
A Scoping Review of the Health of African Immigrant and Refugee Children

 ,
,  ,
,  , , , ,
, , , ,  and
and
Abstract
1. Introduction
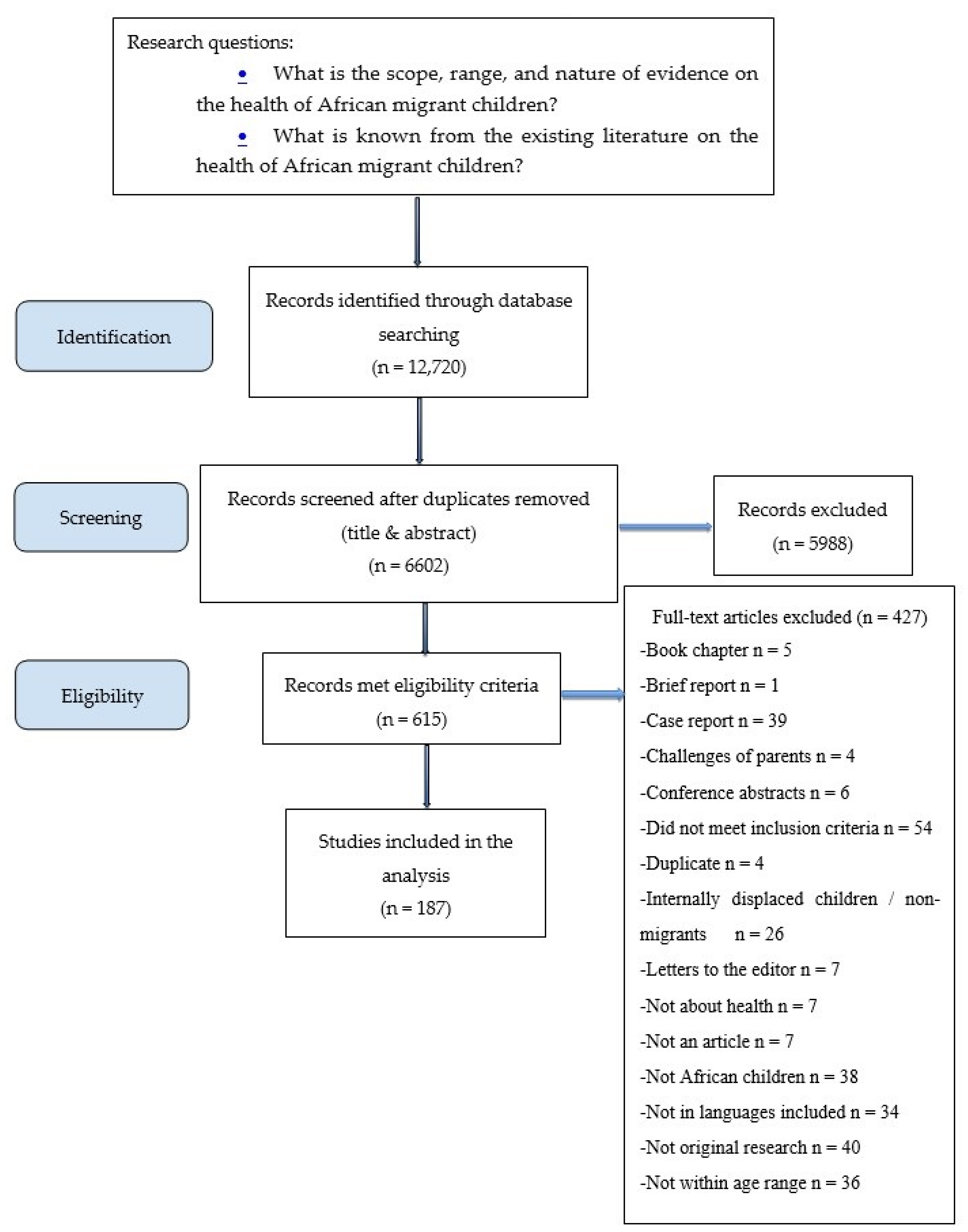
2. Materials and Methods
- What is the scope, range, and nature of evidence on the health of African migrant children?
- What is known from the existing literature on the health of African migrant children?
3. Results
3.1. Characteristics of Included Studies
3.2. Characteristics of Study Participants
3.3. Identified Themes
3.3.1. Infectious Diseases, Including Parasitic Infections
3.3.2. Nutrition
3.3.3. Mental Health
3.3.4. Birth Outcomes and Reproductive and Sexual Health
3.3.5. Physical and Developmental Health
3.3.6. Oral Health
3.3.7. Respiratory Health
3.3.8. Preventative Health
3.3.9. Endocrine Health
3.3.10. Health care Services
3.3.11. Haematological Conditions
4. Discussion
5. Conclusions
6. Limitations
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- International Organization for Migration. World Migration Report 2020; United Nations: Geneva, Switzerland, 2019. [Google Scholar]
- McDonald, J.T.; Kennedy, S. Insights into the ‘healthy immigrant effect’: Health status and health service use of immigrants to Canada. Soc. Sci. Med. 2004, 59, 1613–1627. [Google Scholar] [CrossRef] [PubMed]
- Kennedy, S.; Kidd, M.P.; McDonald, J.T.; Biddle, N. The healthy immigrant effect: Patterns and evidence from four countries. J. Int. Migr. Integr. 2015, 16, 317–332. [Google Scholar] [CrossRef]
- Lu, C.; Ng, E. Healthy immigrant effect by immigrant category in Canada. Health Rep. 2009, 30, 3–11. [Google Scholar] [CrossRef]
- Harker, K. Immigrant generation, assimilation, and adolescent psychological well-being. Soc. Forces 2001, 79, 969–1004. [Google Scholar] [CrossRef]
- Stevens, G.W.; Walsh, S.D.; Huijts, T.; Maes, M.; Madsen, K.R.; Cavallo, F.; Molcho, M. An internationally comparative study of immigration and adolescent emotional and behavioral problems: Effects of generation and gender. J. Adolesc. Health 2015, 57, 587–594. [Google Scholar] [CrossRef]
- Anderson, K.K.; Cheng, J.; Susser, E.; McKenzie, K.J.; Kurdyak, P. Incidence of psychotic disorders among first-generation immigrants and refugees in Ontario. Can. Med. Assoc. J. 2015, 187, E279–E286. [Google Scholar] [CrossRef]
- Omenka, O.I.; Watson, D.P.; Hendrie, H.C. Understanding the healthcare experiences and needs of African immigrants in the United States: A scoping review. BMC Public Health 2020, 20, 27. [Google Scholar] [CrossRef]
- Venters, H.; Gany, F. African immigrant health. J. Immigr. Minor. Health 2011, 13, 333–344. [Google Scholar] [CrossRef]
- Ahmed, S.; Rasmussen, A. Changes in social status and postmigration mental health among West African immigrants. Am. J. Orthopsychiatry 2020, 90, 171–180. [Google Scholar] [CrossRef]
- Woodgate, R.L.; Busolo, D.S.; Crockett, M.; Dean, R.A.; Armaladas, M.R.; Plourde, P.J. A qualitative study on African immigrant and refugee families’ experiences of accessing primary health care services in Manitoba, Canada: It’s not easy! Int. J. Equity Health 2017, 16, 5–17. [Google Scholar] [CrossRef]
- Migration Policy Institute. Sub-Saharan African Immigrants in the United States; Migration Policy Institute: Washington, DC, USA, 2019. [Google Scholar]
- Salami, B.; Yaskina, M.; Hegadoren, K.; Diaz, E.; Meherali, S.; Rammohan, A.; Ben-Shlomo, Y. Migration and social determinants of mental health: Results from the Canadian Health Measures Survey. Can. J. Public Health 2017, 108, 362–367. [Google Scholar] [CrossRef] [PubMed]
- Salami, B.; Hirani, S.; Meherali, S.; Amodu, O.; Chambers, T. Parenting practices of African immigrants in destination countries: A qualitative research synthesis. J. Pediatr. Nurs. 2017, 36, 30–40. [Google Scholar] [CrossRef] [PubMed]
- Hamilton, H.A.; Noh, S.; Adlaf, E.M. Adolescent risk behaviours and psychological distress across immigrant generations. Can. J. Public Health 2009, 100, 221–225. [Google Scholar] [CrossRef]
- Kwak, K. An evaluation of the healthy immigrant effect with adolescents in Canada: Examinations of gender and length of residence. Soc. Sci. Med. 2016, 157, 87–95. [Google Scholar] [CrossRef]
- Bronstein, I.; Montgomery, P. Psychological distress in refugee children: A systematic review. Clin. Child Fam. Psychol. Rev. 2011, 14, 44–56. [Google Scholar] [CrossRef]
- Crowley, C. The mental health needs of refugee children: A review of literature and implications for nurse practitioners. J. Am. Acad. Nurse Pract. 2009, 21, 322–331. [Google Scholar] [CrossRef] [PubMed]
- Lustig, S.L.; Kia-Keating, M.; Knight, W.G.; Geltman, P.; Ellis, H.; Kinzie, J.D.; Keane, T.; Saxe, G.N. Review of child and adolescent refugee mental health. J. Am. Acad. Child Adolesc. Psychiatry 2004, 43, 24–36. [Google Scholar] [CrossRef] [PubMed]
- Pieloch, K.A.; McCullough, M.B.; Marks, A.K. Resilience of children with refugee statuses: A research review. Can. Psychol./Psychol. Can. 2016, 57, 330–339. [Google Scholar] [CrossRef]
- Baauw, A.; Kist-van Holthe, J.; Slattery, B.; Heymans, M.; Chinapaw, M.; van Goudoever, H. Health needs of refugee children identified on arrival in reception countries: A systematic review and meta-analysis. BMJ Paediatr. Open 2019, 3, e000516. [Google Scholar] [CrossRef]
- Reza, M.; Amin, M.S.; Sgro, A.; Abdelaziz, A.; Ito, D.; Main, P.; Azarpazhooh, A. Oral health status of immigrant and refugee children in North America: A scoping review. J. Can. Dent. Assoc. 2016, 82, 1488–2159. [Google Scholar]
- Peters, M.D.; Godfrey, C.M.; Khalil, H.; McInerney, P.; Parker, D.; Soares, C.B. Guidance for conducting systematic scoping reviews. Int. J. Evid. Based Healthc. 2015, 13, 141–146. [Google Scholar] [CrossRef]
- Munn, Z.; Peters, M.D.J.; Stern, C.; Tufanaru, C.; McArthur, A.; Aromataris, E. Systematic review or scoping review? Guidance for authors when choosing between a systematic or scoping review approach. BMC Med. Res. Methodol. 2018, 18, 143. [Google Scholar] [CrossRef]
- Arksey, H.; O’Malley, L. Scoping studies: Towards a methodological framework. Int. J. Soc. Res. Methodol. 2005, 8, 19–32. [Google Scholar] [CrossRef]
- Tricco, A.C.; Lillie, E.; Zarin, W.; O’Brien, K.K.; Colquhoun, H.; Levac, D.; Moher, D.; Peters, M.D.J.; Horsley, T.; Weeks, L.; et al. PRISMA extension for scoping reviews (PRISMA-ScR): Checklist and explanation. Ann. Intern. Med. 2018, 169, 467–473. [Google Scholar] [CrossRef]
- Faustini, A.; Franco, E.; Saitto, C.; Cauletti, M.; Zaratti, L.; Papini, P.; Ahmed, A.; Zampieri, F.; Lerussi, A.; Panna, A.; et al. Hepatitis A, B, C and D in a community in Italy of immigrants from NE Africa. J. Public Health 1994, 16, 71–78. [Google Scholar] [CrossRef]
- Huerga, H.; López-Vélez, R. Infectious diseases in sub-Saharan African immigrant children in Madrid, Spain. Pediatr. Infect. Dis. J. 2002, 21, 830–834. [Google Scholar] [CrossRef] [PubMed]
- Javaloy, J.; Ferrer, C.; Vidal, M.T.; Alió, J.L. Follicular conjunctivitis caused by chlamydia trachomatis in an infant Saharan population: Molecular and clinical diagnosis. Br. J. Ophthalmol. 2003, 87, 142–146. [Google Scholar] [CrossRef] [PubMed]
- Nysse, L.J.; Pinsky, N.A.; Bratberg, J.P.; Babar-Weber, A.Y.; Samuel, T.T.; Krych, E.H.; Ziegler, A.; Jimale, M.A.; Vierkant, R.A.; Jacobson, R.M.; et al. Seroprevalence of antibody to varicella among Somali refugees. Mayo Clin. Proc. 2007, 82, 175–180. [Google Scholar] [CrossRef]
