
From Physical Distancing to Social Loneliness among Gay Men and Other Men Having Sex with Men in Belgium: Examining the Disruption of the Social Network and Social Support Structures

 , ,
, ,
Abstract
:1. Introduction
1.1. Problem Statement
1.2. Physical Distancing among LGBTQI+ during the SARS-CoV-2 Pandemic
1.3. Conditions for LGBTQI+ during Lockdown in Flanders, Belgium
1.4. Theoretical Framework
1.4.1. Social Loneliness
1.4.2. Remote Communication
1.4.3. Model of Social Provisions
1.4.4. Type of Tie
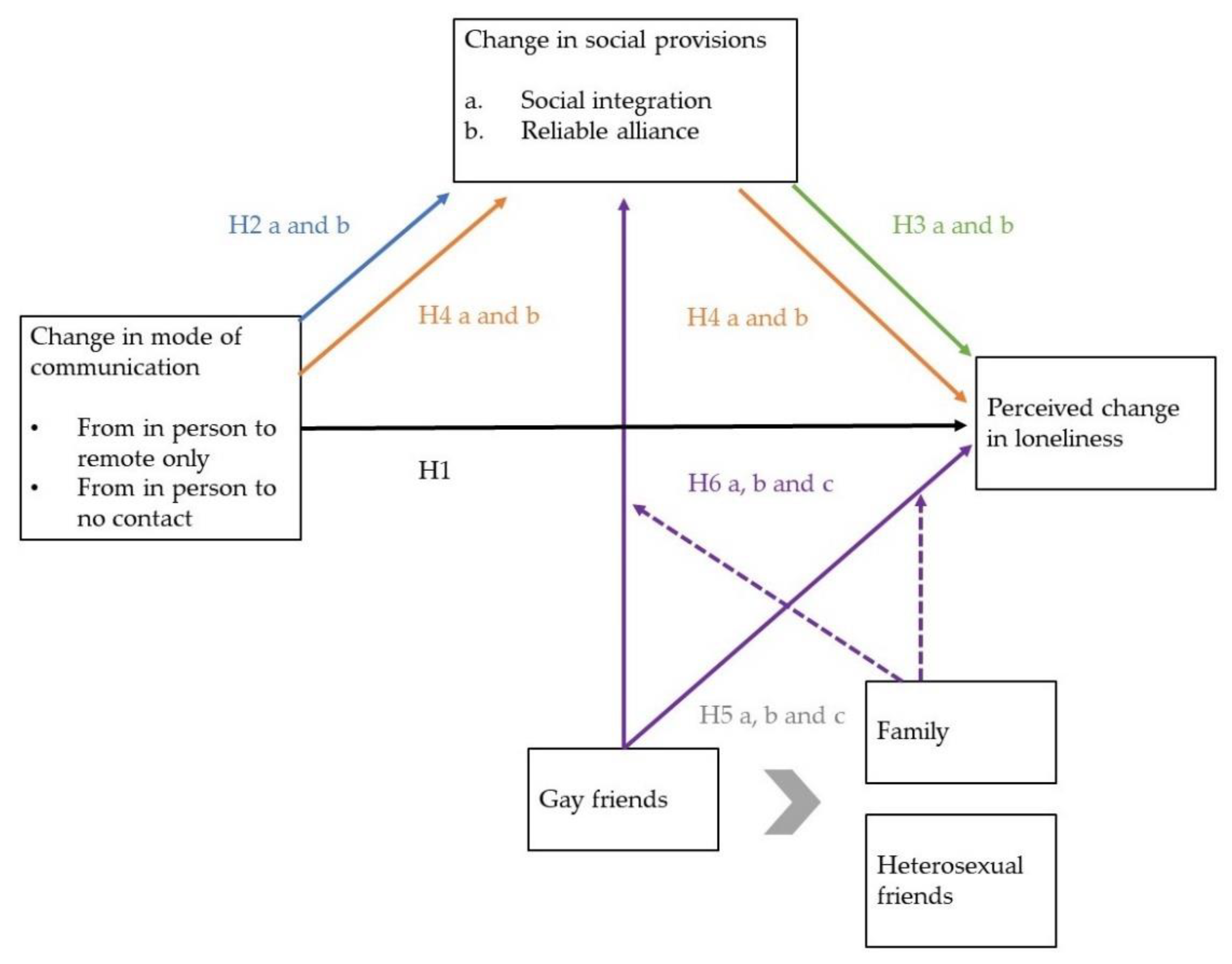
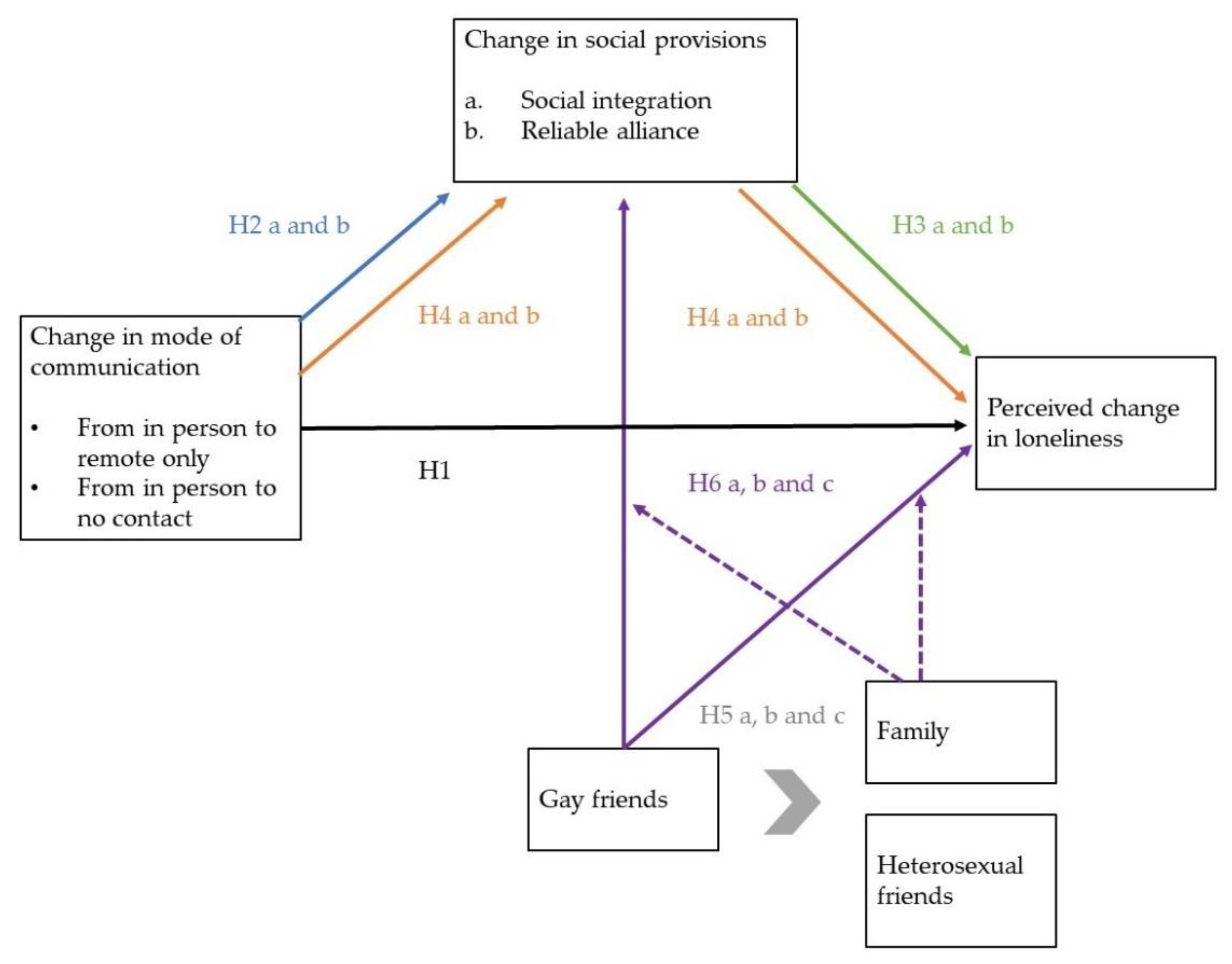
1.5. Hypotheses
2. Materials and Methods
2.1. Participants
2.2. Procedures
2.3. Measures
2.3.1. Mode of Communication
2.3.2. Social Integration
2.3.3. Reliable Alliance
2.3.4. Social Loneliness
2.3.5. Control Variables of Age and Economic Hardship
2.4. Analysis
3. Results
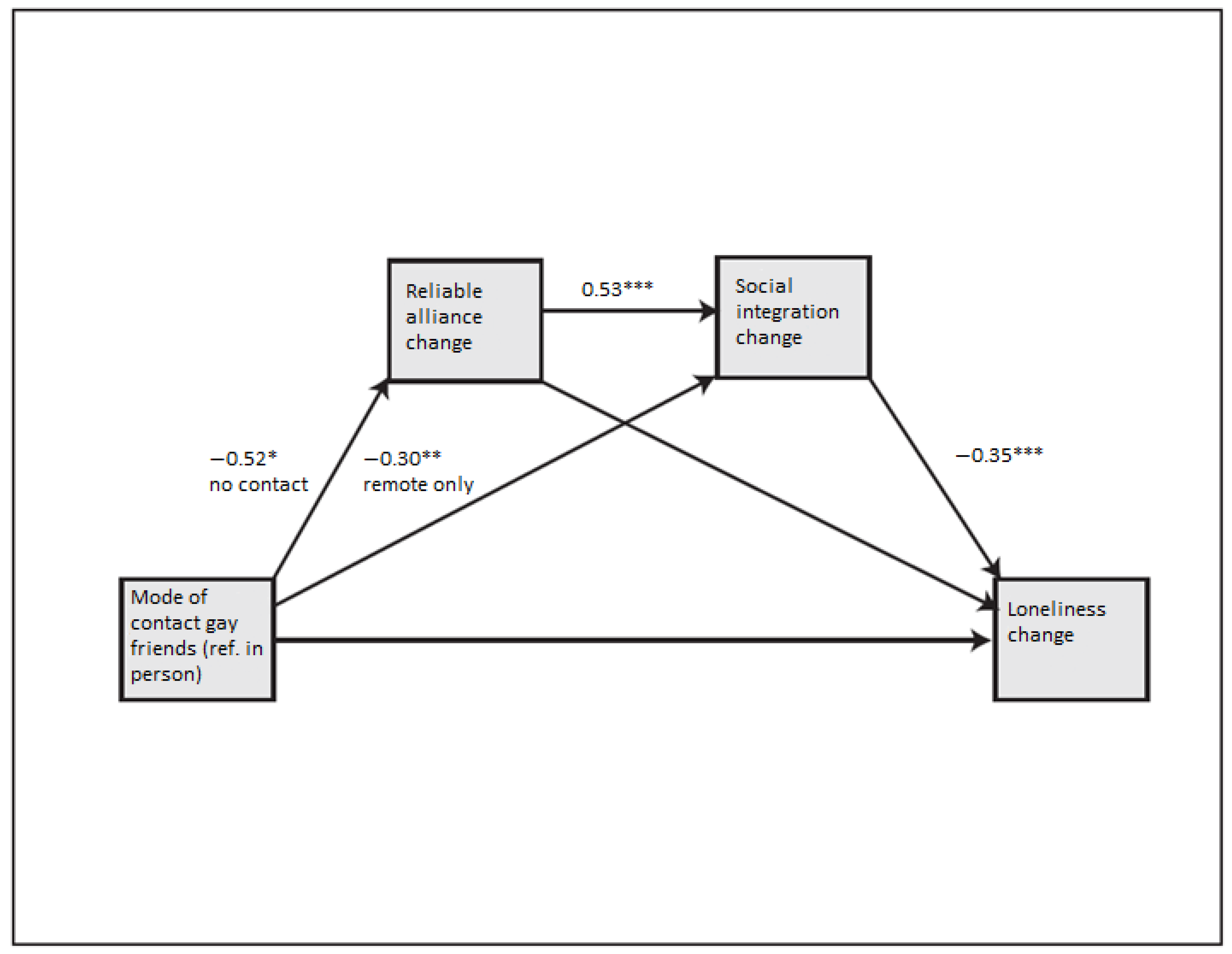
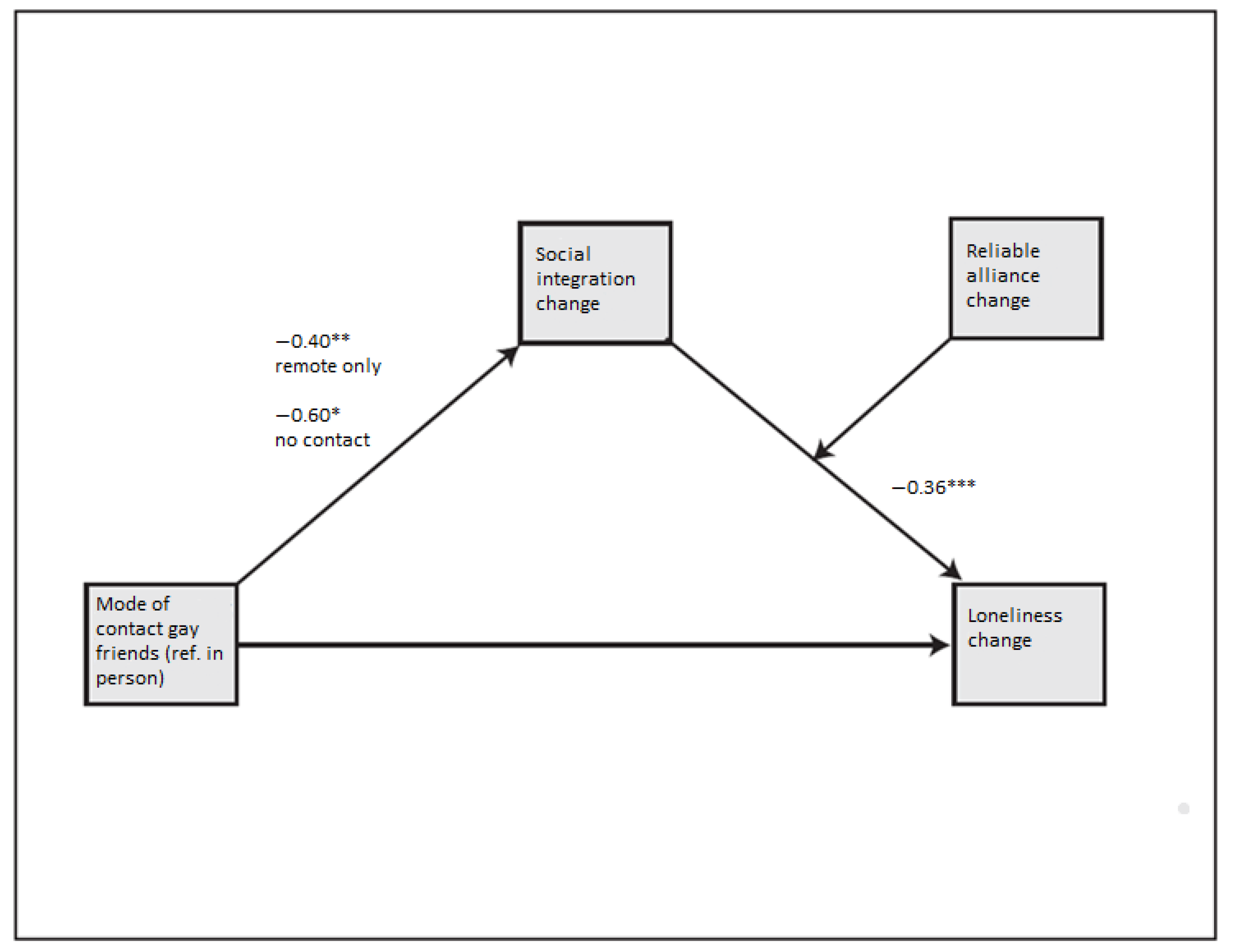
3.1. Social Integration
3.2. Reliable Aliance
3.3. Social Loneliness
4. Discussion
4.1. The Relationship between Remote Communication and Loneliness
4.2. Increase in Social Integration and Reliable Alliance in the Initial Stages of the Pandemic
4.3. Exacerbation Mechanisms of Loneliness in the Context of the Pandemic
4.4. The Danger of Loneliness that Has Passed: Network Shrinkage
4.5. The Pandemic and Other Types of Loneliness
4.6. Limitations
4.7. Public Health Implications
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Appendix A

{kind=link}
{kind=link}
{kind=link}
| Path | Mode of Communication | b | s.e. | LLCI | ULCI | ||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| Communication | to | Reliable Alliance | to | Loneliness | Remote only | −0.01 | 0.02 | −0.06 | 0.03 | ||
| No contact | −0.03 | 0.06 | −0.16 | 0.07 | |||||||
| Communication | to | Social Integration | to | Loneliness | Remote only | 0.11 | 0.05 | 0.03 | 0.21 | ||
| No contact | 0.11 | 0.07 | −0.01 | 0.26 | |||||||
| Communication | to | Reliable Alliance | to | Social Integration | to | Loneliness | Remote only | 0.04 | 0.03 | −0.01 | 0.09 |
| No contact | 0.10 | 0.05 | 0.00 | 0.22 | |||||||
| Communication to Social Integration to Loneliness | |||||
|---|---|---|---|---|---|
| Reliable Alliance | Effect | s.e. | LLCI | ULCI | |
| Remote only | 0.00 | 0.14 | 0.06 | 0.05 | 0.28 |
| Remote only | 2.00 | 0.14 | 0.06 | 0.04 | 0.28 |
| Index of moderated mediation | |||||
| Reliable Alliance | Index | s.e. | LLCI | ULCI | |
| 0.00 | 0.02 | −0.05 | 0.04 | ||
| Reliable Alliance | Effect | s.e. | LLCI | ULCI | |
| No contact | 0.00 | 0.21 | 0.10 | 0.04 | 0.45 |
| No contact | 2.00 | 0.21 | 0.10 | 0.04 | 0.43 |
| Index of moderated mediation | |||||
| Reliable Alliance | Index | s.e. | LLCI | ULCI | |
| 0.00 | 0.03 | −0.08 | 0.06 | ||
References
- Miller, E.D. Loneliness in the Era of COVID-19. Front. Psychol. 2020, 11, 2219. [Google Scholar] [CrossRef] [PubMed]
- Gorczynski, P.; Fasoli, F. Loneliness in sexual minority and heterosexual individuals: A comparative meta-analysis. J. Gay Lesbian Ment. Health 2021, 1–18. [Google Scholar] [CrossRef]
