
Effects of Patient Education on Pain and Function and Its Impact on Conservative Treatment in Elderly Patients with Pain Related to Hip and Knee Osteoarthritis: A Systematic Review

 ,
,  ,
,  and
and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Search Strategy
2.2. Eligibility Criteria
2.3. Data Extraction
2.4. Quality Assessment
2.5. Risk of Bias Assessment
3. Results
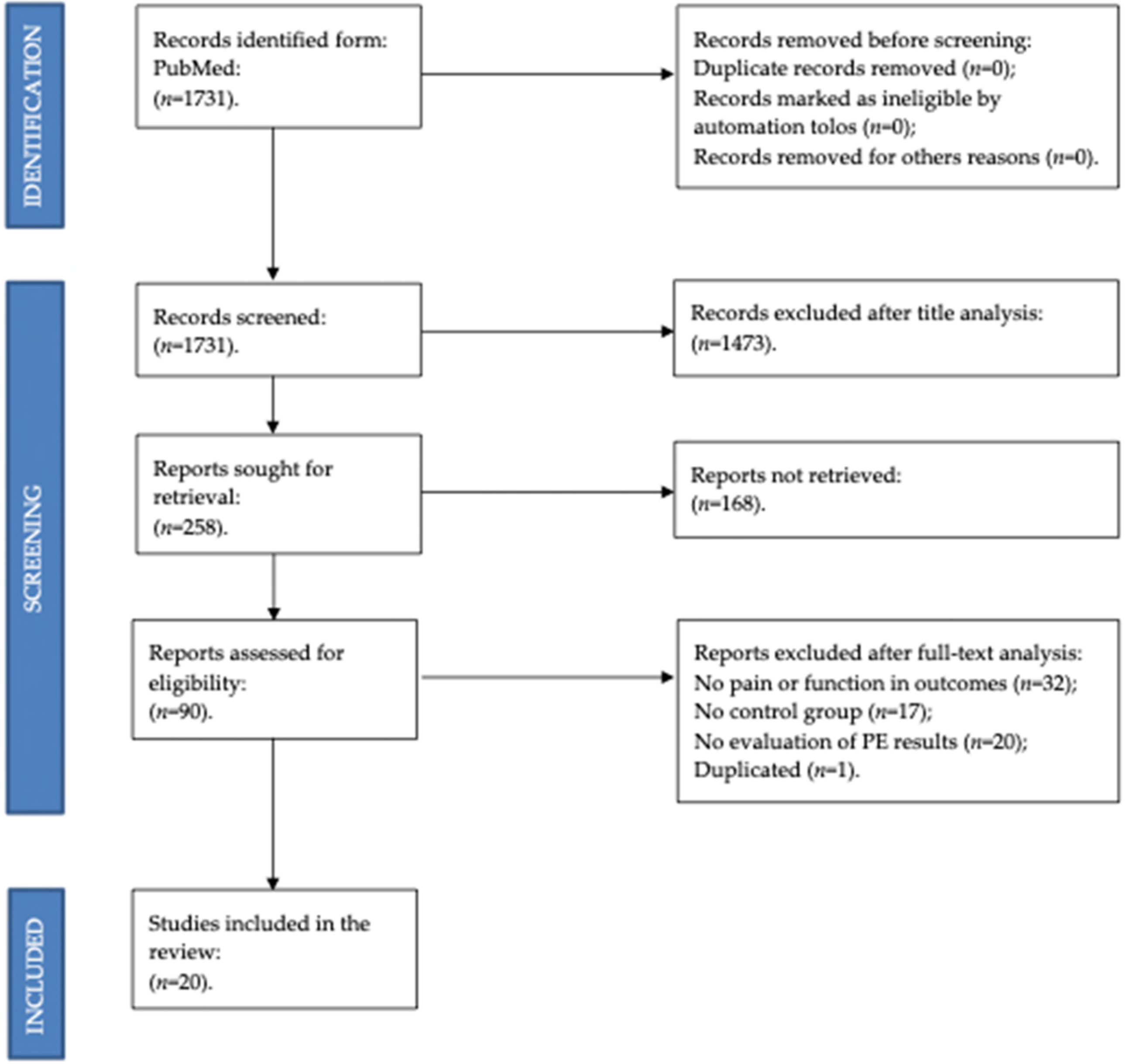
3.1. Study Selection
3.2. Quality Assessment
3.3. Risk of Bias within and across the Studies
3.4. Data from Studies
3.4.1. Effects of Patient Education on Pain
3.4.2. Effects of Patient Education on Function
4. Discussion
4.1. Discussion on the Effects of Patient Education on Pain
4.2. Discussion on the Effects of Patient Education on Function
4.3. Discussion on the Impact of Patient Education on Conservative Treatment
4.4. Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Hunter, D.J.; Bierma-Zeinstra, S. Osteoarthritis. Lancet 2019, 393, 1745–1759. [Google Scholar] [CrossRef]
- Cross, M.; Smith, E.; Hoy, D.; Nolte, S.; Ackerman, I.; Fransen, M.; Bridgett, L.; Williams, S.; Guillemin, F.; Hill, C.L.; et al. The global burden of hip and knee osteoarthritis: Estimates from the global burden of disease 2010 study. Ann. Rheum. Dis. 2014, 73, 1323–1330. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. Muskoskeletal Conditions. Available online: https://www.who.int/news-room/fact-sheets/detail/musculoskeletal-conditions (accessed on 8 February 2021).