- Swerdlow, D.L.; Malenga, G.; Begkoyian, G.; Nyangulu, D.; Toole, M.; Waldma, R.J.; Puhr, D.N.; Tauxe, R.V. Epidemic cholera among refugees in Malawi, Africa: Treatment and transmission. Epidemiol. Infect. 1997, 118, 207–214. [Google Scholar] [CrossRef]
- Kouadio, I.K.; Koffi, A.K.; Attoh-Toure, H.; Kamigaki, T.; Oshitani, H. Outbreak of measles and rubella in refugee transit camps. Epidemiol. Infect. 2009, 137, 1593–1601. [Google Scholar] [CrossRef]
- Ndombo, P.K.; Ndze, V.N.; Mbarga, F.D.; Anderson, R.; Acho, A.; Ebua Chia, J.; Njamnshi, A.K.; Rota, P.A.; Waku-Kouomou, D. Molecular tilizationion of measles virus strains among refugees from Central African Republic in Cameroon in 2014. Epidemiol. Infect. 2018, 146, 319–323. [Google Scholar] [CrossRef]
- Cherian, S.; Forbes, D.A.; Cook, A.G.; Sanfilippo, F.M.; Kemna, E.H.J.M.; Swinkels, D.W.; Burgner, D.P. An insight into the relationships between hepcidin, anemia, infections and inflammatory cytokines in pediatric refugees: A cross-sectional study. PLoS ONE 2008, 3, e4030. [Google Scholar] [CrossRef]
- Cherian, S.; Forbes, D.; Sanfilippo, F.; Cook, A.; Burgner, D. The epidemiology of Helicobacter pylori infection in African refugee children resettled in Australia. Med. J. Aust. 2008, 189, 438–441. [Google Scholar] [CrossRef] [PubMed]
- Cherian, S.; Forbes, D.; Sanfilippo, F.; Cook, A.; Burgner, D. Helicobacter pylori, helminth infections and growth: A cross-sectional study in a high prevalence population. Acta Paediatr. 2009, 98, 860–864. [Google Scholar] [CrossRef] [PubMed]
- Cherian, S.; Burgner, D.P.; Cook, A.G.; Sanfilippo, F.M.; Forbes, D.A. Associations between helicobacter pylori infection, co-morbid infections, gastrointestinal symptoms, and circulating cytokines in African children. Helicobacter 2010, 15, 88–97. [Google Scholar] [CrossRef]
- Lamb, S.R.; Rademaker, M. Tinea due to trichophyton violaceum and trichophyton soudanense in Hamilton, New Zealand. Australas. J. Dermatol. 2001, 42, 260–263. [Google Scholar] [CrossRef]
- Mashiah, J.; Kutz, A.; Ami, R.B.; Savion, M.; Goldberg, I.; Or, T.G.; Zidan, O.; Sprecher, E.; Harel, A. Tinea capitis outbreak among paediatric refugee population, an evolving healthcare challenge. Mycoses 2016, 59, 553–557. [Google Scholar] [CrossRef] [PubMed]
- Cuetara, M.S.; Palacio, A.; Pereiro, M.; Amor, E.; Alvarez, C.; Noriega, A.R. Prevalence of undetected tinea capitis in a school survey in Spain. Mycoses 1997, 40, 131–137. [Google Scholar] [CrossRef]
- Cuetara, M.S.; Palacio, A.D.; Pereiro, M.; Noriega, A.R. Prevalence of undetected tinea capitis in a prospective school survey in Madrid: Emergence of new causative fungi. Br. J. Dermatol. 1998, 138, 658–660. [Google Scholar] [CrossRef] [PubMed]
- McPherson, M.E.; Woodgyer, A.J.; Simpson, K.; Chong, A.H. High prevalence of tinea capitis in newly arrived migrants at an English-language school, Melbourne, 2005. Med. J. Aust. 2008, 189, 13–16. [Google Scholar] [CrossRef]
- Grigoryan, K.V.; Tollefson, M.M.; Olson, M.A.; Newman, C.C. Pediatric tinea capitis caused by Trichophyton violaceum and Trichophyton soudanense in Rochester, Minnesota, United States. Int. J. Dermatol. 2018, 58, 912–915. [Google Scholar] [CrossRef]
- Hällgren, J.; Petrini, B.; Wahlgren, C. Increasing tinea capitis prevalence in Stockholm reflects immigration. Med. Mycol. 2004, 42, 505–509. [Google Scholar] [CrossRef] [PubMed]
- Agmon-Levin, N.; Elbirt, D.; Asher, I.; Torten, D.; Cohen, Y.; Gradestein, S.; Werner, B.; Turner, D.; Chowers, M.; Gotteseman, G.; et al. Prevention of human immunodeficiency virus mother–to–child transmission in Israel. Int. J. STD AIDS 2009, 20, 473–476. [Google Scholar] [CrossRef]
- Asander, A.S.; Björkman, A.; Belfrage, E.; Faxelid, E. HIV-infected African parents living in Stockholm, Sweden: Disclosure and planning for their children’s future. Health Soc. Work 2009, 34, 107–115. [Google Scholar] [CrossRef] [PubMed]
- Cohen, S.; Bilsen, W.P.; van Smit, C.; Fraaij, P.L.; Warris, A.; Kuijpers, T.W.; Geelen, S.; Worlfs, T.; Scherpbrier, H.; van Rossum, A.; et al. Country of birth does not influence long-term clinical, virologic, and immunological outcome of HIV-infected children living in the Netherlands: A cohort study comparing children born in the Netherlands with children born in Sub-Saharan Africa. J. Acquir. Immune Defic. Syndr. 2015, 68, 178–185. [Google Scholar] [CrossRef] [PubMed]
- Feiterna-Sperling, C.; Königs, C.; Notheis, G.; Buchholz, B.; Krüger, R.; Weizsäcker, K.; Eberle, J.; Hanhoff, N.; Gartner, B.; Heider, H.; et al. High seroprevalence of antibodies against Kaposi’s sarcoma-associated herpesvirus (KSHV) among HIV-1-infected children and adolescents in a non-ethnic population. Med. Microbiol. Immunol. 2016, 205, 425–434. [Google Scholar] [CrossRef]
- Irova, T.; Burtonboy, G.; Ninane, J. HIV infection in children born before and after immigration to Belgium. J. Travel Med. 1995, 2, 169–173. [Google Scholar] [CrossRef][Green Version]
- Nesheim, S.; Linley, L.; Gray, K.; Zhang, T.; Shi, J.; Lampe, M.; FitzHarris, L.F. Country of birth of children with diagnosed HIV infection in the United States, 2008–2014. J. Acquir. Immune Defic. Syndr. 2018, 77, 23–30. [Google Scholar] [CrossRef]
- Neubert, J.; Michalsky, N.; Laws, H.J.; Borkhardt, A.; Jensen, B.; Lübke, N. HIV-1 Subtype diversity and prevalence of primary drug resistance in a single-center pediatric cohort in Germany. Intervirology 2017, 59, 301–306. [Google Scholar] [CrossRef]
- Arnáez, J.; Roa, M.A.; Albert, L.; Cogollos, R.; Rubio, J.M.; Villares, R.; Alarabe, A.; Cervera, A.; Lopez-Velez, R. Imported malaria in children: A comparative study between recent immigrants and immigrant travelers (VFRs). J. Travel Med. 2010, 17, 221–227. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Asch, A.J. Malaria at the Hospital for Sick Children, Toronto. CMAJ Can. Med. Assoc. J. 1976, 115, 405–406. [Google Scholar]
- Wolday, D.; Kibreab, T.; Bukenya, D.; Kodes, R. Sensitivity of Plasmodium falciparum in vivo to chloroquine and pyrimethamine-sulfadoxine in Rwandan patients in a refugee camp in Zaire. Trans. R. Soc. Trop. Med. Hyg. 1995, 89, 654–656. [Google Scholar] [CrossRef]
- Cherian, S.; Burgner, D. Selective ambulatory management of plasmodium falciparum malaria in paediatric refugees. Arch. Dis. Child. 2007, 92, 983–986. [Google Scholar] [CrossRef][Green Version]
- Depoortere, E.; Guthmann, J.; Sipilanyambe, N.; Nkandu, E.; Fermon, F.; Balkan, S.; Legros, D. Adherence to the combination of sulphadoxine–pyrimethamine and artesunate in the Maheba refugee settlement, Zambia. Trop. Med. Int. Health 2004, 9, 62–67. [Google Scholar] [CrossRef] [PubMed]
- Lavoie, P.M.; Carceller, A.; Robert, M.; Lebel, M.H.; Moore, D.L.; Rashed, S. Malaria in immigrant and traveler children: Clinical presentation and risk factors for complications. J. Pediatr. Infect. Dis. 2006, 1, 29–37. [Google Scholar] [CrossRef]
- Williams, J.P.; Chitre, M.; Sharland, M. Increasing Plasmodium falciparum malaria in southwest London: A 25 year observational study. Arch. Dis. Child. 2002, 86, 428–430. [Google Scholar] [CrossRef] [PubMed]
- Thompson, R.G.; Hutchison, J.G.; Johnston, N.M. Survey of intestinal pathogens from immigrant children. BMJ 1972, 1, 591–594. [Google Scholar] [CrossRef][Green Version]
