
A Placebo-Controlled, Pseudo-Randomized, Crossover Trial of Botanical Agents for Gulf War Illness: Reishi Mushroom (Ganoderma lucidum), Stinging Nettle (Urtica dioica), and Epimedium (Epimedium sagittatum)


Abstract
1. Introduction
2. Materials and Methods
2.1. Participants
2.2. Botanicals
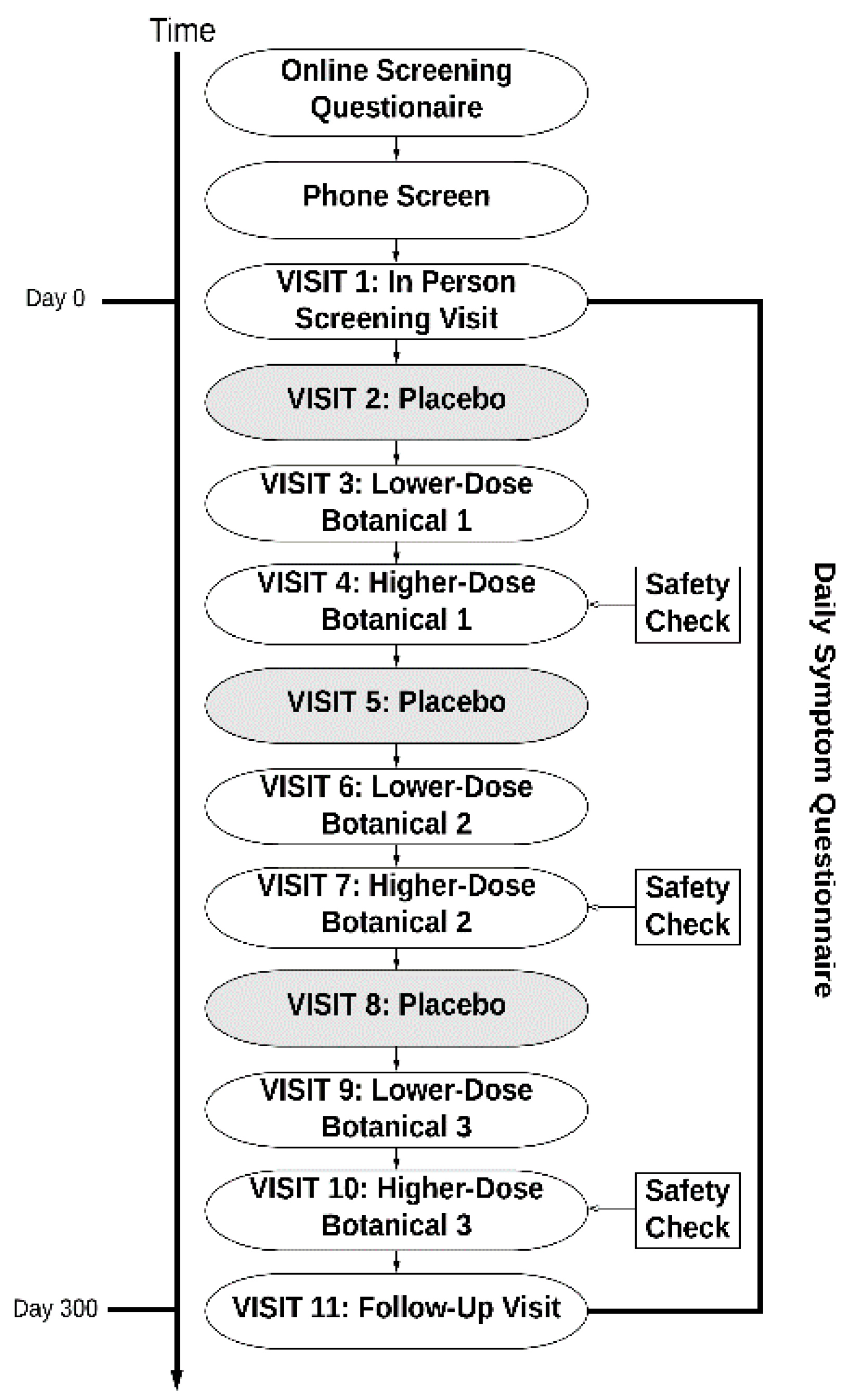
2.3. Study Protocol
2.4. Outcome Measures
2.5. Secondary Outcome Measures
2.6. Statistical Analyses
3. Results
3.1. Participant Attrition
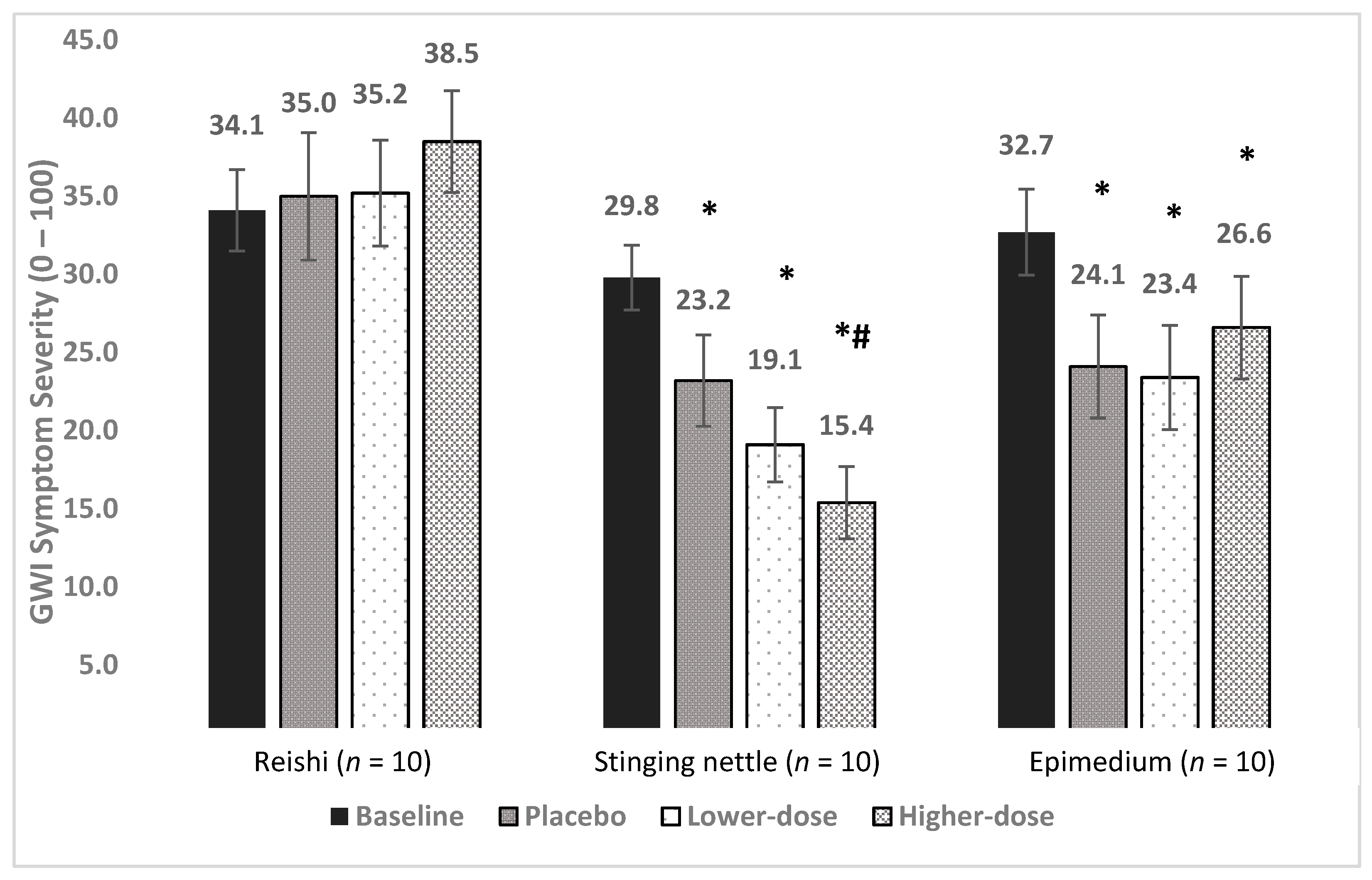
3.2. Reishi
3.3. Stinging Nettle
3.4. Epimedium
3.5. Secondary Outcomes
3.6. Adverse Events
4. Discussion
Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Mawson, A.R.; Croft, A.M. Gulf War Illness: Unifying Hypothesis for a Continuing Health Problem. Int. J. Environ. Res. Public Health 2019, 16, 111. [Google Scholar] [CrossRef]
- Alhasson, F.; Das, S.; Seth, R.; Dattaroy, D.; Chandrashekaran, V.; Ryan, C.N.; Chan, L.S.; Testerman, T.; Burch, J.; Hofseth, L.J.; et al. Altered gut microbiome in a mouse model of Gulf War Illness causes neuroinflammation and intestinal injury via leaky gut and TLR4 activation. PLoS ONE 2017, 12, e0172914. [Google Scholar] [CrossRef]
- Janulewicz, P.A.; Seth, R.K.; Carlson, J.M.; Ajama, J.; Quinn, E.; Heeren, T.; Klimas, N.; Lasley, S.M.; Horner, R.D.; Sullivan, K.; et al. The Gut-Microbiome in Gulf War Veterans: A Preliminary Report. Int. J. Environ. Res. Public Health. 2019, 16, 3751. [Google Scholar] [CrossRef]
- Alshelh, Z.; Albrecht, D.S.; Bergan, C.; Akeju, O.; Clauw, D.J.; Conboy, L.; Edwards, R.R.; Kim, M.; Lee, Y.C.; Protsenko, E.; et al. In-vivo imaging of neuroinflammation in veterans with Gulf War illness. Brain. Behav. Immun. 2020, 87, 498–507. [Google Scholar] [CrossRef] [PubMed]
- Parihar, V.K.; Hattiangady, B.; Shuai, B.; Shetty, A.K. Mood and memory deficits in a model of Gulf War illness are linked with reduced neurogenesis, partial neuron loss, and mild inflammation in the hippocampus. Neuropsychopharmacology 2013, 38, 2348–2362. [Google Scholar] [CrossRef] [PubMed]
- Johnson, G.J.; Slater, B.C.; Leis, L.A.; Rector, T.S.; Bach, R.R. Blood Biomarkers of Chronic Inflammation in Gulf War Illness. PLoS ONE 2016, 11, e0157855. [Google Scholar] [CrossRef] [PubMed]
