
Is Team Resilience More Than the Sum of Its Parts? A Quantitative Study on Emergency Healthcare Teams during the COVID-19 Pandemic





Abstract
:1. Introduction
2. Materials and Methods
2.1. Data Collection
2.2. Operationalization and Measurements
2.2.1. Dependent Variable—Team Resilience
2.2.2. Mediator—Individual Resilience
2.2.3. Predictors
2.3. Data Analysis
3. Results
3.1. Context Study
3.2. Descriptive Statistics and Correlation
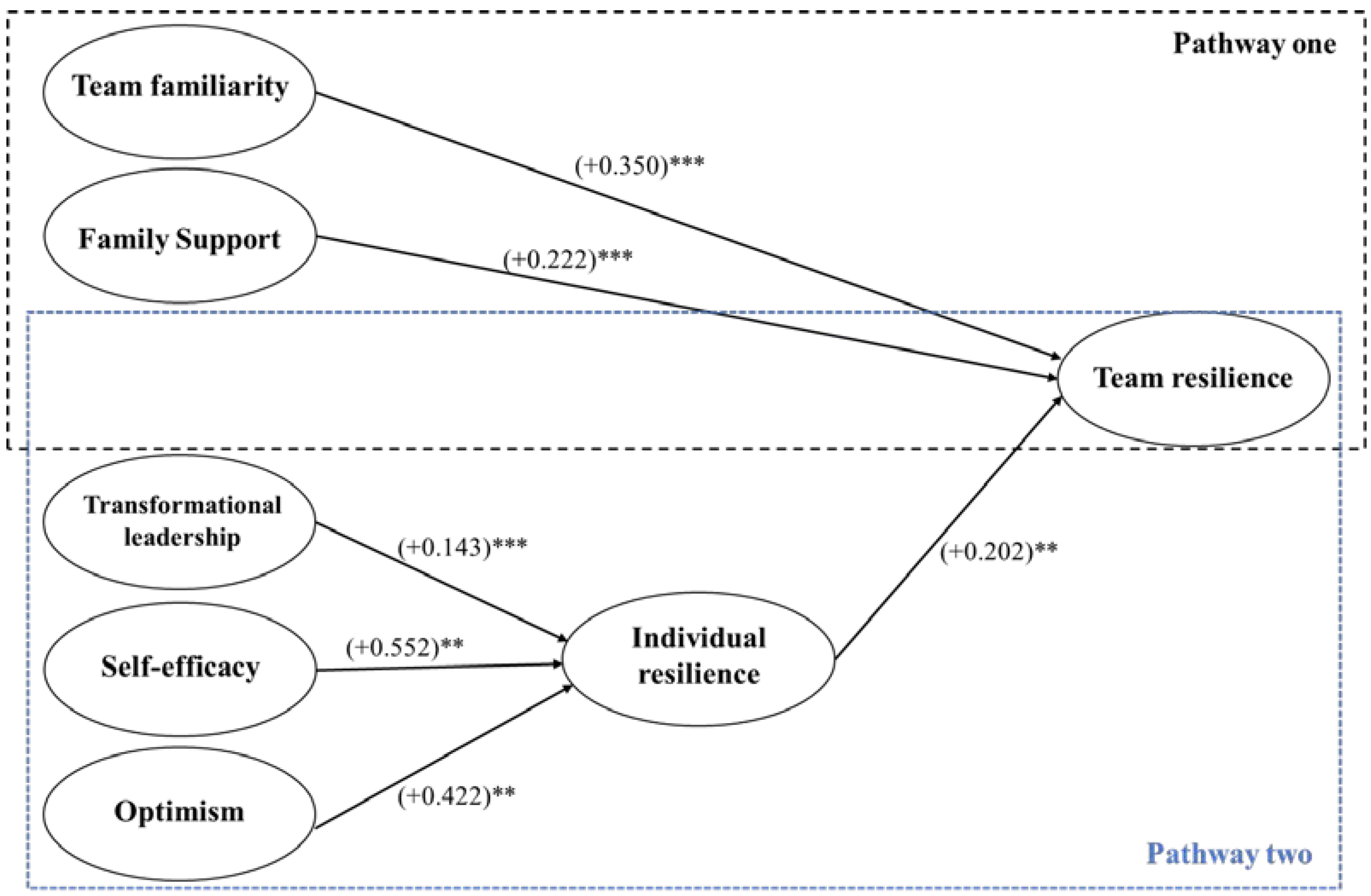
3.3. SEM Results
4. Discussion
4.1. Practical Implications
4.2. Limitations and Future Research
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Rodriguez, S.B.; Bardacci, Y.; El Aoufy, K.; Bazzini, M.; Caruso, C.; Giusti, G.D.; Mezzetti, A.; Bambi, S.; Guazzini, A.; Rasero, L. Promoting and Risk Factors of Nurses’ Hardiness Levels during the COVID-19 Pandemic: Results from an Italian Cohort. Int. J. Environ. Res. Public Health 2022, 19, 1523. [Google Scholar] [CrossRef] [PubMed]
- Hoefnagels, J.W.; Schoen, A.B.; van der Laan, S.E.; Rodijk, L.H.; van der Ent, C.K.; van de Putte, E.M.; Dalmeijer, G.W.; Nijhof, S.L. The Impact of the COVID-19 Outbreak on Mental Wellbeing in Children with a Chronic Condition Compared to Healthy Peers. Int. J. Environ. Res. Public Health 2022, 19, 2953. [Google Scholar] [CrossRef]
- Stocchetti, N.; Segre, G.; Zanier, E.R.; Zanetti, M.; Campi, R.; Scarpellini, F.; Clavenna, A.; Bonati, M. Burnout in intensive care unit workers during the second wave of the covid-19 pandemic: A single center cross-sectional Italian study. Int. J. Environ. Res. Public Health 2021, 18, 6102. [Google Scholar] [CrossRef]
- Batra, K.; Singh, T.P.; Sharma, M.; Batra, R.; Schvaneveldt, N. Investigating the psychological impact of COVID-19 among healthcare workers: A meta-analysis. Int. J. Environ. Res. Public Health 2020, 17, 9096. [Google Scholar] [CrossRef]
- Finstad, G.L.; Giorgi, G.; Lulli, L.G.; Pandolfi, C.; Foti, G.; León-Perez, J.M.; Cantero-Sánchez, F.J.; Mucci, N. Resilience, Coping Strategies and Posttraumatic Growth in the Workplace Following COVID-19: A Narrative Review on the Positive Aspects of Trauma. Int. J. Environ. Res. Public Health 2021, 18, 9453. [Google Scholar] [CrossRef]
- De Vries, A.P.J.; Alwayn, I.P.J.; Hoek, R.A.S.; van den Berg, A.P.; Ultee, F.C.W.; Vogelaar, S.M.; Haase-Kromwijk, B.J.J.M.; Heemskerk, M.B.A.; Hemke, A.C.; Nijboer, W.N.; et al. Immediate impact of COVID-19 on transplant activity in the Netherlands. Transpl. Immunol. 2020, 61, 101304. [Google Scholar] [CrossRef] [PubMed]