- Goel, K.M.; Logan, R.W.; House, F.; Connell, M.D.; Strevens, E.; Watson, W.H.; Bulloch, C.B. The prevalence of haemoglobinopathies, nutritional iron and folate deficiencies in native and immigrant children in Glasgow. Health Bull. 1978, 36, 176–183. [Google Scholar]
- Geltman, P.L.; Radin, M.; Zhang, Z.; Cochran, J.; Meyers, A.F. Growth status and related medical conditions among refugee children in Massachusetts, 1995–1998. Am. J. Public Health 2001, 91, 1800–1805. [Google Scholar] [CrossRef]
- Belhassen-García, M.; Pardo-Lledias, J.; Pérez del Villar, L.; Muro, A.; Velasco-Tirado, V.; Muñoz Bellido, J.L.; Vicente, B.; Blazquez de Castro, A.; Cordero-Sanchez, M. Should parasitic disease be investigated in immigrant children with relative eosinophilia from tropical and sub-tropical regions? Paediatr. Int. Child Health 2017, 37, 42–45. [Google Scholar] [CrossRef] [PubMed]
- Rice, J.E.; Skull, S.A.; Pearce, C.; Mulholland, N.; Davie, G.; Carapetis, J.R. Screening for intestinal parasites in recently arrived children from east Africa. J. Paediatr. Child Health 2003, 39, 456–459. [Google Scholar] [CrossRef] [PubMed]
- Mumcuoglu, K.Y.; Miller, J.; Manor, O.; Ben-Yshai, F.; Klaus, S. The prevalence of ectoparasites in Ethiopian immigrants. Isr. J. Med. Sci. 1993, 29, 371–373. [Google Scholar] [CrossRef] [PubMed]
- Shah, A.; Suchdev, P.; Mitchell, T.; Shetty, S.; Warner, C.; Oladele, A.; Reines, S. Nutritional status of refugee children entering DeKalb County, Georgia. J. Immigr. Minor. Health 2014, 16, 959–967. [Google Scholar] [CrossRef]
- Wandel, M.; Terragni, L.; Nguyen, C.; Lyngstad, J.; Amundsen, M.; de Paoli, M. Breastfeeding among Somali mothers living in Norway: Attitudes, practices and challenges. Women Birth 2016, 29, 487–493. [Google Scholar] [CrossRef]
- Grewal, N.K.; Andersen, L.F.; Sellen, D.; Mosdøl, A.; Torheim, L.E. Breast-feeding and complementary feeding practices in the first 6 months of life among Norwegian-Somali and Norwegian-Iraqi infants: The InnBaKost survey. Public Health Nutr. 2016, 19, 703–715. [Google Scholar] [CrossRef] [PubMed]
- Tyler, L.; Kirby, R.; Rogers, C. Infant feeding practices among Sudanese women now living in regional south east Queensland, Australia. Breastfeed. Rev. 2014, 22, 13–19. [Google Scholar]
- Woldeghebriel, M.; Hromi-Fiedler, A.; Lartey, A.; Gallego-Perez, D.; Sandow, A.; Pérez-Escamilla, R. Length of time in Ghana is associated with the likelihood of exclusive breastfeeding among Liberian refugees living in Buduburam. Matern. Child Nutr. 2017, 13, e12363. [Google Scholar] [CrossRef]
- Aakre, I.; Strand, T.A.; Bjøro, T.; Norheim, I.; Barikmo, I.; Ares, S.; Alcorta, M.D.; Henjum, S. Thyroid function among breastfed children with chronically excessive iodine intakes. Nutrients 2016, 8, 398. [Google Scholar] [CrossRef]
- Aakre, I.; Lilleengen, A.M.; Lerseth Aarsand, M.; Strand, T.A.; Barikmo, I.; Henjum, S. Infant feeding practices in the Saharawi refugee camps Algeria, a cross-sectional study among children from birth to six months of age. Int. Breastfeed. J. 2016, 12, 8. [Google Scholar] [CrossRef]
- Montero, M.D.P.; Mora-Urda, A.I.; Anzid, K.; Cherkaoui, M.; Marrodan, M.D. Diet quality of Moroccan adolescents living in Morocco and in Spain. J. Biosoc. Sci. 2017, 49, 173–186. [Google Scholar] [CrossRef]
- Rätsch, I.M.; Catassi, C. Coeliac disease: A potentially treatable health problem of Saharawi refugee children. Bull. World Health Organ. 2001, 79, 542–545. [Google Scholar]
- Toselli, S.; Zaccagni, L.; Celenza, F.; Albertini, A.; Gualdi-Russo, E. Risk factors of overweight and obesity among preschool children with different ethnic background. Endocrine 2015, 49, 717–725. [Google Scholar] [CrossRef]
- Grewal, N.K.; Andersen, L.F.; Kolve, C.S.; Kverndalen, I.; Torheim, L.E. Food and nutrient intake among 12-month-old Norwegian-Somali and Norwegian-Iraqi infants. Nutrients 2016, 8, 602. [Google Scholar] [CrossRef] [PubMed]
- Mescher-Benbenek, M.; Garwick, A.W. Enablers and barriers to dietary practices contributing to bone health among early adolescent Somali girls living in Minnesota. J. Spec. Pediatr. Nurs. 2012, 17, 205–214. [Google Scholar] [CrossRef]
- Dharod, J.M.; Croom, J.E. Child hunger: Its prevalence and association with body mass index and dietary intake among Somali refugee children in the United States. NAPA Bull. 2010, 34, 126–140. [Google Scholar] [CrossRef]
- Hadley, C.; Sellen, D. Food security and child hunger among recently resettled Liberian refugees and asylum seekers: A pilot study. J. Immigr. Minor. Health 2006, 8, 369–375. [Google Scholar] [CrossRef] [PubMed]
- Mulugeta, W.; Glick, M.; Min, J.; Xue, H.; Noe, F.N.; Wang, Y. Longitudinal changes and high-risk subgroups for obesity and overweight/obesity among refugees in Buffalo, NY, 2004–2014. J. Racial Ethn. Health Dispar. 2018, 5, 187–194. [Google Scholar] [CrossRef]
- Renzaho, A.M.N.; Swinburn, B.; Burns, C. Maintenance of traditional cultural orientation is associated with lower rates of obesity and sedentary behaviours among African migrant children to Australia. Int. J. Obes. 2008, 32, 594–600. [Google Scholar] [CrossRef]
- Renzaho, A.M.N.; Gibbons, C.; Swinburn, B.; Jolley, D.; Burns, C. Obesity and undernutrition in sub-Saharan African immigrant and refugee children in Victoria, Australia. Asia Pac. J. Clin. Nutr. 2006, 15, 482–490. [Google Scholar] [PubMed]
- Stellinga-Boelen, A.; Storm, H.; Wiegersma, P.; Bijleveld, C.; Verkade, H. Iron deficiency among children of asylum seekers in the Netherlands. J. Pediatr. Gastroenterol. Nutr. 2007, 45, 591–595. [Google Scholar] [CrossRef]
- Kaufman-Shriqui, V.; Fraser, D.; Friger, M.; Bilenko, N.; Vardi, H.; Abu-Saad, K.; Elhadad, N.; Mor, K.; Feine, Z.; Shahar, D.R. Factors associated with childhood overweight and obesity among acculturated and new immigrants. Ethn. Dis. 2013, 23, 329–335. [Google Scholar]
- Hintzpeter, B.; Scheidt-Nave, C.; Müller, M.J.; Schenk, L.; Mensink, G.B.M. Higher prevalence of vitamin d deficiency is associated with immigrant background among children and adolescents in Germany. J. Nutr. 2008, 138, 1482–1490. [Google Scholar] [CrossRef]
- McGillivray, G.; Skull, S.A.; Davie, G.; Kofoed, S.E.; Frydenberg, A.; Rice, J.; Cooke, R.; Carapetis, J. High prevalence of asymptomatic vitamin D and iron deficiency in east African immigrant children and adolescents living in a temperate climate. Arch. Dis. Child. 2007, 92, 1088–1093. [Google Scholar] [CrossRef]
- Sheikh, M.; Wang, S.; Pal, A.; MacIntyre, C.R.; Wood, N.; Gunesekera, H. Vitamin D deficiency in refugee children from conflict zones. J. Immigr. Minor. Health 2011, 13, 87–93. [Google Scholar] [CrossRef]
- Beukeboom, C.; Arya, N. Prevalence of nutritional deficiencies among populations of newly arriving government assisted refugee children to Kitchener/Waterloo, Ontario, Canada. J. Immigr. Minor. Health 2018, 20, 1317–1323. [Google Scholar] [CrossRef]
- Khayri, H.O.; Munee, S.E.; Ahmed, S.B.; Osman, M.A.; Babiker, E.E. Assessment of the nutritional status of Sudanese primary school pupils in Riyadh City, Kingdom of Saudi Arabia. J. Immigr. Minor. Health 2016, 18, 28–33. [Google Scholar] [CrossRef]
- Bern, C.; Nathanail, L. Is mid-upper-arm circumference a useful tool for screening in emergency settings? J. Immigr. Minor. Health 1995, 345, 631–633. [Google Scholar] [CrossRef]
