
I Need to Know: Using the CeHRes Roadmap to Develop a Treatment Feedback Tool for Youngsters with Mental Health Problems

 , ,
, ,
Abstract
:1. Introduction
2. Methods
2.1. Expert Panel
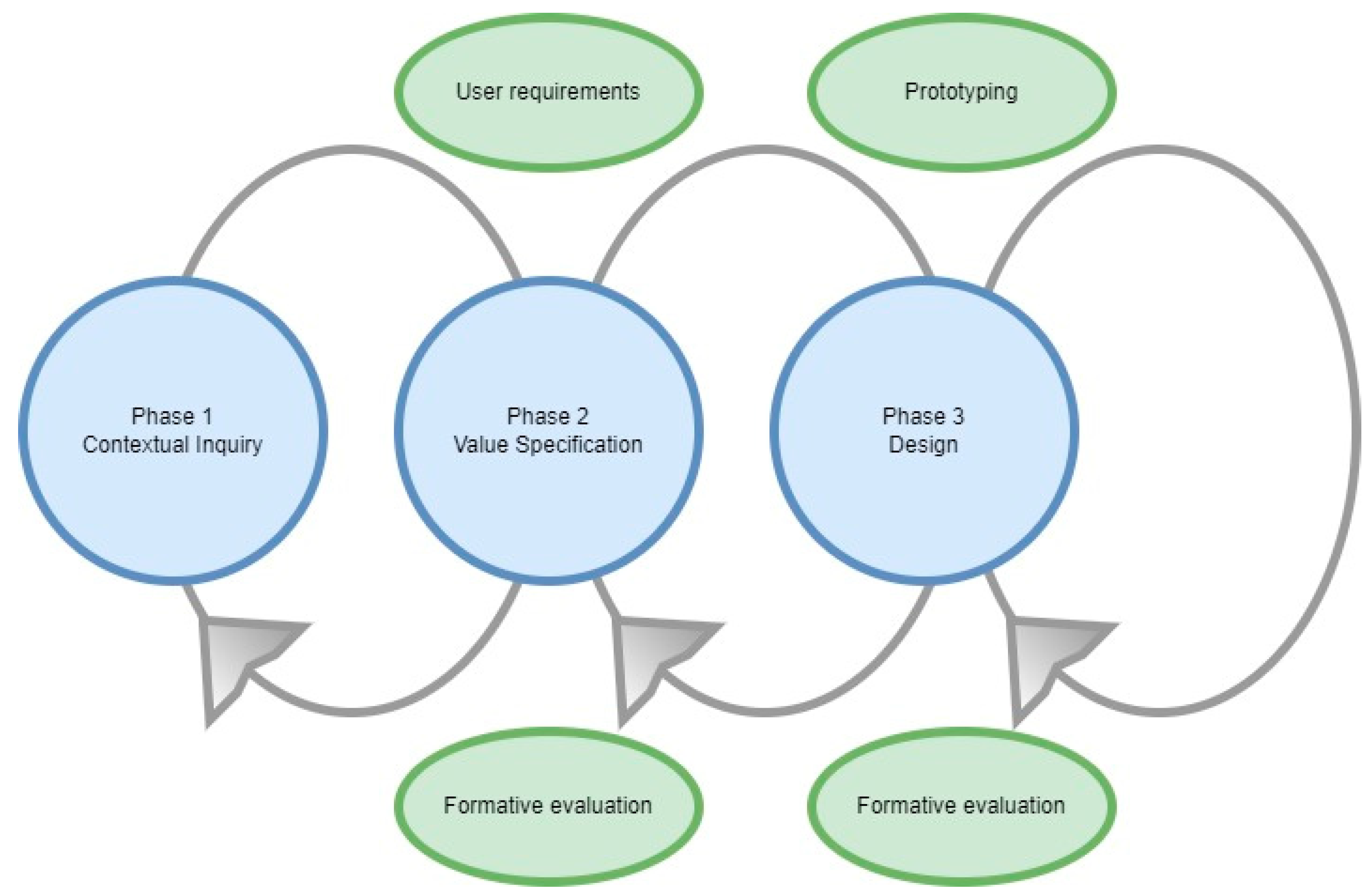
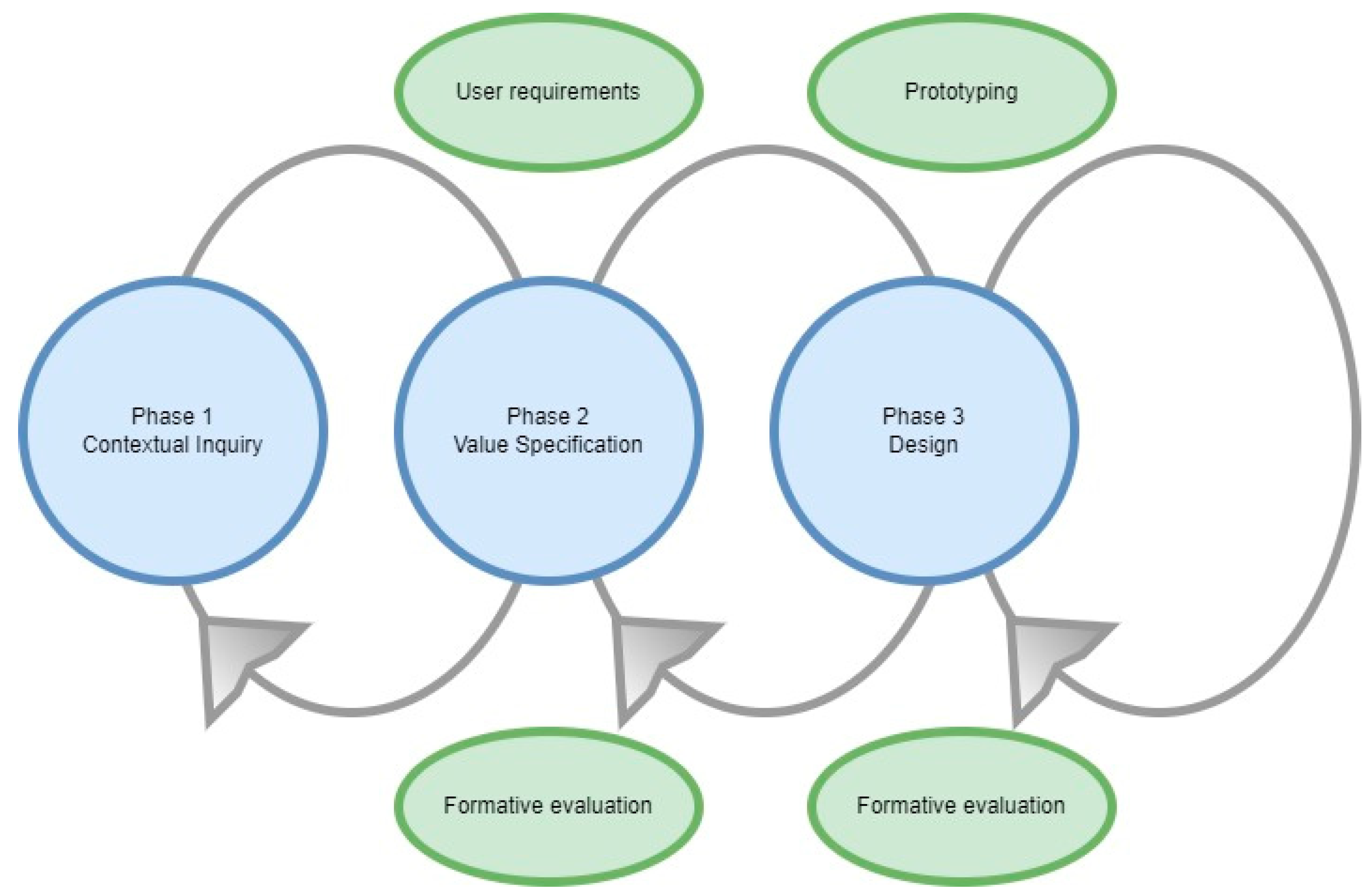
2.2. Development Process
2.2.1. Phase 1: Contextual Inquiry
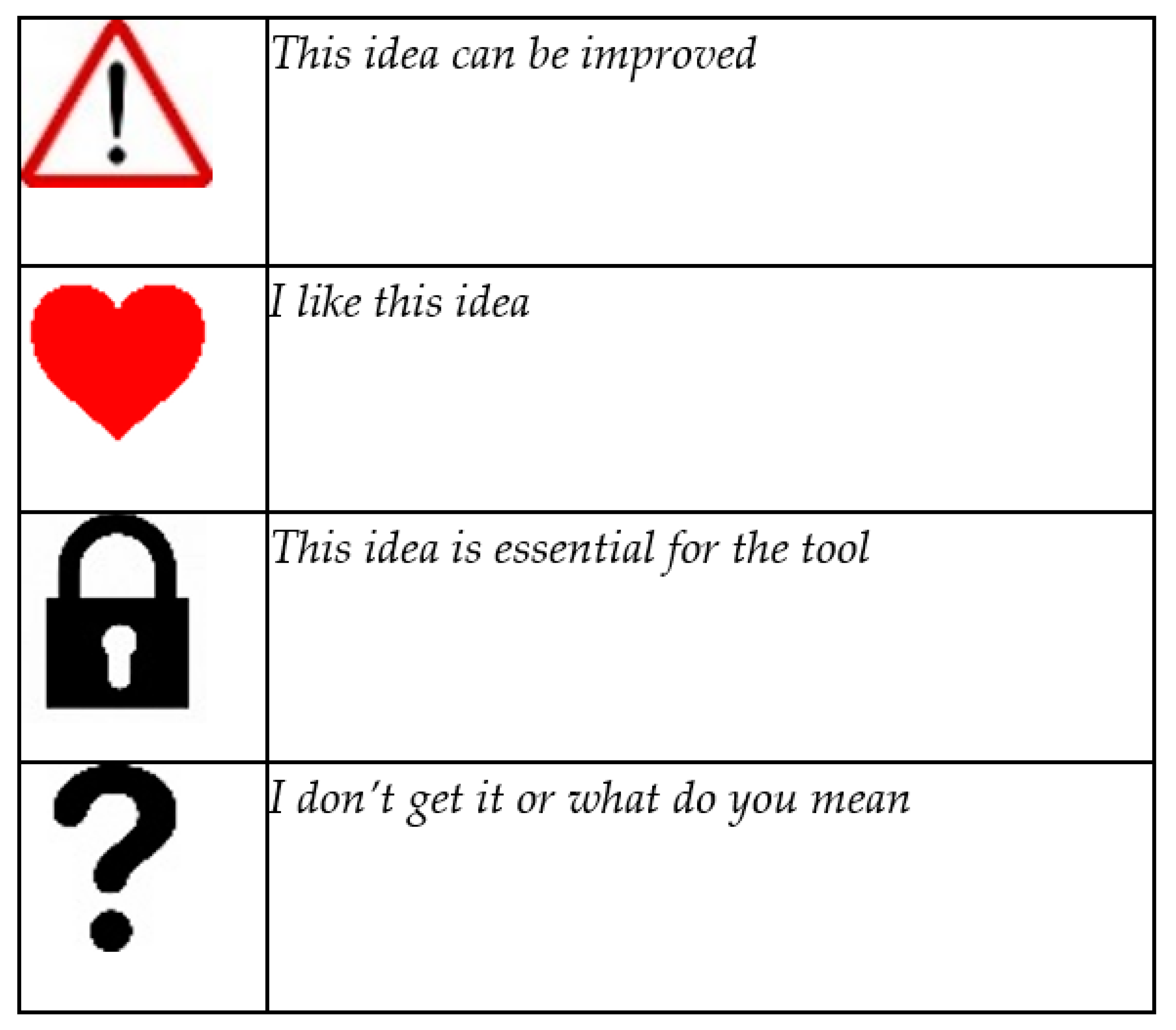
2.2.2. Phase 2: Value Specification
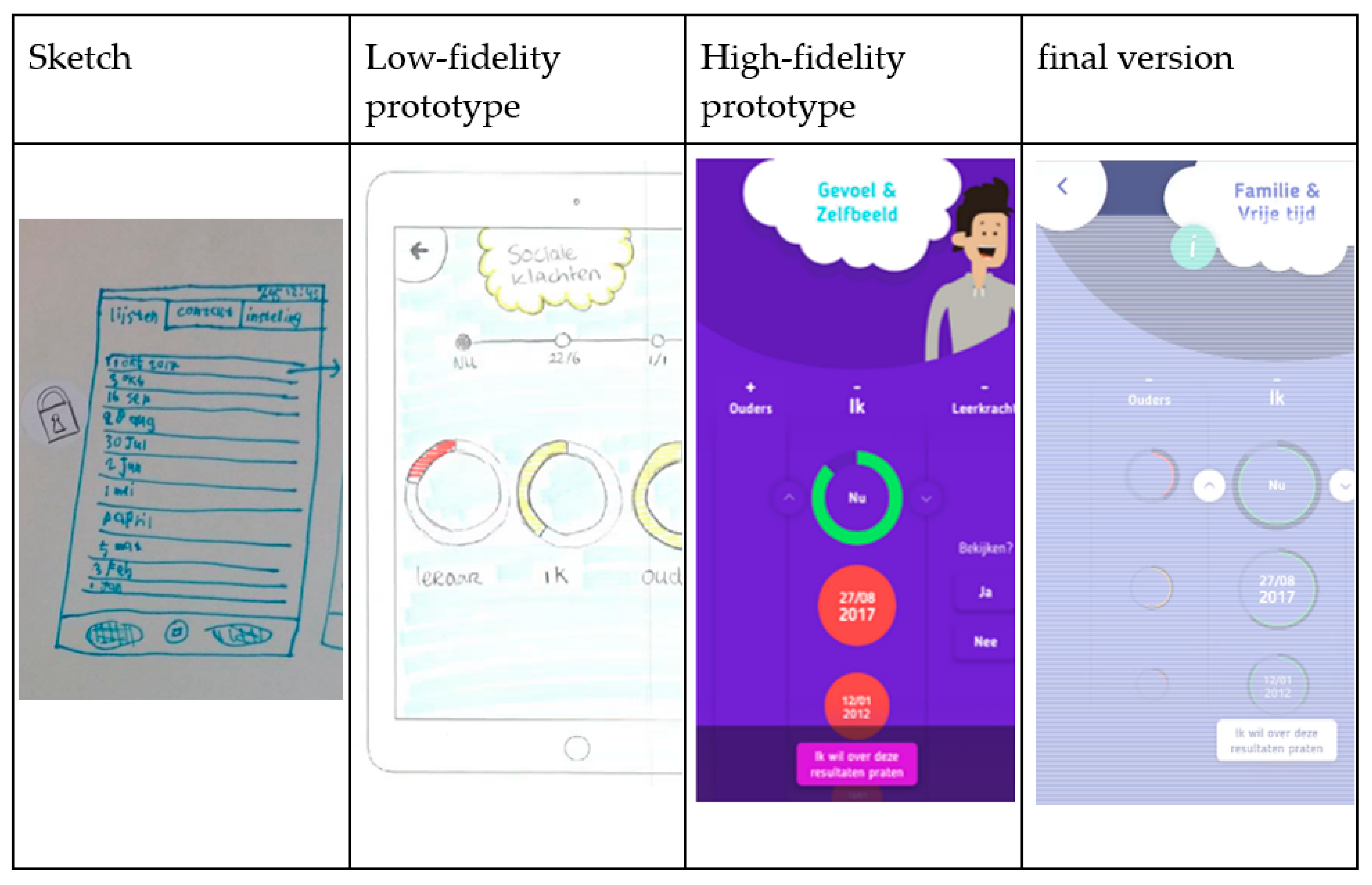
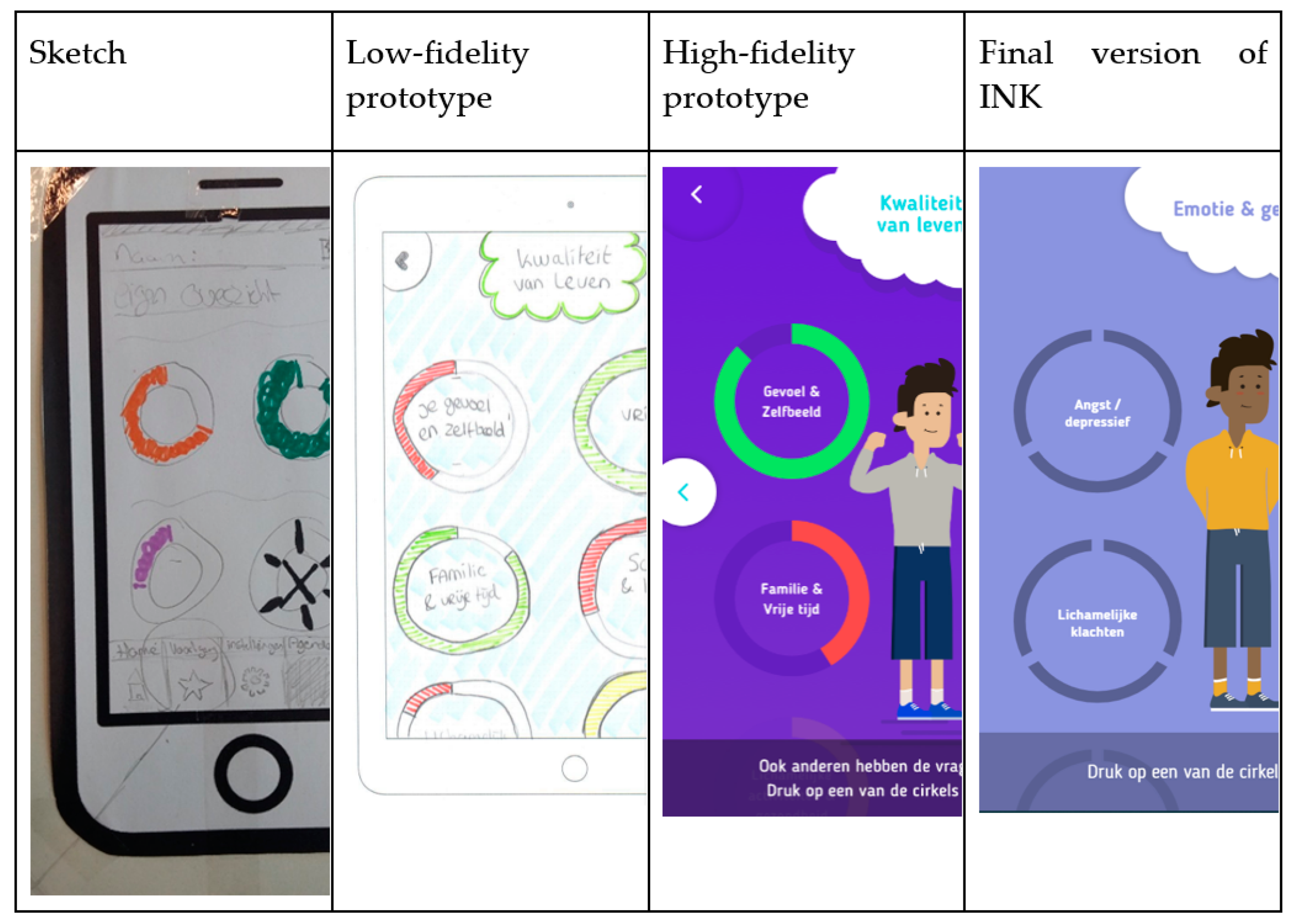
2.2.3. Phase 3: Design
2.2.4. Formative Evaluation
2.3. Ethical Approval
3. Results
3.1. Phase 1: Contextual Inquiry
3.2. Phase 2: Value Specification
3.2.1. Phase 2 Value 1: Being Well-Informed
3.2.2. Phase 2 Value 2: Personalized User Experience
3.2.3. Phase 2 Value 3: User Friendly
3.2.4. Phase 2 Value 4: Being in Control
3.2.5. Phase 2 Value 5: Privacy and Safety
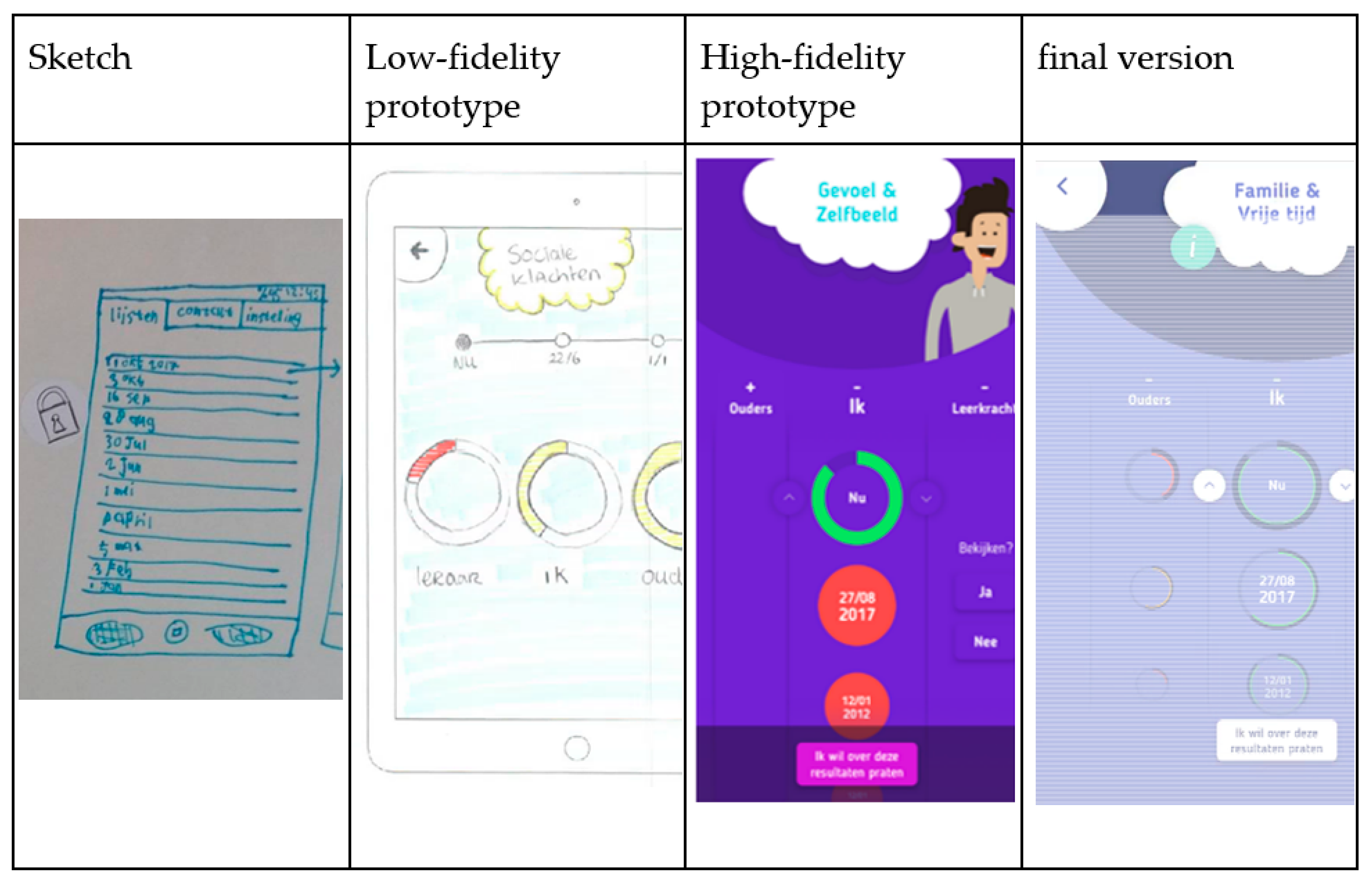
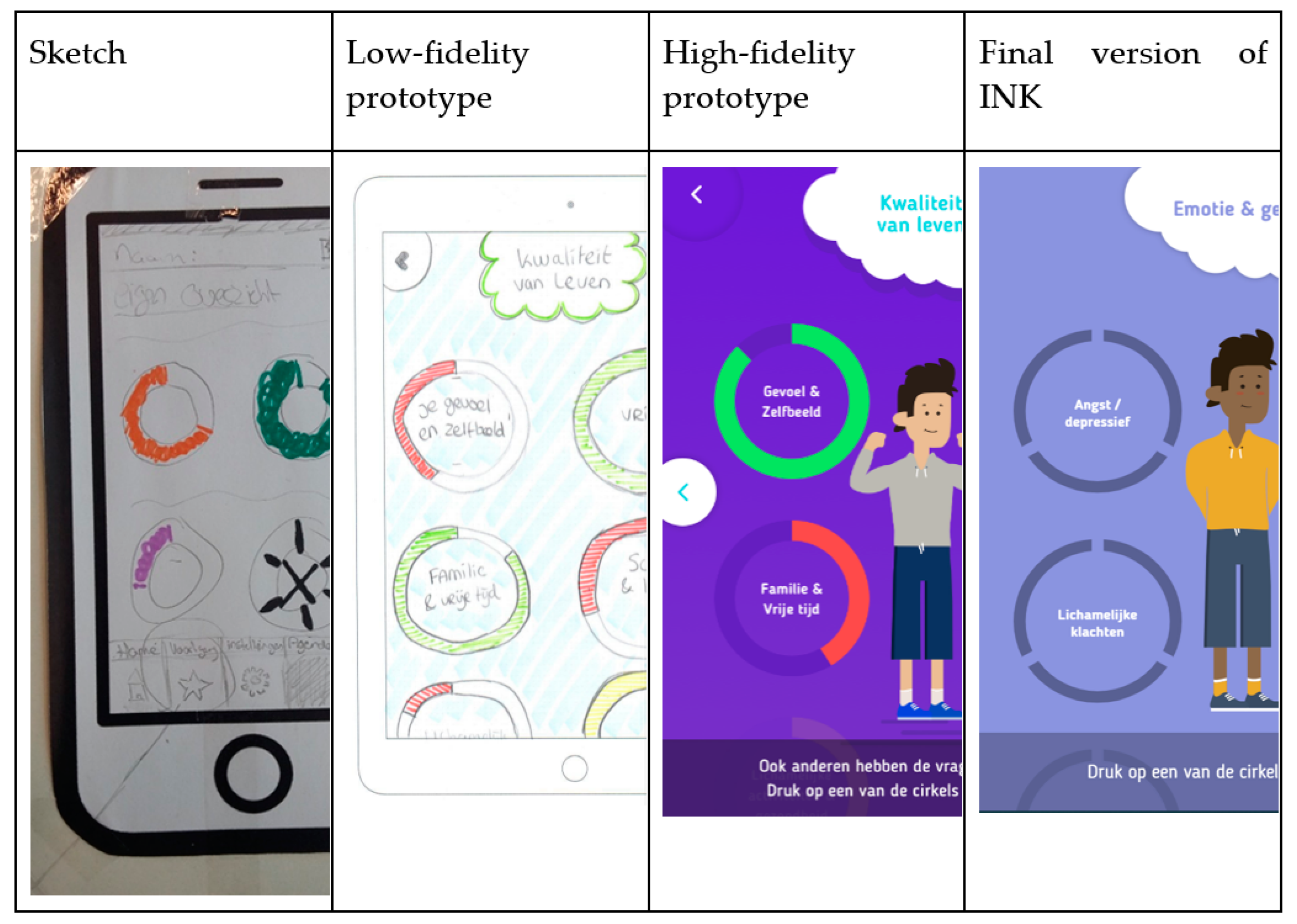
3.3. Phase 3: Design
4. Discussion
5. Strengths and Limitations
6. Future Research
7. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Conflicts of Interest
References
- De Jong, K.; Conijn, J.M.; Gallagher, R.A.; Reshetnikova, A.S.; Heij, M.; Lutz, M.C. Using progress feedback to improve outcomes and reduce drop-out, treatment duration, and deterioration: A multilevel meta-analysis. Clin. Psychol. Rev. 2021, 85, 102002. [Google Scholar] [CrossRef] [PubMed]
- De Jong, K.; Timman, R.; Hakkaart-Van Roijen, L.; Vermeulen, P.; Kooiman, K.; Passchier, J.; Busschbach, J.V. The effect of outcome monitoring feedback to clinicians and patients in short and long-term psychotherapy: A randomized controlled trial. Psychother. Res. 2014, 24, 629–639. [Google Scholar] [CrossRef] [PubMed]
- Krause, K.R.; Chung, S.; Adewuya, A.O.; Albano, A.M.; Babins-Wagner, R.; Birkinshaw, L.; Brann, P.; Creswell, C.; Delaney, K.; Falissard, B. International consensus on a standard set of outcome measures for child and youth anxiety, depression, obsessive-compulsive disorder, and post-traumatic stress disorder. Lancet Psychiatry 2021, 8, 76–86. [Google Scholar] [CrossRef]
- Tam, H.; Ronan, K. The application of a feedback-informed approach in psychological service with youth: Systematic review and meta-analysis. Clin. Psychol. Rev. 2017, 55, 41–55. [Google Scholar] [CrossRef]
- Gondek, D.; Edbrooke-Childs, J.; Fink, E.; Deighton, J.; Wolpert, M. Feedback from outcome measures and treatment effectiveness, treatment efficiency, and collaborative practice: A systematic review. Adm. Policy Ment. Health Ment. Health Serv. Res. 2016, 43, 325–343. [Google Scholar] [CrossRef] [PubMed]
