
Sleep Quality and Physical Activity as Predictors of Mental Wellbeing Variance in Older Adults during COVID-19 Lockdown: ECLB COVID-19 International Online Survey

 ,
,  ,
,  , , , ,
, , , , 
 , ,
, ,  ,
,  ,
,  , , ,
, , , 
 ,
,  , ,
, ,  , ,
, ,  , ,
, , 
 ,
,  ,
,
Abstract
1. Introduction
2. Materials and Methods
2.1. Sample Size
2.2. Survey Development and Promotion
2.2.1. SWEMWBS
2.2.2. PSQI
2.2.3. IPAQ-SF
2.3. Data Analysis
3. Results
3.1. Data Set Selection and Sample Description
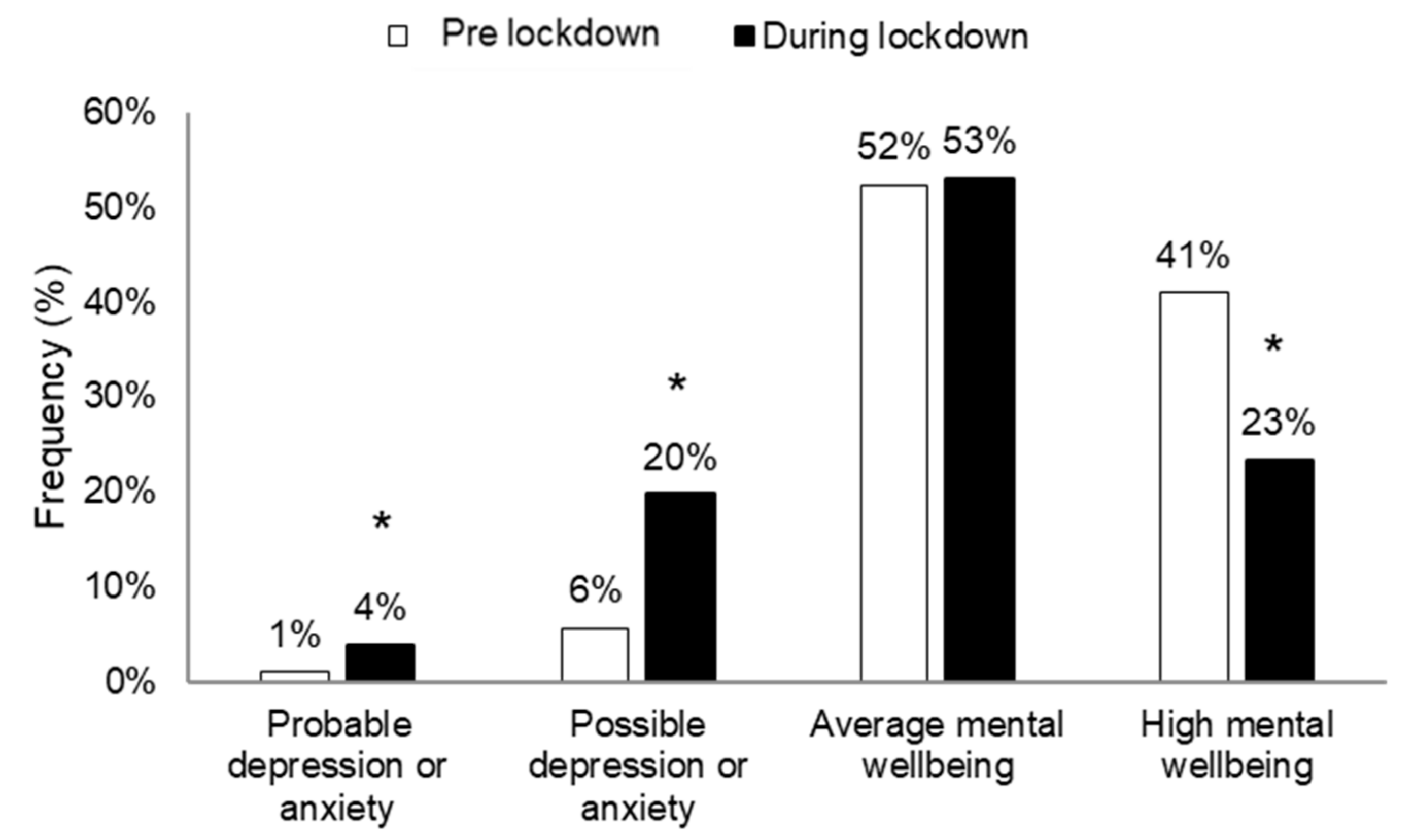
3.2. SWEMWBS
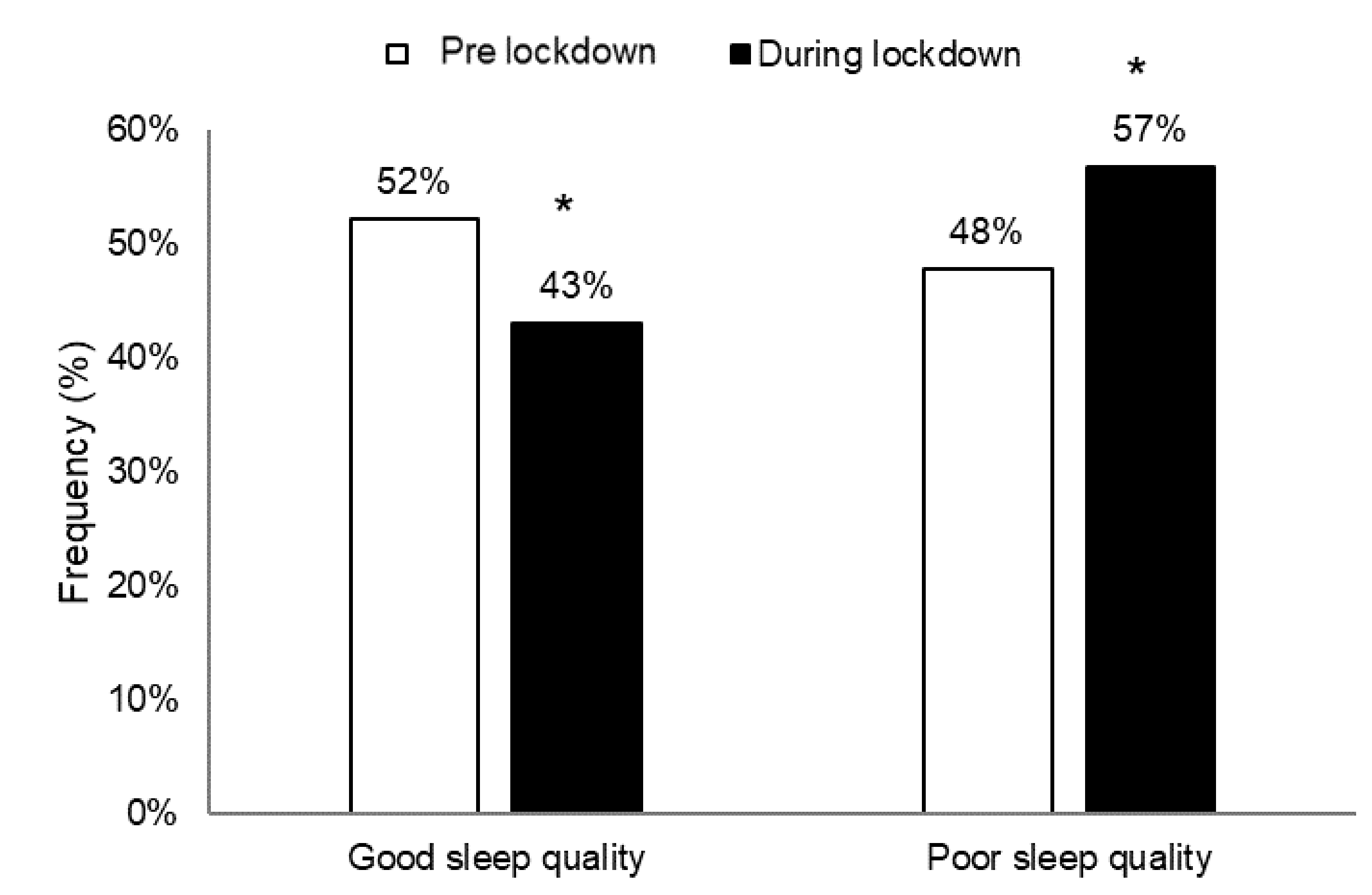
3.3. PSQI
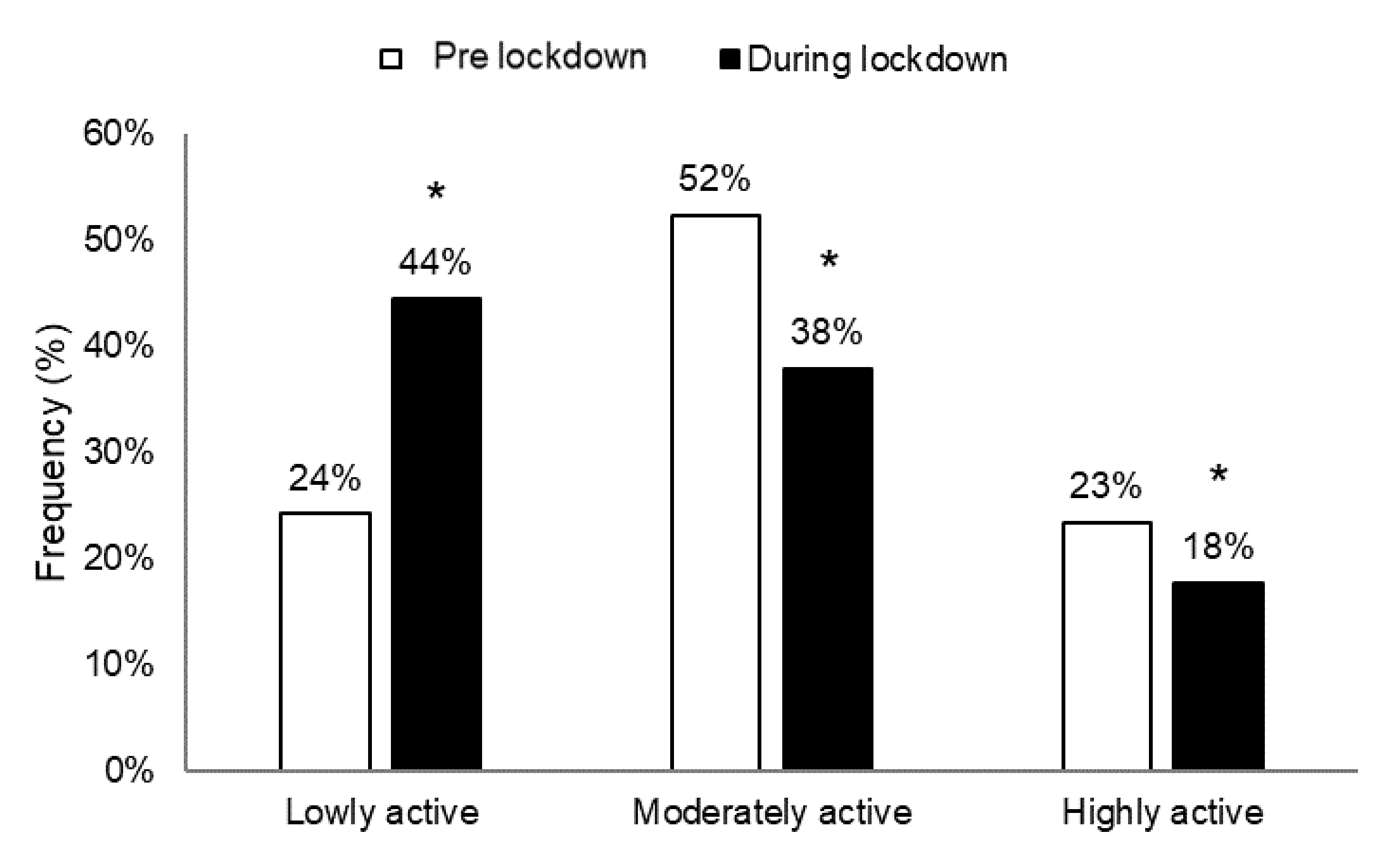
3.4. IPAQ-SF
3.5. Predictors of Mental Wellbeing Change
4. Discussion
4.1. Effects of COVID-19 Lockdown on Mental Wellbeing
4.2. Effects of COVID-19 Lockdown on PA
4.3. Effects of COVID-19 Lockdown on Sleep Patterns
4.4. Predictors of Self-Reported Change in Mental Wellbeing
4.5. Strengths and Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- World Health Organization. Coronavirus Disease (COVID-2019) Situation Reports. Coronavirus Disease 2019 (COVID-19) Situation Report. WHO. 2019. Available online: https://www.who.int/emergencies/diseases/novel-coronavirus-2019/situation-reports (accessed on 20 April 2020).