- Reifen, R.; Haftel, L.; Manor, G.; Sklan, D.; Edris, M.; Khoshoo, V.; Ghebremeskel, K. Ethiopian-born and native Israeli school children have different growth patterns. Nutrition 2003, 19, 427–431. [Google Scholar] [CrossRef]
- Polonsky, J.A.; Ronsse, A.; Ciglenecki, I.; Rull, M.; Porten, K. High levels of mortality, malnutrition, and measles, among recently-displaced Somali refugees in Dagahaley camp, Dadaab refugee camp complex, Kenya. Confl. Health 2013, 7, 1. [Google Scholar] [CrossRef] [PubMed]
- Seal, A.J.; Creeke, P.I.; Mirghani, Z.; Abdalla, F.; McBurney, R.P.; Pratt, L.S.; Brookes, D.; Ruth, L.J.; Machand, E. Iron and vitamin A deficiency in long-term African refugees. J. Nutr. 2005, 135, 808–813. [Google Scholar] [CrossRef]
- Tumwine, J.K.; Obala, A.A. Nutrition status of children in Kasese district at the Uganda–Congo border. East Afr. Med. J. 2002, 79, 427–434. [Google Scholar] [CrossRef] [PubMed]
- Renzaho, A.M.N.; Halliday, J.A.; Mellor, D.; Green, J. The healthy migrant families initiative: Development of a culturally competent obesity prevention intervention for African migrants. BMC Public Health 2015, 15, 272. [Google Scholar] [CrossRef]
- Tondeur, M.C.; Salse, U.N.; Wilkinson, C.; Spiegel, P.; Seal, A.J. Rapid acceptability and adherence testing of a lipid-based nutrient supplement and a micronutrient powder among refugee children and pregnant and lactating women in Algeria. Public Health Nutr. 2016, 19, 1852–1861. [Google Scholar] [CrossRef]
- Lopriore, C.; Guidoum, Y.; Briend, A.; Branca, F. Spread fortified with vitamins and minerals induces catch-up growth and eradicates severe anemia in stunted refugee children aged 3–6 y. Am. J. Clin. Nutr. 2004, 80, 973–981. [Google Scholar] [CrossRef] [PubMed]
- Seal, A.; Kafwembe, E.; Kassim, I.A.; Hong, M.; Wesley, A.; Wood, J.; Abdalla, F.; van den Briel, T. Maize meal fortification is associated with improved vitamin A and iron status in adolescents and reduced childhood anaemia in a food aid-dependent refugee population. Public Health Nutr. 2008, 11, 720–728. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Taylor, W.R. An evaluation of supplementary feeding in Somali refugee camps. Int. J. Epidemiol. 1983, 12, 433–436. [Google Scholar] [CrossRef] [PubMed]
- Ndemwa, P.; Klotz, C.L.; Mwaniki, D.; Sun, K.; Muniu, E.; Andango, P.; Owigar, J.; Rah, J.H.; Kraemer, K.; Spiegel, P.B.; et al. Relationship of the availability of micronutrient powder with iron status and hemoglobin among women and children in the Kakuma Refugee Camp, Kenya. Food Nutr. Bull. 2011, 32, 286–291. [Google Scholar] [CrossRef]
- Renzaho, A.; Renzaho, C. In the shadow of the volcanoes: The impact of intervention on the nutrition and health status of Rwandan refugee children in Zaire two years on from the exodus. Nutr. Diet 2003, 60, 85–91. [Google Scholar]
- Aakre, I.; Henjum, S.; Folven Gjengedal, E.L.; Haugstad, C.R.; Vollset, M.; Moubarak, K.; Ahmed, T.S.; Alexander, J.; Kjellevoid, M.; Molin, M. Trace element concentrations in drinking water and urine among Saharawi women and young children. Toxics 2018, 6, 40. [Google Scholar] [CrossRef] [PubMed]
- Dawson-Hahn, E.E.; Pak-Gorstein, S.; Hoopes, A.J.; Matheson, J. Comparison of the nutritional status of overseas refugee children with low income children in Washington State. PLoS ONE 2016, 11, e0147854. [Google Scholar] [CrossRef]
- Ercolini, D.; Francavilla, R.; Vannini, L.; De Filippis, F.; Capriati, T.; Di Cagno, R.; Lacono, G.; De Angelis, M.; Gobbetti, M. From an imbalance to a new imbalance: Italian-style gluten-free diet alters the salivary microbiota and metabolome of African celiac children. Sci. Rep. 2015, 5, 18571. [Google Scholar] [CrossRef] [PubMed]
- Paardekooper, B.; de Jong, J.T.V.M.; Hermanns, J.M.A. The psychological impact of war and the refugee situation on south Sudanese children in refugee camps in Northern Uganda: An exploratory study. J. Child Psychol. Psychiatry 1999, 40, 529–536. [Google Scholar] [CrossRef]
- Peltzer, K. Trauma and mental health problems of Sudanese refugees in Uganda. Cent. Afr. J. Med. 1999, 45, 110–114. [Google Scholar] [CrossRef]
- Völkl-Kernstock, S.; Völkl-Kernstock, S.; Karnik, N.; Karnik, N.; Mitterer-Asadi, M.; Mitterer-Asadi, M. Responses to conflict, family loss and flight: Posttraumatic stress disorder among unaccompanied refugee minors from Africa. Neuropsychiatry 2014, 28, 6–11. [Google Scholar] [CrossRef] [PubMed]
- Aviad-Wilchek, Y.; Levy, I.; Ben-David, S. Readiness to use psychoactive substances among second-generation adolescent immigrants and perceptions of parental immigration-related trauma. Subst. Use Misuse 2017, 52, 1646–1655. [Google Scholar] [CrossRef] [PubMed]
- Walsh, S.D.; Edelstein, A.; Vota, D. Suicidal ideation and alcohol use among Ethiopian adolescents in Israel. Eur. Psychol. 2012, 17, 131–142. [Google Scholar] [CrossRef]
- Wilchek-Aviad, Y. Meaning in life and suicidal tendency among immigrant (Ethiopian) youth and native-born Israeli Youth. J. Immigr. Minor. Health 2015, 17, 1041–1048. [Google Scholar] [CrossRef] [PubMed]
- Meyer, S.R.; Steinhaus, M.; Bangirana, C.; Onyango-Mangen, P.; Stark, L. The influence of caregiver depression on adolescent mental health outcomes: Findings from refugee settlements in Uganda. BMC Psychiatry 2017, 17, 405. [Google Scholar] [CrossRef]
- Meyer, S.R.; Meyer, E.; Bangirana, C.; Mangen, P.O.; Stark, L. Protection and well-being of adolescent refugees in the context of a humanitarian crisis: Perceptions from South Sudanese refugees in Uganda. Soc. Sci. Med. 2019, 221, 79–86. [Google Scholar] [CrossRef] [PubMed]
- Jensen, T.K.; Fjermestad, K.W.; Granly, L.; Wilhelmsen, N.H. Stressful life experiences and mental health problems among unaccompanied asylum-seeking children. Clin. Child Psychol. Psychiatry 2015, 20, 106–116. [Google Scholar] [CrossRef]
- Zwi, K.; Woodland, L.; Williams, K.; Palasanthiran, P.; Rungan, S.; Jaffe, A.; Woolfenden, S. Protective factors for social-emotional well-being of refugee children in the first three years of settlement in Australia. Arch. Dis. Child. 2018, 103, 261–268. [Google Scholar] [CrossRef] [PubMed]
- Stevens, G.W.J.M.; Thijs, J. Perceived group discrimination and psychological well-being in ethnic minority adolescents. J. Appl. Soc. Psychol. 2018, 48, 559–570. [Google Scholar] [CrossRef]
- Beiser, M.; Taa, B.; Fenta-Wube, H.; Baheretibeb, Y.; Pain, C.; Araya, M. A comparison of levels and predictors of emotional problems among preadolescent Ethiopians in Addis Ababa, Ethiopia, and Toronto, Canada. Transcult. Psychiatry 2012, 49, 651–677. [Google Scholar] [CrossRef]
- Astell-Burt, T.; Maynard, M.J.; Lenguerrand, E.; Harding, S. Racism, ethnic density and psychological well-being through adolescence: Evidence from the determinants of adolescent social well-being and health longitudinal study. Ethn. Health 2012, 17, 71–87. [Google Scholar] [CrossRef]
- Stevens, G.W.J.; Vollebergh, W.A.; Pels, T.V.; Crijnen, A.A. Problem behavior and acculturation in Moroccan immigrant adolescents in the Netherlands. J. Cross Cult. Psychol. 2007, 38, 310–317. [Google Scholar] [CrossRef]
- Abdullahi, I.; Kruger, E.; Tennant, M. Service access and perceptions for Somali Australian migrants at risk of autism. Int. J. Migr. Health Soc. Care 2017, 13, 119–125. [Google Scholar] [CrossRef]
- Goldblatt, H.; Rosenblum, S. Navigating among worlds: The experience of Ethiopian adolescents in Israel. J. Adolesc. Res. 2007, 22, 585–611. [Google Scholar] [CrossRef]
