
Comparisons of the Prevalence, Severity, and Risk Factors of Dysmenorrhea between Japanese Female Athletes and Non-Athletes in Universities

 ,
,  ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
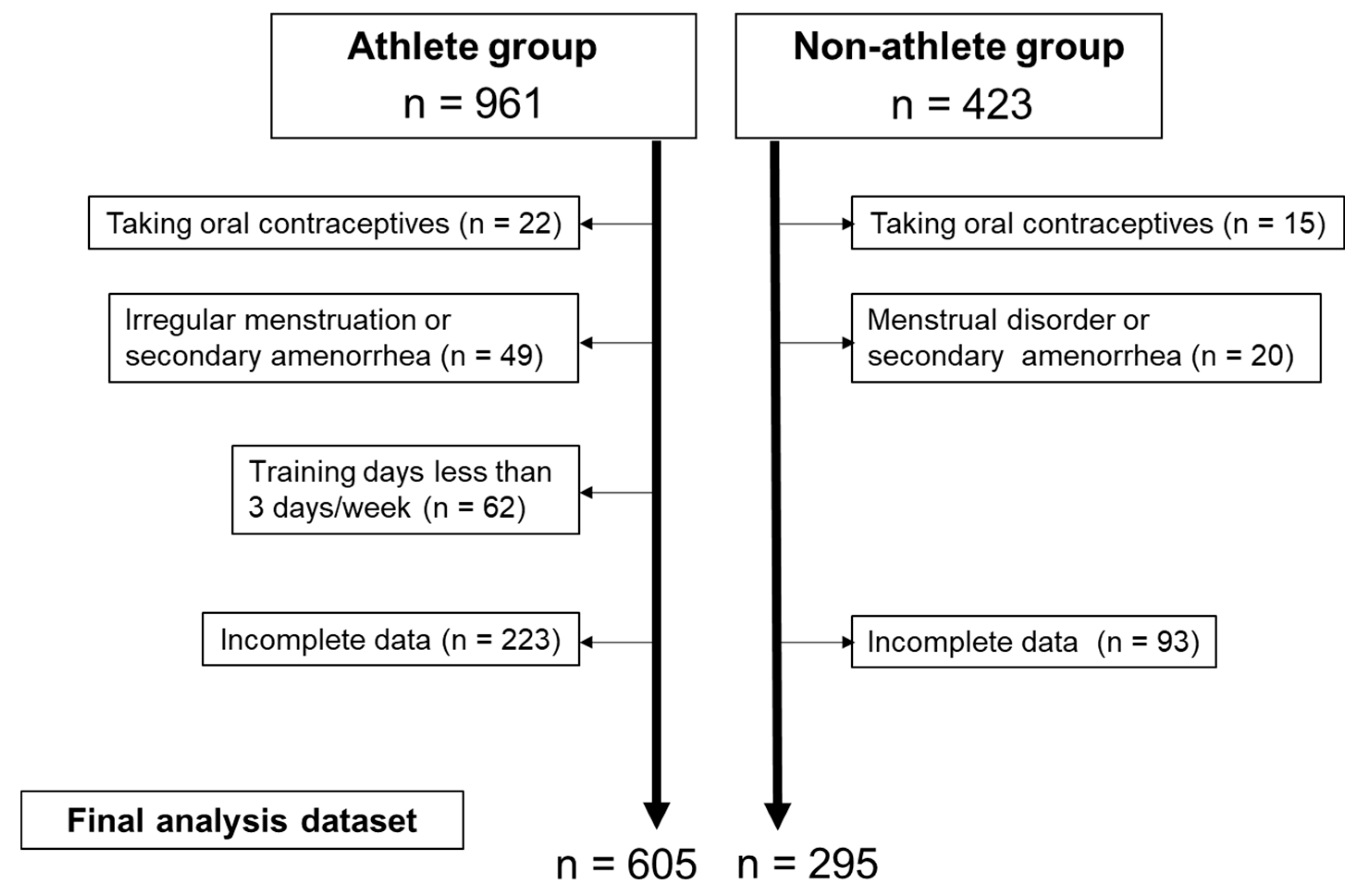
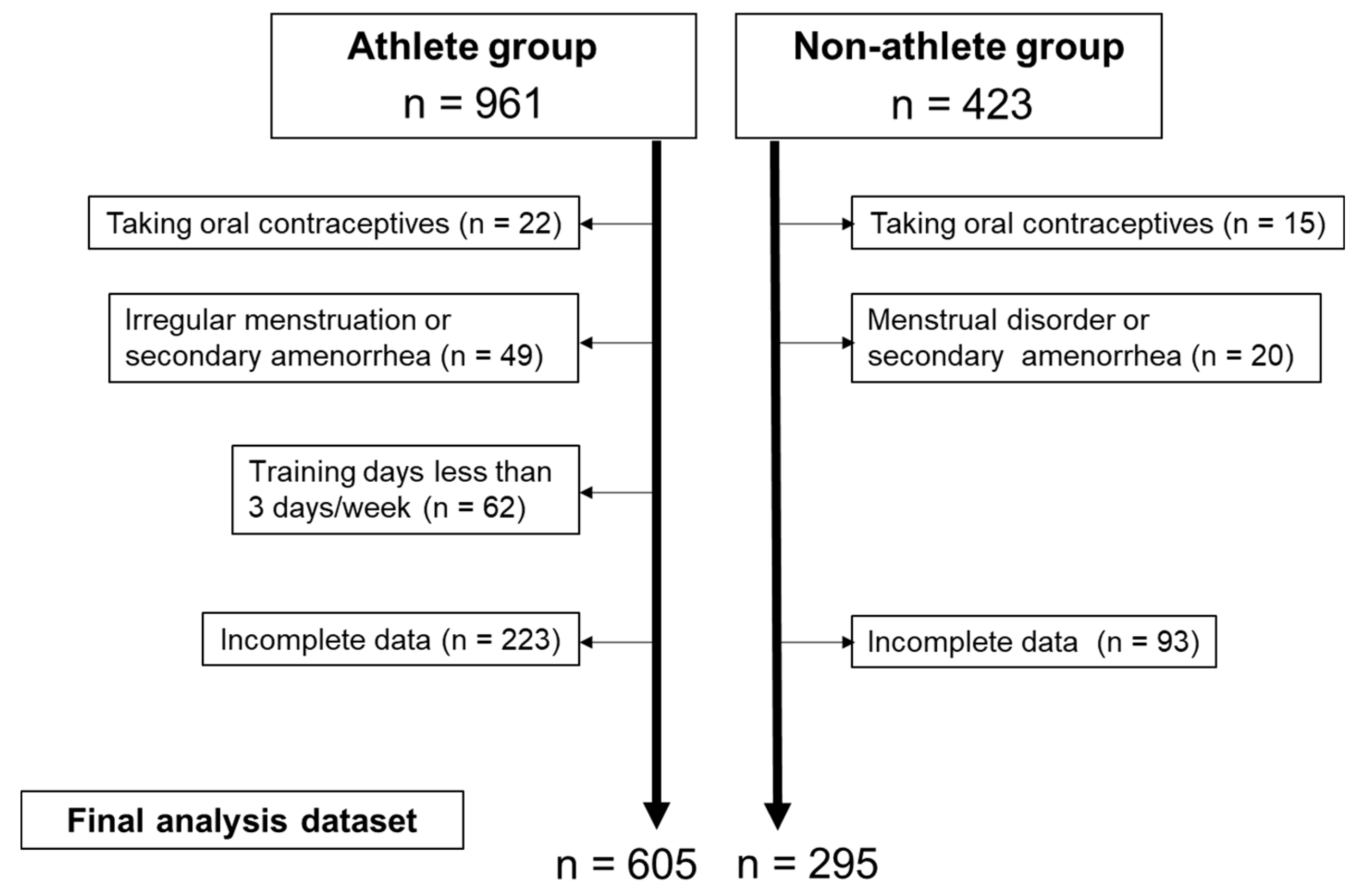
2.2. Participants
2.3. Questionnaire
2.4. Statistical Analysis
3. Results
3.1. Participant Characteristics
3.2. Dysmenorrhea Severity
3.3. Factors Related to Severe Dysmenorrhea
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Sultan, C.; Gaspari, L.; Paris, F. Adolescent dysmenorrhea. Endocr. Dev. 2012, 22, 171–180. [Google Scholar] [PubMed]
- Zaiei, S.; Faghihzadeh, S.; Sohrabvand, F.; Lamyian, M.; Emamgholy, T. A randomised placebo-controlled trial to determine the effect of vitamin E in treatment of primary dysmenorrhoea. BJOG 2001, 108, 1181–1183. [Google Scholar]
- Nohara, M.; Momoeda, M.; Kubota, T.; Nakabayashi, M. Menstrual cycle and menstrual pain problem and related risk factors among Japanese workers. Ind. Health 2011, 49, 228–234. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ameade, K.P.E.; Amalba, A.; Mohammed, S.B. Prevalence of dysmenorrhea among university students in Northern Ghana, its impact and management strategies. BMC Women’s Health 2018, 18, 39. [Google Scholar] [CrossRef] [Green Version]
- Soderman, L.; Edlund, M.; Marions, L. Prevalence and impact of dysmenorrhea in Swedish adolescent. Acta Obstet. Gynecil. Scan. 2019, 98, 215–221. [Google Scholar] [CrossRef] [Green Version]
- Lacovides, S.; Avidon, I.; Bentley, A.; Baker, F. Reduced quality of life when experiencing menstrual pain in women with primary dysmenorrhea. Acta Obstet. Gynecil. Scan. 2014, 93, 213–217. [Google Scholar] [CrossRef]
- Quick, F.; Mohammad-Alizadeh-Charandab, S.; Mirghafourvand, M. Primary dysmenorrhea with and without premenstrual syndrome: Variation in quality of life over menstrual phases. Qual. Life Res. 2019, 28, 99–107. [Google Scholar] [CrossRef]
- Kazama, M.; Maruyama, K.; Nakamura, K. Prevalence of dysmenorrhea and Its correlating lifestyle factors in Japanese female junior high school students. Tohoku J. Exp. Med. 2015, 236, 107–113. [Google Scholar] [CrossRef] [Green Version]