- Biswas, A.; Bhattacharjee, U.; Chakrabarti, A.K.; Tewari, D.N.; Banu, H.; Dutta, S. Emergence of Novel Coronavirus and COVID-19: Whether to stay or die out? Crit. Rev. Microbiol. 2020, 46, 182–193. [Google Scholar] [CrossRef] [PubMed]
- Yang, Y.; Li, W.; Zhang, Q.; Zhang, L.; Cheung, T.; Xiang, Y.-T. Mental health services for older adults in China during the COVID-19 outbreak. Lancet Psychiatry 2020, 7, e19. [Google Scholar] [CrossRef]
- Harman, D. The free radical theory of aging. Antioxid. Redox Signal. 2003, 5, 557–561. [Google Scholar] [CrossRef] [PubMed]
- Lee, K.; Jeong, G.C.; Yim, J. Consideration of the Psychological and Mental Health of the Elderly during COVID-19: A Theoretical Review. Int. J. Environ. Res. Public Health 2020, 17, 8098. [Google Scholar] [CrossRef]
- Niu, S.; Tian, S.; Lou, J.; Kang, X.; Zhang, L.; Lian, H.; Zhang, J. Clinical characteristics of older patients infected with COVID-19: A descriptive study. Arch. Gerontol. Geriatr. 2020, 89, 104058. [Google Scholar] [CrossRef]
- Rubin, G.J.; Wessely, S. The psychological effects of quarantining a city. BMJ 2020, 368. [Google Scholar] [CrossRef]
- CDC. “Older Adults”. 2020. Available online: https://www.cdc.gov/coronavirus/2019-ncov/need-extra-precautions/olderadults.html (accessed on 8 May 2020).