- Delgadillo, J.; de Jong, K.; Lucock, M.; Lutz, W.; Rubel, J.; Gilbody, S.; Ali, S.; Aguirre, E.; Appleton, M.; Nevin, J. Feedback-informed treatment versus usual psychological treatment for depression and anxiety: A multisite, open-label, cluster randomised controlled trial. Lancet Psychiatry 2018, 5, 564–572. [Google Scholar] [CrossRef]
- Garnett, C.V.; Crane, D.; Brown, J.; Kaner EF, S.; Beyer, F.R.; Muirhead, C.R.; Hickman, M.; Beard, E.; Redmore, J.; de Vocht, F.; et al. Behavior change techniques used in digital behavior change interventions to reduce excessive alcohol consumption: A meta-regression. Ann. Behav. Med. 2018, 52, 530–543. [Google Scholar] [CrossRef]
- Jensen-Doss, A.; Haimes EM, B.; Smith, A.M.; Lyon, A.R.; Lewis, C.C.; Stanick, C.F.; Hawley, K.M. Monitoring treatment progress and providing feedback is viewed favorably but rarely used in practice. Adm. Policy Ment. Health Ment. Health Serv. Res. 2018, 45, 48–61. [Google Scholar] [CrossRef]
- Lyon, A.R.; Lewis, C.C.; Boyd, M.R.; Hendrix, E.; Liu, F. Capabilities and characteristics of digital measurement feedback systems: Results from a comprehensive review. Adm. Policy Ment. Health Ment. Health Serv. Res. 2016, 43, 441–466. [Google Scholar] [CrossRef]
- Bucci, S.; Morris, R.; Berry, K.; Berry, N.; Haddock, G.; Barrowclough, C.; Lewis, S.; Edge, D. Early psychosis service user views on digital technology: Qualitative analysis. JMIR Ment. Health 2018, 5, e10091. [Google Scholar] [CrossRef]
- Hidalgo-Mazzei, D.; Mateu, A.; Reinares, M.; Murru, A.; del Mar Bonnín, C.; Varo, C.; Valentí, M.; Undurraga, J.; Strejilevich, S.; Sánchez-Moreno, J. Psychoeducation in bipolar disorder with a SIMPLe smartphone application: Feasibility, acceptability and satisfaction. J. Affect. Disord. 2016, 200, 58–66. [Google Scholar] [CrossRef] [PubMed]
- Beck, A.K.; Kelly, P.J.; Deane, F.P.; Baker, A.L.; Hides, L.; Manning, V.; Shakeshaft, A.; Neale, J.; Kelly, J.F.; Gray, R.M. Developing a mHealth Routine Outcome Monitoring and Feedback App (“SMART Track”) to Support Self-Management of Addictive Behaviours. Front. Psychiatry 2021, 12, 820. [Google Scholar] [CrossRef] [PubMed]
- Torous, J.; Nicholas, J.; Larsen, M.E.; Firth, J.; Christensen, H. Clinical review of user engagement with mental health smartphone apps: Evidence, theory and improvements. Evid.-Based Ment. Health 2018, 21, 116–119. [Google Scholar] [CrossRef] [PubMed]
- Basnet, S.; Tamminen, M.; Lahti, T. The feasibility of eHealth in mental health care. J. Addict. Res. Ther. 2014, 5, 205. [Google Scholar] [CrossRef]
