
A Longitudinal Study Regarding the Health Profile of the 2017 South African Hajj Pilgrims

 ,
,  , , and
, , and
Abstract
1. Introduction
2. Methodology
2.1. Study Design and Data Collection
2.2. Study Population
2.3. Statistical Analysis
2.4. Ethics and Confidentiality
3. Results
3.1. Characteristics of the Study Population
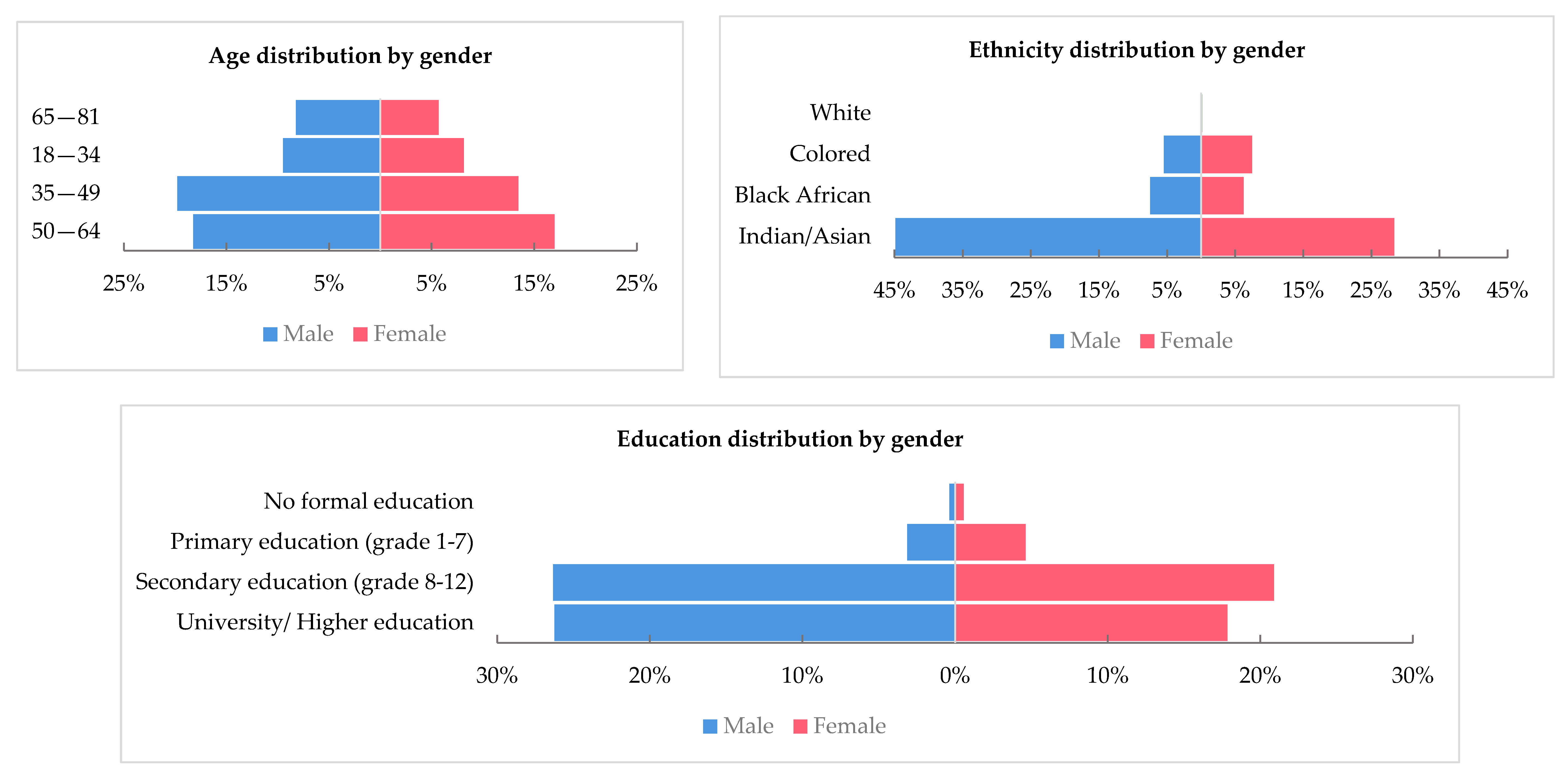
3.1.1. Demographics
3.1.2. Vaccination and Underlying Health Conditions
3.1.3. Pre-Hajj Training and Health Promotion
3.1.4. Health Profile upon Arrival to Saudi Arabia
3.2. Health Profile during and Post-Hajj
3.2.1. Experienced Symptoms
3.2.2. Diagnosis and Prescribed Medications
3.2.3. Treatment Source
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Yezli, S.; Yassin, Y.M.; Awam, A.H.; Attar, A.A.; Al-Jahdali, E.A.; Alotaibi, B.M. Umrah. An Opportunity for Mass Gatherings Health Research. Saudi Med. J. 2017, 38, 868–871. [Google Scholar] [CrossRef]
- Ahmed, Q.A.; Arabi, Y.M.; Memish, Z.A. Health Risks at the Hajj. Lancet 2006, 367, 1008–1015. [Google Scholar] [CrossRef]
- Yezli, S.; Assiri, A.M.; Alhakeem, R.F.; Turkistani, A.M.; Alotaibi, B. Meningococcal Disease during the Hajj and Umrah Mass Gatherings. Int. J. Infect. Dis. 2016, 47, 60–64. [Google Scholar] [CrossRef] [PubMed]
- Yezli, S.; Zumla, A.; Yassin, Y.; Al-Shangiti, A.M.; Mohamed, G.; Turkistani, A.M.; Alotaibi, B. Undiagnosed Active Pulmonary Tuberculosis among Pilgrims during the 2015 Hajj Mass Gathering: A Prospective Cross-Sectional Study. Am. J. Trop. Med. Hyg. 2017, 97, 1304–1309. [Google Scholar] [CrossRef][Green Version]