- Ndengeyingoma, A.; de Montigny, F.; Miron, J.M. Development of personal identity among refugee adolescents: Facilitating elements and obstacles. J. Child Health Care 2013, 18, 369–377. [Google Scholar] [CrossRef]
- Inguglia, C.; Musso, P. Intercultural profiles and adaptation among immigrant and autochthonous adolescents. Eur. J. Psychol. 2015, 11, 79–99. [Google Scholar] [CrossRef] [PubMed]
- Sanchez-Cao, E.; Kramer, T.; Hodes, M. Psychological distress and mental health service contact of unaccompanied asylum-seeking children. Child Care Health Dev. 2013, 39, 651–659. [Google Scholar] [CrossRef]
- Iyakaremye, I.; Mukagatare, C. Forced migration and sexual abuse: Experience of Congolese adolescent girls in Kigeme refugee camp, Rwanda. Health Psychol. Rep. 2016, 4, 261–271. [Google Scholar] [CrossRef]
- Williams, T.P.; Chopra, V.; Chikanya, S.R. “It isn’t that we’re prostitutes”: Child protection and sexual exploitation of adolescent girls within and beyond refugee camps in Rwanda. Child Abus. Negl. 2018, 86, 158–166. [Google Scholar] [CrossRef]
- Warria, A. Challenges in assistance provision to child victims of transnational trafficking in South Africa. Eur. J. Soc. Work 2018, 21, 710–723. [Google Scholar] [CrossRef]
- Berman, H. Stories of growing up amid violence by refugee children of war and children of battered women living in Canada. J. Nurs. Scholarsh. 1999, 31, 57–63. [Google Scholar] [CrossRef] [PubMed]
- Paalman, C.H.; van Domburgh, L.; Stevens, G.W.; Doreleijers, T.A.H. Individual, family and offence characteristics of high risk childhood offenders: Comparing non-offending, one-time offending and re-offending Dutch-Moroccan migrant children in the Netherlands. Child Adolesc. Psychiatry Ment. Health 2011, 5, 33. [Google Scholar] [CrossRef]
- Ravid, C.; Spitzer, A.; Tamir, B.; Granot, M.; Noam, R. Internal body perceptions of Ethiopian Jews who emigrated to Israel. West. J. Nurs. Res. 1995, 17, 631–646. [Google Scholar] [CrossRef] [PubMed]
- Stevens, G.W.J.M.; Pels, T.; Bengi-Arslan, L.; Verhulst, F.C.; Vollebergh, W.A.M.; Crijnen, A.A.M. Parent, teacher and self-reported problem behavior in the Netherlands. Soc. Psychiatry Psychiatr. Epidemiol. 2003, 38, 576–585. [Google Scholar] [CrossRef] [PubMed]
- Stevens, G.W.J.M.; Veen, V.C.; Vollebergh, W.A.M. Psychological acculturation and juvenile delinquency: Comparing Moroccan immigrant families from a general and pretrial detention population. Cult. Divers. Ethn. Minor. Psychol. 2014, 20, 254–265. [Google Scholar] [CrossRef] [PubMed]
- Zlot, A. Body-perception among Ethiopian-Israeli teenage girls. Int. J. Adolesc. Med. Health 1999, 11, 61–92. [Google Scholar] [CrossRef]
- Harding, S.; Boroujerdi, M.; Santana, P.; Cruickshank, J. Decline in, and lack of difference between, average birth weights among African and Portuguese babies in Portugal. Int. J. Epidemiol. 2006, 35, 270–276. [Google Scholar] [CrossRef]
- Harding, S.; Santana, P.; Cruickshank, J.K.; Boroujerdi, M. Birth weights of Black African babies of migrant and nonmigrant mothers compared with those of babies of European mothers in Portugal. Ann. Epidemiol. 2006, 16, 572–579. [Google Scholar] [CrossRef] [PubMed]
- Racape, J.; De Spiegelaere, M.; Alexander, S.; Dramaix, M.; Buekens, P.; Haelterman, E. High perinatal mortality rate among immigrants in Brussels. Eur. J. Public Health 2010, 20, 536–542. [Google Scholar] [CrossRef] [PubMed]
- Jamieson, D.J.; Meikle, S.F.; Hillis, S.D.; Mtsuko, D.; Mawji, S.; Duerr, A. An evaluation of poor pregnancy outcomes among Burundian refugees in Tanzania. JAMA 2000, 283, 397–402. [Google Scholar] [CrossRef] [PubMed]
- Vang, Z.M. Infant mortality among the Canadian-born offspring of immigrants and non-immigrants in Canada: A population-based study. Popul. Health Metr. 2016, 14, 32–47. [Google Scholar] [CrossRef]
- Simeoni, S.; Frova, L.; De Curtis, M. Inequalities in infant mortality in Italy. Ital. J. Pediatr. 2019, 45, 11–18. [Google Scholar] [CrossRef]
- Hargreaves, J.R.; Collinson, M.A.; Kahn, K.; Clark, S.J.; Tollman, S.M. Childhood mortality among former Mozambican refugees and their hosts in rural South Africa. Int. J. Epidemiol. 2004, 33, 1271–1278. [Google Scholar] [CrossRef]
- Essén, B.; Hanson, B.S.; Östergren, P.O.; Lindquist, P.G.; Gudmundsson, S. Increased perinatal mortality among sub-Saharan immigrants in a city-population in Sweden. Acta Obstet. Gynecol. Scand. 2000, 79, 737–743. [Google Scholar] [CrossRef]
- Juárez, S.P.; Revuelta-Eugercios, B.A. Too heavy, too late: Investigating perinatal health outcomes in immigrants residing in Spain. A cross-sectional study (2009–2011). J. Epidemiol. Community Health 2014, 68, 863–868. [Google Scholar] [CrossRef]
- Legg, S.; Davies, A.M.; Prywes, R.; Sterk, V.V.; Weiskopf, P. Patterns of low birth weight in west Jerusalem with special reference to maternal origin. Br. J. Prev. Soc. Med. 1970, 24, 89–96. [Google Scholar] [CrossRef]
- Racape, J.; Schoenborn, C.; Sow, M.; Alexander, S.; De Spiegelaere, M. Are all immigrant mothers really at risk of low birth weight and perinatal mortality? The crucial role of socio-economic status. BMC Pregnancy Childbirth 2016, 16, 75–85. [Google Scholar] [CrossRef]
- Yudkin, P.L.; Harlap, S.; Baras, M. High birthweight in an ethnic group of low socioeconomic status. BJOG 1983, 90, 291–296. [Google Scholar] [CrossRef] [PubMed]
- Agudelo-Suárez, A.A.; Ronda-Pérez, E.; Gil-González, D.; González-Zapata, L.I.; Regidor, E. Relationship in Spain of the length of the gestation and the birth weight with mother’s nationality during the period 2001–2005. Rev. Esp. Salud Publica 2009, 83, 331–337. [Google Scholar] [CrossRef] [PubMed]
- Buekens, P.; Masuy-Stroobant, G.; Delvaux, T. High birthweights among infants of North African immigrants in Belgium. Am. J. Public Health 1998, 88, 808–811. [Google Scholar] [CrossRef]
- Vahratian, A.; Buekens, P.; Delvaux, T.; Boutsen, M.; Wang, Y.; Kupper, L.L. Birthweight differences among infants of north African immigrants and Belgians in Belgium. Eur. J. Public Health 2004, 14, 381–383. [Google Scholar] [CrossRef]
- Johnson, E.B.; Reed, S.D.; Hitti, J.; Batra, M. Increased risk of adverse pregnancy outcome among Somali immigrants in Washington State. Am. J. Obstet. Gynecol. 2005, 193, 475–482. [Google Scholar] [CrossRef]
- Flynn, P.M.; Foster, E.M.; Brost, B.C. Indicators of acculturation related to Somali refugee women’s birth outcomes in Minnesota. J. Immigr. Minor. Health 2011, 13, 224–231. [Google Scholar] [CrossRef] [PubMed]
- Ortiz-Echevarria, L.; Greeley, M.; Bawoke, T.; Zimmerman, L.; Robinson, C.; Schlecht, J. Understanding the unique experiences, perspectives and sexual and reproductive health needs of very young adolescents: Somali refugees in Ethiopia. Confl. Health 2017, 11, 26–34. [Google Scholar] [CrossRef]
- Gaspar, T.; Matos-Gaspar, M. Adolescent’s lifestyles, ethnicity and socioeconomic status in Portugal. J. Poverty 2009, 13, 49–57. [Google Scholar]
- Essén, B.; Bödker, B.; Sjöberg, N.O.; Gudmundsson, S.; Östergren, P.O.; Langhoff-Roos, J. Is there an association between female circumcision and perinatal death? Bull. World Health Organ. 2002, 80, 629–632. [Google Scholar]
