
Association between Psychopathological Dimensions and Sexual Functioning/Sexual Arousal in Young Adults

 ,
,  ,
,  , , ,
, , ,  and
and 
Abstract
1. Introduction
- To examine the association between psychopathological dimensions and dimensions of sexual functioning (i.e., desire, arousal, erection, orgasm, and sexual satisfaction).
- To examine the association of psychopathological dimensions with a specific dimension of sexual response within a laboratory task (i.e., subjective sexual arousal).
2. Study 1
2.1. Materials and Methods
2.1.1. Participants
2.1.2. Instruments
2.1.3. Procedure
2.1.4. Data Analysis
2.2. Results
Discussion Study 1
3. Study 2
3.1. Materials and Methods
3.1.1. Participants
3.1.2. Procedure
3.1.3. Instruments
3.2. Results
Discussion Study 2
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement.
Conflicts of Interest
References
- American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders, 5th ed.; American Psychiatric Association: Washington, DC, USA, 2008. [Google Scholar]
- Chapa, H.O.; Fish, J.T.; Hagar, C.; Wilson, T. Prevalence of female sexual dysfunction among women attending college presenting for gynecological care at a university student health center. J. Am. Coll. Health 2018, 68, 52–60. [Google Scholar] [CrossRef]
- Shifren, J.L.; Monz, B.U.; Russo, P.A.; Segreti, A.; Johannes, C.B. Sexual problems and distress in United States women: Prevalence and correlates. Obstet. Gynecol. 2008, 112, 970–978. [Google Scholar] [CrossRef] [PubMed]
- Worsley, R.; Bell, R.J.; Gartoulla, P.; Davis, S.R. Prevalence and predictors of low sexual desire, sexually related personal distress, and hypoactive sexual desire dysfunction in a community-based sample of midlife women. J. Sex. Med. 2017, 14, 675–686. [Google Scholar] [CrossRef] [PubMed]
- De Rose, A.F.; Gallo, F.; Bini, P.M.; Gattuccio, I.; Chiriaco, V.; Terrone, C. Epidemiology of sexual disorders in general medical practice: An Italian survey. Urol. J. 2019, 86, 79–85. [Google Scholar] [CrossRef] [PubMed]
- Hendrickx, L.; Gijs, L.; Enzlin, P. Age-related prevalence rates of sexual difficulties, sexual dysfunctions and sexual distress in heterosexual men: Results from an online survey in Flanders. Sex. Relatsh. Ther. 2019, 34, 440–461. [Google Scholar] [CrossRef]
- Lewis, R.W.; Fugl-Meyer, K.S.; Bosch, R.; Fugl-Meyer, A.R.; Laumann, E.O.; Lizza, E.; Martin-Morales, A. Epidemiology/Risk Factors of Sexual Dysfunction. J. Sex. Med. 2004, 1, 35–39. [Google Scholar] [CrossRef]
- Christensen, B.S.; Gronbaek, M.; Osler, M.; Pedersen, B.V.; Graugaard, C.; Frisch, M. Sexual dysfunctions and difficulties in Denmark: Prevalence and associated sociodemographic factors. Arch. Sex. Behav. 2011, 40, 121–132. [Google Scholar] [CrossRef] [PubMed]
- Clayton, A.H.; Vallarades Juarez, E.M. Female sexual dysfunction. Psychiatr. Clin. N. Am. 2017, 40, 267–284. [Google Scholar] [CrossRef]
- Mattoo, S.K.; Ghosh, A.; Subodh, B.N.; Basu, D.; Satapathy, A.; Prasad, S.; Sharma, M.P. Sexual dysfunction in men on buprenorphine—naloxone-based substitution therapy. Indian J. Psychiatry 2020, 62, 66–72. [Google Scholar] [CrossRef]
- Lin, C.F.; Juang, Y.Y.; Wen, J.K.; Liu, C.Y.; Hung, C.I. Correlations between sexual dysfunction, depression, anxiety, and somatic symptoms among patients with major depressive disorder. Chang Gung Med. J. 2012, 35, 323–331. [Google Scholar]
- Lourenço, M.; Azevedo, L.P.; Gouveia, J.L. Depression and Sexual Desire: An exploratory study in psychiatric patients. J. Sex Marital Ther. 2011, 37, 32–44. [Google Scholar] [CrossRef]
- Mahmoud, O.E.; Ahmed, A.R.; Arafa, A.E. Patterns of female sexual dysfunction in premenopausal women with moderate to severe depression in Beni-Suef, Egypt. Middle East Fertil. Soc. J. 2018, 23, 501–504. [Google Scholar] [CrossRef]
- De Boer, M.K.; Castelein, S.; Wiersma, D.; Schoevers, R.A.; Knegtering, H. The facts about sexual (dys)function in schizophrenia: An overview of clinically relevant findings. Schizophr. Bull. 2015, 41, 674–686. [Google Scholar] [CrossRef]
- Rezaei, O.; Fadai, F.; Sayadnasiri, M.; Palizvan, M.A.; Armoon, B.; Noroozi, M. The effect of bupropion on sexual function in patients with schizophrenia: A randomized clinical trial. Eur. J. Psychiatry 2018, 32, 11–15. [Google Scholar] [CrossRef]
- Sreelakshmy, R.; Velayudhan, R.; Kuriakose, D.; Nair, R. Sexual dysfunction in females with depression: A cross-sectional study. Trends Psychiatry Psychother. 2017, 39, 106–109. [Google Scholar] [CrossRef]
- Kendurkar, A.; Kaur, B. Major depressive disorder, obsessive-compulsive disorder, and generalized anxiety disorder: Do the sexual dysfunctions differ? Prim. Care Companion J. Clin. Psychiatry 2008, 10, 299–305. [Google Scholar] [CrossRef] [PubMed]
- Van Minnen, A.; Kampman, M. The interaction between anxiety and sexual functioning: A controlled study of sexual functioning in women with anxiety disorders. Sex. Relatsh. Ther. 2000, 15, 47–57. [Google Scholar] [CrossRef]