- Lal, S. E-mental health: Promising advancements in policy, research, and practice. Healthc. Manag. Fórum 2019, 32, 56–62. [Google Scholar] [CrossRef]
- Van Gemert-Pijnen, J.E.; Kip, H.; Kelders, S.M.; Sanderman, R. Introducing ehealth. In eHealth Research, Theory and Development; Routledge: London, UK, 2018; pp. 3–26. [Google Scholar]
- Kip, H.; Kelders, S.M.; Bouman, Y.H.; van Gemert-Pijnen, L.J. The importance of systematically reporting and reflecting on eHealth development: Participatory development process of a virtual reality application for forensic mental health care. J. Med. Internet Res. 2019, 21, e12972. [Google Scholar] [CrossRef]
- Mulvale, A.; Miatello, A.; Hackett, C.; Mulvale, G. Applying experience-based co-design with vulnerable populations: Lessons from a systematic review of methods to involve patients, families and service providers in child and youth mental health service improvement. Patient Exp. J. 2016, 3, 117–129. [Google Scholar] [CrossRef]
- Thabrew, H.; Fleming, T.; Hetrick, S.; Merry, S. Co-design of eHealth interventions with children and young people. Front. Psychiatry 2018, 9, 481. [Google Scholar] [CrossRef]
- Van Gemert-Pijnen, J.E.; Nijland, N.; van Limburg, M.; Ossebaard, H.C.; Kelders, S.M.; Eysenbach, G.; Seydel, E.R. A holistic framework to improve the uptake and impact of eHealth technologies. J. Med. Internet Res. 2011, 13, e1672. [Google Scholar] [CrossRef]
- Mayworm, A.M.; Kelly, B.M.; Duong, M.T.; Lyon, A.R. Middle and high school student perspectives on digitally-delivered mental health assessments and measurement feedback systems. Adm. Policy Ment. Health Ment. Health Serv. Res. 2020, 47, 531–544. [Google Scholar] [CrossRef]
- Simonse, L.; Albayrak, A.; Starre, S. Patient journey method for integrated service design. Des. Health 2019, 3, 82–97. [Google Scholar] [CrossRef]
- Kelly, P.J.; Beck, A.K.; Deane, F.P.; Larance, B.; Baker, A.L.; Hides, L.; Manning, V.; Shakeshaft, A.; Neale, J.; Kelly, J.F.; et al. Feasibility of a Mobile Health App for Routine Outcome Monitoring and Feedback in SMART Recovery Mutual Support Groups: Stage 1 Mixed Methods Pilot Study. J. Med. Internet Res. 2021, 23, e25217. [Google Scholar] [CrossRef]
- Cooper, M.; Duncan, B.; Golden, S.; Toth, K. Systematic client feedback in therapy for children with psychological difficulties: Pilot cluster randomised controlled trial. Couns. Psychol. Q. 2021, 34, 21–36. [Google Scholar] [CrossRef]
- Oinas-Kukkonen, H.; Harjumaa, M. Persuasive Systems Design: Key Issues, Process Model, and System Features. Commun. Assoc. Inf. Syst. 2009, 24, 28. [Google Scholar] [CrossRef]