- Bose, D.; Mondal, A.; Saha, P.; Kimono, D.; Sarkar, S.; Seth, R.K.; Janulewicz, P.; Sullivan, K.; Horner, R.; Klimas, N.; et al. TLR Antagonism by Sparstolonin B Alters Microbial Signature and Modulates Gastrointestinal and Neuronal Inflammation in Gulf War Illness Preclinical Model. Brain Sci. 2020, 10, 532. [Google Scholar] [CrossRef] [PubMed]
- Wu, Y.L.; Han, F.; Luan, S.S.; Ai, R.; Zhang, P.; Li, H.; Chen, L.X. Triterpenoids from Ganoderma lucidum and Their Potential Anti-inflammatory Effects. J. Agric Food Chem. 2019, 67, 5147–5158. [Google Scholar] [CrossRef] [PubMed]
- Dudhgaonkar, S.; Thyagarajan, A.; Sliva, D. Suppression of the inflammatory response by triterpenes isolated from the mushroom Ganoderma lucidum. Int. Immunopharmacol. 2009, 9, 1272–1280. [Google Scholar] [CrossRef] [PubMed]
- Liang, C.J.; Lee, C.W.; Sung, H.C.; Chen, Y.H.; Chiang, Y.C.; Hsu, H.Y.; Tseng, Y.; Li, C.; Wang, S.; Chen, Y. Ganoderma lucidum Polysaccharides Reduce Lipopolysaccharide-Induced Interleukin-1 beta Expression in Cultured Smooth Muscle Cells and in Thoracic Aortas in Mice. Evid Based Complement. Alternat Med. 2014, 2014, 305149. [Google Scholar] [CrossRef]
- Joseph, S.; Sabulal, B.; George, V.; Antony, K.R.; Janardhanan, K.K. Antitumor and anti-inflammatory activities of polysaccharides isolated from Ganoderma lucidum. Acta Pharm. 2011, 61, 335–342. [Google Scholar] [CrossRef]
- Feng, X.; Wang, Y. Anti-inflammatory, anti-nociceptive and sedative-hypnotic activities of lucidone D extracted from Ganoderma lucidum. Cell. Mol. Biol. 2019, 65, 37–42. [Google Scholar] [CrossRef]
- Cai, Q.; Li, Y.; Pei, G. Polysaccharides from Ganoderma lucidum attenuate microglia-mediated neuroinflammation and modulate microglial phagocytosis and behavioural response. J. Neuroinflammation 2017, 14, 63. [Google Scholar] [CrossRef] [PubMed]
- Sun, L.X.; Lin, Z.B.; Lu, J.; Li, W.D.; Niu, Y.D.; Sun, Y.; Hu, C.; Zhang, G.; Duan, X. The improvement of M1 polarization in macrophages by glycopeptide derived from Ganoderma lucidum. Immunol. Res. 2017, 65, 658–665. [Google Scholar] [CrossRef] [PubMed]