- Cieza, A.; Causey, K.; Kamenov, K.; Hanson, S.W.; Chatterji, S.; Vos, T. Global estimates of the need for rehabilitation based on the Global Burden of Disease study 2019: A systematic analysis for the Global Burden of Disease Study 2019. Lancet 2021, 396, 2006–2017. [Google Scholar] [CrossRef]
- Chen, A.; Gupte, C.; Akhtar, K.; Smith, P.; Cobb, J. The global economic cost of osteoarthritis: How the UK compares. Arthritis 2012, 2012, 698709. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Basile, M.; Rumi, F.; Palmeri, M.; Mattozzi, I.; Manzoli, L.; Mammuccari, M.; Gigliotti, S.; Bernabei, R.; Cicchetti, A. Economic burden of prescriptive inadequacy in the management of osteoarthritis in Italy. Glob. Reg. Health. Technol. Assess. 2020, 2020, 2130. [Google Scholar] [CrossRef]
- Kolasinski, S.L.; Neogi, T.; Hochberg, M.C.; Oatis, C.; Guyatt, G.; Block, J.; Callahan, L.; Copenhaver, C.; Dodge, C.; Felson, D.; et al. 2019 American College of Rheumatology/Arthritis Foundation Guideline for the management of osteoarthritis of the hand, hip, and knee. Arthritis Care Res. 2020, 72, 149–162. [Google Scholar] [CrossRef]
- Bannuru, R.R.; Osani, M.C.; Vaysbrot, E.E.; Arden, N.K.; Bennell, K.; Bierma-Zeinstra, S.M.A.; Kraus, V.B.; Lohmander, L.S.; Abbott, J.H.; Bhandari, M.; et al. OARSI guidelines for the non-surgical management of knee, hip, and polyarticular osteoarthritis. Osteoarthr. Cartil. 2019, 27, 1578–1589. [Google Scholar] [CrossRef] [Green Version]
- Villafañe, J.H. Exercise and osteoarthritis: An update. J. Exerc. Rehabil. 2018, 14, 538–539. [Google Scholar] [CrossRef]
- Gay, C.; Chabaud, A.; Guilley, E.; Coudeyre, E. Educating patients about the benefits of physical activity and exercise for their hip and knee osteoarthritis. Systematic literature review. Ann. Phys. Rehabil. Med. 2016, 59, 174–183. [Google Scholar] [CrossRef]
- Villafañe, J.H.; Pirali, C.; Dughi Testa, A.; Manno, A.; Bishop, M.D.; Negrini, S. Association between malnutrition and barthel index in a cohort of hospitalized older adults article information. J. Phys. Sci. 2016, 28, 607–612. [Google Scholar] [CrossRef] [Green Version]
- Sánchez Romero, E.A.; Meléndez Oliva, E.; Alonso Pérez, J.L.; Pérez, S.M.; Turroni, S.; Marchese, L.; Villafañe, J.H. Relationship between the gut microbiome and osteoarthritis pain: Review of the literature. Nutrients 2021, 13, 716. [Google Scholar] [CrossRef] [PubMed]
- Villafañe, J.H.; Valdes, K.; Pedersini, P.; Berjano, P. Osteoarthritis: A call for research on central pain mechanism and personalized prevention strategies. Clin. Rheumatol. 2019, 38, 583–584. [Google Scholar] [CrossRef] [PubMed]
- Joypaul, S.; Kelly, F.; McMillan, S.S.; King, M.A. Multi-disciplinary interventions for chronic pain involving education: A systematic review. PLoS ONE 2019, 14, e0223306. [Google Scholar] [CrossRef] [PubMed]
- Goff, A.J.; De Oliveira Silva, D.; Merolli, M.; Bell, E.C.; Crossley, K.M.; Barton, C.J. Patient education improves pain and function in people with knee osteoarthritis with better effects when combined with exercise therapy: A systematic review. J. Physiother. 2021, 67, 177–189. [Google Scholar] [CrossRef] [PubMed]
- Kroon, F.P.; van der Burg, L.R.; Buchbinder, R.; Osborne, R.H.; Johnston, R.V.; Pitt, V. Self-management education programmes for osteoarthritis. Cochrane. Database Syst. Rev. 2014, 1, CD008963. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. Therapeutic Patient Education. Available online: https://www.euro.who.int/__data/assets/pdf_file/0007/145294/E63674.pdf (accessed on 23 January 2022).
