
Vegetarian and Vegan Diet in Fibromyalgia: A Systematic Review



Abstract
1. Introduction
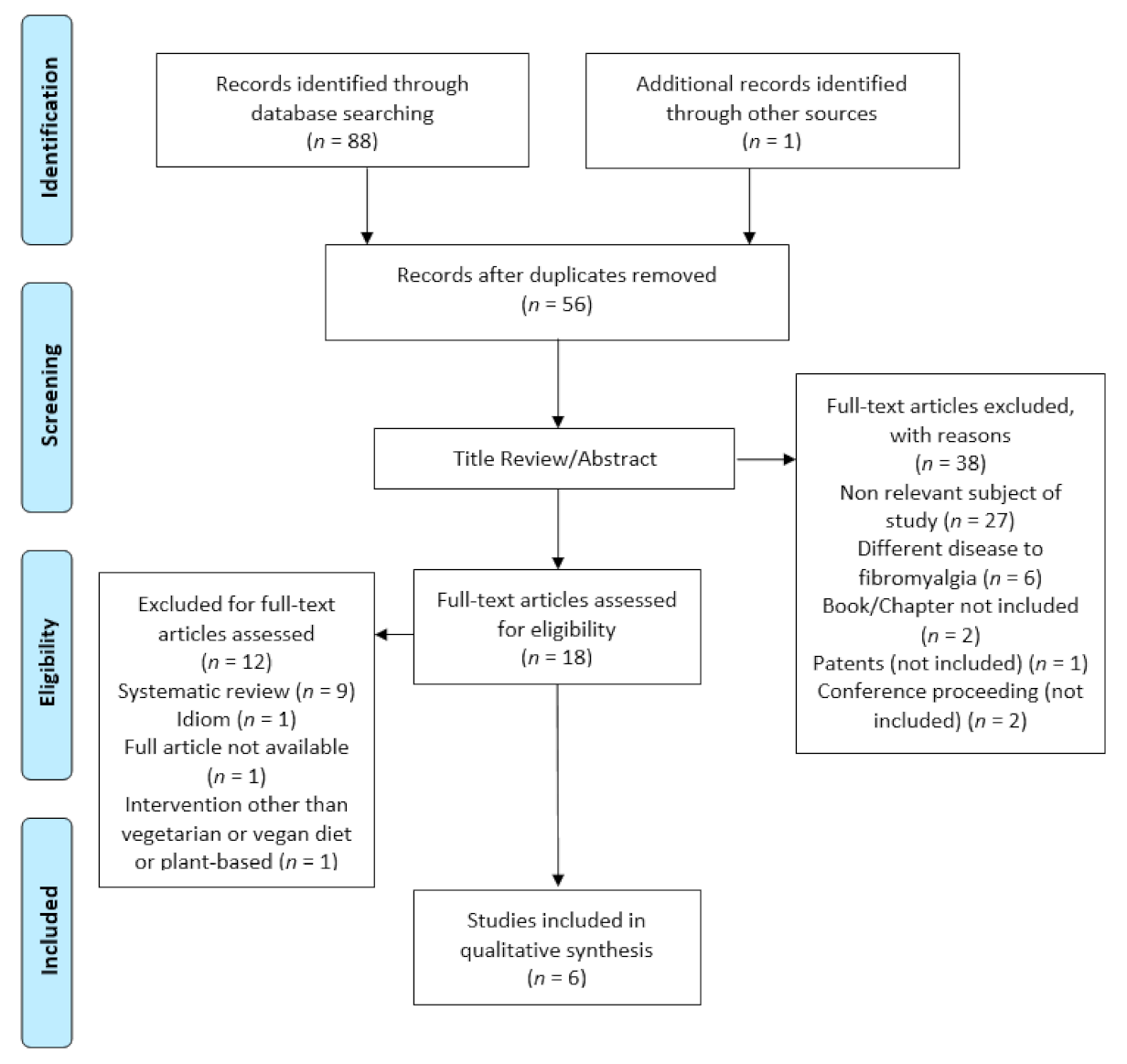
2. Materials and Methods
2.1. Design
2.2. Eligibility Criteria
2.3. Search Strategy
2.4. Data Collection
2.5. Data Synthesis
2.6. Methodological Quality
3. Results
3.1. Overview of Included Studies
3.2. Effect on Biochemical Parameters and Biomarkers
3.3. Effects on Quality of Life and Health Status
3.4. Effects on Body Weight and Body Mass Index
3.5. Effects on Fibromyalgia Symptoms
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Úbeda-D’Ocasar, E.; Jiménez Díaz-Benito, V.; Gallego-Sendarrubias, G.M.; Valera-Calero, J.A.; Vicario-Merino, Á.; Hervás-Pérez, J.P. Pain and Cortisol in Patients with Fibromyalgia: Systematic Review and Meta-Analysis. Diagnostics 2020, 10, 922. [Google Scholar] [CrossRef] [PubMed]
- Heidari, F.; Afshari, M.; Moosazadeh, M. Prevalence of Fibromyalgia in General Population and Patients, a Systematic Review and Meta-Analysis. Rheumatol. Int. 2017, 37, 1527–1539. [Google Scholar] [CrossRef] [PubMed]
- Sarzi-Puttini, P.; Giorgi, V.; Marotto, D.; Atzeni, F. Fibromyalgia: An Update on Clinical Characteristics, Aetiopathogenesis and Treatment. Nat. Rev. Rheumatol. 2020, 16, 645–660. [Google Scholar] [CrossRef] [PubMed]
- Holton, K. The Role of Diet in the Treatment of Fibromyalgia. Pain Manag. 2016, 6, 317–320. [Google Scholar] [CrossRef]
- Arranz, L.I. Effects of Obesity on Function and Quality of Life in Chronic Pain. In Nutritional Modulators of Pain in the Aging Population; Academic Press: New York, NY, USA, 2017; pp. 151–170. ISBN 9780128053362. [Google Scholar]
- Lowry, E.; Marley, J.; McVeigh, J.G.; McSorley, E.; Allsopp, P.; Kerr, D. Dietary Interventions in the Management of Fibromyalgia: A Systematic Review and Best-Evidence Synthesis. Nutrients 2020, 12, 2664. [Google Scholar] [CrossRef]
- Baranowsky, J.; Klose, P.; Musial, F.; Haeuser, W.; Dobos, G.; Langhorst, J. Qualitative Systemic Review of Randomized Controlled Trials on Complementary and Alternative Medicine Treatments in Fibromyalgia. Rheumatol. Int. 2009, 30, 1–21. [Google Scholar] [CrossRef] [PubMed]
- Donaldson, M.S.; Speight, N.; Loomis, S. Fibromyalgia Syndrome Improved Using a Mostly Raw Vegetarian Diet: An Observational Study. BMC Complement. Altern. Med. 2001, 1. [Google Scholar] [CrossRef]
- Elma, Ö.; Yilmaz, S.T.; Deliens, T.; Coppieters, I.; Clarys, P.; Nijs, J.; Malfliet, A. Nutritional Factors in Chronic Musculoskeletal Pain: Unravelling the Underlying Mechanisms. Br. J. Anaesth. 2020, 125, e231–e233. [Google Scholar] [CrossRef]