- Cai, Z.; Wong, C.K.; Dong, J.; Jiao, D.; Chu, M.; Leung, P.C.; Lau, C.B.S.; Lau, C.P.; Tam, L.S.; Lam, C.W.K. Anti-inflammatory activities of Ganoderma lucidum (Lingzhi) and San-Miao-San supplements in MRL/lpr mice for the treatment of systemic lupus erythematosus. Chin. Med. 2016, 11, 23. [Google Scholar] [CrossRef] [PubMed]
- Batbayar, S.; Kim, M.J.; Kim, H.W. Medicinal mushroom Lingzhi or Reishi, Ganoderma lucidum (W.Curt.:Fr.) P. Karst., beta-glucan induces Toll-like receptors and fails to induce inflammatory cytokines in NF-kappaB inhibitor-treated macrophages. Int. J. Med. Mushrooms 2011, 13, 213–225. [Google Scholar] [CrossRef] [PubMed]
- Habijanic, J.; Berovic, M.; Boh, B.; Plankl, M.; Wraber, B. Submerged cultivation of Ganoderma lucidum and the effects of its polysaccharides on the production of human cytokines TNF-alpha, IL-12, IFN-gamma, IL-2, IL-4, IL-10 and IL-17. N Biotechnol. 2015, 32, 85–95. [Google Scholar] [CrossRef] [PubMed]
- Li, E.K.; Tam, L.S.; Wong, C.K.; Li, W.C.; Lam, C.W.; Wachtel-Galor, S.; Benzie, I.F.F.; Bao, Y.X.; Leung, P.C.; Tomlinson, B. Safety and efficacy of Ganoderma lucidum (lingzhi) and San Miao San supplementation in patients with rheumatoid arthritis: A double-blind, randomized, placebo-controlled pilot trial. Arthritis Rheum. 2007, 57, 1143–1150. [Google Scholar] [CrossRef]
- Riehemann, K.; Behnke, B.; Schulze-Osthoff, K. Plant extracts from stinging nettle (Urtica dioica), an antirheumatic remedy, inhibit the proinflammatory transcription factor NF-kappaB. FEBS Lett. 1999, 442, 89–94. [Google Scholar] [CrossRef]
- Konrad, A.; Mahler, M.; Arni, S.; Flogerzi, B.; Klingelhofer, S.; Seibold, F. Ameliorative effect of IDS 30, a stinging nettle leaf extract, on chronic colitis. Int. J. Colorectal Dis. 2005, 20, 9–17. [Google Scholar] [CrossRef]
- Franciskovic, M.; Gonzalez-Perez, R.; Orcic, D.; de Medina, F.S.; Martinez-Augustin, O.; Svircev, E.; Simin, N.; Mimica-Dukić, N. Chemical Composition and Immuno-Modulatory Effects of Urtica dioica L. (Stinging Nettle) Extracts. Phytother. Res. 2017, 31, 1183–1191. [Google Scholar] [CrossRef] [PubMed]
- Obertreis, B.; Ruttkowski, T.; Teucher, T.; Behnke, B.; Schmitz, H. Ex-vivo in-vitro inhibition of lipopolysaccharide stimulated tumor necrosis factor-alpha and interleukin-1 beta secretion in human whole blood by extractum urticae dioicae foliorum. Arzneimittelforschung 1996, 46, 389–394. [Google Scholar]