- Preferred reporting items for systematic review and meta-analysis protocols (PRISMA-P) 2015: Elaboration and explanation. BMJ 2016, 354, i4086. [CrossRef] [Green Version]
- Maher, C.G.; Sherrington, C.; Herbert, R.D.; Moseley, A.M.; Elkins, M. Reliability of the PEDro scale for rating quality of randomized controlled trials. Phys. Ther. 2003, 83, 713–721. [Google Scholar] [CrossRef] [Green Version]
- Farrah, K.; Young, K.; Tunis, M.C.; Zhao, L. Risk of bias tools in systematic reviews of health interventions: An analysis of PROSPERO-registered protocols. Syst. Rev. 2019, 8, 280. [Google Scholar] [CrossRef]
- Bennell, K.L.; Nelligan, R.K.; Rini, C.; Keefe, F.J.; Kasza, J.; French, S.; Forbes, A.; Dobson, F.; Abbott, J.H.; Dalwood, A.; et al. Effects of internet-based pain coping skills training before home exercise for individuals with hip osteoarthritis (HOPE trial): A randomised controlled trial. Pain 2018, 159, 1833–1842. [Google Scholar] [CrossRef]
- Bennell, K.L.; Egerton, T.; Martin, J.; Haxby Abbott, J.; Metcalf, B.; McManus, F.; Sims, K.; Pua, Y.-H.; Wrigley, T.V.; Forbes, A.; et al. Effect of physical therapy on pain and function in patients with hip osteoarthritis: A randomized clinical trial. JAMA 2014, 311, 1987–1997. [Google Scholar] [CrossRef]
- Allen, K.D.; Oddone, E.Z.; Coffman, C.J.; Datta, S.K.; Juntilla, K.A.; Lindquist, J.H.; Walker, T.A.; Weinberger, M.; Bosworth, H.B. Telephone-based self-management of osteoarthritis: A randomized trial. Ann. Intern. Med. 2010, 153, 570–579. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Giraudet-Le Quintrec, J.S.; Coste, J.; Vastel, L.; Pacault, V.; Jeanne, L.; Lamas, J.-P.; Kerboull, L.; Fougeray, M.; Conseiller, C.; Kahan, A.; et al. Positive effect of patient education for hip surgery: A randomized trial. Clin. Orthop. Relat. Res. 2003, 414, 112–120. [Google Scholar] [CrossRef] [PubMed]
- Heuts, P.H.; de Bie, R.; Drietelaar, M.; Aretz, K.; Hopman-Rock, M.; Bastiaenen, C.H.G.; Metsemakers, J.F.M.; van Weel, C.; van Schayck, O. Self-management in osteoarthritis of hip or knee: A randomized clinical trial in a primary healthcare setting. J. Rheumatol. 2005, 32, 543–549. [Google Scholar] [PubMed]
- Somers, T.J.; Blumenthal, J.A.; Guilak, F.; Kraus, V.B.; Schmitt, D.O.; Babyak, M.A.; Craighead, L.W.; Caldwell, D.S.; Rice, J.R.; McKee, D.C.; et al. Pain coping skills training and lifestyle behavioral weight management in patients with knee osteoarthritis: A randomized controlled study. Pain 2012, 153, 1199–1209. [Google Scholar] [CrossRef] [Green Version]
- Arnold, C.M.; Faulkner, R.A.; Gyurcsik, N.C. The relationship between falls efficacy and improvement in fall risk factors following an exercise plus educational intervention for older adults with hip osteoarthritis. Physiother. Can. 2011, 63, 410–420. [Google Scholar] [CrossRef] [Green Version]
- Lawford, B.J.; Hinman, R.S.; Kasza, J.; Nelligan, R.; Keefe, F.; Rini, C.; Bennell, K.L. Moderators of effects of internet-delivered exercise and pain coping skills training for people with knee osteoarthritis: Exploratory analysis of the IMPACT randomized controlled trial. J. Med. Internet. Res. 2018, 20, e10021. [Google Scholar] [CrossRef] [Green Version]
- Ganji, R.; Pakniat, A.; Armat, M.R.; Tabatabaeichehr, M.; Mortazavi, H. The effect of self-management educational program on pain intensity in elderly patients with knee osteoarthritis: A randomized clinical trial. Open Access Maced. J. Med. Sci. 2018, 6, 1062–1066. [Google Scholar] [CrossRef] [Green Version]
- Ravaud, P.; Flipo, R.M.; Boutron, I.; Roy, C.; Mahmoudi, A.; Giraudeau, B.; Pham, T. ARTIST (osteoarthritis intervention standardized) study of standardised consultation versus usual care for patients with osteoarthritis of the knee in primary care in France: Pragmatic randomised controlled trial. BMJ 2009, 338, b421. [Google Scholar] [CrossRef] [Green Version]
- Lluch, E.; Dueñas, L.; Falla, D.; Baert, I.; Meeus, M.; Sánchez-Frutos, J.; Nijs, J. Preoperative pain neuroscience education combined with knee joint mobilization for knee osteoarthritis: A randomized controlled trial. Clin. J. Pain 2018, 34, 44–52. [Google Scholar] [CrossRef]
- Allen, K.D.; Somers, T.J.; Campbell, L.C.; Arbeeva, L.; Coffman, C.J.; Cené, C.W.; Oddone, E.Z.; Keefe, F.J. Pain coping skills training for African Americans with osteoarthritis: Results of a randomized controlled trial. Pain 2019, 160, 1297–1307. [Google Scholar] [CrossRef]
