
Attitude and Level of COVID-19 Vaccination among Women in Reproductive Age during the Fourth Pandemic Wave: A Cross-Sectional Study in Poland


Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Questionnaire Development
2.3. Data Source and Study Population
2.4. Data
2.4.1. Sociodemographic Data
2.4.2. Obstetric Data
2.4.3. Assessment of Women’s Knowledge Level concerning COVID-19 Vaccination
2.4.4. Women’s Knowledge and Attitude concerning SARS-CoV-2 Infections and COVID Vaccination
2.4.5. COVID-19 Vaccine Preference and Attitude
2.5. Statistical Analysis
3. Results
3.1. Sociodemographic and Obstetric Data
3.2. Sociodemographic and Obstetric Data in Relation to COVID-19 Vaccination
3.3. Women’s Knowledge concerning COVID-19 Vaccination
3.4. Women’s Knowledge concerning COVID-19 Vaccination in Relation to Sociodemographic and Obstetric Variables
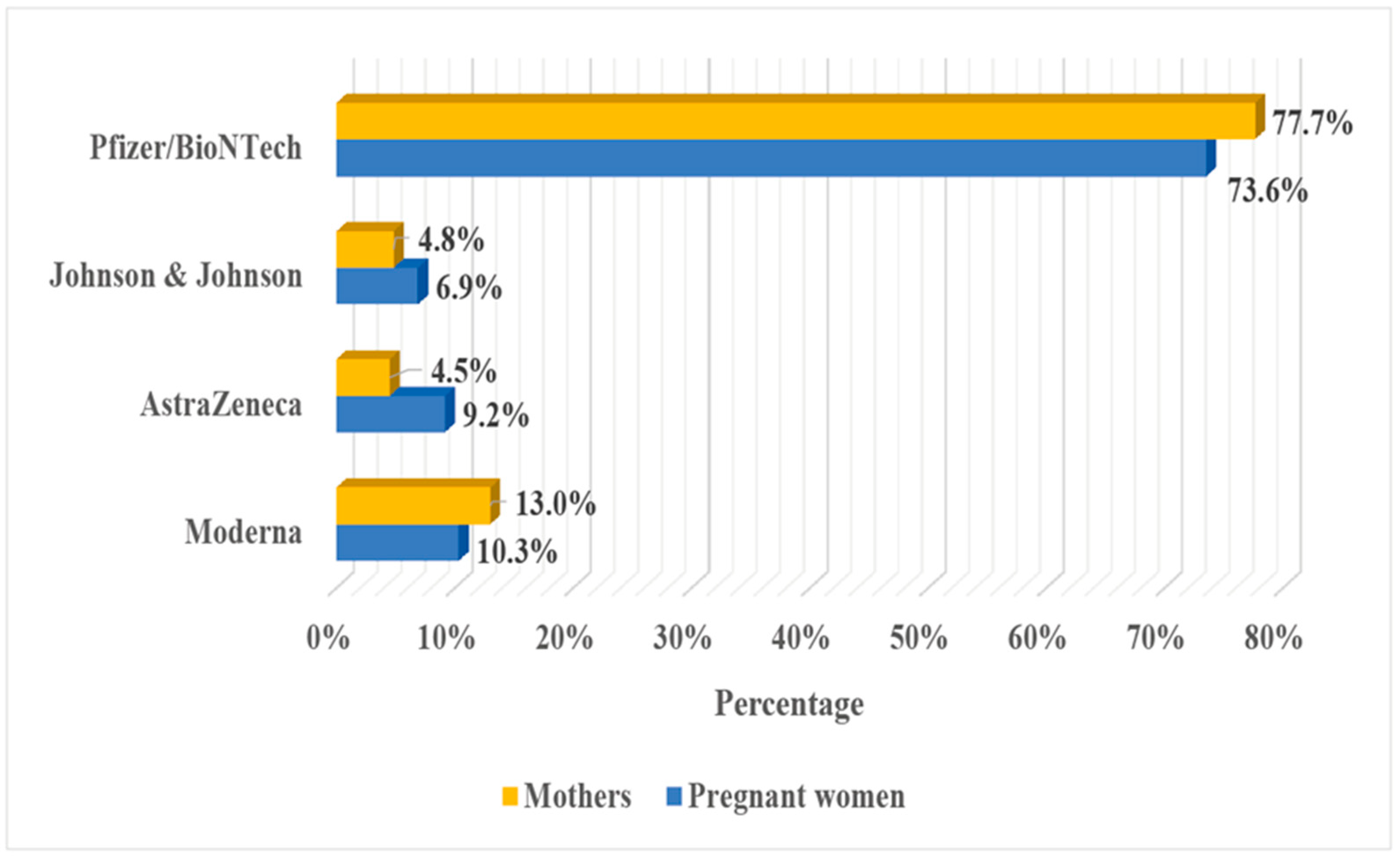
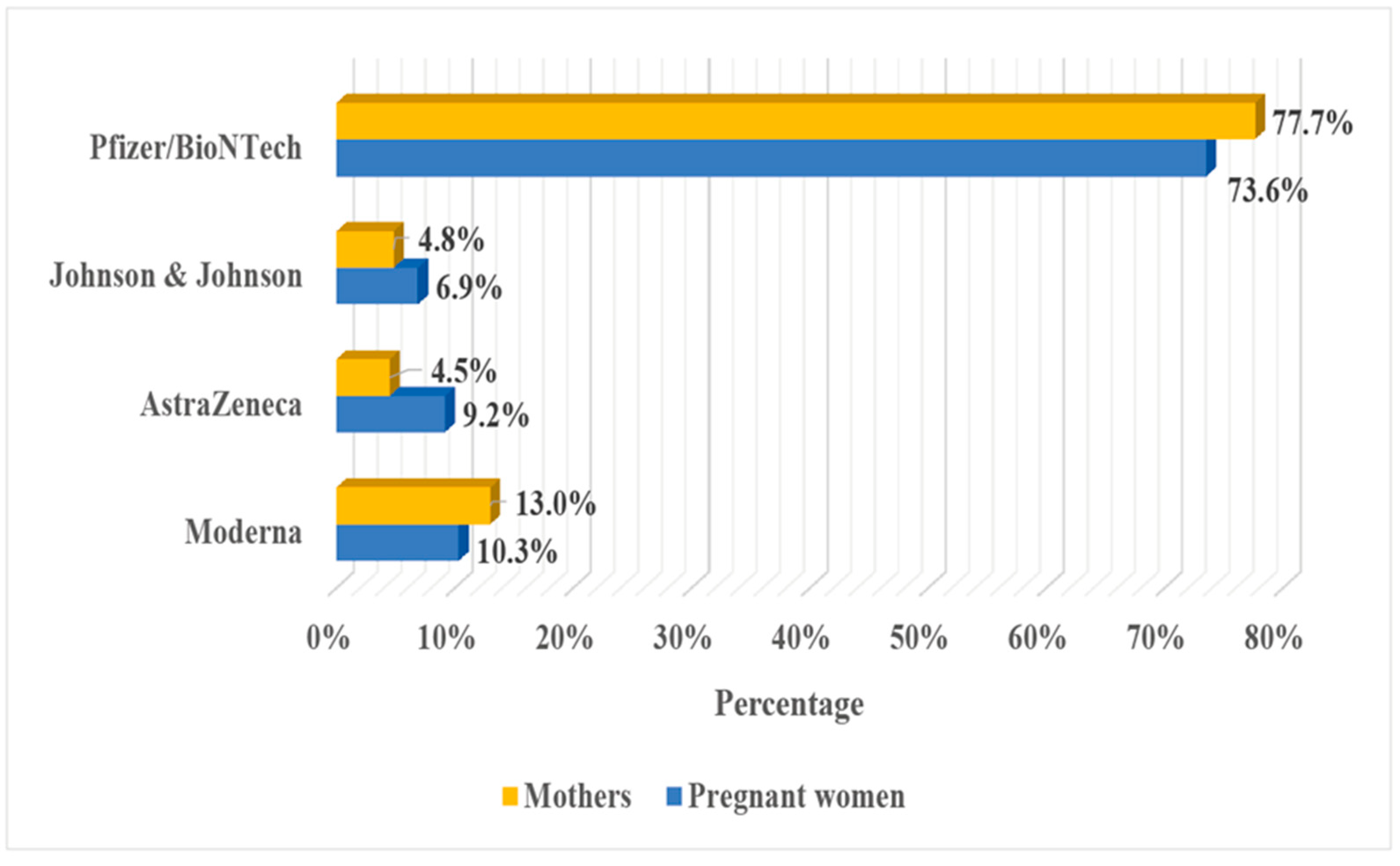
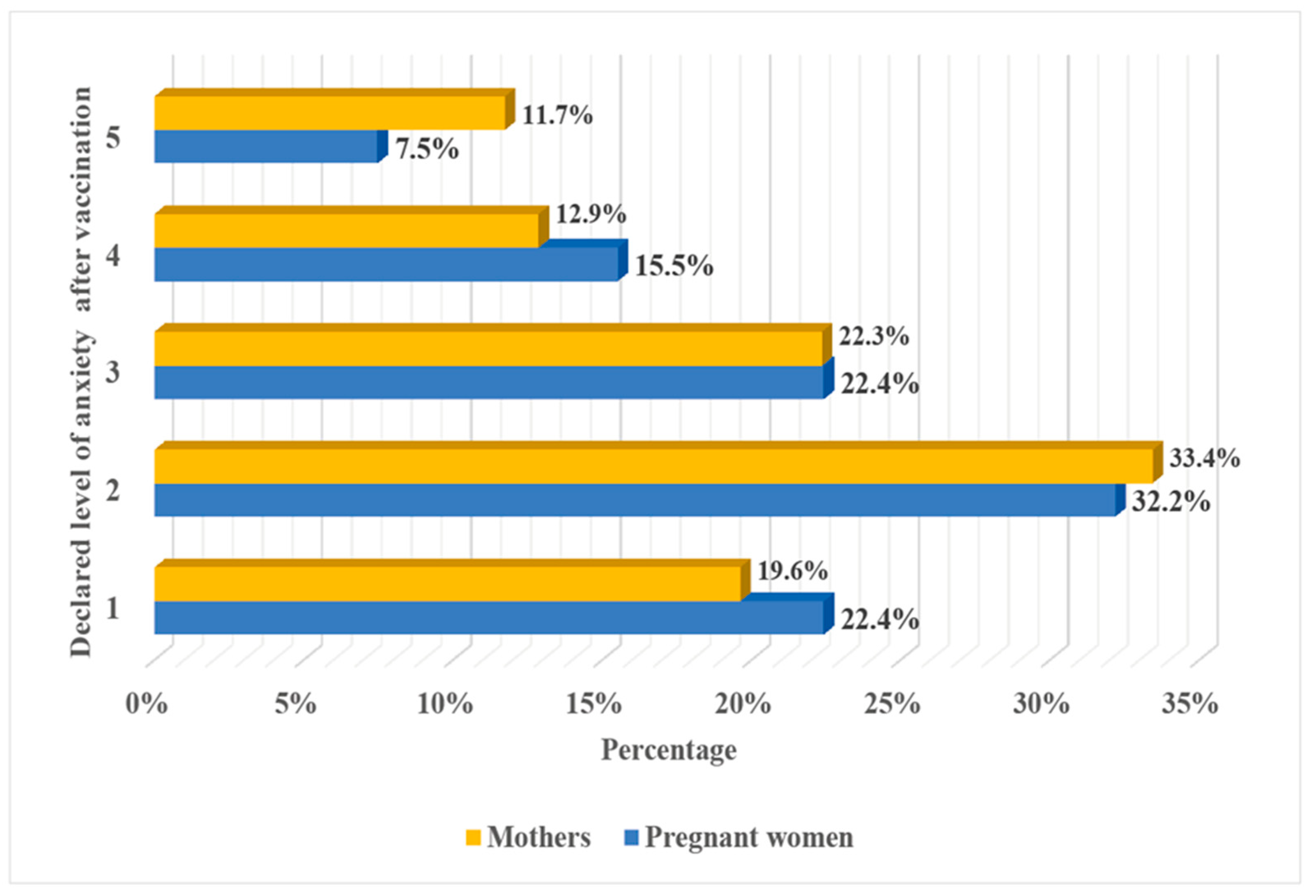
3.5. COVID-19 Vaccine Preference and Attitude
3.6. Respondents’ Reasons for COVID-19 Vaccination
3.7. Respondents’ Reasons to Avoid COVID-19 Vaccination
3.8. Predictors of a Lack of COVID-19 Vaccination among Women
4. Discussion
Strengths and Limitations of Our Study
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Muralidar, S.; Ambi, S.V.; Sekaran, S.; Krishnan, U.M. The emergence of COVID-19 as a global pandemic: Understanding the epidemiology, immune response and potential therapeutic targets of SARS-CoV-2. Biochimie 2020, 179, 85–100. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization (WHO). Coronavirus Disease (COVID-19) Pandemic. Available online: https://www.who.int/emergencies/diseases/novel-coronavirus-2019 (accessed on 17 February 2022).
- Pradhan, A.; Olsson, P.-E. Sex differences in severity and mortality from COVID-19: Are males more vulnerable? Biol. Sex Differ. 2020, 11, 53. [Google Scholar] [CrossRef] [PubMed]
- Wang, M.; Jiang, N.; Li, C.; Wang, J.; Yang, H.; Liu, L.; Tan, X.; Chen, Z.; Gong, Y.; Yin, X.; et al. Sex-disaggregated data on clinical characteristics and outcomes of hospitalized patients with COVID-19: A retrospective study. Front. Cell. Infect. Microbiol. 2021, 11, 680422. [Google Scholar] [CrossRef]
- Kotlar, B.; Gerson, E.; Petrillo, S.; Langer, A.; Tiemeier, H. The impact of the COVID-19 pandemic on maternal and perinatal health: A scoping review. Reprod. Health 2021, 18, 10. [Google Scholar] [CrossRef] [PubMed]
- Saadaoui, M.; Kumar, M.; Al Khodor, S. COVID-19 infection during pregnancy: Risk of vertical transmission, fetal, and neonatal outcomes. J. Pers. Med. 2021, 11, 483. [Google Scholar] [CrossRef] [PubMed]
- Rzymski, P.; Zeyland, J.; Poniedziałek, B.; Małecka, I.; Wysocki, J. The perception and attitudes toward COVID-19 vaccines: A cross-sectional study in Poland. Vaccines 2021, 9, 382. [Google Scholar] [CrossRef]
- World Health Organization (WHO). Situation by Region, Country, Territory & Area. Available online: https://covid19.who.int/table (accessed on 17 February 2022).