- Buecker, S.; Horstmann, K.T.; Krasko, J.; Kritzler, S.; Terwiel, S.; Kaiser, T.; Luhmann, M. Changes in daily loneliness for German residents during the first four weeks of the COVID-19 pandemic. Soc. Sci. Med. 2020, 265, 113541. [Google Scholar] [CrossRef] [PubMed]
- Bu, F.; Steptoe, A.; Fancourt, D. Loneliness during a strict lockdown: Trajectories and predictors during the COVID-19 pandemic in 38,217 United Kingdom adults. Soc. Sci. Med. 2020, 265, 113521. [Google Scholar] [CrossRef]
- Killgore, W.D.S.; Cloonan, S.A.; Taylor, E.C.; Lucas, D.A.; Dailey, N.S. Loneliness during the first half-year of COVID-19 Lockdowns. Psychiatry Res. 2020, 294, 113551. [Google Scholar] [CrossRef] [PubMed]
- van Tilburg, T.G.; Steinmetz, S.; Stolte, E.; van der Roest, H.; de Vries, D.H. Loneliness and Mental Health During the COVID-19 Pandemic: A Study Among Dutch Older Adults. J. Gerontol. B Psychol. Sci. Soc. Sci. 2021, 76, e249–e255. [Google Scholar] [CrossRef]
- Kneale, D.; Becares, L. The mental health and experiences of discrimination of LGBTQ+ people during the COVID-19 pandemic: Initial findings from the Queerantine study. MedRxiv 2020. [Google Scholar] [CrossRef]
- Peterson, Z.; Vaughan, E.; Carver, D. Sexual identity and psychological reactions to COVID-19. Traumatology 2020. advance online publication. [Google Scholar]
- Drabble, L.A.; Eliason, M.J. Introduction to Special Issue: Impacts of the COVID-19 Pandemic on LGBTQ+ Health and Well-Being. J. Homosex. 2021, 68, 545–559. [Google Scholar] [CrossRef]
- Groarke, J.M.; Berry, E.; Graham-Wisener, L.; McKenna-Plumley, P.E.; McGlinchey, E.; Armour, C. Loneliness in the UK during the COVID-19 pandemic: Cross-sectional results from the COVID-19 Psychological Wellbeing Study. PLoS ONE 2020, 15, e0239698. [Google Scholar] [CrossRef]
- Fokkema, T.; Kuyper, L. The relation between social embeddedness and loneliness among older lesbian, gay, and bisexual adults in the Netherlands. Arch. Sex Behav. 2009, 38, 264–275. [Google Scholar] [CrossRef]
- Kuyper, L.; Fokkema, T. Loneliness among older lesbian, gay, and bisexual adults: The role of minority stress. Arch. Sex Behav. 2010, 39, 1171–1180. [Google Scholar] [CrossRef] [PubMed]
- Hubach, R.D.; DiStefano, A.S.; Wood, M.M. Understanding the influence of loneliness on HIV risk behavior in young men who have sex with men. J. Gay Lesbian Soc. Serv. 2012, 24, 371–395. [Google Scholar] [CrossRef]
- Martin, J.I.; D’Augelli, A.R. How lonely are gay and lesbian youth? Psychol. Rep. 2003, 93, 486. [Google Scholar] [CrossRef]
- Wang, J.; Mann, F.; Lloyd-Evans, B.; Ma, R.; Johnson, S. Associations between loneliness and perceived social support and outcomes of mental health problems: A systematic review. BMC Psychiatry 2018, 18, 156. [Google Scholar] [CrossRef] [Green Version]
- McConnell, E.A.; Birkett, M.A.; Mustanski, B. Typologies of Social Support and Associations with Mental Health Outcomes among LGBT Youth. LGBT Health 2015, 2, 55–61. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Davis, T.S.; Saltzburg, S.; Locke, C.R. Assessing community needs of sexual minority youths: Modeling concept mapping for service planning. J. Gay Lesbian Soc. Serv. 2010, 22, 226–249. [Google Scholar] [CrossRef]
