
Traditional Korean Medicine Home Care for the Older Adults during the COVID-19 Pandemic in South Korea

 , , , ,
, , , ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Scope of the Survey
2.2. Development of the Questionnaire
2.3. Survey Method
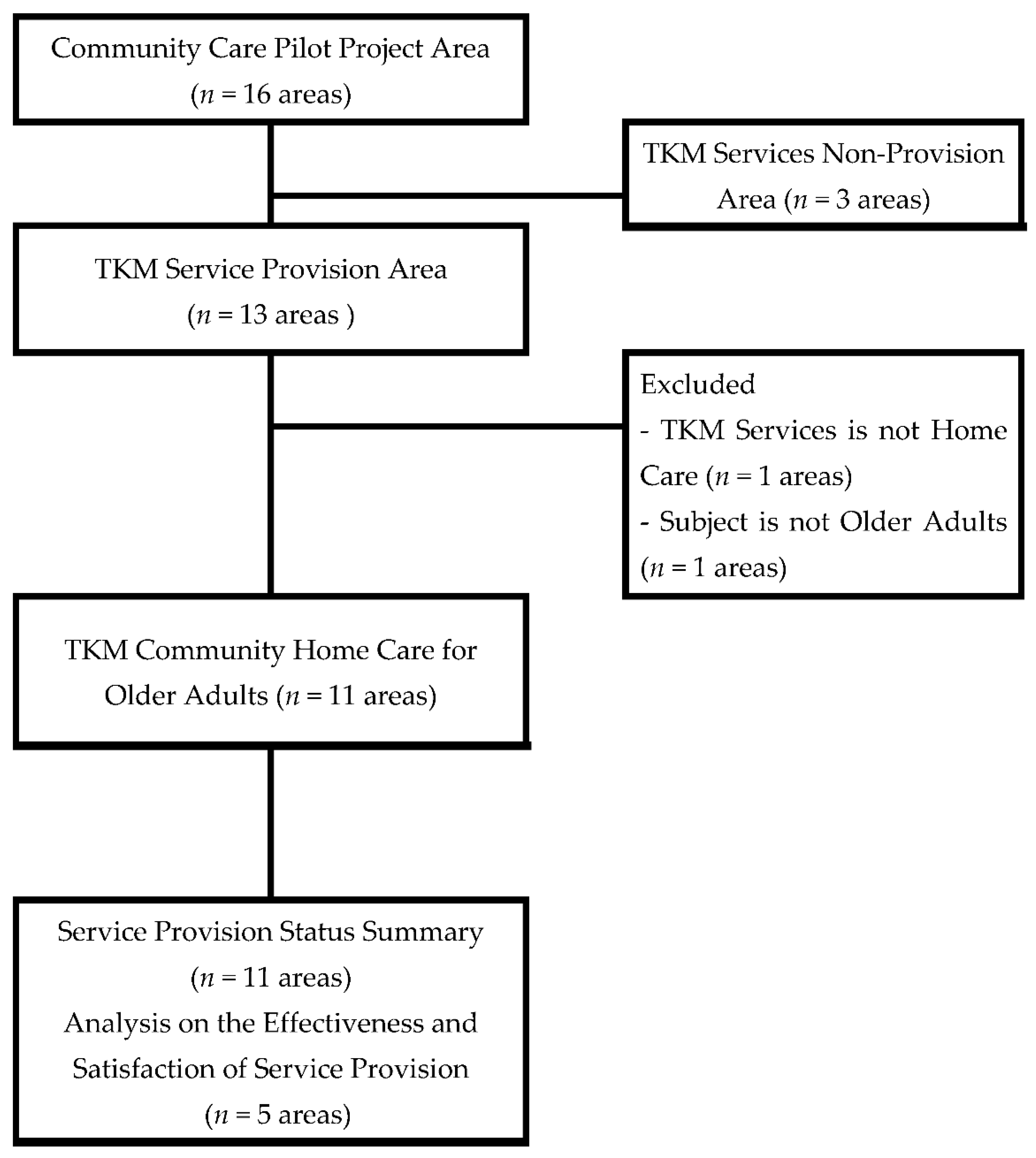
2.4. Study Selection
2.5. Statistical Analysis
3. Results
3.1. Basic Characteristics of Areas
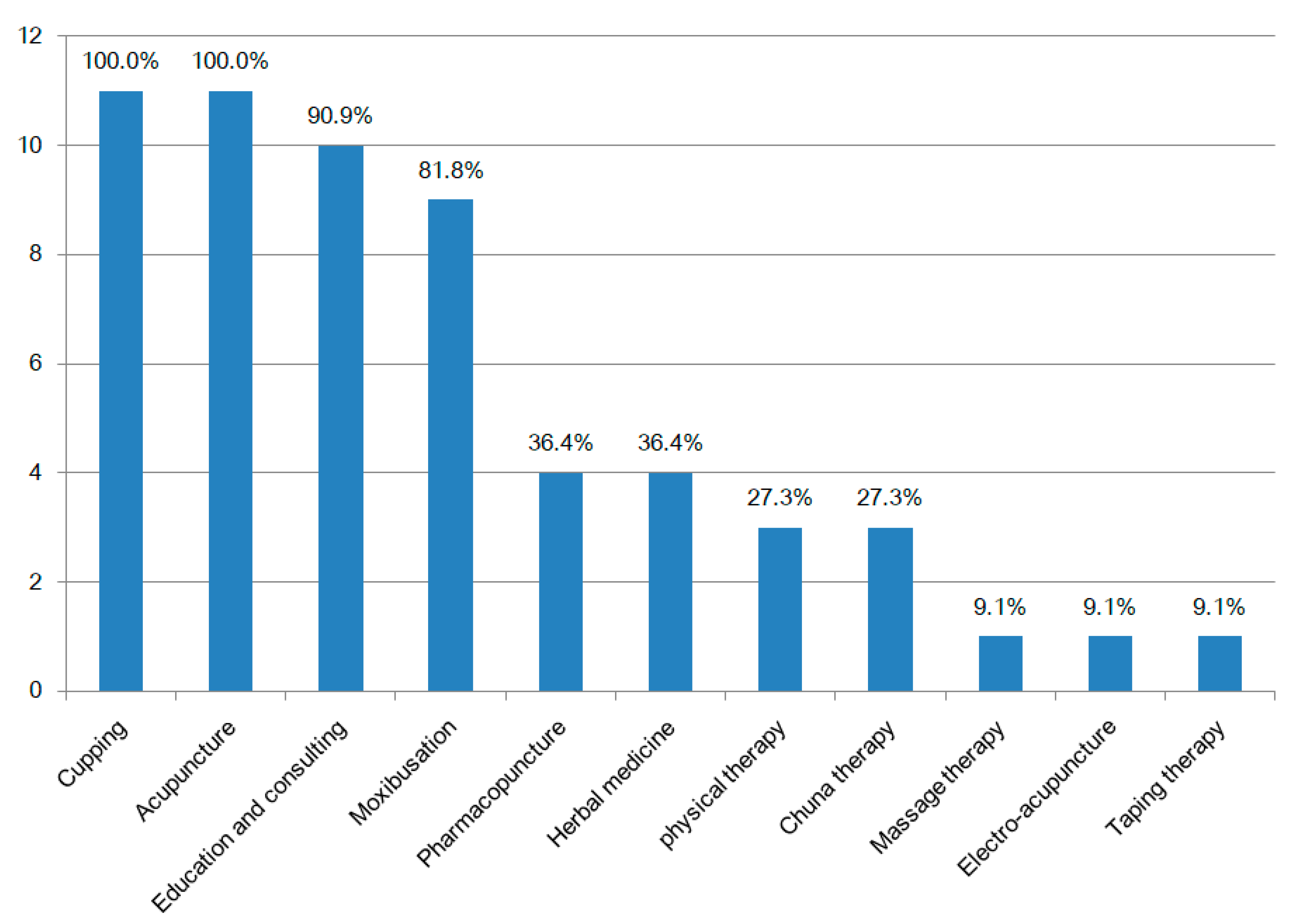
3.2. Current Provision of TKM Community Home Care Service
3.3. Effectiveness of and Satisfaction with TKM Service Provision
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Sabeerabi, B.; Vemula, S.; Vadde, R.; Nagaraju, G.P. COVID-19: Where is the treatment? World J. Clin. Oncol. 2021, 12, 309–322. [Google Scholar] [CrossRef] [PubMed]
- Zheng, Y.Y.; Ma, Y.T.; Zhang, J.Y.; Xie, X. COVID-19 and the cardiovascular system. Nat. Rev. Cardiol. 2020, 17, 259–260. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Worldometer. Current World Population. Available online: https://www.worldometers.info/world-population (accessed on 4 September 2021).