- World Health Organization (WHO). The Pfizer BioNTech (BNT162b2) COVID-19 Vaccine: What You Need to Know. Available online: https://www.who.int/news-room/feature-stories/detail/who-can-take-the-pfizer-biontech-COVID-19--vaccine-what-you-need-to-know (accessed on 17 February 2022).
- Stanowisko Fundacji Bank Mleka Kobiecego, Centrum Nauki o Laktacji i Polskiego Towarzystwa Wakcynologii w Sprawie Szczepienia Przeciwko SARS-CoV-2 Kobiet w Okresie Laktacji. Available online: https://ptwakc.kylos.pl/wytyczne-i-stanowiska/stanowisko-fundacji-bank-mleka-kobiecego-centrum-nauki-o-laktacji-i-polskiego-towarzystwa-wakcynologii-w-sprawie-szczepienia-przeciwko-SARS-CoV-2-kobiet-w-okresie-laktacji/ (accessed on 17 February 2022).
- Stanowisko Polskiego Towarzystwa Neonatologicznego ws. Szczepień Przeciwko COVID-19. Available online: https://www.mp.pl/szczepienia/artykuly/wytyczne/256987,stanowisko-polskiego-towarzystwa-neonatologicznego-ws-szczepien-przeciwko-COVID-19 (accessed on 17 February 2022).
- Villar, J.; Ariff, S.; Gunier, R.B.; Thiruvengadam, R.; Rauch, S.; Kholin, A.; Roggero, P.; Prefumo, F.; do Vale, M.S.; Cardona-Perez, J.A.; et al. Maternal and neonatal morbidity and mortality among pregnant women with and without COVID-19 infection: The INTERCOVID multinational cohort study. JAMA Pediatr. 2021, 175, 817–826. [Google Scholar] [CrossRef]
- Allotey, J.; Stallings, E.; Bonet, M.; Yap, M.; Chatterjee, S.; Kew, T.; Debenham, L.; Llavall, A.C.; Dixit, A.; for PregCOV-19 Living Systematic Review Consortium; et al. Clinical manifestations, risk factors, and maternal and perinatal outcomes of coronavirus disease 2019 in pregnancy: Living systematic review and meta-analysis. BMJ 2020, 370, m3320. [Google Scholar] [CrossRef] [PubMed]
- Atyeo, C.; Pullen, K.M.; Bordt, E.A.; Fischinger, S.; Burke, J.; Michell, A.; Slein, M.D.; Loos, C.; Shook, L.L.; Boatin, A.A.; et al. Compromised SARS-CoV-2-specific placental antibody transfer. Cell 2021, 184, 628–642. [Google Scholar] [CrossRef] [PubMed]
- Goncu Ayhan, S.; Oluklu, D.; Atalay, A.; Menekse Beser, D.; Tanacan, A.; Moraloglu Tekin, O.; Sahin, D. COVID-19 vaccine acceptance in pregnant women. Int. J. Gynaecol. Obstet. 2021, 154, 291–296. [Google Scholar] [CrossRef]
- Abdelazim, I.A.; AbuFaza, M.; Al-Munaifi, S. COVID-19 positive woman presented with preterm labor: Case report. Gynecol. Obstet. Reprod. Med. 2021, 27, 294–296. [Google Scholar] [CrossRef]
- Martinez-Portilla, R.J.; Sotiriadis, A.; Chatzakis, C.; Torres-Torres, J.; Espino, Y.; Sosa, S.; Sandoval-Mandujano, K.; Castro-Bernabe, D.A.; Medina-Jimenez, V.; Monarrez-Martin, J.C.; et al. Pregnant women with SARS-CoV-2 infection are at higher risk of death and pneumonia: Propensity score matched analysis of a nationwide prospective cohort (COV19Mx). Ultrasound Obstet. Gynecol. 2021, 57, 224–231. [Google Scholar] [CrossRef] [PubMed]
- Vassilopoulou, E.; Feketea, G.; Koumbi, L.; Mesiari, C.; Berghea, E.C.; Konstantinou, G.N. Breastfeeding and COVID-19: From nutrition to immunity. Front. Immunol. 2021, 12, 661806. [Google Scholar] [CrossRef] [PubMed]
- Mor, G.; Cardenas, I. The immune system in pregnancy: A unique complexity. Am. J. Reprod. Immunol. 2010, 63, 425–433. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gonçalves, G.; Cutts, F.T.; Hills, M.; Rebelo-Andrade, H.; Trigo, F.A.; Barros, H. Transplacental transfer of measles and total IgG. Epidemiol. Infect. 1999, 122, 273–279. [Google Scholar] [CrossRef]
- Munoz, F.M.; Bond, N.H.; Maccato, M.; Pinell, P.; Hammill, H.A.; Swamy, G.K.; Walter, E.B.; Jackson, L.A.; Englund, J.A.; Edwards, M.S.; et al. Safety and immunogenicity of tetanus diphtheria and acellular pertussis (Tdap) immunization during pregnancy in mothers and infants: A randomized clinical trial. JAMA 2014, 311, 1760–1769. [Google Scholar] [CrossRef]
- Martinez, D.R.; Fong, Y.; Li, S.H.; Yang, F.; Jennewein, M.F.; Weiner, J.A.; Harrell, E.A.; Mangold, J.F.; Goswami, R.; Seage, G.R., 3rd; et al. Fc Characteristics mediate selective placental transfer of IgG in HIV-Infected women. Cell 2019, 178, 190–201.e11. [Google Scholar] [CrossRef] [PubMed]
- Beharier, O.; Plitman Mayo, R.; Raz, T.; Nahum Sacks, K.; Schreiber, L.; Suissa-Cohen, Y.; Chen, R.; Gomez-Tolub, R.; Hadar, E.; Gabbay-Benziv, R.; et al. Efficient maternal to neonatal transfer of antibodies against SARS-CoV-2 and BNT162b2 mRNA COVID-19 vaccine. J. Clin. Investig. 2021, 131, e154834. [Google Scholar] [CrossRef]
- Bäuerl, C.; Randazzo, W.; Sánchez, G.; Selma-Royo, M.; García Verdevio, E.; Martínez, L.; Parra-Llorca, A.; Lerin, C.; Fumadó, V.; Crovetto, F.; et al. MilkCORONA study team. SARS-CoV-2 RNA and antibody detection in breast milk from a prospective multicentre study in Spain. Arch. Dis. Child Fetal Neonatal Ed. 2022, 107, 216–221. [Google Scholar] [CrossRef] [PubMed]
- Juncker, H.G.; Romijn, M.; Loth, V.N.; Ruhé, E.J.M.; Bakker, S.; Kleinendorst, S.; de Groot, C.J.M.; Pajkrt, D.; Korosi, A.; van Goudoever, J.B.; et al. Antibodies against SARS-CoV-2 in human milk: Milk conversion rates in the Netherlands. J. Hum. Lact. 2021, 37, 469–476. [Google Scholar] [CrossRef]
- Perl, S.H.; Uzan-Yulzari, A.; Klainer, H.; Asiskovich, L.; Youngster, M.; Rinott, E.; Youngster, I. SARS-CoV-2-Specific antibodies in breast milk after COVID-19 vaccination of breastfeeding women. JAMA 2021, 325, 2013–2014. [Google Scholar] [CrossRef] [PubMed]