- Hashim, T.R.; Alkhalifah, S.S.; Alsalman, A.A.; Alfaris, D.M.; Alhussaini, A.M.; Qasim, R.S.; Shaik, S.A. Prevalence of primary dysmenorrhea and its effect on the quality of life amongst female medical students at King Saud University, Riyadh, Saudi Arabia. Saudi Med. J. 2020, 41, 283–289. [Google Scholar] [CrossRef]
- Qin, L.-L.; Hu, Z.; Kaminga, A.C.; Luo, B.-A.; Xu, H.-L.; Feng, X.-L.; Liu, J.-H. Association between cigarette smoking and the risk of dysmenorrhea: A meta-analysis of observational studies. PLoS ONE 2020, 15, e0231201. [Google Scholar] [CrossRef] [Green Version]
- Ju, H.; Jones, M.; Mishra, G. The prevalence and risk factors of dysmenorrhea. Epidemiol. Rev. 2014, 36, 104–113. [Google Scholar] [CrossRef] [Green Version]
- Wang, L.; Wang, X.; Wang, W.; Chen, C.; Ronnennberg, A.G.; Guang, W.; Huang, A.; Fang, Z.; Zang, T.; Wang, L.; et al. Stress and dysmenorrhoea: A population based prospective study. Occup. Environ. Med. 2004, 61, 1021–1026. [Google Scholar] [CrossRef] [Green Version]
- Rafique, N.; Al-Sheikh, H.M. Prevalence of menstrual problems and their association with psychological stress in young female students studying health sciences. Saudi Med. J. 2018, 39, 67–73. [Google Scholar] [CrossRef] [PubMed]
- Khotimah, K.; Jauzak, R.R.R.A.; Nurunniyah, S.; Maharani, O.; Wahyuningsih, W. Association of BMI and Sport activity habits with dysmenorhea. J. Ners Dan Kebidanan Indones. 2020, 7, 96–104. [Google Scholar] [CrossRef]
- Armour, M.; Parry, K.A.; Steel, K.; Smith, C.A. Australian female athlete perceptions of the challenges associated with training and competing when menstrual symptoms are present. J. Sports Sci. Coach. 2020, 15, 316–323. [Google Scholar] [CrossRef]
- Kartal, B.; Kissal, A.; Kaya, M. Comparison of Athletes and Sedentary Students in Terms of Premenstrual Syndrome and Dysmenorrhea. Ordu Univ. J. Nurs. Stud. 2020, 3, 125–135. [Google Scholar]
- Findlay, J.R.; Marcrae, H.E.; Whyte, Y.I.; Easton, C.; Forrest, J.L. How the menstrual cycle and menstruation affect sporting performance: Experiences and perceptions of elite female rugby players. Br. J. Sports Med. 2020, 54, 1108–1113. [Google Scholar] [CrossRef]