- Buitenweg, D.C.; van de Mheen, D.; Grund, J.-P.; van Oers, H.; van Nieuwenhuizen, C.H. Visual and personalized quality of life assessment app for people with severe mental health problems: Qualitative evaluation. JMIR Ment. Health 2020, 7, e19593. [Google Scholar] [CrossRef] [PubMed]
- Hetrick, S.E.; Robinson, J.; Burge, E.; Blandon, R.; Mobilio, B.; Rice, S.M.; Simmons, M.B.; Alvarez-Jimenez, M.; Goodrich, S.; Davey, C.G. Youth codesign of a mobile phone app to facilitate self-monitoring and management of mood symptoms in young people with major depression, suicidal ideation, and self-harm. JMIR Ment. Health 2018, 5, e9041. [Google Scholar] [CrossRef] [PubMed]
- Morton, E.; Hole, R.; Murray, G.; Buzwell, S.; Michalak, E. Experiences of a web-based quality of life self-monitoring tool for individuals with bipolar disorder: A qualitative exploration. JMIR Ment. Health 2019, 6, e16121. [Google Scholar] [CrossRef]
- Ospina-Pinillos, L.; Davenport, T.A.; Ricci, C.S.; Milton, A.C.; Scott, E.M.; Hickie, I.B. Developing a mental health eClinic to improve access to and quality of mental health care for young people: Using participatory design as research methodologies. J. Med. Internet Res. 2018, 20, e9716. [Google Scholar] [CrossRef]
- Westermann, G.M.; Verheij, F.; Winkens, B.; Verhulst, F.C.; Van Oort, F.V. Structured shared decision-making using dialogue and visualization: A randomized controlled trial. Patient Educ. Couns. 2013, 90, 74–81. [Google Scholar] [CrossRef]
- Borghouts, J.; Eikey, E.; Mark, G.; De Leon, C.; Schueller, S.M.; Schneider, M.; Stadnick, N.; Zheng, K.; Mukamel, D.; Sorkin, D.H. Barriers to and facilitators of user engagement with digital mental health interventions: Systematic review. J. Med. Internet Res. 2021, 23, e24387. [Google Scholar] [CrossRef]
- Radomski, A.D.; Wozney, L.; McGrath, P.; Huguet, A.; Hartling, L.; Dyson, M.P.; Bennett, K.J.; Newton, A.S. Potential reduction of symptoms with the use of persuasive systems design features in internet-based cognitive behavioral therapy programs for children and adolescents with anxiety: A realist synthesis. JMIR Ment. Health 2019, 6, e13807. [Google Scholar] [CrossRef] [PubMed]
- Wahle, F.; Bollhalder, L.; Kowatsch, T.; Fleisch, E. Toward the design of evidence-based mental health information systems for people with depression:A systematic literature review and meta-analysis. J. Med. Internet Res. 2017, 19, 325–356. [Google Scholar] [CrossRef] [PubMed]
- Rasing, S.; Stikkelbroek, Y.A.; Bodden, D.H. Is digital treatment the Holy Grail? Literature review on computerized and blended treatment for depressive disorders in youth. Int. J. Environ. Res. Public Health 2020, 17, 153. [Google Scholar] [CrossRef] [PubMed]
