
Municipal Solid Waste Management and Adverse Health Outcomes: A Systematic Review

 ,
,  , ,
, , 

Abstract
1. Introduction
2. Methods
2.1. Definitions
- Municipal solid waste (MSW): any material from residential, commercial, and institutional activities which is discarded. It is important to note that industrial, medical, hazardous, electronic, and construction and demolition wastes belong to other categories [2].
- Engineered landfill: site characterized by the registration and placement/compaction of waste. Such landfills typically use daily cover material, surface and ground water monitoring, infrastructure, and a waterproof liner at the bottom [6].
- Sanitary landfill: site characterized by the registration and placement/compaction of waste. Best practices include a waterproof liner at the bottom, leachate and gas collection systems, daily cover, a final top cover and closure, infrastructure as well as a post-closure plan [6].
- Transfer stations: facilities in which waste is transferred from smaller vehicles used for waste collection into bigger vehicles for hauling to a disposal or treatment site [32].
- Incinerators: a specialized engineered system where waste is burned. Through combustion waste is converted into ash, flue gas, and heat. The flue gases are treated to reduce impact of air pollution on environment and health. Energy from an incinerator can be recovered [32].
- Open burning of waste: burning of solid waste in open areas without air pollution controls [32].
2.2. Study Eligibility
2.3. Search Strategy; Screening and Data Extraction; Narrative Review
2.4. Risk of Bias; Quantity and Strength of Evidence
3. Results
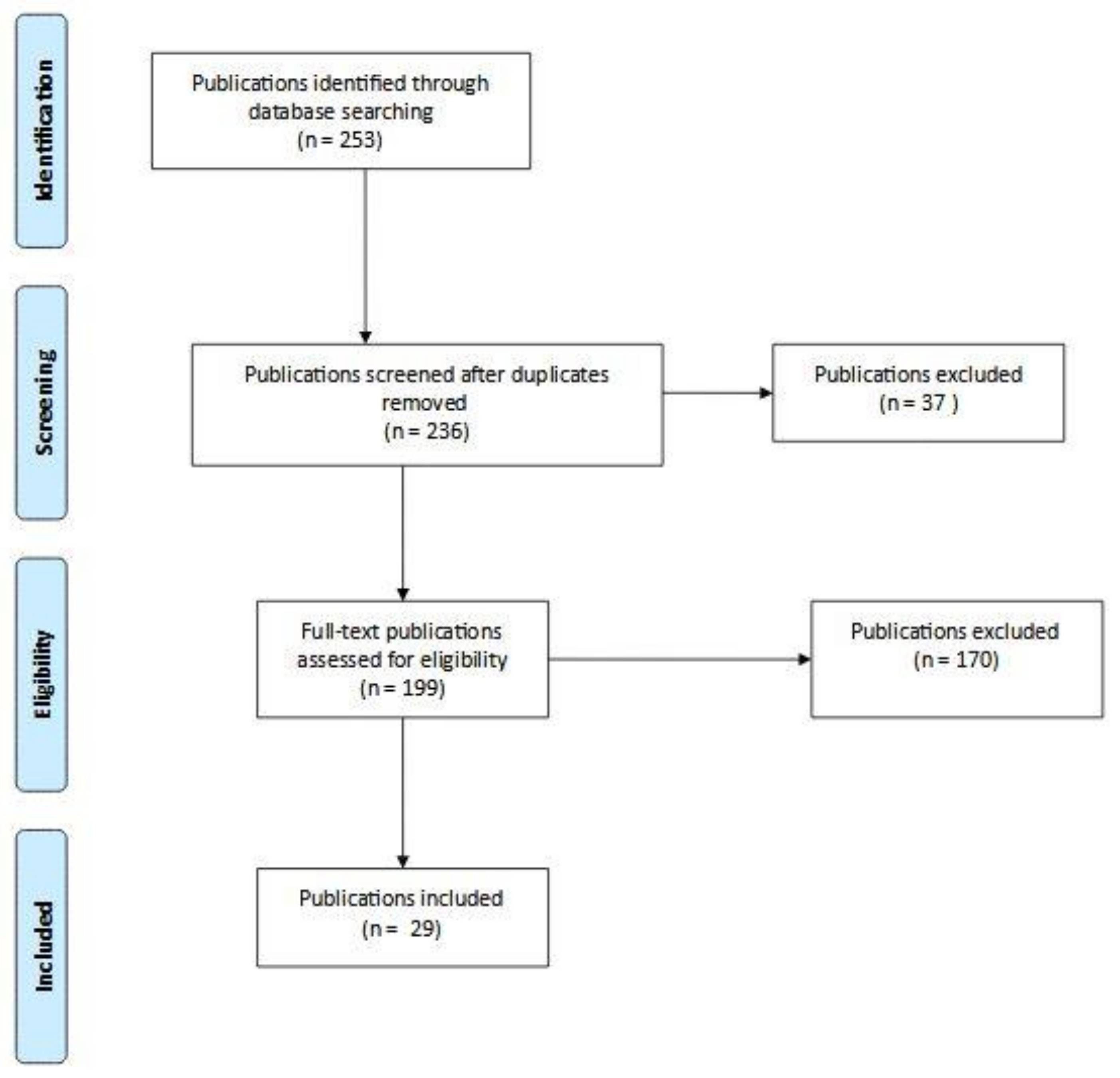
3.1. Study Selection
3.2. MSW Transfer and Treatment Sites
3.3. MSW Disposal Sites
3.3.1. Landfills
3.3.2. Incinerators
3.3.3. Dumpsites and Open Burning
3.4. Study Quality
3.5. Summary of Results
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- WHO (World Health Organization). Waste and Human Health: Evidence and Needs; WHO Meeting Report; World Health Organization: Bonn, Germany, 5–6 November 2015. [Google Scholar]
- Kaza, S.; Yao, L.C.; Bhada-Tata, P.; Van Woerden, F. What a Waste 2.0: A Global Snapshot of Solid Waste Management to 2050; Urban Development; World Bank: Washington, DC, USA, 2018. [Google Scholar]
- Perteghella, A.; Gilioli, G.; Tudor, T.; Vaccari, M. Utilizing an integrated assessment scheme for sustainable waste management in low and middle-income countries: Case studies from Bosnia-Herzegovina and Mozambique. Waste Manag. 2018, 113, 176–185. [Google Scholar] [CrossRef]
- Wilson, D.C.; Rodic, L.; Modak, P.; Soos, R.; Carpintero Rogero, A.; Velis, C.; Iyer, M.; Simonett, O. Global Waste Management Outlook Report; UNEP: Nairobi, Kenya, 2015. [Google Scholar]
- Ferronato, N.; Torretta, V. Waste mismanagement in developing countries: A review of global issues. Int. J. Environ. Res. Public Health 2019, 16, 1060. [Google Scholar] [CrossRef] [PubMed]
- Vaccari, M.; Tudor, T.; Vinti, G. Characteristics of leachate from landfills and dumpsites in Asia, Africa and Latin America: An overview. Waste Manag. 2019, 95, 416–431. [Google Scholar] [CrossRef]
- Di Bella, V.; Vaccari, M. Constraints for solid waste management in Somaliland. Proceedings of institution of civil engineers. Waste Resour. Manag. 2014, 167, 62–71. [Google Scholar] [CrossRef]
- Ziraba, A.K.; Haregu, T.N.; Mberu, B. A review and framework for understanding the potential impact of poor solid waste management on health in developing countries. Arch. Public Health 2016, 74, 55. [Google Scholar] [CrossRef]
- Xu, P.; Chen, Z.; Wu, L.; Chen, Y.; Xu, D.; Shen, H.; Han, J.; Wang, X.; Lou, X. Health risk of childhood exposure to PCDD/Fs emitted from a municipal waste incinerator in Zhejiang, China. Sci. Total Environ. 2019, 689, 937–944. [Google Scholar] [CrossRef]
- Vaccari, M.; Vinti, G.; Tudor, T. An analysis of the risk posed by leachate from dumpsites in developing countries. Environments 2018, 5, 99. [Google Scholar] [CrossRef]
- Negi, P.; Mor, S.; Ravindra, K. Impact of landfill leachate on the groundwater quality in three cities of North India and health risk assessment. Environ. Dev. Sustain. 2020, 22, 1455–1474. [Google Scholar] [CrossRef]
- Cointreau, S. Occupational and Environmental Health Issues of Solid Waste Management: Special Emphasis on Middle and Lower-Income Countries; World Bank: Washington, DC, USA, 2006. [Google Scholar]
- Porta, D.; Milani, S.; Lazzarino, A.I.; Perucci, C.A.; Forastiere, F. Systematic review of epidemiological studies on health effects associated with management of solid waste. Environ. Health 2009, 8, 60. [Google Scholar] [CrossRef] [PubMed]
- Mattiello, A.; Chiodini, P.; Bianco, E.; Forgione, N.; Flammia, I.; Gallo, C.; Pizzuti, R.; Panico, S. Health effects associated with the disposal of solid waste in landfills and incinerators in populations living in surrounding areas: A systematic review. Int. J. Public Health 2013, 58, 725–735. [Google Scholar] [CrossRef]
- Ashworth, D.C.; Elliott, P.; Toledano, M.B. Waste incineration and adverse birth and neonatal outcomes: A systematic review. Environ. Int. 2014, 69, 120–132. [Google Scholar] [CrossRef] [PubMed]
