
Nurses’ Occupational Stress and Presenteeism: The Mediating Role of Public Service Motivation and the Moderating Role of Health

Abstract
1. Introduction
2. Material and Methods
2.1. Participants
2.2. Ethical Consideration
2.3. Measure Tools
2.4. Data Analysis
3. Results
3.1. Participant Characteristics
3.2. Correlation Matrix
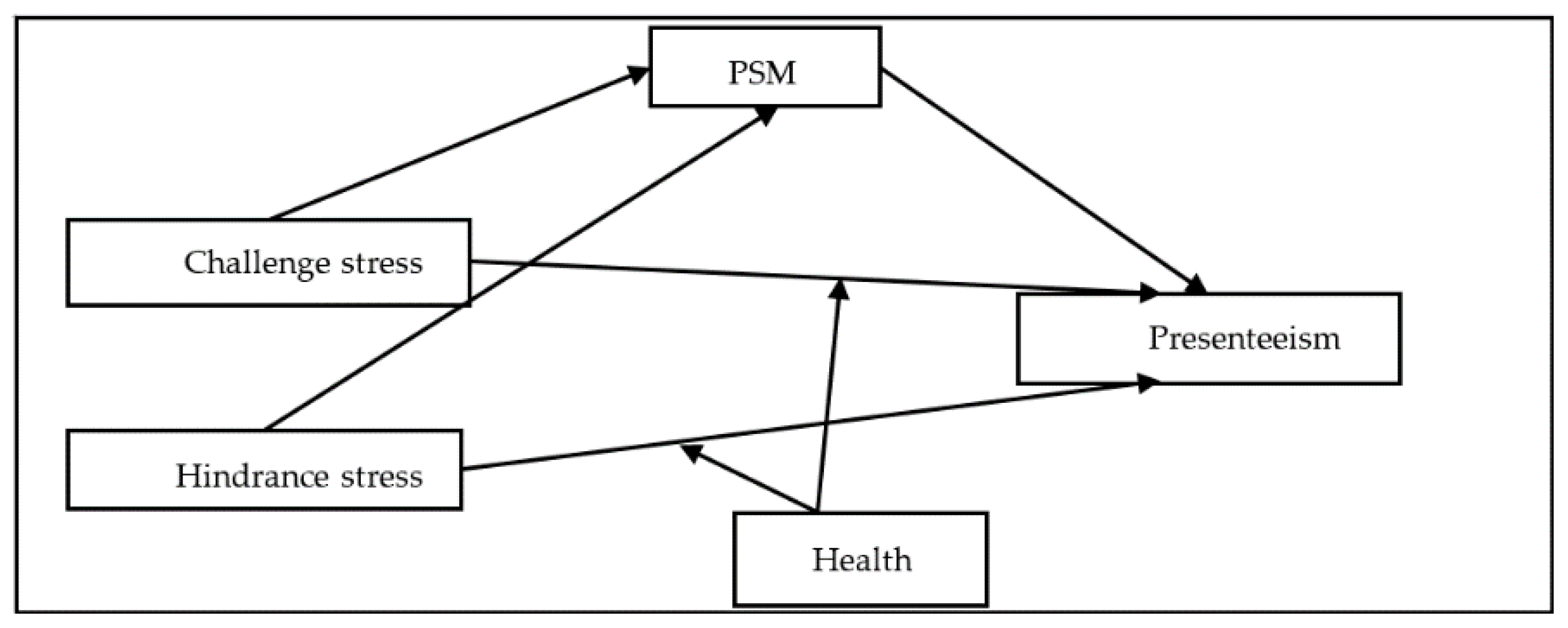
3.3. Testing for the Moderated Mediation Model
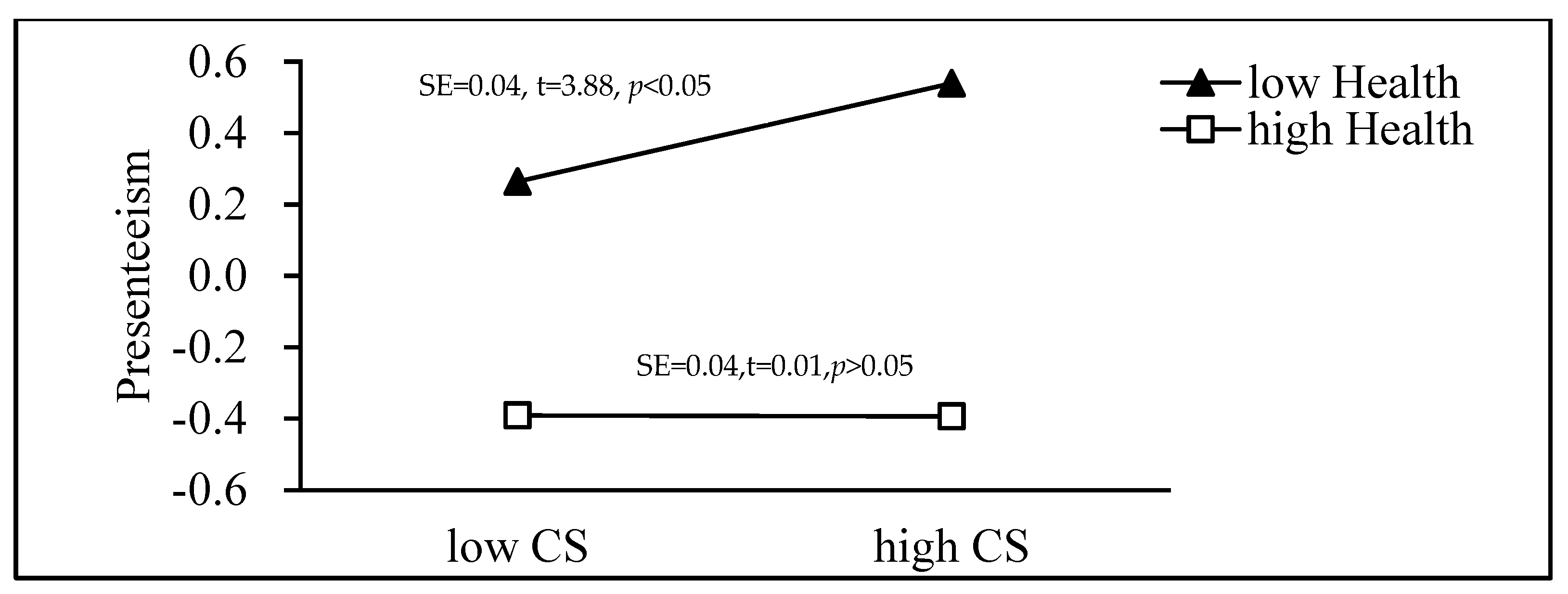
3.4. Simple Slope Analysis
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Burton, W.N.; Conti, D.J.; Chen, C.-Y.; Schultz, A.B.; Edington, D.W. The Role of Health Risk Factors and Disease on Worker Productivity. J. Occup. Environ. Med. 1999, 41, 863–877. [Google Scholar] [CrossRef]
- Aronsson, G.; Gustafsson, K.; Dallner, M. Sick but Yet at Work. An Empirical Study of Sickness Presenteeism. J. Epidemiol. Community Health 2000, 54, 502–509. [Google Scholar] [CrossRef]
- Johansson, G.; Lundberg, I. Adjustment Latitude and Attendance Requirements as Determinants of Sickness Absence or Attendance. Empirical Tests of the Illness Flexibility Model. Soc. Sci. Med. 2004, 58, 1857–1868. [Google Scholar] [CrossRef]
- Johns, G. Presenteeism in the Workplace: A Review and Research Agenda. J. Organ. Behav. 2009, 31, 519–542. [Google Scholar] [CrossRef]
- Evans-Lacko, S.; Knapp, M. Global Patterns of Workplace Productivity for People with Depression: Absenteeism and Presen-Teeism Costs Across Eight Diverse Countries. Soc. Psychiatry Psychiatr. Epidemiol. 2016, 51, 1525–1537. [Google Scholar] [CrossRef]
- Nagata, T.; Mori, K.; Ohtani, M.; Nagata, M.; Kajiki, S.; Fujino, Y.; Matsuda, S.; Loeppke, R. Total Health-Related Costs Due to Absenteeism, Presenteeism, and Medical and Pharmaceutical Expenses in Japanese Employers. J. Occup. Environ. Med. 2018, 60, e273–e280. [Google Scholar] [CrossRef]
- Warren, C.L.; White-Means, S.I.; Wicks, M.N.; Chang, C.F.; Gourley, D.; Rice, M. Cost Burden of the Presenteeism Health Outcome: Diverse Workforce of Nurses and Pharmacists. J. Occup. Environ. Med. 2011, 53, 90–99. [Google Scholar] [CrossRef]
- Shan, G.; Wang, S.; Wang, W.; Guo, S.; Li, Y. Presenteeism in Nurses: Prevalence, Consequences, and Causes from the Perspectives of Nurses and Chief Nurses. Front. Psychiatry 2021, 11, 584040. [Google Scholar] [CrossRef]