- Macipe-Costa, R.; Macipe-Costa, R.; García-Sanchez, N.; García-Sanchez, N.; Gimeno-Feliu, L.; Gimeno-Feliu, L.; Navarra-Vicente, B.; Jimenez-Hereza, J.M.; Moneo-Hernandez, I.M.; Castillo-Laita, J.A.; et al. Non-therapeutic male circumcision performed on immigrant children from Africa in Spain. Int. J. Public Health 2014, 59, 351–358. [Google Scholar] [CrossRef] [PubMed]
- Pruitt, C.N.; Reese, C.S.; Grossardt, B.R.; Shire, A.M.; Creedon, D.J. Completion of the human papillomavirus vaccination series lags in Somali adolescents. J. Low. Genit. Tract Dis. 2013, 17, 280–288. [Google Scholar] [CrossRef]
- Vang, Z.M.; Elo, I.T. Exploring the health consequences of majority–minority neighborhoods: Minority diversity and birthweight among native-born and foreign-born blacks. Soc. Sci. Med. 2013, 97, 56–65. [Google Scholar] [CrossRef]
- Mor, Z.; Amit Aharon, A.; Sheffer, R.; Nehama, H. Growth, developmental achievements and vaccines timeliness of undocumented migrant children from Eritrea compared with Israelis. PLoS ONE 2018, 13, e0193219. [Google Scholar] [CrossRef]
- Sarafoglou, K.; Bentler, K.; Gaviglio, A.; Redlinger-Grosse, K.; Anderson, C.; McCann, M.; Bloom, B.; Babovic-Vuksanovic, D.; Gavrillow, D.; Berry, S.A. High incidence of profound biotinidase deficiency detected in newborn screening blood spots in the Somalian population in Minnesota. J. Inherit. Metab. Dis. 2009, 32, 169–173. [Google Scholar] [CrossRef]
- Goel, K.M.; Thomson, R.B.; Sweet, E.M.; Halliday, S. Growth of immigrant children in the centre of Glasgow. Scott. Med. J. 1981, 26, 340–345. [Google Scholar] [CrossRef]
- Kamer, A.; Zohar, A.; Youngmann, R.; Diamond, G.; Inbar, D.; Senecky, Y. A prevalence estimate of pervasive developmental disorder among Immigrants to Israel and Israeli natives. Soc. Psychiatry Psychiatr. Epidemiol. 2004, 39, 141–145. [Google Scholar] [CrossRef] [PubMed]
- Barnevik-Olsson, M.; Gillberg, C.; Fernell, E. Prevalence of autism in children of Somali origin living in Stockholm: Brief report of an at-risk population. Dev. Med. Child Neurol. 2010, 52, 1167–1168. [Google Scholar] [CrossRef]
- Barnevik-Olsson, M.; Gillberg, C.; Fernell, E. Prevalence of autism in children born to Somali parents living in Sweden: A brief report. Dev. Med. Child Neurol. 2008, 50, 598–601. [Google Scholar] [CrossRef] [PubMed]
- Esler, A.; Hall-Lande, J.; Hewitt, A. Phenotypic characteristics of Autism Spectrum Disorder in a diverse sample of Somali and other children. J. Autism Dev. Disord. 2017, 47, 3150–3165. [Google Scholar] [CrossRef] [PubMed]
- Fox, F.; Aabe, N.; Turner, K.; Redwood, S.; Rai, D. “It was like walking without knowing where I was going”: A qualitative study of autism in a UK Somali migrant community. J. Autism Dev. Disord. 2017, 47, 305–315. [Google Scholar] [CrossRef]
- Wijtzes, A.; Jansen, W.; Jaddoe, V.; Moll, H.; Tiemeier, H.; Verhulst, F.; Hofman, A.; Mackenbach, J.; Raat, H. Ethnic background and television viewing time among 4-year-old preschool children: The generation R study. J. Dev. Behav. Pediatr. 2013, 34, 63–71. [Google Scholar] [CrossRef] [PubMed]
- Mude, W.; Mwanri, L. Barriers to participation in physical activity among south Sudanese children in South Australia: Parents’ perspectives. Fam. Community Health 2016, 39, 293–300. [Google Scholar] [CrossRef]
- Thul, C.M.; LaVoi, N.M. Reducing physical inactivity and promoting active living: From the voices of East African immigrant adolescent girls. Qual. Res. Sport Exerc. Health 2011, 3, 211–237. [Google Scholar] [CrossRef]
- Thul, C.M.; Eisenberg, M.E.; Larson, N.I.; Neumark-Sztainer, D. Physical activity patterns among Minnesota Somali adolescents. J. Phys. Act. Health 2015, 12, 1320–1326. [Google Scholar] [CrossRef] [PubMed]
- Bakken, K.S.; Skjeldal, O.H.; Stray-Pedersen, B. Neonatal jaundice and the immigrant population: A comparison study at a low-risk maternity ward in Norway. Nord. J. Nurs. Res. 2015, 35, 165–171. [Google Scholar] [CrossRef]
- Montanaro, M.; Colombatti, R.; Pugliese, M.; Migliozzi, C.; Zani, F.; Guerzoni, M.E.; Manoli, S.; Manara, R.; Meneghetti, G.; Rampazzo, P.; et al. Intellectual function evaluation of first generation immigrant children with sickle cell disease: The role of language and sociodemographic factors. Ital. J. Pediatr. 2013, 39, 36–43. [Google Scholar] [CrossRef] [PubMed]
- Gorrab, A.A.; Fournier, A.; Bouaziz, A.A.; Spigelblatt, L.; Scuccimarri, R.; Mrabet, A.; Dahdah, N. Incidence rate and epidemiological and clinical aspects of Kawasaki disease in children of Maghrebi origin in the Province of Quebec, Canada, compared to the country of origin. Glob. Pediatr. Health 2016, 3, 1–8. [Google Scholar] [CrossRef]
- Rovillé-Sausse, F. Growth rates of children of tilization African ancestry born to immigrant parents and of French children in Paris. Am. J. Hum. Biol. 1998, 10, 757–763. [Google Scholar] [CrossRef]
- Davidovich, E.; Kooby, E.; Shapira, J.; Ram, D. The traditional practice of canine bud removal in the offspring of Ethiopian immigrants. BMC Oral Health 2013, 13, 34. [Google Scholar] [CrossRef] [PubMed]
- Holan, G.; Mamber, E. Extraction of primary canine tooth buds: Prevalence and associated dental abnormalities in a group of Ethiopian Jewish children. Int. J. Paediatr. Dent. 1994, 4, 25–30. [Google Scholar] [CrossRef]
- Cote, S.; Geltman, P.; Nunn, M.; Lituri, K.; Henshaw, M.; Garcia, R.I. Dental caries of refugee children compared with US children. Pediatrics 2004, 114, e733–e740. [Google Scholar] [CrossRef]
- Quach, A.; Laemmle-Ruff, I.L.; Polizzi, T.; Paxton, G.A. Gaps in smiles and services: A cross-sectional study of dental caries in refugee-background children. BMC Oral Health 2015, 15, 10. [Google Scholar] [CrossRef]
- Sarnat, H.; Cohen, S.; Gat, H. Changing patterns of dental caries in Ethiopian adolescents who immigrated to Israel. Community Dent. Oral Epidemiol. 1987, 15, 286–288. [Google Scholar] [CrossRef] [PubMed]
- Sgan-Cohen, H.D.; Steinberg, D.; Zusman, S.P.; Sela, M.N. Dental caries and its determinants among recent immigrants from rural Ethiopia. Community Dent. Oral Epidemiol. 1992, 20, 338–342. [Google Scholar] [CrossRef] [PubMed]
- Davidovich, E.; Kooby, E.; Shapira, J.; Ram, D. Oral hygiene habits, dental home, and toothbrushing among immigrant and native low socioeconomic class populations. J. Clin. Pediatr. Dent. 2013, 37, 341–344. [Google Scholar] [CrossRef] [PubMed]
- Amin, M.; Perez, A.; Nyachhyon, P. Parental awareness and dental attendance of children among African immigrants. J. Immigr. Minor. Health 2015, 17, 132–138. [Google Scholar] [CrossRef] [PubMed]
- Almerich-Silla, J.M.; Montiel-Company, J.M.; Ruiz-Miravet, A. Caries and dental fluorosis in a western Saharan population of refugee children. Eur. J. Oral Sci. 2008, 116, 512–517. [Google Scholar] [CrossRef] [PubMed]
- Svensson, I.; Gustafsson, J.; Matsson, L.; Uleskog, E.; Molla, N.; Kahlmeter, A.; Matsson, L. Oral condition and background factors in Somali immigrant children newly arrived in Sweden. Swed. Dent. J. 2016, 40, 153–164. [Google Scholar]
- Amin, M.; Perez, A. Is the wait-for-patient-to-come approach suitable for African newcomers to Alberta, Canada? Community Dent. Oral Epidemiol. 2012, 40, 523–531. [Google Scholar] [CrossRef] [PubMed]
- Metsäniitty, M.; Waltimo-Sirén, J.; Ranta, H.; Fieuws, S.; Thevissen, P. Dental age estimation in Somali children and sub-adults combining permanent teeth and third molar development. Int. J. Leg. Med. 2019, 133, 1207–1215. [Google Scholar] [CrossRef]
