 2018, 22, 1416–1423. [Google Scholar] [CrossRef]
- Sun, Y.; Ji, M.; Leng, M.; Li, X.; Zhang, X.; Wang, Z. Comparative Efficacy of 11 Non-Pharmacological Interventions on Depression, Anxiety, Quality of Life, and Caregiver Burden for Informal Caregivers of People with Dementia: A Systematic Review and Network Meta-Analysis. Int. J. Nurs. Stud. 2022, 129, 104204. [Google Scholar] [CrossRef]
- Etxeberria, I.; Salaberria, K.; Gorostiaga, A. Online Support for Family Caregivers of People with Dementia: A Systematic Review and Meta-Analysis of RCTs and Quasi-Experimental Studies. Aging Ment. Health 2021, 25, 1165–1180. [Google Scholar] [CrossRef] [PubMed]
- Cheng, S.-T.; Zhang, F. A Comprehensive Meta-Review of Systematic Reviews and Meta-Analyses on Nonpharmacological Interventions for Informal Dementia Caregivers. BMC Geriatr. 2020, 20, 137. [Google Scholar] [CrossRef] [Green Version]
- Lee, M.; Ryoo, J.H.; Crowder, J.; Byon, H.D.; Wiiliams, I.C. A Systematic Review and Meta-Analysis on Effective Interventions for Health-Related Quality of Life among Caregivers of People with Dementia. J. Adv. Nurs. 2020, 76, 475–489. [Google Scholar] [CrossRef]
- Lapid, M.I.; Atherton, P.J.; Kung, S.; Sloan, J.A.; Shahi, V.; Clark, M.M.; Rummans, T.A. Cancer Caregiver Quality of Life: Need for Targeted Intervention. Psychooncology 2016, 25, 1400–1407. [Google Scholar] [CrossRef] [PubMed]
- Phillipson, L.; Johnson, K.; Fielding, E.; Cridland, E.; Hall, D.; Neville, C.; Hasan, H. Rethinking Respite in Australia: A Naturalistic Effect Study of a Multicomponent Community Program to Promote Respite Knowledge, Attitudes and Behaviours of Carers of People with Dementia. Health Soc. Care Community 2021, 29, 1566–1583. [Google Scholar] [CrossRef]
- Au, A.; Gallagher-Thompson, D.; Wong, M.K.; Leung, J.; Chan, W.C.; Chan, C.C.; Lu, H.J.; Lai, M.K.; Chan, K. Behavioral activation for dementia caregivers: Scheduling pleasant events and enhancing communications. Clin. Interv. Aging 2015, 10, 611–619. [Google Scholar] [CrossRef] [Green Version]
- Chien, W.T.; Lee, I.Y.M. Randomized controlled trial of a dementia care programme for families of home-resided older people with dementia. J. Adv. Nurs. 2011, 67, 774–787. [Google Scholar] [CrossRef]
- Fei, J.X.; Zhao, X.P.; Shen, L.Z. Investigation on nursing intervention improving coping style and emotional disorder of relatives of the senile dementia in hospital. Chin. J. Mod. Nurs. 2009, 15, 2249–2251. [Google Scholar] [CrossRef]
- Gonyea, J.G.; O’Connor, M.K.; Boyle, P.A. Project CARE: A randomized controlled trial of a behavioral intervention group for Alzheimer’s disease caregivers. Gerontologist 2006, 46, 827–832. [Google Scholar] [CrossRef] [Green Version]
- Han, A.; Kim, T.H.; Hong, H. A factorial randomized controlled trial to examine separate and combined effects of a simulation-based empathy enhancement program and a lecture-based education program on family caregivers of people with dementia. Aging Ment. Health 2020, 25, 1930–1940. [Google Scholar] [CrossRef]
- Huang, Y.N. Impact of comprehensive intervention on caregivers of patients with Alzheimer’s disease. Health Guide Med. Res. 2015, 7, 66–67. (In Chinese) [Google Scholar]
- Liu, Q.S.; Shang, S.M.; Wang, Z.W.; Fu, Y.; Yue, P.; Zhang, H.; Liu, Y. Effects of a one-year nursing intervention on depression and anxiety in family caregivers of homebound patients with dementia. Chin. J. Behav. Med. Sci. 2007, 16, 172–174. (In Chinese) [Google Scholar] [CrossRef]
- Luo, L.C.; Wang, J.A. Effect evaluation of nursing intervention on alleviating depression and anxiety among caregivers with Alzheimer’s disease at home. Today Nurse 2012, 10, 22–24. (In Chinese) [Google Scholar]
- Yao, A.H. Effect of cognitive-behavior intervention on caregivers of alzheimer’s disease patients. Chin. J. Mod. Nurs. 2011, 17, 373–375. (In Chinese) [Google Scholar] [CrossRef]
- Yoo, R.; Yeom, J.; Kim, G.H.; Park, H.K.; Kang, Y.; Hwang, J.; Choi, S.H.; Na, H.R.; Cho, S.J.; Yu, K.H.; et al. A multicenter, randomized clinical trial to assess the efficacy of a therapeutic intervention program for caregivers of people with dementia. J. Clin. Neurol. 2019, 15, 235–242. [Google Scholar] [CrossRef] [PubMed]
- Zhu, B.; Lin, Z.; He, X.J.; Shao, Z.M. Influence of collaborative care model on the burden of family caregivers of senile dementia patients in the community. Mod. Med. J. 2016, 44, 1780–1784. (In Chinese) [Google Scholar] [CrossRef]
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
He, J.; Wang, J.; Zhong, H.; Guan, C. The Effectiveness of Multi-Component Interventions on the Positive and Negative Aspects of Well-Being among Informal Caregivers of People with Dementia: A Systematic Review and Meta-Analysis. Int. J. Environ. Res. Public Health 2022, 19, 6973. https://doi.org/10.3390/ijerph19126973
He J, Wang J, Zhong H, Guan C. The Effectiveness of Multi-Component Interventions on the Positive and Negative Aspects of Well-Being among Informal Caregivers of People with Dementia: A Systematic Review and Meta-Analysis. International Journal of Environmental Research and Public Health. 2022; 19(12):6973. https://doi.org/10.3390/ijerph19126973
Chicago/Turabian StyleHe, Jinjie, Jing Wang, Hongmei Zhong, and Chengguo Guan. 2022. "The Effectiveness of Multi-Component Interventions on the Positive and Negative Aspects of Well-Being among Informal Caregivers of People with Dementia: A Systematic Review and Meta-Analysis" International Journal of Environmental Research and Public Health 19, no. 12: 6973. https://doi.org/10.3390/ijerph19126973
APA StyleHe, J., Wang, J., Zhong, H., & Guan, C. (2022). The Effectiveness of Multi-Component Interventions on the Positive and Negative Aspects of Well-Being among Informal Caregivers of People with Dementia: A Systematic Review and Meta-Analysis. International Journal of Environmental Research and Public Health, 19(12), 6973. https://doi.org/10.3390/ijerph19126973