
Pain Acceptance Creates an Emotional Context That Protects against the Misuse of Prescription Opioids: A Study in a Sample of Patients with Chronic Noncancer Pain

 ,
, 
 and
and 
Abstract
1. Introduction
2. Materials and Methods
2.1. Participants
2.2. Procedure
2.3. Variables and Instruments
2.3.1. Demographic and Clinical Variables
2.3.2. Pain Intensity
2.3.3. Pain Acceptance
2.3.4. Pain Catastrophizing
2.3.5. Anxiety and Depression Symptoms
2.3.6. Current Misuse of Prescribed Opioids
2.4. Statistical Analyses
3. Results
3.1. Participants
3.2. Descriptive Statistics
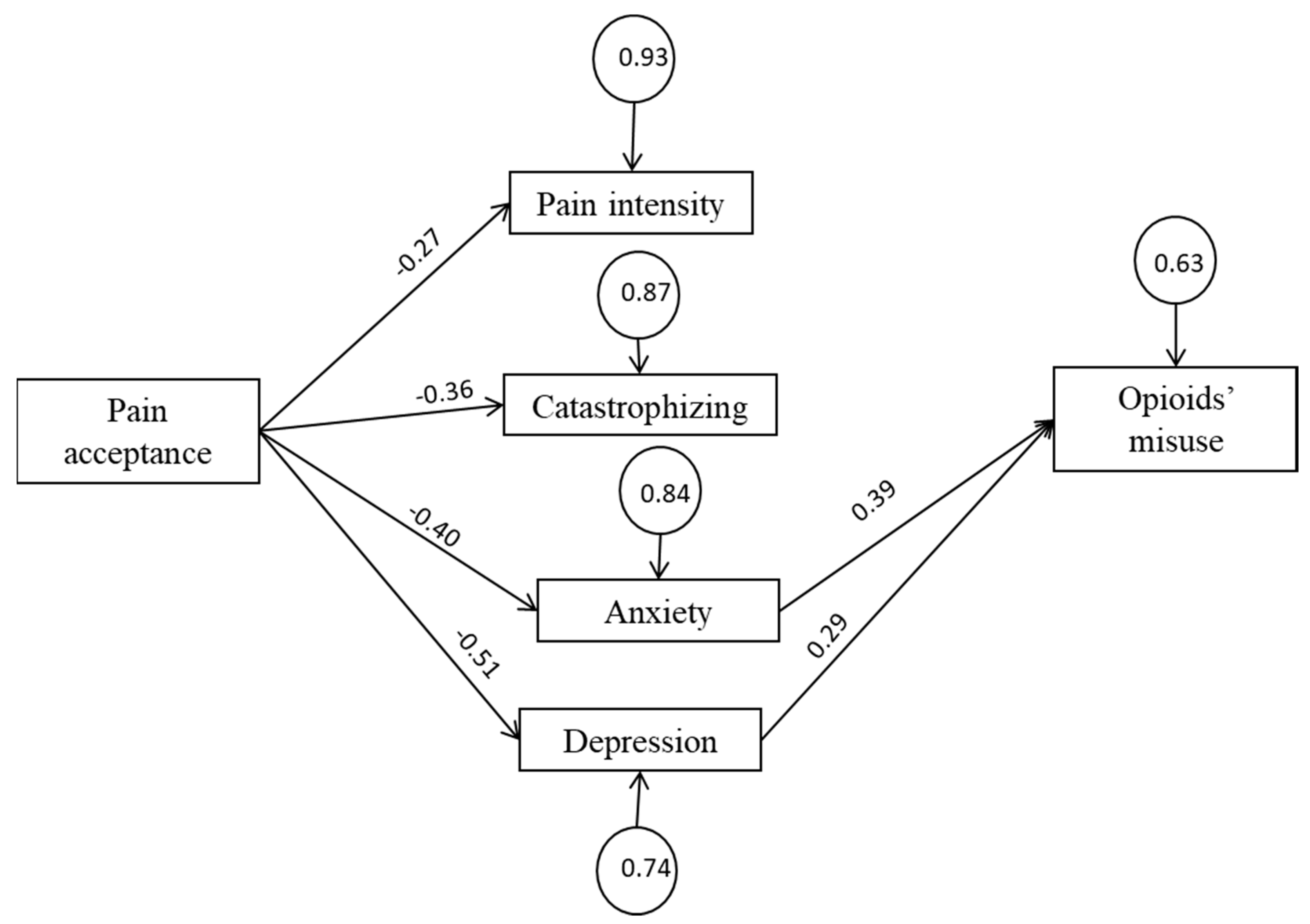
3.3. Structural Equation Modeling
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Leadley, R.M.; Armstrong, N.; Lee, Y.C.; Allen, A.; Kleijnen, J. Chronic diseases in the European Union: The prevalence and health cost implications of chronic pain. J. Pain Palliat. Care Pharmacother. 2012, 26, 310–325. [Google Scholar] [CrossRef] [PubMed]
- Gaskin, D.J.; Richard, P. The economic costs of pain in the United States. J. Pain 2012, 13, 715–724. [Google Scholar] [CrossRef] [PubMed]
- Els, C.; Jackson, T.D.; Kunyk, D.; Lappi, V.G.; Sonnenberg, B.; Hagtvedt, R.; Sharma, S.; Kolahdooz, F.; Straube, S. Adverse events associated with medium-and long-term use of opioids for chronic non-cancer pain: An overview of Cochrane Reviews. Cochrane Database Syst. Rev. 2017, 10, CD012509. [Google Scholar] [CrossRef] [PubMed]
- Berterame, S.; Erthal, J.; Thomas, J.; Fellner, S.; Vosse, B.; Clare, P.; Hao, W.; Johnson, D.T.; Mohar, A.; Pavadia, J.; et al. Use of and barriers to access to opioid analgesics: A worldwide, regional, and national study. Lancet 2016, 387, 1644–1656. [Google Scholar] [CrossRef]
- Ray, W.A.; Chung, C.P.; Murray, K.T.; Hall, K.; Stein, C.M. Prescription of long-acting opioids and mortality in patients with chronic noncancer pain. JAMA 2016, 315, 2415–2423. [Google Scholar] [CrossRef]
- Cicero, T.J.; Ellis, M.S.; Kasper, Z.A. Psychoactive substance use prior to the development of iatrogenic opioid abuse: A descriptive analysis of treatment-seeking opioid abusers. Addict. Behav. 2017, 65, 242–244. [Google Scholar] [CrossRef]
- Savage, S.R.; Joranson, D.E.; Covington, E.C.; Schnoll, S.H.; Heit, H.A.; Gilson, A.M. Definitions related to the medical use of opioids: Evolution towards universal agreement. J. Pain Symptom Manag. 2003, 26, 655–667. [Google Scholar] [CrossRef]
- Kertesz, S.G.; Gordon, A.J. A crisis of opioids and the limits of prescription control: United States. Addiction 2019, 114, 169–180. [Google Scholar] [CrossRef]
- Turk, D.C.; Monarch, E.S. Biopsychosocial perspective on chronic pain. In Psychological Approaches to Pain Management: A Practitioner’s Handbook; Turk, D., Gatchel, R.J., Eds.; Guilford Press: New York, NY, USA, 2002; pp. 3–29. [Google Scholar]