- Flannery, D.D.; Gouma, S.; Dhudasia, M.B.; Mukhopadhyay, S.; Pfeifer, M.R.; Woodford, E.C.; Triebwasser, J.E.; Gerber, J.S.; Morris, J.S.; Weirick, M.E.; et al. Assessment of maternal and neonatal cord blood SARS-CoV-2 antibodies and placental transfer ratios. JAMA Pediatr. 2021, 175, 594–600. [Google Scholar] [CrossRef]
- Shook, L.L.; Atyeo, C.G.; Yonker, L.M.; Fasano, A.; Gray, K.J.; Alter, G.; Edlow, A.G. Durability of anti-spike antibodies in infants after maternal COVID-19 vaccination or natural infection. JAMA 2022, 327, 1087–1089. [Google Scholar] [CrossRef]
- Demers-Mathieu, V.; Do, D.M.; Mathijssen, G.B.; Sela, D.A.; Seppo, A.; Järvinen, K.M.; Medo, E. Difference in levels of SARS-CoV-2 S1 and S2 subunits- and nucleocapsid protein-reactive SIgM/IgM, IgG and SIgA/IgA antibodies in human milk. J. Perinatol. 2021, 41, 850–859. [Google Scholar] [CrossRef]
- Pace, R.M.; Williams, J.E.; Järvinen, K.M.; Belfort, M.B.; Pace, C.D.; Lackey, K.A.; Gogel, A.C.; Nguyen-Contant, P.; Kanagaiah, P.; Fitzgerald, T.; et al. COVID-19 and human milk: SARS-CoV-2, antibodies, and neutralizing capacity. medRxiv 2020. [Google Scholar] [CrossRef]
- Kim, L.; Whitaker, M.; O’Halloran, A.; Kambhampati, A.; Chai, S.J.; Reingold, A.; Armistead, I.; Kawasaki, B.; Meek, J.; Yousey-Hindes, K.; et al. COVID-NET surveillance team. Hospitalization rates and characteristics of children aged <18 years hospitalized with laboratory-confirmed COVID-19-COVID-NET, 14 States, 1 March–25 July 2020. MMWR Morb. Mortal. Wkly. Rep. 2020, 69, 1081–1088. [Google Scholar] [CrossRef] [PubMed]
- Dong, L.; Tian, J.; He, S.; Zhu, C.; Wang, J.; Liu, C.; Yang, J. Possible vertical transmission of SARS-CoV-2 from an infected mother to her newborn. JAMA 2020, 323, 1846–1848. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hardelid, P.; Favarato, G.; Wijlaars, L.; Fenton, L.; McMenamin, J.; Clemens, T.; Dibben, C.; Milojevic, A.; Macfarlane, A.; Taylor, J.; et al. Risk of SARS-CoV-2 testing, PCR-confirmed infections and COVID-19-related hospital admissions in children and young people: Birth cohort study. medRxiv 2021. [Google Scholar] [CrossRef]
- Elsaddig, M.; Khalil, A. Effects of the COVID pandemic on pregnancy outcomes. Best Pract. Res. Clin. Obstet. Gynaecol. 2021, 73, 125–136. [Google Scholar] [CrossRef]
- Gurzenda, S.; Castro, M.C. COVID-19 poses alarming pregnancy and postpartum mortality risk in Brazil. EClinicalMedicine. 2021, 36, 100917. [Google Scholar] [CrossRef]
- World Health Organization (WHO). Maternal, Newborn, Child and Adolescent Health and Ageing. Available online: https://platform.who.int/data/maternal-newborn-child-adolescent-ageing/indicator-explorer-new/mca/number-of-births-(thousands) (accessed on 17 February 2022).
- World Health Organization (WHO). Body Mass Index. Available online: https://www.euro.who.int/en/health-topics/disease-prevention/nutrition/a-healthy-lifestyle/body-mass-index-bmi (accessed on 17 February 2022).
- Ramli, N.; Rahman, N.A.A.; Haque, M. Knowledge, attitude, and practice regarding osteoporosis among allied health sciences students in a public University in Malaysia. Erciyes Med. J. 2018, 40, 210–217. [Google Scholar] [CrossRef]
- Lis-Kuberka, J.; Orczyk-Pawiłowicz, M. Polish women have moderate knowledge of gestational diabetes mellitus and breastfeeding benefits. Int. J. Environ. Res. Public Health 2021, 18, 10409. [Google Scholar] [CrossRef] [PubMed]
- Stuckelberger, S.; Favre, G.; Ceulemans, M.; Nordeng, H.; Gerbier, E.; Lambelet, V.; Stojanov, M.; Winterfeld, U.; Baud, D.; Panchaud, A.; et al. SARS-CoV-2 vaccine willingness among pregnant and breastfeeding women during the first pandemic wave: A cross-sectional study in Switzerland. Viruses 2021, 13, 1199. [Google Scholar] [CrossRef]
- Carbone, L.; Mappa, I.; Sirico, A.; Di Girolamo, R.; Saccone, G.; Di Mascio, D.; Donadono, V.; Cuomo, L.; Gabrielli, O.; Migliorini, S.; et al. Pregnant women’s perspectives on severe acute respiratory syndrome coronavirus 2 vaccine. Am. J. Obstet. Gynecol. MFM 2021, 3, 100352. [Google Scholar] [CrossRef] [PubMed]
- Sutton, D.; D’Alton, M.; Zhang, Y.; Kahe, K.; Cepin, A.; Goffman, D.; Staniczenko, A.; Yates, H.; Burgansky, A.; Coletta, J.; et al. COVID-19 vaccine acceptance among pregnant, breastfeeding, and nonpregnant reproductive-aged women. Am. J. Obstet. Gynecol. MFM 2021, 3, 100403. [Google Scholar] [CrossRef]
- Skjefte, M.; Ngirbabul, M.; Akeju, O.; Escudero, D.; Hernandez-Diaz, S.; Wyszynski, D.F.; Wu, J.W. COVID-19 vaccine acceptance among pregnant women and mothers of young children: Results of a survey in 16 countries. Eur. J. Epidemiol. 2021, 36, 197–211. [Google Scholar] [CrossRef] [PubMed]
- Schaal, N.K.; Zöllkau, J.; Hepp, P.; Fehm, T.; Hagenbeck, C. Pregnant and breastfeeding women’s attitudes and fears regarding the COVID-19 vaccination. Arch. Gynecol. Obstet. 2021, 27, 1–8. [Google Scholar] [CrossRef]
- Blakeway, H.; Prasad, S.; Kalafat, E.; Heath, P.T.; Ladhani, S.N.; Le Doare, K.; Magee, L.A.; O’Brien, P.; Rezvani, A.; von Dadelszen, P.; et al. COVID-19 vaccination during pregnancy: Coverage and safety. Am. J. Obstet. Gynecol. 2022, 226, 236.e1–236.e14. [Google Scholar] [CrossRef]
- Qiu, X.; Bailey, H.; Thorne, C. Barriers and facilitators associated with vaccine acceptance and uptake among pregnant women in high income countries: A mini-review. Front. Immunol. 2021, 12, 626717. [Google Scholar] [CrossRef]