- Namazi, N.; Esfanjani, A.T.; Heshmati, J.; Bahrami, A. The effect of hydro alcoholic Nettle (Urtica dioica) extracts on insulin sensitivity and some inflammatory indicators in patients with type 2 diabetes: A randomized double-blind control trial. Pak. J. Biol. Sci. 2011, 14, 775–779. [Google Scholar] [CrossRef] [PubMed]
- Teucher, T.; Obertreis, B.; Ruttkowski, T.; Schmitz, H. Cytokine secretion in whole blood of healthy subjects following oral administration of Urtica dioica L. plant extract. Arzneimittelforschung 1996, 46, 906–910. [Google Scholar] [PubMed]
- Johnson, T.A.; Sohn, J.; Inman, W.D.; Bjeldanes, L.F.; Rayburn, K. Lipophilic stinging nettle extracts possess potent anti-inflammatory activity, are not cytotoxic and may be superior to traditional tinctures for treating inflammatory disorders. Phytomedicine 2013, 20, 143–147. [Google Scholar] [CrossRef]
- Xu, C.Q.; Liu, B.J.; Wu, J.F.; Xu, Y.C.; Duan, X.H.; Cao, Y.X.; Dong, J.C. Icariin attenuates LPS-induced acute inflammatory responses: Involvement of PI3K/Akt and NF-kappaB signaling pathway. Eur. J. Pharmacol. 2010, 642, 146–153. [Google Scholar] [CrossRef] [PubMed]
- El-Shitany, N.A.; Eid, B.G. Icariin modulates carrageenan-induced acute inflammation through HO-1/Nrf2 and NF-kB signaling pathways. Biomed. Pharm. 2019, 120, 109567. [Google Scholar] [CrossRef]
- Jin, J.; Wang, H.; Hua, X.; Chen, D.; Huang, C.; Chen, Z. An outline for the pharmacological effect of icariin in the nervous system. Eur. J. Pharmacol. 2019, 842, 20–32. [Google Scholar] [CrossRef]
- Wang, G.Q.; Li, D.D.; Huang, C.; Lu, D.S.; Zhang, C.; Zhou, S.Y.; Liu, J.; Zhang, F. Icariin Reduces Dopaminergic Neuronal Loss and Microglia-Mediated Inflammation in Vivo and in Vitro. Front. Mol. Neurosci. 2017, 10, 441. [Google Scholar] [CrossRef]
- Wang, Y.; Zhu, T.; Wang, M.; Zhang, F.; Zhang, G.; Zhao, J.; Zhang, Y.; Wu, E.; Li, X. Icariin Attenuates M1 Activation of Microglia and Abeta Plaque Accumulation in the Hippocampus and Prefrontal Cortex by Up-Regulating PPARgamma in Restraint/Isolation-Stressed APP/PS1 Mice. Front. Neurosci. 2019, 13, 291. [Google Scholar] [CrossRef]