- Ncube, F.; Ncube, E.J.; Voyi, K. A systematic critical review of epidemiological studies on public health concerns of municipal solid waste handling. Perspect. Public Health 2017, 137, 102–108. [Google Scholar] [CrossRef] [PubMed]
- Tait, P.W.; Brew, J.; Che, A.; Costanzo, A.; Danyluk, A.; Davis, M.; Khalaf, A.; McMahon, K.; Watson, A.; Rowcliff, K.; et al. The health impacts of waste incineration: A systematic review. Aust. N. Z. J. Public Health 2020, 44, 40–48. [Google Scholar] [CrossRef]
- Pearson, C.; Littlewood, E.; Douglas, P.; Robertson, S.; Gant, T.W.; Hansell, A.L. Exposures and health outcomes in relation to bioaerosol emissions from composting facilities: A systematic review of occupational and community studies. J. Toxicol. Environ. Health B Crit. Rev. 2015, 18, 43–69. [Google Scholar] [CrossRef]
- Robertson, S.; Douglas, P.; Jarvis, D.; Marczylo, E. Bioaerosol exposure from composting facilities and health outcomes in workers and in the community: A systematic review update. Int. J. Hyg. Environ. Health 2019, 222, 364–386. [Google Scholar] [CrossRef]
- Abul, S. Environmental and health impact of solid waste disposal at Mangwaneni dumpsite in Manzini: Swaziland. J. Sustain. Dev. Afr. 2010, 12, 7. [Google Scholar]
- Krystosik, A.; Njoroge, G.; Odhiambo, L.; Forsyth, J.E.; Mutuku, F.; LaBeaud, A.D. Solid wastes provide breeding sites, burrows, and food for biological disease vectors, and urban zoonotic reservoirs: A call to action for solutions-based research. Front. Public Health 2020, 7, 405. [Google Scholar] [CrossRef]
- Liberati, A.; Altman, D.G.; Tetzlaff, J.; Mulrow, C.; Gøtzsche, P.C.; Ioannidis, J.; Clarke, M.; Devereaux, P.J.; Kleijnen, J.; Moher, D. The PRISMA statement for reporting systematic reviews and meta-analyses of studies that evaluate health care interventions: Explanation and elaboration. PLoS Med. 2009, 6, e1000100. [Google Scholar] [CrossRef] [PubMed]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G. The PRISMA group. preferred reporting items for systematic reviews and meta-analyses: The PRISMA statement. PLoS Med. 2009, 6, e1000097. [Google Scholar] [CrossRef] [PubMed]
- Ghosh, R.E.; Freni-Sterrantino, A.; Douglas, P.; Parkes, B.; Fecht, D.; de Hoogh, K.; Fuller, G.; Gulliver, J.; Font, A.; Smith, R.B.; et al. Fetal growth, stillbirth, infant mortality and other birth outcomes near UK municipal waste incinerators; retrospective population based cohort and case-control study. Environ. Int. 2019, 122, 151–158. [Google Scholar] [CrossRef]
- Parkes, B.; Hansell, A.L.; Ghosh, R.E.; Douglas, P.; Fecht, D.; Wellesley, D.; Kurinczuk, J.J.; ì Rankin, J.; de Hoogh, K.; Fuller, G.W.; et al. Risk of congenital anomalies near municipal waste incinerators in England and Scotland: Retrospective population-based cohort study. Environ. Int. 2020, 134, 104845. [Google Scholar] [CrossRef]
- Rosenfeld, P.E.; Feng, L.G.H. Risks of Hazardous Wastes; Hardcover; Elsevier: Amsterdam, The Netherlands, 2011; ISBN 9781437778427. [Google Scholar]
- Pellizzari, E.D.; Woodruff, T.J.; Boyles, R.R.; Kannan, K.; Beamer, P.I.; Buckley, J.P.; Wang, A.; Zhu, Y.; Bennett, D.H. Identifying and prioritizing chemicals with uncertain burden of exposure: Opportunities for biomonitoring and health-related research. Environ. Health Perspect. 2019, 127, 126001. [Google Scholar] [CrossRef]
- Seltenrich, N. Beyond the light under the lamppost: New chemical candidates for biomonitoring in young children. Environ. Health Perspect. 2020, 128, 84005. [Google Scholar] [CrossRef] [PubMed]
- La Merrill, M.A.; Johnson, C.L.; Smith, M.T.; Kandula, N.R.; Macherone, A.; Pennell, K.D.; Kanaya, A.M. Exposure to persistent organic pollutants (POPs) and their relationship to hepatic fat and insulin insensitivity among asian indian immigrants in the united states. Environ. Sci. Technol. 2019, 53, 13906–13918. [Google Scholar] [CrossRef] [PubMed]
- Vinti, G.; Bauza, V.; Clasen, T.; Tudor, T.; Vaccari, M.; Zurbrügg, C. Municipal Solid Waste Management and Adverse Health Outcomes of Nearby Residents: A Systematic Review. PROSPERO 2020 CRD42020176495. Available online: https://www.crd.york.ac.uk/prospero/display_record.php?ID=CRD42020176495 (accessed on 10 December 2020).
- Mavropoulos, A.; Newman, D. Wasted Health. The Tragic Case of Dumpsites; International Solid Waste Association: Vienna, Austria, 2015; Available online: https://www.iswa.org/fileadmin/galleries/Task_Forces/THE_TRAGIC_CASE_OF_DUMPSITES.pdf (accessed on 26 March 2020).
- Chandrappa, R.; Das, D.B. Solid Waste Management. Principles and Practice; Springer: Berlin/Heidelberg, Germany, 2012; ISBN 978-3-642-28680-3. [Google Scholar]
- WHO (World Health Organization). Vector-Borne Diseases. Available online: https://www.who.int/news-room/fact-sheets/detail/vector-borne-diseases (accessed on 16 June 2020).
- Wells, G.A.; Shea, B.; O’Connell, D.; Peterson, J.; Welch, V.; Losos, M.; Tugwell, P. The Newcastle-Ottawa Scale (NOS) for Assessing the Quality of Nonrandomised Studies in Meta-Analyses; University of Ottawa: Ottawa, Canada, 2019; Available online: http://www.ohri.ca/programs/clinical_epidemiology/oxford.asp (accessed on 20 January 2020).