- Roberton, T.; Carter, E.D.; Chou, V.B.; Stegmuller, A.R.; Jackson, B.D.; Tam, Y.; Sawadogo-Lewis, T.; Walker, N. Early estimates of the indirect effects of the COVID-19 pandemic on maternal and child mortality in low-income and middle-income countries: A modelling study. Lancet Glob. Health 2020, 8, e901–e908. [Google Scholar] [CrossRef]
- Ammar, A.; Brach, M.; Trabelsi, K.; Chtourou, H.; Boukhris, O.; Masmoudi, L.; Bouaziz, B.; Bentlage, E.; How, D.; Ahmed, M.; et al. Effects of COVID-19 Home Confinement on Eating Behaviour and Physical Activity: Results of the ECLB-COVID19 International Online Survey. Nutrients 2020, 12, 1583. [Google Scholar] [CrossRef]
- Trabelsi, K.; Ammar, A.; Masmoudi, L.; Boukhris, O.; Chtourou, H.; Bouaziz, B.; Brach, M.; Bentlage, E.; How, D.; Ahmed, M.; et al. Globally altered sleep patterns and physical activity levels by confinement in 5056 individuals: ECLB COVID-19 international online survey. Biol. Sport 2021, 38, 495–506. [Google Scholar]
- Ammar, A.; Trabelsi, K.; Brach, M.; Chtourou, H.; Boukhris, O.; Masmoudi, L.; Bouaziz, B.; Bentlage, E.; How, D.; Ahmed, M.; et al. Effects of home confinement on mental health and lifestyle behaviours during the COVID-19 outbreak: Insight from the ECLB-COVID19 multicenter study. Biol. Sport 2021. [Google Scholar] [CrossRef]
- Ammar, A.; Mueller, P.; Trabelsi, K.; Boukhris, O.; Masmoudi, L.; Bouaziz, B.; Brach, M.; Schmicker, M.; Bentlage, E.; How, D.; et al. Psychological consequences of COVID-19 home confinement: The ECLB-COVID19 multicenter study. PLoS ONE 2020. [Google Scholar] [CrossRef]
- Chtourou, H.; Trabelsi, K.; H’mida, C.; Boukhris, O.; Glenn, J.M.; Brach, M.; Bentlage, E.; Bott, N.; Shephard, R.J.; Ammar, A.; et al. Staying physically active during the quarantine and self-isolation period for controlling and mitigating the COVID-19 pandemics: An overview. Front. Psychol. 2020, 11. [Google Scholar] [CrossRef]
- Seligman, M.E. Flourish: A visionary new understanding of happiness and well-being. Policy 2011, 27, 60–61. [Google Scholar] [CrossRef]
- The NHS Confederation. Public Mental Health and Wellbeing—The Local Perspective. 2011. Available online: http://www.nhsconfed.org/~/media/Confederation/Files/Publications/Documents/Report_Public_mental_health_well_being.pdf (accessed on 5 December 2014).
- Gale, C.; Deary, I.J.; Stafford, M. A life course approach to psychological and social wellbeing. In A Life Course Approach to Healthy Ageing, 1st ed.; Kuh, D., Cooper, R., Hardy, R., Richards, M., Ben-Shlomo, Y., Eds.; Oxford University Press: Oxford, UK, 2014. [Google Scholar]
- Boehm, J.K.; Peterson, C.; Kivimaki, M.; Kubzansky, L. A prospective study of positive psychological wellbeing and coronary heart disease. Health Psychol. 2011, 30, 259–267. [Google Scholar] [CrossRef]
- Chida, Y.; Steptoe, A. Positive psychological wellbeing and mortality: A quantitative review of prospective observational studies. Psychosom. Med. 2008, 70, 741–756. [Google Scholar] [CrossRef]
- Steptoe, A.; de Oliveira, C.; Demakakos, P.; Zaninotto, P. Enjoyment of life and declining physical function at older ages: A longitudinal cohort study. CMAJ 2014, 186, E150–E156. [Google Scholar] [CrossRef]
- Carstensen, L.L. The influence of a sense of time on human development. Science 2006, 312, 1913–1915. [Google Scholar] [CrossRef]
- Hardy, S.E.; Concato, J.; Gill, T.M. Resilience of community-dwelling older persons. J. Am. Geriatr. Soc. 2004, 52, 257–262. [Google Scholar] [CrossRef]
- Charles, S.T. Strength and vulnerability integration (SAVI): A model of emotional wellbeing across adulthood. Psychology 2010, 136, 1068. [Google Scholar]
- García-Fernández, L.; Romero-Ferreiro, V.; López-Roldán, P.D.; Padilla, S.; Rodriguez-Jimenez, R. Mental health in elderly Spanish people in times of COVID-19 outbreak. Am. J. Geriatr. Psychiatry 2020, 28, 1040–1045. [Google Scholar] [CrossRef]
- Philip, J. Impact of COVID-19 on mental health of the elderly. Int. J. Community Med. Public Health 2020, 7, 2435. [Google Scholar] [CrossRef]
- Charles, S.T.; Carstensen, L.L. Social and emotional aging. Annu. Rev. Clin. Psychol. 2010, 61, 383–409. [Google Scholar] [CrossRef]
- Santini, Z.I.; Jose, P.E.; Cornwell, E.Y.; Koyanagi, A.; Nielsen, L.; Hinrichsen, C.; Mailstrup, C.; Madsen, K.R.; Koushede, V. Social disconnectedness, perceived isolation, and symptoms of depression and anxiety among older Americans (NSHAP): A longitudinal mediation analysis. Lancet Public Health 2020, 5, e62–e70. [Google Scholar] [CrossRef]
- Krendl, A.C.; Perry, B.L. The impact of sheltering in place during the COVID-19 pandemic on older adults’ social and mental wellbeing. J. Gerontol. Ser. B Psychol. Sci. Soc. Sci. 2020, 76, e53–e58. [Google Scholar]
- Draper, B.M. Suicidal behaviour and suicide prevention in later life. Maturitas 2014, 79, 179–183. [Google Scholar] [CrossRef] [PubMed]
- Novotney, A. The risks of social isolation. Monit. Psychol. APA 2019, 50, 32. [Google Scholar]
- Mura, G.; Carta, M.G. Physical activity in depressed elderly. A systematic review. Clin. Pr. Epidemiol. Ment. Health 2013, 9, 125–135. [Google Scholar] [CrossRef] [PubMed]
- Black, S.V.; Cooper, R.; Martin, K.R.; Brage, S.; Kuh, D.; Stafford, M. Physical activity and mental wellbeing in a cohort aged 60–64 years. Am. J. Prev. Med. 2015, 49, 172–180. [Google Scholar] [CrossRef] [PubMed]
- Lee, P.H.; Macfarlane, D.J.; Lam, T.H.; Stewart, S.M. Validity of the international physical activity questionnaire short from (PAQ-SF): A systematic review. Int. J. Behav. Nutr. Phys. Act. 2011, 8, 1–11. [Google Scholar] [CrossRef]