- Letvak, S.A.; Ruhm, C.J.; Gupta, S.N. Original Research: Nurses’ Presenteeism and Its Effects on Self-Reported Quality of Care and Costs. AJN Am. J. Nurs. 2012, 112, 30–38. [Google Scholar] [CrossRef] [PubMed]
- Martinez, L.F.; Ferreira, A.I. Sick at Work: Presenteeism among Nurses in a Portuguese Public Hospital. Stress Health 2011, 28, 297–304. [Google Scholar] [CrossRef] [PubMed]
- Ruggiero, J.S. Health, Work Variables, and Job Satisfaction among Nurses. JONA J. Nurs. Adm. 2005, 35, 254–263. [Google Scholar] [CrossRef] [PubMed]
- Motowidlo, S.J.; Packard, J.S.; Manning, M.R. Occupational Stress: Its Causes and Consequences for Job Performance. J. Appl. Psychol. 1986, 71, 618–629. [Google Scholar] [CrossRef]
- Milliken, T.F.; Clements, P.T.; Tillman, H.J. The Impact of Stress Management on Nurse Productivity and Retention. Nurs. Econ. 2007, 25. [Google Scholar]
- Elstad, J.I.; Vabø, M. Job Stress, Sickness Absence and Sickness Presenteeism in Nordic Elderly Care. Scand. J. Public Health 2008, 36, 467–474. [Google Scholar] [CrossRef] [PubMed]
- Chun, B.; Song, C. A Moderated Mediation Analysis of Occupational Stress, Presenteeism, and Turnover Intention among Occupational Therapists in Korea. J. Occup. Health 2020, 62, e12153. [Google Scholar] [CrossRef]
- Brunner, B.; Igic, I.; Keller, A.C.; Wieser, S. Who Gains the Most from Improving Working Conditions? Health-Related Absenteeism and Presenteeism Due to Stress at Work. Eur. J. Health Econ. 2019, 20, 1165–1180. [Google Scholar] [CrossRef] [PubMed]
- Webster, J.R.; Beehr, T.A.; Love, K. Extending the Challenge-Hindrance Model of Occupational Stress: The Role of Appraisal. J. Vocat. Behav. 2011, 79, 505–516. [Google Scholar] [CrossRef]
- Bergström, G.; Bodin, L.; Hagberg, J.; Lindh, T.; Aronsson, G.; Josephson, M. Does Sickness Presenteeism Have an Impact on Future General Health? Int. Arch. Occup. Environ. Health 2009, 82, 1179–1190. [Google Scholar] [CrossRef] [PubMed]
- Vandenabeele, W. Toward a Public Administration Theory of Public Service Motivation. Public Manag. Rev. 2007, 9, 545–556. [Google Scholar] [CrossRef]
- Wise, P.L.R. The Motivation Bases of Public Service. Public Adm. Rev. 1990, 50, 367–373. [Google Scholar]