- Homai, H.M.; Shafai, F.S.; Zoodfekr, L. Comparing menarche age, menstrual regularity, dysmenorrhea and analgesic consumption among athletic and non-athletic female students at universities of Tabriz-Iran. Int. J. Women’s Health Reprod. Sci. 2014, 2, 307–310. [Google Scholar] [CrossRef]
- Bourdel, N.; Alves, J.; Pickering, G.; Ramilo, I.; Roman, H.; Canis, M. Systematic review of endometriosis pain assessment: How to choose a scale? Hum. Reprod. 2015, 21, 136–152. [Google Scholar] [CrossRef]
- Arafa, A.E.; Senosy, S.A.; Helmy, H.K.; Mohamed, A.A. Prevalence and patterns of dysmenorrhea and premenstrual syndrome among Egyptian girls (12–25 years). Middle East. Fertil. Soc. J. 2018, 23, 486–490. [Google Scholar] [CrossRef]
- Tomczak, M.; Tomczac, E. The need to report effect size estimates revisited. An overview of some recommended measures of effect size. TRENDS Sport Sci. 2014, 1, 19–25. [Google Scholar]
- Polat, A.; Celik, H.; Gurates, B.; Kaya, D.; Nalbant, M.; Ebru, K.; Hanay, F. Prevalence of primary dysmenorrhea in young adult female university students. Arch. Gynecol. Obset. 2009, 279, 527–532. [Google Scholar] [CrossRef]
- Ortiz, I.M.; Rangel-Flores, E.; Carrillo-Alarcón, C.L.; Veras-Godoy, A.H. Prevalence and impact of primary dysmenorrhea among Mexican high school students. Int. J. Gynaecol. Obstet. 2009, 107, 240–270. [Google Scholar] [CrossRef]
- Bavil, A.D.; Dolatian, M.; Mahmoodi, Z.; Baghban, A.A. A comparison of physical activity and nutrition in young women with and without primary dysmenorrhea [version 1, peer review: 2 approved, 1 approved with reservations]. F1000Research 2019, 7, 59. [Google Scholar] [CrossRef] [Green Version]
- Tsai, S.-Y. Effect of yoga exercise on premenstrual symptoms among female employees in Taiwan. Int. J. Environ. Res. Public Health 2016, 13, 721. [Google Scholar] [CrossRef] [Green Version]
- Motahari-Tabari, N.; Shirvani, A.M.; Alipour, A. Comparison of the effect of stretching exercises and mefenamic acid on the reduction of pain and menstruation characteristics in primary dysmenorrhea: A randomized clinical trial. Oman Med. J. 2017, 32, 47–53. [Google Scholar] [CrossRef]