- Hall, H. The effect of the COVID-19 pandemic on healthcare workers’ mental health. J. Am. Acad. Pas. 2020, 33, 45–48. [Google Scholar] [CrossRef]
- Chen, Q.; Liang, M.; Li, Y.; Guo, J.; Fei, D.; Wang, L.; He, L.; Sheng, C.; Cai, Y.; Li, X.; et al. Mental health care for medical staff in China during the COVID-19 outbreak. Lancet Psychiatry 2020, 7, e15–e16. [Google Scholar] [CrossRef]
- Keenan, J.M. COVID, resilience, and the built environment. Environ. Syst. Decis. 2020, 40, 216–221. [Google Scholar] [CrossRef] [PubMed]
- Taylor, R.A. Contemporary issues: Resilience training alone is an incomplete intervention. Nurse Educ. Today 2019, 78, 10–13. [Google Scholar] [CrossRef] [PubMed]
- Vera, M.; Rodríguez-Sánchez, A.M.; Salanova, M. May the force be with you: Looking for resources that build team resilience. J. Workplace Behav. Health 2017, 32, 119–138. [Google Scholar] [CrossRef]
- Näswall, K.; Malinen, S.; Kuntz, J.; Hodliffe, M. Employee resilience: Development and validation of a measure. J. Manag. Psychol. 2019, 34, 353–367. [Google Scholar] [CrossRef]
- Hartmann, S.; Weiss, M.; Newman, A.; Hoegl, M. Resilience in the workplace: A multilevel review and synthesis. Appl. Psychol. 2020, 69, 913–959. [Google Scholar] [CrossRef]
- Kossek, E.E.; Perrigino, M.B. Resilience: A review using a grounded integrated occupational approach. Acad. Manag. Ann. 2016, 10. [Google Scholar] [CrossRef]
- Luthans, F.; Youssef, C.M.; Avolio, B.J. Psychological Capital: Developing the Human Competitive Edge; Oxford University Press: Oxford, UK, 2007; Volume 198. [Google Scholar]
- Hartwig, A.; Clarke, S.; Johnson, S.; Willis, S. Workplace team resilience: A systematic review and conceptual development. Organ. Psychol. Rev. 2020, 10, 169–200. [Google Scholar] [CrossRef]
- Alliger, G.M.; Cerasoli, C.P.; Tannenbaum, S.I.; Vessey, W.B. Team resilience: How teams flourish under pressure. Organ. Dyn. 2015, 44, 176–184. [Google Scholar] [CrossRef]
- Berg, S.H.; Aase, K. Resilient characteristics as described in empirical studies on health care. In Exploring Resilience; Springer: Cham, Switzerland, 2019; pp. 79–87. [Google Scholar]
- Chapman, M.T.; Lines, R.L.; Crane, M.; Ducker, K.J.; Ntoumanis, N.; Peeling, P.; Parker, S.K.; Quested, E.; Temby, P.; Thøgersen-Ntoumani, C.; et al. Team resilience: A scoping review of conceptual and empirical work. Work. Stress 2020, 34, 57–81. [Google Scholar] [CrossRef]
- Kozlowski, S.W.; Klein, K.J. A Multilevel Approach to Theory and Research in Organizations: Contextual, Temporal, and Emergent Processes; Jossey-Bass: Hoboken, NJ, USA, 2000. [Google Scholar]
