
What Competencies Does a Community Occupational Therapist Need in Neurorehabilitation? Qualitative Perspectives

 , and
, and
Abstract
1. Introduction
1.1. Neurological Disease and Occupation
1.2. Competencies in Occupational Therapy
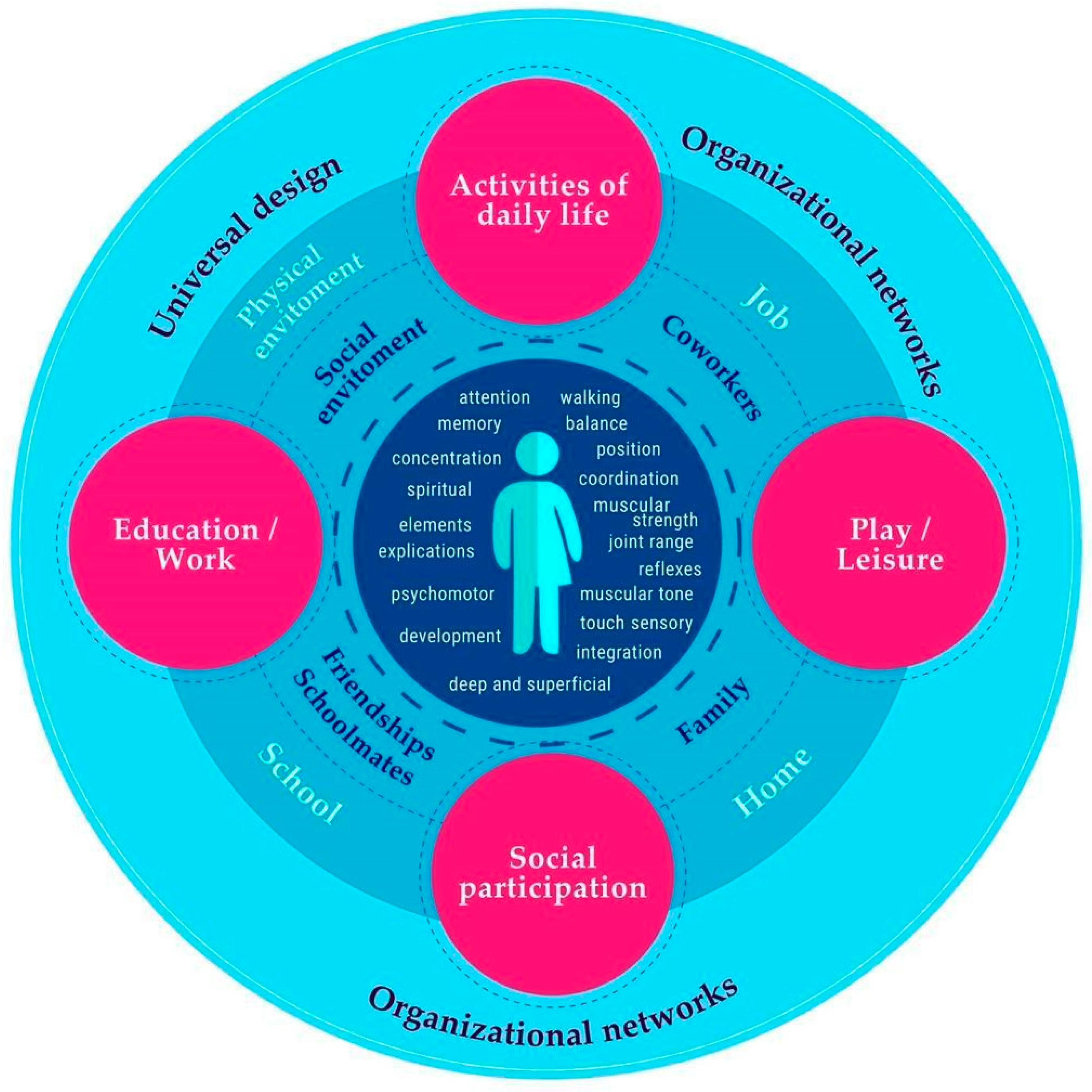
1.3. Community Occupational Therapy
1.4. Experiences of Community Occupational Therapy
2. Materials and Methods
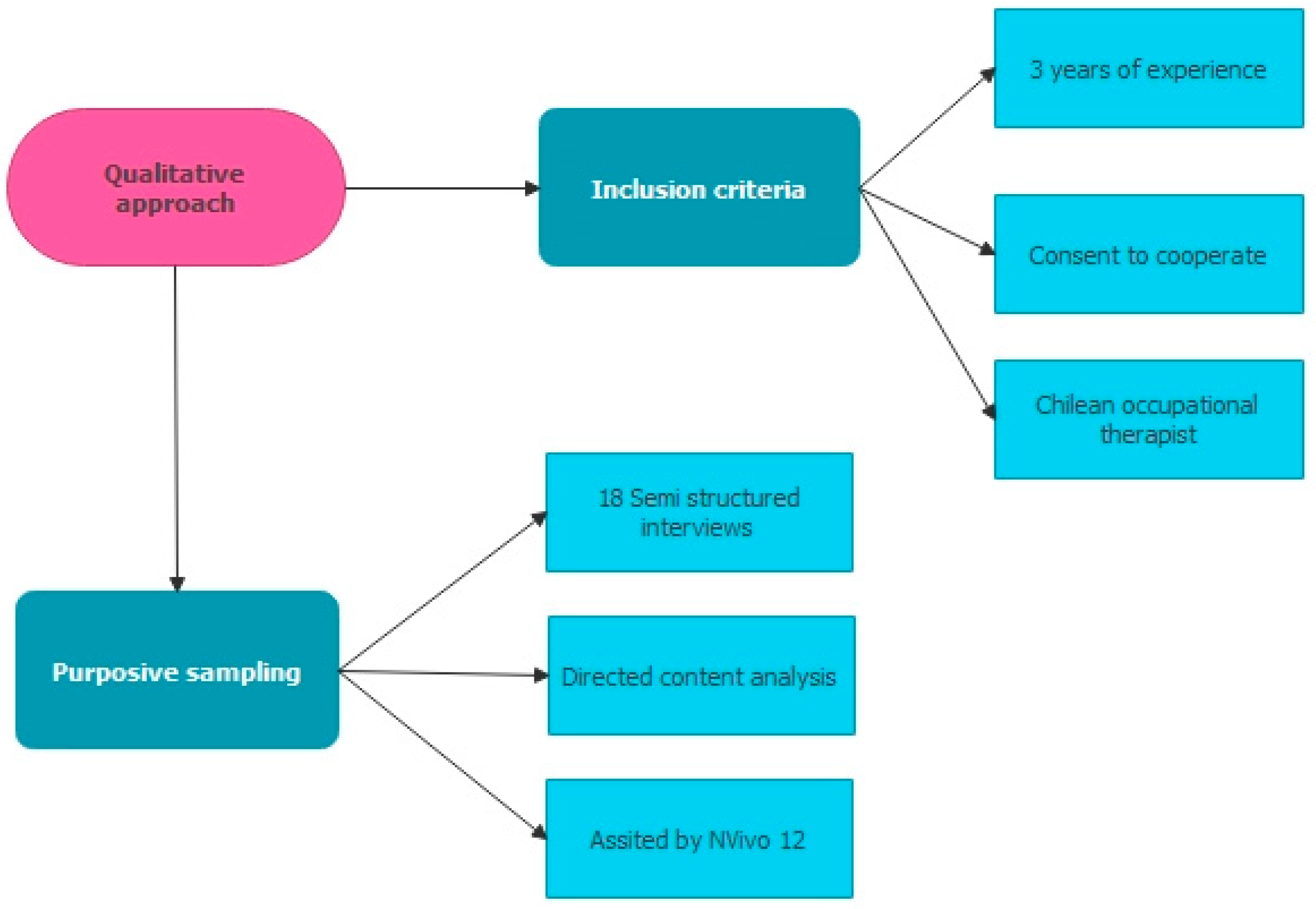
2.1. Study Design
2.2. Research Context
2.3. Participants
2.4. Data Collection
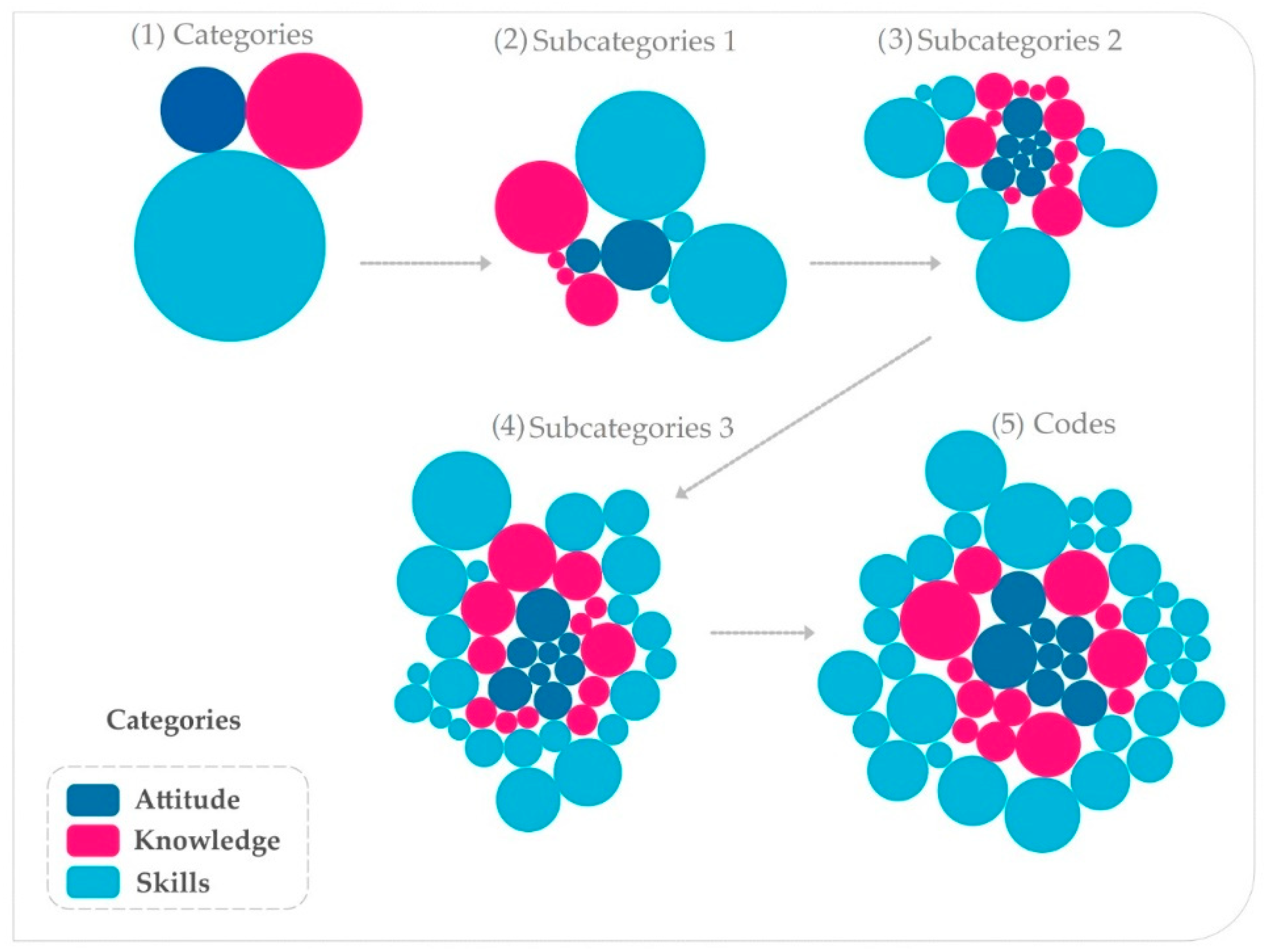
2.5. Data Analysis
2.6. Ethical Statement
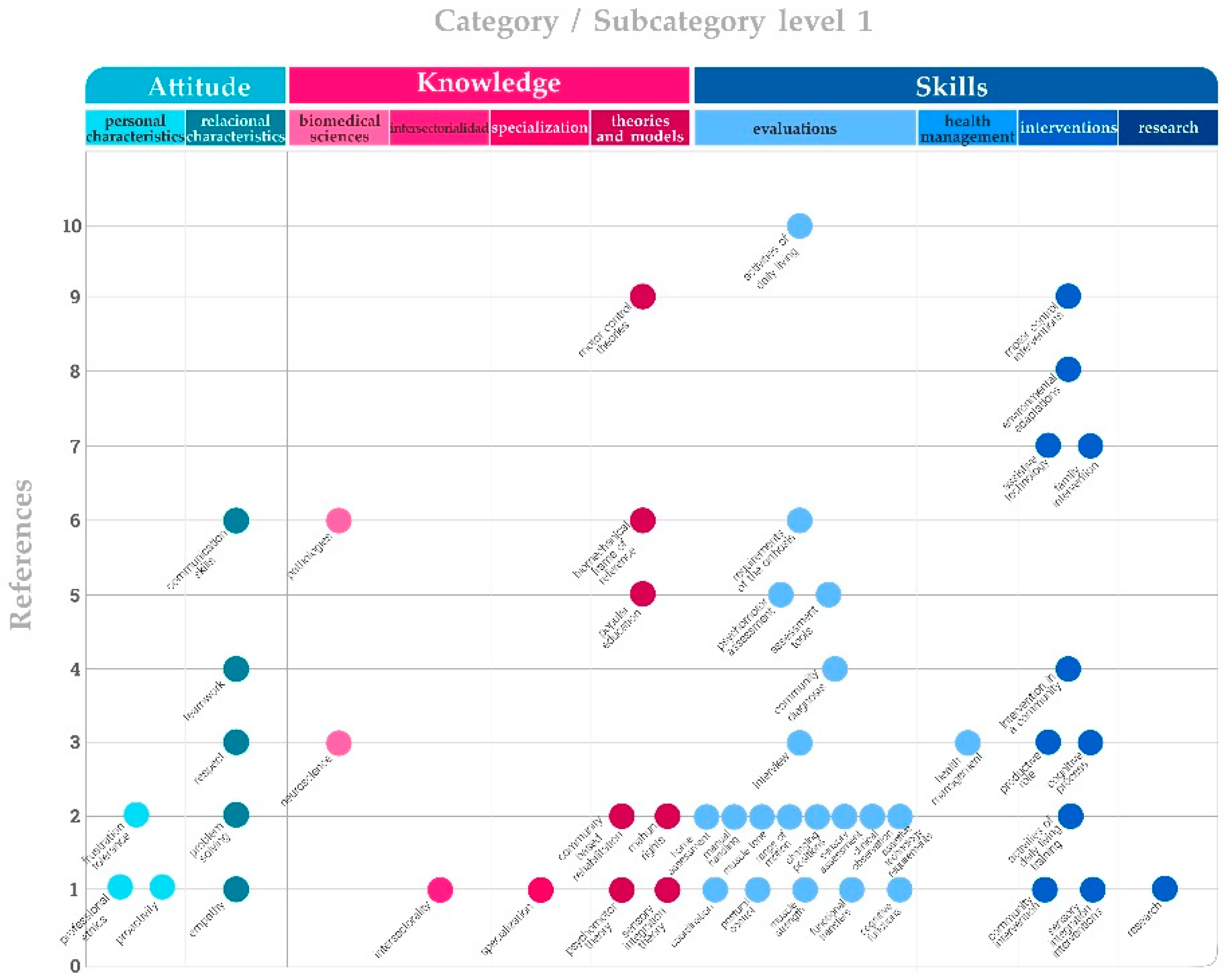
3. Results
3.1. Knowledge
‘The first thing is knowledge of the main neurological pathologies, such as hemiplegia, cerebrovascular accidents, head injuries, Parkinson’s disease, etc.’‘To know all the structures and functions of the central, peripheral, and autonomic nervous system.’
‘It is important for neurorehabilitation to know about motor control, activity-oriented motor learning, neuronal plasticity, neuromuscular facilitation, the Bobath concept, which is the one that is most used.’‘You need to know about the biomechanical model, about biomechanics as such, to know the angles of the body, the principles of orthotics for making orthoses.’