- Zeinab, K.A.; Mohamadreza, T.M.; Alireza, J.K. The effects of pilates exercise and careway supplementation on the levels of prostaglamdin E2 and perception dysmenorrhea in adolescent girls non-athlete. Asian Exerc. Sport Sci. J. 2017, 1, 1–6. [Google Scholar]
- Dehnavi, M.Z.; Jafarnejad, F.; Kamali, Z. The Effect of aerobic exercise on primary dysmenorrhea: A clinical trial study. J. Educ. Health Promot. 2018, 7, 3. [Google Scholar] [CrossRef]
- Czajkowska, M.; Drosdzol-Cop, A.; Galazka, I.; Naworska, B.; Skrzypulec-Plinta, V. Menstrual cycle and the prevalence of premenstrual syndrome/premenstrual dysphoric disorder in adolescent athletes. Pediatr. Adolesc. Gynecol. 2015, 28, 492–498. [Google Scholar] [CrossRef]
- Kitamura, M.; Takeda, T.; Koga, S.; Nagase, S.; Yaegashi, N. Relationship between premenstrual symptoms and dysmenorrhea in Japanese high school students. Arch. Womens Ment. Health. 2012, 15, 131–133. [Google Scholar] [CrossRef]
- Pascoe, M.C.; Thompson, D.R.; Ski, C.F. Yoga, mindfulness-based stress reduction and stress-related physiological measures: A meta-analysis. Psychoneuroendocrinology 2017, 86, 152–168. [Google Scholar] [CrossRef]
- Casey, M.L.; MacDonald, P.C.; Mitchell, M.D. Despite a massive increase in cortisol secretion in women during parturition, there is an equally massive increase in prostaglandin synthesis. A paradox? J. Clin. Investig. 1985, 75, 1852–1857. [Google Scholar] [CrossRef] [Green Version]
- Febbraio, M.A. Exercise and inflammation. J. Appl. Physiol. 2007, 103, 376–377. [Google Scholar] [CrossRef] [PubMed]
- Fernandez-Martinez, E.; Onieva-Zafra, M.D.; Parra-Fernandez, M.L. Lifestyle and prevalence of dysmenorrhea among Spanish female university students. PLoS ONE 2018, 13, e0201894. [Google Scholar] [CrossRef]
- Kural, M.R.; Noor, N.N.; Pandit, D.; Joshi, T.; Patil, A. Menstrual characteristics and prevalence of dysmenorrhea in college going girls. J. Family Med. Prim. Care 2015, 4, 426–431. [Google Scholar]


{kind=link}
{kind=link}
| Athletes (n = 605) | Non-Athletes (n = 295) | p | ES | |||