- Memish, Z.A.; Zumla, A.; Alhakeem, R.F.; Assiri, A.; Turkestani, A.; al Harby, K.D.; Alyemni, M.; Dhafar, K.; Gautret, P.; Barbeschi, M.; et al. Hajj: Infectious Disease Surveillance and Control. Lancet 2014, 383, 2073–2082. [Google Scholar] [CrossRef]
- Shujaa, A.; Alhamid, S. Health Response to Hajj Mass Gathering from Emergency Perspective, Narrative Review. Turk. J. Emerg. Med. 2015, 15, 172–176. [Google Scholar] [CrossRef] [PubMed]
- Ezat, S.; Puteh, W.; al Salem, A.; Radwan, N.A.; Dahliah, S.; Zannah, A. The Causes of Malaysian and Indonesian Pilgrims’ Hospitalization during the Hajj Season 1440 (2019) in Mena and Arafat Hospitals. Saudi J. Biomed. Res. Abbreviated Key Title Saudi J. Biomed. Res. 2019. [Google Scholar] [CrossRef]
- Khan, I.D.; Khan, S.A.; Asima, B.; Hussaini, S.B.; Zakiuddin, M.; Faisal, F.A. Morbidity and Mortality amongst Indian Hajj Pilgrims: A 3-Year Experience of Indian Hajj Medical Mission in Mass-Gathering Medicine. J. Infect. Public Health 2018, 11, 165–170. [Google Scholar] [CrossRef]
- Yezli, S.; Elganainy, A.; Awam, A. Strengthening Health Security at the Hajj Mass Gatherings: A Harmonised Hajj Health Information System. J. Travel Med. 2018, 25, 1–2. [Google Scholar] [CrossRef]
- Statistic South Africa Community Survey 2016 IN BRIEF. Available online: http://www.statssa.gov.za/wp-content/uploads/2016/03/CS-FW-ID.pdf (accessed on 10 September 2020).