- Zeng, K.W.; Fu, H.; Liu, G.X.; Wang, X.M. Icariin attenuates lipopolysaccharide-induced microglial activation and resultant death of neurons by inhibiting TAK1/IKK/NF-kappaB and JNK/p38 MAPK pathways. Int. Immunopharmacol. 2010, 10, 668–678. [Google Scholar] [CrossRef] [PubMed]
- Mo, Z.T.; Liao, Y.L.; Zheng, J.; Li, W.N. Icariin protects neurons from endoplasmic reticulum stress-induced apoptosis after OGD/R injury via suppressing IRE1alpha-XBP1 signaling pathway. Life Sci. 2020, 255, 117847. [Google Scholar] [CrossRef] [PubMed]
- Liu, L.; Zhao, Z.; Lu, L.; Liu, J.; Sun, J.; Dong, J. Icariin and icaritin ameliorated hippocampus neuroinflammation via mediating HMGB1 expression in social defeat model in mice. Int. Immunopharmacol. 2019, 75, 105799. [Google Scholar] [CrossRef] [PubMed]
- Steele, L. Prevalence and patterns of Gulf War illness in Kansas veterans: Association of symptoms with characteristics of person, place, and time of military service. Am. J. Epidemiol. 2000, 152, 992–1002. [Google Scholar] [CrossRef]
- Zigmond, A.S.; Snaith, R.P. The hospital anxiety and depression scale. Acta Psychiatr. Scand. 1983, 67, 361–370. [Google Scholar] [CrossRef]
- Weathers, F.W.; Huska, J.A.; Keane, T.M. PCL-M for DSM-IV.; National Center for PTSD-Behavioral Science Division: Boston, MA, USA, 1991. [Google Scholar]
- Weathers, F.W.; Blake, D.D.; Schnurr, P.P.; Kaloupek, D.G.; Marx, B.P.; Keane, T.M. The Clinician-Administered PTSD Scale for DSM-5 (CAPS-5). Interview Available from the National Center for PTSD. 2013. Available online: www.ptsdva.gov (accessed on 29 March 2021).
- Weathers, F.W.; Bovin, M.J.; Lee, D.J.; Sloan, D.M.; Schnurr, P.P.; Kaloupek, D.G.; Keane, T.M.; Marx, B.P. The Clinician-Administered PTSD Scale for DSM-5 (CAPS-5): Development and initial psychometric evaluation in military veterans. Psychol. Assess. 2018, 30, 383–395. [Google Scholar] [CrossRef]
- Randall, C.; Dickens, A.; White, A.; Sanders, H.; Fox, M.; Campbell, J. Nettle sting for chronic knee pain: A randomised controlled pilot study. Complement. Ther. Med. 2008, 16, 66–72. [Google Scholar] [CrossRef]