- Central Disater Management Headquarters. Coronavirus Disease-19, South Korea. Available online: http://ncov.mohw.go.kr/tcmBoardView.do?brdId=&brdGubun=&dataGubun=&ncvContSeq=352435&contSeq=352435&board_id=&gubun=ALL (accessed on 4 September 2021).
- Powdthavee, N.; Riyanto, Y.E.; Wong, E.C.L.; Yeo, J.X.W.; Chan, Q.Y. When face masks signal social identity: Explaining the deep face-mask divide during the COVID-19 pandemic. PLoS ONE 2021, 16, e0253195. [Google Scholar] [CrossRef] [PubMed]
- Anand, S.V.; Shuy, Y.K.; Lee, P.S.S.; Lee, E.S. One Year on: An overview of Singapore’s response to COVID-19—What we did, how we fared, how we can move forward. Int. J. Environ. Res. Public Health 2021, 18, 9125. [Google Scholar] [CrossRef]
- Kim, H. Lesson learned from the power of open data: Resolving the mask shortage problem caused by COVID-19 in South Korea. Sustainability 2021, 13, 278. [Google Scholar] [CrossRef]
- Aw, J.; Seng, J.; Seah, S.; Low, L.L. COVID-19 vaccine hesitancy-A scoping review of literature in high-income countries. Vaccines 2021, 9, 900. [Google Scholar] [CrossRef]
- CNN. Singapore and the UK Are Both Planning to ‘Live with Covid’. They Are Worlds Apart on How to Do That. Available online: https://edition.cnn.com/2021/07/16/asia/singapore-uk-covid-reopening-intl-hk-gbr/index.html (accessed on 5 September 2021).
- Korea Health Promotion Institute. 2021 Integrated Community Health Promotion Program: Traditional & Complementary Medicine (T&CAM) Health Promotion; Korea Health Promotion Institute: Seoul, Korea, 2020. Available online: https://www.khealth.or.kr/kps/publish/view?menuId=MENU00890&page_no=B2017003&board_idx=10454 (accessed on 11 September 2021).
- Central Disater Management Headquarters and Central Disease Control Headquarters. Guidelines for Managing to COVID-19 for Local Governments; Central Disater Management Headquarters and Central Disease Control Headquarters: Sejong, Korea, 2021. Available online: http://www.kdca.go.kr/board/board.es?mid=a20507020000&bid=0019 (accessed on 11 September 2021).
- Kim, H.S. Towards telemedicine adoption in Korea: 10 practical recommendations for physicians. J. Korean Med. Sci. 2021, 36, e103. [Google Scholar] [CrossRef]
- Lee, S.H.; Bae, S.M.; Shin, B.M.; Shin, S.J. Types of perception of home visiting oral health care services for Korean older persons: A Q methodology study. Int. J. Environ. Res. Public Health 2020, 18, 214. [Google Scholar] [CrossRef]
- Ministry of Health & Welfare. Community Care Promotion Guidebook for Local Government; Ministry of Health & Welfare: Sejong, Korea, 2020. Available online: http://www.mohw.go.kr/react/al/sal0301vw.jsp?PAR_MENU_ID=04&MENU_ID=0403&page=1&CONT_SEQ=357215 (accessed on 11 September 2021).