- Mataloni, F.; Badaloni, C.; Golini, M.N.; Bolignano, A.; Bucci, S.; Sozzi, R.; Forastiere, F.; Davoli, M.; Ancona, C. Morbidity and mortality of people who live close to municipal waste landfills: A multisite cohort study. Int. J. Epidemiol. 2016, 45, 806–815. [Google Scholar] [CrossRef]
- Palmer, S.R.; Dunstan, F.D.; Fielder, H.; Fone, D.L.; Higgs, G.; Senior, M.L. Risk of congenital anomalies after the opening of landfill sites. Environ. Health Perspect. 2005, 113, 1362–1365. [Google Scholar] [CrossRef]
- Gumede, P.R.; Savage, M.J. Respiratory health effects associated with indoor particulate matter (PM2.5) in children residing near a landfill site in Durban, South Africa. Air Qual. Atmos. Health 2017, 10, 853–860. [Google Scholar] [CrossRef]
- Heaney, C.D.; Wing, S.; Campbell, R.L.; Caldwell, D.; Hopkins, B.; Richardson, D.; Yeatts, K. Relation between malodor, ambient hydrogen sulfide, and health in a community bordering a landfill. Environ. Res. 2011, 111, 847–852. [Google Scholar] [CrossRef]
- Kret, J.; Dalidowitz Dame, L.; Tutlam, N.; DeClue, R.W.; Schmidt, S.; Donaldson, K.; Lewis, R.; Rigdon, S.E.; Davis, S.; Zelicoff, A.; et al. A respiratory health survey of a subsurface smoldering landfill. Environ. Res. 2018, 166, 427–436. [Google Scholar] [CrossRef]
- Yu, Y.; Yu, Z.; Sun, P.; Lin, B.; Li, L.; Wang, Z.; Ma, R.; Xiang, M.; Li, H.; Guo, S. Effects of ambient air pollution from municipal solid waste landfill on children’s non-specific immunity and respiratory health. Environ. Pollut 2018, 236, 382–390. [Google Scholar] [CrossRef] [PubMed]
- Elliott, P.; Richardson, S.; Abellan, J.J.; Thomson, A.; de Hoogh, C.; Jarup, L.; Briggs, D.J. Geographic density of landfill sites and risk of congenital anomalies in England. Occup. Environ. Med. 2009, 66, 81–89. [Google Scholar] [CrossRef]
- Jarup, L.; Morris, S.; Richardson, S.; Briggs, D.; Cobley, N.; de Hoogh, C.; Gorog, K.; Elliott, P. Down syndrome in births near landfill sites. Prenat. Diagn. 2007, 27, 1191–1196. [Google Scholar] [CrossRef]
- Kloppenborg, S.C.H.; Brandt, U.K.; Gulis, G.; Ejstrud, B. Risk of congenital anomalies in the vicinity of waste landfills in Denmark; An epidemiological study using GIS. Cent. Eur. J. Public Health 2005, 13, 137–143. [Google Scholar] [PubMed]
- Ranzi, A.; Fano, V.; Erspamer, L.; Lauriola, P.; Perucci, C.A.; Forastiere, F. Mortality and morbidity among people living close to incinerators: A cohort study based on dispersion modeling for exposure assessment. Environ. Health 2011, 10, 22. [Google Scholar] [CrossRef] [PubMed]
- Candela, S.; Ranzi, A.; Bonvicini, L.; Baldacchini, F.; Marzaroli, P.; Evangelista, A.; Luberto, F.; Carretta, E.; Angelini, P.; Sterrantino, A.F.; et al. Air pollution from incinerators and reproductive outcomes: A multisite study. Epidemiology 2013, 24, 863–870. [Google Scholar] [CrossRef] [PubMed]
- Cordier, S.; Lehébel, A.; Amar, E.; Anzivino-Viricel, L.; Hours, M.; Monfort, C.; Chevrier, C.; Chiron, M.; Robert-Gnansia, E. Maternal residence near municipal waste incinerators and the risk of urinary tract birth defects. Occup. Environ. Med. 2010, 67, 493–499. [Google Scholar] [CrossRef] [PubMed]
- Xu, P.; Wu, L.; Chen, Y.; Xu, D.; Wang, X.; Shen, H.; Han, J.; Fu, Q.; Chen, Z.; Lou, X. High intake of persistent organic pollutants generated by a municipal waste incinerator by breastfed infants. Environ. Pollut 2019, 250, 662–668. [Google Scholar] [CrossRef] [PubMed]
- Viel, J.F.; Clément, M.C.; Hägi, M.; Grandjean, S.; Challier, B.; Danzon, A. Dioxin emissions from a municipal solid waste incinerator and risk of invasive breast cancer: A population-based case-control study with GIS-derived exposure. Int. J. Health Geogr. 2008, 7, 4. [Google Scholar] [CrossRef] [PubMed]
- Vinceti, M.; Malagoli, C.; Teggi, S.; Fabbi, S.; Goldoni, C.; De Girolamo, G.; Ferrari, P.; Astolfi, G.; Rivieri, F.; Bergomi, M. Adverse pregnancy outcomes in a population exposed to the emissions of a municipal waste incinerator. Sci. Total Environ. 2008, 407, 116–121. [Google Scholar] [CrossRef]
- Vinceti, M.; Malagoli, C.; Fabbi, S.; Teggi, S.; Rodolfi, R.; Garavelli, L.; Astolfi, G.; Rivieri, F. Risk of congenital anomalies around a municipal solid waste incinerator: A GIS-based case-control study. Int. J. Health Geogr. 2009, 8, 8. [Google Scholar] [CrossRef]
- Lin, C.M.; Li, C.Y.; Mao, I.F. Birth outcomes of infants born in areas with elevated ambient exposure to incinerator generated PCDD/Fs. Environ. Int. 2006, 32, 624–629. [Google Scholar] [CrossRef] [PubMed]
- Candela, S.; Bonvicini, L.; Ranzi, A.; Baldacchini, F.; Broccoli, S.; Cordioli, M.; Carretta, E.; Luberto, F.; Angelini, P.; Evangelista, A.; et al. Exposure to emissions from municipal solid waste incinerators and miscarriages: A multisite study of the MONITER Project. Environ. Int. 2015, 78, 51–60. [Google Scholar] [CrossRef]
- Parera, J.; Serra-Prat, M.; Palomera, E.; Mattioli, L.; Abalos, M.; Rivera, J.; Abad, E. Biological monitoring of PCDD/Fs and PCBs in the City of Mataró. A population-based cohort study (1995–2012). Sci. Total Environ. 2013, 461–462, 612–617. [Google Scholar] [CrossRef]
- IARC (International Agency for Research on Cancer). IARC Monographs on the Evaluation of Carcinogenic Risks to Humans, No. 100F. 2,3,7,8-TETRACHLORODIBENZO-para-DIOXIN, 2,3,4,7,8-PENTACHLORODIBENZOFURAN, AND 3,3′,4,4′,5-PENTACHLOROBIPHENYL; IARC Working Group on the Evaluation of Carcinogenic Risks to Humans: Lyon, France, 2012. Available online: https://www.ncbi.nlm.nih.gov/books/NBK304398/ (accessed on 26 March 2020).
- WHO (World Health Organization). Preventing Disease through Healthy Environments: Exposure to Dioxins and Dioxin-Like Substances: A Major Public Health Concern; World Health Organization: Geneva, Switzerland, 2019; Available online: https://apps.who.int/iris/bitstream/handle/10665/329485/WHO-CED-PHE-EPE-19.4.4-eng.pdf?ua=1 (accessed on 26 March 2020).
- US EPA (United States Environmental Protection Agency). Toxics Release Inventory (TRI) Program. Dioxin and Dioxin-Like Compounds Toxic Equivalency Information; United States Environmental Protection Agency: Washington, DC, USA, 2016. Available online: https://www.epa.gov/toxics-release-inventory-tri-program/dioxin-and-dioxin-compounds-toxic-equivalency-information (accessed on 7 April 2020).
- EFSA (European Food Safety Authority); Knutsen, H.K.; Alexander, J.; Barregård, L.; Bignami, M.; Bruschweiler, B.; Ceccatelli, S.; Cottrill, B.; Dinovi, M.; Edler, L.; et al. Risk for animal and human health related to the presence of dioxins and dioxin-like PCBs in food and feed. EFSA J. 2018, 16, 05333. [Google Scholar]
- Gilbreath, S.; Kass, P.H. Adverse birth outcomes associated with open dumpsites in Alaska Native Villages. Am. J. Epidemiol 2006, 164, 518–528. [Google Scholar] [CrossRef] [PubMed]
- Gouveia, N.; do Prado, R.R. Health risks in areas close to urban solid waste landfill sites. Rev. Saude Publica 2010, 44, 859–866. [Google Scholar] [CrossRef] [PubMed]
- Gilbreath, S.; Kass, P.H. Fetal and neonatal deaths and congenital anomalies associated with open dumpsites in Alaska Native villages. Int. J. Circumpolar Health 2006, 65, 133–147. [Google Scholar] [CrossRef] [PubMed]
- Babs-Shomoye, F.; Kabir, R. Health effects of solid waste disposal at a dumpsite on the surrounding human settlements. J. Public Health Dev. Coutries 2016, 2, 268–275. [Google Scholar]
- Sankoh, F.P.; Yan, X.; Tran, Q. Environmental and health impact of solid waste disposal in developing cities: A case study of granville brook dumpsite, freetown, sierra leone. J. Environ. Prot. 2013, 4, 665–670. [Google Scholar] [CrossRef]
- Suleman, Y.; Darko, E.T.; Agyemang-Duah, W. Solid waste disposal and community health implications in Ghana: Evidence from sawaba, asokore mampong municipal assembly. J. Civ. Environ. Eng. 2015, 5, 1000202. [Google Scholar] [CrossRef]
- HMSO. Control of Pollution Act (COPA); The Stationery Office Books: London, UK, 1974; ISBN 0105440744. [Google Scholar]
- HMSO. Waste Management Licensing Regulations 1994 (S.I. No 1056 of 1994). Available online: https://www.legislation.gov.uk/uksi/1994/1056/made (accessed on 5 March 2021).