- Wells, S.Y.; Glassman, L.H.; Talkovsky, A.M.; Chatfield, M.A.; Sohn, M.J.; Morland, L.A.; Mackintosh, M.A. Examining changes in sexual functioning after cognitive processing therapy in a sample of women trauma survivors. Womens Health Issues 2019, 29, 72–79. [Google Scholar] [CrossRef]
- Yehuda, R.; Lehrner, A.; Rosenbaum, T.Y. PTSD and sexual dysfunction in men and women. J. Sex. Med. 2015, 12, 1107–1119. [Google Scholar] [CrossRef] [PubMed]
- Elkhiat, Y.I.; Seif, A.F.A.; Khalil, M.A.; Din, S.F.G.; Hassan, N.S. Sexual functions in male and female patients with bipolar disorder during remission. J. Sex. Med. 2018, 15, 1111–1116. [Google Scholar] [CrossRef]
- Dunkley, C.R.; Svatko, Y.; Brotto, L.A. Eating disorders and sexual function reviewed: A trans-diagnostic, dimensional perspective. Curr. Sex. Health Rep. 2020, 12, 1–14. [Google Scholar] [CrossRef]
- Gonidakis, F.; Kravvariti, V.; Varsou, E. Sexual function of women suffering from anorexia nervosa and bulimia nervosa. J. Sex Marital Ther. 2014, 41, 368–378. [Google Scholar] [CrossRef] [PubMed]
- Grauvogl, A.; Pelzer, B.; Radder, V.; van Lankveld, J. Associations between personality disorder characteristics, psychological symptoms, and sexual functioning in young women. J. Sex. Med. 2018, 15, 192–200. [Google Scholar] [CrossRef] [PubMed]
- Kayhan, F.; Kucuk, A.; Satan, Y.; İlgün, E.; Arslan, Ş.; İlik, F. Sexual dysfunction, mood, anxiety, and personality disorders in female patients with fibromyalgia. Neuropsychiatr. Dis. Treat. 2016, 12, 349–355. [Google Scholar] [CrossRef]
- Khazaie, H.; Rezaie, L.; Payam, N.R.; Najafi, F. Antidepressant-induced sexual dysfunction during treatment with fluoxetine, sertraline and trazodone; a randomized controlled trial. Gen. Hosp. Psychiatry 2015, 37, 40–45. [Google Scholar] [CrossRef] [PubMed]
- Montejo, A.L.; Montejo, L.; Baldwin, D.S. The impact of severe mental disorders and psychotropic medications on sexual health and its implications for clinical management. World Psychiatry 2018, 17, 3–11. [Google Scholar] [CrossRef] [PubMed]
- Sierra, J.C.; Vallejo-Medina, P.; Santos-Iglesias, P.; Fernández, M.L. Validación del Massachusetts General Hospital-Sexual Functioning Questionnaire (MGH-SFQ) en población española. Aten. Primaria 2012, 44, 516–526. [Google Scholar] [CrossRef]
- Arnett, J.J. Emerging adulthood: A theory of development from the late teens through the twenties. Am. Psychol. 2000, 55, 469–480. [Google Scholar] [CrossRef]
- Davison, M.K.; Bershadsky, B.; Bieber, L.; Silversmith, D.; Maruish, M.E.; Kane, R.L. Development of a brief, multidimensional, self-report instrument for treatment outcomes assessment in psychiatric settings: Preliminary findings. Assessment 1997, 4, 259–276. [Google Scholar] [CrossRef]
- Sandín, B.; Valiente, R.M.; Chorot, P.; Santed, M.A.; Lostao, L. SA-45: Forma abreviada del SCL-90. Psicothema 2008, 20, 290–296. [Google Scholar]
- Fava, M.; Rankin, M.A.; Alpert, J.E.; Nierenberg, A.A.; Worthington, J.J. An open trial of oral sildenafil in antidepressant-induced sexual dysfunction. Psychother. Psychosom. 1998, 67, 328–331. [Google Scholar] [CrossRef]
- R Core Team. R: A Language and Environment or Statistical Computing Vienna; R Foundation for Statistical Computing: Vienna, Austria, 2017. [Google Scholar]
- Rosseel, Y.; Lavaan. An R package for structural equation modeling. J. Stat. Softw. 2012, 48, 1–36. [Google Scholar] [CrossRef]
- Bazarganipour, F.; Ziaei, S.; Montazeri, A.; Foroozanfard, F.; Kazemnejad, A.; Faghihzadeh, S. Health-related quality of life in patients with polycystic ovary syndrome (PCOS): A model-based study of predictive factors. J. Sex. Med. 2014, 11, 1023–1032. [Google Scholar] [CrossRef] [PubMed]
- Skrepnek, G.H. Regression methods in the empiric analysis of health care data. J. Manag. Care Spec. Pharm. 2005, 11, 240–251. [Google Scholar] [CrossRef]
- Kolacz, J.; Hu, Y.; Gesselman, A.N.; Garcia, J.R.; Lewis, G.F.; Porges, S.W. Sexual function in adults with a history of childhood maltreatment: Mediating effects of self-reported autonomic reactivity. Psychol. Trauma 2020, 12, 281–290. [Google Scholar] [CrossRef] [PubMed]
- Lin, C.Y.; Burri, A.; Fridlund, B.; Pakpour, A.H. Female sexual function mediates the effects of medication adherence on quality of life in people with epilepsy. Epilepsy Behav. 2017, 67, 60–65. [Google Scholar] [CrossRef]
- Sullivan, G.M.; Feinn, R. Using effect size—Or why the P value is not enough. J. Grad. Med. Educ. 2012, 4, 279–282. [Google Scholar] [CrossRef]
- Çokluk, Ö.; Kayri, M. The effects of methods of imputation for missing values on the validity and reliability of scales. Educ. Sci. Theory Pract. 2011, 11, 303–309. [Google Scholar]
- IBM Knowledge Center. Estimation Methods for Replacing Missing Values. Available online: https://www.ibm.com/support/knowledgecenter/en/SSLVMB_subs/statistics_mainhelp_ddita/spss/base/replace_missing_values_estimation_methods.html (accessed on 18 March 2021).