- Narici, M.; De Vito, G.; Franchi, M.; Paoli, A.; Moro, T.; Marcolin, G.; Grassi, B.; Baldassarre, G.; Zuccarelli, L.; Biolo, G. Impact of sedentarism due to the COVID-19 home confinement on neuromuscular, cardiovascular and metabolic health: Physiological and pathophysiological implications and recommendations for physical and nutritional countermeasures. Eur. J. Sport Sci. 2020, 1–22. [Google Scholar] [CrossRef]
- Yousfi, N.; Bragazzi, N.L.; Briki, W.; Zmijewski, P.; Chamari, K. The COVID-19 pandemic: How to maintain a healthy immune system during the lockdown—A multidisciplinary approach with special focus on athletes. Biol. Sport 2020, 37, 211. [Google Scholar] [CrossRef]
- Castañeda-Babarro, A.; Arbillaga-Etxarri, A.; Gutiérrez-Santamaría, B.; Coca, A. Physical activity change during COVID-19 confinement. Int. J. Environ. Res. Public Health 2020, 17, 6878. [Google Scholar] [CrossRef]
- Yamada, M.; Kimura, Y.; Ishiyama, D.; Otobe, Y.; Suzuki, M.; Koyama, S.; Arai, H. Effect of the COVID-19 epidemic on physical activity in community-dwelling older adults in Japan: A cross-sectional online survey. J. Nutr. Health Aging 2020, 24, 948–950. [Google Scholar] [CrossRef]
- Suzuki, Y.; Maeda, N.; Hirado, D.; Shirakawa, T.; Urabe, Y. Physical activity changes and its risk factors among community-dwelling japanese older adults during the COVID-19 epidemic: Associations with subjective wellbeing and health-related quality of life. Int. J. Environ. Res. Public Health 2020, 17, 6591. [Google Scholar] [CrossRef]
- Callow, D.D.; Arnold-Nedimala, N.A.; Jordan, L.S.; Pena, G.S.; Won, J.; Woodard, J.L.; Smith, J.C. The Mental Health Benefits of Physical Activity in Older Adults Survive the COVID-19 Pandemic. Am. J. Geriatr. Psychiatry 2020, 28, 1046–1057. [Google Scholar] [CrossRef]
- Zielinski, M.R.; Krueger, J.M. Sleep and immunity. Front. Biosci. 2011, 3, 632–642. [Google Scholar]
- Dimitrov, S.; Lange, T.; Goutefangeas, C.; Jensen, A.T.R.; Szczepanski, M.; Lehnnolz, J.; Soekadar, S.; Rammensee, H.G.; Born, J.; Besedovsky, L. Gαs-coupled receptor signaling and sleep regulate integrin activation of human antigen-specifc T cells. J. Exp. Med. 2019, 216, 517–526. [Google Scholar] [CrossRef]
- Alcañiz, M.; Riera-Prunera, M.C.; Solé-Auró, A. “When I Retire, I’ll Move Out of the City”: Mental Wellbeing of the Elderly in Rural vs. Urban Settings. Int. J. Environ. Res. Public Health 2020, 17, 2442. [Google Scholar] [CrossRef]
- Ghram, A.; Briki, W.; Mansoor, H.; Al-Mohannadi, A.S.; Lavie, C.J.; Chamari, K. Home-based exercise can be beneficial for counteracting sedentary behavior and physical inactivity during the COVID-19 pandemic in older adults. Postgrad. Med. 2020, 30, 1–12. [Google Scholar] [CrossRef]
- Gulia, K.K.; Kumar, V.M. Sleep disorders in the elderly: A growing challenge. Psychogeriatrics 2018, 18, 155–165. [Google Scholar] [CrossRef]
- Yaremchuk, K. Sleep disorders in the elderly. Clin. Geriatr. Med. 2018, 34, 205–216. [Google Scholar] [CrossRef] [PubMed]
- Gulia, K.K.; Kumar, V.M. Importance of sleep for health and wellbeing amidst covid-19 pandemic. Sleep Vigil. 2020, 4, 49–50. [Google Scholar] [CrossRef] [PubMed]
- Wang, J.; Gong, Y.; Chen, Z.; Wu, J.; Feng, J.; Yan, S.; Lv, C.; Lu, Z.; Mu, K.; Yin, X. Sleep disturbances among Chinese residents during the Coronavirus Disease 2019 outbreak and associated factors. Sleep Med. 2020, 74, 199–203. [Google Scholar] [CrossRef] [PubMed]
- Emerson, K.G. Coping with being cooped up: Social distancing during COVID-19 among 60+ in the United States. Rev. Panam. Salud. Publica. 2020, 44, e81. [Google Scholar] [CrossRef] [PubMed]
- Knepple Carney, A.; Graf, A.S.; Hudson, G.; Wilson, E. Age moderates perceived COVID-19 disruption on well-being. Gerontologist 2021, 61, 30–35. [Google Scholar] [CrossRef]
- Röhr, S.; Reininghaus, U.; Riedel-Heller, S.G. Mental wellbeing in the German old age population largely unaltered during COVID-19 lockdown: Results of a representative survey. BMC Geriatr. 2020, 20, 1–12. [Google Scholar] [CrossRef]
- Lopez, J.; Perez-Rojo, G.; Noriega, C.; Carretero, I.; Velasco, C.; Martinez-Huertas, J.A.; López-Frutos, P.; Galarraga, L. Psychological well-being among older adults during the COVID-19 outbreak: A comparative study of the young–old and the old–old adults. Int. Psychogeriatr. 2020, 32, 1365–1370. [Google Scholar] [CrossRef]
- Scudellari, M. The pandemic’s future. Nature 2020, 584, 22–25. [Google Scholar] [CrossRef]
- Ammar, A.; Chtourou, H.; Boukhris, O.; Trabelsi, K.; Masmoudi, L.; Brach, M.; Bouaziz, B.; Bentlage, E.; How, D.; Ahmed, M.; et al. COVID-19 home confinement negatively impacts social participation and life satisfaction: A worldwide multicentre study. Int. J. Environ. Res. Public Health 2020, 17, 6237. [Google Scholar] [CrossRef] [PubMed]
- Stewart-Brown, S.; Tennant, A.; Tennant, R.; Platt, S.; Parkinson, J.; Weich, S. Internal construct validity of the Warwick-Edinburgh Mental Wellbeing Scale (WEMWBS): A Rasch analysis using data from the Scottish Health Education Population Survey. Health Qual. Life Outcomes 2009, 7, 1–8. [Google Scholar] [CrossRef]
- Fat, L.N.; Scholes, S.; Boniface, S.; Mindell, J.; Stewart-Brown, S. Evaluating and establishing national norms for mental wellbeing using the short Warwick–Edinburgh mental wellbeing scale (SWEMWBS): Findings from the health survey for England. Qual. Life Res. 2017, 26, 1129–1144. [Google Scholar] [CrossRef] [PubMed]
- Warwick Medical School. Collect, Score, Analyse and Interpret WEMWBS. 2020. Available online: https://warwick.ac.uk/fac/sci/med/research/platform/wemw (accessed on 1 April 2020).