- Bowers, C.; Kreutzer, C.; Cannon-Bowers, J.; Lamb, J. Team resilience as a second-order emergent state: A theoretical model and research directions. Front. Psychol. 2017, 8, 1360. [Google Scholar] [CrossRef]
- Gucciardi, D.F.; Crane, M.; Ntoumanis, N.; Parker, S.K.; Thøgersen-Ntoumani, C.; Ducker, K.J.; Peeling, P.; Chapman, M.T.; Quested, E.; Temby, P. The emergence of team resilience: A multilevel conceptual model of facilitating factors. J. Occup. Organ. Psychol. 2018, 91, 729–768. [Google Scholar] [CrossRef] [Green Version]
- Quemada, A. From Team Huddle to Team Cuddle: Rekindling Caring, Self-Compassion, and Joy in Work! Master’s Thesis, School of Nursing and Health Professions, San Francisco, CA, USA, 2020. [Google Scholar]
- Rangachari, P.; L Woods, J. Preserving organizational resilience, patient safety, and staff retention during COVID-19 requires a holistic consideration of the psychological safety of healthcare workers. Int. J. Environ. Res. Public Health 2020, 17, 4267. [Google Scholar] [CrossRef]
- Smith-Jentsch, K.A.; Kraiger, K.; Cannon-Bowers, J.A.; Salas, E. Do familiar teammates request and accept more backup? Transactive memory in air traffic control. Hum. Factors 2009, 51, 181–192. [Google Scholar] [CrossRef]
- Faraj, S.; Sproull, L. Coordinating expertise in software development teams. Manag. Sci. 2000, 46, 1554–1568. [Google Scholar] [CrossRef]
- Sieweke, J.; Zhao, B. The impact of team familiarity and team leader experience on team coordination errors: A panel analysis of professional basketball teams. J. Organ. Behav. 2015, 36, 382–402. [Google Scholar] [CrossRef] [Green Version]
- Bass, B.M. Two decades of research and development in transformational leadership. Eur. J. Work. Organ. Psychol. 1999, 8, 9–32. [Google Scholar] [CrossRef] [Green Version]
- Bass, B.M. From transactional to transformational leadership: Learning to share the vision. Organ. Dyn. 1990, 18, 19–31. [Google Scholar] [CrossRef] [Green Version]
- Podsakoff, P.M.; MacKenzie, S.B.; Lee, J.Y.; Podsakoff, N.P. Common method biases in behavioral research: A critical review of the literature and recommended remedies. J. Appl. Psychol. 2003, 88, 879. [Google Scholar] [CrossRef]
- Harland, L.; Harrison, W.; Jones, J.R.; Reiter-Palmon, R. Leadership behaviors and subordinate resilience. J. Leadersh. Organ. Stud. 2005, 11, 2–14. [Google Scholar] [CrossRef]
- Kozlowski, S.W.; Ilgen, D.R. Enhancing the effectiveness of work groups and teams. Psychol. Sci. Public Interest 2006, 7, 77–124. [Google Scholar] [CrossRef] [Green Version]