- Duong, M.C.; Duong, B.T.; Nguyen, H.T.; Nguyen Thi Quynh, T.; Nguyen, D.P. Knowledge about COVID-19 Vaccine and Vaccination in Vietnam: A Population Survey. J. Am. Pharm. Assoc. 2022; in press. [Google Scholar] [CrossRef]
- Rzymski, P.; Borkowski, L.; Drąg, M.; Flisiak, R.; Jemielity, J.; Krajewski, J.; Mastalerz-Migas, A.; Matyja, A.; Pyrć, K.; Simon, K.; et al. The strategies to support the COVID-19 vaccination with evidence-based communication and tackling misinformation. Vaccines 2021, 9, 109. [Google Scholar] [CrossRef]
- Saeed, B.Q.; Al-Shahrabi, R.; Bolarinwa, O.A. Socio-demographic correlate of knowledge and practice toward COVID-19 among people living in Mosul-Iraq: A cross-sectional study. PLoS ONE 2021, 16, e0249310. [Google Scholar] [CrossRef] [PubMed]
- Bjelica, A.; Cetkovic, N.; Trninic-Pjevic, A.; Mladenovic-Segedi, L. The phenomenon of pregnancy—A psychological view. Ginekol. Pol. 2018, 89, 102–106. [Google Scholar] [CrossRef]
- Farrell, T.; Reagu, S.; Mohan, S.; Elmidany, R.; Qaddoura, F.; Ahmed, E.E.; Corbett, G.; Lindow, S.; Abuyaqoub, S.M.; Alabdulla, M.A. The impact of the COVID-19 pandemic on the perinatal mental health of women. J. Perinat. Med. 2020, 48, 971–976. [Google Scholar] [CrossRef] [PubMed]
- Takubo, Y.; Tsujino, N.; Aikawa, Y.; Fukiya, K.; Iwai, M.; Uchino, T.; Ito, M.; Akiba, Y.; Mizuno, M.; Nemoto, T. Psychological impacts of the COVID-19 pandemic on one-month postpartum mothers in a metropolitan area of Japan. BMC Pregnancy Childbirth 2021, 21, 845. [Google Scholar] [CrossRef]
- Ostacoli, L.; Cosma, S.; Bevilacqua, F.; Berchialla, P.; Bovetti, M.; Carosso, A.R.; Malandrone, F.; Carletto, S.; Benedetto, C. Psychosocial factors associated with postpartum psychological distress during the COVID-19 pandemic: A cross-sectional study. BMC Pregnancy Childbirth 2020, 20, 703. [Google Scholar] [CrossRef] [PubMed]
- Vesga-Lopez, O.; Blanco, C.; Keyes, K.; Olfson, M.; Grant, B.F.; Hasin, D.S. Psychiatric disorders in pregnant and postpartum women in the United States. Arch. Gen. Psychiatry 2008, 65, 805–815. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Stein, A.; Pearson, R.M.; Goodman, S.H.; Rapa, E.; Rahman, A.; McCallum, M.; Howard, L.M.; Pariante, C.M. Effects of perinatal mental disorders on the fetus and child. Lancet 2014, 384, 1800–1819. [Google Scholar] [CrossRef]
- Caparros-Gonzalez, R.A.; Ganho-Avila, A.; Torre-Luque, A. The COVID-19 pandemic can impact perinatal mental health and the health of the offspring. Behav. Sci. 2020, 10, 162. [Google Scholar] [CrossRef]
- Hirshberg, J.S.; Huysman, B.C.; Oakes, M.C.; Cater, E.B.; Odibo, A.O.; Raghuraman, N.; Kelly, J.C. Offering onsite COVID-19 vaccination to high-risk obstetrical patients: Initial findings. Am. J. Obstet. Gynecol. MFM 2021, 3, 100478. [Google Scholar] [CrossRef]
- Dror, A.A.; Eisenbach, N.; Taiber, S.; Morozov, N.G.; Mizrachi, M.; Zigron, A.; Srouji, S.; Sela, E. Vaccine hesitancy: The next challenge in the fight against COVID-19. Eur. J. Epidemiol. 2020, 35, 775–779. [Google Scholar] [CrossRef]
- Laine, C.; Cotton, D.; Moyer, D.V. COVID-19 Vaccine: Promoting vaccine acceptance. Ann. Intern. Med. 2021, 174, 252–253. [Google Scholar] [CrossRef]
- Kachikis, A.; Englund, J.A.; Singleton, M.; Covelli, I.; Drake, A.L.; Eckert, L.O. Short-term reactions among pregnant and lactating individuals in the first wave of the COVID-19 vaccine rollout. JAMA Netw. Open 2021, 4, e2121310. [Google Scholar] [CrossRef] [PubMed]
- Zauche, L.H.; Wallace, B.; Smoots, A.N.; Olson, C.K.; Oduyebo, T.; Kim, S.Y.; Petersen, E.E.; Ju, J.; Beauregard, J.; Wilcox, A.J.; et al. CDC v-safe COVID-19 Pregnancy Registry Team. Receipt of mRNA COVID-19 vaccines and risk of spontaneous abortion. N. Engl. J. Med. 2021, 385, 1533–1535. [Google Scholar] [CrossRef] [PubMed]
- Magnus, M.C.; Gjessing, H.K.; Eide, H.N.; Wilcox, A.J.; Fell, D.B.; Håberg, S.E. COVID-19 vaccination during pregnancy and first-trimester miscarriage. N. Engl. J. Med. 2021, 385, 2008–2010. [Google Scholar] [CrossRef]
- Kharbanda, E.O.; Haapala, J.; DeSilva, M.; Vazquez-Benitez, G.; Vesco, K.K.; Naleway, A.L.; Lipkind, H.S. Spontaneous abortion following COVID-19 vaccination during pregnancy. JAMA 2021, 326, 1629–1631. [Google Scholar] [CrossRef]
- Wainstock, T.; Yoles, I.; Sergienko, R.; Sheiner, E. Prenatal maternal COVID-19 vaccination and pregnancy outcomes. Vaccine 2021, 39, 6037–6040. [Google Scholar] [CrossRef]
- Bookstein Peretz, S.; Regev, N.; Novick, L.; Nachshol, M.; Goffer, E.; Ben-David, A.; Asraf, K.; Doolman, R.; Levin, E.G.; Regev Yochay, G.; et al. Short-term outcome of pregnant women vaccinated with BNT162b2 mRNA COVID-19 vaccine. Ultrasound Obstet. Gynecol. 2021, 58, 450–456. [Google Scholar] [CrossRef]
- Rottenstreich, M.; Sela, H.Y.; Rotem, R.; Kadish, E.; Wiener-Well, Y.; Grisaru-Granovsky, S. COVID-19 vaccination during the third trimester of pregnancy: Rate of vaccination and maternal and neonatal outcomes, a multicentre retrospective cohort study. BJOG 2022, 129, 248–255. [Google Scholar] [CrossRef] [PubMed]
- Rodríguez-Blanco, N.; Tuells, J. Knowledge and attitudes about the flu vaccine among pregnant women in the valencian community (Spain). Medicina 2019, 55, 467. [Google Scholar] [CrossRef] [Green Version]
- The Central Statistical Office. GUS: Mobile Broadband is Growing in Importance. Available online: https://ictmarketexperts.com/en/news/gus-mobile-broadband-is-growing-in-importance/ (accessed on 25 April 2022).