- Bevers, K.; Watts, L.; Kishino, N.D.; Gatchel, R.J. The biopsychosocial model of the assessment, prevention, and treatment of chronic pain. US Neurol. 2016, 12, 98–104. [Google Scholar] [CrossRef]
- Williams, A.C.; Fisher, E.; Hearn, L.; Eccleston, C. Psychological therapies for the management of chronic pain (excluding headache) in adults. Cochrane Database Syst. Rev. 2020, 8, CD007407. [Google Scholar] [CrossRef]
- McCracken, L.M.; Morley, S. The psychological flexibility model: A basis for integration and progress in psychological approaches to chronic pain management. J. Pain 2014, 15, 221–234. [Google Scholar] [CrossRef]
- Ditre, J.W.; Zale, E.L.; LaRowe, L.R. A reciprocal model of pain and substance use: Transdiagnostic considerations, clinical implications, and future directions. Ann. Rev. Clin. Psychol. 2019, 15, 503–528. [Google Scholar] [CrossRef]
- Hayes, S.C.; Luoma, J.B.; Bond, F.W.; Masuda, A.J. Acceptance and commitment therapy: Model, processes and outcomes. Behav. Res. Ther. 2006, 44, 1–25. [Google Scholar] [CrossRef]
- Hayes, S.C.; Follette, V.M.; Linehan, M.M. Mindfulness and Acceptance: Expanding the Cognitive-Behavioral Tradition, 1st ed.; Guilford Press: New York, NY, USA, 2004. [Google Scholar]
- Levin, M.E.; Hildebrandt, M.J.; Lillis, J.; Hayes, S.C. The impact of treatment components suggested by the psychological flexibility model: A meta-analysis of laboratory-based component studies. Behav. Ther. 2012, 43, 741–756. [Google Scholar] [CrossRef]
- Hayes, S.C.; Wilson, K.G.; Gifford, E.; Follette, V.M.; Strosahl, K.D. Emotional avoidance and behavior disorders: A functional dimensional approach to diagnosis and treatment. J. Consult Clin. Psychol. 1996, 64, 1152–1168. [Google Scholar] [CrossRef]
- Wilson, K.G.; Hayes, S.C.; Byrd, M.R. Exploring compatibilities between acceptance and commitment therapy and 12-step treatment for substance abuse. J. Ration. Emot. Cogn. Behav. Ther. 2000, 18, 209–234. [Google Scholar] [CrossRef]
- Luoma, J.; Drake, C.E.; Kohlenberg, B.S.; Hayes, S.C. Substance abuse and psychological flexibility: The development of a new measure. Addict. Res. Theory 2011, 19, 3–13. [Google Scholar] [CrossRef]
- Hayes, S.C.; Strosahl, K.; Wilson, K.G.; Bissett, R.T.; Pistorello, J.; Toarmino, D.; Polusny, M.A.; Dykstra, T.A.; Batten, S.V.; Bergan, J.; et al. Measuring experiential avoidance: A preliminary test of a working model. Psychol. Rec. 2004, 54, 553–578. [Google Scholar] [CrossRef]
- Bissett, R.T. Processes of change: Acceptance versus 12-step in polysubstance-abusing methadone clients. ProQuest Inf. Learn. 2002, 63, 10146. [Google Scholar]