- Moreau, C.; Kågesten, A.E.; Blum, R.W. Sexual dysfunction among youth: An overlooked sexual health concern. BMC Public Health 2016, 16, 1170. [Google Scholar] [CrossRef] [PubMed]
- O’Sullivan, L.F.; Byers, E.S.; Brotto, L.A.; Majerovich, J.A.; Fletcher, J. A longitudinal study of problems in sexual functioning and related sexual distress among middle to late adolescents. J. Adolesc. Health 2016, 59, 318–324. [Google Scholar] [CrossRef]
- Sánchez-Fuentes, M.M.; Moyano, N.; Granados, R.; Sierra, J.C. Validation of the Spanish version of the Arizona Sexual Experience Scale (ASEX) using self-reported and psychophysiological measures. Rev. Iberoam. Psicol. Salud 2019, 10, 1–14. [Google Scholar] [CrossRef]
- Sierra, J.C.; Granados, R.; Sánchez-Fuentes, M.M.; Moyano, N.; López, C. Activación sexual ante estímulos sexuales visuales: Comparación entre hombres y mujeres [Poster]. In Proceedings of the XXXV Congreso Interamericano de Psicología, Lima, Peru, 12–16 July 2015. [Google Scholar]
- Sierra, J.C.; Arcos-Romero, A.I.; Granados, M.R.; Sánchez-Fuentes, M.M.; Calvillo, C.; Moyano, N. Escalas de Valoración de Excitación Sexual y Valoración de Sensaciones Genitales: Propiedades psicométricas en muestras españolas. Rev. Int. Androl. 2017, 15, 99–107. [Google Scholar] [CrossRef]
- Mosher, D.L. Multiple indicators of subjective sexual arousal. In Handbookof Sexuality-Related Measures; Fisher, T.D., Davis, C.M., Yarber, W.L., Davis, S.L., Eds.; Routledge: London, UK, 2011; pp. 59–61. [Google Scholar]
- Elliott, A.N.; O’Donohue, W.T. The effects of anxiety and distraction on sexual arousal in a nonclinical sample of heterosexual women. Arch. Sex. Behav. 1997, 26, 607–624. [Google Scholar] [CrossRef]
- Arcos-Romero, A.I.; Sierra, J.C. Factors associated with subjective orgasm experience in heterosexual relationships. J. Sex Marital Ther. 2020, 46, 314–329. [Google Scholar] [CrossRef]
- Carpenter, L.M.; Nathanson, C.A.; Kim, Y.J. Physical women, emotional men: Gender and sexual satisfaction in midlife. Arch. Sex. Behav. 2009, 38, 87–107. [Google Scholar] [CrossRef]
- Petersen, J.L.; Hyde, J.S. A meta-analytic review of research on gender differences in sexuality: 1993 to 2007. Psychol. Bull. 2010, 136, 21–38. [Google Scholar] [CrossRef]
- Nicolosi, A.; Laumann, E.O.; Glasser, D.B.; Moreira, E.D., Jr.; Paik, A.; Gingell, C. Sexual behavior and sexual dysfunctions after age 40: The global study of sexual attitudes and behaviors. Urology 2004, 64, 991–997. [Google Scholar] [CrossRef]
- Carvalho, J.; Nobre, P. Predictors of men’s sexual desire: The role of psychological, cognitive-emotional, relational, and medical factors. J. Sex Res. 2011, 48, 254–262. [Google Scholar] [CrossRef] [PubMed]
- Tutino, J.S.; Ouimet, A.J.; Shaughnessy, K. How do psychological risk factors predict sexual outcomes? A comparison of four models of young women’s sexual outcomes. J. Sex. Med. 2017, 14, 1232–1240. [Google Scholar] [CrossRef] [PubMed]
- Brotto, L.; Atallah, S.; Johnson-Agbakwu, C.; Rosenbaum, T.; Abdo, C.; Byers, E.S.; Graham, C.; Nobre, P.; Wylie, K. Psychological and interpersonal dimensions of sexual function and dysfunction. J. Sex. Med. 2016, 13, 538–571. [Google Scholar] [CrossRef] [PubMed]
- Nobre, P.J.; Pinto-Gouveia, J. Cognitive and emotional predictors of female sexual dysfunctions: Preliminary findings. J. Sex Marital Ther. 2008, 34, 325–342. [Google Scholar] [CrossRef]