- EC (European Commission). Council Directive 1999/31/EC of 26 April 1999 on the Landfill of Waste. Available online: https://eur-lex.europa.eu/legal-content/EN/TXT/?uri=celex%3A31999L0031 (accessed on 5 March 2021).
- D Lgs. 36/2003. Supplemento Ordinario N. 40 alla Gazzetta Ufficiale 12 Marzo 2003 N. 59. Implementation of the European Directive 1999/31/CE in Italy. Available online: https://www.minambiente.it/sites/default/files/dlgs_13_01_03_36.pdf (accessed on 26 December 2020).
- Godfrey, L.; Oelofse, S. Historical review of waste management and recycling in South Africa. Resources 2017, 6, 57. [Google Scholar] [CrossRef]
- US EPA (United States Environmental Protection Agency). Municipal Solid Waste Landfills. Available online: https://www.epa.gov/landfills/municipal-solid-waste-landfills#regs (accessed on 11 February 2021).
- Paladino, O.; Massabò, M. Health risk assessment as an approach to manage an old landfill and to propose integrated solid waste treatment: A case study in Italy. Waste Manag. 2017, 68, 344–354. [Google Scholar] [CrossRef] [PubMed]
- EC (European Commission). Directive 2000/76/EC of the European Parliament and of the Council of 4 December 2000 on the Incineration of Waste; European Commission: Brussels, Belgium, 2000. [Google Scholar]
- EC (European Commission). Best Available Techniques (BAT) Reference Document for Waste Treatment. Publications Office of the European Union, 2018. Available online: https://eippcb.jrc.ec.europa.eu/sites/default/files/2019-11/JRC113018_WT_Bref.pdf (accessed on 10 February 2021).
- Autret, E.; Berthier, F.; Luszezanec, A.; Nicolas, F. Incineration of municipal and assimilated wastes in France: Assessment of latest energy and material recovery performances. J. Hazard. Mater. 2007, 139, 569–574. [Google Scholar] [CrossRef]
- Lu, J.W.; Zhang, S.; Hai, J.; Lei, M. Status and perspectives of municipal solid waste incineration in China: A comparison with developed regions. Waste Manag. 2017, 69, 170–186. [Google Scholar] [CrossRef] [PubMed]
- Nixon, J.D.; Dey, P.K.; Ghosh, S.K. Energy recovery from waste in India: An evidence-based analysis. Sustain. Energy Technol. Assess. 2017, 21, 23–32. [Google Scholar] [CrossRef]
- FAO (Food and Agriculture Organization); WHO (World Health Organization). Joint FAO/WHO Food Standards Programme. Codex Committee on Contaminants in Foods. 12th Session, Utrecht, 12–16 March 2018. Proposed Draft Revision of the Code of Practice for the Prevention and Reduction of Dioxins and Dioxin-Like PCBs in Food and Feed. 2018. Available online: http://www.fao.org/fao-who-codexalimentarius/sh-proxy/en/?lnk=1&url=https%253A%252F%252Fworkspace.fao.org%252Fsites%252Fcodex%252FMeetings%252FCX-735-12%252FWD%252Fcf12_08e.pdf (accessed on 26 March 2020).
- Scaramozzino, P.; Battisti, S.; Desiato, R.; Tamba, M.; Fedrizzi, G.; Ubaldi, A.; Neri, B.; Abete, M.C.; Ru, G. Application of a risk-based standardized animal biomonitoring approach to contaminated sites. Environ. Monit. Assess. 2019, 191, 526. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Study Location | Study Design | Study Participants | Study Period | Exposure Source | Outcomes Investigated | Ref. |
|---|---|---|---|---|---|---|
| England (UK) | Cohort study (retrospective) | 10,064,382 live births, 52,532 stillbirths and 12,373 terminations | Births between 1983 and 1998 | 8804 landfills, including 607 which handled special (hazardous) waste | The risk of congenital anomalies in relation to an index of geographic density of landfill sites (within 2 km from landfills) | [41] |
| South Africa | Cross-sectional study | 23 children aged 6–12 years residing within 2 km from the landfill site for at least 5 years | Study conducted between November 2013 and January 2014 | The Bisasar Road MSW landfill | Assessment of PM2.5 concentration in indoor environments of the subjects involved in the study and its association with lung function patterns | [37] |
| North Carolina (USA) | Cross-sectional study | 23 participants among people living within 0.75 miles to a landfill | Between January and November 2009 | A MSW landfill | Relationships between H2S, odour, and health outcomes in a community living close to a landfill | [38] |
| England and Wales (UK) | Cohort study (retrospective) | 4,584,541 births in England and Wales | Births between 1989 and 1998 | 6289 landfill sites processing special (hazardous), non-special and unknown waste | The risk of giving birth to a child with Down syndrome associated with residence near landfill sites (within 2 km) | [42] |
| Denmark | Cohort study (retrospective) | 2477 live births with congenital anomalies in Denmark in three different zones of distance from landfills (0–2 km; 2–4 km; 4–6 km) | Births between 1997 and 2001 | 48 landfills | Risk of congenital anomalies combined and congenital anomalies of the cardiovascular and nervous systems with maternal residence in function of distance from landfills | [43] |
| Missouri (USA) | Cross-sectional study | Health survey through 170 households within a 3.2-km radius from a landfill and 173 households more distant (comparison group) from the landfill | Conducted from February to March 2016 | The Bridgeton Landfill in St. Louis County, in which MSW is disposed of | Respiratory symptoms and diseases were assessed, though household interviews | [39] |
| Italy | Cohort study (retrospective) | 242,409 people living within 5 km from landfills | Residents between 1996 and 2008, followed for mortality and hospitalizations until 2012 | 9 MSW landfills operating in the Lazio region, in which the exposure to landfills was assessed using H2S as a tracer in air (calculated with a model) | The association between landfill H2S exposure and mortality (both natural and cause-specific) and hospital admissions for cardiorespiratory diseases was evaluated | [35] |
| Wales (UK) | Cohort study (retrospective) | 542,682 births in Wales between 1983 and 1997. 97,292 births in Wales between 1998 and 2000 | See previous column | 24 landfill sites for commercial, industrial, and household waste | The increased risk of births with at least one congenital malformation in population living within 2 km from landfill sites, comparing it with population living at least 4 km away | [36] |
| China | Cross-sectional study | 951 children from primary school studying and residing near a landfill. 4 schools within 5 km of the landfill (exposed area). 1 school (non-exposed area) more distant (5.8 km away) | Not specified | A MSW landfill | Association between air pollutants and respiratory health in exposed area, considering lysozyme and secretory immunoglobulin A (which are typically considered as the first line of defence from air pollutants and higher levels show good related health conditions) | [40] |
| Study Location | Study Design | Main Findings (e.g., Estimated Risk, CI, p-Value) | Ref. |
|---|---|---|---|
| Mortality | |||
| Italy | Cohort study (retrospective) | Associations between H2S (>75° quartile) and cause-specific mortality (hazard ratio (HR) and 95% Confidence Interval): - natural cases: 0.98 (0.91, 1.05) - all cancers: 1.03 (0.91, 1.16) - specific cancers:stomach: 0.88 (0.54, 1.42) - colorectal: 0.91 (0.64, 1.28) - liver: 0.76 (0.48, 1.2) - pancreas: 0.73 (0.41, 1.32) - larynx: 0.26 (0.07, 0.95) - lung: 1.34 (1.06, 1.71), p < 0.05 a - bladder: 0.94 (0.5, 1.80) - kidney: 0.86 (0.41, 1.83) - brain: 1.76 (0.81, 3.81) - lymphatic and hematopoietic - tissue: 1.12 (0.74, 1.17) - tissue: 1.12 (0.74, 1.17) - cardiovascular diseases: 0.91 (0.81, 1.02) - ischemic heart diseases 0.78 (0.64, 0.95) - respiratory diseases: 1.30 (0.99, 1.70) - digestive diseases: 0.97 (0.69, 1.35) - urinary system diseases: 1.42 (0.84, 2.40) | [35] |