- Alzeer, A.H. Respiratory Tract Infection during Hajj. Ann. Thorac. Med. 2009, 4, 50–53. [Google Scholar] [CrossRef] [PubMed]
- Aleeban, M.; Mackey, T.K. Global Health and Visa Policy Reform to Address Dangers of Hajj during Summer Seasons. Front. Public Health 2016, 4. [Google Scholar] [CrossRef] [PubMed]
- Pane, M.; Yin Mei Kong, F.; Bayu Purnama, T.; Glass, K.; Imari, S.; Samaan, G.; Oshitani, H. Indonesian Hajj Cohorts and Mortality in Saudi Arabia From. J. Epidemiol. Glob. Health 2004, 9, 11–18. [Google Scholar] [CrossRef]
- Al-Ghamdi, S.M.G.; Akbar, H.O.; Qari, Y. Pattern of Admission to Hospitals during Muslim Pilgrimage (Hajj) Sleep Disorders View Project Liver Fibrosis View Project. Saudi Med. J. 2003, 24, 1073–1076. [Google Scholar]
- Khan, N.A.; Ishag, A.M.; Ahmad, M.S.; El-Sayed, F.M.; Bachal, Z.A.; Abbas, T.G. Pattern of Medical Diseases and Determinants of Prognosis of Hospitalization during 2005 Muslim Pilgrimage (Hajj) in a Tertiary Care Hospital. A Prospective Cohort Study. Saudi Med. J. 2006, 27, 1373–1380. [Google Scholar] [PubMed]
- Al Shimemeri, A. Cardiovascular Disease in Hajj Pilgrims. J. Saudi Heart Assoc. 2012, 24, 123–127. [Google Scholar] [CrossRef]
- Yezli, S.; Alotaibi, B.M.; Saeed, A.A.B. The Hajj Health Requirements: Time for a Serious Review? Lancet 2016, 387, 845–846. [Google Scholar] [CrossRef]
- Sridhar, S.; Benkouiten, S.; Belhouchat, K.; Drali, T.; Memish, Z.A.; Parola, P.; Brouqui, P.; Gautret, P. Foot Ailments during Hajj: A Short Report. J. Epidemiol. Glob. Health 2015, 5, 291–294. [Google Scholar] [CrossRef] [PubMed]
- Kim, H.-Y. Statistical Notes for Clinical Researchers: Chi-Squared Test and Fisher’s Exact Test. Restor. Dent. Endod. 2017, 42, 152. [Google Scholar] [CrossRef] [PubMed]
- Ebrahim, S.H.; Memish, Z.A.; Uyeki, T.M.; Khoja, T.A.M.; Marano, N.; McNabb, S.J.N. Pandemic H1N1 and the 2009 Hajj. Science 2009, 326, 938–940. [Google Scholar] [CrossRef]
- General Authority for Statistics (Saudi Arabia). Hajj Statistics 2017. Available online: https://www.stats.gov.sa/sites/default/files/haj_1438.pdf (accessed on 13 February 2020).
- Verhoeven, P.O.; Gautret, P.; Haddar, C.H.; Benkouiten, S.; Gagnaire, J.; Belhouchat, K.; Grattard, F.; Charrel, R.; Pozzetto, B.; Drali, T.; et al. Molecular Dynamics of Staphylococcus Aureus Nasal Carriage in Hajj Pilgrims. Clinical Microbiology and Infection 2015, 21, 650.e5–650.e8. [Google Scholar] [CrossRef]
- Zhang, Y.; Shi, F.; Yu, Z.; Yang, A.; Zeng, M.; Wang, J.; Yin, H.; Zhang, B.; Ma, X. A Cross-Sectional Study on Factors Associated with Hypertension and Genetic Polymorphisms of Renin-Angiotensin-Aldosterone System in Chinese Hui Pilgrims to Hajj. BMC Public Health 2019, 19, 1–11. [Google Scholar] [CrossRef]
- Gautret, P.; Benkouiten, S.; Griffiths, K.; Sridhar, S. The Inevitable Hajj Cough: Surveillance Data in French Pilgrims, 2012–2014. Travel Med. Infect. Dis. 2015, 13, 485–489. [Google Scholar] [CrossRef]
- Parker, S.; Parker, S. The Hajj: A Constant Travel Destination amidst Changing Times. South. Afr. J. Epidemiol. Infect. 2010, 25, 14–18. [Google Scholar] [CrossRef]