‘In pediatrics, knowledge of psychomotor development will provide guidelines and directives for intervention.’‘Theories of play and how children relate at a certain age, how they play at a certain age, why we decide to give them one toy and not another.’‘The issue of sensory integration is also important to understand some behaviors of children.’
‘We use Paulo Freire’s strategies a lot, in other words, in this sense, popular education is an essential tool for us.’‘I believe that the main thing is that occupational therapists themselves, as they are socio-community professionals, should work based on the network model, strengthening people’s networks and the health area from a functional rehabilitation point of view, with a human rights vision, I believe that this is fundamental.’‘Intersectoriality is a very important issue because even though it can be a primary health care device, it has to do with the intersectoral, like, for example, the community-based rehabilitation strategy, which is a Primary Health Care strategy.’
‘The whole world does groups and workshops, but they don’t know how they do it and where they get it or how they have been informed, and the same applies to community work. Now all the occupational therapists think they are community, but they don’t specialize in the area.’
3.2. Skills
‘Assessment guidelines should be managed to look at skills, manipulation as such; assessment guidelines for activities of daily living, postural control, joint range, muscle strength, muscle tone, turns, transfers, transitions, manual functionality, coordination, technical aids, and orthotics requirements and cognitive functions.’
‘In pediatrics, you need knowledge of psychomotor development, motor development tests such as the Bayley Scale, the VMI, and sensory integration guidelines. It is required to have mastery of therapeutic play techniques, of how children of a certain age relate to each other, how to give them one type of toy or another, how to adapt it to their needs.’
‘One must evaluate the dynamics of the parents since they are the ones who must replicate the therapies at home, as well as the knowledge about the pathology, the school, and the architectural barriers that are found in the spaces where the patient develops.’‘The first stage mentioned in the diagnosis is to get to know each other, to get to know the community, who are part of, and this implies recognizing each other, where they come from, what their interests are, aspects that are basic to human communication and occupational therapy.’
‘Treatment sessions where we work on training skills such as independence and indications of daily living, and training in technical aids, so it is often necessary to work previously on postural control, passive mobilization, manual functionality, muscle activity, and cognitive stimulation.’‘Technical aids such as wheelchair training, transfer from bed to chair and from chair to shower, going up and down sidewalks. We take the patient out of the clinic to go shopping, take the elevator, go to the mall, university, school, work, and address architectural barriers that may arise.’
‘The intervention processes have to do with empowering the collective as a space for daily life, training, spaces of struggle, spaces of liberation, it is privileged, that is, being a citizen to the extent that you are part of a community, you are included, or you generate processes of inclusion in communities.’
‘The entire process of managing both resources and coordination with other programs is important.’‘Evidence-based occupational therapy is the class for neurorehabilitation processes as much from the clinical as from the community.’
3.3. Attitude
‘The most important thing in neurorehabilitation is teamwork. It is fundamental. And being able to listen to what the patient needs and wants, what motivations he has, being able to take these motivations and then move toward therapeutic goals.’