| Adverse birth and neonatal outcomes | |||
| England (UK) | Cohort study (retrospective) | Rates of congenital anomalies in the category with the highest exposure index (the fourth), for non-special or unknown waste sites (adjusted odds ratio (OR) and 95% Credible Interval): - all congenital anomalies (hypospadias and epispadias, cardiovascular defects, neural tube defects, abdominal wall defects): 1.02 (0.98, 1.07) - hypospadias and epispadias: 0.97 (0.89, 1.06) - neural tube defects: 1.04 (0.93, 1.18) - cardiovascular defects: 0.94 (0.82, 1.07) - abdominal wall defects: 1.11 (0.94, 1.32) | [41] |
| Denmark | Cohort study (retrospective) | Risk rate b, comparing the closest zones with the others. When RR < 1.000 the risk is lower, compared to the closest zone: - combined congenital anomalies: 1.000 (closest zone), 0.991 (middle zone), 1.013 (farthest zone) - congenital anomalies in the cardiovascular system: 1.000 (closest zone), 0.926 (middle zone), 0.854 (farthest zone) | [43] |
| England and Wales (UK) | Cohort study (retrospective) | Relative risk (RR) c (95% Credible Interval) of Down’s syndrome near landfill sites: - considering both operating and closed sites (non-special waste): 1.000 (0.909, 1.095) - considering only operating sites (non-special waste): 1.011 (0.901, 1.126) | [42] |
| Wales (UK) | Cohort study (retrospective) | Ratio between risk of congenital anomalies (in live births) after and before opening of sites (95% Confidence Interval): 1.39 (1.21, 1.72), p < 0.05 a | [36] |
| Cardiovascular diseases | |||
| Italy | Cohort study (retrospective) | Associations between H2S (>75° quartile) and cardiorespiratory morbidity (HR and 95% Confidence Interval): - (all) cardiovascular diseases: 1.02 (0.97, 1.07) - cardiac disease: 1.04 (0.97, 1.11) - ischemic heart diseases: 0.99 (0.88, 1.10) - cerebrovascular diseases: 0.98 (0.88, 1.10) | [35] |
| Respiratory conditions | |||
| Italy | Cohort study (retrospective) | Associations between H2S (>75° quartile) and cardiorespiratory morbidity (HR and 95% Confidence Interval): - (all) respiratory diseases: 1.05 (0.99, 1.11) - acute respiratory infections: 1.07 (0.97, 1.18) - COPD (chronic obstructive pulmonary disease): 1.06 (0.90, 1.25) - asthma: 1.09 (0.90, 1.33) - (all) respiratory diseases (age ≤ 14 years): 1.11 (1.01, 1.22), p < 0.05 a - Acute respiratory infections (age ≤ 14 years): 1.20 (1.04, 1.38), p < 0.05 a - asthma (age ≤ 14 years): 1.13 (0.91, 1.41) | [35] |
| South Africa | Cross-sectional study | Regression models expressing the association between a 24-h average indoor PM2.5 exposure and lung function outcomes, in terms of slope coefficient (95% CI): - PM2.5 concentration level and forced expiratory volume in 1s (FEV1): −0.60 (−1.23, 0.01) - PM2.5 concentration level and forced vital capacity (FVC): −2.12 (−3.39, −0.85), p < 0.05 d - PM2.5 concentration level and FEV1/FVC: −1.42 (−4.85, 2.01) | [37] |
| Missouri (USA) | Cross-sectional study | Differences in the prevalence of diseases, between the two groups, in terms of significance: - p > 0.05 e: ever told asthma; asthma attack in last 12 months; ever told have chronic obstructive pulmonary disease (COPD); nasal allergies in last 12 months; wheezing, cough, eye irritation, fatigue (tiredness), headaches, nausea, trouble sleeping in the last 12 months - PM2.5 concentration level and forced vital capacity (FVC): −2.12 (−3.39, −0.85), p < 0.05 d - p < 0.05 e: other respiratory conditions (the most commonly reported included pneumonia, sleep-related disorders, and bronchitis) - p < 0.01 e: attack of shortness of breath in the last 12 months | [39] |
| China | Cross-sectional study | Students in non-exposure areas had significantly (p < 0.05 f) higher levels of lysozyme, secretory immunoglobulin A (SIgA), and better lung capacity than students in exposed areas | [40] |
| North Carolina (USA) | Cross-sectional study | Symptoms associated to odour (odds ratio (OR) and 95% confidence interval (CI)): - p > 0.05 e: ever told asthma; asthma attack in last 12 months; ever told have chronic obstructive pulmonary disease (COPD); nasal allergies in last 12 months; wheezing, cough, eye irritation, fatigue (tiredness), headaches, nausea, trouble sleeping in the last 12 months - upper respiratory symptoms 3.9 (2.2, 7.0), p < 0.05 a | [38] |
| Gastroenteritis | |||
| North Carolina (USA) | Cross-sectional study | Symptoms associated to odour (odds ratio (OR) and 95% confidence interval (CI)): - gastrointestinal symptoms 1.0 (0.4, 2.6) | [38] |
| Mental and social health conditions | |||
| North Carolina (USA) | Cross-sectional study | Symptoms associated to odour (odds ratio (OR) and 95% confidence interval (CI)): - alteration of daily activities: 9.0 (3.5, 23.5), p < 0.05 a - negative mood states: 5.2 (2.8, 9.6), p < 0.05 a - positive mood states: 0.6 (0.2, 1.5) | [38] |
| Study Location | Study Design | Study Participants | Study Period | Exposure Source | Outcomes Investigated | Ref. |
|---|---|---|---|---|---|---|
| Italy | Cohort study (retrospective) | 21,517 births in women (aged 15–49 years) residing within 4 km from an incinerator | Residents between 2003 and 2010 | 8 MSW incinerators operating in the Emilia Romagna region | Assessment of the effects of air emissions from MSW incinerators (simulated with a dispersion model) on reproductive outcomes a | [45] |
| Italy | Cohort study (retrospective) | 11,875 pregnancies with 1375 miscarriages from women (aged 15–24 years) residing within 4 km from a MSW incinerator | Residents between 2002 and 2006 | 7 MSW incinerators operating in the Emilia Romagna region | Assessment of the effects of air emissions from MSW incinerators (simulated with a dispersion model) on spontaneous abortions | [52] |
| France | Case-control study | Comparison of 304 infants with urinary tract birth defects with a control group of 226 infants randomly selected in the same region | Between 2001 and 2004 | 21 MSW incinerators active in the Rhone-Alps region | Association between the risk of urinary tract birth defects and living near MSW incinerators, using a model to predict the exposure to dioxins | [46] |
| Great Britain (UK) | Cohort study (retrospective) | 1,025,064 births and 18,694 infant deaths in Great Britain. Incinerators emissions within 10 km were considered | Births and deaths between 2003 and 2010 | 22 MSW incinerators (operating between 2003 and 2010) | Associations between modelled ground-level particulate matter from incinerators emission within 10 km and selected reproductive/birth outcomes | [24] |
| Taiwan | Cohort study (retrospective) | 6697 neonates assessed one year before the MSW incinerator started, and 6282 neonates assessed five years later incinerator opening | Neonates in 1991 and in 1997 | The MSW incinerator of Taipei | The relationships between exposure to elevated PCDD/Fs concentration generated by a MSW incinerator (using a model), and various birth outcomes | [51] |
| Spain | Cohort study (perspective) | 104 exposed subjects (living < 1 km from the MSW incinerator) and 97 non-exposed subjects (living > 3 km from the incinerator) were randomly selected. From 1999 one additional group (100 unexposed subjects, in Arenys de Mar, about 11 km from the incinerator) was selected | 7 different campaigns were performed between 1995 and 2012 | The MSW incinerator of Matarò (activated in 1995) | To monitor PCDD/Fs and PCBs levels in blood samples in the different exposed groups | [53] |