- Yezli, S.; Mushi, A.; Yassin, Y.; Maashi, F.; Khan, A. Knowledge, Attitude and Practice of Pilgrims Regarding Heat-Related Illnesses during the 2017 Hajj Mass Gathering. Int. J. Environ. Res. Public Health 2019, 16, 3215. [Google Scholar] [CrossRef]
- Pane, M.; Imari, S.; Alwi, Q.; Nyoman Kandun, I.; Cook, A.R.; Samaan, G. Causes of Mortality for Indonesian Hajj Pilgrims: Comparison between Routine Death Certificate and Verbal Autopsy Findings. PLoS ONE 2013, 8, e73243. [Google Scholar] [CrossRef] [PubMed]
- Alqahtani, A.S.; Althimiri, N.A.; BinDhim, N.F. Saudi Hajj Pilgrims’ Preparation and Uptake of Health Preventive Measures during Hajj 2017. J. Infect. Public Health 2019, 12, 772–776. [Google Scholar] [CrossRef] [PubMed]
- UNU-WIDER Morné Oosthuizen UNU-WIDER: Research Brief: Racial Inequality and Demographic Change in South Africa. Available online: https://www.wider.unu.edu/publication/racial-inequality-and-demographic-change-south-africa (accessed on 10 September 2020).
- Yezli, S.; Mushi, A.; Almuzaini, Y.; Balkhi, B.; Yassin, Y.; Khan, A. Prevalence of Diabetes and Hypertension among Hajj Pilgrims: A Systematic Review. Int. J. Environ. Res. Public Health 2021, 18, 1155. [Google Scholar] [CrossRef] [PubMed]
- Hoang, V.T.; Ali-Salem, S.; Belhouchat, K.; Meftah, M.; Sow, D.; Dao, T.L.; Ly, T.D.A.; Drali, T.; Ninove, L.; Yezli, S.; et al. Respiratory Tract Infections among French Hajj Pilgrims from 2014 to 2017. Sci. Rep. 2019, 9, 1–8. [Google Scholar] [CrossRef]
- Tashani, M.; Barasheed, O.; Azeem, M.; Alfelali, M.; Badahdah, A.-M.; Bokhary, H.; Almasri, N.; Alshehri, J.; Matbouly, G.; Kalantan, N.; et al. Pneumococcal Vaccine Uptake Among Australian Hajj Pilgrims in 2011-13. Infect. Disord. Drug Targets 2014, 14, 117–124. [Google Scholar] [CrossRef] [PubMed]
- Razavi, S.M.; Sabouri-Kashani, A.; Ziaee-Ardakani, H.; Tabatabaei, A.; Karbakhsh, M.; Sadeghipour, H.; Mortazavi-Tabatabaei, S.A.; Salamati, P. Trend of Diseases among Iranian Pilgrims during Five Consecutive Years Based on a Syndromic Surveillance System in Hajj. Med J. Islamic Repub. Iran 2013, 27, 179–185. [Google Scholar]
- World Health Organization GHO|by Category|Raised Blood Pressure (SBP ≥ 140 OR DBP ≥ 90), Age-Standardized (%)—Estimates by Country [Internet]. 2015. Available online: https://www.who.int/diabetes/country-profiles/zaf_en.pdf?ua=1 (accessed on 10 September 2020).
- Madani, T.A.; Ghabrah, T.M.; Albarrak, A.M.; Alhazmi, M.A.; Alazraqi, T.A.; Althaqafi, A.O.; Ishaq, A.H. Causes of Admission to Intensive Care Units in the Hajj Period of the Islamic Year 1424 (2004). Ann. Saudi Med. 2007, 27, 101–105. [Google Scholar] [CrossRef]
- Yezli, S.; bin Saeed, A.A.; Assiri, A.M.; Alhakeem, R.F.; Yunus, M.A.; Turkistani, A.M.; Booy, R.; Alotaibi, B.M. Prevention of Meningococcal Disease during the Hajj and Umrah Mass Gatherings: Past and Current Measures and Future Prospects. Int. J. Infect. Dis. 2016, 47, 71–78. [Google Scholar] [CrossRef]
- Saudi Arabia Ministry of Health. 1441H.-Hajj Season—Health Regulations. Available online: https://www.moh.gov.sa/en/Hajj/Pages/HealthRegulations.aspx (accessed on 10 September 2020).