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- World Health Organization. Neurological Disorders. Challenges for Public Health; World Health Organization, Ed.; World Health Organization: Ginebra, Switzerland, 2015. [Google Scholar]
- United Nations Nearly 1 in 6 of World’s Population Suffer from Neurological Disorders. Available online: https://news.un.org/es/story/2007/02/1098731 (accessed on 3 January 2022).
- Fernández, R.; Urteaga, G.; Agorreta, E.; Durán, P. Intervención del Terapeuta Ocupacional en Patología Neurológica y/o Disfunción Física; Cotona Nalte: Pamplona, Spain, 2016; 25p. [Google Scholar]
- Neumann-Collyer, V.E.; Hernández-Pérez, K.A.; Pohl-Montt, P.G. Design of a performance evaluation instrument for the activities of daily living Vivian. Rev. Salud Publica 2018, 20, 554–559. [Google Scholar] [CrossRef] [PubMed]
- Hernández Lozano, D.; Fernández Hawrylak, M.; Grau Rubio, C. Occupational therapy in Huntington’s disease: Prolonging the autonomy. Rev. Electrónica Ter. Ocup. Galicia TOG 2014, 11, 8. [Google Scholar]
- Pan American Health Organization. Core Competencies for Public Health: A Regional Framework for the Americas; United Recurs; Unit of Human Resources for Health, Bioethics and Research Department of Health System and Services (HSS), Department of Health and Health Services: Washington, DC, USA, 2013; 5p. [Google Scholar]
- Charumbira, M.Y.; Berner, K.; Louw, Q.A. Research competencies for undergraduate rehabilitation students: A scoping review. Afr. J. Health Prof. Educ. 2021, 13, 52. [Google Scholar] [CrossRef]
- World Federation of Occupational Therapy. Definitions of Occupational Therapy. World Fed. Occup. Ther. 2019, 1–68. [Google Scholar] [CrossRef]
- Canadian Association of Occupational Therapists. Profile of Practice of Occupational Therapists; Canadian Association of Occupational Therapists, Ed.; Primera; Canadian Association of Occupational Therapists: Ottawa, ON, Canada, 2012. [Google Scholar]
- Ministerio de Salud y Protección. Social y Colegio Colombiano de Terapia Ocupacional Perfil profesional y Competencias del Terapeuta Ocupacional. 2014; pp. 1–18. Available online: https://www.minsalud.gov.co/sites/rid/Lists/BibliotecaDigital/RIDE/VS/TH/perfil-competencias-terapeuta-ocupacional.pdf (accessed on 3 January 2022).
- Marshall, C.A.; Cooke, A.; Gewurtz, R.; Barbic, S.; Roy, L.; Lysaght, R.; Kirsh, B. Competencies for occupational therapy practice in homelessness: A Delphi study. Scand. J. Occup. Ther. 2021, 1–15. [Google Scholar] [CrossRef]
- Agencia de Calidad Sanitaria de Andalucía. Manual de Competencias Profesionales: Terapeuta Ocupacional. 2015, pp. 1–86. Available online: https://www.sspa.juntadeandalucia.es/agenciadecalidadsanitaria/archivo/MACP-Terapeuta-Ocupacional.pdf (accessed on 3 January 2022).
- Fields, S.M.; Unsworth, C.A.; Harreveld, B. The revision of competency standards for occupational therapy driver assessors in Australia: A mixed methods approach. Aust. Occup. Ther. J. 2021, 68, 257–271. [Google Scholar] [CrossRef]
- Zango, I. Terapia Ocupacional Comunitaria; Proyecto Editorial Terapia Ocupacional, Ed.; Primera; Editorial Síntesis: Madrid, Spain, 2017. [Google Scholar]
- World Federation of Occupational Therapy. Occupational Therapy and Community Centred Practice. 2019, pp. 1–2. Available online: https://www.wfot.org/resources/occupational-therapy-and-community-centred-practice (accessed on 5 January 2022).