| England and Scotland (UK) | Cohort study (retrospective) | 219,486 births, stillbirths, and terminations of pregnancy for foetal anomaly, in which 5154 were cases of congenital anomalies. Incinerators emissions within 10 km were considered | Birth and adverse birth outcomes between 2003 and 2010 | 10 MWIs in England and Scotland (operating between 2003 and 2010) | Associations between modelled ground-level particulate matter from incinerators emission within 10 km and selected reproductive/birth outcomes | [25] |
| Italy | Cohort study (retrospective) | 31,347 residents within a 3.5 km radius of two incinerators | Residents between 1990 and 2003 | An MSW incinerator and a hospital waste incinerator in Forlì | Health outcomes among people living close to incinerators (using a dispersion model for exposure assessment) | [44] |
| France | Case-control study | 434 incident cases of invasive breast cancer diagnosed (case group) compared with 2170 controls randomly selected | Between 1996 and 2002 (cancer diagnosis in the case group).1999 (control group) b | The MSW incinerator in Besançon | The association between dioxins emitted from a MSW incinerator (air exposure using a model) and invasive breast cancer risk among women residing in the area | [48] |
| Italy | Cohort study (retrospective) | Women residing or working near a MSW incinerator of Modena | Residents or workers between 2003 and 2006 | The MSW incinerator of Modena | Rates of spontaneous abortion and prevalence of birth defects among women living or working near a MSW incinerator, modelling incinerator emissions exposure | [49] |
| Italy | Case-control study | Women (aged 16–44 years) residing near a MSW incinerators, assessing 228 cases of congenital anomalies | Birth defects between 1998 and 2006 | The MSW incinerator of Reggio Emilia | The relationship between exposure to the emissions from an MSW incinerator and risk of birth defects, modelling incinerator emissions exposure | [50] |
| China | Cross-sectional study | 82 children living near a MSW incinerator in China and 49 from a control area, both in Zhejiang Province | Samples collected in October 2013 | A MSW incinerator in the Zhejiang Province | To monitor PCDD/F levels in blood in different exposed groups | [9] |
| China | Cross-sectional study | 14 mothers living near a MSW incinerator (exposure area) and 18 mothers from a control area, both in Zhejiang Province | Samples collected in September and October 2013 | A MSW incinerator in the Zhejiang Province | To monitor PCDD/Fs and PCBs in the breast milk of mothers in different exposed groups | [47] |
| Study Location | Study Design | Main Findings (e.g., Estimated Risk, CI, p-Value) | Ref. |
|---|---|---|---|
| Mortality | |||
| Italy | Cohort study (retrospective) |
Associations between heavy metals concentration and mortality in the highest exposed group using the lowest exposure category as the reference (rate ratio (RR) and 95% CI): - all causes (men): 1.01 (0.86, 1.20) - all causes (women): 1.12 (1.00, 1.27) a - >cardiovascular diseases (men): 0.98 (0.75, 1.29) - cardiovascular diseases (women): 1.32 (1.00, 1.72) - ischemic heart diseases (men): 0.79 (0.51, 1.22) - ischemic heart diseases (women): 1.14 (0.72, 1.82) - respiratory diseases (men): 1.01 (0.42, 2.45) - respiratory diseases (women): 0.53 (0.18, 1.56) - chronic pulmonary diseases (men): 0.53 (0.15, 1.86) - chronic pulmonary diseases (women): 0.27 (0.03, 2.06) Associations between heavy metals concentration and cancer mortality in the highest exposed group using the lowest exposure category as the reference (rate ratio (RR) and 95% CI): - all cancer (men): 0.85 (0.64, 1.12) - all cancer (women): 1.47 (1.09, 1.99) a - stomach (men): 0.85 (0.35, 2.03) - stomach (women): 1.86 (0.73, 4.75) - colon rectum (men): 2.05 (0.92, 4.58) - colon rectum (women): 2.15 (0.86, 5.37) - liver (men): 0.27 (0.03, 2.18) - liver (women): 5.10 (0.94, 27.80) - larynx (men): no cases - larynx (women): no cases - lung (men): 0.91 (0.53, 1.57) - lung (women): 0.96 (0.31, 2.97) - soft tissue sarcoma (men): no cases - soft tissue sarcoma (women): no cases - breast (women): 2.00 (1.00, 3.99) - prostate (men): 1.57 (0.66, 3.74) - bladder (men): 1.48 (0.52, 4.22) - bladder (women): 3.06 (0.64, 14.70) - central nervous system (men): no cases - central nervous system (women): no cases - lymph. system (men): 0.42 (0.15, 1.23) - lymph. system (women): 1.78 (0.74, 4.25) - non-Hodgkin lymphoma (men): 0.52 (0.11, 2.45) - non-Hodgkin lymphoma (women): 2.03 (0.48, 8.67) - myeloma (men): no cases - myeloma (women): 4.28 (0.77, 23.80) - leukaemia (men): 0.67 (0.14, 3.16) - leukaemia (women): 1.31 (0.25, 6.95) | [44] |
| Cancer | |||
| Italy | Cohort study (retrospective) | Associations between heavy metals concentration and cancer incidence in the highest exposed group using the lowest exposure category as the reference (Rate Ratio (RR) and 95% CI): - all cancer (men): 0.87 (0.72, 1.06) - all cancer (women): 0.90 (0.73, 1.11) - stomach (men): 1.24 (0.64, 2.40) - stomach (women): 1.09 (0.49, 2.44) - colon rectum (men): 1.00 (0.57, 1.75) - colon rectum (women): 1.33 (0.71, 2.48) - liver (men): 0.26 (0.03, 2.01) - liver (women): 0.94 (0.20, 4.53) - larynx (men): 0.15 (0.02, 1.14) - larynx (women): 1.60 (0.15, 17.64) - lung (men): 0.96 (0.61, 1.52) - lung (women): 0.81 (0.27, 2.42) - soft tissue sarcoma (men): 0.84 (0.09, 8.06) - soft tissue sarcoma (women): no cases - breast (women): 0.76 (0.51, 1.13) - prostate (men): 1.27 (0.82, 1.99) - bladder (men): 0.78 (0.43, 1.42) - bladder (women): 2.30 (0.73, 7.24) - central nervous system (men): 1.35 (0.34, 5.39) - central nervous system (women): no cases - lymph. system (men): 0.70 (0.38, 1.28) - lymph. system (women): 1.23 (0.65, 2.33) - non-Hodgkin lymphoma (men): 0.59 (0.23, 1.57) - non-Hodgkin lymphoma (women): 1.06 (0.39, 2.93) - myeloma (men): 0.61 (0.17, 2.13) - myeloma (women): 0.95 (0.26, 3.45) - leukaemia (men): 1.01 (0.36, 2.84) - leukaemia (women): 1.23 (0.33, 4.62) | [44] |
| France | Case-control study | Odds ratio (OR) of invasive breast cancer by age bands and dioxin exposure categories (comparing very low with high exposure) (95% CI): - women aged 20–59 years: 0.88 (0.43, 1.79) - women aged 60 years and over: 0.31 (0.08, 0.89) | [48] |
| Adverse birth and neonatal outcomes | |||
| Italy | Cohort study (retrospective) | Associations between modelled exposure levels to PM10 from the incinerators and reproductive outcomes, for the highest versus the lowest quintile exposure (odds ratio (OR), 95% confidence interval and significance): - preterm births: 1.30 (1.08, 1.57) b, p < 0.05 c; 1.44 (1.11, 1.85) d, p < 0.05 c - sex ratio: 0.91 (0.83, 0.99) b; 0.88 (0.78, 0.99) - multiple births: 0.87 (0.57, 1.33) b; 1.12 (0.60, 2.08) d - small for gestational age (SGA): 1.11 (0.96, 1.28) b; 1.06 (0.87, 1.29) d | [45] |
| Italy | Cohort study (retrospective) | Associations between modelled exposure levels to PM10 from the incinerators and miscarriages, for the highest versus the lowest quintile exposure (adjusted odds ratio (OR), 95% confidence interval and significance p): - spontaneous abortions: 1.29 (0.97, 1.72) e | [52] |
| Italy | Cohort study (retrospective) | Associations between modelled exposure levels of pollutants from the incinerator and reproductive outcomes, in terms of Relative Risk computed as the ratio between observed and expected incidence, (95% confidence interval): - Spontaneous abortion: - residents from both areas A and B 1.00 (0.65, 1.48) - area A residents (highest exposure): 0.87 (0.22, 2.38) - area B residents (intermediate exposure): 1.03 (0.64, 1.56) - workers from both areas A and B: 1.04 (0.38, 2.30) - area A workers: 0.00 (0.00, 1.46) - area B workers: 1.81 (0.66, 4.02) - Spontaneous abortion: - residents from both areas A and B: 0.64 (0.20, 1.55) - area A residents: 0.00 (0.00, 4.41) - area B residents: 0.72 (0.23, 1.75) - workers from both areas A and B: 2.26 (0.57, 6.14) - area A workers: 2.22 (0.37, 7.34) - area B workers: 2.27 (0.11, 11.21) | [49] |