- Domingo, S.; Kinzy, T.; Thompson, N.; Gales, S.; Stone, L.; Sullivan, A. Factors associated with sexual dysfunction in individuals with multiple sclerosis: Implications for assessment and treatment. Int. J. MS Care 2018, 20, 191–197. [Google Scholar] [CrossRef]
- Molina-Leyva, A.; Almodovar-Real, A.; Carrascosa, J.C.; Molina-Leyva, I.; Naranjo-Sintes, R.; Jimenez-Moleon, J.J. Distribution pattern of psoriasis, anxiety and depression as possible causes of sexual dysfunction in patients with moderate to severe psoriasis. An. Bras. Dermatol. 2015, 90, 338–345. [Google Scholar] [CrossRef]
- Gomes, A.L.Q.; Nobre, P. Personality traits and psychopathology on male sexual dysfunction: An empirical study. J. Sex. Med. 2011, 8, 461–469. [Google Scholar] [CrossRef]
- Arcos-Romero, A.I.; Sierra, J.C. Systematic review of the subjective experience of orgasm. Rev. Int. Androl. 2018, 16, 75–81. [Google Scholar] [CrossRef] [PubMed]
- Johannes, C.B.; Clayton, A.H.; Odom, D.M.; Rosen, R.C.; Russo, P.A.; Shifren, J.L.; Monz, B.U. Distressing sexual problems in United State women revisited: Prevalence after accounting for depression. J. Clin. Psychiatry 2009, 70, 1698–1706. [Google Scholar] [CrossRef] [PubMed]
- Malakouti, S.K.; Salehi, M.; Nojomi, M.; Zandi, T.; Eftekhar, M. Sexual functioning among the elderly population in Tehran, Iran. J. Sex. Marital Ther. 2012, 38, 365–377. [Google Scholar] [CrossRef] [PubMed]
- Corretti, G.; Baldi, I. The relationship between anxiety disorders and sexual dysfunction. Psychiatr. Times 2007, 24, 58–59. [Google Scholar]
- Theofilou, P.A. Sexual functioning in chronic kidney disease: The association with depression and anxiety. Hemodial. Internat. 2012, 16, 76–81. [Google Scholar] [CrossRef]
- Culha, M.G.; Tuken, M.; Gonultas, S.; Cakir, O.O.; Serefoglu, E.C. Frequency of etiological factors among patients with acquired premature ejaculation: Prospective, observational, single-center study. Int. J. Impot. Res. 2019, 32, 352–357. [Google Scholar] [CrossRef]
- Kane, L.; Dawson, S.J.; Shaughnessy, K.; Reissing, E.D.; Ouimet, A.J.; Ashbaugh, A.R. A review of experimental research on anxiety and sexual arousal: Implications for the treatment of sexual dysfunction using cognitive behavioral therapy. J. Exp. Psychopathol. 2019, 10, 1–24. [Google Scholar] [CrossRef]
- Liu, T.; Jia, C.J.; Peng, Y.; Zhong, W.; Fang, X. Correlation between premature ejaculation and psychological disorders in 270 Chinese outpatients. Psychiatry Res. 2019, 272, 69–72. [Google Scholar] [CrossRef] [PubMed]
- Sánchez-Fuentes, M.M.; Santos-Iglesias, P.; Sierra, J.C. A systematic review of sexual satisfaction. Int. J. Clin. Health Psychol. 2014, 14, 67–75. [Google Scholar] [CrossRef]
- Calvillo, C.; Sánchez-Fuentes, M.M.; Sierra, J.C. Revisión sistemática sobre la satisfacción sexual en parejas del mismo sexo [Systematic review of sexual satisfaction in same-sex couples]. Rev. Iberoam. Psicol. Salud 2018, 9, 115–136. [Google Scholar] [CrossRef]
- Rajkumar, R.P.; Kumaran, A.K. The association of anxiety with the subtypes of premature ejaculation: A chart review. Prim. Care Companion CNS Disord. 2014, 16. [Google Scholar] [CrossRef]
- Corona, G.; Mannucci, E.; Petrone, L.; Giommi, R.; Mansani, R.; Fei, L.; Forti, G.; Maggi, M. Psycho-biological correlates of hypoactive sexual desire in patients with erectile dysfunction. Int. J. Impot. Res. 2004, 16, 275–281. [Google Scholar] [CrossRef][Green Version]