- Schulze, N.B.; Salemi, M.d.M.; de Alencar, G.G.; Moreira, M.C.; de Siqueira, G.R. Efficacy of Manual Therapy on Pain, Impact of Disease, and Quality of Life in the Treatment of Fibromyalgia: A Systematic Review. Pain Physician 2020, 23, 461–476. [Google Scholar] [CrossRef]
- Sosa-Reina, M.D.; Nunez-Nagy, S.; Gallego-Izquierdo, T.; Pecos-Martín, D.; Monserrat, J.; Álvarez-Mon, M. Effectiveness of Therapeutic Exercise in Fibromyalgia Syndrome: A Systematic Review and Meta-Analysis of Randomized Clinical Trials. Biomed. Res. Int. 2017, 2017, 2356346. [Google Scholar] [CrossRef]
- Goldenberg, D.L. Multidisciplinary Modalities in the Treatment of Fibromyalgia. J. Clin. Psychiatry 2008, 69 (Suppl. S2), 30–34. [Google Scholar]
- Silva, A.R.; Bernardo, A.; Costa, J.; Cardoso, A.; Santos, P.; de Mesquita, M.F.; Vaz Patto, J.; Moreira, P.; Silva, M.L.; Padrão, P. Dietary Interventions in Fibromyalgia: A Systematic Review. Ann. Med. 2019, 51, 2–14. [Google Scholar] [CrossRef] [PubMed]
- Nadal-Nicolás, Y.; Rubio-Arias, J.Á.; Martínez-Olcina, M.; Reche-García, C.; Hernández-García, M.; Martínez-Rodríguez, A. Effects of Manual Therapy on Fatigue, Pain, and Psychological Aspects in Women with Fibromyalgia. Int. J. Environ. Res. Public Health 2020, 17, 4611. [Google Scholar] [CrossRef]
- Gluba-Brzózka, A.; Franczyk, B.; Rysz, J. Vegetarian Diet in Chronic Kidney Disease-A Friend or Foe. Nutrients 2017, 9, 374. [Google Scholar] [CrossRef] [PubMed]
- Holton, K.F.; Taren, D.L.; Thomson, C.A.; Bennett, R.M.; Jones, K.D. The Effect of Dietary Glutamate on Fibromyalgia and Irritable Bowel Symptoms. Clin. Exp. Rheumatol. 2012, 30, 10–17. [Google Scholar] [PubMed]
- Craig, W.J.; Mangels, A.R. Position of the American Dietetic Association: Vegetarian Diets. J. Am. Diet. Assoc. 2009, 109, 1266–1282. [Google Scholar] [CrossRef]
- Melina, V.; Craig, W.; Levin, S. Position of the Academy of Nutrition and Dietetics: Vegetarian Diets. J. Acad. Nutr. Diet. 2016, 116. [Google Scholar] [CrossRef]
- Mangels, A.R.; Messina, V.; Melina, V. Position of the American Dietetic Association and Dietitians of Canada: Vegetarian Diets. J. Am. Diet. Assoc. 2003, 103, 748–765. [Google Scholar]
- Menzel, J.; Jabakhanji, A.; Biemann, R.; Mai, K.; Abraham, K.; Weikert, C. Systematic Review and Meta-Analysis of the Associations of Vegan and Vegetarian Diets with Inflammatory Biomarkers. Sci. Rep. 2020, 10, 21736. [Google Scholar] [CrossRef]
- Craddock, J.C.; Probst, Y.C.; Peoples, G.E. Vegetarian and Omnivorous Nutrition—Comparing Physical Performance. Int. J. Sport Nutr. Exerc. Metab. 2016, 26, 212–220. [Google Scholar] [CrossRef]
- Pilis, W.; Stec, K.; Zych, M.; Pilis, A. Health Benefits and Risk Associated with Adopting a Vegetarian Diet. Rocz. Panstw. Zakl. Hig. 2014, 65, 9–14. [Google Scholar]