- Steinke, J.; Root-Bowman, M.; Estabrook, S.; Levine, D.S.; Kantor, L.M. Meeting the Needs of Sexual and Gender Minority Youth: Formative Research on Potential Digital Health Interventions. J. Adolesc. Health 2017, 60, 541–548. [Google Scholar] [CrossRef] [Green Version]
- Meyer, I.H. Prejudice, social stress, and mental health in lesbian, gay, and bisexual populations: Conceptual issues and research evidence. Psychol. Bull. 2003, 129, 674–697. [Google Scholar] [CrossRef]
- Pai, N.; Vella, S.L. COVID-19 and loneliness: A rapid systematic review. Aust. N. Z. J. Psychiatry 2021, 55, 1144–1156. [Google Scholar] [CrossRef]
- Kovacs, B.; Caplan, N.; Grob, S.; King, M. Social Networks and Loneliness during the COVID-19 Pandemic. Socius Sociol. Res. A Dyn. World 2021, 7, 2378023120985254. [Google Scholar] [CrossRef]
- Ohme, J.; Vanden Abeele, M.M.; Van Gaeveren, K.; Durnez, W.; De Marez, L. Staying informed and bridging “social distance”: Smartphone news use and mobile messaging behaviors of flemish adults during the first weeks of the COVID-19 pandemic. Socius 2020, 6, 2378023120950190. [Google Scholar] [CrossRef] [PubMed]
- Krendl, A.C.; Perry, B.L. The Impact of Sheltering in Place during the COVID-19 Pandemic on Older Adults’ Social and Mental Well-Being. J. Gerontol. B Psychol. Sci. Soc. Sci. 2021, 76, e53–e58. [Google Scholar] [CrossRef] [PubMed]
- Van Damme, W.; Dahake, R.; Delamou, A.; Ingelbeen, B.; Wouters, E.; Vanham, G.; Van De Pas, R.; Dossou, J.-P.; Ir, P.; Abimbola, S. The COVID-19 pandemic: Diverse contexts; different epidemics—how and why? BMJ Glob. Health 2020, 5, e003098. [Google Scholar] [CrossRef] [PubMed]
- Belgisch Staatsblad. 2020. Available online: https://economie.fgov.be/sites/default/files/Files/Entreprises/AM-MB-20200318-covid-19.pdf (accessed on 6 March 2022).
- Unia. COVID-19: Een Test Voor Mensenrechten; Unia: Kingston, Jamaica, 2020. [Google Scholar]
- Carr, M.; Schellenbach, C. Reflective monitoring in lonely adolescents. Adolescence 1993, 28, 737–747. [Google Scholar]
- Austin, A.G. Becoming immune to loneliness helping the elderly fill a void. J. Gerontol. Nurs. 1989, 15, 25–28. [Google Scholar] [CrossRef] [PubMed]
- Francis, G.M. Loneliness: Measuring the abstract. Int. J. Nurs. Stud. 1976, 13, 153–160. [Google Scholar] [CrossRef]
- Weiss, R.S. Loneliness: The Experience of Emotional and Social Isolation; The MIT Press: Cambridge, MA, USA, 1973. [Google Scholar]
- Russell, D.; Cutrona, C.E.; Rose, J.; Yurko, K. Social and emotional loneliness: An examination of Weiss’s typology of loneliness. J. Personal. Soc. Psychol. 1984, 46, 1313–1321. [Google Scholar] [CrossRef]
- Weinberg, R.B.; Marlowe, H.A., Jr. Recognizing the social in psychosocial competence: The importance of social network interventions. Psychosoc. Rehabil. J. 1983, 6, 25. [Google Scholar] [CrossRef]