- Bezalel, T.; Carmeli, E.; Katz-Leurer, M. The effect of a group education programme on pain and function through knowledge acquisition and home-based exercise among patients with knee osteoarthritis: A parallel randomised single-blind clinical trial. Physiotherapy 2010, 96, 137–143. [Google Scholar] [CrossRef] [PubMed]
- Hansson, E.E.; Jönsson-Lundgren, M.; Ronnheden, A.M.; Sörensson, E.; Bjärnung, A.; Dahlberg, L.E. Effect of an education programme for patients with osteoarthritis in primary care—A randomized controlled trial. BMC Musculoskelet. Disord. 2010, 11, 244. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mazzuca, S.A.; Brandt, K.D.; Katz, B.P.; Chambers, M.; Byrd, D.; Hanna, M. Effects of self-care education on the health status of inner-city patients with osteoarthritis of the knee. Arthritis Rheum. 1997, 40, 1466–1474. [Google Scholar] [CrossRef] [PubMed]
- Coleman, S.; Briffa, N.K.; Carroll, G.; Inderjeeth, C.; Cook, N.; McQuade, J. A randomised controlled trial of a self-management education program for osteoarthritis of the knee delivered by health care professionals. Arthritis Res. Ther. 2012, 14, R21. [Google Scholar] [CrossRef] [Green Version]
- Arnold, C.M.; Faulkner, R.A. The effect of aquatic exercise and education on lowering fall risk in older adults with hip osteoarthritis. J. Aging Phys. Act. 2010, 18, 245–260. [Google Scholar] [CrossRef]
- Keefe, F.J.; Caldwell, D.S.; Baucom, D.; Salley, A.; Robinson, E.; Timmons, K.; Beaupre, P.; Weisberg, J.; Helms, M. Spouse-assisted coping skills training in the management of osteoarthritic knee pain. Arthritis Care Res. 1996, 9, 279–291. [Google Scholar] [CrossRef]
- Hughes, S.L.; Seymour, R.B.; Campbell, R.; Pollak, N.; Huber, G.; Sharma, L. Impact of the fit and strong intervention on older adults with osteoarthritis. Gerontologist 2004, 44, 217–228. [Google Scholar] [CrossRef] [Green Version]
- Saraboon, Y.; Aree-Ue, S.; Maruo, S.J. The effect of multifactorial intervention programs on health behavior and symptom control among community-dwelling overweight older adults with knee osteoarthritis. Orthop. Nurs. 2015, 34, 296–308. [Google Scholar] [CrossRef]

{kind=link}
| 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | 9 | 10 | 11 | Score | |
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Keefe et al., (1996) | Yes | Yes | No | Yes | No | No | No | Yes | No | Yes | Yes | 5 |
| Mazzuca et al., (1997) | Yes | Yes | Yes | Yes | No | No | No | No | Yes | Yes | Yes | 6 |
| Giraudet-Le et al., (2003) | Yes | Yes | Yes | No | No | No | Yes | Yes | Yes | Yes | Yes | 7 |
| Heuts et al., (2005) | Yes | Yes | No | Yes | No | No | Yes | No | Yes | Yes | Yes | 6 |
| Ravaud et al., (2009) | Yes | Yes | Yes | Yes | No | No | No | Yes | Yes | Yes | Yes | 7 |
| Arnold et al., (2010) | No | Yes | Yes | Yes | No | No | Yes | No | No | Yes | Yes | 6 |
| Allen et al., (2010) | Yes | Yes | No | Yes | Yes | No | Yes | Yes | Yes | Yes | Yes | 8 |
| Hansson et al., (2010) | Yes | Yes | Yes | Yes | No | No | Yes | Yes | Yes | Yes | Yes | 8 |
| Bezalel et al., (2010) | Yes | Yes | No | Yes | No | No | Yes | No | Yes | Yes | Yes | 6 |
| Arnold et al., (2011) | Yes | Yes | No | No | No | No | Yes | Yes | Yes | Yes | Yes | 6 |
| Somers et al., (2012) | Yes | Yes | No | Yes | No | No | Yes | No | Yes | Yes | Yes | 6 |
| Coleman et al., (2012) | Yes | Yes | Yes | Yes | No | No | Yes | Yes | Yes | Yes | Yes | 8 |
| Hughes et al., (2014) | Yes | Yes | No | Yes | No | No | No | No | No | Yes | Yes | 4 |
| Bennell et al., (2014) | Yes | Yes | Yes | Yes | Yes | No | Yes | Yes | Yes | Yes | Yes | 9 |
| Saraboon et al., (2015) | Yes | Yes | No | No | No | No | No | Yes | Yes | Yes | Yes | 5 |
| Bennell et al., (2018) | Yes | Yes | Yes | Yes | Yes | No | Yes | Yes | Yes | Yes | Yes | 9 |
| Lawford et al., (2018) | Yes | Yes | No | Yes | Yes | No | Yes | Yes | Yes | Yes | Yes | 8 |
| Ganji et al., (2018) | Yes | Yes | No | Yes | No | No | No | Yes | Yes | Yes | Yes | 6 |
| Lluch et al., (2018) | Yes | Yes | No | Yes | Yes | No | Yes | Yes | Yes | Yes | Yes | 8 |
| Allen et al., (2019) | Yes | Yes | Yes | Yes | No | No | No | Yes | Yes | Yes | Yes | 7 |
| Risk of Bias | Randomization Process | Deviations from Intended Interventions | Missing Outcome Data | Measurement of the Outcome | Selection of the Reported Result | Overall Bias in % | Results |