- Dinu, M.; Abbate, R.; Gensini, G.F.; Casini, A.; Sofi, F. Vegetarian, Vegan Diets and Multiple Health Outcomes: A Systematic Review with Meta-Analysis of Observational Studies. Crit. Rev. Food Sci. Nutr. 2017, 57, 3640–3649. [Google Scholar] [CrossRef]
- Haghighatdoost, F.; Bellissimo, N.; Totosy de Zepetnek, J.O.; Rouhani, M.H. Association of Vegetarian Diet with Inflammatory Biomarkers: A Systematic Review and Meta-Analysis of Observational Studies. Public Health Nutr. 2017, 20, 2713–2721. [Google Scholar] [CrossRef]
- Aleksandrova, K.; Koelman, L.; Rodrigues, C.E. Dietary Patterns and Biomarkers of Oxidative Stress and Inflammation: A Systematic Review of Observational and Intervention Studies. Redox Biol. 2021, 42, 101869. [Google Scholar] [CrossRef]
- Craddock, J.C.; Neale, E.P.; Peoples, G.E.; Probst, Y.C. Vegetarian-Based Dietary Patterns and Their Relation with Inflammatory and Immune Biomarkers: A Systematic Review and Meta-Analysis. Adv. Nutr. (BethesdaMd.) 2019, 10, 433–451. [Google Scholar] [CrossRef]
- Hanninen, O.; Rauma, A.-L.; Kaartinen, K.; Nenonen, M. Vegan Diet in Physiological Health Promotion. Acta Physiol. Hung. 1999, 86, 171–180. [Google Scholar]
- Kahleova, H.; Pelikanova, T. Vegetarian Diets in the Prevention and Treatment of Type 2 Diabetes. J. Am. Coll. Nutr. 2015, 34, 448–458. [Google Scholar] [CrossRef]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G.; Group, P. Preferred Reporting Items for Systematic Reviews and Meta-Analyses: The PRISMA Statement. PLoS Med. 2009, 6, e1000097. [Google Scholar] [CrossRef]
- Perestelo-Pérez, L. Standards on How to Develop and Report Systematic Reviews in Psychology and Health. Int. J. Clin. Health Psychol. 2013, 13, 49–57. [Google Scholar] [CrossRef]
- Wolfe, F.; Clauw, D.J.; Fitzcharles, M.-A.; Goldenberg, D.L.; Katz, R.S.; Mease, P.; Russell, A.S.; Russell, I.J.; Winfield, J.B.; Yunus, M.B. The American College of Rheumatology Preliminary Diagnostic Criteria for Fibromyalgia and Measurement of Symptom Severity. Arthritis Care Res. 2010, 62, 600–610. [Google Scholar] [CrossRef]
- von Elm, E.; Altman, D.G.; Egger, M.; Pocock, S.J.; Gøtzsche, P.C.; Vandenbroucke, J.P. The Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) Statement: Guidelines for Reporting Observational Studies. Int. J. Surg. 2014, 12, 1495–1499. [Google Scholar] [CrossRef] [PubMed]
- de Morton, N.A. The PEDro Scale Is a Valid Measure of the Methodological Quality of Clinical Trials: A Demographic Study. Aust. J. Physiother. 2009, 55, 129–133. [Google Scholar] [CrossRef]