- Valero, J.N.; Jung, K.; Andrew, S.A. Does transformational leadership build resilient public and nonprofit organizations? Disaster Prev. Manag. 2015, 24, 4–20. [Google Scholar] [CrossRef]
- Labrague, L.J. Psychological resilience, coping behaviours and social support among health care workers during the COVID-19 pandemic: A systematic review of quantitative studies. J. Nurs. Manag. 2021, 29, 1893–1905. [Google Scholar] [CrossRef]
- Ungureanu, P.; Bertolotti, F. Backing up emergency teams in healthcare and law enforcement organizations: Strategies to socialize newcomers in the time of COVID-19. J. Risk Res. 2020, 23, 888–901. [Google Scholar] [CrossRef]
- Tannenbaum, S.I.; Traylor, A.M.; Thomas, E.J.; Salas, E. Managing teamwork in the face of pandemic: Evidence-based tips. BMJ Qual. Saf. 2021, 30, 59–63. [Google Scholar] [CrossRef]
- Heesakkers, H.; Zegers, M.; van Mol, M.M.; van den Boogaard, M. The impact of the first COVID-19 surge on the mental well-being of ICU nurses: A nationwide survey study. Intensive Crit. Care Nurs. 2021, 65, 103034. [Google Scholar] [CrossRef]
- Ojo, A.O.; Fawehinmi, O.; Yusliza, M.Y. Examining the Predictors of Resilience and Work Engagement during the COVID-19 Pandemic. Sustainability 2021, 13, 2902. [Google Scholar] [CrossRef]
- Smith, B.W.; Dalen, J.; Wiggins, K.; Tooley, E.; Christopher, P.; Bernard, J. The brief resilience scale: Assessing the ability to bounce back. Int. J. Behav. Med. 2008, 15, 194–200. [Google Scholar] [CrossRef]
- Tsang, S.; Royse, C.F.; Terkawi, A.S. Guidelines for developing, translating, and validating a questionnaire in perioperative and pain medicine. Saudi J. Anaesth. 2017, 11, S80. [Google Scholar] [CrossRef]
- Campbell-Sills, L.; Stein, M.B. Psychometric analysis and refinement of the Connor–Davidson Resilience Scale (CD-RISC): Validation of a 10-item measure of resilience. J. Trauma. Stress 2007, 20, 1019–1028. [Google Scholar] [CrossRef]
- Connor, K.M.; Davidson, J.R. Development of a new resilience scale: The Connor-Davidson resilience scale (CD-RISC). Depress. Anxiety 2003, 18, 76–82. [Google Scholar] [CrossRef]
- Carless, S.A.; Wearing, A.J.; Mann, L. A Short Measure of Transformational Leadership. J. Bus. Psychol. 2000, 14, 389–405. [Google Scholar] [CrossRef]
- Gevers, J.M.; Rispens, S.; Li, J. Pacing style diversity and team collaboration: The moderating effects of temporal familiarity and action planning. Group Dyn. Theory Res. Pract. 2016, 20, 78. [Google Scholar] [CrossRef]