|---|---|---|---|---|---|---|---|
| Assignment to intervention (the ‘intention to-treat’ effect) | |||||||
| Total number of studies = 19 | |||||||
| Low risk | 73.7% | 94.7% | 89.5% | 63.2% | 94.7% | 42.1% | 8 studies |
| Some concerns | 26.3% | 5.3% | 0% | 21.1% | 5.3% | 31.6% | 6 studies |
| High risk | 0% | 0% | 10.5% | 15.8% | 0% | 26.3% | 5 studies |
| Adhering to intervention (the ‘per-protocol’ effect) | |||||||
| Total number of studies = 1 | |||||||
| Low risk | 100% | 100% | 100% | 100% | 100% | 100% | 1 study |
| Some concerns | 0 | 0 | 0 | 0 | 0 | 0 | 0 |
| High risk | 0 | 0 | 0 | 0 | 0 | 0 | 0 |
| Authors | Population | Design | Assessment | Outcomes | Intervention | Results |
|---|---|---|---|---|---|---|
| Keefe et al., (1996) | Total: 88. Age: 62.6 (average, SD 10.1 years). Inclusion criteria: knee OA. | RCT | Pre- and post-intervention (10 weeks treatment period). | Pain: AIMS scale. Coping: Coping Strategies Questionnaire. Pain Behaviour: video. | G1: Spouse-assisted. G2: Coping skills training. CT: Arthritis education spouse-support. (2 h per week (10 weeks of treatment) to all groups) | Pain: Lower pain levels G1 vs. Control post-treatment (AIMS scale). Lower pain levels G2 vs. Control post-treatment, but not statistically significant. G1 vs. G2 did not differ significantly. Pain coping: G1 higher post-treatment scores in Coping Attempts factor than Control (p < 0.0005). G2 slightly higher than control (p < 0.43). Pain behavior: G1 had lower levels of pain behavior than control (p < 0.011). G2 had lower levels of pain behavior than control (p < 0.14), but not statistically significant. |
| Mazzuca et al., (1997) | Total: 211. Age: 62.8 in G1 (average, SD 12.2) and 62 in CG (average, SD 11) Inclusion criteria: OA. | CT | Pre- and post-intervention at 4 months intervals for 1 year. | Disability: HAQ. Pain: HAQ. | G1: individualized 30–60 min education. CG: attention group (20 min standardized public education presentations on arthritis). | Disability: G1 had significantly lower scores for disability than C. Pain: G1 had a significantly lower score for resting knee pain throughout the year of post-intervention follow-up. |
| Giraudet-Le et al., (2003) | Total: 99. Age: 62.7 (avg, SD 8.8). Inclusion criteria: hip OA. | RCT | Pre-intervention (2–6 weeks before surgery) and post-surgery (1 week after). | Anxiety: State Anxiety Inventory. Pain: VAS. | G1: Education (1 session). CT: Usual care (leaflet). | Anxiety: Better results in G1, but not statistically different. Pain: Pre-surgery and post-surgery pain were lower in G1 than CT. |
| Heuts et al., (2005) | Total: 273. Age: 51 (5.0) in G1 and 52.2 (5.1) in CT. Inclusion criteria: knee or hip OA. | RCT | Pre- and post-intervention (21 months). | Pain: VAS. Function: WOMAC. QoL: SF-36. Kinesiophobia: TSK. | G1: Education (6 sessions of 2 h) CT: Usual care. | G1 improved pain and WOMAC, while CT did not improve VAS and worsened WOMAC at 3 months and 21 months follow-up. |
| Ravaud et al., (2009) | Total: 327. Age: 64.3 (SD 8.3). Inclusion criteria: knee OA. | RCT | Pre- and post-intervention (4 and 12 months). | Pain: NRS. Function: WOMAC. Mental health: SF- 12. | G1: Education + Proposed exercise (through education). CT: Usual care. | G1 showed less pain (−1.65 NRS) than CT at 4 months. G1 showed less pain (−1.35 NRS) and function (−8.67 WOMAC) than CT at 12 months. |
| Allen et al., (2010) | Total: 515. Age: 60.1 (average, SD 10.4 years). Inclusion criteria: knee OA or hip OA. | RCT | Pre- and post-intervention (12 months). | Pain: AIMS scale. Physical function: AIMS2. Mood and tension: AIMS2. Self-efficacy: Arthritis Self-efficacy Scale. | G1: Self-management OA education. G2: General health education. CT: Usual care. | Pain: 0.4 lower G1 than CT, 0.6 lower G1 than G2 (AIMS). Physical function and mood/tension (AIMS2): Not statistically different. The mean AIMS2 walking and bending improved by 0.5 in G1 than G2 at 12 months. Self-efficacy: G1 was 0.4 higher than G2 or CT. |