|---|---|---|---|---|---|---|
| Age (years) | 20.0 | [19.0–21.0] | 20.0 | [19.0–21.0] | 0.82 | 0.01 |
| Height (cm) | 161.0 | [157.0–165.0] | 158.0 | [155.0–162.0] | <0.01 | 0.23 |
| Weight (kg) | 55.5 | [52.0–60.0] | 50.0 | [47.0–54.0] | <0.01 | 0.40 |
| BMI (kg/m²) | 21.5 | [20.3–22.8] | 19.8 | [18.8–21.3] | <0.01 | 0.34 |
| Sleeping hours (hours) | 7.0 | [6.0–7.8] | 6.0 | [5.5–7.0] | <0.01 | 0.19 |
| Skipping meals (yes, %) | 124 | (20.5%) | 76 | (25.8%) | 0.07 | 0.06 |
| Age at menarche (years) | 13.0 | [12.0–14.0] | 12.0 | [11.0–14.0] | <0.01 | 0.20 |
| Menstrual cycle (days) | 30.0 | [28.0–30.0] | 30.0 | [28.0–31.0] | 0.03 | 0.07 |
| Menstrual period (days) | 5.0 | [5.0–7.0] | 6.0 | [5.0–7.0] | <0.01 | 0.10 |
| Gynecological age (years) | 7.0 | [6.0–8.5] | 8.0 | [6.0–10.0] | <0.01 | 0.16 |
| Prevalence of dysmenorrhea (yes, %) | 518 | (85.6%) | 267 | (90.5%) | 0.04 | 0.07 |
| Training/exercise hours (hours/week) | 18.0 | [12.5–24.0] | 0.0 | [0.0–0.0] | <0.01 | 0.37 |
| Competition level (n, %) | ||||||
| International | 49 | (8.1%) | ||||
| National | 323 | (53.4%) | ||||
| Regional | 142 | (23.5%) | ||||
| Prefectural | 75 | (12.4%) | ||||
| Other | 16 | (2.6%) | ||||
| No/Mild (n = 168) | Medium (n = 117) | Severe (n = 320) | ES | |||||
|---|---|---|---|---|---|---|---|---|
| Age (years) | 20.0 | [19.0–21.0] | 20.0 | [19.0–21.0] | 20.0 | [20.0–21.0] | 0.02 | # |
| Height (cm) | 161.0 | [157.5–166.0] | 160.2 | [155.9–164.2] | 161.0 | [157.0–165.0] | <0.01 | |
| Weight (kg) | 55.1 | [51.0–60.0] | 55.0 | [52.0–60.0] | 56.0 | [52.0–61.0] | <0.01 | |
| BMI (kg/m2) | 21.4 | [20.1–22.6] | 21.3 | [20.2–22.8] | 21.6 | [20.4–22.9] | <0.01 | |
| Sleeping hours (hours) | 6.8 | [6.0–7.5] | 7.0 | [6.1–7.9] | 7.0 | [6.0–7.8] | <0.01 | |
| Skipping meals (yes, %) | 30 | (17.9%) | 18 | (15.4%) | 76 | (23.8%) | 0.09 | |
| Age at menarche (years) | 14.0 | [12.0–15.0] | 13.0 | [12.0–14.0] | 13.0 | [12.0–14.0] | 0.03 | # |
| Menstrual cycle (days) | 30.0 | [28.0–30.0] | 30.0 | [28.0–30.0] | 30.0 | [28.0–30.0] | <0.01 | |
| Menstrual period (days) | 5.0 | [4.0–6.0] | 5.0 | [4.0–6.0] | 6.0 | [5.0–7.0] | 0.03 | #$ |