- Hendrickx, L.; Gijs, L.; Enzlin, P. Age-related prevalence rates of sexual difficulties, sexual dysfunctions, and sexual distress in heterosexual women: Results from an online survey in Flanders. J. Sex. Med. 2015, 12, 424–435. [Google Scholar] [CrossRef]
- Koc, Z.; Saglam, Z. Determining the correlation between sexual satisfaction and loneliness levels in patients with hemodialysis in a Muslim community. Sex. Disabil. 2013, 31, 13–29. [Google Scholar] [CrossRef]
- Sánchez-Fuentes, M.M.; Sierra, J.C. Sexual satisfaction in a heterosexual and homosexual Spanish sample: The role of socio-demographic characteristics, health indicators, and relational factors. Sex. Relatsh. Ther. 2015, 30, 226–242. [Google Scholar] [CrossRef]
- Flynn, K.E.; Lin, L.; Bruner, D.W.; Cyranowski, J.M.; Hahn, E.A.; Jeffery, D.D.; Weinfurt, K.P. Sexual satisfaction and the importance of sexual health to quality of life throughout the life course of US adults. J. Sex. Med. 2016, 13, 1642–1650. [Google Scholar] [CrossRef]
- Scott, V.C.; Sandberg, J.G.; Harper, J.M.; Miller, R.B. The impact of depressive symptoms and health on sexual satisfaction for older couples: Implications for clinicians. Contemp. Fam. Ther. 2012, 34, 376–390. [Google Scholar] [CrossRef]
- Yazdanpanahi, Z.; Beygi, Z.; Akbarzadeh, M.; Zare, N. To investigate the relationship between stress, anxiety and depression with sexual function and its domains in women of reproductive age. Int. J. Med. Res. Health Sci. 2016, 5, 223–231. [Google Scholar]
- MacDonald, S.; Halliday, J.; MacEwan, T.; Sharkey, V.; Farrington, S.; Wall, S.; McCreadie, R.G. Nithsdale Schizophrenia Surveys 24: Sexual dysfunction: Case–control study. Br. J. Psychiatry 2003, 182, 50–56. [Google Scholar] [CrossRef] [PubMed]
- Álvarez-Muelas, A.; Gómez-Berrocal, C.; Sierra, J.C. Study of sexual satisfaction in different typologies of adherence to the sexual double standard. Front. Psychol. 2021, 11, 609571. [Google Scholar] [CrossRef]
- Sánchez-Fuentes, M.M.; Salinas, J.M.; Sierra, J.C. Use of an ecological model to study sexual satisfaction in a heterosexual Spanish sample. Arch. Sex. Behav. 2016, 45, 1973–1988. [Google Scholar] [CrossRef]
- Calvillo, C.; Sánchez-Fuentes, M.M.; Sierra, J.C. An explanatory model of sexual satisfaction in adults with a same-sex partner: An analysis based on gender differences. Int. J. Environ. Res. Public Health 2020, 17, 3393. [Google Scholar] [CrossRef] [PubMed]
- Feldman, H.A.; Goldstein, I.; Hatzichristou, D.G.; Krane, R.J.; McKinlay, J.B. Impotence and its medical and psychosocial correlates: Results of the Massachusetts Male Aging Study. J. Urol. 1994, 151, 54–61. [Google Scholar] [CrossRef]
- Bozman, A.W.; Beck, J.C. Covariation of sexual desire and sexual arousal: The effects with anger and anxiety. Arch. Sex. Behav. 1991, 20, 47–60. [Google Scholar] [CrossRef]
- Pérez, R. TOC y Sexualidad. Anu. Anxia 2014, 20, 38–46. [Google Scholar]
- Barlow, D.H. Causes of sexual dysfunction: The role of anxiety and cognitive interference. J. Consult. Clin. Psychol. 1986, 54, 140–148. [Google Scholar] [CrossRef]
- Arcos-Romero, A.I.; Calvillo, C.; Sánchez-Fuentes, M.M.; Granados, R.; Moyano, N.; Sierra, J.C. Relación entre ansiedad estado y excitación sexual [Poster]. In Proceedings of the VIII Congreso Internacional y XIII Nacional de Psicología Clínica, Granada, Spain, 9–22 November 2015. [Google Scholar]