- Buysse, D.J.; Reynolds, C.F.; Monk, T.H.; Berman, S.R.; Kupfer, D.J. The Pittsburgh Sleep Quality Index: A new instrument for psychiatric practice and research. Psychiatry Res. 1989, 28, 193–213. [Google Scholar] [CrossRef]
- Chehri, A.; Nourozi, M.; Eskandari, S.; Khazaie, H.; Hemati, N.; Jalali, A. Validation of the Persian version of the Pittsburgh Sleep Quality Index in elderly population. Sleep Sci. 2020, 13, 119. [Google Scholar] [CrossRef] [PubMed]
- IPAQ Research Committee. International Physical Activity Questionnaire: Short Last 7 Days Self-Administered Format. 2005. Available online: http//www.Ipaq.Ki.Se (accessed on 1 April 2020).
- Rosenthal, R.; Cooper, H.; Hedges, L. Parametric measures of effect size. Handb. Res. Synth. 1994, 621, 231–244. [Google Scholar]
- Petry, N.M. A comparison of young, middle-aged, and older adult treatment-seeking pathological gamblers. Gerontologist 2002, 42, 92–99. [Google Scholar] [CrossRef] [PubMed]
- Coolidge, F.L.; Segal, D.L.; Hook, J.N.; Stewart, S. Personality disorders and coping among anxious older adults. J. Anxiety Disord. 2000, 14, 157–172. [Google Scholar] [CrossRef]
- Laguna, K.; Babcock, R.L. Computer anxiety in young and older adults: Implications for human-computer interactions in older populations. Comput. Hum. Behav. 1997, 13, 317–326. [Google Scholar] [CrossRef]
- Reynolds, K.; Pietrzak, R.H.; El-Gabalawy, R.; Mackenzie, C.S.; Sareen, J. Prevalence of psychiatric disorders in US older adults: Findings from a nationally representative survey. World Psychiatry 2015, 14, 74–81. [Google Scholar] [CrossRef]
- O’Connor, R.C.; Wetherall, K.; Cleare, S.; McClelland, H.; Melson, A.J.; Niedzwiedz, C.L.; O’Carroll, R.E.; O’Connor, D.B.; Platt, S.; Scowcroft, E.; et al. Mental health and wellbeing during the COVID-19 pandemic: Longitudinal analyses of adults in the UK COVID-19 Mental Health & Wellbeing study. Br. J. Psychiatry 2020, 1–8. [Google Scholar]
- Kivi, M.; Hansson, I.; Bjälkebring, P. Up and about: Older adults’ wellbeing during the COVID-19 pandemic in a Swedish longitudinal study. J. Gerontol. Ser. B 2020, 76, e4–e9. [Google Scholar] [CrossRef]
- Brandtstädter, J.; Renner, G. Tenacious goal pursuit and flexible goal adjustment: Explication and age-related analysis of assimilative and accommodative strategies of coping. Psychol. Aging 1990, 5, 58. [Google Scholar] [CrossRef]
- Okely, J.A.; Corley, J.; Welstead, M.; Taylor, A.M.; Page, D.; Skarabela, B.; Redmond, P.; Cox, S.R.; Russ, T.C. Change in Physical Activity, Sleep Quality, and Psychosocial Variables during COVID-19 Lockdown: Evidence from the Lothian Birth Cohort 1936. Int. J. Environ. Res. Public Health 2021, 18, 210. [Google Scholar] [CrossRef]
- Bentlage, E.; Ammar, A.; How, D.; Ahmed, M.; Trabelsi, K.; Chtourou, H.; Brach, M. Practical Recommendations for Maintaining Active Lifestyle during the COVID-19 Pandemic: A Systematic Literature Review. Int. J. Environ. Res. Public Health 2020, 17, 6265. [Google Scholar] [CrossRef]
- World Health Organization. Global Recommendations on Physical Activity for Health; WHO Press: Geneva, Switzerland; Available online: http://apps.who.int/iris/bitstream/10665/44399/1/9789241599979_eng.pdf (accessed on 22 April 2020).
- Sañudo, B.; Fennell, C.; Sánchez-Oliver, A.J. Objectively-assessed physical activity, sedentary behavior, smartphone use, and sleep patterns pre-and during-COVID-19 quarantine in young adults from Spain. Sustainability 2020, 12, 5890. [Google Scholar] [CrossRef]
- Patterson, R.; McNamara, E.; Tainio, M.; de Sá, T.H.; Smith, A.D.; Sharp, S.J.; Edwards, P.; Woodcock, J.; Brage, S.; Wijndaele, K. Sedentary behaviour and risk of all-cause, cardiovascular and cancer mortality, and incident type 2 diabetes: A systematic review and dose response meta-analysis. Eur. J. Epidemiol. 2018, 33, 811–829. [Google Scholar] [CrossRef]
- Hirshkowitz, M.; Whiton, K.; Albert, S.M.; Alessi, C.; Bruni, O.; DonCarlos, L.; Hazen, N.; Herman, J.; Adams Hillard, P.J.; Katz, E.S.; et al. National Sleep Foundation’s updated sleep duration recommendations: Final report. Sleep Health 2015, 1, 233–243. [Google Scholar] [CrossRef]
- Kripke, D.F.; Langer, R.D.; Elliott, J.A.; Klauber, M.R.; Rex, K.M. Mortality related to actigraphic long and short sleep. Sleep Med. 2011, 12, 28–33. [Google Scholar] [CrossRef]
- Buxton, O.M.; Marcelli, E. Short and long sleep are positively associated with obesity, diabetes, hypertension, and cardiovascular disease among adults in the United States. Soc. Sci. Med. 2010, 71, 1027–1036. [Google Scholar] [CrossRef]
- Stone, C.R.; Haig, T.R.; Fiest, K.M.; McNeil, J.; Brenner, D.R.; Friedenreich, C.M. The association between sleep duration and cancer-specific mortality: A systematic review and meta-analysis. Cancer Causes Control 2019, 30, 501–525. [Google Scholar] [CrossRef]
- Yeo, Y.; Ma, S.H.; Park, S.K.; Chang, S.H.; Shin, H.R.; Kang, D.; Yoo, K.Y. A prospective cohort study on the relationship of sleep duration with all-cause and disease-specific mortality in the Korean Multi-center Cancer Cohort study. J. Prev. Med. Public Health 2013, 46, 271–281. [Google Scholar] [CrossRef]