- Ministry of Health & Welfare. Guidelines for the Pilot Program of National Health Insurance for the Payment of Home-Based Primary Care; Ministry of Health & Welfare: Sejong, Korea, 2021. Available online: http://www.mohw.go.kr/react/jb/sjb0406vw.jsp?PAR_MENU_ID=03&MENU_ID=030406&CONT_SEQ=364265 (accessed on 11 September 2021).
- Ministry of Health & Welfare. Research for Developing Community-Based Traditional Korean Medicine (TKM) and Social Welfare Service Model and System; Ministry of Health & Welfare: Sejong, Korea, 2019.
- Kim, H.T.; Hwang, E.H.; Heo, I.; Cho, J.H.; Kim, K.W.; Ha, I.H.; Shin, B.C. Clinical practice guidelines for the use of traditional Korean medicine in the treatment of patients with traffic-related injuries: An evidence-based approach. Eur. J. Integr. Med. 2018, 18, 34–41. [Google Scholar] [CrossRef]
- Ministry of Health & Welfare; National Development Institute of Korean Medicine; Gallup Korea. 2020 Years National Survey for Traditional Korean Medicine (TKM) Usage; National Development Institute of Korean Medicine: Seoul, Korea, 2020. Available online: https://www.koms.or.kr/board/researchReport/view.do?post_no=161&menu_no=21 (accessed on 27 November 2021).
- Mazza, C.; Ricci, E.; Biondi, S.; Colasanti, M.; Ferracuti, S.; Napoli, C.; Roma, P. A nationwide survey of psychological distress among Italian people during the COVID-19 pandemic: Immediate psychological responses and associated factors. Int. J. Environ. Res. Public Health 2020, 17, 3165. [Google Scholar] [CrossRef]
- Lee, M.; You, M. Psychological and behavioral responses in South Korea during the early stages of coronavirus disease 2019 (COVID-19). Int. J. Environ. Res. Public Health 2020, 17, 2977. [Google Scholar] [CrossRef]
- Wang, C.; Pan, R.; Wan, X.; Tan, Y.; Xu, L.; Ho, C.S.; Ho, R.C. Immediate psychological responses and associated factors during the initial stage of the 2019 coronavirus disease (COVID-19) epidemic among the general population in China. Int. J. Environ. Res. Public Health 2020, 17, 1729. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kim, J.; You, M.; Shon, C. Impact of the COVID-19 pandemic on unmet healthcare needs in Seoul, South Korea: A cross-sectional study. BMJ Open 2021, 11, e045845. [Google Scholar] [CrossRef] [PubMed]
- Sung, S.-H.; Park, M.; Kim, J.; Jeon, S.-W.; Sung, A.D.-M.; Lee, E.-J.; Oh, D.; Park, J.-Y.; Park, J.-K.; Kim, K.H. Current status of traditional Korean medicine services in public sector: A study for integrating traditional Korean medicine into community care system. Healthcare 2021, 9, 93. [Google Scholar] [CrossRef] [PubMed]
- Lee, J.A.; Jang, S.B.; Go, H.Y.; Kim, K.H.; Park, S.J. Perception of the health promotion programme using traditional Korean medicine (HaPP TKM): A survey of traditional Korean medicine public health doctors. Eur. J. Integr. Med. 2019, 27, 65–69. [Google Scholar] [CrossRef]
- Park, J.S.; Jang, S.B.; Lee, J.A.; Go, H.Y.; Park, S.J. A national-wide survey of public health promotion programs in traditional Korean medicine targeted on public officials. J. Soc. Prev. Korean Med. 2017, 21, 61–68. [Google Scholar] [CrossRef]
- Kim, E.S.; Kim, J.; Kim, B.; Park, K.S. Classification of regional age structure based on dynamic age structure model and an analysis of association among regional population, economy, education and welfare environment. Korea J. Popul. Stud. 2019, 42, 83–113. [Google Scholar] [CrossRef]
- Statistics Korea. 2019 Older Adults Person Statistics; Statistics Korea: Daejeon, Korea, 2019. Available online: https://www.kostat.go.kr/portal/korea/kor_nw/1/1/index.board?bmode=read&aSeq=377701 (accessed on 17 October 2021).