- Dèttore, D.; Pucciarelli, M.; Santarnecchi, E. Anxiety and female sexual functioning: An empirical study. J. Sex Marital Ther. 2013, 39, 216–240. [Google Scholar] [CrossRef] [PubMed]
- Palace, E.M.; Gorzalka, B.B. The enhancing effects of anxiety on arousal in sexually dysfunctional and functional women. J. Abnorm. Psychol. 1990, 99, 403–411. [Google Scholar] [CrossRef] [PubMed]
- Handy, A.B.; Stanton, A.M.; Meston, C.M. Understanding women’s subjective sexual arousal within the laboratory: Definition, measurement, and manipulation. Sex. Med. Rev. 2018, 6, 201–216. [Google Scholar] [CrossRef]
- Calvillo, C.; Sánchez-Fuentes, M.M.; Parrón-Carreño, T.; Sierra, J.C. Validation of the Interpersonal Exchange Model of Sexual Satisfaction Questionnaire in adults with a same-sex partner. Int. J. Clin. Health Psychol. 2020, 20, 140–150. [Google Scholar] [CrossRef] [PubMed]
- Sánchez-Fuentes, M.M.; Santos-Iglesias, P. Sexual satisfaction in Spanish heterosexual couples: Testing the Interpersonal Exchange Model of Sexual. J. Sex Marital Ther. 2016, 42, 223–242. [Google Scholar] [CrossRef]
- Carosa, E.; Sansone, A.; Jannini, E.A. Management of endocrine disease: Female sexual dysfunction for the endocrinologist. Eur. J. Endocrinol. 2020, 182, R101–R116. [Google Scholar] [CrossRef]
- Sansone, A.; Romanelli, F.; Gianfrilli, D.; Lenzi, A. Endocrine evaluation of erectile dysfunction. Endocrine 2014, 46, 423–430. [Google Scholar] [CrossRef] [PubMed]
- Corona, G.; Sansone, A.; Pallotti, F.; Ferlin, A.; Pivonello, R.; Isidori, A.M.; Maggi, M.; Jannini, E.A. People smoke for nicotine, but lose sexual and reproductive health for tar: A narrative review on the effect of cigarette smoking on male sexuality and reproduction. J. Endocrinol. Investig. 2020, 43, 1391–1408. [Google Scholar] [CrossRef] [PubMed]
- Mollaioli, D.; Ciocca, G.; Limoncin, E.; Di Sante, S.; Gravina, G.L.; Carosa, E.; Lenzi, A.; Jannini, E.A. Lifestyles and sexuality in men and women: The gender perspective in sexual medicine. Reprod. Biol. Endocrinol. 2020, 18, 10. [Google Scholar] [CrossRef]
- Hald, G.M. Gender differences in pornography consumption among young heterosexual Danish adults. Arch. Sex. Behav. 2006, 35, 577–585. [Google Scholar] [CrossRef]
- Oliver, M.B.; Hyde, J.S. Gender differences in sexuality: A meta-analysis. Psychol. Bull. 1993, 114, 29–51. [Google Scholar] [CrossRef] [PubMed]
- Ghasemi, V.; Simbar, M.; Ozgoli, G.; Nabavi, S.M.; Majd, H.A. Prevalence, dimensions, and predictor factors of sexual dysfunction in women of Iran Multiple Sclerosis Society: A cross-sectional study. Neurol. Sci. 2020, 41, 1105–1113. [Google Scholar] [CrossRef] [PubMed]
- Malik, P.; Kemmler, G.; Hummer, M.; Riecher-Roessler, A.; Kahn, R.S.; Fleischhacker, W.W.; EUFEST Study Group. Sexual dysfunction in first-episode schizophrenia patients: Results from European First Episode Schizophrenia Trial. J. Clin. Psychopharmacol. 2011, 31, 274–280. [Google Scholar] [CrossRef] [PubMed]
- McMillan, E.; Sanchez, A.A.; Bhaduri, A.; Pehlivan, N.; Monson, K.; Badcock, P.; O’Donoghue, B. Sexual functioning and experiences in young people affected by mental health disorders. Psychiatry Res. 2017, 253, 249–255. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Variable | Men (n = 516) | Women (n = 700) | U/χ2 | Cohen′s d |
|---|---|---|---|---|
| M (SD)/n (%) | M (SD)/n (%) | |||
| Age | 22.14 (3.76) | 20.93 (3.05) | 143,573 * | 0.35 |