- Chen, J.C.; Espeland, M.A.; Brunner, R.L.; Lovato, L.C.; Wallace, R.B.; Leng, X.; Phillips, L.S.; Robinson, J.G.; Kotchen, J.M.; Johnson, K.C.; et al. Sleep duration, cognitive decline, and dementia risk in older women. Alzheimers Dement. 2016, 12, 21–33. [Google Scholar] [CrossRef]
- Thomas, D.; Anderson, W.M. Multiple Sleep Latency Test (MSLT); Encyclopedia of Sleep; Kushida, C.A., Ed.; Academic Press: Waltham, MA, USA, 2013; pp. 96–99. [Google Scholar]
- Verity, R.; Okell, L.C.; Dorigatti, I.; Winskill, P.; Whittaker, C.; Imai, N.; Cuomo-Dannenburg, G.; Thompson, H.; Walker, P.G.T.; Fu, H.; et al. Estimates of the severity of coronavirus disease 2019: A model-based analysis. Lancet Infect. Dis. 2020, 20, 669–677. [Google Scholar] [CrossRef]
- Altena, E.; Baglioni, C.; Espie, C.A.; Ellis, J.; Gavriloff, D.; Holzinger, B.; Schlarb, A.; Frase, L.; Jernelöv, S.; Riemann, D. Dealing with sleep problems during home confinement due to the COVID-19 outbreak: Practical recommendations from a task force of the European CBT-I Academy. J. Sleep Res. 2020, 29, e13052. [Google Scholar] [CrossRef]
- Bower, B.; Bylsma, L.M.; Morris, B.H.; Rottenberg, J. Poor reported sleep quality predicts low positive affect in daily life among healthy and mood-disordered persons. J. Sleep Res. 2010, 19, 323–332. [Google Scholar] [CrossRef] [PubMed]
- Desjardins, S.; Lapierre, S.; Hudon, C.; Desgagné, A. Factors involved in sleep efficiency: A population-based study of community-dwelling elderly persons. Sleep 2019, 42, zsz038. [Google Scholar] [CrossRef] [PubMed]
- Dew, M.A.; Hoch, C.C.; Buysse, D.J.; Monk, T.H.; Begley, A.E.; Houck, P.R.; Hall, M.; Kupfer, D.J.; Reynolds, C.F., III. Healthy older adults’ sleep predicts all-cause mortality at 4 to 19 years of follow-up. Psychosom. Med. 2003, 65, 63–73. [Google Scholar] [CrossRef] [PubMed]
- Chan, J.S.; Liu, G.; Liang, D.; Deng, K.; Wu, J.; Yan, J.H. Special issue—Therapeutic benefits of physical activity for mood: A systematic review on the effects of exercise intensity, duration, and modality. J. Psychol. 2019, 153, 102–125. [Google Scholar] [CrossRef]
- Lippi, G.; Mattiuzzi, C.; Sanchis-Gomar, F. Updated overview on interplay between physical exercise, neurotrophins, and cognitive function in humans. J. Sport Health Sci. 2020, 9, 74–81. [Google Scholar] [CrossRef]
- Phillips, C. Brain-derived neurotrophic factor, depression, and physical activity: Making the neuroplastic connection. Neural Plast. 2017. [Google Scholar] [CrossRef]
- Sun, Y.; Shi, L.; Bao, Y.; Sun, Y.; Shi, J.; Lu, L. The bidirectional relationship between sleep duration and depression in community-dwelling middle-aged and elderly individuals: Evidence from a longitudinal study. Sleep Med. 2018, 52, 221–229. [Google Scholar] [CrossRef]
- Ben Simon, E.; Vallat, R.; Barnes, C.M.; Walker, M.P. Sleep Loss and the Socio-Emotional Brain. Trends Cogn. Sci. 2020, 24, 435–450. [Google Scholar] [CrossRef]
- Wu, C.Y.; Su, T.P.; Fang, C.L.; Chang, M.Y. Sleep quality among community-dwelling elderly people and its demographic, mental, and physical correlates. J. Chin. Med. Assoc. 2012, 75, 75–80. [Google Scholar] [CrossRef]
- Van den Berg, J.F.; Luijendijk, H.J.; Tulen, J.H.; Hofman, A.; Neven, A.K.; Tiemeier, H. Sleep in depression and anxiety disorders: A population-based study of elderly persons. J. Clin. Psychiat. 2009, 70, 1105–1113. [Google Scholar] [CrossRef]
- Braun, V.; Clarke, V.; Boulton, E.; Davey, L.; McEvoy, C. The online survey as a qualitative research tool. Int. J. Soc. Res. Methodol. 2020, 1–14. [Google Scholar] [CrossRef]
- Sharma, A.J.; Subramanyam, M.A. A cross-sectional study of psychological wellbeing of Indian adults during the Covid-19 lockdown: Different strokes for different folks. PLoS ONE 2020, 15, e0238761. [Google Scholar] [CrossRef]
- Lee, P.H.; Marek, J.; Nálevka, P. Sleep pattern in the US and 16 European countries during the COVID-19 outbreak using crowdsourced smartphone data. Eur. J. Public Health 2020, 31, 23–30. [Google Scholar] [CrossRef]
- Tran, D.V.; Lee, A.H.; Au, T.B.; Nguyen, C.T.; Hoang, D.V. Reliability and validity of the International Physical Activity Questionnaire—Short Form for older adults in Vietnam. Health Promot. J. Austr. 2013, 24, 126–131. [Google Scholar] [CrossRef]
- Xin, C.; Zhang, B.; Fang, S.; Zhou, J. Daytime napping and successful aging among older adults in China: A cross-sectional study. BMC Geriatr. 2020, 20, 1–12. [Google Scholar] [CrossRef]
- Ammar, A.; Bouaziz, B.; Trabelsi, K.; Glenn, J.; Zmijewski, P.; Müller, P.; Chtourou, H.; Jmaiel, M.; Chamari, K.; Driss, T.; et al. Applying digital technology to promote active and healthy confinement lifestyle during pandemics in the elderly. Biol. Sport 2021, 38, 391–396. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Variables | n | (%) |
|---|---|---|
| Age (years) | ||
| 56–60 | 255 | (49.3%) |
| 61–65 | 138 | (26.7%) |
| 66–70 | 76 | (14.7%) |
| 71–75 | 23 | (4.4%) |
| 76–80 | 18 | (3.5%) |
| >80 | 7 | (1.4%) |
| Sex | ||
| Female | 270 | (52.2%) |
| Male | 247 | (47.8%) |