- Pluye, P.; Robert, E.; Cargo, M.; Bartlett, G.; O’cathain, A.; Griffiths, F.; Boardman, F.; Gagnon, M.-P.; Rousseau, M.C. Proposal: A Mixed Methods Appraisal Tool for Systematic Mixed Studies Reviews; Mcgill Univ.: Montréal, QC, Canada, 2011; Volume 2, pp. 1–8. [Google Scholar]
- Kaartinen, K.; Lammi, K.; Hypen, M.; Nenonen, M.; Hänninen, O. Vegan Diet Alleviates Fibromyalgia Symptoms. Scand. J. Rheumatol. 2000, 29, 308–313. [Google Scholar] [CrossRef]
- Martínez-Rodríguez, A.; Leyva-Vela, B.; Martínez-García, A.; Nadal-Nicolás, Y. Effects of Lacto-Vegetarian Diet and Stabilization Core Exercises on Body Composition and Pain in Women with Fibromyalgia: Randomized Controlled Trial | Efectos de La Dieta Lacto-Vegetariana y Ejercicios de Estabilización Del Core Sobre La Composición Cor. Nutr. Hosp. 2018, 35, 392–399. [Google Scholar] [CrossRef]
- Hostmark, A.T.; Lystad, E.; Vellar, O.D.; Hovi, K.; Berg, J.E. Reduced Plasma-Fibrinogen, Serum Peroxides, Lipids, and Apolipoproteins after a 3-Week Vegetarian Diet. Plant Foods Hum. Nutr. 1993, 43, 55–61. [Google Scholar] [CrossRef]
- Hanninen, O.; Kaartinen, K.; Rauma, A.L.; Nenonen, M.; Torronen, R.; Hakkinen, S.; Adlercreutz, H.; Laakso, J. Antioxidants in Vegan Diet and Rheumatic Disorders. Toxicology 2000, 155, 45–53. [Google Scholar] [CrossRef]
- Michalsen, A. Naturopathic and Complementary Medicine in the Treatment of Rheumatic Diseases. Aktuelle Rheumatol. 2015, 40, 454–460. [Google Scholar] [CrossRef][Green Version]
- Beck, A.T.; Steer, R.A.; Carbin, M.G. Psychometric Properties of the Beck Depression Inventory: Twenty-Five Years of Evaluation. Clin. Psychol. Rev. 1988, 8, 77–100. [Google Scholar] [CrossRef]
- Ware, J.E.J.; Sherbourne, C.D. The MOS 36-Item Short-Form Health Survey (SF-36). I. Conceptual Framework and Item Selection. Med. Care 1992, 30, 473–483. [Google Scholar] [CrossRef]
- Burckhardt, C.S.; Anderson, K.L. The Quality of Life Scale (QOLS): Reliability, Validity, and Utilization. Health Qual. Life Outcomes 2003, 1, 60. [Google Scholar] [CrossRef]
- Shapiro, J.R.; Anderson, D.A.; Danoff-Burg, S. A Pilot Study of the Effects of Behavioral Weight Loss Treatment on Fibromyalgia Symptoms. J. Psychosom. Res. 2005, 59, 275–282. [Google Scholar] [CrossRef]
- Bennett, R. The Fibromyalgia Impact Questionnaire (FIQ): A Review of Its Development, Current Version, Operating Characteristics and Uses. Clin. Exp. Rheumatol. 2005, 23, S154–S162. [Google Scholar]
- Labronici, P.J.; dos Santos-Viana, A.M.; dos Santos-Filho, F.C.; Santos-Pires, R.E.; Labronici, G.J.; Penteado-da Silva, L.H. Evaluation of the Pain in Older People. Acta Ortop. Mex. 2016, 30, 73–80. [Google Scholar] [PubMed]
- Wallace, D.J.; Hallegua, D.S. Fibromyalgia: The Gastrointestinal Link. Curr. Pain Headache Rep. 2004, 8, 364–368. [Google Scholar] [CrossRef]