- Randall, C.; Randall, H.; Dobbs, F.; Hutton, C.; Sanders, H. Randomized controlled trial of nettle sting for treatment of base-of-thumb pain. J. R. Soc. Med. 2000, 93, 305–309. [Google Scholar] [CrossRef]
- Rayburn, K.; Fleischbein, E.; Song, J.; Allen, B.; Kundert, M.; Leiter, C.; Bush, T. Stinging nettle cream for osteoarthritis. Altern. Ther. Health Med. 2009, 15, 60–61. [Google Scholar]
- Jacquet, A.; Girodet, P.O.; Pariente, A.; Forest, K.; Mallet, L.; Moore, N. Phytalgic, a food supplement, vs. placebo in patients with osteoarthritis of the knee or hip: A randomised double-blind placebo-controlled clinical trial. Arthritis Res. Ther. 2009, 11, R192. [Google Scholar] [CrossRef]
- Lin, Z.; Deng, A. Antioxidative and Free Radical Scavenging Activity of Ganoderma (Lingzhi). Adv. Exp. Med. Biol. 2019, 1182, 271–297. [Google Scholar] [CrossRef] [PubMed]
- Cor, D.; Knez, Z.; Knez Hrncic, M. Antitumour, Antimicrobial, Antioxidant and Antiacetylcholinesterase Effect of Ganoderma Lucidum Terpenoids and Polysaccharides: A Review. Molecules 2018, 23, 649. [Google Scholar] [CrossRef] [PubMed]
- Dhouibi, R.; Affes, H.; Ben Salem, M.; Hammami, S.; Sahnoun, Z.; Zeghal, K.M.; Ksouda, K. Screening of pharmacological uses of Urtica dioica and others benefits. Prog. Biophys. Mol. Biol. 2020, 150, 67–77. [Google Scholar] [CrossRef] [PubMed]
- He, C.; Wang, Z.; Shi, J. Pharmacological effects of icariin. Adv. Pharmacol. 2020, 87, 179–203. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Baseline | Placebo | Lower Dose | Higher Dose | LMM | |
|---|---|---|---|---|---|
| Reishi | |||||
| Pain | 31.1 (24.0) | 31.9 (23.5) | 32.2 (24.7) | 33.8 (25.6) | F (3, 549) = 2.6, p = 0.050 |
| Fatigue | 31.2 (21.8) | 28.6 (19.4) | 30.4 (17.8) | 31.9 (17.9) | F (3, 556) = 5.5, p = 0.001 |
| Stinging Nettle | |||||
| Pain | 29.3 (16.4) | 22.5 (21.4) * | 18.2 (14.6) * | 17.8 (13.2) * | F (3, 626) = 26.1, p < 0.0001 |
| Fatigue | 40.6 (23.1) | 40.3 (27.6) | 38.6 (26.7) | 33.5 (27.4) | F (3, 626) = 0.93, p = 0.424 |
| Epimedium | |||||
| Pain | 29.4 (20.7) | 23.4 (14.8) * | 24.4 (19.5) * | 24.3 (16.8) * | F (3, 635) = 8.4, p < 0.0001 |
| Fatigue | 33.2 (20.8) | 32.2 (19.8) | 30.4 (19.5) * | 34.7 (21.7) | F (3, 635) = 3.8, p = 0.010 |