- Martínez, V. El Enfoque Comunitario: El Desafio de Incorporar a las Comunidades en las Intervenciones Sociales; Universidad de Chile, Ed.; Universida; Universidad de Chile: Santiago, Chile, 2006. [Google Scholar]
- Guajardo, A.; Recabarren, E.; Parraguez, V. Rehabilitación de Base Comunitaria: Diálogos, Reflexiones y Prácticas en Chile; Guajardo, A., Recabarren, E., Parraguez, V., Eds.; Primera; Senadis y Universidad Andres Bello: Santiago, Chile, 2014; ISBN 9789567247783. [Google Scholar]
- Laymon, B.P.; Chudgar, R.; Huang, T.; Kulkarni, M.; Holtgrave, P.L.; Gore, K. Partnering on the Social Determinants of Health with the Community Health Improvement Matrix. J. Public Health Manag. Pract. 2021, 27, 459–463. [Google Scholar] [CrossRef]
- Scaffa, M.E. Occupational therapy interventions for groups, communities, and populations. In Willard and Spackman’s Occupational Therapy; Schell, B.A., Gillen, G., Scaffa, M., Cohn, E.S., Eds.; Lippincott Williams & Wilkins: Philadelphia, PA, USA, 2018; pp. 436–447. [Google Scholar]
- Iwama, M.; Simó Algado, S. Aspectos de significado, cultura e inclusión en Terapia Ocupacional. Rev. Electrónica Ter. Ocup. Galicia TOG 2008, 5, 1–23. [Google Scholar]
- Johnston, M.V.; Goverover, Y.; Dijkers, M. Community activities and individuals’ satisfaction with them: Quality of life in the first year after traumatic brain injury. Arch. Phys. Med. Rehabil. 2005, 86, 735–745. [Google Scholar] [CrossRef]
- de la Salud, O.M. Rehabilitación Basada en la Comunidad. Guías Para la RBC; Khhasnabis, C., Heinicke, K., Eds.; Ediciones; Organización Mundial de la Salud: Ginebra, Switzerland, 2012. [Google Scholar]
- Dudgeon, B. Community Integration. In Willard & Spackman’s Occupational Therapy; Willard, H.S., Crepeau, E.B., Cohn, E.S., Spackman, C.S., Schell, B.A.B., Eds.; Willard and Spackman’s Occupational Therapy; Wolters Kluwer Health/Lippincott Williams & Wilkins: Philadelphia, PA, USA, 2009; pp. 181–191. ISBN 9780781760041. [Google Scholar]
- Ulloa, F.; Pino, J. Perspectiva Crítica Desde Latinoamérica: Hacia una Desobediencia Epistémica en Terapia Ocupacional Contemporánea. Cad. Ter. Ocup. UFSCar 2016, 24, 421–427. [Google Scholar] [CrossRef]
- Farias, M.N.; Lopes, R.E. Occupational therapy and Paulo Freire: A scoping review. Braz. J. Occup. Ther. 2022, 30, 1–20. [Google Scholar] [CrossRef]
- Gontijo, D.T.; Santiago, M.E. Terapia Ocupacional e Pedagogia Paulo Freire: Configurações do encontro na produção científica nacional. Reflexão Ação 2018, 26, 132–148. [Google Scholar] [CrossRef]
- Sikkes, S.A.M.; Tang, Y.; Jutten, R.J.; Wesselman, L.M.P.; Turkstra, L.S.; Brodaty, H.; Clare, L.; Cassidy-Eagle, E.; Cox, K.L.; Chételat, G.; et al. Toward a theory-based specification of non-pharmacological treatments in aging and dementia: Focused reviews and methodological recommendations. Alzheimer’s Dement. 2021, 17, 255–270. [Google Scholar] [CrossRef] [PubMed]
- Vibholm, A.P.; Christensen, J.R.; Pallesen, H. Nature-based rehabilitation for adults with acquired brain injury: A scoping review. Int. J. Environ. Health Res. 2020, 30, 661–676. [Google Scholar] [CrossRef] [PubMed]
- Öst Nilsson, A.; Johansson, U.; Ekbladh, E.; Bernspång, B.; Hellman, T.; Eriksson, G. Work potential and work performance during the first try-out of the person-centred return to work rehabilitation programme rework-stroke: A case study. Healthcare 2020, 8, 454. [Google Scholar] [CrossRef]
- Gharib, M.; Shayesteh Azar, M.; Vameghi, R.; Hosseini, S.A.; Nobakht, Z.; Dalvand, H. Relationship of Environmental Factors With Social Participation of Children With Cerebral Palsy Spastic Diplegia: A Preliminary Study. J. Rehabil. 2021, 21, 422–435. [Google Scholar] [CrossRef]
- Kendall, M.; Harre, D.; Schuurs, S.; Hinchy, K.; Booth, S. Returning to rural communities following transitional rehabilitation after spinal cord injury. Aust. J. Rural Health 2021, 29, 572–577. [Google Scholar] [CrossRef]
- Ministerio de Salud. Orientaciones Para la Implementación del Modelo de Atención Integral de Salud Familiar y Comunitario; Ministerio de Salud: Región Metropolitana de Santiago, Chile, 2012; pp. 1–143. [Google Scholar]
- Powell, J.; Heslin, J.; Greenwood, R. Community based rehabilitation after severe traumatic brain injury: A randomised controlled trial. J. Neurol. Neurosurg. Psychiatry 2002, 72, 193–202. [Google Scholar] [CrossRef]