- Benkouiten, S.; Al-Tawfiq, J.A.; Memish, Z.A.; Albarrak, A.; Gautret, P. Clinical Respiratory Infections and Pneumonia during the Hajj Pilgrimage: A Systematic Review. Travel Med. Infect. Dis. 2019, 28, 15–26. [Google Scholar] [CrossRef] [PubMed]
- Hoang, V.-T.; Dao, T.-L.; Duc Anh Ly, T.; Belhouchat, K.; Larbi Chaht, K.; Gaudart, J.; Mmadi Mrenda, B.; Drali, T.; Yezli, S.; Alotaibi, B.; et al. The Dynamics and Interactions of Respiratory Pathogen Carriage among French Pilgrims during the 2018 Hajj. Taylor Francis 2019, 8, 1701–1710. [Google Scholar] [CrossRef] [PubMed]
- Lessler, J.; Reich, N.G.; Brookmeyer, R.; Perl, T.M.; Nelson, K.E.; Cummings, D.A. Incubation Periods of Acute Respiratory Viral Infections: A Systematic Review. Lancet Infect. Dis. 2009, 9, 291–300. [Google Scholar] [CrossRef]
- Salmon-Rousseau, A.; Piednoir, E.; Cattoir, V.; de La Blanchardière, A. Infections Liées Au Hadj. Médecine et Maladies Infectieuses 2016, 46, 346–354. [Google Scholar] [CrossRef]
- Centers for Disease Control and Prevention Food Poisoning Symptoms|Food Safety|CDC. Available online: https://www.cdc.gov/foodsafety/symptoms.html (accessed on 10 September 2020).
- Yezli, S.; Zaraa, S.; Yassin, Y.; Mushi, A.; Stergachis, A.; Khan, A. Medication Utilization Pattern among Outpatients during the Hajj Mass Gathering. Saudi Pharm. J. 2020, 28, 1122–1128. [Google Scholar] [CrossRef]
- Hoang, V.T.; Nguyen, T.T.T.; Belhouchat, K.; Meftah, M.; Sow, D.; Benkouiten, S.; Dao, T.L.; Anh Ly, T.D.; Drali, T.; Yezli, S.; et al. Antibiotic Use for Respiratory Infections among Hajj Pilgrims: A Cohort Survey and Review of the Literature. Travel Med. Infect. Dis. 2019, 30, 39–45. [Google Scholar] [CrossRef]
- Hoang, V.T.; Meftah, M.; Anh Ly, T.D.; Drali, T.; Yezli, S.; Alotaibi, B.; Raoult, D.; Parola, P.; Pommier de Santi, V.; Gautret, P. Bacterial Respiratory Carriage in French Hajj Pilgrims and the Effect of Pneumococcal Vaccine and Other Individual Preventive Measures: A Prospective Cohort Survey. Travel Med. Infect. Dis. 2019, 31, 101343. [Google Scholar] [CrossRef]
- Yezli, S.; Khan, A.; Bouchama, A. Summer Hajj Pilgrimage in the Era of Global Warming: A Call for Vigilance and Better Understanding of the Risks. J. Travel Med. 2019, 26. [Google Scholar] [CrossRef]
- Alqahtani, A.S.; Wiley, K.E.; Tashani, M.; Willaby, H.W.; Heywood, A.E.; BinDhim, N.F.; Booy, R.; Rashid, H. Exploring Barriers to and Facilitators of Preventive Measures against Infectious Diseases among Australian Hajj Pilgrims: Cross-Sectional Studies before and after Hajj. Int. J. Infect. Dis. 2016, 47, 53–59. [Google Scholar] [CrossRef]
- Badahdah, A.-M.; Alghabban, F.; Falemban, W.; Albishri, A.; Rani Banik, G.; Alhawassi, T.; Abuelizz, H.; Bakarman, M.A.; Khatami, A.; Booy, R.; et al. Meningococcal Vaccine for Hajj Pilgrims: Compliance, Predictors, and Barriers. Trop. Med. Infect. Dis. 2019, 4, 127. [Google Scholar] [CrossRef]