- Romppel, M.; Herrmann-Lingen, C.; Wachter, R.; Edelmann, F.; Düngen, H.D.; Pieske, B.; Grande, G. A short form of the General Self-Efficacy Scale (GSE-6): Development, psychometric properties and validity in an intercultural non-clinical sample and a sample of patients at risk for heart failure. GMS Psycho Soc. Med. 2013, 10. [Google Scholar] [CrossRef]
- Schwarzer, R.; Jerusalem, M. Generalized Self-Efficacy scale. In Measures in Health Psychology: A User’s Portfolio. Causal and Control Beliefs; Weinman, J., Wright, S., Johnston, M., Eds.; NFER-NELSON: Windsor, UK, 1995; pp. 35–37. [Google Scholar]
- Kline, R.B. Principles and Practice of Structural Equation Modeling, 4th ed.; Guilford Press: New York, NY, USA, 2016; ISBN 978-1-4625-2334-4. [Google Scholar]
- Morgan, P.B.; Fletcher, D.; Sarkar, M. Understanding team resilience in the world’s best athletes: A case study of a rugby union World Cup winning team. Psychol. Sport Exerc. 2015, 16, 91–100. [Google Scholar] [CrossRef] [Green Version]
- Wegner, D.M. Transactive memory: A contemporary analysis of the group mind. In Theories of Group Behavior; Springer: New York, NY, USA, 1987; pp. 185–208. [Google Scholar]
- Kalisch, B.J.; Russell, K.; Lee, K.H. Nursing Teamwork and Unit Size. West. J. Nurs. Res. 2013, 35, 214–225. [Google Scholar] [CrossRef] [PubMed]
- Di Giuseppe, M.; Nepa, G.; Prout, T.A.; Albertini, F.; Marcelli, S.; Orrù, G.; Conversano, C. Stress, burnout, and resilience among healthcare workers during the COVID-19 emergency: The role of defense mechanisms. Int. J. Environ. Res. Public Health 2021, 18, 5258. [Google Scholar] [CrossRef] [PubMed]
- Bender, A.; Ingram, R. Connecting attachment style to resilience: Contributions of self-care and self-efficacy. Personal. Individ. Differ. 2018, 130, 18–20. [Google Scholar] [CrossRef]
- Sinclair, V.G.; Wallston, K.A. The development and psychometric evaluation of the Brief Resilient Coping Scale. Assessment 2004, 11, 94–101. [Google Scholar] [CrossRef]
- Kenneally, C. The Effects of Optimism, Transformational Leadership, and Work Engagement on Work Outcomes: A Moderated Mediation Model. Master’s Thesis, Old Dominion University, Norfolk, VA, USA, 2020. [Google Scholar] [CrossRef]
- Gilmartin, S.; Martin, L.; Kenny, S.; Callanan, I.; Salter, N. Promoting hot debriefing in an emergency department. BMJ Open Qual. 2020, 9, e000913. [Google Scholar] [CrossRef]
- Allen, J.P.; van der Velden, R. The role of self-assessment in measuring skills. Economics 2005, 1–24. Available online: https://www.academia.edu/download/43167399/The_role_of_self-assessment_in_measuring20160228-4193-1rnh6oe.pdf (accessed on 28 April 2022).