- Litwin, H.; Levinsky, M. Social networks and mental health change in older adults after the COVID-19 outbreak. Aging Ment Health 2021, 26, 925–931. [Google Scholar] [CrossRef]
- Jen, S.; Stewart, D.; Woody, I. Serving LGBTQ+/SGL Elders during the Novel Corona Virus (COVID-19) Pandemic: Striving for Justice, Recognizing Resilience. J. Gerontol. Soc. Work 2020, 63, 607–610. [Google Scholar] [CrossRef]
- Weiss, R. The Provision of Social Relationships; Rubin, Z., Ed.; Prentice Hall: Hoboken, NJ, USA, 1974; pp. 17–26. [Google Scholar]
- Di Tommaso, E.; Spinner, B. Social and emotional loneliness: A re-examination of Weiss’ typology of loneliness. Personal. Individ. Differ. 1997, 22, 417–427. [Google Scholar] [CrossRef]
- Kraus, L.A.; Bazzini, D.; Davis, M.H.; Church, M.; Kirchman, C.M. Personal and Social Influences on Loneliness—The Mediating Effect of Social Provisions. Soc. Psychol. Q. 1993, 56, 37–53. [Google Scholar] [CrossRef]
- Vaux, A. Social and Emotional Loneliness—The Role of Social and Personal Characteristics. Personal. Soc. Psychol. Bull. 1988, 14, 722–734. [Google Scholar] [CrossRef]
- Spinner, B.; Byers, E. Loneliness and social support in married and unmarried individuals. In Proceedings of the Annual Convention of the Canadian Psychological Association, Toronto, ON, Canada, 20 June 1986. [Google Scholar]
- Tiikkainen, P.; Heikkinen, R.L. Associations between loneliness, depressive symptoms and perceived togetherness in older people. Aging Ment. Health 2005, 9, 526–534. [Google Scholar] [CrossRef]
- Niu, S.; Bartolome, A.; Mai, C.; Ha, N.B. # StayHome# WithMe: How Do YouTubers Help with COVID-19 Loneliness? In Proceedings of the 2021 CHI Conference on Human Factors in Computing Systems, Yokohama, Japan, 8–13 May 2021; pp. 1–15. [Google Scholar]
- Omoto, A.M.; Snyder, M. Considerations of community—The context and process of volunteerism. Am. Behav. Sci. 2002, 45, 846–867. [Google Scholar] [CrossRef]
- Camargo, E.L.S.; de Oliveira, B.I.A.; Siffoni, I.F.; de Sousa, A.R.; Teixeira, J.R.B.; Mendes, I.A.C.; de Sousa, A.F.L. Low Psychological Well-Being Among Men Who Have Sex with Men (MSM) During the Shelter-In-Place Orders to Prevent The COVID-19 Spread: Results From A Nationwide Study. MedRxiv 2020. [Google Scholar] [CrossRef]
- Reyniers, T.; Rotsaert, A.; Thunissen, E.; Buffel, V.; Masquillier, C.; Van Landeghem, E.; Vanhamel, J.; Nöstlinger, C.; Wouters, E.; Laga, M. Reduced sexual contacts with non-steady partners and less PrEP use among MSM in Belgium during the first weeks of the COVID-19 lockdown: Results of an online survey. Sex. Transm. Infect. 2021, 97, 414–419. [Google Scholar] [CrossRef]
- Salerno, J.P.; Williams, N.D.; Gattamorta, K.A. LGBTQ populations: Psychologically vulnerable communities in the COVID-19 pandemic. Psychol. Trauma 2020, 12, S239–S242. [Google Scholar] [CrossRef]
- Lee, H.; Miller, V.J. The Disproportionate Impact of COVID-19 on Minority Groups: A Social Justice Concern. J. Gerontol. Soc. Work 2020, 63, 580–584. [Google Scholar] [CrossRef]