- Education GPS. Poland. Overview of the Education System (EAG 2021). Available online: https://gpseducation.oecd.org/CountryProfile?primaryCountry=POL&treshold=10&topic=EO (accessed on 25 April 2022).



{kind=link}
{kind=link}
{kind=link}
| Data | n/N 1196 | % | |
|---|---|---|---|
| Age (years) | 18–25 | 131/1196 | 11.0 |
| 26–30 | 461/1196 | 38.5 | |
| 31–35 | 422/1196 | 35.3 | |
| 36–40 | 164/1196 | 13.7 | |
| ≥41 | 18/1196 | 1.5 | |
| Pre-pregnancy BMI (kg/m2) | underweight (<18.5) | 84/1196 | 7.0 |
| normal weight (18.5–24.9) | 765/1196 | 64.0 | |
| overweight (25–29.9) | 219/1196 | 18.3 | |
| obesity class 1 (30–34.9) | 101/1196 | 8.4 | |
| obesity class 2 (35–39.9) | 26/1196 | 2.2 | |
| obesity class 3 (≥40) | 1/1196 | 0.1 | |
| Residence | urban, above 100,000 residents | 632/1196 | 52.8 |
| urban, 10,000–100,000 residents | 226/1196 | 18.9 | |
| urban, <10,000 residents | 76/1196 | 6.4 | |
| rural | 262/1196 | 21.9 | |
| Education | vocational and primary | 30/1196 | 2.5 |
| high school | 223/1196 | 18.7 | |
| university | 943/1196 | 78.8 | |
| Marital status | married | 959/1196 | 80.2 |
| cohabiting | 214/1196 | 17.9 | |
| single parent and divorced | 23/1196 | 1.9 | |
| Currently obstetric state | pregnant women in 1 trimester | 16/1196 | 1.3 |
| pregnant women in 2 trimester | 64/1196 | 5.4 | |
| pregnant women in 3 trimester | 176/1196 | 14.7 | |
| women after delivery | 940/1196 | 78.6 | |
| Mode of delivery | vaginal birth | 528/940 | 56.2 |
| elective cesarean section | 215/940 | 22.8 | |
| emergency cesarean section | 197/940 | 21.0 | |
| Physiological pregnancy | Yes | 993/1196 | 83.0 |
| No | 203/1196 | 17.0 | |
| Difficulties in conceiving a child | Yes | 278/1196 | 23.2 |
| No | 918/1196 | 76.8 | |
| Medically assisted procreation | Yes | 93/1196 | 7.8 |
| No | 1103/1196 | 92.2 | |
| Miscarriage in the past | Yes | 259/1196 | 21.7 |
| No | 937/1196 | 78.3 | |
| Sociodemographic Data | Vaccinated N = 796 % (n) | Unvaccinated N = 400 % (n) | χ2 Test | p-Value | |
|---|---|---|---|---|---|
| Age (years) | 18–25 | 7.9% (63) | 17.0% (68) | 35.95 | <0.001 |
| 26–30 | 36.7% (292) | 42.2% (169) | |||
| 31–35 | 38.8% (309) | 28.3% (113) | |||
| 36–40 | 14.6% (116) | 12.0% (48) | |||
| ≥41 | 2.0% (16) | 0.5% (2) | |||
| Pre-pregnancy BMI, kg/m2 | underweight (<18.5) | 6.7% (53) | 7.8% (31) | 1.06 | 0.95 |
| normal weight (18.5–24.9) | 64.2% (511) | 63.5% (254) | |||
| overweight (25–29.9) | 18.3% (146) | 18.2% (73) | |||
| obesity class 1 (30–34.9) | 8.4% (67) | 8.5% (34) | |||
| obesity class 2 (35–39.9) | 2.3% (18) | 2.0% (8) | |||
| obesity class 3 (≥40) | 0.1% (1) | 0% (0) | |||
| Residence | urban, above 100,000 residents | 60.0% (478) | 38.5% (154) | 55.17 | <0.001 |
| urban, 10,000–100,000 residents | 17.6% (140) | 21.5% (86) | |||
| urban, <10,000 residents | 4.8% (38) | 9.5% (38) | |||
| rural | 17.6% (140) | 30.5% (122) | |||
| Education | vocational and primary | 1.6% (13) | 4.3% (17) | 48.682 | <0.001 |
| high school | 13.7% (109) | 28.5% (114) | |||
| university | 84.7% (674) | 67.2% (269) | |||
| Marital status | married | 84.1% (669) | 72.5% (290) | 22.36 | <0.001 |
| cohabiting | 14.4% (115) | 24.8% (99) | |||
| single parent and divorced | 1.5% (12) | 2.7% (11) | |||
| Current obstetric state | pregnant women 1 trimester | 1.0% (8) | 2.0% (8) | 3.27 | 0.35 |
| pregnant women 2 trimester | 5.3% (42) | 5.5% (22) | |||
| pregnant women 3 trimester | 15.6% (124) | 13.0% (52) | |||
| women after delivery | 78.2% (622) | 79.6% (318) | |||
| Type of delivery | vaginal birth | 53.9% (335) | 60.7% (193) | 4.32 | 0.11 |
| elective cesarean section | 23.6% (147) | 21.4% (68) | |||
| emergency cesarean section | 22.5% (140) | 17.9% (57) | |||
| Physiological pregnancy | Yes | 82.7% (658) | 83.8% (335) | 0.22 | 0.63 |
| No | 17.3% (138) | 16.2% (65) | |||
| Difficulties in conceiving a child | Yes | 23.7% (189) | 22.3% (89) | 0.33 | 0.56 |
| No | 48.5% (607) | 77.8% (311) | |||
| Medically assisted procreation | Yes | 8.3% (66) | 6.7% (27) | 0.88 | 0.34 |
| No | 91.7% (730) | 93.3% (373) | |||
| Miscarriage in the past | Yes | 22.0% (175) | 21.0% (84) | 0.20 | 0.69 |
| No | 78.0% (621) | 79.0% (316) |
| Sociodemographic Data | Pregnant Women | Women after Delivery | Vaccinated Women, Pregnant vs. after Delivery | Unvaccinated Women, Pregnant vs. after Delivery | |||||
|---|---|---|---|---|---|---|---|---|---|
| Vaccinated N = 174 % (n) | Unvaccinated N = 82 % (n) | Vaccinated N = 622 % (n) | Unvaccinated N = 318 % (n) | χ2 Test | p-Value | χ2 Test | p-Value | ||