- Obeng, C.S. Dental care issues for African immigrant families of preschoolers. Early Child. Res. Pract. 2008, 10, 1–5. [Google Scholar]
- Vered, Y.; Schwarts, N.; Mann, J.; Sgan-Cohen, H.D. Periodontal health among recent immigrants from Quara, rural Ethiopia and indications for periodontal health care. Int. Dent. J. 2003, 53, 92–96. [Google Scholar] [CrossRef]
- Patel, A.R.; Zietlow, J.; Jacobson, R.M.; Poland, G.A.; Juhn, Y.J. Asthma and the immune response to MMR vaccine viruses in Somali immigrant children: A cross-sectional retrospective cohort study. Prim. Care Respir. J. 2013, 22, 278–283. [Google Scholar] [CrossRef]
- Shani, M.; Band, Y.; Kidon, M.I.; Segel, M.J.; Rosenberg, R.; Nakar, S.; Vinker, S. The second generation and asthma: Prevalence of asthma among Israeli born children of Ethiopian origin. Respir. Med. 2013, 107, 519–523. [Google Scholar] [CrossRef]
- Veenstra-van Schie, M.T.M.; Coenen, K.; Koopman, H.M.; Versteegh, F.G.A. Higher perceived HRQoL in Moroccan children with asthma and their parents. Pan Afr. Med. J. 2015, 21, 18–22. [Google Scholar] [CrossRef]
- Bennet, R.; Eriksson, M. Tuberculosis infection and disease in the 2015 cohort of unaccompanied minors seeking asylum in Northern Stockholm, Sweden. Infect. Dis. 2017, 49, 501–506. [Google Scholar] [CrossRef]
- Chemtob, D.; Weiler-Ravell, D.; Leventhal, A.; Bibi, H. Epidemiologic characteristics of pediatric active tuberculosis among immigrants from high to low tuberculosis-endemic countries: The Israeli experience. Isr. Med. Assoc. J. 2006, 8, 21–26. [Google Scholar]
- Lucas, M.; Nicol, P.; McKinnon, E.; Whidborne, R.; Lucas, A.; Thambiran, A.; Burgner, D.; Waring, J.; French, M. A prospective large-scale study of methods for the detection of latent Mycobacterium tuberculosis infection in refugee children. Thorax 2010, 65, 442–448. [Google Scholar] [CrossRef]
- Nejat, S.; Bennet, R. Interferon-gamma release assays can effectively screen migrants for the tuberculosis infection, but urgent, active cases need clinical recognition. Acta Paediatr. 2016, 105, 671–675. [Google Scholar] [CrossRef]
- Mor, Z.; Cedar, N.; Pinsker, G.; Bibi, H.; Grotto, I. Childhood tuberculosis in Israel: Epidemiological trends and treatment outcomes, 1999–2010. Eur. Respir. J. 2013, 41, 1157–1162. [Google Scholar] [CrossRef]
- Paxton, G.A.; Rice, J.; Davie, G.; Carapetis, J.R.; Skull, S.A. East African immigrant children in Australia have poor tilization coverage. Paediatr. Child Health 2011, 47, 888–892. [Google Scholar] [CrossRef]
- Chiappini, E.; Zaffaroni, M.; Bianconi, M.; Veneruso, G.; Grasso, N.; Garazzino, S.; Arancio, R.; Valentini, P.; Ficcadenti, A.; Da Riol, M.R.; et al. Italian tilization study found infectious and vaccine-preventable diseases in children adopted from Africa and recommends prompt medical screening. Acta Paediatr. 2018, 107, 1581–1586. [Google Scholar] [CrossRef]
- Porter, J.D.; Gastellu-Etchegorry, M.; Navarre, I.; Lungu, G.; Moren, A. Measles outbreaks in the Mozambican refugee camps in Malawi: The continued need for an effective vaccine. Int. J. Epidemiol. 1990, 19, 1072–1077. [Google Scholar] [CrossRef]
- St. Sauver, J.L.; Jacobson, R.M.; Vierkant, R.A.; Jacobsen, S.J.; Green, E.M.; Poland, G.A. Association of parental vaccination reports with measles, mumps, and rubella protective antibody levels: Comparison of Somali immigrant, Hispanic migrant, and US children in Rochester, Minn. Mayo Clin. Proc. 2002, 77, 241–245. [Google Scholar] [CrossRef]
- Colombatti, R.; Palazzi, G.; Masera, N.; Notarangelo, L.D.; Bonetti, E.; Samperi, P.; Barone, A.; Perrotta, S.; Facchini, E.; Miano, M.; et al. Hydroxyurea prescription, availability and use for children with sickle cell disease in Italy: Results of a national multicenter survey. Ital. J. Pediatr. 2018, 65, e26774. [Google Scholar] [CrossRef]
- Bawa, S.; Afolabi, M.; Abdelrahim, K.; Abba, G.; Ningi, A.; Tafida, S.Y.; Tegegne, S.G.; Warigon, C.; Nomhwange, T.; Umar, S.A.; et al. Transboundary nomadic population movement: A potential for import-export of poliovirus. BMC Public Health 2018, 18, 1316. [Google Scholar] [CrossRef]
- Cadario, F.; Bruno, G.; Cerutti, F.; Savastio, S.; Tumini, S. Increasing prevalence and younger age at onset of type 1 diabetes in migrant than Italian children with type 1 diabetes: An emerging problem. Acta Diabetol. 2014, 51, 263–267. [Google Scholar] [CrossRef]
- Hussen, H.I.; Moradi, T.; Persson, M. The risk of type 1 diabetes among offspring of immigrant mothers in relation to the duration of residency in Sweden. BMJ Open 2015, 38, 934–936. [Google Scholar] [CrossRef]
- Vos, C.; Reeser, H.M.; Hirasing, R.A.; Bruining, G.J. Confirmation of high incidence of type 1 (insulin-dependent) diabetes mellitus in Moroccan children in the Netherlands. Diabet. Med. 1997, 14, 397–400. [Google Scholar] [CrossRef]
- Oilinki, T.; Otonkoski, T.; Ilonen, J.; Knip, M.; Miettinen, P. Prevalence and characteristics of diabetes among Somali children and adolescents living in Helsinki, Finland. Pediatr. Diabetes 2012, 13, 176–180. [Google Scholar] [CrossRef]
- Aakre, I.; Strand, T.A.; Moubarek, K.; Barikmo, I.; Henjum, S. Associations between thyroid dysfunction and developmental status in children with excessive iodine status. PLoS ONE 2017, 12, e0187241. [Google Scholar] [CrossRef]
- Henjum, S.; Barikmo, I.; Gjerlaug, A.K.; Mohamed-Lehabib, A.; Oshaug, A.; Arne Strand, T.; Torheim, L.E. Endemic tiliz and excessive iodine in urine and drinking water among Saharawi refugee children. Public Health Nutr. 2010, 13, 1472–1477. [Google Scholar] [CrossRef] [PubMed]
- Luboshitzky, R.; Dgani, Y.; Atar, S.; Qupty, G.; Tamir, A.; Flatau, E. Goiter prevalence in children immigrating from an endemic goiter area in Ethiopia to Israel. J. Pediatr. Endocrinol. 1995, 8, 123–125. [Google Scholar] [CrossRef] [PubMed]
- Nudelman, A. Culture and health behaviour: The case of adolescent Ethiopian immigrants In Israel. Int. J. Adolesc. Med. Health 1999, 11, 3–20. [Google Scholar] [CrossRef] [PubMed]
- Meyer-Weitz, A.; Oppong Asante, K.; Lukobeka, B.J. Healthcare service delivery to refugee children from the Democratic Republic of Congo living in Durban, South Africa: A caregivers’ perspective. BMC Med. 2018, 16, 163. [Google Scholar] [CrossRef] [PubMed]
- Soriano, E.; Ruiz, D.; Higginbottom, G. Health promotion in the Moroccan child population in Spain: The healthy child program. Procedia Soc. Behav. Sci. 2014, 132, 675–681. [Google Scholar] [CrossRef][Green Version]
- Zwi, K.; Rungan, S.; Woolfenden, S.; Woodland, L.; Palasanthiran, P.; Williams, K. Refugee children and their health, development and well-being over the first year of settlement: A longitudinal study. J. Trop. Pediatr. 2017, 53, 841–849. [Google Scholar] [CrossRef]
- Cooke, R.; Murray, S.; Carapetis, J.; Rice, J.; Mulholland, N.; Skull, S. Demographics and utilisation of health services by paediatric refugees from East Africa: Implications for service planning and provision. Aust. Health Rev. 2004, 27, 40–45. [Google Scholar] [CrossRef][Green Version]
- Bennett, F.J.; Jelliffe, D.B. The health of immigrant babies in an East African town. Trop. Geogr. Med. 1965, 17, 213–224. [Google Scholar] [PubMed]
- Plotinsky, R.N.; Straetemans, M.; Wong, L.Y.; Brown, M.J.; Dignam, T.; Dana Flanders, W.; Tehan, M.; Azziz-Baumgartner, E.; Dipentima, R.; Talbot, E.A. Risk factors for elevated blood lead levels among African refugee children in New Hampshire, 2004. Environ. Res. 2008, 108, 404–412. [Google Scholar] [CrossRef]