- Luoma, J.B.; Kohlenberg, B.S.; Hayes, S.C.; Bunting, K.; Rye, A.K. Reducing self-stigma in substance abuse through acceptance and commitment therapy: Model, manual development, and pilot outcomes. Addict. Res. Theory 2008, 16, 149–165. [Google Scholar] [CrossRef] [PubMed]
- Kingston, J.; Clarke, S.; Remington, B. Experiential avoidance and problem behavior: A mediational analysis. Behav. Modif. 2010, 34, 145–163. [Google Scholar] [CrossRef]
- Levin, M.E.; Lillis, J.; Seeley, J.; Hayes, S.C.; Pistorello, J.; Biglan, A. Exploring the relationship between experiential avoidance, alcohol use disorders, and alcohol-related problems among first year college students. J. Am. Coll. Health 2012, 60, 443–448. [Google Scholar] [CrossRef]
- Serowik, K.L.; Orsillo, S.M. The relationship between substance use, experiential avoidance, and personally meaningful experiences. Subst. Use Misuse 2019, 54, 1834–1844. [Google Scholar] [CrossRef]
- Lee, E.B.; An, W.; Levin, M.E.; Twohig, M.P. An initial meta-analysis of Acceptance and Commitment Therapy for treating substance use disorders. Drug Alcohol Depend. 2015, 155, 1–7. [Google Scholar] [CrossRef] [PubMed]
- Öst, L.G. The efficacy of acceptance and commitment therapy: An updated systematic review and meta-analysis. Behav. Res. Ther. 2014, 61, 105–121. [Google Scholar] [CrossRef]
- de Boer, M.J.; Steinhagen, H.E.; Versteegen, G.J.; Struys, M.M.; Sanderman, R. Mindfulness, acceptance and catastrophizing in chronic pain. PLoS ONE 2014, 9, e87445. [Google Scholar] [CrossRef]
- McCracken, L.M.; Vowles, K.E. Acceptance of chronic pain. Curr. Pain Headache Rep. 2006, 10, 90–94. [Google Scholar] [CrossRef]
- Esteve, R.; López-Martínez, A.E.; Ruíz-Párraga, G.T.; Serrano-Ibáñez, E.R.; Ramírez-Maestre, C. Pain Acceptance and Pain-Related Disability Predict Healthcare Utilization and Medication Intake in Patients with Non-Specific Chronic Spinal Pain. Int. J. Environ. Res. Public Health 2020, 17, 5556. [Google Scholar] [CrossRef] [PubMed]
- McCracken, L.M.; Eccleston, C. A prospective study of acceptance of pain and patient functioning with chronic pain. Pain 2005, 118, 164–169. [Google Scholar] [CrossRef] [PubMed]
- McCracken, L.M.; Vowles, K.E. A prospective analysis of acceptance of pain and values-based action in patients with chronic pain. Health Psychol. 2008, 27, 215–220. [Google Scholar] [CrossRef] [PubMed]
- McCracken, L.M.; Vowles, K.E.; Gauntlett-Gilbert, J. A prospective investigation of acceptance and control-oriented coping with chronic pain. J. Behav. Med. 2007, 30, 339–349. [Google Scholar] [CrossRef]
- McCracken, L.M.; Vowles, K.E.; Zhao-O’Brien, J. Further development of an instrument to assess psychological flexibility in people with chronic pain. J. Behav. Med. 2010, 33, 346–354. [Google Scholar] [CrossRef]