| Gynecological age (years) | 7.0 | [5.0–8.0] | 7.0 | [6.0–9.0] | 7.0 | [6.0–9.0] | 0.05 | *# |
| Training hours(hours/week) | 18.0 | [12.0–24.0] | 18.0 | [12.3–21.0] | 18.0 | [12.5–24.0] | <0.01 | |
| Competition level (n, %) | 0.10 | |||||||
| International | 12 | (7.1%) | 12 | (10.3%) | 25 | (7.8%) | ||
| National | 90 | (53.6%) | 64 | (54.7%) | 169 | (52.8%) | ||
| Regional | 46 | (27.4%) | 23 | (19.7%) | 73 | (22.8%) | ||
| Prefectural | 15 | (8.9%) | 14 | (12.0%) | 46 | (14.4%) | ||
| Other | 5 | (3.0%) | 4 | (3.4%) | 7 | (2.2%) | ||
| No/Mild (n = 61) | Medium (n = 51) | Severe (n = 183) | ES | ||||
|---|---|---|---|---|---|---|---|
| Age (years) | 20.0 | [19.0–21.0] | 20.0 | [19.0–22.0] | 20.0 | [19.0–21.0] | 0.01 |
| Height (cm) | 158.0 | [153.6–161.1] | 158.7 | [155.4–161.0] | 158.0 | [155.0–162.0] | <0.01 |
| Weight (kg) | 50.0 | [48.0–54.0] | 51.0 | [47.8–54.0] | 50.0 | [47.0–54.2] | <0.01 |
| BMI (kg/m2) | 20.4 | [19.1–21.4] | 20.0 | [19.0–21.0] | 19.6 | [18.7–21.3] | 0.01 |
| Sleeping hours (hours) | 6.0 | [5.1–7.0] | 6.5 | [5.8–7.5] | 6.0 | [5.5–7.0] | <0.01 |
| Skipping meals (yes, %) | 14 | (23.0%) | 14 | (27.5%) | 48 | (26.2%) | 0.03 |
| Age at menarche (years) | 13.0 | [11.0–14.0] | 12.0 | [12.0–14.0] | 12.0 | [11.0–13.0] | 0.01 |
| Menstrual cycle (days) | 30.0 | [28.0–31.0] | 30.0 | [28.0–35.0] | 30.0 | [28.0–30.0] | 0.01 |
| Menstrual period (days) | 5.0 | [4.8–7.0] | 5.0 | [5.0–6.0] | 6.0 | [5.0–7.0] | 0.03 |
| Gynecological age (years) | 8.0 | [6.0–9.0] | 8.0 | [6.0–10.0] | 8.0 | [7.0–10.0] | 0.01 |
| Exercise hours (hours/week) | 0.0 | [0.0–0.3] | 0.0 | [0.0–0.0] | 0.0 | [0.0–0.0] | 0.01 |
| B | Exp(B) | 95% CI | p | ||
|---|---|---|---|---|---|
| Age (years) | 0.123 | 1.130 | 0.977 | 1.308 | 0.10 |
| BMI (kg/m2) | 0.051 | 1.052 | 0.968 | 1.144 | 0.23 |
| Sleeping hours (hours) | −0.047 | 0.954 | 0.832 | 1.094 | 0.50 |
| Skipping meals (yes) | 0.386 | 1.471 | 0.957 | 2.262 | 0.07 |
| Age at menarche (years) | −0.160 | 0.852 | 0.765 | 0.950 | <0.01 |
| Menstrual cycle (days) | −0.018 | 0.982 | 0.956 | 1.009 | 0.19 |
| Menstrual period (days) | 0.269 | 1.309 | 1.154 | 1.484 | <0.01 |