- Crutzen, R.; de Nooijer, J.; Brouwer, W.; Oenema, A.; Brug, J.; de Vries, N.K. Strategies to facilitate exposure to internet-delivered health behavior change interventions aimed at adolescents or young adults: A systematic review. Health Educ. Behav. 2011, 38, 49–62. [Google Scholar] [CrossRef] [PubMed]
- Milward, J.; Drummond, C.; Fincham-Campbell, S.; Deluca, P. What makes online substance-use interventions engaging? A systematic review and narrative synthesis. Digit. Health 2018, 4, 2055207617743354. [Google Scholar] [CrossRef]
- Berry, K.; Salter, A.; Morris, R.; James, S.; Bucci, S. Assessing therapeutic alliance in the context of mHealth interventions for mental health problems: Development of the mobile Agnew relationship measure (mARM) questionnaire. J. Med. Internet Res. 2018, 20, e8252. [Google Scholar] [CrossRef]
- Maathuis, I.; Niezen, M.; Buitenweg, D.C.; Bongers, I.L.; van Nieuwenhuizen, C.h. Exploring human values in the design of a web-based QoL-Instrument for people with mental health problems: A value sensitive design approach. Sci. Eng. Ethics 2020, 26, 871–898. [Google Scholar] [CrossRef]
- Van Sonsbeek, M.A.; Hutschemaekers, G.J.; Veerman, J.W.; Vermulst, A.; Kleinjan, M.; Tiemens, B.G. Challenges in investigating the effective components of feedback from routine outcome monitoring (ROM) in youth mental health care. Child Youth Care Forum 2021, 50, 307–332. [Google Scholar] [CrossRef]
- Davies, F.; Shepherd, H.L.; Beatty, L.; Clark, B.; Butow, P.; Shaw, J. Implementing web-based therapy in routine mental health care: Systematic review of health professionals’ perspectives. J. Med. Internet Res. 2020, 22, e17362. [Google Scholar] [CrossRef]
- Hennemann, S.; Beutel, M.E.; Zwerenz, R. Ready for eHealth? Health professionals’ acceptance and adoption of eHealth interventions in inpatient routine care. J. Health Commun. 2017, 22, 274–284. [Google Scholar] [CrossRef]
- Damschroder, L.J.; Aron, D.C.; Keith, R.E.; Kirsh, S.R.; Alexander, J.A.; Lowery, J.C. Fostering implementation of health services research findings into practice: A consolidated framework for advancing implementation science. Implement. Sci. 2009, 4, 50. [Google Scholar] [CrossRef] [PubMed]
- Proctor, E.; Silmere, H.; Raghavan, R.; Hovmand, P.; Aarons, G.; Bunger, A.; Griffey, R.; Hensley, M. Outcomes for implementation research: Conceptual distinctions, measurement challenges, and research agenda. Adm. Policy Ment. Health Ment. Health Serv. Res. 2011, 38, 65–76. [Google Scholar] [CrossRef] [PubMed]