- Lepine, J.A.; Podsakoff, N.P.; Lepine, M.A. A Meta-Analytic Test of the Challenge Stressor-Hindrance Stressor Framework: An Explanation for Inconsistent Relationships among Stressors and Performance. Acad. Manag. J. 2005, 48, 764–775. [Google Scholar] [CrossRef]
- De Simone, S.; Cicotto, G.; Pinna, R.; Giustiniano, L. Engaging Public Servants. Manag. Decis. 2016, 54, 1569–1594. [Google Scholar] [CrossRef]
- Boles, M.; Pelletier, B.; Lynch, W. The Relationship between Health Risks and Work Productivity. J. Occup. Environ. Med. 2004, 46, 737–745. [Google Scholar] [CrossRef]
- Yu, J.; Wang, S.; Yu, X. Health Risk Factors Associated with Presenteeism in a Chinese Enterprise. Occup. Med. 2015, 65, 732–738. [Google Scholar] [CrossRef] [PubMed]
- O’Donnell, M.P. Health and Productivity Management: The Concept, Impact, and Opportunity: Commentary to Goetzel and Ozminkowski. Am. J. Health Promot. 2000, 14, 215–217. [Google Scholar] [CrossRef]
- Zhai, X.; Wu, N.; Koriyama, S.; Wang, C.; Shi, M.; Huang, T.; Wang, K.; Sawada, S.S.; Fan, X. Mediating Effect of Perceived Stress on the Association between Physical Activity and Sleep Quality among Chinese College Students. Int. J. Environ. Res. Public Health 2021, 18, 289. [Google Scholar] [CrossRef]
- Buddeberg-Fischer, B.; Klaghofer, R.; Stamm, M.; Siegrist, J.; Buddeberg, C. Work Stress and Reduced Health in Young Physicians: Prospective Evidence from Swiss Residents. Int. Arch. Occup. Environ. Health 2008, 82, 31–38. [Google Scholar] [CrossRef]
- Cavanaugh, M.A.; Boswell, W.R.; Roehling, M.V.; Boudreau, J.W. An Empirical Examination of Self-Reported Work Stress among U.S. Managers. J. Appl. Psychol. 2000, 85, 65–74. [Google Scholar] [CrossRef]
- Yi, Z.; Zhan-Biao, S.; Li-Ying, Z.; Jian-Zhou, C.; Mei, F.; Jie, Y.; Xiu-Ling, G.U. Application of Challenge-and Hin-Drance-Related Self-Reported Stress Scale in Chinese Occupational People. Chin. Ment. Health J. 2013, 27, 384–388. [Google Scholar]
- Yang, T.; Guo, Y.; Ma, M.; Li, Y.; Tian, H.; Deng, J. Job Stress and Presenteeism among Chinese Healthcare Workers: The Mediating Effects of Affective Commitment. Int. J. Environ. Res. Public Health 2017, 14, 978. [Google Scholar] [CrossRef]
- Koopman, C.; Pelletier, K.R.; Murray, J.F.; Sharda, C.E.; Berger, M.L.; Turpin, R.S.; Hackleman, P.; Gibson, P.; Holmes, D.M.; Bendel, T. Stanford Presenteeism Scale: Health Status and Employee Productivity. J. Occup. Environ. Med. 2002, 44, 14–20. [Google Scholar] [CrossRef]