| Having a partner | ||||
| Yes | 227 (44%) | 409 (58%) | 26.92 * | 0.30 |
| No | 271 (53%) | 263 (38%) | ||
| Age of first sexual relationship | 16.42 (2.97) | 16.13 (1.74) | 137,149 * | 0.42 |
| Number of sexual partners | 8.3 (15.19) | 5.9 (8.52) | 147,527.50 * | 0.32 |
| Sexual orientation | ||||
| Heterosexual | 388 (75%) | 603 (86%) | 23.59 * | 0.14 |
| Non-heterosexual | 123 (24%) | 92 (13%) |
| Variables | Range | Men (n = 516) | Women (n = 700) | U | Cohen′s d |
|---|---|---|---|---|---|
| M (SD) | M (SD) | ||||
| Psychopathological dimensions | |||||
| Depression | 0–20 | 5.26 (3.92) | 5.36 (4.17) | 180,479.50 | |
| Hostility | 2.21 (2.63) | 2.26 (2.86) | 178,151.50 | ||
| Interpersonal sensitivity | 4.23 (3.57) | 4.78 (3.78) | 196,722 ** | 0.15 | |
| Somatization | 2.53 (2.70) | 3.09 (2.92) | 201,473.50 *** | 0.19 | |
| Anxiety | 3.65 (3.09) | 4.51 (3.42) | 208,000.50 *** | 0.26 | |
| Psychoticism | 1.47 (1.93) | 1.29 (1.75) | 173,687.50 | ||
| Obsession compulsion | 4.97 (3.62) | 5.17 (3.64) | 186,821.50 | ||
| Phobic anxiety | 1.22 (1.94) | 1.60 (2.41) | 195,165.50 * | 0.13 | |
| Paranoid ideation | 4.55 (3.37) | 4.58 (3.28) | 181,975 | ||
| Sexual functioning | |||||
| Desire | 0–4 | 3.38 (1.03) | 3.30 (1.08) | 173,448.50 | |
| Excitation | 3.63 (0.79) | 3.34 (1.04) | 154,256 *** | 0.25 | |
| Orgasm | 3.72 (0.72) | 3.22 (1.20) | 140,049 *** | 0.39 | |
| Satisfaction | 3.02 (1.25) | 3.01 (1.31) | 183,314.50 | ||
| Erection | 3.74 (0.62) |
| Men | Women | |||
|---|---|---|---|---|
| Sexual Orientation | Having a Partner | Sexual Orientation | Having a Partner | |
| Desire | 26,989.50 ** | 33,506.50 * | 30,389.00 | 58,918.50 * |
| Arousal | 26,048.00 * | 32,815.00 | 30,010.00 | 59,884.00 ** |
| Orgasm | 24,409.50 | 31,185.00 | 26,914.50 | 59,403.50 ** |
| Satisfaction | 25,854.00 | 37,498.00 *** | 27,696.50 | 71,892.00 *** |
| Erection | 23,569.00 | 31,939.00 | ||
| Variable | β | Std. Err | z-Value | R2 | χ2 | |
|---|---|---|---|---|---|---|
| Men | ||||||
| Desire | ||||||
| Somatization | −0.12 | 0.019 | −2.48 * | 0.074 | 34.14 *** | |
| Anxiety | −0.16 | 0.015 | −3.63 *** | |||
| Having a partner | 0.13 | 0.088 | 3.07 ** | |||
| Arousal | ||||||
| Anxiety | −0.22 | 0.013 | −4.44 *** | 0.058 | 21.51 *** | |
| Having a partner | 0.10 | 0.072 | 2.36 * | |||
| Orgasm | ||||||
| Psychoticism | −0.15 | 0.020 | −2.85 ** | 0.059 | 13.03 ** | |
| Phobic anxiety | −0.15 | 0.024 | −2.41 * | |||
| Satisfaction | ||||||
| Depression | −0.17 | 0.016 | −3.28 ** | 0.119 | 56.46 *** | |
| Phobic anxiety | −0.14 | 0.032 | −2.82 ** | |||
| Having a partner | 0.22 | 0.11 | 5.08 *** | |||
| Erection | ||||||
| Depression | −0.16 | 0.010 | −2.82 ** | 0.056 | 15.20 ** | |
| Hostility | 0.10 | 0.011 | 2.03 * | |||
| Paranoid ideation | −0.14 | 0.012 | −2.18 * | |||
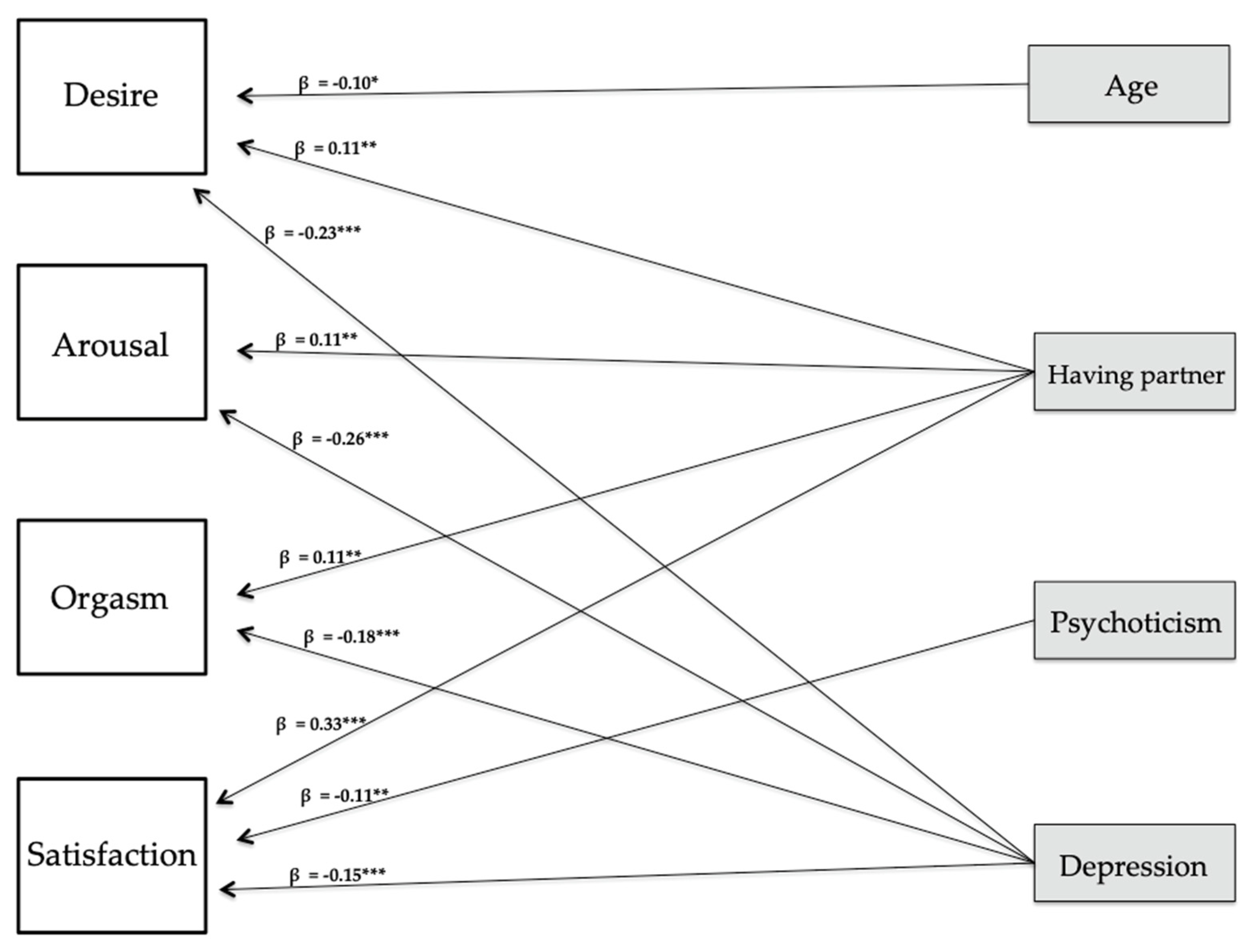
| Women | ||||||
| Desire | ||||||
| Depression | −0.23 | 0.011 | −5.74 *** | 0.073 | 40.42 *** | |
| Having a partner | 0.11 | 0.086 | 2.77 ** | |||
| Age | −0.10 | 0.017 | −2.06 * | |||
| Arousal | ||||||
| Depression | −0.26 | 0.010 | −6.42 *** | 0.086 | 41.40 *** | |
| Having a partner | 0.11 | 0.082 | 2.99 ** | |||
| Orgasm | ||||||
| Depression | −0.18 | 0.012 | −4.38 *** | 0.048 | 23.47 *** | |
| Having a partner | 0.11 | 0.096 | 2.80 ** | |||
| Satisfaction | ||||||
| Depression | −0.15 | 0.013 | −3.80 *** | 0.165 | 93.87 *** | |
| Psychoticism | −0.11 | 0.031 | −2.65 ** | |||