- Ellis, L.A.; Augustsson, H.; Grødahl, A.I.; Pomare, C.; Churruca, K.; Long, J.C.; Ludlow, K.; Zurynski, Y.A.; Braithwaite, J. Implementation of e-mental health for depression and anxiety: A critical scoping review. J. Community Psychol. 2020, 48, 904–920. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| CeHRes Phases | Goals | Activities |
|---|---|---|
| Contextual Inquiry | Identify stakeholders | Compose expert panel |
| Investigate the strong and weak points | Patient journey | |
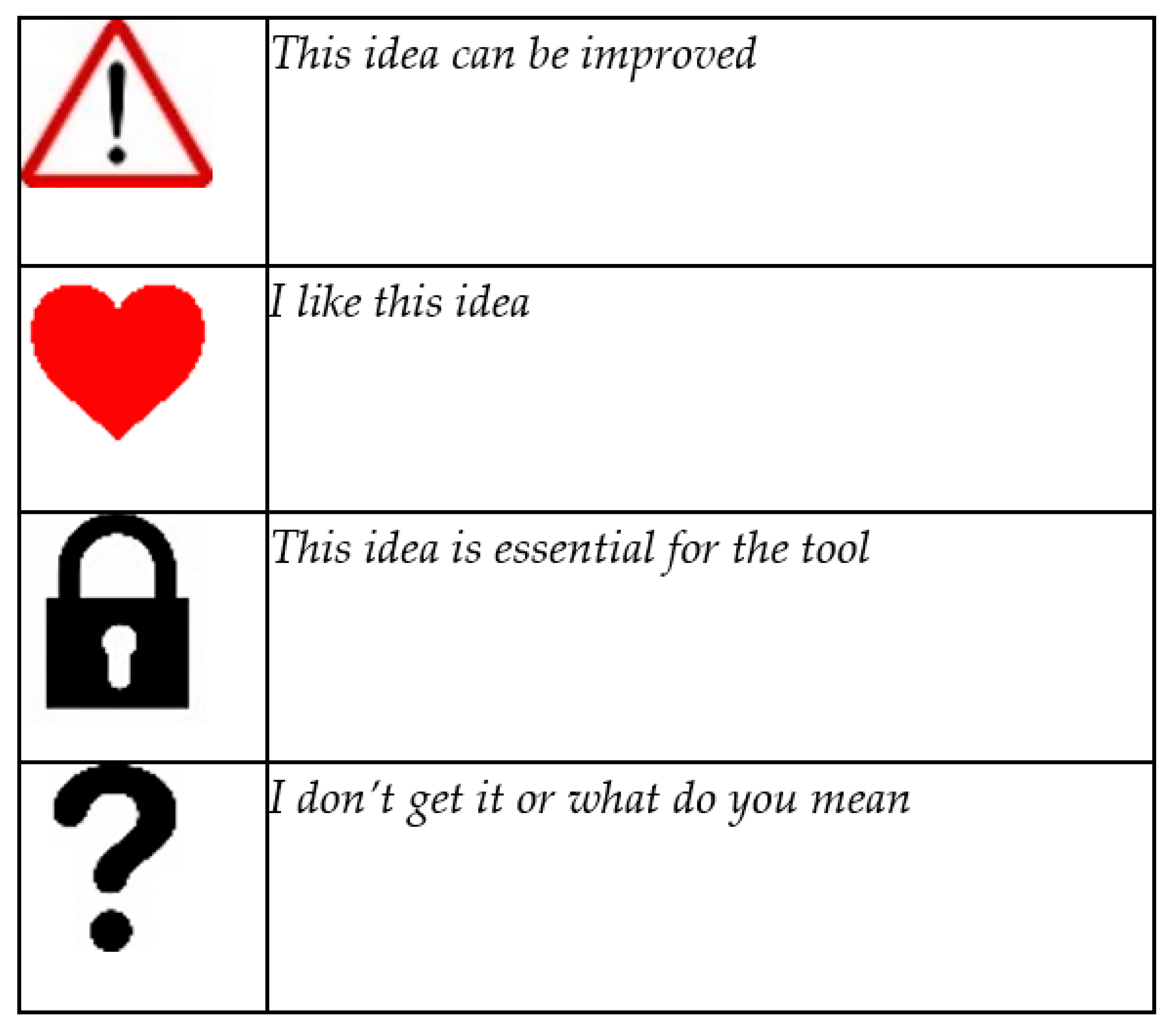
| Value Specification | Identify values of stakeholders | Brainstorm |
| Prioritize values | Use stickers and smileys | |
| Technology requirements | Sticky notes and votes | |
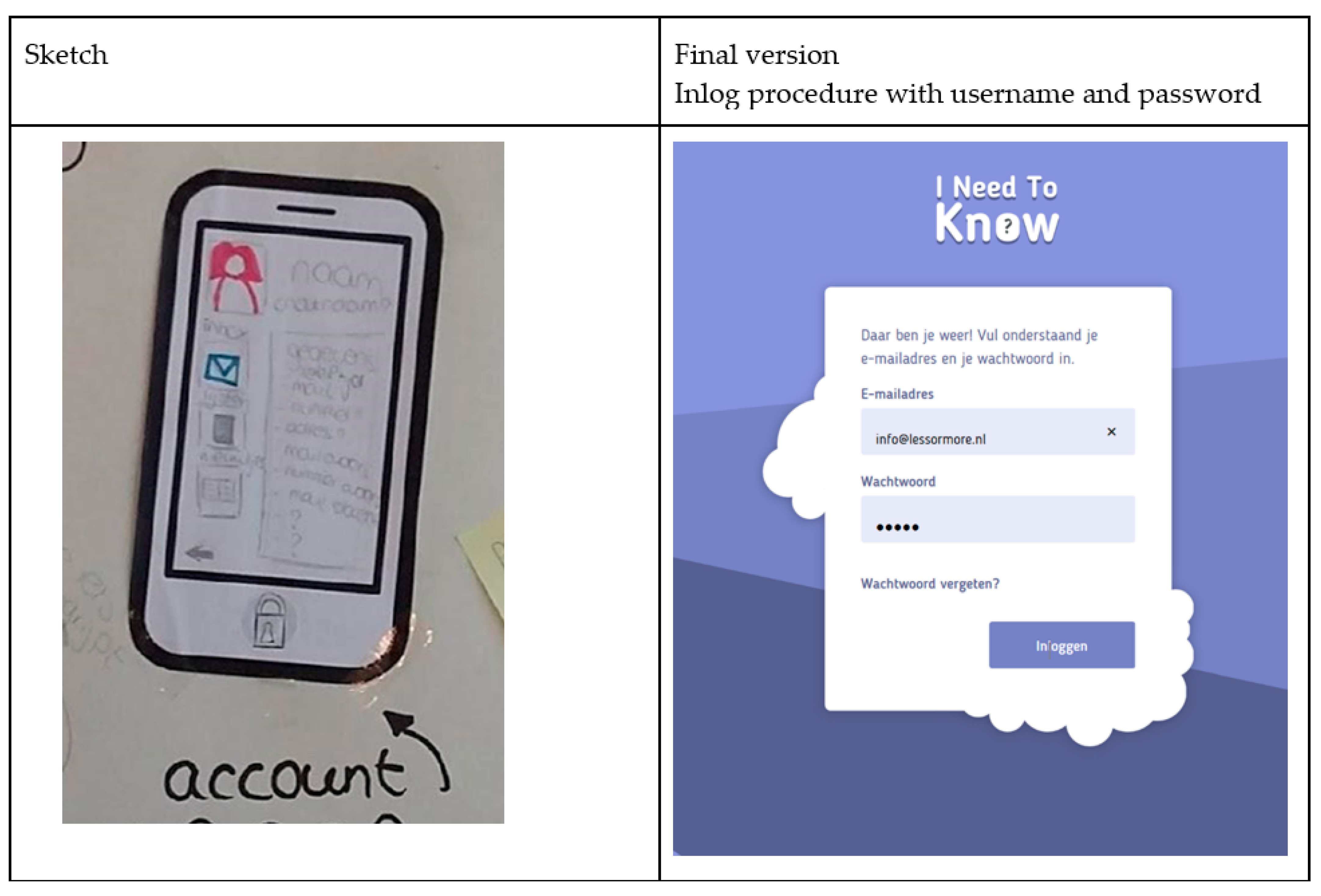
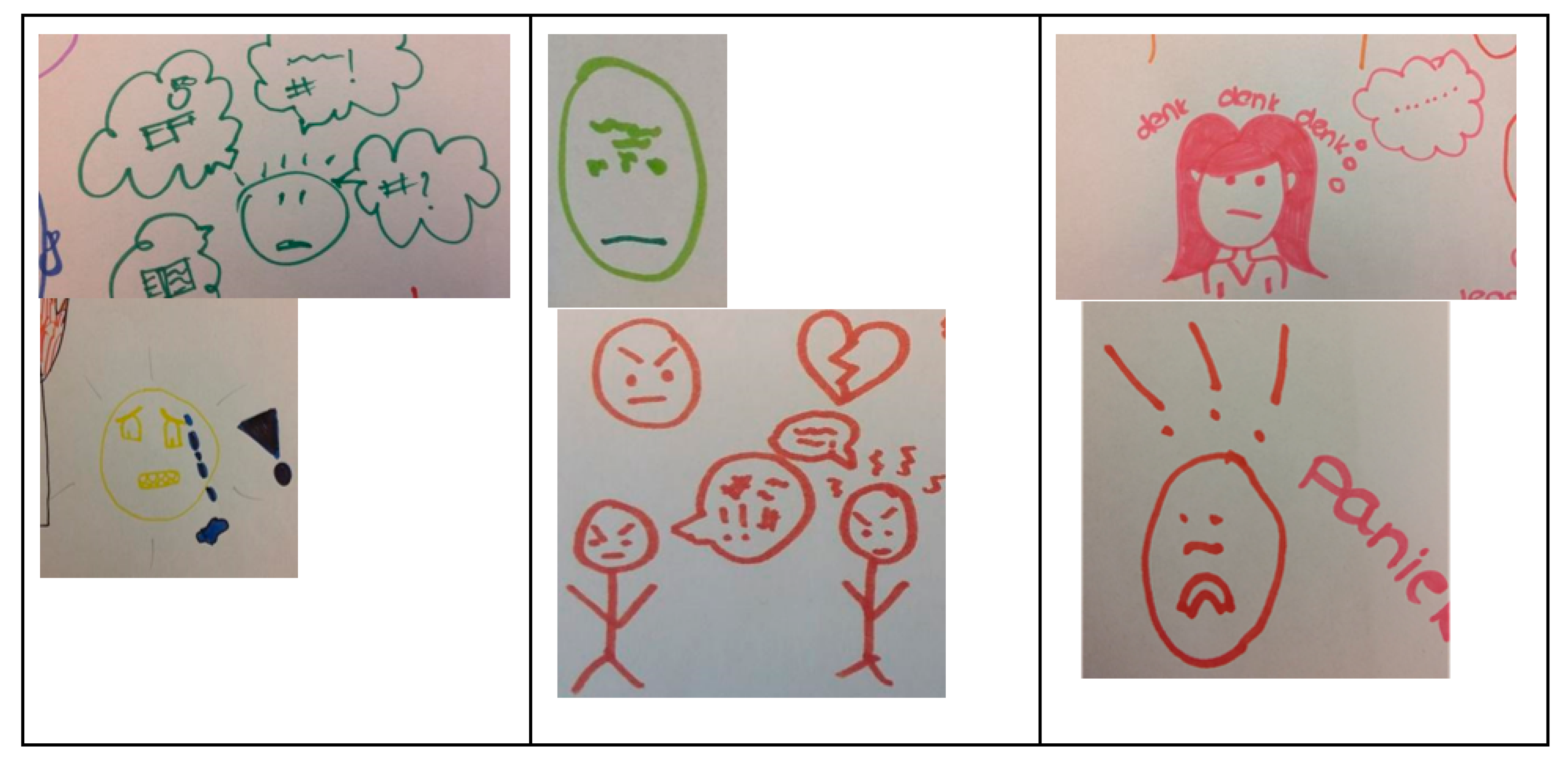
| Design | Introduction of questionnaires | Sketches by youngsters |
| Low-fidelity prototypes | Usability test | |
| High-fidelity prototypes | Structured interview |
| Value | Needs | Translation of Needs in INK |
|---|---|---|
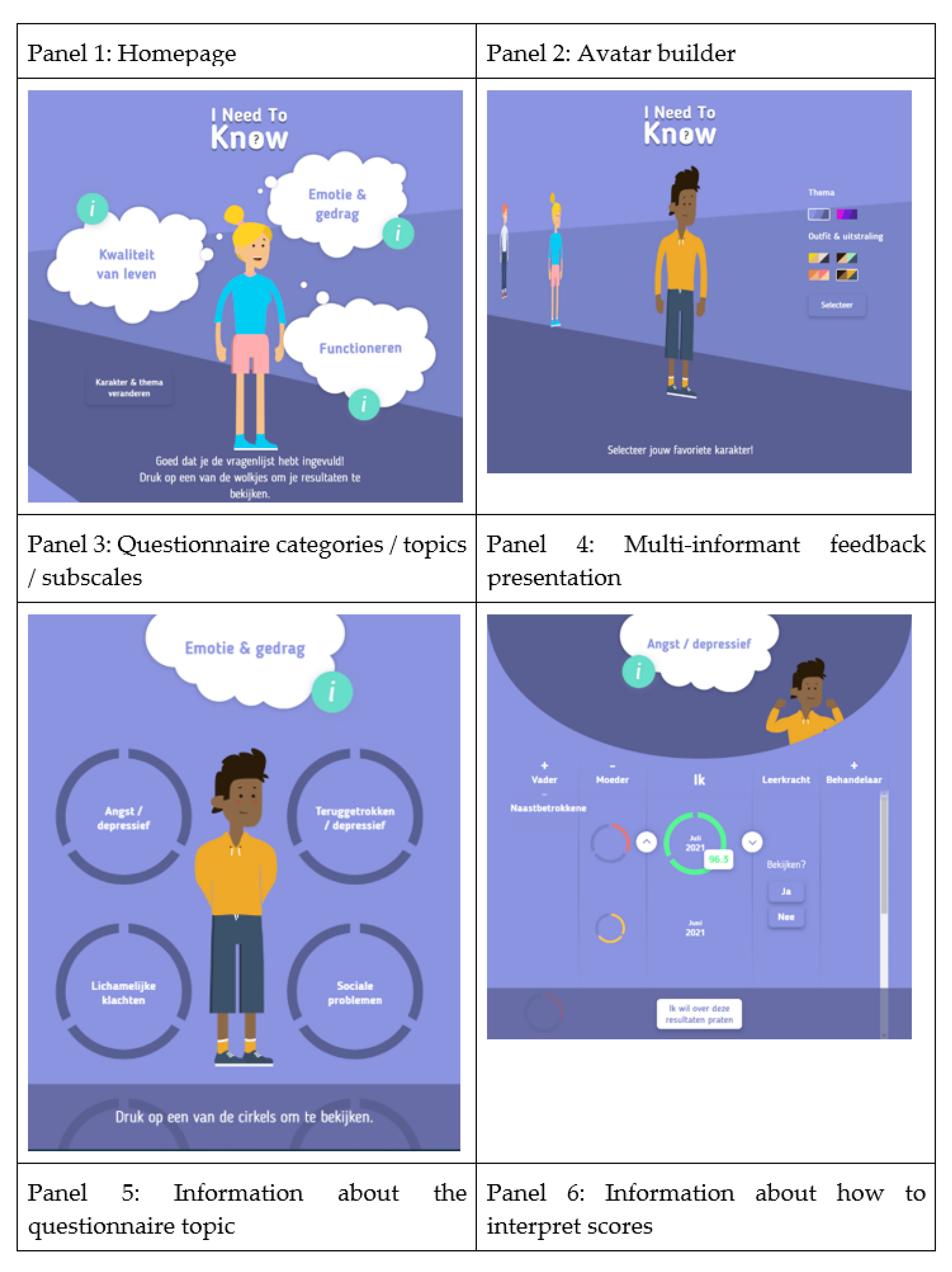
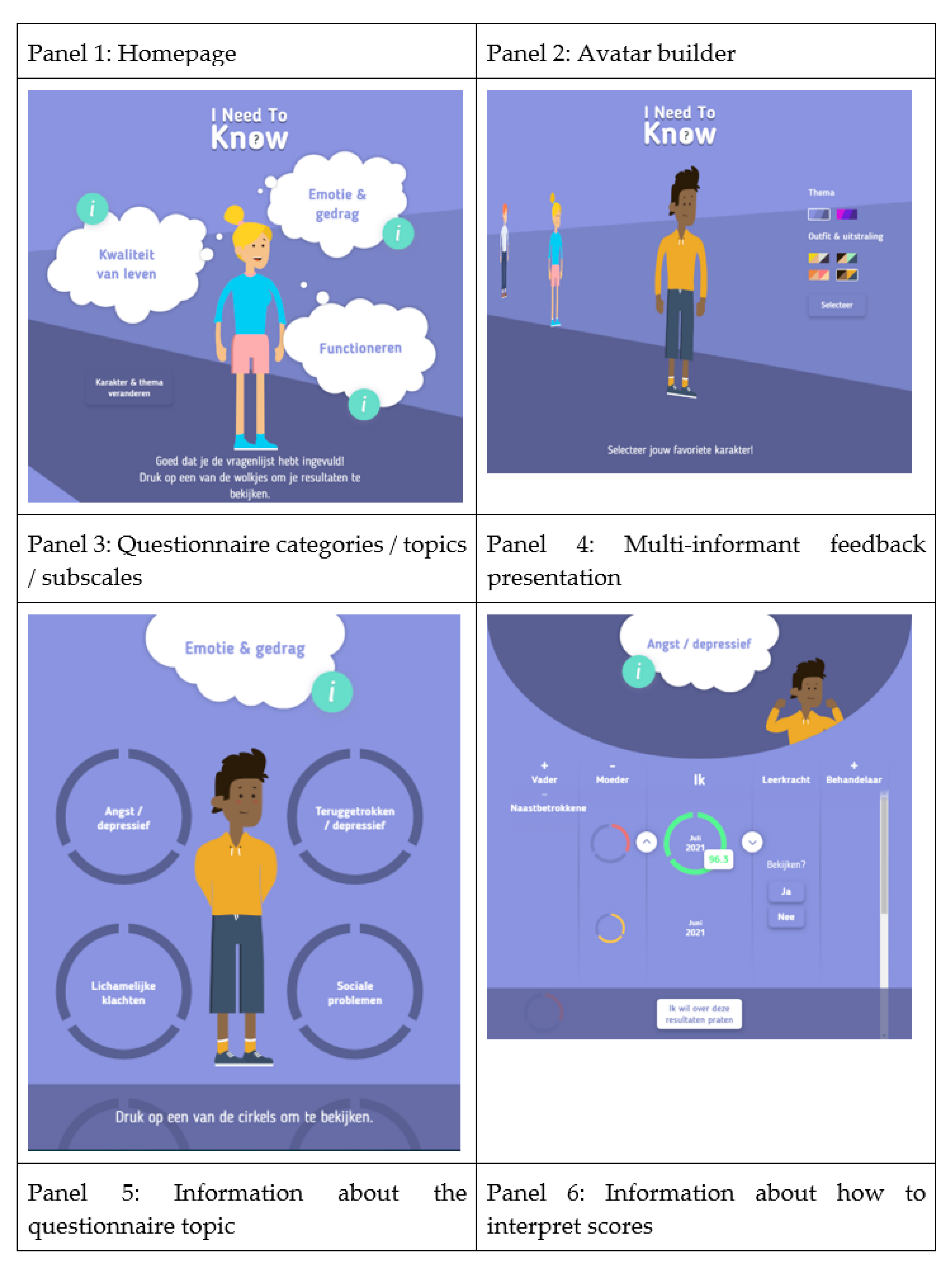
| Being well-informed | Track feedback over time | The INK application enables users to keep track of their treatment feedback over time. |
| Being well-informed | Multi-informant feedback | The INK application allows users to select and compare treatment feedback from multiple informants. |
| Being well-informed | Comprehensive and well-organized feedback | Take in everything at a single glance. The INK application shows all feedback related to one (subscale of a) questionnaire at a glance. |
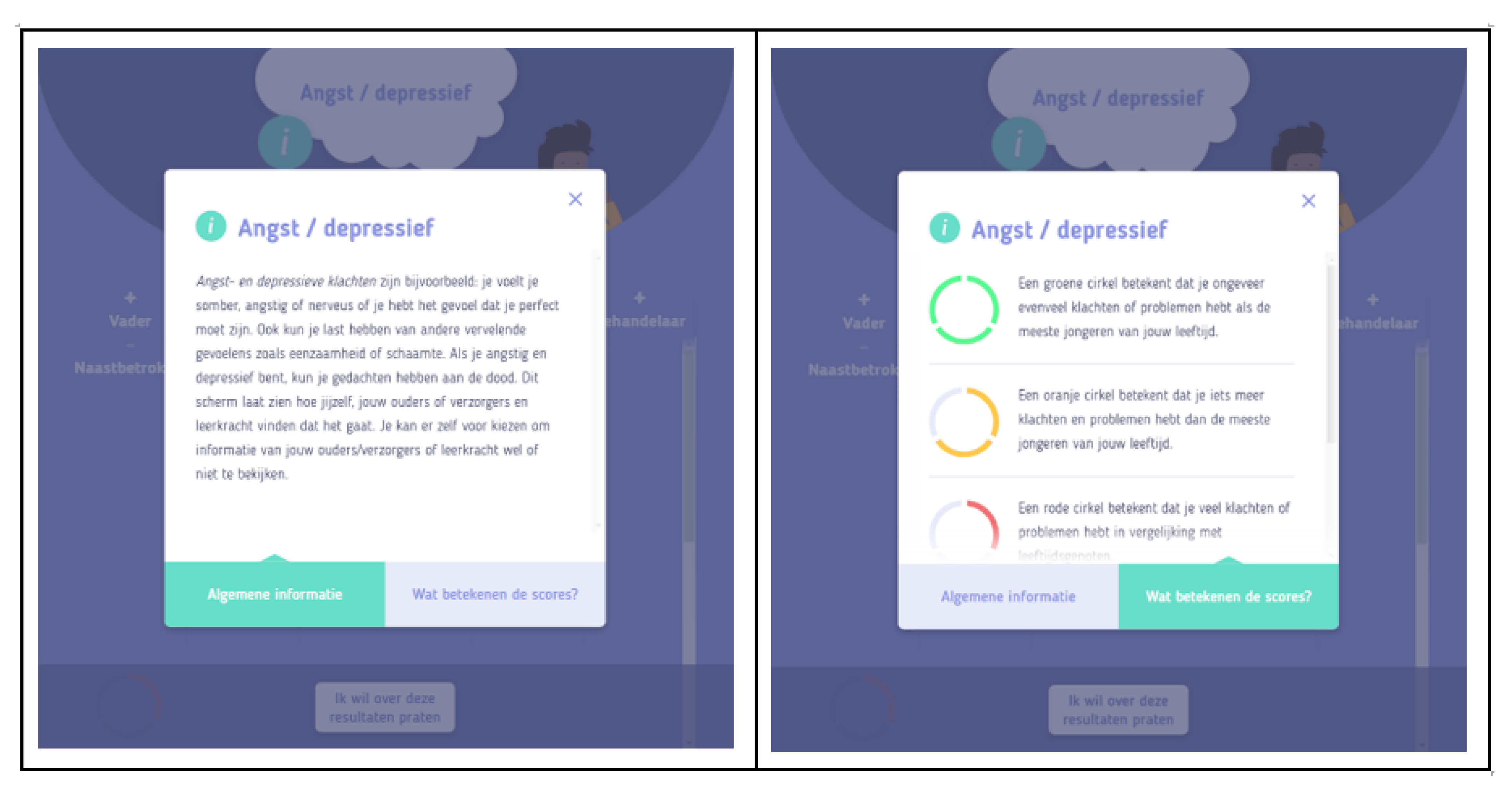
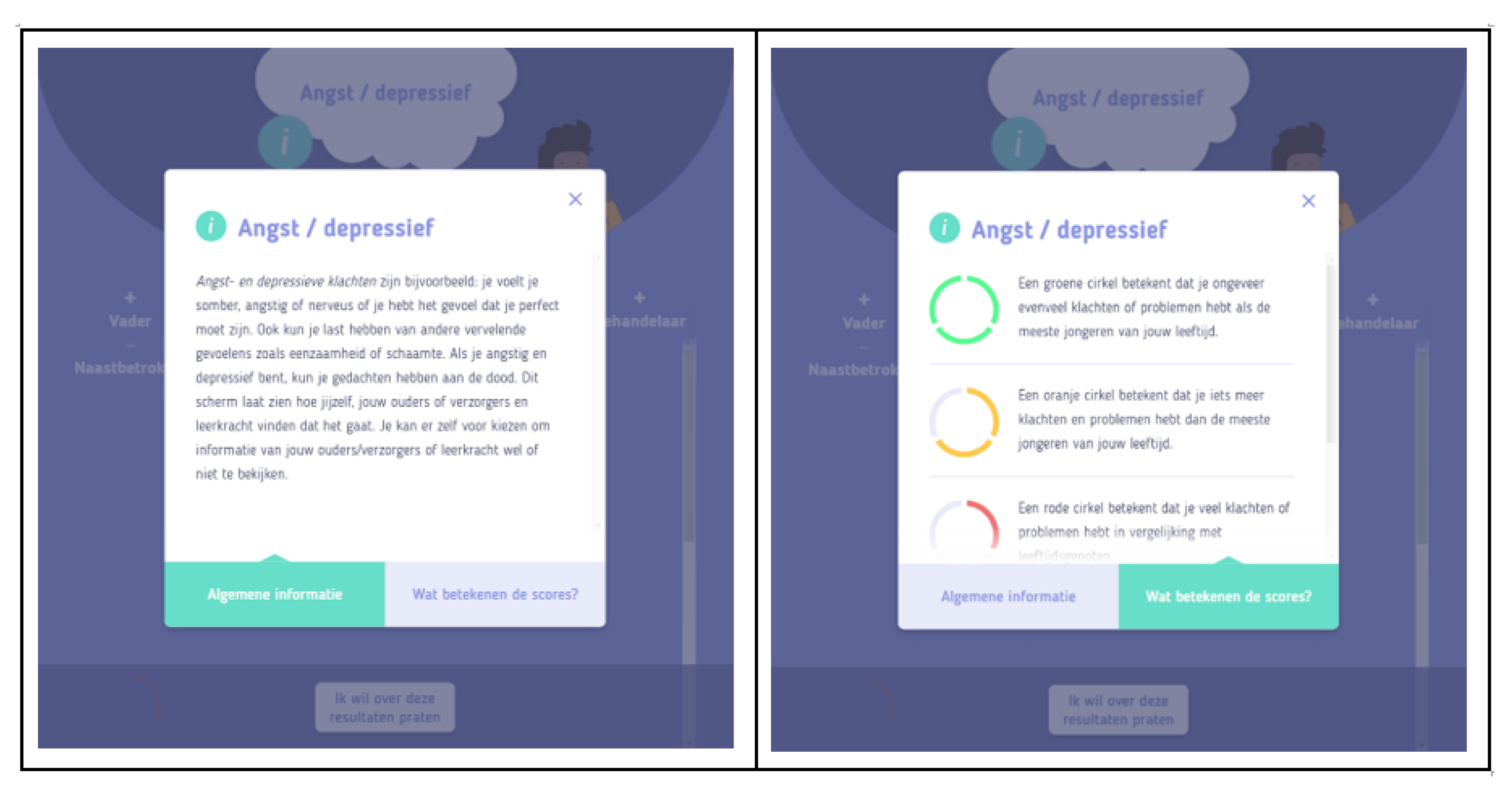
| Being well-informed | General and specific feedback | The INK application provides both general (normal, subclinical and clinical) and specific scores (0–100). |
| Being well-informed | General feedback | The colours green, orange and red are used modestly to represent normal, subclinical and clinical scores, respectively. |
| Being well-informed | Specific feedback | The INK application provides insight into the treatment progress within a specific score on a subscale of a questionnaire (0–100). |
| Being well-informed | Information about (subscales of) questionnaires | The INK application informs users about the meaning of (subscales of) questionnaires in easy-to-understand language. Mentioning positive and negative examples. |
| Personalized user experience | Profile page * | Profile page, including the possibility to upload a picture and personal information such as name, age and personal interests. |
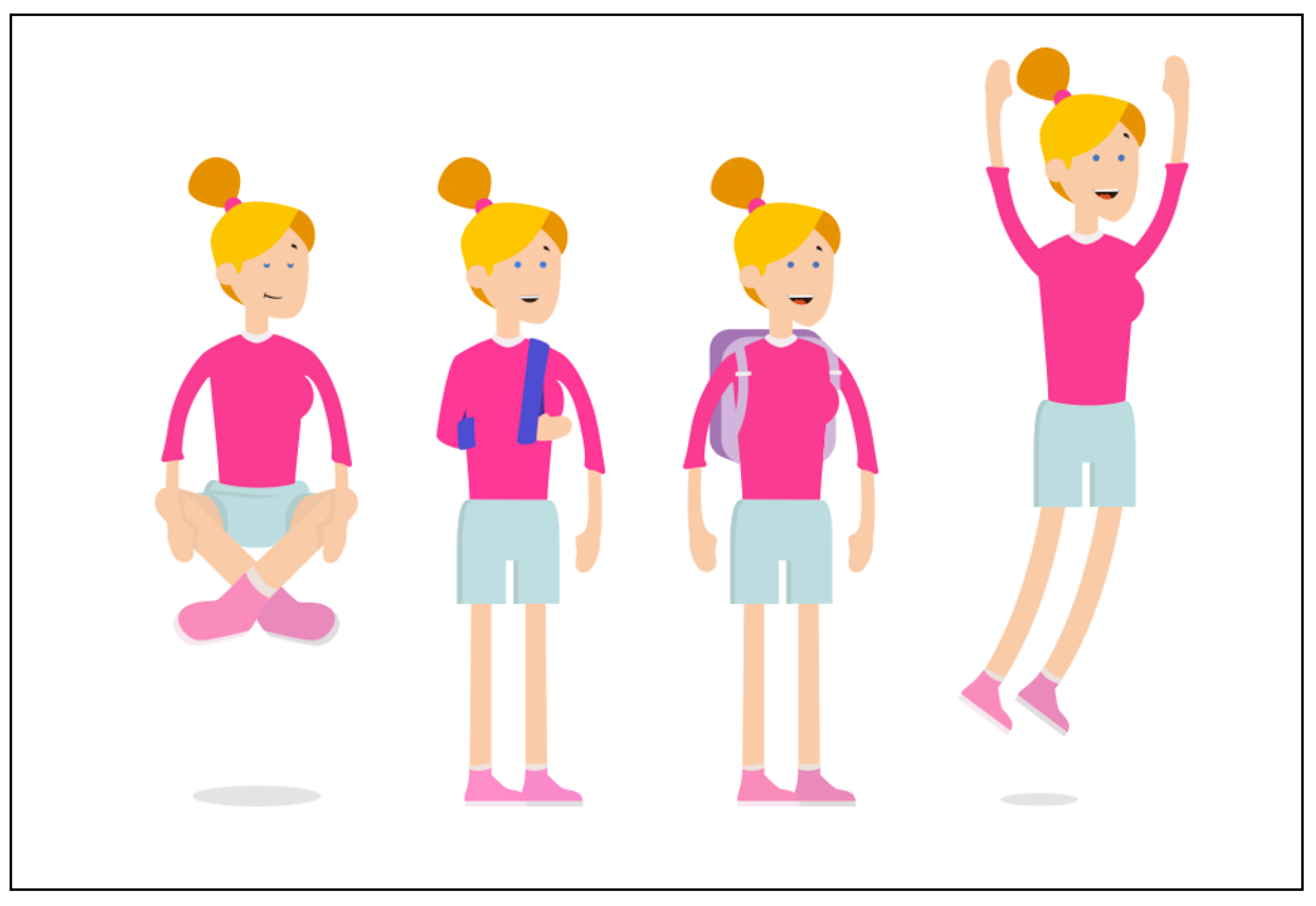