- Gibb, J.K.; DuBois, L.Z.; Williams, S.; McKerracher, L.; Juster, R.P.; Fields, J. Sexual and gender minority health vulnerabilities during the COVID-19 health crisis. Am. J. Hum. Biol. 2020, 32, e23499. [Google Scholar] [CrossRef]
- Kline, N.S. Rethinking COVID-19 Vulnerability: A Call for LGTBQ+ Im/migrant Health Equity in the United States During and After a Pandemic. Health Equity 2020, 4, 239–242. [Google Scholar] [CrossRef] [PubMed]
- Signorelli, M.; Moretti-Pires, R.O.; de Oliveira, D.C.; Miskolci, R.; Polidoro, M.; Pereira, P.P.G. The health of LGBTI+ people and the COVID-19 pandemic: A call for visibility and health responses in Latin America. Sexualities 2020, 24, 979–983. [Google Scholar] [CrossRef]
- Brennan, D.J.; Card, K.G.; Collict, D.; Jollimore, J.; Lachowsky, N.J. How Might Social Distancing Impact Gay, Bisexual, Queer, Trans and Two-Spirit Men in Canada? AIDS Behav. 2020, 24, 2480–2482. [Google Scholar] [CrossRef] [PubMed]
- Lakens, D. Sample Size Justification. arXiv 2021. [Google Scholar] [CrossRef]
- MacKenzie, S.B.; Lee, J.Y.; Podsakoff, N.P. Common method biases in behavioral research: A critical review of the literature and recommended remedies. J. Appl. Psychol. 2003, 88, 879. [Google Scholar]
- McCrae, R.R.; Kurtz, J.E.; Yamagata, S.; Terracciano, A. Internal consistency, retest reliability, and their implications for personality scale validity. Personal. Soc. Psychol. Rev. 2011, 15, 28–50. [Google Scholar] [CrossRef]
- Mund, M.; Maes, M.; Drewke, P.M.; Gutzeit, A.; Jaki, I.; Qualter, P. Would the Real Loneliness Please Stand Up? The Validity of Loneliness Scores and the Reliability of Single-Item Scores. Assessment 2022. Pre-publication. [Google Scholar] [CrossRef]
- Alsubheen, S.A.; Oliveira, A.; Habash, R.; Goldstein, R.; Brooks, D. Systematic review of psychometric properties and cross-cultural adaptation of the University of California and Los Angeles loneliness scale in adults. Curr. Psychol. 2021, 1–15. [Google Scholar] [CrossRef]
- Hughes, M.E.; Waite, L.J.; Hawkley, L.C.; Cacioppo, J.T. A Short Scale for Measuring Loneliness in Large Surveys: Results from Two Population-Based Studies. Res. Aging 2004, 26, 655–672. [Google Scholar] [CrossRef]
- Das, A.; Padala, K.P.; Crawford, C.G.; Teo, A.; Mendez, D.M.; Phillips, O.A.; Wright, B.C.; House, S.; Padala, P.R. A systematic review of loneliness and social isolation scales used in epidemics and pandemics. Psychiatry Res. 2021, 306, 114217. [Google Scholar] [CrossRef]
- Blome, C.; Augustin, M. Measuring Change in Quality of Life: Bias in Prospective and Retrospective Evaluation. Value Health 2015, 18, 110–115. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bu, F.; Steptoe, A.; Fancourt, D. Who is lonely in lockdown? Cross-cohort analyses of predictors of loneliness before and during the COVID-19 pandemic. Public. Health 2020, 186, 31–34. [Google Scholar] [CrossRef] [PubMed]
- Liu, S.; Haucke, M.N.; Heinzel, S.; Heinz, A. Long-term impact of economic downturn and loneliness on psychological distress: Triple crises of COVID-19 pandemic. J. Clin. Med. 2021, 10, 4596. [Google Scholar] [CrossRef] [PubMed]