- Jiang, X.W.; Liu, J.N.; Liu, F.J.; Zheng, Z.J.; Chang, C. Reliability and Validity of Stanford Presenteeism Scale (SPS-6) in Chinese Occupational Population. Zhonghua Laodong Weisheng Zhiyebing Zazhi Chin. J. Ind. Hyg. Occup. Dis. 2020, 38, 898–902. [Google Scholar] [CrossRef]
- Kim, S. Individual-Level Factors and Organizational Performance in Government Organizations. J. Public Adm. Res. Theory 2004, 15, 245–261. [Google Scholar] [CrossRef]
- Perry, J.L. Measuring Public Service Motivation: An Assessment of Construct Reliability and Validity. J. Public Adm. Res. Theory 1996, 6, 5–22. [Google Scholar] [CrossRef]
- Coursey, D.; Yang, K.; Pandey, S.K. Public Service Motivation (PSM) and Support for Citizen Participation: A Test of Perry and Vandenabeele’s Reformulation of PSM Theory. Public Adm. Rev. 2012, 72, 572–582. [Google Scholar] [CrossRef]
- Turner-Bowker, D.M.; Bayliss, M.S.; Ware, J.E., Jr.; Kosinski, M. Usefulness of the SF-8™ Health Survey for comparing the impact of migraine and other conditions. Qual. Life Res. 2003, 12, 1003–1012. [Google Scholar] [CrossRef] [PubMed]
- Onagbiye, S.O.; Moss, S.J.; Cameron, M. Validity and Reliability of the Setswana Translation of the Short Form-8 Health-Related Quality of Life Health Survey in Adults. Health SA Gesondheid 2018, 23, 1092. [Google Scholar] [CrossRef] [PubMed]
- Hayes, A.F. Introduction to Mediation, Moderation, and Conditional Process Analysis: A Regression-Based Approach; Guilford Press: New York, NY, USA, 2013; p. 507. [Google Scholar]
- Hayes, A.F. Beyond Baron and Kenny: Statistical Mediation Analysis in the New Millennium. Commun. Monogr. 2009, 76, 408–420. [Google Scholar] [CrossRef]
- Liu, B.; Yang, K.; Yu, W. Work-Related Stressors and Health-Related Outcomes in Public Service: Examining the Role of Pub-lic Service Motivation. Am. Rev. Public Adm. 2015, 45, 653–673. [Google Scholar] [CrossRef]
- Deng, J.; Li, Y.; Sun, Y.; Lei, R.; Yang, T. Public Service Motivation as a Mediator of the Relationship between Job Stress and Presenteeism: A Cross-Sectional Study from Chinese Public Hospitals. BMC Health Serv. Res. 2019, 19, 1–8. [Google Scholar] [CrossRef]
- Gross, H.P.; Thaler, J.; Winter, V. Integrating Public Service Motivation in the Job-Demands-Resources Model: An Empirical Analysis to Explain Employees’ Performance, Absenteeism, and Presenteeism. Int. Public Manag. J. 2018, 22, 176–206. [Google Scholar] [CrossRef]