| Age (years) | 18–25 | 12.6% (22) | 18.3% (15) | 6.6% (41) | 16.7% (53) | 9.17 | 0.057 | 3.87 | 0.42 |
| 26–30 | 36.2% (63) | 40.2% (33) | 36.8% (229) | 42.8% (136) | |||||
| 31–35 | 39.1% (68) | 34.2% (28) | 38.7% (241) | 26.7% (85) | |||||
| 36–40 | 10.9% (19) | 7.3% (6) | 15.6% (97) | 13.2% (42) | |||||
| ≥41 | 1.2% (2) | 0.0% (0) | 2.3% (14) | 0.6% (2) | |||||
| Pre-pregnancy BMI (kg/m2) | underweight (<18.5) | 4.6% (8) | 11.0% (9) | 7.2% (45) | 6.9% (22) | 6.96 | 0.22 | 22.61 | <0.001 |
| normal weight (18.5–24.9) | 66.1% (115) | 53.6% (44) | 63.7% (396) | 66.1% (210) | |||||
| overweight (25–29.9) | 20.1% (35) | 12.2% (10) | 17.8% (111) | 19.8% (63) | |||||
| obesity class 1 (30–34.9) | 7.5% (13) | 17.1% (14) | 8.7% (54) | 6.3% (20) | |||||
| obesity class 2 (35–39.9) | 1.2% (2) | 6.1% (5) | 2.6% (16) | 0.9% (3) | |||||
| obesity class 3 (≥40) | 0.6% (1) | 0.0% (0) | 0.0% (0) | 0.0% (0) | |||||
| Residence | urban, above 100,000 residents | 71.8% (125) | 57.3% (47) | 56.8% (353) | 33.7% (107) | 13.93 | <0.005 | 18.5 | <0.001 |
| urban, 10,000–100,000 residents | 10.3% (18) | 18.3% (15) | 19.6% (122) | 22.3% (71) | |||||
| urban, <10,000 residents | 3.4% (6) | 9.8% (8) | 5.1% (32) | 9.4% (30) | |||||
| rural | 14.4% (25) | 14.6% (12) | 18.5% (115) | 34.6% (110) | |||||
| Education | vocational and primary | 1.7% (3) | 3.7% (3) | 1.6% (10) | 4.4% (14) | 0.50 | 0.77 | 0.11 | 0.94 |
| high school | 12.1% (21) | 29.2% (24) | 14.2% (88) | 28.3% (90) | |||||
| university | 86.2% (150) | 67.1% (55) | 84.2% (524) | 67.3% (214) | |||||
| Marital status | married | 79.9% (139) | 61.0% (50) | 85.2% (530) | 75.5% (240) | 3.13 | 0.20 | 2.37 | 0.12 |
| cohabiting | 17.8% (31) | 37.8% (31) | 13.5% (84) | 21.4% (68) | |||||
| single parent and divorced | 2.3% (4) | 1.2% (1) | 1.1% (8) | 0.6% (10) | |||||
| Physiological pregnancy | Yes | 89.7% (156) | 89.0% (73) | 80.7% (502) | 82.4% (262) | 7.60 | <0.006 | 2.11 | 0.14 |
| No | 10.3% (18) | 11.0% (9) | 19.3% (120) | 17.6% (56) | |||||
| Difficulties in conceiving a child | Yes | 22.4% (39) | 25.6% (21) | 24.1% (150) | 21.4% (68) | 0.22 | 0.64 | 0.67 | 0.41 |
| No | 77.6% (135) | 74.4% (61) | 75.9% (472) | 78.6% (250) | |||||
| Medically assisted procreation | Yes | 18.0% (14) | 3.7% (3) | 8.4% (52) | 7.5% (24) | 0.02 | 0.89 | 1.56 | 0.21 |
| No | 92.0% (160) | 96.3% (79) | 91.6% (570) | 92.5% (294) | |||||
| Miscarriage in the past | Yes | 21.8% (38) | 23.2% (19) | 22.0% (137) | 20.4% (65) | 0.003 | 0.95 | 0.29 | 0.58 |
| No | 78.2% (136) | 76.8% (63) | 78.0% (485) | 79.6% (253) | |||||
| COVID-19 Knowledge Level | Vaccinated N = 796 % (n) | Unvaccinated N = 400 % (n) | χ2 Test | p-Value | |
|---|---|---|---|---|---|
| Were you afraid of SARS-CoV-2 infection during pregnancy/lactation? | 1 | 4.9% (39) | 21.5% (86) | 197.04 | <0.001 |
| 2 | 3.6% (29) | 14.3% (57) | |||
| 3 | 14.7% (117) | 25.5% (102) | |||
| 4 | 21.5% (171) | 16.3% (65) | |||
| 5 | 55.3% (440) | 22.5% (90) | |||
| Did you suffer from COVID-19 during pregnancy? | Yes | 11.2% (89) | 15.3% (61) | 45.94 | <0.001 |
| No | 79.8% (635) | 63.0% (252) | |||
| I do not know | 9.0% (72) | 21.8% (87) | |||
| Is SARS-CoV-2 transmitted through breastfeeding? | Yes | 4.5% (36) | 7.5% (30) | 22.75 | <0.001 |
| No | 75.3% (599) | 62.0% (248) | |||
| I do not know | 20.2% (161) | 30.5% (122) | |||
| Can breastfeeding after the mother has COVID-19 protect the baby from SARS-CoV-2 infection? | Yes | 72.7% (579) | 45.0% (180) | 92.32 | <0.001 |
| No | 8.7% (69) | 22.3% (89) | |||
| I do not know | 18.6% (148) | 32.8% (131) | |||
| Do you think that immunity achieved after COVID-19 vaccination might provide immune protection to the fetus and newborn (placental transfer)? | Yes | 88.1% (701) | 28.5% (114) | 449.63 | <0.001 |
| No | 2.0% (16) | 28.8% (115) | |||
| I do not know | 9.9% (79) | 42.8% (171) | |||
| Do you think that immunity achieved after COVID-19 vaccination might be transferred with human milk to the newborns/infants? | Yes | 79.6% (634) | 24.5% (98) | 346.43 | <0.001 |
| No | 6.8% (54) | 33.5% (134) | |||
| I do not know | 13.6% (108) | 42.0% (168) | |||
| Pregnant Women | Women after Delivery | Vaccinated Women, Pregnant vs. after Delivery | Unvaccinated Women, Pregnant vs. after Delivery | ||||||
|---|---|---|---|---|---|---|---|---|---|
| Vaccinated N = 174 % (n) | Unvaccinated N = 82 % (n) | Vaccinated N = 622 % (n) | Unvaccinated N = 318 % (n) | χ2 Test | p-Value | χ2 Test | p-Value | ||
| Were you afraid of SARS-CoV-2 infection during pregnancy/lactation? | 1 | 4.6% (8) | 23.2% (19) | 5.0% (31) | 21.1% (67) | 37.22 | <0.001 | 2.91 | 0.57 |