- Triadafilopoulos, G.; Simms, R.W.; Goldenberg, D.L. Bowel Dysfunction in Fibromyalgia Syndrome. Dig. Dis. Sci. 1991, 36, 59–64. [Google Scholar] [CrossRef]
- Carding, S.; Verbeke, K.; Vipond, D.T.; Corfe, B.M.; Owen, L.J. Dysbiosis of the Gut Microbiota in Disease. Microb. Ecol. Health Dis. 2015, 26, 26191. [Google Scholar] [CrossRef]
- Riva, R.; Mork, P.J.; Westgaard, R.H.; Rø, M.; Lundberg, U. Fibromyalgia Syndrome Is Associated with Hypocortisolism. Int. J. Behav. Med. 2010, 17, 223–233. [Google Scholar] [CrossRef]
- Romano, G.F.; Tomassi, S.; Russell, A.; Mondelli, V.; Pariante, C.M. Fibromyalgia and Chronic Fatigue: The Underlying Biology and Related Theoretical Issues. Adv. Psychosom. Med. 2015, 34, 61–77. [Google Scholar] [CrossRef]
- Kadetoff, D.; Lampa, J.; Westman, M.; Andersson, M.; Kosek, E. Evidence of Central Inflammation in Fibromyalgia-Increased Cerebrospinal Fluid Interleukin-8 Levels. J. Neuroimmunol. 2012, 242, 33–38. [Google Scholar] [CrossRef]
- Steck, S.; Shivappa, N.; Tabung, F.K.; Harmon, B.E.; Wirth, M.D.; Hurley, T.G.; Hebert, J.R. The Dietary Inflammatory Index: A New Tool for Assessing Diet Quality Based on Inflammatory Potential. Digest 2014, 49, 1–10. [Google Scholar]
- Senna, M.K.; Sallam, R.A.-E.R.; Ashour, H.S.; Elarman, M. Effect of Weight Reduction on the Quality of Life in Obese Patients with Fibromyalgia Syndrome: A Randomized Controlled Trial. Clin. Rheumatol. 2012, 31, 1591–1597. [Google Scholar] [CrossRef] [PubMed]
- Barnard, N.D.; Levin, S.M.; Yokoyama, Y. A Systematic Review and Meta-Analysis of Changes in Body Weight in Clinical Trials of Vegetarian Diets. J. Acad. Nutr. Diet. 2015, 115, 954–969. [Google Scholar] [CrossRef] [PubMed]
- Cordero, M.D.; Alcocer-Gómez, E.; Cano-García, F.J.; Sánchez-Domínguez, B.; Fernández-Riejo, P.; Moreno Fernández, A.M.; Fernández-Rodríguez, A.; de Miguel, M. Clinical Symptoms in Fibromyalgia Are Associated to Overweight and Lipid Profile. Rheumatol. Int. 2014, 34, 419–422. [Google Scholar] [CrossRef] [PubMed]
- Cong, L.; Cao, C.; Cheng, Y.; Qin, X.-Y. Green Tea Polyphenols Attenuated Glutamate Excitotoxicity via Antioxidative and Antiapoptotic Pathway in the Primary Cultured Cortical Neurons. Oxidative Med. Cell. Longev. 2016, 2016, 2050435. [Google Scholar] [CrossRef] [PubMed]
- Wang, J.-Y.; Wen, L.-L.; Huang, Y.-N.; Chen, Y.-T.; Ku, M.-C. Dual Effects of Antioxidants in Neurodegeneration: Direct Neuroprotection against Oxidative Stress and Indirect Protection via Suppression of Glia-Mediated Inflammation. Curr. Pharm. Des. 2006, 12, 3521–3533. [Google Scholar] [CrossRef] [PubMed]