- Bieh, K.L.; Khan, A.; Yezli, S.; El-Ganainy, A.; Asiri, S.; Alotaibi, B.; Ghallab, S.; Elkholy, A.; Abubakar, A.; Jokhdar, H. Implementing the Health Early Warning System Based on Syndromic and Event-Based Surveillance at the 2019 Hajj. East. Mediterr. Health J. 2020, 26, 1570–1575. [Google Scholar] [CrossRef]
- Alotaibi, B.M.; Yezli, S.; bin Saeed, A.A.A.; Turkestani, A.; Alawam, A.H.; Bieh, K.L. Strengthening Health Security at the Hajj Mass Gatherings: Characteristics of the Infectious Diseases Surveillance Systems Operational during the 2015 Hajj. J. Travel Med. 2017, 24. [Google Scholar] [CrossRef] [PubMed]
- Soon, S.; Svavarsdottir, H.; Downey, C.; Jayne, D.G. Wearable Devices for Remote Vital Signs Monitoring in the Outpatient Setting: An Overview of the Field. BMJ Innov. 2020, 6, 55. [Google Scholar] [CrossRef]
- Zhao, F.; Li, M.; Tsien, J.Z. Technology Platforms for Remote Monitoring of Vital Signs in the New Era of Telemedicine. Expert Rev. Med Devices 2015, 12, 411–429. [Google Scholar] [CrossRef]
- Alghamdi, S.; Alqahtani, J.; Aldhahir, A. Current Status of Telehealth in Saudi Arabia during COVID-19. J. Fam. Community Med. 2020, 27, 208–211. [Google Scholar] [CrossRef]
- Jokhdar, H.; Khan, A.; Asiri, S.; Motair, W.; Assiri, A.; Alabdulaali, M. COVID-19 M Itigation Plans D Uring H Ajj 2020: A S Uccess S Tory of Z Ero C Ases. Health Secur. 2020. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Variable | Number (n) | Percentage (%) |
|---|---|---|
| Pilgrims enrolled | 1138 * | |
| Gender | 1114 | |
| Male | 622 | 55.8 |
| Age Group | 1130 | |
| 18–34 | 199 | 17.6 |
| 35–49 | 372 | 32.9 |
| 50–64 | 398 | 35.2 |
| 65–81 | 161 | 14.2 |
| Highest education level | 1098 | |
| No formal education | 10 | 0.9 |
| Primary education (grade 1–7) | 88 | 8.0 |
| Secondary education (grade 8–12) | 519 | 47.3 |
| University/Higher education | 481 | 43.8 |
| Read | 1127 | |
| Yes | 1124 | 99.73 |
| Write | 1112 | |
| Yes | 1108 | 99.64 |
| Marital status | 1125 | |
| Married | 992 | 88.2 |
| Single | 88 | 7.8 |
| Others | 45 | 4.0 |
| Ethnicity | 652 | |
| Indian/Asian | 476 | 73.0 |
| Black African | 92 | 14.1 |
| Colored | 83 | 12.7 |
| White | 1 | 0.2 |
| Travel insurance | 1011 | |
| No | 446 | 44.1 |
| Yes, including Hajj | 348 | 34.4 |
| Yes, without Hajj | 65 | 6.4 |
| Do not know | 152 | 15.0 |
| Previously performed Hajj | 1126 | |
| Yes | 113 | 10.0 |
| Hajj performance, how long ago | 484 | |
| Last year | 3 | 6.3 |
| 1–5 Years | 4 | 8.3 |
| More than 5 years | 41 | 85.4 |
| Previously performed Umrah | 1114 | |
| Yes | 495 | 44.4 |
| Umrah performance, how long ago | 224 | |