- Ryan, T.; Enderby, P.; Rigby, A.S. A randomized controlled trial to evaluate intensity of community-based rehabilitation provision following stroke or hip fracture in old age. Clin. Rehabil. 2006, 20, 123–131. [Google Scholar] [CrossRef]
- Coetzer, R. Holistic neuro-rehabilitation in the community: Is identity a key issue? Neuropsychol. Rehabil. 2008, 18, 766–783. [Google Scholar] [CrossRef]
- Yu, J.J.; Hu, Y.S.; Wu, Y.; Chen, W.H.; Zhu, Y.L.; Cui, X.; Lu, W.B.; Qi, Q.; Qu, P.Y.; Shen, X.H. The effects of community-based rehabilitation on stroke patients in China: A single-blind, randomized controlled multicentre trial. Clin. Rehabil. 2009, 23, 408–417. [Google Scholar] [CrossRef]
- Guajardo, A.; Recabarren-Hernández, E.; Asún Salazar, D.; Zamora-Astudillo, C.; Cottet-Soto, P. Evaluación de la estrategia de rehabilitación de base comunitaria (RBC) desde la perspectiva de la comunidad y los equipos locales de rehabilitación. Rev. La Fac. Med. 2015, 63, 41–50. [Google Scholar] [CrossRef]
- González-Bernal, J.J.; Eiguren-Munitis, L.; González-Santos, J.; Santamaría-Peláez, M.; Soto-Cámara, R.; Rodríguez-Fernández, P. Effectiveness of community occupational therapy intervention in, with and from the community in people with disabilities in Azrou (Morocco). Int. J. Environ. Res. Public Health 2021, 18, 5602. [Google Scholar] [CrossRef] [PubMed]
- Bianchi, P.; Serrata, A. Professional practice of occupational therapist in Latin American countries: What characterizes a territorial-community action? Cad. Bras. Ter. Ocup. 2022, 30, 1–23. [Google Scholar] [CrossRef]
- Hernández, R.; Fernández, C.; Baptista, P. Metodología de la Investigación; Chacón, J., Ed.; Quinta; Mc Graw Hill: Contadero, Mexico, 2010; ISBN 9786071502919. [Google Scholar]
- Gibbs, G. Analyzing Qualitative Data, 2nd ed.; Flick, U., Ed.; SAGE Publishing: London, UK, 2018. [Google Scholar]
- Strauss, A.; Corbin, J. Basics of Qualitative Research and Procedures for Developing Grpunded Theory, 2nd ed.; Sage: Thousand Oaks, CA, USA, 1998. [Google Scholar]
- Sandoval Casilimas, C. Investigación Cualitativa: Programa de Especialización en Teoría, Métodos y Técnicas de Investigación Social; Instituto Colombiano para el fomento de la educación superior, ICFES: Bogotá, Colombia, 1996; ISBN 9589329098. [Google Scholar]
- World Federation of Occupational Therapy. Human Resources Project. Available online: https://www.google.com/maps/d/viewer?mid=1kTWZHTDCk-lrbthSP-qoSWq4u38&ll=-19.42328547731865%2C-52.33822827332851&z=4 (accessed on 18 April 2022).
- Subsecretaría de Redes Asistenciales. Redes de Rehabilitación 2013; Primera; Ministerio de Salud: Santiago, Chile, 2013. [Google Scholar]
- Mang, C.S.; Peters, S. Advancing motor rehabilitation for adults with chronic neurological conditions through increased involvement of kinesiologists: A perspective review. BMC Sports Sci. Med. Rehabil. 2021, 13, 132. [Google Scholar] [CrossRef]
- Flick, U. Designing Qualitative Research; Qualitative Research Kit; SAGE Publications: London, UK, 2018; ISBN 9781473911987. [Google Scholar]
- Hsieh, H.-F.; Shannon, S. Three Approaches to Qualitative Content Analysis. Qual. Health Res. 2005, 15, 1277–1288. [Google Scholar] [CrossRef]
- Kvale, S.; Brinkmann, S. Interviews: Learning the Craft of Qualitative Research Interviewing; SAGE Editions: London, UK, 2014. [Google Scholar]
- MacQueen, K.M.; McLellan, E.; Kay, K.; Milstein, B. Codebook Development for Team-Based Qualitative Analysis. Field Methods 1998, 10, 31–36. [Google Scholar] [CrossRef]
- Gómez, G.R.; Flores, J.G.; Jiménez, E.G. Metodología de la Investigación Cualitativa; Ediciones Aljibe: Málaga, Spain, 1996. [Google Scholar]
- Freburger, J.K.; Li, D.; Fraher, E.P. Community Use of Physical and Occupational Therapy After Stroke and Risk of Hospital Readmission. Arch. Phys. Med. Rehabil. 2018, 99, 26–34.e5. [Google Scholar] [CrossRef]
- Scrivener, K.; Dorsch, S.; McCluskey, A.; Schurr, K.; Graham, P.L.; Cao, Z.; Shepherd, R.; Tyson, S. Bobath therapy is inferior to task-specific training and not superior to other interventions in improving lower limb activities after stroke: A systematic review. J. Physiother. 2020, 66, 225–235. [Google Scholar] [CrossRef]