| Having a partner | 0.33 | 0.10 | 8.57 *** | |||
| Variable | Men (n = 123) | Women (n = 143) | U/χ2 | Cohen′s d |
|---|---|---|---|---|
| M (SD)/n (%) | M (SD)/n (%) | |||
| Age | 21.42 (2.67) | 20.51 (2.28) | 6998 * | 0.36 |
| Having a partner | ||||
| Yes | 50 (41%) | 94 (66%) | 20.85 * | 0.58 |
| No | 71 (58%) | 47 (33%) | ||
| Age of first sexual relationship | 16.68 (1.69) | 16.16 (1.44) | 6338 * | 0.50 |
| Number of sexual partners | 5.28 (6.63) | 5.15 (6.52) | 7937 |
| Variable | Range | Men (n = 123) | Women (n = 143) | U | Cohen′s d |
|---|---|---|---|---|---|
| M (SD) | M (SD) | ||||
| Psychopathological dimensions | |||||
| Depression | 0–20 | 4.68 (3.50) | 4.50 (3.29) | 8532.50 | |
| Hostility | 2.05 (2.54) | 2.06 (2.46) | 8906 | ||
| Interpersonal sensitivity | 3.27 (3.00) | 4.30 (3.28) | 10,472 ** | 0.33 | |
| Somatization | 2.28 (2.88) | 2.75 (3.17) | 9648.50 | ||
| Anxiety | 2.85 (2.64) | 3.93 (2.72) | 11,024 ** | 0.44 | |
| Psychoticism | 1.02 (1.40) | 1.03 (1.58) | 8550 | ||
| Obsessive compulsion | 4.54 (3.26) | 4.30 (3.14) | 8421 | ||
| Phobic anxiety | 0.70 (1.29) | 1.03 (1.69) | 9542 | ||
| Paranoid ideation | 4.37 (3.43) | 4.22 (2.88) | 8845 | ||
| Global score SA-45 | 0–180 | 25.76 (16.10) | 28.12 (17.62) | 9311.50 | |
| Sexual arousal | |||||
| Subjective sexual arousal | 1–35 | 18.30 (6.59) | 18.92 (5.47) | 9353.50 | |
| Assessment of genital sensations | 1–11 | 3.20 (1.46) | 3.55 (1.40) | 10,222 * | 0.28 |
| Variables | Β | Std. Err | z-Value | R2 | χ2 |
|---|---|---|---|---|---|
| Subjective sexual arousal | |||||
| Men | |||||
| Anxiety | 0.22 | 0.273 | 1.97 * | 0.029 | 4.26 |
| Women | |||||
| Anxiety | 0.16 | 0.151 | 2.11 * | 0.025 | 4.31 * |
| Assessment of genital sensations | |||||
| Men | |||||
| Anxiety | 0.25 | 0.069 | 1.98 * | 0.043 | 7.05 |
| Phobic anxiety | −0.14 | 0.075 | −2.10 * | ||
| Obsessive compulsion | −0.22 | 0.045 | −2.15 * |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Soler, F.; Granados, R.; Arcos-Romero, A.I.; Calvillo, C.; Álvarez-Muelas, A.; Sánchez-Fuentes, M.d.M.; Moyano, N.; Sierra, J.C. Association between Psychopathological Dimensions and Sexual Functioning/Sexual Arousal in Young Adults. Int. J. Environ. Res. Public Health 2021, 18, 3584. https://doi.org/10.3390/ijerph18073584
Soler F, Granados R, Arcos-Romero AI, Calvillo C, Álvarez-Muelas A, Sánchez-Fuentes MdM, Moyano N, Sierra JC. Association between Psychopathological Dimensions and Sexual Functioning/Sexual Arousal in Young Adults. International Journal of Environmental Research and Public Health. 2021; 18(7):3584. https://doi.org/10.3390/ijerph18073584
Chicago/Turabian StyleSoler, Franklin, Reina Granados, Ana I. Arcos-Romero, Cristóbal Calvillo, Ana Álvarez-Muelas, María del Mar Sánchez-Fuentes, Nieves Moyano, and Juan Carlos Sierra. 2021. "Association between Psychopathological Dimensions and Sexual Functioning/Sexual Arousal in Young Adults" International Journal of Environmental Research and Public Health 18, no. 7: 3584. https://doi.org/10.3390/ijerph18073584
APA StyleSoler, F., Granados, R., Arcos-Romero, A. I., Calvillo, C., Álvarez-Muelas, A., Sánchez-Fuentes, M. d. M., Moyano, N., & Sierra, J. C. (2021). Association between Psychopathological Dimensions and Sexual Functioning/Sexual Arousal in Young Adults. International Journal of Environmental Research and Public Health, 18(7), 3584. https://doi.org/10.3390/ijerph18073584