| Less than a Year | 16 | 7.1 |
| 1–5 Years | 137 | 61.2 |
| More than 5 years | 71 | 31.7 |
| Travel outside South Africa in the past 6 months | 1112 | |
| Yes | 167 | 15.0 |
| Country frequency (Most visited countries in the past 6 months) | 225 | |
| India | 18 | 8.0 |
| Mauritius | 10 | 4.4 |
| Saudi Arabia | 23 | 10.2 |
| UAE ** | 30 | 13.3 |
| Other (# of countries less than 4%) | 144 | 64.1 |
| Currently pregnant (pregnancy status) | 475 | |
| No | 460 | 96.8 |
| Yes | 7 | 1.5 |
| Do not know | 8 | 1.7 |
| Pregnancy months | 7 | |
| First Trimester | 6 | 85.8 |
| Second Trimester | 1 | 14.3 |
| Variable | n | Yes | % |
|---|---|---|---|
| Vaccination | |||
| Yellow fever vaccination | 1137 | 1082 | 95.2 |
| Polio vaccination | 1018 | 89 | 8.7 |
| Influenza vaccination | 1019 | 241 | 23.7 |
| Pneumococcal vaccination | 1019 | 48 | 4.7 |
| Meningococcal vaccination | 1131 | 1113 | 98.4 |
| Health conditions | |||
| High blood pressure | 1057 | 239 | 22.6 |
| Diabetes mellitus | 1057 | 139 | 13.2 |
| Type 1 | 67 | 8 | 11.9 |
| Type 2 | 67 | 59 | 88.1 |
| Heart attack | 1055 | 32 | 3.0 |
| Chronic respiratory illness | 1055 | 72 | 6.8 |
| Chronic kidney disease | 1056 | 15 | 1.4 |
| Hemodialysis | 15 | 5 | 33.0 |
| Epilepsy | 1055 | 9 | 0.9 |
| Angina | 1055 | 30 | 2.8 |
| High cholesterol | 1057 | 122 | 11.5 |
| Cancer | 1055 | 16 | 1.5 |
| Allergy | 1058 | 84 | 7.9 |
| Environment | 90 | 53 | 58.8 |
| Food | 90 | 8 | 8.8 |
| Medication | 90 | 35 | 38.8 |
| Other | 90 | 2 | 2.2 |
| Other condition | 1054 | 17 | 1.6 |
| Variable | n | Yes | % |
|---|---|---|---|
| know where to seek medical care in KSA before arrival | 1126 | 863 | 76.6 |
| know where medical mission clinics location in KSA before arrival | 1113 | 738 | 66.3 |
| Hajj training received before arrival to KSA | 1126 | 1019 | 90.5 |
| Information about health risks in KSA before arrival | 1103 | 733 | 66.5 |
| Heat related illnesses | 127 | 46 | 36.2 |
| Respiratory related illness | 127 | 52 | 40.9 |
| Gastrointestinal disorders | 127 | 15 | 11.8 |
| Other | 127 | 77 | 60.6 |
| Information on how to seek medical help received before arrival to KSA | 1113 | 976 | 87.7 |
| Health messages received before arrival to KSA | 1106 | 625 | 56.5 |
| Hand hygiene | 1131 | 505 | 44.7 |
| Heat-related illnesses | 1131 | 479 | 42.4 |
| Cough etiquette | 1131 | 380 | 33.6 |
| No messages received | 1131 | 215 | 19.0 |
| Others health messages received | 1131 | 36 | 3.2 |
| Health messages received before arrival were easy to understand | 602 | ||
| No | 602 | 29 | 4.8 |
| Yes | 602 | 573 | 95.2 |
| Variable | During | Post | p Value | ||||
|---|---|---|---|---|---|---|---|
| n | Yes | % | n | Yes | % | ||
| Fall ill | 916 | 596 | 65.1 | 915 | 365 | 39.9 | 0.000 |
| Symptoms | |||||||