- Falvo, I.; Zufferey, M.C.; Albanese, E.; Fadda, M. Lived experiences of older adults during the first COVID-19 lockdown: A qualitative study. PLoS ONE 2021, 16, e0252101. [Google Scholar] [CrossRef]
- Siette, J.; Dodds, L.; Seaman, K.; Wuthrich, V.; Johnco, C.; Earl, J.; Dawes, P.; Westbrook, J.I. The impact of COVID-19 on the quality of life of older adults receiving community-based aged care. Australas. J. Ageing 2021, 40, 84–89. [Google Scholar] [CrossRef] [PubMed]
- Amukotuwa, S.A.; Bammer, R.; Maingard, J. Where have our patients gone? The impact of COVID-19 on stroke imaging and intervention at an Australian stroke center. J. Med. Imaging Radiat. Oncol. 2020, 64, 607–614. [Google Scholar] [CrossRef]
- Heid, A.R.; Cartwright, F.; Wilson-Genderson, M.; Pruchno, R. Challenges experienced by older people during the initial months of the COVID-19 pandemic. Gerontologist 2021, 61, 48–58. [Google Scholar] [CrossRef]
- Health Insurance Review & Assessment Service, Healthcare Bigdata Hub, South Korea. Available online: http://opendata.hira.or.kr/op/opc/olapHthInsRvStatInfo.do (accessed on 28 November 2021).
- Siette, J.; Seaman, K.; Dodds, L.; Ludlow, K.; Johnco, C.; Wuthrich, V.; Earl, J.K.; Dawes, P.; Strutt, P.; Westbrook, J.I. A national survey on COVID-19 second-wave lockdowns on older adults’ mental wellbeing, health-seeking behaviours and social outcomes across Australia. BMC Geriatr. 2021, 21, 400. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
{kind=link}
{kind=link}
| Areas | Area Type | Area Characteristics | ||||
|---|---|---|---|---|---|---|
| Total Population (Persons) | Older Adult Population Rate | Single Older Adult Household Rate | Unmet Medical Need Rate | Number of Medical Institution Medical Doctors * (Persons) | ||
| Median | - | 450,168 | 14.0% | 20.0% | 7.0% | 3.0 |
| Seo-gu Gwangju | 2 type | 300,975 | 13.4% | 20.3% | 7.1% | 3.6 |
| Buk-gu Busan | 2 type | 291,132 | 15.8% | 23.2% | 14.1% | 2.4 |
| Busanjin-gu Busan | 2 type | 357,880 | 18.8% | 21.6% | 4.4% | 5.2 |
| Ansan Gyeonggi | 1 type | 650,918 | 10.2% | 19.9% | 9.6% | 2.7 |
| Bucheon Gyeonggi | 2 type | 829,996 | 12.5% | 18.3% | 7.8% | 3.0 |
| Namyangju Gyeonggi | 1 type | 701,830 | 13.3% | 14.6% | 3.4% | 1.5 |
| Cheonan Chungnam | 1 type | 652,268 | 10.3% | 19.4% | 17.6% | 3.3 |
| Jincheon Chungbuk | 4 type | 81,084 | 17.1% | 21.7% | 6.8% | 1.7 |
| Gimhae Gyeongnam | 2 type | 542,455 | 10.6% | 20.3% | 6.5% | 1.9 |
| Suncheon Jeonnam | 4 type | 279,598 | 15.1% | 21.6% | 9.5% | 2.7 |
| Seoguipo Jeju | 1 type | 181,584 | 18.6% | 17.0% | 5.6% | 1.7 |
| Areas | Type of Care (Number of Participating Institutions) | Treatment Diseases/Number of Subject | Intervention | Number of Assistants | ||
|---|---|---|---|---|---|---|
| Type of Used Intervention | Treatment Duration, Sessions | Cost | ||||