| Training hours(hours/week) | 0.026 | 1.026 | 1.004 | 1.048 | 0.02 |
| Competition level (low) | 0.117 | 1.124 | 0.923 | 1.368 | 0.25 |
| B | Exp(B) | 95% CI | p | ||
|---|---|---|---|---|---|
| Age (years) | 0.115 | 1.122 | 0.908 | 1.386 | 0.29 |
| BMI (kg/m2) | −0.066 | 0.936 | 0.834 | 1.052 | 0.27 |
| Sleeping hours (hours) | −0.067 | 0.935 | 0.743 | 1.177 | 0.57 |
| Skipping meals (yes) | 0.170 | 1.185 | 0.665 | 2.114 | 0.57 |
| Age at menarche (years) | −0.119 | 0.888 | 0.758 | 1.040 | 0.14 |
| Menstrual cycle (days) | −0.044 | 0.957 | 0.918 | 0.997 | 0.04 |
| Menstrual period (days) | 0.355 | 1.426 | 1.161 | 1.752 | <0.01 |
| Exercise hours (hours/week) | −0.067 | 0.935 | 0.843 | 1.038 | 0.20 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Momma, R.; Nakata, Y.; Sawai, A.; Takeda, M.; Natsui, H.; Mukai, N.; Watanabe, K. Comparisons of the Prevalence, Severity, and Risk Factors of Dysmenorrhea between Japanese Female Athletes and Non-Athletes in Universities. Int. J. Environ. Res. Public Health 2022, 19, 52. https://doi.org/10.3390/ijerph19010052
Momma R, Nakata Y, Sawai A, Takeda M, Natsui H, Mukai N, Watanabe K. Comparisons of the Prevalence, Severity, and Risk Factors of Dysmenorrhea between Japanese Female Athletes and Non-Athletes in Universities. International Journal of Environmental Research and Public Health. 2022; 19(1):52. https://doi.org/10.3390/ijerph19010052
Chicago/Turabian StyleMomma, Reiko, Yoshio Nakata, Akemi Sawai, Maho Takeda, Hiroaki Natsui, Naoki Mukai, and Koichi Watanabe. 2022. "Comparisons of the Prevalence, Severity, and Risk Factors of Dysmenorrhea between Japanese Female Athletes and Non-Athletes in Universities" International Journal of Environmental Research and Public Health 19, no. 1: 52. https://doi.org/10.3390/ijerph19010052
APA StyleMomma, R., Nakata, Y., Sawai, A., Takeda, M., Natsui, H., Mukai, N., & Watanabe, K. (2022). Comparisons of the Prevalence, Severity, and Risk Factors of Dysmenorrhea between Japanese Female Athletes and Non-Athletes in Universities. International Journal of Environmental Research and Public Health, 19(1), 52. https://doi.org/10.3390/ijerph19010052