| Respiratory symptoms | 588 | 413 | 70.2 | 349 | 287 | 82.2 | 0.000 |
| GIT * symptoms | 588 | 32 | 5.4 | 349 | 5 | 1.4 | 0.002 |
| Fever | 588 | 68 | 11.6 | 349 | 34 | 9.7 | 0.387 |
| Dehydration | 588 | 64 | 10.9 | 349 | 0 | 0.0 | 0.000 |
| Walking Related symptoms | 588 | 59 | 10.0 | 349 | 25 | 7.1 | 0.137 |
| Other symptoms | 588 | 226 | 38.4 | 349 | 95 | 27.7 | 0.000 |
| Diagnosis | |||||||
| Respiratory disease | 536 | 375 | 70.0 | 309 | 252 | 81.5 | 0.000 |
| Muscular illnesses | 536 | 28 | 5.2 | 309 | 1 | 0.3 | 0.000 |
| Blood pressure disorders | 536 | 17 | 3.2 | 309 | 1 | 0.3 | 0.006 |
| Gastrointestinal disorders | 536 | 15 | 2.8 | 309 | 3 | 1.0 | 0.076 |
| Urinary tract disease | 536 | 8 | 1.5 | 309 | 1 | 0.3 | 0.102 |
| Diabetes | 536 | 8 | 1.5 | 309 | 0 | 0.0 | 0.260 |
| Ear infection | 536 | 4 | 0.7 | 309 | 2 | 0.6 | 0.087 |
| Allergy | 536 | 4 | 0.7 | 309 | 0 | 0.0 | 0.161 |
| Cancer diagnosis | 536 | 1 | 0.2 | 309 | 0 | 0.0 | 0.634 |
| Heat related illnesses | 536 | 1 | 0.2 | 309 | 0 | 0.0 | 0.634 |
| Medications | |||||||
| Antibiotic | 523 | 346 | 66.2 | 268 | 184 | 68.7 | 0.479 |
| Respiratory symptoms medication | 523 | 168 | 32.1 | 268 | 119 | 44.4 | 0.001 |
| Vitamins | 523 | 122 | 23.3 | 268 | 4 | 1.5 | 0.000 |
| Analgesic medication | 523 | 65 | 12.4 | 268 | 13 | 4.9 | 0.001 |
| Gastrointestinal symptom medication | 523 | 17 | 3.3 | 268 | 0 | 0.0 | 0.003 |
| Asthma medication | 523 | 15 | 2.9 | 268 | 8 | 3.0 | 0.926 |
| Diabetes medication | 523 | 3 | 0.6 | 268 | 0 | 0.0 | 0.288 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Mushi, A.; Yassin, Y.; Khan, A.; Alotaibi, B.; Parker, S.; Mahomed, O.; Yezli, S. A Longitudinal Study Regarding the Health Profile of the 2017 South African Hajj Pilgrims. Int. J. Environ. Res. Public Health 2021, 18, 3607. https://doi.org/10.3390/ijerph18073607
Mushi A, Yassin Y, Khan A, Alotaibi B, Parker S, Mahomed O, Yezli S. A Longitudinal Study Regarding the Health Profile of the 2017 South African Hajj Pilgrims. International Journal of Environmental Research and Public Health. 2021; 18(7):3607. https://doi.org/10.3390/ijerph18073607
Chicago/Turabian StyleMushi, Abdulaziz, Yara Yassin, Anas Khan, Badriah Alotaibi, Salim Parker, Ozayr Mahomed, and Saber Yezli. 2021. "A Longitudinal Study Regarding the Health Profile of the 2017 South African Hajj Pilgrims" International Journal of Environmental Research and Public Health 18, no. 7: 3607. https://doi.org/10.3390/ijerph18073607
APA StyleMushi, A., Yassin, Y., Khan, A., Alotaibi, B., Parker, S., Mahomed, O., & Yezli, S. (2021). A Longitudinal Study Regarding the Health Profile of the 2017 South African Hajj Pilgrims. International Journal of Environmental Research and Public Health, 18(7), 3607. https://doi.org/10.3390/ijerph18073607