{kind=link}
| Function Group | Function |
|---|---|
| Nurses (51.9%) | Nurses (51.9%) |
| Sepcialists (23.3%) | Doctor assistants (11.6%) |
| Managers (caregiver 0.8%) | |
| Paramedics (7.8%) | |
| Medical specialists (3.1%) | |
| Non-medical (24.8%) | Administrative staff (7.0%) |
| Supporting staff (7.0%) | |
| Managers (10.9%) |
| Extra stress at the workplace | 66.9% |
| Extra work hours | 65.9% |
| Work together with different colleagues from other departments | 56.9% |
| Felt insecure about the ability to guarantee the right care for all patients | 53.1% |
| Felt insecurity around following the right procedures | 51.5% |
| Other duties and responsibilities | 50.8% |
| Other shared goals | 37.7% |
| Less time for personal health | 37.7% |
| Less times for personal development | 31.5% |
| Mean | SD | Min. | Max. | |
|---|---|---|---|---|
| 1. Team Resilience | 3.739 | 0.445 | 2.600 | 5.000 |
| 2. Individual Resilience | 3.767 | 0.630 | 1.667 | 5.000 |
| 3. Transformational Leadership | 3.595 | 0.672 | 2.000 | 5.000 |
| 4. Team Familiarity | 3.846 | 0.511 | 1.429 | 5.000 |
| 5. Self-Efficacy | 3.814 | 0.427 | 2.500 | 5.000 |
| 6. Optimism | 3.752 | 0.462 | 2.333 | 4.667 |
| 7. Family Support | 4.222 | 0.572 | 2.667 | 5.000 |
| 8. Friend Support | 4.269 | 0.628 | 2.667 | 5.000 |
| 9. Tenure | 10.678 | 9.994 | 0.000 | 40.000 |
| 10. Age | 4.000 | 1.358 | 2.000 | 6.000 |
| 11. Specialist | 0.233 | 0.424 | 0.000 | 1.000 |
| 12. Non-Medical Staff | 0.248 | 0.434 | 0.000 | 1.000 |
| 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | 9 | 10 | 11 | |
|---|---|---|---|---|---|---|---|---|---|---|---|
| 1 | - | ||||||||||
| 2 | 0.352 *** | - | |||||||||
| 3 | 0.362 *** | 0.299 *** | - | ||||||||
| 4 | 0.498 *** | 0.166 † | 0.354 *** | - | |||||||
| 5 | 0.197 * | 0.545 *** | 0.269 ** | 0.206 * | - | ||||||
| 6 | 0.247 ** | 0.476 *** | 0.184 * | 0.152 † | 0.398 *** | - | |||||
| 7 | 0.259 ** | 0.092 | 0.121 | 0.105 | 0.068 | 0.276 ** | - | ||||
| 8 | 0.092 | 0.181 * | 0.125 | 0.129 | 0.180 * | 0.271 ** | 0.531 *** | - | |||
| 9 | 0.004 | 0.056 | −0.028 | −0.039 | −0.017 | 0.023 | 0.032 | −0.009 | - | ||
| 10 | 0.130 | 0.172 † | 0.066 | −0.003 | 0.085 | 0.075 | 0.027 | −0.015 | 0.487 *** | - | |
| 11 | 0.101 | −0.132 | −0.062 | 0.089 | −0.176 * | 0.004 | −0.075 | −0.021 | 0.005 | −0.041 | - |
| 12 | 0.095 | 0.132 | 0.233 ** | −0.013 | 0.258 ** | 0.121 | −0.067 | 0.021 | −0.066 | 0.133 | −0.316 *** |
| Total Effects | Direct Effects | Direct Effects | ||||
|---|---|---|---|---|---|---|
| DV: Team Resilience | M: Individual Resilience | DV: Team Resilience | ||||
| B | SE | B | SE | B | SE | |