| Great Britain (UK) | Cohort study (retrospective) | Associations between modelled exposure levels of pollutants from the incinerator and reproductive outcomes (adjusted OR and 95% CI): - stillbirths f: 0.99 (0.97, 1.00) - stillbirths g: 1.00 (0.99, 1.02) - neonatal mortality (pregnancy exposure) f: 0.99 (0.96, 1.02) - neonatal mortality (pregnancy exposure) g: 1.01 (1.00, 1.03) - post-neonatal mortality (pregnancy exposure) f: 1.02 (0.96, 1.07) - post-neonatal mortality (pregnancy exposure) g: 0.99 (0.97, 1.02) - post-neonatal mortality (birth to death of case exposure) f: 1.01 (0.98, 1.04) - multiple births f: 0.99 (0.99, 1.00) - multiple births g: 1.00 (0.99, 1.00) - sex ratio f: 1.00 (1.00, 1.00) - sex ratio g: 1.00 (1.00, 1.00) - preterm delivery f: 0.99 (0.97, 1.01) - preterm delivery g: 1.00 (0.99, 1.00) - terms small for gestational age (SGA) f: 0.99 (0.98, 1.00) - terms SGA g: 1.00 (0.99, 1.01) | [24] |
| England and Scotland (UK) | Cohort study (retrospective) |
Adjusted odds ratio (OR) (95% CI): - all congenital anomalies f: 1.00 (0.98, 1.02) - all congenital anomalies g: 1.02 (1.00, 1.04) - all congenital anomalies excluding chromosomal f: 0.99 (0.97, 1.01) - all congenital anomalies excluding chromosomal g: 1.02 (1.00, 1.04) - nervous system f: 0.97 (0.92, 1.02) - nervous system g: 0.97 (0.93, 1.02) - congenital heart defects f: 0.99 (0.93, 1.05) - congenital heart defects g: 1.04 (1.01, 1.08), p < 0.05 h - abdominal wall defects f: 1.00 (0.92, 1.08) - abdominal wall defects g: 1.00 (0.94, 1.07) - oro-facial clefts f: 1.00 (0.94, 1.07) - oro-facial clefts g: 0.99 (0.94, 1.05) - limb defects f: 1.01 (0.94, 1.08) - limb defects g: 1.02 (0.97, 1.08) - digestive system f: 1.00 (0.92, 1.09) - digestive system g: 1.00 (0.95, 1.06) - urinary system f: 1.00 (0.94, 1.07) - urinary system g: 1.02 (0.97, 1.06) - genital system f: 1.03 (0.95, 1.13) - genital system g: 1.07 (1.02, 1.12), p < 0.05 h - neural tube defects (from congenital anomaly sub-groups (CAS)) f: 1.00 (0.92, 1.07) - neural tube defects (from CAS) g: 0.97 (0.91, 1.03) - severe congenital heart defects (from CAS) f: 1.03 (0.97, 1.10) - severe congenital heart defects (from CAS) g: 1.02 (0.97, 1.07) - gastroschisis (from CAS) f: 1.04 (0.94, 1.15) - gastroschisis (from CAS) g: 0.97 (0.89, 1.05) - cleft palate (from CAS) f: 1.02 (0.92, 1.13) - cleft palate (from CAS) g: 0.98 (0.90, 1.06) - cleft lip with or without cleft palate (from CAS) f: 1.00 (0.93, 1.08) - cleft lip with or without cleft palate (from CAS) g: 1.00 (0.94, 1.07) - limb reduction defects (from CAS) f: 1.02 (0.91, 1.14) - limb reduction defects (from CAS) g: 0.98 (0.90, 1.08) - oesophageal atresia (from CAS) f: 1.04 (0.88, 1.22) - oesophageal atresia (from CAS) g: 0.92 (0.80, 1.05) - anomalies of the renal system (from CAS) f: 1.02 (0.95, 1.10) - anomalies of the renal system (from CAS) g: 1.00 (0.93, 1.07) - obstructive defects of renal pelvis (from CAS) f: 0.97 (0.90, 1.04) - obstructive defects of renal pelvis (from CAS) g: 1.03 (0.97, 1.10) - hypospadias (from CAS) f: 1.00 (0.90, 1.12) - hypospadias (from CAS) g: 1.07 (1.01, 1.12), p < 0.05h | [25] |
| Taiwan | Cohort study (retrospective) | Difference of birth outcomes between higher exposure and control areas in 1997 (adjusted OR and 95% CI): - birth weight: 1.06 (0.71, 1.57) - gestation weeks, in 1997: 1.22 (0.97, 1.52) - gender, in 1997: 0.90 (0.78, 1.05) | [51] |
| Italy | Case-control study | Prevalence (odds ratio) for congenital anomalies according to maternal exposure to air emissions from the incinerator (95% confidence interval), with low exposure area as reference: All congenital anomalies: - area B (medium exposure) i: 1.55 (0.67, 3.56) - area B j: 1.10 (0.39, 3.06) - area B k: 3.17 (0.65, 15.46) - area C (high exposure) i: 0.67 (0.25, 1.77) - area C j: 0.41 (0.11, 1.61) - area C k: 1.30 (0.29, 5.82) Cardiovascular anomalies: - area B i: 0.94 (0.27, 3.31) - area C i: 0.58 (0.14, 2.45) - area B j: 0.59 (0.14, 2.49) | [50] |
| France | Case-control study | Risk of urinary tract birth defects, in terms of OR (with 95% CI), for not exposed group versus exposed above the median: - considering atmospheric dioxins: 2.84 (1.32, 6.09) h - considering dioxin deposits: 2.95 (1.47, 5.92) h - considering metals: 0.73 (0.45, 1.19) - considering consumption of local food and dioxin deposits: 1.88 (0.55, 6.35) | [46] |
| Cardiovascular diseases | |||
| Italy | Cohort study (retrospective) | Associations between heavy metals concentration and hospitalization for specific causes in the highest exposed group using the lowest exposure category as the reference (rate ratio (RR) and 95% CI): - acute myocardic infarction (men): 0.81 (0.51, 1.28) - acute myocardic infarction (women): 1.40 (0.66, 2.98) - chronic heart failure (men): 0.78 (0.46, 1.33) - chronic heart failure (women): 1.48 (0.90, 2.46) | [44] |
| Respiratory conditions | |||
| Italy | Cohort study (retrospective) | Associations between heavy metals concentration and hospitalization for specific causes in the highest exposed group using the lowest exposure category as the reference (rate ratio (RR) and 95% CI): - chronic obstructive pulmonary disease (men): 1.43 (0.89, 2.31) - chronic obstructive pulmonary disease (women): 0.63 (0.35, 1.14) - acute respiratory diseases (men): 0.89 (0.63, 1.27) - acute respiratory diseases (women): 1.29 (0.94, 1.78) - asthma (men): 1.16 (0.36, 3.71) - asthma (women): 1.01 (0.40, 2.55) | [44] |
| Human biomonitoringl, m, n | |||
| China | Cross-sectional study |
Blood PCDD/F levels comparing exposed group with control group: - TEQΣPCDD/Fs: 0.40 vs. 0.28 pg TEQ/g wet weight, p < 0.05 o | [9] |
| China | Cross-sectional study |
PCDD/Fs and PCBs levels in breast milk comparing exposed and control groups: - TEQ (PCDD/Fs + DL-PCBs): 0.28 vs. 0.16 pg TEQ/g wet weight, p < 0.05 p Mean EDI level in infants comparing exposed and control groups: 22.0 vs. 13.0 pg TEQ/kg bw day, p < 0.05 p | [47] |
| Spain | Cohort study (perspective) | Concentrations of PCDD/Fs, expressed as pg TEQ/g fat in whole blood samples in exposed/non-exposed (Matarò)/non-exposed (Arenys de Mar): - 1995: 13.0/13.1/Not Measured (NM) - 1997: 15.9/16.4/NM - 1999: 17.8/18.1/18.7 - 2002: 15.1/18.2/16.02 - 2005: 11.7/12.3/17.9 - 2008: 14.6/12.6/14.5 - 2012: 12.9/13.3/12.5 | [53] |
| Study Location | Study Design | Study Participants | Study Period | Exposure Source | Outcomes Investigated | Ref. |
|---|---|---|---|---|---|---|
| Swaziland | Cross-sectional study | 78 residents in an area very close to a dumpsite and 39 people closer (<200 m) and 39 further away (>200 m) from the dumpsite | The authors did not specify the period of the questionnaires | A dumpsite in Manzini city | To determine the health effects of a dumpsite on the surrounding human settlement through self-administered questionnaires | [20] |
| Nigeria | Cross-sectional study | 100 household residents within 250 m radius of a dumpsite and 100 household residents between 250–500 metres from the same dumpsite | Data collected from 23 October 2015 to 5 November 2015 | A dumpsite in Lagos | To determine the health effects of a dumpsite on the surrounding human population through self-administered questionnaires | [61] |