- Corriveau-Bourque, C.; Bruce, A.A.K. The changing epidemiology of pediatric hemoglobinopathy patients in northern Alberta, Canada. J. Pediatr. Hematol. Oncol. 2015, 37, 595–599. [Google Scholar] [CrossRef]
- McMahon, C.; Callaghan, C.O.; O’Brien, D.; Smith, O.P. The increasing prevalence of childhood sickle-cell disease in Ireland. Ir. J. Med. Sci. 2001, 170, 183–185. [Google Scholar] [CrossRef]
- Oppenheim, C.E.; Axelrod, K.; Menyongai, J.; Chukwuezi, B.; Tam, A.; Henderson, D.C.; Borba, C.P.C. The HEAAL project: Applying Community-Based Participatory Research (CBPR) methodology in a health and mental health needs assessment with an African immigrant and refugee faith community in Lowell, Massachusetts. J. Public Health Manag. Pract. 2019, 25, E1–E6. [Google Scholar] [CrossRef]
- Murray, K.E.; Mohamed, A.S.; Dawson, D.B.; Syme, M.; Abdi, S.; Barnack-Taviaris, J. Somali perspectives on physical activity: Photovoice to address barriers and resources in San Diego. Prog. Community Health Partnersh. 2015, 9, 83–90. [Google Scholar] [CrossRef] [PubMed]
- Collins, C.S.; Stockton, C.M. The central role of theory in qualitative research. Int. J. Qual. Methods 2018, 17, 1–10. [Google Scholar] [CrossRef]
- Lynch, E.A.; Mudge, A.; Knowles, S.; Kitson, A.L.; Hunter, S.C.; Harvey, G. “There is nothing so practical as a good theory”: A pragmatic guide for selecting theoretical approaches for implementation projects. BMC Health Serv. Res. 2018, 18, 857. [Google Scholar] [CrossRef] [PubMed]
- Stewart, D.; Klein, S. The use of theory in research. Int. J. Clin. Pharm. 2016, 38, 615–619. [Google Scholar] [CrossRef]
- UNICEF. Data Snapshot of Migrant and Displaced Children in Africa; United Nations: Geneva, Switzerland, 2019. [Google Scholar]
- Statistics Canada. Diversity of Black Population in Canada—An Overview; Ethnicity, Language and Immigration Thematic Series; Statistics Canada: Ottawa, ON, Canada, 2019. [Google Scholar]
- Odeniyi, A.O.; Embleton, N.; Ngongalah, L.; Akor, W.; Rankin, J. Breastfeeding beliefs and experiences of African immigrant mothers in high-income countries: A systematic review. Matern. Child Nutr. 2020, 16, e12970. [Google Scholar] [CrossRef]
- Jakub, K.E.; Turk, M.T.; Fapohunda, A.; Zoucha, R. Cultural beliefs, perceptions, and practices of young adult offspring of African immigrants regarding healthy eating and activity. J. Transcult. Nurs. 2018, 29, 548–554. [Google Scholar] [CrossRef] [PubMed]
- Cooper Brathwaite, A.; Lemonde, M. Health beliefs and practices of African immigrants in Canada. Clin. Nurs. Res. 2015, 25, 626–645. [Google Scholar] [CrossRef]
- Kim, M.S.; Song, I.G.; An, A.R.; Kim, K.H.; Sohn, J.H.; Yang, S.W. Healthcare access challenges facing six African refugee mothers in South Korea: A qualitative multiple-case study. Korean J. Pediatr. 2017, 60, 138–144. [Google Scholar] [CrossRef] [PubMed]
- Chekero, T.; Ross, F.C. “On paper” and “having papers”: Zimbabwean migrant women’s experiences in accessing healthcare in Giyani, Limpopo province, South Africa. Anthropol. S. Afr. 2018, 41, 41–54. [Google Scholar] [CrossRef]
- Fatahi, N.; Krupic, F. Factors beyond the language barrier in providing health care to immigrant patients. Med. Arch. 2016, 70, 61–65. [Google Scholar] [CrossRef]
- Mbanya, V.N.; Terragni, L.; Gele, A.A.; Diaz, E.; Kumar, B.N. Access to Norwegian healthcare system—Challenges for sub-Saharan African immigrants. Int. J. Equity Health 2019, 18, 125–138. [Google Scholar] [CrossRef] [PubMed]
- Pérez-Urdiales, I.; Goicolea, I.; San Sebastián, M.; Irazusta, A.; Linander, I. Sub-Saharan African immigrant women’s experiences of (lack of) access to appropriate healthcare in the public health system in the Basque Country, Spain. Int. J. Equity Health 2019, 18, 59–70. [Google Scholar] [CrossRef]
- Berge, J.M.; Fertig, A.; Tate, A.; Trofholz, A.; Neumark-Sztainer, D. Who is meeting the Healthy People 2020 objectives?: Comparisons between racially/ethnically diverse and immigrant children and adults. Fam. Syst. Health 2018, 36, 451–470. [Google Scholar] [CrossRef]
- Truong, M.; Paradies, Y.; Priest, N. Interventions to improve cultural competency in healthcare: A systematic review of reviews. BMC Health Serv. Res. 2014, 14, 99. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization (WHO). Child Health; World Health Organization Regional Office for Africa: Geneva, Switzerland, 2020. [Google Scholar]
- UNICEF. A Deadly Journey for Children: The Migration Route from North Africa to Europe; United Nations: Geneva, Switzerland, 2017. [Google Scholar]
- Markides, K.S.; Rote, S. The healthy immigrant effect and aging in the United States and other western countries. Gerontologist 2019, 59, 205–214. [Google Scholar] [CrossRef]
- WHO. Universal Health Coverage. Key Facts. 2019. Available online: https://www.who.int/news-room/fact-sheets/detail/universal-health-coverage-(uhc) (accessed on 1 March 2020).


{kind=link}
| Keywords Used | |
|---|---|
| Child Health | Adolescent health services, child care, infant care, infant, newborn, infant health, child welfare, infant welfare, child nutrition disorders, infant nutrition disorders, child nutritional physiological phenomena, adolescent nutritional physiological phenomena, adolescent development, adolescent health, adolescent medicine, adolescent psychiatry, psychology, adolescent or child psychiatry, adolescent development, child development, psychology, child, children, childhood, infant *, newborn *, neonate *, baby, babies, preschool *, toddler *, adolescen *, teen *, youth *, pediatric *, paediatric * |
| Immigrant | Emigrants, refugee *, immigra *, asylum seeker *, migrant *, displace *, transient * |
| Africa | African * and the name of each African country |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Salami, B.; Fernandez-Sanchez, H.; Fouche, C.; Evans, C.; Sibeko, L.; Tulli, M.; Bulaong, A.; Kwankye, S.O.; Ani-Amponsah, M.; Okeke-Ihejirika, P.; et al. A Scoping Review of the Health of African Immigrant and Refugee Children. Int. J. Environ. Res. Public Health 2021, 18, 3514. https://doi.org/10.3390/ijerph18073514
Salami B, Fernandez-Sanchez H, Fouche C, Evans C, Sibeko L, Tulli M, Bulaong A, Kwankye SO, Ani-Amponsah M, Okeke-Ihejirika P, et al. A Scoping Review of the Health of African Immigrant and Refugee Children. International Journal of Environmental Research and Public Health. 2021; 18(7):3514. https://doi.org/10.3390/ijerph18073514
Chicago/Turabian StyleSalami, Bukola, Higinio Fernandez-Sanchez, Christa Fouche, Catrin Evans, Lindiwe Sibeko, Mia Tulli, Ashley Bulaong, Stephen Owusu Kwankye, Mary Ani-Amponsah, Philomina Okeke-Ihejirika, and et al. 2021. "A Scoping Review of the Health of African Immigrant and Refugee Children" International Journal of Environmental Research and Public Health 18, no. 7: 3514. https://doi.org/10.3390/ijerph18073514
APA StyleSalami, B., Fernandez-Sanchez, H., Fouche, C., Evans, C., Sibeko, L., Tulli, M., Bulaong, A., Kwankye, S. O., Ani-Amponsah, M., Okeke-Ihejirika, P., Gommaa, H., Agbemenu, K., Ndikom, C. M., & Richter, S. (2021). A Scoping Review of the Health of African Immigrant and Refugee Children. International Journal of Environmental Research and Public Health, 18(7), 3514. https://doi.org/10.3390/ijerph18073514