| Continent | ||
| Europe (16 countries) | 259 | (50.1%) |
| America (5 countries) | 155 | (30%) |
| North-Africa (3 countries) | 48 | (9.3%) |
| Western-Asia (4 countries) | 35 | (6.8%) |
| Others (5 countries) | 20 | (3.9%) |
| Level of Education | ||
| Master/doctorate degree | 256 | (49.5%) |
| Bachelor’s degree | 138 | (26.7%) |
| High school graduate, diploma, professional degree or the equivalent | 114 | (22.1%) |
| No schooling completed | 9 | (1.7%) |
| Marital Status | ||
| Single | 52 | (10.1%) |
| Married/Living as couple | 376 | (72.7%) |
| Widowed/Divorced/Separated | 89 | (17.2%) |
| Employment Status | ||
| Employed for wages | 239 | (46.2%) |
| Self-employed | 60 | (11.6%) |
| Out of work/Unemployed | 16 | (3.1%) |
| Student | 2 | (0.4%) |
| Retired | 169 | (32.7%) |
| Unable to work | 8 | (1.5%) |
| Problem/unemployment caused by COVID-19 | 11 | (2.1%) |
| Other | 12 | (2.3%) |
| Health Status | ||
| Healthy | 349 | (67.5%) |
| With risk factors for cardiovascular disease | 150 | (29%) |
| With cardiovascular disease | 18 | (3.5%) |
| Members Sharing the Same House | ||
| 0 (live alone) | 85 | (16.4%) |
| 1 | 241 | (46.6%) |
| 2 | 107 | (20.7%) |
| 3 | 55 | (10.6%) |
| >3 | 29 | (5.6%) |
| Parameters | Means ± SD | Δ (Δ%) | T (Wilcoxon) | Z | p-Value | ES | |
|---|---|---|---|---|---|---|---|
| Pre-Lockdown | During Lockdown | ||||||
| I’ve been feeling optimistic about the future | 4.01 ± 0.83 | 3.47 ± 1.01 | −0.54 (−13.5%) | 1634.0 | 12.28 | <0.001 | 0.78 |
| I’ve been feeling useful | 4.12 ± 0.77 | 3.74 ± 1 | −0.38 (−9.2%) | 1885.0 | 9.42 | <0.001 | 0.69 |
| I’ve been feeling relaxed | 3.7 ± 0.87 | 3.27 ± 1 | −0.43 (−11.6%) | 7849.0 | 8.60 | <0.001 | 0.52 |
| I’ve been dealing with problems well | 4.02 ± 0.69 | 3.78 ± 0.79 | −0.25 (−6.1%) | 1655.0 | 7.65 | <0.001 | 0.62 |
| I’ve been thinking clearly | 4.2±0.67 | 3.93±0.83 | −0.27 (−6.5%) | 1398.5 | 8.06 | <0.001 | 0.66 |
| I’ve been feeling close to other people | 4.11±0.76 | 3.6±1.04 | −0.51 (−12.4%) | 2977.0 | 10.57 | <0.001 | 0.69 |
| I’ve been able to make up my own mind about things | 4.37±0.69 | 4.12±0.85 | −0.25 (−5.7%) | 918.5 | 7.82 | <0.001 | 0.68 |
| Total metric score | 28.54±3.83 | 25.91±4.66 | −2.63 (−9.2%) | 6942.0 | 14.30 | <0.001 | 0.72 |
| Parameters | Means ±SD | Δ (Δ%) | T (Wilcoxon) | Z | p-Value | ES | |
|---|---|---|---|---|---|---|---|
| Pre-Lockdown | During Lockdown | ||||||
| Sleep latency (min) | 19.99 ± 27.05 | 26.53 ± 39.18 | 6.54 (32.7%) | 1042.5 | 8.56 | <0.001 | 0.70 |
| Sleep duration (h) | 6.80 ± 1.23 | 6.96 ± 1.42 | 0.16 (2.4%) | 9946 | 3.30 | <0.001 | 0.22 |
| Subjective sleep quality (A.U) | 0.90 ± 0.66 | 1.05 ± 0.77 | 0.15 (16.6%) | 1340 | 5.66 | <0.001 | 0.53 |
| Time in bed (h) | 7.99 ± 1.46 | 8.31 ± 1.56 | 0.32 (4%) | 16,096.5 | 6.98 | <0.001 | 0.38 |
| Sleep efficiency (%) | 86.10 ± 13.1 | 84.70 ± 14.7 | −1.36 (−1.6%) | 27,022.5 | 2.61 | 0.009 | 0.14 |
| Sleep disturbance (A.U) | 1.41 ± 0.64 | 1.53 ± 0.69 | 0.13 (9.1%) | 728 | 5.67 | <0.001 | 0.58 |
| Daytime dysfunction (A.U) | 0.80 ± 0.99 | 1.17 ± 1.24 | 0.37 (46.6%) | 3755 | 7.28 | <0.001 | 0.52 |
| Use of hypnotic medication (A.U) | 0.38 ± 0.85 | 0.44 ± 0.94 | 0.06 (17%) | 292.5 | 3.47 | <0.001 | 0.49 |
| Total score of PSQI (A.U) | 4.88 ± 2.86 | 5.69 ± 3.37 | 0.81 (16.7%) | 15011 | 8.00 | <0.001 | 0.43 |
| Parameters | Means ±SD | Δ (Δ%) | T (Wilcoxon) | Z | p-Value | ES | ||
|---|---|---|---|---|---|---|---|---|
| Pre-Lockdown | During Lockdown | |||||||
| Vigorous intensity | Days/week | 1.95 ± 2.05 | 1.61 ± 2.1 | −0.34 (−17.4%) | 7523 | 4.82 | <0.001 | 0.33 |
| min/week | 37.84 ± 52.58 | 29.73 ± 50.13 | −8.12 (−21.4%) | 2688 | 5.92 | <0.001 | 0.48 | |
| MET values | 954 ± 1807 | 783 ± 1868 | −171 (−17.9%) | 8671 | 4.90 | <0.001 | 0.32 | |
| Moderate intensity | Days/week | 2.38 ± 2.11 | 1.86 ± 2.24 | −0.52 (−22%) | 8943.5 | 6.26 | <0.001 | 0.39 |
| min/week | 45.21 ± 50.77 | 35.3 ± 49.59 | −9.91 (−21.9%) | 3626.5 | 6.68 | <0.001 | 0.49 | |
| MET values | 574 ± 853 | 457 ± 844 | −116 (−20.3%) | 10,910 | 5.82 | <0.001 | 0.35 | |
| Walking | Days/week | 3.91 ± 2.39 | 2.89 ± 2.63 | −1.03 (−26.2%) | 9449.5 | 9.22 | <0.001 | 0.52 |
| min/week | 44.48 ± 45.86 | 36.58 ± 38 | −7.9 (−17.8%) | 7960 | 5.03 | <0.001 | 0.33 | |
| MET values | 673 ± 870 | 518 ± 792 | −155 (−23.1%) | 17,299 | 6.24 | <0.001 | 0.34 | |
| All PA | Days/week | 5.62 ± 2.11 | 4.34 ± 2.73 | −1.28 (−22.7%) | 3263 | 11.25 | <0.001 | 0.70 |
| min/week | 128 ± 108 | 102 ± 106 | −26 (−20.3%) | 9886 | 8.72 | <0.001 | 0.50 | |
| MET values | 2201 ± 2604 | 1759 ± 2748 | −443 (−20.1%) | 23,207.5 | 7.77 | <0.001 | 0.38 | |
| Sitting | hours/day | 5.33 ± 3.03 | 6.78 ± 3.47 | 1.45 (27.2%) | 3416.5 | 12.99 | <0.001 | 0.74 |
| Models | Predictor Variable | UC | SC | T | p-Value | R | SEE | Adjusted R2 | F | p-Value | |
|---|---|---|---|---|---|---|---|---|---|---|---|
| b | SE | β | |||||||||
| Model 1 | (Constant) | −2.307 | 1.972 | −1.170 | 0.242 | 3.31 | 0.015 | 1.99 | 0.045 | ||
| Age | 0.006 | 0.028 | 0.011 | 0.225 | 0.822 | −0.030 | |||||
| Sex | −0.283 | 0.303 | −0.043 | −0.935 | 0.350 | −0.062 | |||||