| 2 | 4.6% (8) | 18.3% (15) | 3.4% (21) | 13.2% (42) | |||||
| 3 | 18.4% (32) | 20.7% (17) | 13.7% (85) | 26.7% (85) | |||||
| 4 | 31.6% (55) | 18.3% (15) | 18.6% (116) | 15.7% (50) | |||||
| 5 | 29.3% (51) | 19.5% (16) | 59.3% (369) | 23.3% (74) | |||||
| Did you suffer from COVID-19 during pregnancy? | Yes | 7.5% (13) | 12.2% (10) | 12.2% (76) | 16.0% (51) | 3.12 | 0.21 | 1.89 | 0.39 |
| No | 82.8% (144) | 69.5% (57) | 78.9% (491) | 61.3% (195) | |||||
| I do not know | 9.8% (17) | 18.3% (15) | 8.8% (55) | 22.6% (72) | |||||
| Is SARS-CoV-2 transmitted through breastfeeding? | Yes | 9.8% (17) | 7.3% (6) | 3.1% (19) | 7.5% (24) | 28.72 | <0.001 | 0.07 | 0.96 |
| No | 60.9% (106) | 61.0% (50) | 79.3% (493) | 62.3% (198) | |||||
| I do not know | 29.3% (51) | 31.7% (26) | 17.7% (110) | 30.2% (96) | |||||
| Can breastfeeding after the mother has COVID-19 protect the baby from SARS-CoV-2 infection? | Yes | 64.9% (113) | 37.8% (31) | 74.9% (466) | 46.9% (149) | 64.03 | <0.001 | 2.47 | 0.29 |
| No | 13.2% (23) | 23.2% (19) | 7.4% (460 | 22.0% (70) | |||||
| I do not know | 21.8% (38) | 39.0% (32) | 17.7% (110) | 31.1% (99) | |||||
| Do you think that immunity achieved after COVID-19 vaccination might provide immune protection to the fetus and newborn (placental transfer)? | Yes | 92.5% (161) | 32.9% (27) | 86.8% (540) | 27.4% (87) | 4.51 | 0.10 | 1.06 | 0.59 |
| No | 1.7% (3) | 28.0% (23) | 2.1% (13) | 28.9% (92) | |||||
| I do not know | 5.7% (10) | 39.0% (32) | 11.1% (69) | 43.7% (139) | |||||
| Do you think that immunity achieved after COVID-19 vaccination might be transferred with human milk to the newborns/infants? | Yes | 68.4% (119) | 26.8% (22) | 82.8% (515) | 23.9% (76) | 17.48 | <0.001 | 0.77 | 0.68 |
| No | 10.9% (19) | 35.4% (29) | 5.6% (35) | 33.0% (105) | |||||
| I do not know | 20.7% (36) | 37.8% (31) | 11.6% (72) | 43.1% (137) | |||||
| Data | Odds Ratio (OR) (95% Lower—Upper Confidence Interval (CI)) | p-Value |
|---|---|---|
| Age (years) | 0.96 (0.92–1.00) | <0.06 |
| Residence urban, above 100,000 residents (ref) urban, 10,000–100,000 residents urban, <10,000 residents rural | 1.52 (0.98–2.37) 2.06 (1.05–4.02) 1.89 (1.25–2.87) | 0.06 <0.04 <0.003 |
| Marital status married (ref) cohabiting single parent & divorced | 1.76 (1.15–2.70) 1.00 (0.34–2.94) | <0.009 0.99 |
| Were you afraid of SARS-CoV-2 infection during pregnancy/lactation? 5 (I was DEFINITELY AFRAID) (ref) 4 3 2 1 (I was DEFINITELY NOT AFRAID) | 1.90 (1.20–3.02) 4.31 (2.75–6.74) 7.21 (3.84–13.54) 5.84 (3.32–10.27) | <0.007 <0.001 <0.001 <0.001 |
| Did you suffer from COVID-19 during your pregnancy? No (ref) Yes I do not know | 2.32 (1.43–3.77) 2.67 (1.66–4.28) | <0.001 <0.001 |
| Is SARS-CoV-2 transmitted through breastfeeding? No (ref) Yes I do not know | 2.32 (1.15–4.70) 1.24 (0.82–1.88) | <0.02 0.3 |
| Does breastfeeding protect children from COVID-19? Yes (ref) No I do not know | 1.86 (1.13–3.07) 1.08 (0.70–1.67) | <0.02 0.73 |
| Do you think that immunity achieved after COVID-19 vaccination might provide immune protection to the fetus and newborn (placental transfer)? Yes (ref) No I do not know | 23.86 (12.99–43.84) 10.77 (7.20–16.10) | <0.001 <0.001 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lis-Kuberka, J.; Berghausen-Mazur, M.; Orczyk-Pawiłowicz, M. Attitude and Level of COVID-19 Vaccination among Women in Reproductive Age during the Fourth Pandemic Wave: A Cross-Sectional Study in Poland. Int. J. Environ. Res. Public Health 2022, 19, 6872. https://doi.org/10.3390/ijerph19116872
Lis-Kuberka J, Berghausen-Mazur M, Orczyk-Pawiłowicz M. Attitude and Level of COVID-19 Vaccination among Women in Reproductive Age during the Fourth Pandemic Wave: A Cross-Sectional Study in Poland. International Journal of Environmental Research and Public Health. 2022; 19(11):6872. https://doi.org/10.3390/ijerph19116872
Chicago/Turabian StyleLis-Kuberka, Jolanta, Marta Berghausen-Mazur, and Magdalena Orczyk-Pawiłowicz. 2022. "Attitude and Level of COVID-19 Vaccination among Women in Reproductive Age during the Fourth Pandemic Wave: A Cross-Sectional Study in Poland" International Journal of Environmental Research and Public Health 19, no. 11: 6872. https://doi.org/10.3390/ijerph19116872
APA StyleLis-Kuberka, J., Berghausen-Mazur, M., & Orczyk-Pawiłowicz, M. (2022). Attitude and Level of COVID-19 Vaccination among Women in Reproductive Age during the Fourth Pandemic Wave: A Cross-Sectional Study in Poland. International Journal of Environmental Research and Public Health, 19(11), 6872. https://doi.org/10.3390/ijerph19116872