| Arnold et al., (2010) | Total: 79. Age: 73.2 in G1 (average, SD 4,8), 74.4 in G2 (average, SD 7.5) and 75.8 in CG (average, SD 6.2). Inclusion criteria: hip OA, at least 1 fall risk factor and 65 years or older. | RCT | Pre- and post-intervention (after 11 weeks). | Balance: The Berg Valance Scale. Walking performance: 6-min walk. Functional perdormance: 30-s chair stand. Falls Efficacy: ABC. Dual task function: TUG. Arthritis impact: AIMS-2. | G1: acquatics exercise and education (exercise twice a week and education once a wk for 11 wks). G2: acquatics exercise (twice a week for 11 wks). CG: usual activity for 11 wks. | Arthritis impact: no significant differences between groups (p = 19). Falls efficacy: significant differences between groups in favour of G1. Functional performance: G1 significantly improved in number of chair stands compare with both G2 and CG. Dual task function: G1 showed more significant improvements than G2 and CG. Walking performance: G1 showed significant improvements than G2 and CG. |
| Hansson et al., (2010) | Total: 144. Age: 62 in G1 (average, SD 9.43) and 63 in CG (average, SD 9.51). Inclusion criteria: knee, hip, or hand OA with pain, stiffness, and limitation of ROM. | RCT | Pre- and post-intervention (at 6 months). | Self-care: EQ5D. Usual activities: EQ5D. Pain/discomfort: EQ5D. Anxiety/depression: EQ5D. | G1: Education program. Five sessions, three hours for each session, once a week for five weeks. CG: Living as usual. | G1 showed higher results after 6 months in all the parameters. |
| Bezalel et al., (2010) | Total: 55. Age: 74 in G1 (average, SD 5.1) and 73 in CG (average, SD 5.5). Inclusion criteria: 65 years old or older and knee OA. | RCT | Pre- and post-intervention (4 and 8 weeks). | Pain: WOMAC. Stiffness: WOMAC. Physical function: WOMAC. Physical function: Sit-to-stand test. Physical function: Get-up-and-go test. | G1: Education followed by a self-executed exercise program. Once a week for a month. Each session lasted 45 min. CG: Short wave diathermy for six 20 min sessions. | Pain: significant improvement after 4 weeks and no differences between groups. At follow-up in week 8, the study group continued to improve, while no change was reported for the CG. Physical function: significant improvement after 4 weeks and no differences between groups. At week 8, G1 continued to improve in all outcome parameters, excluding the sit-to-stand test and stiffness variables. |
| Arnold et al., (2011) | Total: 54. Age: >70. Inclusion criteria: hip OA. | RCT | Pre- and post-intervention (11 weeks). | Balance: Berg, Modified Test of Sensory Interaction. Function: TUG, 30-s chair stand. Walking: 6MWT. Falls: ABC scale. Activity level: PASE. | G1: Education + Exercise. (Education: 30 mins/week during 11 weeks). CT: Exercise only. | Intervention group: improvements in terms of risk of falls compared to control. Statistical changes in balance (Modified test of Sensory Interaction) and falls (ABC). Control group: No significant changes with respect to baseline. |
| Somers et al., (2012) | Total: 232. Age: 57.95 (avg, SD 10.41). Inclusion criteria: knee OA. | RCT | Pre- and post-intervention (6 months). | Pain: AIMS. Function: WOMAC. Catastrophizing: PCS. Self-Efficacy: Arthritis Self-Efficacy Scale. | G1: Pain coping skill training. G2: Behavioral weight management. G3: Pain coping skill + Behavioral weight management. CT: Usual care. | Pain (AIMS) and function (WOMAC): patients in G3 showed the lowest pain post-treatment, followed by G1, G2, and CT. Statistical differences between G3 and G2, but not G1. PCS: G3 showed the lowest post-treatment levels, followed by G1, CT, and G2. Statistical differences between G3 and G2, but not G1. Self-Efficacy: patients in G3 showed the lowest pain post-treatment, followed by G1, G2, and CT. |
| Coleman et al., (2012) | Total: 146. Age: 65 (average, SD 8). Inclusion criteria: knee OA. | RCT | Pre- and post-intervention (at 8 weeks and 6 months). | Pain: WOMAC. Physical function: WOMAC. Physical function: SF-36. Physical function: TUG. Role physical: SF-36. Body pain: SF-36. Vitality: SF-36. Social function: SF-36. Knee range of motion: goniometer. Muscle strenght: Kg. | G1: 6 weeks self-management education program on OA, six weekly sessions of 2.5 h. CG: 6 months waiting period before entering the G1 program. | Pain: significant improvement in G1 compared with C Physical function: significant improvement in G1 compared with C. Role physical: there were improvements in G1 compared with CG. Body pain: there were improvements in G1 compared with CG. Vitality: there were improvements in G1 compared with CG. Social function: there were improvements in G1 compared with CG. Knee range of motion: small increases in ROM were observed in G1 compared with C. Muscle strength: G1 showed improvements in quadriceps and hamstring strength during isometric contraction compared with C. |