| Personalized user experience | Tailoring | Youngsters expressed different ways to adapt the application to youngsters’ characteristics. For example: showing different icons based on age, as well as allowing users to ‘build’ their own character and upload their own picture. |
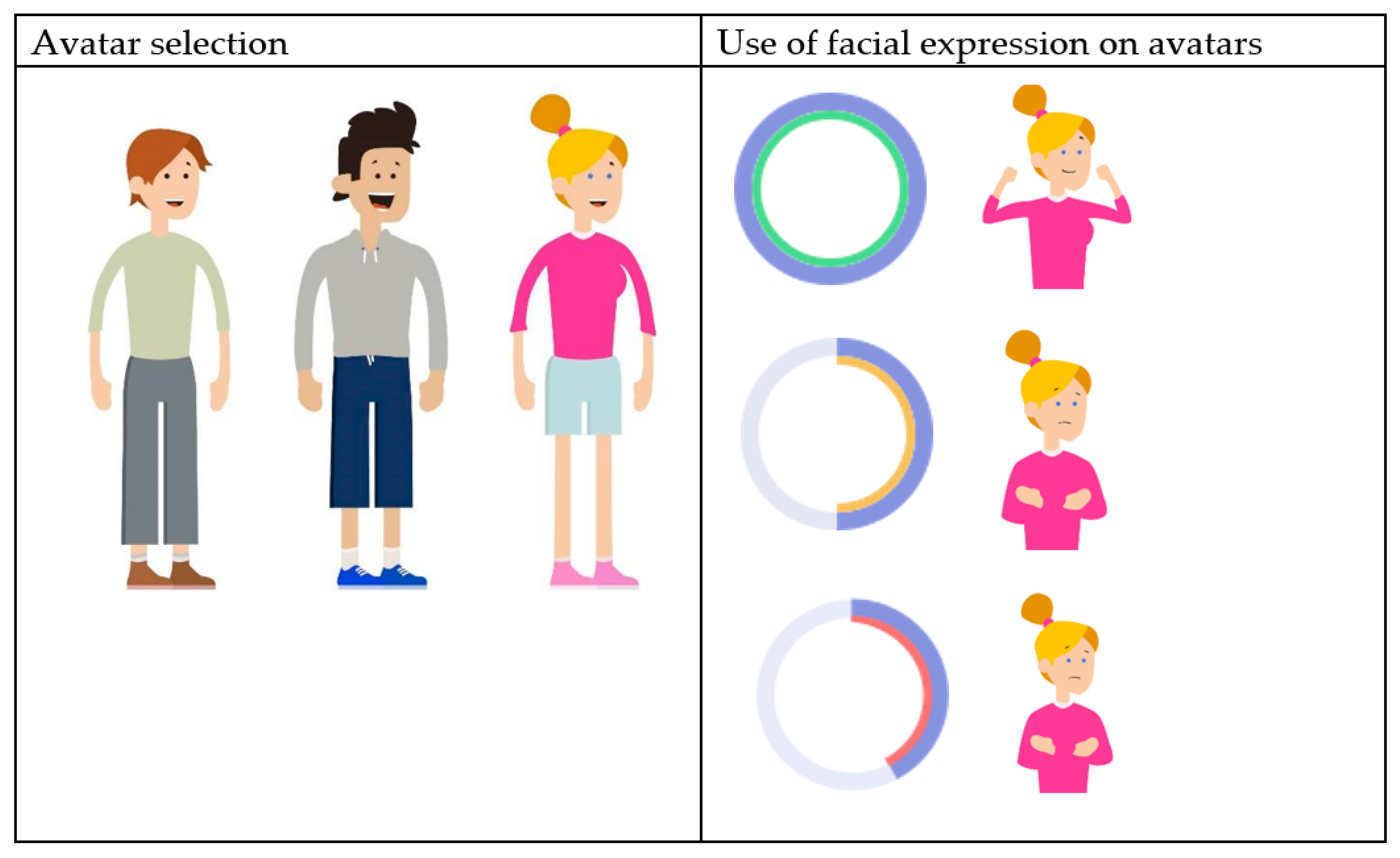
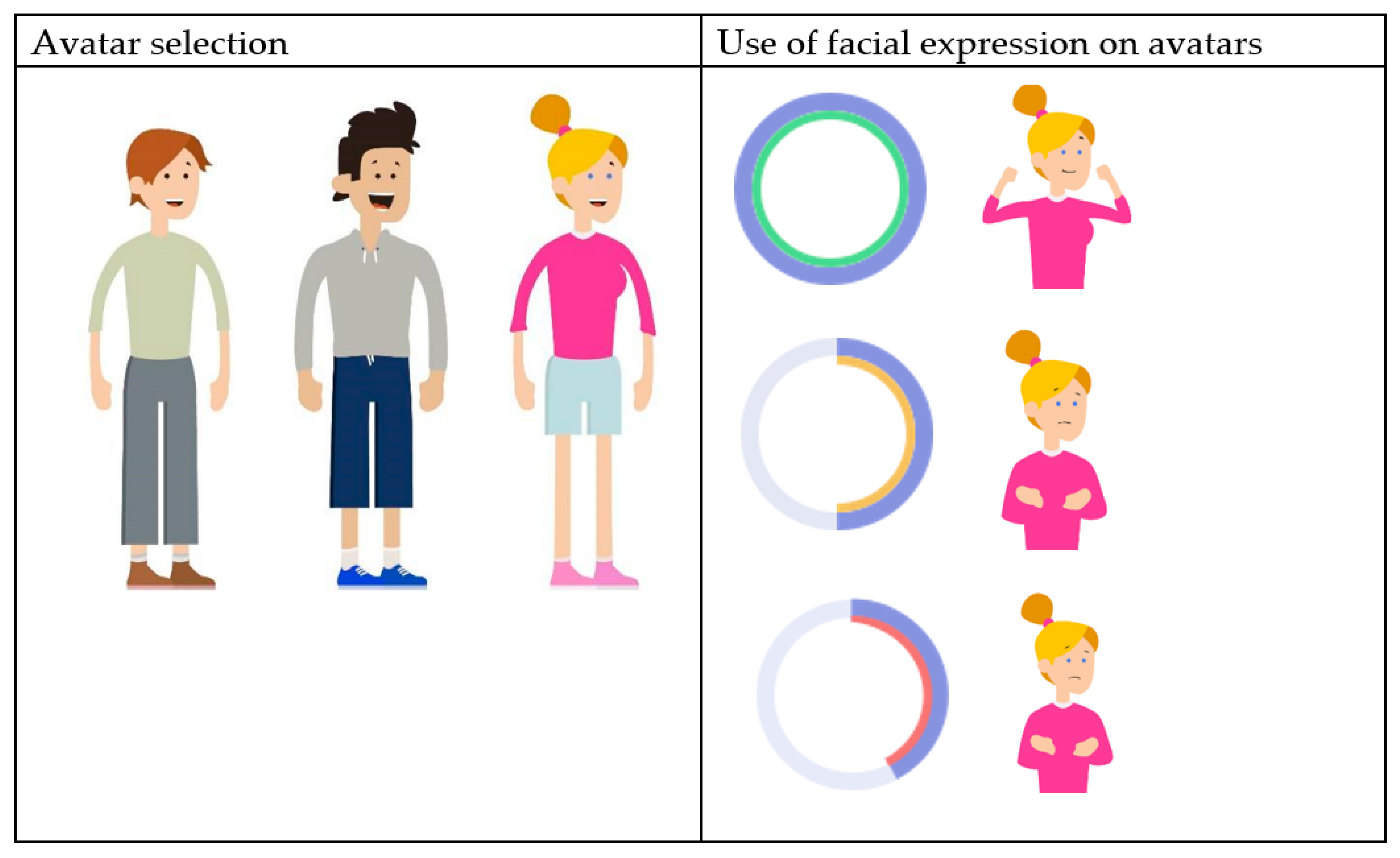
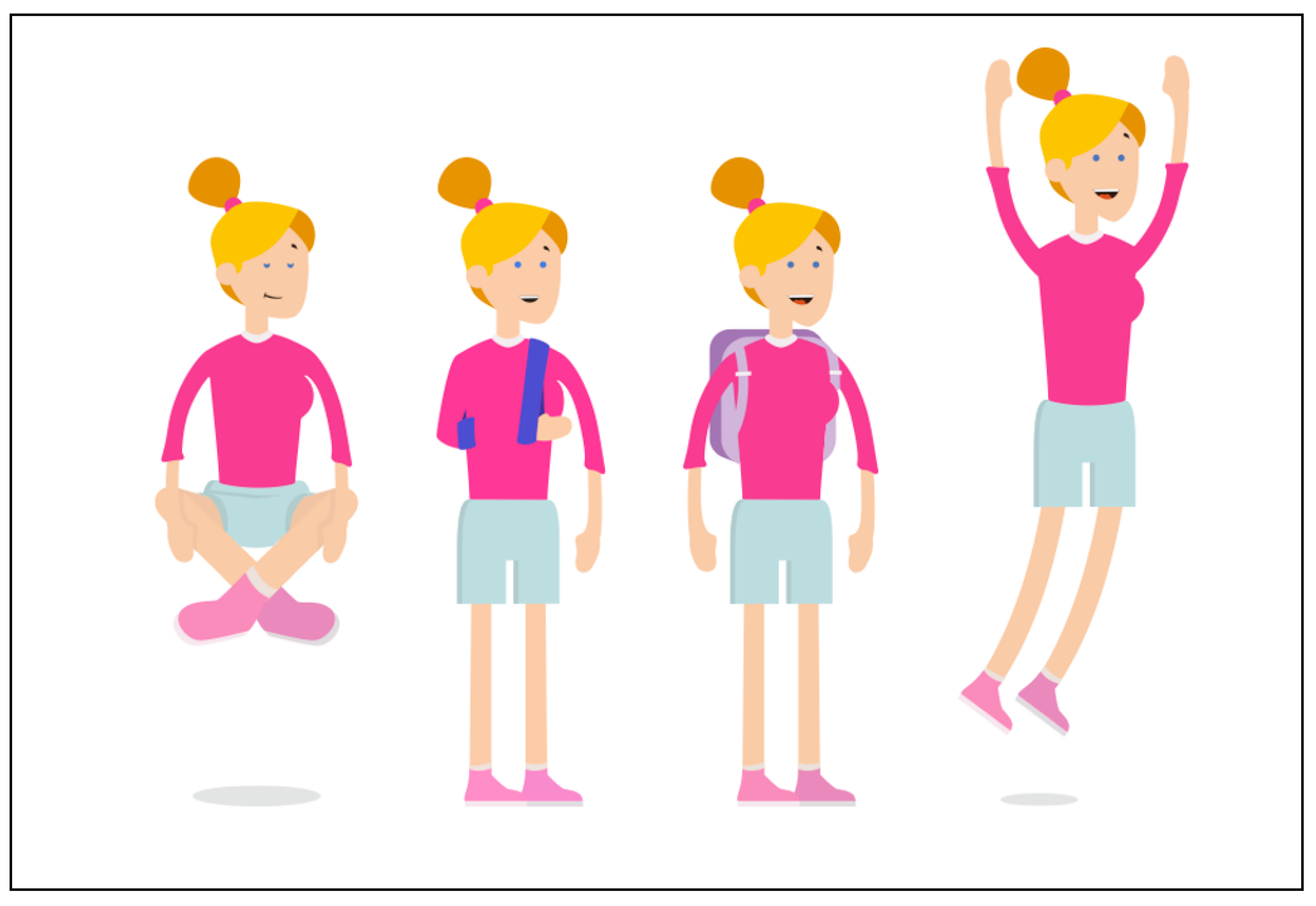
| Personalized user experience | Avatar | The avatar in INK shows personality and facial expressions. |
| Personalized user experience | Content tailoring | The avatar in INK shows different emotions based on the topic of the questionnaire and the score. |
| Personalized user experience | Age-appropriate | The design and user experience of the INK application should be age-appropriate (12–18 years). |
| Personalized user experience | Minimalistic design | The INK application has a minimalistic, simple design, which is colourful but not too vibrant in order to maintain a simplistic design. Users are able to select their colour scheme of preference in the INK application: pastel shades or bright, cheerful colours. |
| User friendly | Cheerful design | The INK application has a cheerful, non-depressing appearance. Predominant use of the colour red and avoidance of sad facial expressions. |
| User friendly | Age-appropriate | Names and descriptions of questionnaires are adapted to the reading level of youngsters. |
| User friendly | Positive affirmation | The INK application rewards end-users for filling out the questionnaires by means of positive affirmations (e.g., ’Thanks for filling out the questionnaire’ or ‘Good job!’) |
| User friendly | Easy to use | The INK application is easy to use. |
| User friendly | Easy to navigate/speed of use | Users are able to reach the desired questionnaire results in only a few clicks. |
| User friendly | Well-functioning | The INK application can be used on a mobile phone, tablet or computer. |
| Being in control | Express agreement * | A desirable feature is to report whether you agree with the reported questionnaire results. For example, when youngsters observe that their parents, teachers and/or clinicians hold different opinions about the youngsters’ behavioural and emotional problems, it is nice to discuss these different opinions. |
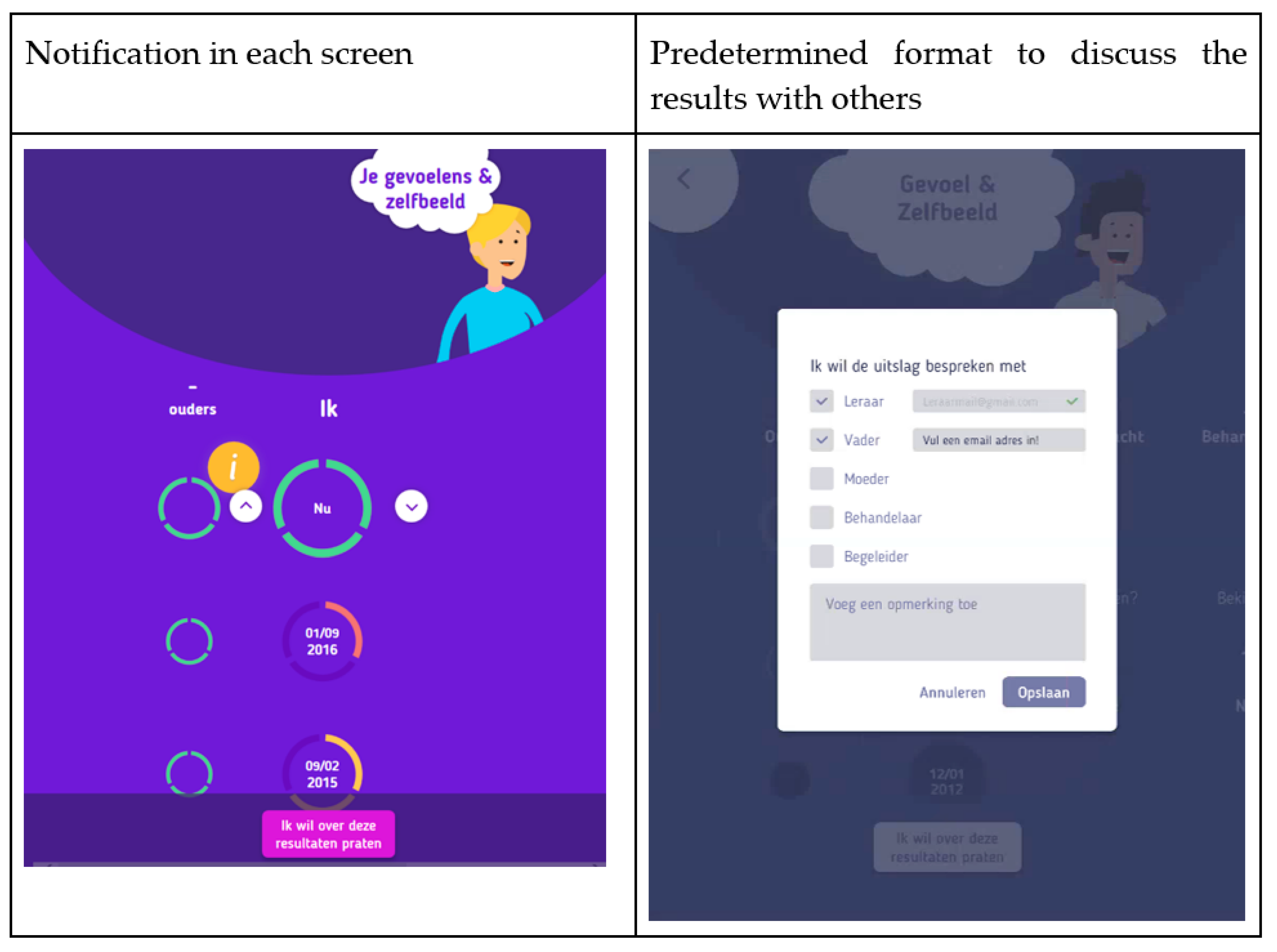
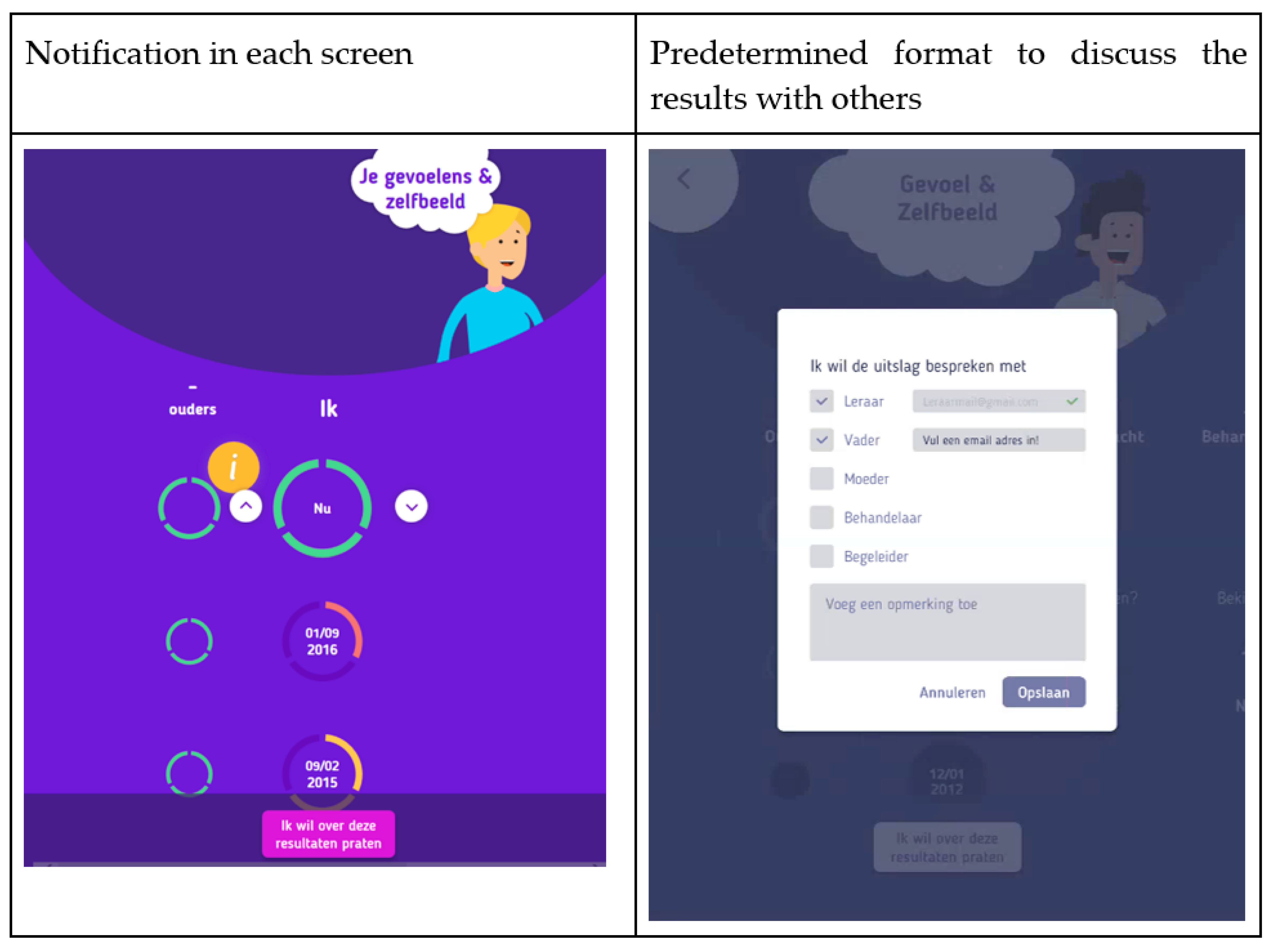
| Being in control | Notification to other informants | Another desirable feature is to mark specific questionnaire results you would like to discuss with others, such as one’s relatives or therapist. |