| Brazil | Cohort study (retrospective) | People living within 2 km from the 15 landfills in the municipality of São Paulo | Between 1998 and 2002. | The 15 solid waste landfill sites within the municipality of São Paulo (all, except one, were controlled dumpsite with no waterproof layer at the bottom) | To evaluate the association between living close to a controlled dumpsite and occurrences of deaths for cancer or congenital malformations | [59] |
| Alaska | Cohort study (retrospective) | 10,073 infants born in 197 villages close to dumpsites (ranked in high, intermediate, and low hazard) | Infants born between 1997 and 2001 | 197 dumpsites | To evaluate adverse birth outcomes (low and very low birth weight, preterm birth, and intrauterine growth restriction (IUGR)) in infants born close to dumpsites | [58] |
| Alaska | Cohort study (retrospective) | 10,360 infants born in 197 villages close to dumpsites (ranked in higher and lower hazard) | Infants born between 1997 and 2001 | 197 dumpsites | To evaluate the rates of adverse pregnancy outcomes as foetal death, neonatal death, congenital anomalies, close to dumpsites | [60] |
| Sierra Leone | Cross-sectional study | 398 residents nearby (<50 m) and 233 residents further away (>50 m) a dumpsite | The authors did not specify the period of the questionnaires | A dumpsites in Freetown | To determine the health effects of a dumpsite on the surrounding human population through self-administered questionnaires | [62] |
| Ghana | Cross-sectional study | 150 residents in a community nearby dumpsites, comparing three distances between people and disposal sites: (a) less than 5 min, (b) 5–10 min, (c) 11–15 min a | The authors did not specify the period of the questionnaires | A dumpsite in the Ashanti Region | To determine the health effects of dumpsites on the surrounding human population through self-administered questionnaires | [63] |
| Study Location | Study Design | Main Findings | Ref. |
|---|---|---|---|
| Mortality | |||
| Brazil | Cohort study (retrospective) |
Standardized mortality ratios (SMRs) for areas of 2 km around the solid waste landfill sites (95% CI): - bladder cancer: 0.98 (0.79, 1.21) - liver cancer: 1.00 (0.86, 1.16) - leukaemia in adults: 0.92 (0.77, 1.10) - leukaemia in children: 0.84 (0.54, 1.31) Standardized mortality ratios (SMRs) for areas of 2 km around the solid waste landfill sites (95% CI): - congenital malformation: 0.86 (0.72, 1.03) | [59] |
| Adverse birth and neonatal outcomes | |||
| Alaska | Cohort study (retrospective) |
Adjusted odds ratios (95% CI) describing the relations between low and high hazard exposure categories and incidence of low and very low birth weight, preterm birth, and intrauterine growth retardation: - low birth weight: 2.06 (1.28, 3.32), p < 0.05 a - low birth weight adjusted for gestation: 2.20 (1.26, 3.85), p < 0.05 a - very low birth weight: 1.17 (0.37, 3.67) - preterm birth: 1.24 (0.89, 1.74) - intrauterine growth retardation: 3.98 (1.93, 8.21), p < 0.05 a | [58] |
| Alaska | Cohort study (retrospective) |
Adjusted rate ratios (95% CI) describing the relationships between lower and higher hazard exposure categories and incidence of foetal and neonatal death and congenital anomalies: - all deaths: 0.65 (0.34, 1.27) - foetal deaths: 0.75 (0.28, 1.99) - neonatal deaths: 0.55 (0.22, 1.38) - all congenital anomalies (CA), (listed separately in the categories below): 1.37 (0.92, 2.04) - central nervous system CA: 2.36 (0.37, 14.71) - circulatory/respiratory CA: 1.42 (0.39, 5.42) - gastrointestinal CA: 0.58 (0.14, 2.40) - urogenital CA: 2.71 (0.67, 10.95) - musculoskeletal/integumental CA: 1.61 (0.79, 3.29) - others CA: 1.38 (0.77, 2.39) - multiple CA: 1.33 (0.34, 5.20) | [60] |
| Gastroenteritis | |||
| Swaziland | Cross-sectional study |
Diseases which affected residents: - diarrhoea: 16% of closer residents vs. 5% of further away residents Reasons for hospitalization among the interviewed: - diarrhoea: 16% of closer residents vs. 26% of further away residents - cholera: 12% of closer residents vs. 0% of further away residents | [20] |
| Nigeria | Cross-sectional study |
Diseases which affected residents b: - cholera and diarrhoea: 10 closer households vs. 5 further away households reported 1–2 cases; 0 closer households vs. 0 further away households reported 3–4 cases; 0 closer households vs. 0 further away households reported at least 5 cases | [61] |
| Sierra Leone | Cross-sectional study |
Diseases which affected residents c: - diarrhoea: about 10% of closer residents vs. about 12% of further away residents - cholera: about 11% of closer residents vs. about 15% of further away residents | [62] |
| Ghana | Cross-sectional study |
Diseases which affected residents d: - cholera: (a) 67%; (b) 33%; (c) 0% (out of a total of 6 people affected) - typhoid fever: (a) 75%; (b) 25%; (c) 0% (out of a total of 12 people affected) | [63] |
| Vector-borne diseases | |||
| Swaziland | Cross-sectional study |
Diseases which affected residents: - malaria: 36% of closer residents vs. 13% of further away residents Reasons for hospitalization among the interviewed: - malaria: 44% of closer residents vs. 18% of further away residents | [20] |
| Nigeria | Cross-sectional study |
Diseases which affected residents b: - malaria: 20 closer households vs. 24 further away households reported 1–2 cases; 4 closer households vs. 8 further away households reported 3–4 cases; 0 closer households vs. 1 further away households reported at least 5 cases | [61] |
| Sierra Leone | Cross-sectional study |
Diseases which affected residents c: - malaria: 40% of closer residents vs. 35% of further away residents | [62] |
| Ghana | Cross-sectional study |
Diseases which affected residents d: - malaria: (a) 73%; (b) 25%; (c) 2% (out of a total of 103 people affected) | [63] |
| Heading | Mortality | Cancer | Adverse Birth and Neonatal Outcomes | Cardiovascular Diseases | Respiratory Conditions | Gastroenteritis | Vector-Borne Diseases | Mental Health Conditions | Human Biomonitoring a |
|---|---|---|---|---|---|---|---|---|---|
| Landfills b | + (1) | 0 | + (4) | − (1) | + (5) | − (1) | 0 | + (1) | 0 |
| Incinerators b | + (1) | − (2) | + (8) | − (1) | − (1) | 0 | 0 | 0 | + (3) |
| Dumpsites and Open Burning b | − (1) | 0 | + (2) | 0 | 0 | − (4) | − (4) | 0 | 0 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Vinti, G.; Bauza, V.; Clasen, T.; Medlicott, K.; Tudor, T.; Zurbrügg, C.; Vaccari, M. Municipal Solid Waste Management and Adverse Health Outcomes: A Systematic Review. Int. J. Environ. Res. Public Health 2021, 18, 4331. https://doi.org/10.3390/ijerph18084331
Vinti G, Bauza V, Clasen T, Medlicott K, Tudor T, Zurbrügg C, Vaccari M. Municipal Solid Waste Management and Adverse Health Outcomes: A Systematic Review. International Journal of Environmental Research and Public Health. 2021; 18(8):4331. https://doi.org/10.3390/ijerph18084331
Chicago/Turabian StyleVinti, Giovanni, Valerie Bauza, Thomas Clasen, Kate Medlicott, Terry Tudor, Christian Zurbrügg, and Mentore Vaccari. 2021. "Municipal Solid Waste Management and Adverse Health Outcomes: A Systematic Review" International Journal of Environmental Research and Public Health 18, no. 8: 4331. https://doi.org/10.3390/ijerph18084331
APA StyleVinti, G., Bauza, V., Clasen, T., Medlicott, K., Tudor, T., Zurbrügg, C., & Vaccari, M. (2021). Municipal Solid Waste Management and Adverse Health Outcomes: A Systematic Review. International Journal of Environmental Research and Public Health, 18(8), 4331. https://doi.org/10.3390/ijerph18084331