| Hughes et al., (2014) | Total: 150. Age: 73.5 in G1 (Average, SD 6.75) and 73.7 in G2 (Average, SD 6.32). Inclusion criteria: hip or knee OA with symptoms. | RCT | Pre- and post-intervention (at 2 and 6 months). | Self-Efficacy for Arthritis Self-Management: LSES. Functional Lower Extremity Muscle Strength: timed-stand. Six-Minute Distance Walk: six-min walk test. Pain: WOMAC. Stiffness: WOMAC. Physical function: WOMAC. Exercise Adherence Self-Efficacy: McAuleye. Adherence: King classification. | G1: exercise program (range of motion, resistance, aerobic) and education problem solving regarding self-efficacy for exercise and adherence. Ninety minutes of intervention held three times per week for 8 weeks. The first 60 min of the intervention included exercise and the last 30 min included education. CG: a copy of “the arthritis helpbook” and a list of exercises. | Self-efficacy for Arthritis Self-management: significant difference in favor of G1. Functional lower extremity muscle strength: no significant differences. Six-minute distance walk: significant differences were seen favoring the G1. WOMAC: significant differences favoring G1 were seen in pain and stiffness. Exercise adherence self-efficacy: no significant difference. Adherence: significant differences in G1. |
| Bennell et al., (2014) | Total: 102. Age: 64.5 in G1 (average, SD 8.6) and 62.7 in CG (average, SD 6.4). Inclusion criteria: hip OA, Pain in groin or hip, and Age > 50. | RCT | Pre- and post-intervention (13 and 36 weeks). | Pain: VAS Function: WOMAC | G1: Manual therapy, home exercise, education and advvice. During the follow-up performation of home exercise 3 times/w. CG: Sham intervention included inactive US and inert gel on the hip region. During the follow-up, application of inert gel for 5 min for 3 times/w Physical therapy was applied over 12 weeks; twice in the first week, once weekly for 6 weeks, then approximately once every 2 weeks. The initial two sessions were 45 to 60 min in duration. The remainder was 30 min. | Pain: the between-group differences for changes in pain were not significantly. Mean difference of 6.9 mm in favour of sham therapy. Function: no between-group differences existed for physical function. Mean difference of 1.4 units in favour of sham therapy. Both groups did not show statistically significant improvements in pain and physical function. |
| Saraboon et al., (2015) | Total: 80. Age: 67.5 (average, SD 7.32) in G1 and 67.30 (average, SD 6.30) in CG. Inclusion criteria: knee OA with symptoms and overweight. | RCT | Pre- and post-intervention (at 8weeks). | Knee pain: NRS. Movement ability: time-up-and-go test. ROM: Goniometers measurements Weight. Perception of illness: brief illness representation. Health behavior on OA: Health behavior questionairre | G1: Health education, weight reduction program, and quads exercise training with home-based exercise program. The program was performed for 8 weeks. CG: OA knee booklet and video compact disc. | Knee pain: G1 reported less pain than C. Movement ability: G1 reported better movements than C. ROM: G1 reported better ROM than C. Weight: lower body weights after G1 than C. Perception of illness: Participants in G1 shows better result than C. Health behaviour on OA: participants in G1 showed better results than participants in CG. |
| Bennell et al., (2018) | Total: 144. Age: >61. Inclusion criteria: hip OA. | RCT | Pre- and post-intervention (8 weeks, 24 weeks, 52 weeks). | Pain: NRS. Function: WOMAC. QoL: AQoLv2. Catastrophizing: PCS. | G1: PCST + Education + Exercise. CT: Education + Exercise. | G1 provided no better clinical outcomes than CT in terms of pain and function at 24–52 weeks. |
| Lawford et al., (2018) | Total: 148. Age: >60. Inclusion criteria: knee OA. | RCT | Pre- and post-intervention (3 months, 9 months). | Pain: NRS. Function: WOMAC. | G1: Education + PCST + Internet-based exercise. CT: Education. | No differences in terms of pain except for employment patients, which patients in G1 showed less pain at 3 months follow-up. No differences between groups in terms of function at any follow-up. |