| Constant | 0.949 | (0.712) | −0.435 | (0.481) | 1.037 | (0.694) |
| Individual Resilience | 0.202 ** | (0.065) | ||||
| Transformational Leadership | 0.106 † | (0.055) | 0.143 *** | (0.033) | 0.077 | (0.056) |
| Team Familiarity | 0.349 *** | (0.063) | −0.005 | (0.076) | 0.350 *** | (0.050) |
| Self-Efficacy | 0.034 | (0.081) | 0.552 ** | (0.174) | −0.077 | (0.091) |
| Optimism | 0.090 | (0.074) | 0.422 ** | (0.140) | 0.005 | (0.068) |
| Family Support | 0.203 *** | (0.053) | −0.092 | (0.130) | 0.222 *** | (0.053) |
| Friend Support | −0.104 | (0.066) | 0.058 | (0.120) | −0.116 * | (0.058) |
| Tenure | 0.037 | (0.033) | 0.055 | (0.039) | 0.026 | (0.032) |
| Age | −0.002 | (0.004) | 0.000 | (0.004) | −0.002 | (0.004) |
| Specialist | 0.135 | (0.088) | −0.127 | (0.103) | 0.161 † | (0.082) |
| Non-Medical Staff | 0.089 | (0.097) | −0.127 | (0.092) | 0.115 | (0.092) |
| R2 | 0.377 | 0.419 | 0.425 | |||
| Indirect Effects | ||
| Via: Individual Resilience | ||
| DV: Team Resilience | ||
| B | SE | |
| Transformational Leadership | 0.029 ** | (0.011) |
| Team Familiarity | −0.001 | (0.016) |
| Self-Efficacy | 0.111 † | (0.059) |
| Optimism | 0.085 ** | (0.031) |
| Family Support | −0.018 | (0.028) |
| Friend Support | 0.012 | (0.026) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Hendrikx, I.E.M.; Vermeulen, S.C.G.; Wientjens, V.L.W.; Mannak, R.S. Is Team Resilience More Than the Sum of Its Parts? A Quantitative Study on Emergency Healthcare Teams during the COVID-19 Pandemic. Int. J. Environ. Res. Public Health 2022, 19, 6968. https://doi.org/10.3390/ijerph19126968
Hendrikx IEM, Vermeulen SCG, Wientjens VLW, Mannak RS. Is Team Resilience More Than the Sum of Its Parts? A Quantitative Study on Emergency Healthcare Teams during the COVID-19 Pandemic. International Journal of Environmental Research and Public Health. 2022; 19(12):6968. https://doi.org/10.3390/ijerph19126968
Chicago/Turabian StyleHendrikx, Inge E. M., Stef C. G. Vermeulen, Vera L. W. Wientjens, and Remco S. Mannak. 2022. "Is Team Resilience More Than the Sum of Its Parts? A Quantitative Study on Emergency Healthcare Teams during the COVID-19 Pandemic" International Journal of Environmental Research and Public Health 19, no. 12: 6968. https://doi.org/10.3390/ijerph19126968
APA StyleHendrikx, I. E. M., Vermeulen, S. C. G., Wientjens, V. L. W., & Mannak, R. S. (2022). Is Team Resilience More Than the Sum of Its Parts? A Quantitative Study on Emergency Healthcare Teams during the COVID-19 Pandemic. International Journal of Environmental Research and Public Health, 19(12), 6968. https://doi.org/10.3390/ijerph19126968