- Chou, R.; Turner, J.A.; Devine, E.B.; Hansen, R.N.; Sullivan, S.D.; Blazina, I.; Dana, T.; Bougatsos, C.; Deyo, R.A. The effectiveness and risks of long-term opioid therapy for chronic pain: A systematic review for a National Institutes of Health Pathways to Prevention Workshop. Ann. Intern. Med. 2015, 162, 276–286. [Google Scholar] [CrossRef]
- Højsted, J.; Sjøgren, P. Addiction to opioids in chronic pain patients: A literature review. Eur. J. Pain 2007, 11, 490–518. [Google Scholar] [CrossRef]
- Kaye, A.D.; Jones, M.R.; Kaye, A.M.; Ripoll, J.G.; Jones, D.E.; Galan, V.; Beakley, B.D.; Calixto, F.; Bolden, J.L.; Urman, R.D.; et al. Prescription opioid abuse in chronic pain: An updated review of opioid abuse predictors and strategies to curb opioid abuse (part 2). Pain Physician 2017, 20, S111–S133. [Google Scholar]
- Volkow, N.; Benveniste, H.; McLellan, A.T. Use and misuse of opioids in chronic pain. Ann. Rev. Med. 2018, 69, 451–465. [Google Scholar] [CrossRef] [PubMed]
- Elander, J.; Duarte, J.; Maratos, F.A.; Gilbert, P. Predictors of painkiller dependence among people with pain in the general population. Pain Med. 2014, 15, 613–624. [Google Scholar] [CrossRef] [PubMed]
- Lin, L.A.; Bohnert, A.S.; Price, A.M.; Jannausch, M.; Bonar, E.E.; Ilgen, M.A. Pain acceptance and opiate use disorders in addiction treatment patients with comorbid pain. Drug Alcohol Depend. 2015, 157, 136–142. [Google Scholar] [CrossRef]
- Rhodes, A.; Marks, D.; Block-Lerner, J.; Lomauro, T. Psychological Flexibility, Pain Characteristics and Risk of Opioid Misuse in Noncancerous Chronic Pain Patients. J. Clin. Psychol. Med. Settings 2020. [Google Scholar] [CrossRef] [PubMed]
- McCracken, L.M. Toward understanding acceptance and psychological flexibility in chronic pain. Pain 2010, 149, 420–421. [Google Scholar] [CrossRef]
- Jackson, D.L. Revisiting sample size and number of parameter estimates: Some support for the N: Q hypothesis. Struct. Equ. Modeling 2003, 10, 128–141. [Google Scholar] [CrossRef]
- Jensen, M.; Karoly, P. Self-Report Scales and Procedures for Assessing Pain in Adults. In Handbook of Pain Assessment; Turk, D., Melzack, R., Eds.; Guilford Press: New York, NY, USA, 2001; pp. 15–34. [Google Scholar]
- Bendayan, R.; Esteve, R.; Blanca, M.J. New Empirical Evidence of the Validity of the Chronic Pain Acceptance Questionnaire: The Differential Influence of Activity Engagement and Pain Willingness on Adjustment to Chronic Pain. Br. J. Health Psychol. 2012, 17, 314–326. [Google Scholar] [CrossRef] [PubMed]
- MCracken, L.M.; Vowles, K.E.; Eccleston, C. Acceptance of Chronic Pain: Component Analysis and a Revised Assessment Method. Pain 2004, 107, 159–166. [Google Scholar] [CrossRef] [PubMed]