- Houston, D.J. Public-Service Motivation: A Multivariate Test. J. Public Adm. Res. Theory 2000, 10, 713–728. [Google Scholar] [CrossRef]
- Folkman, S. Stress: Appraisal and Coping. In Encyclopedia of Behavioral Medicine; Gellman, M.D., Turner, J.R., Eds.; Springer: New York, NY, USA, 2013; pp. 1913–1915. [Google Scholar] [CrossRef]
- Kinman, G.; Clements, A.J.; Hart, J. Job Demands, Resources and Mental Health in UK Prison Officers. Occup. Med. 2017, 67, 456–460. [Google Scholar] [CrossRef]
- Schultz, A.B.; Chen, C.; Edington, D.W. The Cost and Impact of Health Conditions on Presenteeism to Employers: A Review of the Literature. Pharm. Econ. 2009, 27, 365–378. [Google Scholar] [CrossRef] [PubMed]
- Podsakoff, N.P.; LePine, J.A.; LePine, M.A. Differential Challenge Stressor-Hindrance Stressor Relationships with Job Attitudes, Turnover Intentions, Turnover, and Withdrawal Behavior: A Meta-Analysis. J. Appl. Psychol. 2007, 92, 438–454. [Google Scholar] [CrossRef]
- Aronsson, G.; Gustafsson, K. Sickness Presenteeism: Prevalence, Attendance-Pressure Factors, and an Outline of a Model for Research. J. Occup. Environ. Med. 2005, 47, 958–966. [Google Scholar] [CrossRef] [PubMed]
- Bergström, G.; Bodin, L.; Hagberg, J.; Aronsson, G.; Josephson, M. Sickness Presenteeism Today, Sickness Absenteeism Tomorrow? A Prospective Study on Sickness Presenteeism and Future Sickness Absenteeism. J. Occup. Environ. Med. 2009, 51, 629–638. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Items | M ± SD/n(%) |
|---|---|
| Gender | |
| Male | 11(1.12) |
| Female | 970(98.88) |
| Age | 35.40 ± 8.31 |
| Marital status | |
| Unmarried | 174(17.74) |
| Married | 778(79.31) |
| Divorced or windowed | 29(2.96) |
| Education Level | |
| Senior high school and below | 425(43.32) |
| bachelor’s degree | 529(53.92) |
| postgraduate | 27(2.75) |
| Working years | 12.35 ± 8.89 |
| Working hours per day | |
| <8 h | 162(16.51) |
| 8~9 h | 661(67.38) |
| 9~10 h | 101(10.30) |
| >10 h | 57(5.81) |
| Variable | M ± SD | CS | HS | PSM | Health | Presenteeism |
|---|---|---|---|---|---|---|
| CS | 12.93 ± 5.08 | 1 | 0.61 ** | −0.29 ** | −0.49 ** | 0.34 ** |
| HS | 8.89 ± 3.69 | 1 | −0.34 ** | −0.49 ** | 0.48 ** | |