| Being in control | List of marked questions * | ‘Marked’ questions should be saved on a list, so they are easy to retrieve. This list can serve as a conversation aid in one’s therapy session. |
| Being in control | Reminder * | Reminder when a new questionnaire is available to fill out and/or when there are new results available. |
| Being in control | Chat * | The INK application should have a chat function to ask feedback-related questions to your therapist and/or (anonymous) contact with peers to share feelings. |
| Being in control | Calendar * | The INK application should have a calendar displaying all (treatment-related) appointments and tasks. |
| Being in control | Tutorial | The INK application shows a pop-up with short instructions on first use (tutorial). |
| Being in control | Homepage | Attractive homepage and an indication of the application’s main features. |
| Being in control | Self-management | The youngsters decide who can access their questionnaire results. |
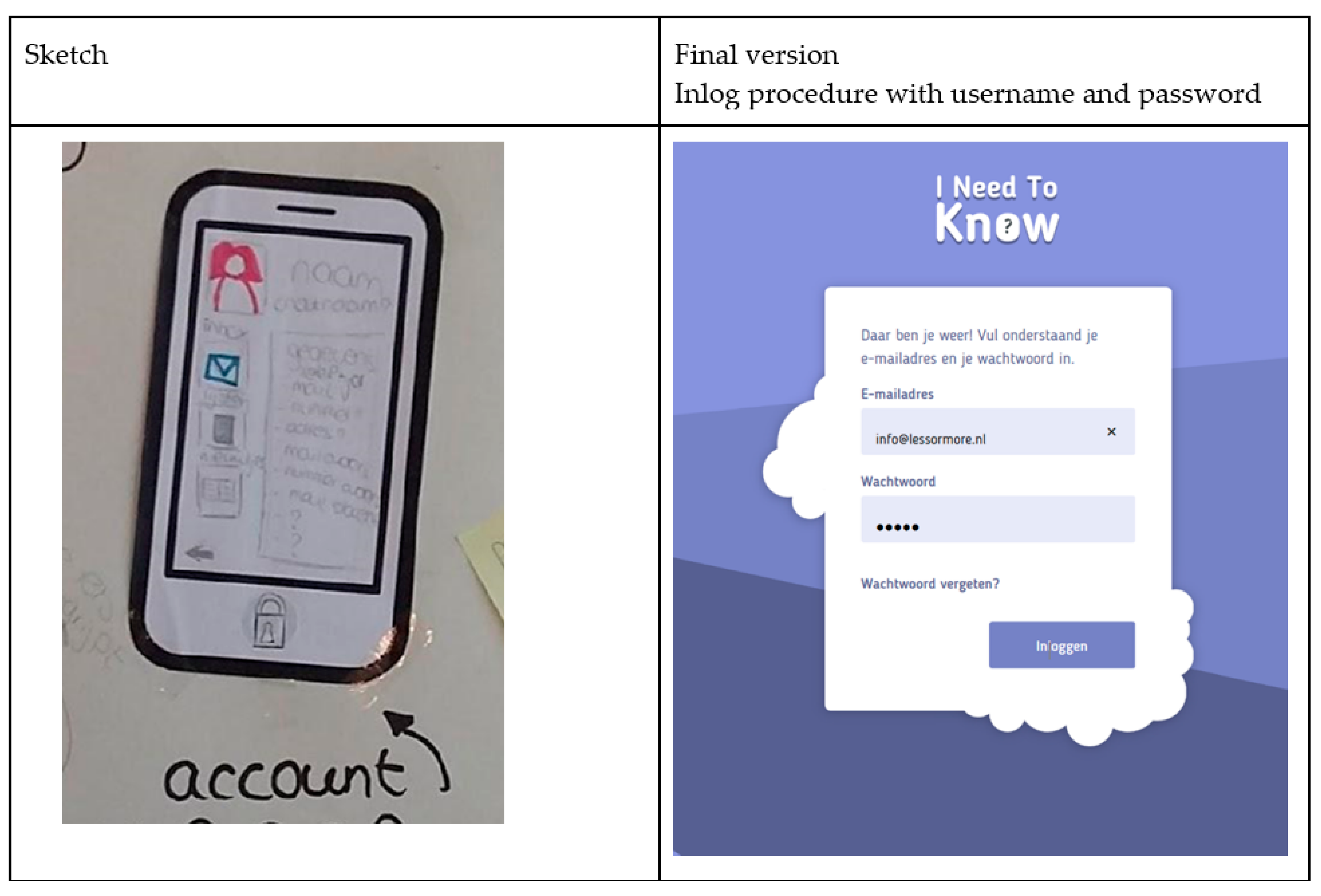
| Being in control | Data access | Only youngsters have access to INK. |
| Privacy and safety | Safe storage of data | Data should be handled confidentially and stored in a safe manner. |
| Privacy and safety | Advertisements | The INK application is free of (personalized) advertisements. |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Bongers, I.L.; Buitenweg, D.C.; van Kuijk, R.E.F.M.; van Nieuwenhuizen, C. I Need to Know: Using the CeHRes Roadmap to Develop a Treatment Feedback Tool for Youngsters with Mental Health Problems. Int. J. Environ. Res. Public Health 2022, 19, 10834. https://doi.org/10.3390/ijerph191710834
Bongers IL, Buitenweg DC, van Kuijk REFM, van Nieuwenhuizen C. I Need to Know: Using the CeHRes Roadmap to Develop a Treatment Feedback Tool for Youngsters with Mental Health Problems. International Journal of Environmental Research and Public Health. 2022; 19(17):10834. https://doi.org/10.3390/ijerph191710834
Chicago/Turabian StyleBongers, Ilja L., David C. Buitenweg, Romy E. F. M. van Kuijk, and Chijs van Nieuwenhuizen. 2022. "I Need to Know: Using the CeHRes Roadmap to Develop a Treatment Feedback Tool for Youngsters with Mental Health Problems" International Journal of Environmental Research and Public Health 19, no. 17: 10834. https://doi.org/10.3390/ijerph191710834
APA StyleBongers, I. L., Buitenweg, D. C., van Kuijk, R. E. F. M., & van Nieuwenhuizen, C. (2022). I Need to Know: Using the CeHRes Roadmap to Develop a Treatment Feedback Tool for Youngsters with Mental Health Problems. International Journal of Environmental Research and Public Health, 19(17), 10834. https://doi.org/10.3390/ijerph191710834