| Continent | 0.018 | 0.138 | 0.006 | 0.127 | 0.899 | 0.018 | |||||
| Level of education | 0.346 | 0.178 | 0.089 | 1.947 | 0.052 | 0.120 | |||||
| Marital status | −0.232 | 0.285 | −0.036 | −0.815 | 0.415 | −0.050 | |||||
| Employment status | −0.086 | 0.080 | −0.054 | −1.075 | 0.283 | −0.084 | |||||
| Health status | −0.371 | 0.275 | −0.061 | −1.347 | 0.179 | −0.087 | |||||
| Δ house members | 0.456 | 0.295 | 0.068 | 1.548 | 0.122 | 0.084 | |||||
| Model 2 | (Constant) | −2.169 | 1.985 | −1.093 | 0.275 | 3.31 | 0.014 | 1.82 | 0.063 | ||
| Age | 0.004 | 0.028 | 0.007 | 0.147 | 0.883 | −0.030 | |||||
| Sex | −0.288 | 0.303 | −0.043 | −0.949 | 0.343 | −0.062 | |||||
| Continent | 0.030 | 0.140 | 0.010 | 0.216 | 0.829 | 0.018 | |||||
| Level of education | 0.346 | 0.178 | 0.089 | 1.943 | 0.053 | 0.120 | |||||
| Marital status | −0.226 | 0.285 | −0.035 | −0.793 | 0.428 | −0.050 | |||||
| Employment status | −0.084 | 0.080 | −0.052 | −1.045 | 0.296 | −0.084 | |||||
| Health status | −0.355 | 0.277 | −0.058 | −1.282 | 0.200 | −0.087 | |||||
| Δ house members | 0.469 | 0.296 | 0.070 | 1.586 | 0.113 | 0.084 | |||||
| Δ sitting | −0.043 | 0.068 | −0.028 | −0.634 | 0.527 | −0.028 | |||||
| Model 3 | (Constant) | −1.838 | 1.903 | −0.965 | 0.335 | 3.17 | 0.094 | 6.35 | <0.001 | ||
| Age | −0.001 | 0.027 | −0.002 | −0.044 | 0.965 | −0.030 | |||||
| Sex | −0.227 | 0.291 | −0.034 | −0.781 | 0.435 | −0.062 | |||||
| Continent | −0.097 | 0.135 | −0.032 | −0.716 | 0.474 | 0.018 | |||||
| Level of education | 0.362 | 0.171 | 0.093 | 1.941 | 0.054 | 0.120 | |||||
| Marital status | −0.208 | 0.273 | −0.032 | −0.761 | 0.447 | −0.050 | |||||
| Employment status | −0.092 | 0.077 | −0.057 | −1.195 | 0.233 | −0.084 | |||||
| Health Status | −0.256 | 0.266 | −0.042 | −0.965 | 0.335 | −0.087 | |||||
| Δ house members | 0.340 | 0.284 | 0.051 | 1.196 | 0.232 | 0.084 | |||||
| Δ sitting | 0.059 | 0.067 | 0.039 | 0.878 | 0.380 | −0.028 | |||||
| Δ All PA (MET values) | 0.0004 | 0.0001 | 0.295 | 7.195 | 0.000 | 0.290 | |||||
| Model 4 | (Constant) | −1.607 | 1.782 | −0.902 | 0.367 | 2.967 | 0.206 | 13.2 | <0.001 | ||
| Age | −0.007 | 0.025 | −0.013 | −0.279 | 0.780 | −0.030 | |||||
| Sex | −0.167 | 0.272 | −0.025 | −0.614 | 0.540 | −0.062 | |||||
| Continent | −0.104 | 0.127 | −0.034 | −0.818 | 0.414 | 0.018 | |||||
| Level of education | 0.346 | 0.160 | 0.089 | 1.734 | 0.067 | 0.120 | |||||
| Marital status | −0.275 | 0.256 | −0.043 | −1.077 | 0.282 | −0.050 | |||||
| Employment status | −0.050 | 0.072 | −0.031 | −0.690 | 0.491 | −0.084 | |||||
| Health status | 0.161 | 0.253 | 0.027 | 0.637 | 0.524 | −0.087 | |||||
| Δ house members | 0.269 | 0.266 | 0.040 | 1.012 | 0.312 | 0.084 | |||||
| Δ sitting | 0.047 | 0.063 | 0.031 | 0.747 | 0.456 | −0.028 | |||||
| Δ All PA (MET values) | 0.0004 | 0.0001 | 0.293 | 7.183 | 0.000 | 0.290 | |||||
| Δ PSQI | −0.518 | 0.061 | −0.343 | −8.526 | 0.000 | −0.354 | |||||
| Model 5 | (Constant) | −1.777 | 0.142 | −12.535 | 0.000 | 2.975 | 0.202 | 66.41 | <0.001 | ||
| Δ All PA (MET values) | 0.0004 | 0.0001 | 0.284 | 7.210 | 0.000 | 0.290 | |||||
| Δ PSQI | −0.525 | 0.059 | −0.348 | −8.854 | 0.000 | −0.354 | |||||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Trabelsi, K.; Ammar, A.; Masmoudi, L.; Boukhris, O.; Chtourou, H.; Bouaziz, B.; Brach, M.; Bentlage, E.; How, D.; Ahmed, M.; et al. Sleep Quality and Physical Activity as Predictors of Mental Wellbeing Variance in Older Adults during COVID-19 Lockdown: ECLB COVID-19 International Online Survey. Int. J. Environ. Res. Public Health 2021, 18, 4329. https://doi.org/10.3390/ijerph18084329
Trabelsi K, Ammar A, Masmoudi L, Boukhris O, Chtourou H, Bouaziz B, Brach M, Bentlage E, How D, Ahmed M, et al. Sleep Quality and Physical Activity as Predictors of Mental Wellbeing Variance in Older Adults during COVID-19 Lockdown: ECLB COVID-19 International Online Survey. International Journal of Environmental Research and Public Health. 2021; 18(8):4329. https://doi.org/10.3390/ijerph18084329
Chicago/Turabian StyleTrabelsi, Khaled, Achraf Ammar, Liwa Masmoudi, Omar Boukhris, Hamdi Chtourou, Bassem Bouaziz, Michael Brach, Ellen Bentlage, Daniella How, Mona Ahmed, and et al. 2021. "Sleep Quality and Physical Activity as Predictors of Mental Wellbeing Variance in Older Adults during COVID-19 Lockdown: ECLB COVID-19 International Online Survey" International Journal of Environmental Research and Public Health 18, no. 8: 4329. https://doi.org/10.3390/ijerph18084329
APA StyleTrabelsi, K., Ammar, A., Masmoudi, L., Boukhris, O., Chtourou, H., Bouaziz, B., Brach, M., Bentlage, E., How, D., Ahmed, M., Mueller, P., Mueller, N., Hsouna, H., Elghoul, Y., Romdhani, M., Hammouda, O., Paineiras-Domingos, L. L., Braakman-Jansen, A., Wrede, C., ... on behalf of the ECLB-COVID19 Consortium. (2021). Sleep Quality and Physical Activity as Predictors of Mental Wellbeing Variance in Older Adults during COVID-19 Lockdown: ECLB COVID-19 International Online Survey. International Journal of Environmental Research and Public Health, 18(8), 4329. https://doi.org/10.3390/ijerph18084329