| Reishi | Stinging Nettle | Epimedium | |||||||
|---|---|---|---|---|---|---|---|---|---|
| Adverse Event | P | LD | HD | P | LD | HD | P | LD | HD |
| Diarrhea | - | 2 | 1 | 1 | 1 | - | 1 | 2 | - |
| Elevated creatinine kinase | - | - | - | - | 1 | - | - | 1 | - |
| Flushing | - | 1 | 1 | - | - | - | - | - | - |
| Headaches | - | 1 | - | 2 | - | - | - | - | - |
| Migraine | 2 | - | 1 | - | - | - | - | - | - |
| Upset stomach, lower GI | 1 | 1 | 1 | - | - | - | - | - | - |
| Worsening fatigue | 1 | 1 | 1 | - | - | - | - | - | - |
| Worsening GERD | 1 | 1 | 1 | - | - | - | - | - | - |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Younger, J.; Donovan, E.K.; Hodgin, K.S.; Ness, T.J. A Placebo-Controlled, Pseudo-Randomized, Crossover Trial of Botanical Agents for Gulf War Illness: Reishi Mushroom (Ganoderma lucidum), Stinging Nettle (Urtica dioica), and Epimedium (Epimedium sagittatum). Int. J. Environ. Res. Public Health 2021, 18, 3671. https://doi.org/10.3390/ijerph18073671
Younger J, Donovan EK, Hodgin KS, Ness TJ. A Placebo-Controlled, Pseudo-Randomized, Crossover Trial of Botanical Agents for Gulf War Illness: Reishi Mushroom (Ganoderma lucidum), Stinging Nettle (Urtica dioica), and Epimedium (Epimedium sagittatum). International Journal of Environmental Research and Public Health. 2021; 18(7):3671. https://doi.org/10.3390/ijerph18073671
Chicago/Turabian StyleYounger, Jarred, Emily K. Donovan, Kathleen S. Hodgin, and Timothy J. Ness. 2021. "A Placebo-Controlled, Pseudo-Randomized, Crossover Trial of Botanical Agents for Gulf War Illness: Reishi Mushroom (Ganoderma lucidum), Stinging Nettle (Urtica dioica), and Epimedium (Epimedium sagittatum)" International Journal of Environmental Research and Public Health 18, no. 7: 3671. https://doi.org/10.3390/ijerph18073671
APA StyleYounger, J., Donovan, E. K., Hodgin, K. S., & Ness, T. J. (2021). A Placebo-Controlled, Pseudo-Randomized, Crossover Trial of Botanical Agents for Gulf War Illness: Reishi Mushroom (Ganoderma lucidum), Stinging Nettle (Urtica dioica), and Epimedium (Epimedium sagittatum). International Journal of Environmental Research and Public Health, 18(7), 3671. https://doi.org/10.3390/ijerph18073671