| Seo-gu Gwangju | Home care (n = 7) | Old adults (Musculoskeletal disorder (1)/n = 60) | Acupuncture Cupping Taping Exercise therapy Chuna manual therapy (3) Education and consulting | 9 month, 12 sessions per person | 100 USD (User charge 0 USD) | n = 0 |
| Cheonan Gyeonggi | Home care (n = 25) | Old adults (Musculoskeletal disorder (1)/n = 73) | Acupuncture Moxibustion (2) Cupping Chuna manual therapy (3) Herbal medicine Massage | 12 month, 12 sessions per person | 95.8 USD (User charge 0 USD) | n = 25 (Nurse’s aide) |
| Seoguipo Jeju | Home care (n = 6) | Old adults (Musculoskeletal disorder (1)/n = 42) | Acupuncture Moxibustion (2) Cupping Education and consulting Herbal medicine | 12 month, 8 sessions per person | 95.8 USD (User charge 0 USD) | n = 0 |
| Ansan Gyeonggi | Home care (n = 32) | Old adults (Musculoskeletal disorder (1)/n = 105) | Acupuncture Moxibustion (2) Cupping Pharmacopuncture Exercise therapy Education and consulting | 6 month, 8 sessions per person | 83.3 USD (User charge 0 USD) | n = 50 (Nurse’s aide or community service centre staff) |
| Jincheon Chungbuk | Home care (n = 3) | Old adults (Musculoskeletal disorder (1)/n = 58) | Acupuncture Moxibustion (2) Cupping Chuna manual therapy (3) Education and consulting | 6 month, 8 sessions per person | 100 USD (User charge 0 USD) | n = 3 (Nurse’s aide) |
| Busanjin-gu Busan | Home care (n = 13) | Old adults (Musculoskeletal disorder (1)/n = 35) | Acupuncture Moxibustion (2) Cupping Education and consulting | 8 month, 8 sessions per person | 166.7 USD (User charge 0 USD) | n = 2 (Nurse’s aide) n = 12 (Community service centre staff) |
| Buk-gu Busan | Home care (n = 16) | Old adults (Musculoskeletal disorder (1)/n = 9) | Acupuncture Moxibustion (2) Cupping Pharmacopuncture Education and consulting | 4 month, 4 sessions per person | 166.7 USD (User charge 0 USD) | n = 3 (Nurse’s aide) n = 13 (Community service centre staff) |
| Bucheon Gyeonggi | Home care (n = 19) | Old adults (Musculoskeletal disorder (1)/n = 80) | Acupuncture Moxibustion (2) Cupping Herbal medicine Chuna manual therapy (3) Education and consulting | 2 month, 12 sessions per person | 100 USD (User charge 0 USD) | n = 10 (Community service centre staff) |
| Gimhae Gyeongnam | Home care (n = 2) | Old adults (Musculoskeletal disorder (1)/n = 21) | Acupuncture Electroacupuncture Pharmacopuncture Moxibustion (2) Cupping Herbal medicine Education and consulting | 12 month, 8 sessions per person | 100 USD (User charge 0 USD) | n = 0 |
| Suncheon Jeonnam | Home care (n = 4) | Old adults (Musculoskeletal disorder (1)/n = 50) | Acupuncture Pharmacopuncture Cupping Education and consulting | 12 month, 4 sessions per person | 98.3 USD (User charge 0 USD) | n = 1(Social worker) n = 1 (Community service centre staff) |