| Ganji et al., (2018) | Total: 82. Age: >60. Inclusion criteria: knee OA. | RCT | Pre- and post-intervention (8 weeks after). | Pain: VAS. | G1: Education. CT: Usual care. Education: 60′/2 per week, for 3 weeks. | G1 diminished pain after intervention and 8 especially 8 weeks after the intervention in comparison with the CT. |
| Lluch et al., (2018) | Total: 44. Inclusion criteria: Knee OA, pain of more than 3 months, and scheduled to undergo total knee replacement. | RCT | Pre-intervention, post-intervention (immediately and after 1 month), and post-surgery (3 months). | Conditioned pain modulation: Catchart protocol Pressure pain thresholds: Fisher algometers Temporal summation: Catchart protocol Symptoms of central sensitization: CSI questionnaire Knee pain: WOMAC Disability: WOMAC Physicosocial variables and pain catastrophizing: PCS Kinesiophobia: TSK-11 | G1: Pain neuroscience education and knee joint mobilization. CG: Biomedical education and knee joint mobilization. | Conditioned pain modulation: only significant change was observed for the experimental treatment between baseline CMP value and the value measured at 3 months post-surgery. Temporal summation: no changes over time. Pressure pain thresholds: it did not differ between treatments but changed over time. For both treatments, there was a significant increase in PPT at all locations immediately post-treatment, at 1 month after treatment, and at 3 months after surgery. Symptoms of central sensitization: improved over time in both groups when measured at 3 months post-surgery with no difference between treatments. Pain: improvements in both groups but no differences between G1 and C. Disability: improvements in both groups but no differences between G1 and C. Physical and social variables: improvements in experimental group at 3 months post-surgery, immediately post treatment and at 1 month after treatment. Signficantly lower values of PCS were seen with the experimental compared to control treatment. |
| Allen et al., (2019) | Total: 248. Age: 59 (average, SD 10.3 years). Inclusion criteria: African Americans, knee or hip symptomatic OA. | RCT | Pre- and post-intervention (3 and 9 months). | Pain: WOMAC Function: WOMAC Coping strategies: CSQ Pain Catastrophizing: PCS Arthritis Self Efficacy: ASES Physical Activity Survey: YPAS Patient Global Impression of Arthritis Symptom Change | G1: Pain coping skills training. CG: usual care. | Pain: no differences between G1 and CG. Function: no differences between G1 and CG. Coping strategies: significant improvements in G1. Pain catastrophizing: significant improvements in G1. Arthritis self-efficacy: better improvements in G1. Physical activity survey: no differences between groups. Patient global impression of symptoms: better improvements in G1. |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Sinatti, P.; Sánchez Romero, E.A.; Martínez-Pozas, O.; Villafañe, J.H. Effects of Patient Education on Pain and Function and Its Impact on Conservative Treatment in Elderly Patients with Pain Related to Hip and Knee Osteoarthritis: A Systematic Review. Int. J. Environ. Res. Public Health 2022, 19, 6194. https://doi.org/10.3390/ijerph19106194
Sinatti P, Sánchez Romero EA, Martínez-Pozas O, Villafañe JH. Effects of Patient Education on Pain and Function and Its Impact on Conservative Treatment in Elderly Patients with Pain Related to Hip and Knee Osteoarthritis: A Systematic Review. International Journal of Environmental Research and Public Health. 2022; 19(10):6194. https://doi.org/10.3390/ijerph19106194
Chicago/Turabian StyleSinatti, Pierluigi, Eleuterio A. Sánchez Romero, Oliver Martínez-Pozas, and Jorge H. Villafañe. 2022. "Effects of Patient Education on Pain and Function and Its Impact on Conservative Treatment in Elderly Patients with Pain Related to Hip and Knee Osteoarthritis: A Systematic Review" International Journal of Environmental Research and Public Health 19, no. 10: 6194. https://doi.org/10.3390/ijerph19106194
APA StyleSinatti, P., Sánchez Romero, E. A., Martínez-Pozas, O., & Villafañe, J. H. (2022). Effects of Patient Education on Pain and Function and Its Impact on Conservative Treatment in Elderly Patients with Pain Related to Hip and Knee Osteoarthritis: A Systematic Review. International Journal of Environmental Research and Public Health, 19(10), 6194. https://doi.org/10.3390/ijerph19106194