- Novak, I.; Mcintyre, S.; Morgan, C.; Campbell, L.; Dark, L.; Morton, N.; Stumbles, E.; Wilson, S.A.; Goldsmith, S. A systematic review of interventions for children with cerebral palsy: State of the evidence. Dev. Med. Child Neurol. 2013, 55, 885–910. [Google Scholar] [CrossRef]
- Martínez Clares, P.; Martínez Juárez, M.; Muñoz Cantero, J.M. Formación basada en competencias en educación sanitaria: Aproximaciones a enfoques y modelos de competencia. Reli. Rev. Electron. Investig. Eval. Educ. 2008, 14, 1–23. [Google Scholar] [CrossRef][Green Version]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Participant | Sex | Age | Care Population Type | Care | Device Type |
|---|---|---|---|---|---|
| 1 | Female | 34 | Juvenile/Adult/Senior | Primary | Public |
| 2 | Female | 31 | Juvenile | Secondary/Tertiary | Public |
| 3 | Female | 35 | Juvenile/Adult/Senior | Primary | Public |
| 4 | Male | 26 | Juvenile/Adult/Senior | Primary | Public |
| 5 | Male | 32 | Adult/Senior | Primary | Public |
| 6 | Female | 40 | Adult/Senior | Secondary | Private |
| 7 | Female | 55 | Juvenile/Adult/Senior | Secondary | Private |
| 8 | Female | 36 | Juvenile/Adult/Senior | Primary | Public |
| 9 | Female | 46 | Juvenile/Adult/Senior | Primary | Public |
| 10 | Male | 26 | Juvenile/Adult/Senior | Primary | Public |
| 11 | Female | 35 | Adult/Senior | Secondary | Private |
| 12 | Female | 31 | Adult/Senior | Secondary | Private |
| 13 | Male | 42 | Juvenile/Adult/Senior | Primary | Public |
| 14 | Female | 31 | Juvenile/Adult/Senior | Primary | Public |
| 15 | Female | 44 | Juvenile | Secondary/Tertiary | Private |
| 16 | Female | 42 | Juvenile | Secondary/Tertiary | Private |
| 17 | Female | 33 | Adult | Secondary | Private |
| 18 | Female | 41 | Adult | Secondary | Private |
| Dimension | Questions |
|---|---|
| Knowledge | What theories or models do you habitually use? What knowledge should an occupational therapist have when working in neurorehabilitation? What theoretical background do you associate with community work? |
| Skills | What procedures do you habitually do? What type of evaluations do you use in your practice? How do you do them? Can you describe the interventions you typically do? How do you link your intervention with community space? What community actions do occupational therapists do in your workspace? |
| Attitudes | What values predominate in OT practice in your area? What attitudes do you believe to be essential for your neurorehabilitation work |
| Type | Main Competencies |
|---|---|
| Theoretical knowledge | Neuroscience Pathologies Biomechanical Frame of Reference Sensory Integration Theory Psychomotor Theory Community-Based Rehabilitation Human Rights Popular Education Social Network Theory |
| Procedural content | Environmental Assessment Sensorimotor Functions Psychomotor Assessment Sensory Assessment Interview Clinical Observation Psychomotor Assessment Sensory Assessment Interview Clinical Observation Assessment Tools |
| Attitudinal content | Empathy Communication Skills Problem Resolution Respect Teamwork Frustration Tolerance Professional Ethics Proactivity |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Avello-Sáez, D.; Helbig-Soto, F.; Lucero-González, N.; Fernández-Martínez, M.d.M. What Competencies Does a Community Occupational Therapist Need in Neurorehabilitation? Qualitative Perspectives. Int. J. Environ. Res. Public Health 2022, 19, 6096. https://doi.org/10.3390/ijerph19106096
Avello-Sáez D, Helbig-Soto F, Lucero-González N, Fernández-Martínez MdM. What Competencies Does a Community Occupational Therapist Need in Neurorehabilitation? Qualitative Perspectives. International Journal of Environmental Research and Public Health. 2022; 19(10):6096. https://doi.org/10.3390/ijerph19106096
Chicago/Turabian StyleAvello-Sáez, Daniela, Fabiola Helbig-Soto, Nayadet Lucero-González, and María del Mar Fernández-Martínez. 2022. "What Competencies Does a Community Occupational Therapist Need in Neurorehabilitation? Qualitative Perspectives" International Journal of Environmental Research and Public Health 19, no. 10: 6096. https://doi.org/10.3390/ijerph19106096
APA StyleAvello-Sáez, D., Helbig-Soto, F., Lucero-González, N., & Fernández-Martínez, M. d. M. (2022). What Competencies Does a Community Occupational Therapist Need in Neurorehabilitation? Qualitative Perspectives. International Journal of Environmental Research and Public Health, 19(10), 6096. https://doi.org/10.3390/ijerph19106096