- Andersson, L. Loneliness research and interventions: A review of the literature. Aging Ment. Health 2010, 2, 264–274. [Google Scholar] [CrossRef]
- Hayes, A.F. Introduction to Mediation, Moderation, and Conditional Process Analysis: A Regression-Based Approach; Guilford Publications: New York, NY, USA, 2017. [Google Scholar]
- Weatherburn, P.; Hickson, F.; Reid, D.S.; Marcus, U.; Schmidt, A.J. European Men-who-have-sex-with-men Internet Survey (EMIS-2017): Design and methods. Sex. Res. Soc. Policy 2020, 17, 543–557. [Google Scholar] [CrossRef] [Green Version]
- Grant, R.; Gorman-Murray, A.; Briohny Walker, B. The Spatial Impacts of COVID-19 Restrictions on LGBTIQ Wellbeing, Visibility, and Belonging in Tasmania, Australia. J. Homosex. 2021, 68, 647–662. [Google Scholar] [CrossRef]
- Ellis, W.E.; Dumas, T.M.; Forbes, L.M. Physically isolated but socially connected: Psychological adjustment and stress among adolescents during the initial COVID-19 crisis. Can. J. Behav. Sci. Rev. Can. Des Sci. Du Comport. 2020, 52, 177–187. [Google Scholar] [CrossRef]
- Lau, J.T.F.; Yang, X.; Tsui, H.Y.; Pang, E.; Wing, Y.K. Positive mental health-related impacts of the SARS epidemic on the general public in Hong Kong and their associations with other negative impacts. J. Infect. 2006, 53, 114–124. [Google Scholar] [CrossRef]
- de Jong Gierveld, J.; Van Tilburg, T.; Dykstra, P.A. Loneliness and social isolation. In Cambridge Handbook of Personal Relationships; Cambridge University Press: Cambridge, UK, 2006; pp. 485–500. [Google Scholar]
- Cacioppo, J.T.; Fowler, J.H.; Christakis, N.A. Alone in the crowd: The structure and spread of loneliness in a large social network. J. Pers. Soc. Psychol. 2009, 97, 977–991. [Google Scholar] [CrossRef] [Green Version]
- Roberts, S.G.B.; Dunbar, R.I.M. Communication in social networks: Effects of kinship, network size, and emotional closeness. Pers. Relatsh. 2011, 18, 439–452. [Google Scholar] [CrossRef]
| Item | Mean | Frequency | |||||
|---|---|---|---|---|---|---|---|
| Statistic | Std. Error | Std. Deviation | Variance | ‘This Is Less the Case’ (Score = −1) | ‘This Is the Same’ (Score = 0) | ‘This Is More the Case’ (Score = 1) | |
| There are people who enjoy the same social activities as I do | 2.16 | 0.03 | 0.58 | 0.33 | 46 | 296 | 119 |
| I feel part of a group of people who share my attitudes and beliefs | 2.05 | 0.02 | 0.47 | 0.22 | 40 | 358 | 63 |
| There is no one who shares my interests and concerns | 2.10 | 0.03 | 0.55 | 0.30 | 49 | 318 | 94 |
| There is no one who likes to do the things I do | 2.16 | 0.02 | 0.49 | 0.24 | 24 | 339 | 98 |
| Item | Mean | Frequency | |||||
|---|---|---|---|---|---|---|---|
| Statistic | Std. Error | Std. Deviation | Variance | ‘This Is Less the Case’ (Score = −1) | ‘This Is the Same’ (Score = 0) | ‘This Is More the Case’ (Score = 1) | |
| There are people I can count on in an emergency | 2.10 | 0.02 | 0.47 | 0.22 | 31 | 354 | 76 |
| There is no one I can depend on for aid if I really need it | 2.23 | 2.23 | 0.53 | 0.28 | 25 | 307 | 129 |