| Namyangju Gyeonggi | Home care (n = 9) | Old adults (Musculoskeletal disorder (1)/n = 65) | Acupuncture Moxibustion (2) Cupping Exercise therapy Education and consulting | 2 month, 6 sessions per person | 125 USD (User charge 0 USD) | n = 0 |
| Outcome | N (Number of Persons) | Pre (Mean ± SD) | After (Mean ± SD) | p-Value |
|---|---|---|---|---|
| VAS | 126 | 7.74 ± 1.90 | 6.13 ± 2.30 | 0.000 ** |
| EQ-5D total score | 34 | 11.09 ± 2.17 | 10.07 ± 2.19 | 0.000 ** |
| Q1 score | 34 | 2.29 ± 0.46 | 2.15 ± 0.44 | 0.000 ** |
| Q2 score | 34 | 1.91 ± 0.79 | 1.81 ± 0.80 | 0.000 ** |
| Q3 score | 34 | 2.21 ± 0.64 | 2.09 ± 0.62 | 0.000 ** |
| Q4 score | 34 | 2.50 ± 0.51 | 2.21 ± 0.54 | 0.003 * |
| Q5 score | 34 | 2.18 ± 0.76 | 1.85 ± 0.61 | 0.000 ** |
| Questionnaire | N (Number of Persons) | Minimum | Maximun | Average (Mean ± SD) |
|---|---|---|---|---|
| Q1. Was the TKM service provide sufficient information? | 60 | 1 | 5 | 4.37 ± 0.82 |
| Q2. Was it convenient to apply for and participate in the TKM service? | 60 | 1 | 5 | 4.30 ± 0.93 |
| Q3. Was the TKM service helpful to health? | 60 | 3 | 5 | 4.76 ± 0.47 |
| Q4. Did your ability to manage your condition yourself improve after the TKM service? | 60 | 3 | 5 | 4.51 ± 0.57 |
| Q5. Are you willing to recommend the TKM service to others? | 60 | 3 | 5 | 4.65 ± 0.58 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Sung, S.-H.; Baik, Y.-S.; Han, J.-E.; Lee, E.-J.; Kim, J.; Park, M.; Lee, J.-Y.; Park, J.-K.; Park, J.-Y.; Lee, E. Traditional Korean Medicine Home Care for the Older Adults during the COVID-19 Pandemic in South Korea. Int. J. Environ. Res. Public Health 2022, 19, 493. https://doi.org/10.3390/ijerph19010493
Sung S-H, Baik Y-S, Han J-E, Lee E-J, Kim J, Park M, Lee J-Y, Park J-K, Park J-Y, Lee E. Traditional Korean Medicine Home Care for the Older Adults during the COVID-19 Pandemic in South Korea. International Journal of Environmental Research and Public Health. 2022; 19(1):493. https://doi.org/10.3390/ijerph19010493
Chicago/Turabian StyleSung, Soo-Hyun, You-Sang Baik, Ji-Eun Han, Eun-Jin Lee, Jihye Kim, Minjung Park, Ji-Yeon Lee, Jang-Kyung Park, Jung-Youn Park, and Eunkyung Lee. 2022. "Traditional Korean Medicine Home Care for the Older Adults during the COVID-19 Pandemic in South Korea" International Journal of Environmental Research and Public Health 19, no. 1: 493. https://doi.org/10.3390/ijerph19010493
APA StyleSung, S.-H., Baik, Y.-S., Han, J.-E., Lee, E.-J., Kim, J., Park, M., Lee, J.-Y., Park, J.-K., Park, J.-Y., & Lee, E. (2022). Traditional Korean Medicine Home Care for the Older Adults during the COVID-19 Pandemic in South Korea. International Journal of Environmental Research and Public Health, 19(1), 493. https://doi.org/10.3390/ijerph19010493