| PSM | 20.78 ± 3.39 | 1 | 0.321 ** | −0.42 ** | ||
| Health | 33.93 ± 4.77 | 1 | −0.52 ** | |||
| Presenteeism | 12.07 ± 4.80 | 1 |
| Equation | Predictors | Outcome | β | t | 95%CI | R2 | F | |
|---|---|---|---|---|---|---|---|---|
| Lower | Upper | |||||||
| Equation (1) | CS | PSM | −0.31 | −9.96 *** | −0.38 | −0.25 | 0.12 | 19.68 *** |
| Equation (2) | CS | Presenteeism | 0.07 | 2.22 * | 0.01 | 0.13 | 0.36 | 54.16 *** |
| PSM | −0.27 | −9.40 *** | −0.32 | −0.21 | ||||
| Health | −0.37 | −11.38 *** | −0.44 | −0.31 | ||||
| CS × Health | −0.07 | −2.86 ** | −0.12 | −0.02 | ||||
| Indirect effect | 0.08 | 0.06 | 0.11 | |||||
| Equation (3) | HS | PSM | −0.35 | −11.74 *** | −0.41 | −0.29 | 0.15 | 29.58 *** |
| Equation (4) | HS | Presenteeism | 0.21 | 6.92 *** | 0.15 | 0.27 | 0.39 | 69.92 *** |
| PSM | −0.23 | −8.27 *** | −0.28 | −0.17 | ||||
| Health | −0.31 | −9.96 *** | −0.37 | −0.25 | ||||
| HS × Health | −0.04 | −1.73 | −0.08 | 0.01 | ||||
| Indirect effect | 0.08 | 0.05 | 0.10 | |||||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Jiang, H.; Jia, H.; Zhang, J.; Li, Y.; Song, F.; Yu, X. Nurses’ Occupational Stress and Presenteeism: The Mediating Role of Public Service Motivation and the Moderating Role of Health. Int. J. Environ. Res. Public Health 2021, 18, 3523. https://doi.org/10.3390/ijerph18073523
Jiang H, Jia H, Zhang J, Li Y, Song F, Yu X. Nurses’ Occupational Stress and Presenteeism: The Mediating Role of Public Service Motivation and the Moderating Role of Health. International Journal of Environmental Research and Public Health. 2021; 18(7):3523. https://doi.org/10.3390/ijerph18073523
Chicago/Turabian StyleJiang, Hairui, Huanhuan Jia, Jingru Zhang, Yingying Li, Fangying Song, and Xihe Yu. 2021. "Nurses’ Occupational Stress and Presenteeism: The Mediating Role of Public Service Motivation and the Moderating Role of Health" International Journal of Environmental Research and Public Health 18, no. 7: 3523. https://doi.org/10.3390/ijerph18073523
APA StyleJiang, H., Jia, H., Zhang, J., Li, Y., Song, F., & Yu, X. (2021). Nurses’ Occupational Stress and Presenteeism: The Mediating Role of Public Service Motivation and the Moderating Role of Health. International Journal of Environmental Research and Public Health, 18(7), 3523. https://doi.org/10.3390/ijerph18073523