| If something went wrong no one would help me | 2.26 | 2.26 | 0.56 | 0.32 | 29 | 283 | 149 |
| There are people I can depend on to help me if I really need it | - | - | - | - | - | - | - |
| Item | Mean | Frequency | ||||||
|---|---|---|---|---|---|---|---|---|
| Statistic | Std. Error | Std. Deviation | Variance | ‘Never to Not at All’ (Score = 0) | ‘Some Days’ (Score = 1) | ‘More than Half of the Days’ (score = 2) | ‘Almost All Days’ (Score = 3) | |
| How often do you feel that you lack companionship? | 1.80 | 0.03 | 0.74 | 0.54 | 162 | 250 | 30 | 19 |
| How often do you feel left out? | 1.46 | 0.03 | 0.68 | 0.46 | 289 | 144 | 18 | 10 |
| How often do you feel isolated from others? | 1.58 | 0.04 | 0.77 | 0.60 | 255 | 164 | 23 | 19 |
| Item | Mean | Frequency | ||||||
|---|---|---|---|---|---|---|---|---|
| Statistic | Std. Error | Std. Deviation | Variance | ‘Never to not at All’ (Score = 0) | ‘Some Days’ (Score = 1) | ‘More than Half of the Days’ (Score = 2) | ‘Almost All Days’ (Score = 3) | |
| How often do you feel that you lack companionship? | 2.55 | 0.04 | 0.94 | 0.90 | 54 | 197 | 114 | 96 |
| How often do you feel left out? | 1.65 | 0.04 | 0.86 | 0.73 | 256 | 136 | 45 | 24 |
| How often do you feel isolated from others? | 2.41 | 0.05 | 1.00 | 1.00 | 88 | 182 | 104 | 87 |
| Model 1a | Model 1b | |||
|---|---|---|---|---|
| b | s.e. | b | s.e. | |
| Age 18–35 (vs. 36+) | −0.07 | 0.13 | −0.10 | 0.13 |
| Economic hardship (ref. no economic hardship) | 0.07 | 0.30 | 0.07 | 0.29 |
| Gay friends, remote only (ref. in person) | −0.58 *** | 0.16 | −0.11 | 0.25 |
| Gay friends, no communication (ref. in person) | −0.25 | 0.31 | 0.00 | 0.47 |
| Heterosexual friends, remote only (ref. in person) | 0.24 | 0.17 | 0.17 | 0.18 |
| Heterosexual friends, no communication (ref. in person) | −0.49 | 0.27 | −0.43 | 0.27 |
| Family, remote only (ref. in person) | 0.03 | 0.14 | 0.46 * | 0.21 |
| Family, no communication (ref. in person) | 0.14 | 0.28 | 0.03 | 0.40 |
| Gay friends, remote only × family, remote only (ref. in person) | −0.73 ** | 0.28 | ||
| Gay friends, remote only × family, no communication (ref. in person) | 0.50 | 0.76 | ||
| Gay friends, no communication × family, remote only (ref. in person) | −0.83 | 0.73 | ||
| Gay friends, no communication × family, no communication (ref. in person) | 0.01 | 0.64 | ||
| Model 1a | Model 1b | |||
|---|---|---|---|---|
| b | s.e. | b | s.e. | |
| Age 18–35 (ref. 36+) | 0.16 | 0.12 | 0.16 | 0.13 |
| Economic hardship (ref. no economic hardship) | 0.12 | 0.28 | 0.10 | 0.28 |
| Gay friends, remote only (ref. in person) | −0.44 ** | 0.15 | −0.49 * | 0.24 |
| Gay friends, no communication (ref. in person) | −0.22 | 0.30 | −0.34 | 0.45 |
| Heterosexual friends, remote only (ref. in person) | 0.41 * | 0.17 | 0.41 * | 0.17 |
| Heterosexual friends, no communication (ref. in person) | −0.14 | 0.26 | −0.11 | 0.26 |
| Family, remote only (ref. in person) | −0.05 | 0.13 | −0.07 | 0.20 |
| Family, no communication (ref. in person) | −0.20 | 0.26 | −0.43 | 0.39 |