- Bjørklund, G.; Dadar, M.; Chirumbolo, S.; Aaseth, J. Fibromyalgia and Nutrition: Therapeutic Possibilities? Biomed. Pharmacother. Biomed. Pharmacother. 2018, 103, 531–538. [Google Scholar] [CrossRef]
- Coskun Benlidayi, I. Role of Inflammation in the Pathogenesis and Treatment of Fibromyalgia. Rheumatol. Int. 2019, 39, 781–791. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Study | Type of Study | Participants | Interventions | Results |
|---|---|---|---|---|
| Kaartinen K, 2000 [35] | Clinical trial | 28 females with FM (average age 51–52 years); intervention group (n = 15), control group (n = 13) |
|
|
| Donaldson M S, 2001 [8] | Observational cohort study | 30 persons with FM (28 female and 2 male) (average 45–54 years) |
|
|
| Martínez-Rodríguez A, 2018 [36] | Randomized clinical trial | 21 females with FM (34 ± 3 years) |
|
|
| Michalsen A, 2005 [39] | Observational cohort study | 51 patients with RA (9 female) or FM (32 female and 3 male). The 4 groups: FM and fasting (n = 21, 52.0 ± 10.0 years); RA and fasting (n = 21, 57.6 ± 6.5 years); FM and vegetarian diet (n = 14, 51.6 ± 13.3 years); RA and vegetarian diet (n = 7, 49.4 ± 14.3 years) |
|
|
| Hanninen O, 2000 [38] | Clinical trial | 115 persons: 40 healthy volunteered, 33 FM patients, 42 RA subjects. They were divided into LF and omnivorous controls |
|
|
| Hostmark A T, 1991 [37] | Clinical trial | 8 female and 2 males with FM (49.9 ± 4.1 years) |
|
|
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Nadal-Nicolás, Y.; Miralles-Amorós, L.; Martínez-Olcina, M.; Sánchez-Ortega, M.; Mora, J.; Martínez-Rodríguez, A. Vegetarian and Vegan Diet in Fibromyalgia: A Systematic Review. Int. J. Environ. Res. Public Health 2021, 18, 4955. https://doi.org/10.3390/ijerph18094955
Nadal-Nicolás Y, Miralles-Amorós L, Martínez-Olcina M, Sánchez-Ortega M, Mora J, Martínez-Rodríguez A. Vegetarian and Vegan Diet in Fibromyalgia: A Systematic Review. International Journal of Environmental Research and Public Health. 2021; 18(9):4955. https://doi.org/10.3390/ijerph18094955
Chicago/Turabian StyleNadal-Nicolás, Yolanda, Laura Miralles-Amorós, María Martínez-Olcina, María Sánchez-Ortega, Juan Mora, and Alejandro Martínez-Rodríguez. 2021. "Vegetarian and Vegan Diet in Fibromyalgia: A Systematic Review" International Journal of Environmental Research and Public Health 18, no. 9: 4955. https://doi.org/10.3390/ijerph18094955
APA StyleNadal-Nicolás, Y., Miralles-Amorós, L., Martínez-Olcina, M., Sánchez-Ortega, M., Mora, J., & Martínez-Rodríguez, A. (2021). Vegetarian and Vegan Diet in Fibromyalgia: A Systematic Review. International Journal of Environmental Research and Public Health, 18(9), 4955. https://doi.org/10.3390/ijerph18094955