| Gay friends, remote only × family, remote only (ref. in person) | 0.06 | 0.27 | ||
| Gay friends, remote only × family, no communication (ref. in person) | 0.29 | 0.73 | ||
| Gay friends, no communication × family, remote only (ref. in person) | −0.17 | 0.70 | ||
| Gay friends, no communication × family, no communication (ref. in person) | 0.39 | 0.61 | ||
| Model 2a | Model 2b | |||
|---|---|---|---|---|
| b | s.e. | b | s.e. | |
| Age 18–35 (ref. 36+) | 0.28 | 0.20 | 0.30 | 0.20 |
| Economic hardship (ref. no economic hardship) | 0.47 | 0.46 | 0.45 | 0.46 |
| Gay friends, remote only (ref. in person) | −0.31 | 0.25 | −0.25 | 0.39 |
| Gay friends, no communication (ref. in person) | −0.35 | 0.48 | −0.89 | 0.73 |
| Heterosexual friends, remote only (ref. in person) | 0.24 | 0.27 | 0.24 | 0.27 |
| Heterosexual friends, no communication (ref. in person) | −0.19 | 0.42 | −0.29 | 0.42 |
| Family, remote only (ref. in person) | −0.14 | 0.22 | −0.21 | 0.33 |
| Family, no communication (ref. in person) | −0.01 | 0.43 | 0.32 | 0.63 |
| Reliable alliance | 0.03 | 0.09 | 0.03 | 0.09 |
| Social integration | −0.34 *** | 0.09 | −0.33 *** | 0.09 |
| Gay friends, remote only × family, remote only (ref. in person) | 0.00 | 0.44 | ||
| Gay friends, remote only × family, no communication (ref. in person) | −1.68 | 1.18 | ||
| Gay friends, no communication × family, remote only (ref. in person) | 1.42 | 1.14 | ||
| Gay friends, no communication × family, no communication (ref. in person) | 0.35 | 0.99 | ||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Thunnissen, E.; Buffel, V.; Reyniers, T.; Nöstlinger, C.; Wouters, E. From Physical Distancing to Social Loneliness among Gay Men and Other Men Having Sex with Men in Belgium: Examining the Disruption of the Social Network and Social Support Structures. Int. J. Environ. Res. Public Health 2022, 19, 6873. https://doi.org/10.3390/ijerph19116873
Thunnissen E, Buffel V, Reyniers T, Nöstlinger C, Wouters E. From Physical Distancing to Social Loneliness among Gay Men and Other Men Having Sex with Men in Belgium: Examining the Disruption of the Social Network and Social Support Structures. International Journal of Environmental Research and Public Health. 2022; 19(11):6873. https://doi.org/10.3390/ijerph19116873
Chicago/Turabian StyleThunnissen, Estrelle, Veerle Buffel, Thijs Reyniers, Christiana Nöstlinger, and Edwin Wouters. 2022. "From Physical Distancing to Social Loneliness among Gay Men and Other Men Having Sex with Men in Belgium: Examining the Disruption of the Social Network and Social Support Structures" International Journal of Environmental Research and Public Health 19, no. 11: 6873. https://doi.org/10.3390/ijerph19116873
APA StyleThunnissen, E., Buffel, V., Reyniers, T., Nöstlinger, C., & Wouters, E. (2022). From Physical Distancing to Social Loneliness among Gay Men and Other Men Having Sex with Men in Belgium: Examining the Disruption of the Social Network and Social Support Structures. International Journal of Environmental Research and Public Health, 19(11), 6873. https://doi.org/10.3390/ijerph19116873