- Rodero, B.; García-Campayo, J.; Casanueva, B.; del Hoyo, Y.L.; Serrano-Blanco, A.; Luciano, J.V. Validation of the Spanish Version of the Chronic Pain Acceptance Questionnaire (CPAQ) for the Assessment of Acceptance in Fibromyalgia. Health Qual. Life Outcomes 2010, 8, 37. [Google Scholar] [CrossRef] [PubMed]
- Chaves, J.E.; Brown, J.M. Spontaneous cognitive strategies for the control of clinical pain and stress. J. Behav. Med. 1987, 10, 263–276. [Google Scholar] [CrossRef]
- Rosenstiel, A.K.; Keefe, E.J. The use of coping strategies in chronic low back pain patients: Relationship to patient characteristics and current adjustment. Pain 1983, 17, 33–44. [Google Scholar] [CrossRef]
- Jensen, M.; Keefe, F.; Lefebvre, J.; Romano, J.; Turner, J. One-and Two-Item Measures of Pain Beliefs and Coping Strategies. Pain 2003, 104, 453–459. [Google Scholar] [CrossRef]
- Zigmond, A.S.; Snaith, R.P. The Hospital Anxiety and Depression Scale. Acta Psychiatr. Scand. 1983, 67, 361–370. [Google Scholar] [CrossRef]
- Quintana, J.M.; Padierna, A.; Esteban, C.; Arostegui, I.; Bilbao, A.; Ruiz, I. Evaluation of the Psychometric Characteristics of the Spanish Version of the Hospital Anxiety and Depression Scale. Acta Psychiatr. Scand. 2003, 107, 216–221. [Google Scholar] [CrossRef]
- Herrero, M.J.; Blanch, J.; Peri, J.M.; De Pablo, J.; Pintor, L.; Bulbena, A. A validation study of the hospital anxiety and depression scale (HADS) in a Spanish population. Gen. Hosp. Psychiatry 2003, 25, 277–283. [Google Scholar] [CrossRef]
- Terol-Cantero, M.C.; Cabrera-Perona, V. Hospital Anxiety and Depression Scale (HADS) review in Spanish Samples. Anales Psicología 2015, 31, 494. [Google Scholar] [CrossRef]
- Butler, S.; Budman, S.; Fernandez, K.; Houle, B.; Benoit, C.; Katz, N.; Jamison, R. Development and Validation of the Current Opioid Misuse Measure. Pain 2007, 130, 144–156. [Google Scholar] [CrossRef] [PubMed]
- Butler, S.; Budman, S.; Fanciullo, G.; Jamison, R. Cross Validation of the Current Opioid Misuse Measure (COMM) to Monitor Chronic Pain Patients on Opioid Therapy. Clin. J. Pain 2010, 26, 770–776. [Google Scholar] [CrossRef] [PubMed]
- Batista, J.; Coenders, G. Modelos de Ecuaciones Estructurales; La Muralla: Madrid, España, 2000. [Google Scholar]
- Bentler, P.M. Comparative Fit Indexes in Structural Models. Psychol. Bull. 1990, 107, 238. [Google Scholar] [CrossRef] [PubMed]
- Kline, R. Principles and Practice of Structural Equation Modelling, 3rd ed.; Guilford Press: New York, NY, USA, 2005. [Google Scholar]
- Hu, L.T.; Bentler, P.M. Fit Indices in Covariance Structure Modeling: Sensitivity to Underparameterized Model Misspecification. Psychol. Methods 1998, 3, 424–453. [Google Scholar] [CrossRef]
- Hu, L.-T.; Bentler, P.M. Structural Equation Modeling: A Multidisciplinary Journal Cutoff Criteria for Fit Indexes in Covariance Structure Analysis: Conventional Criteria versus New Alternatives. Multidiscip J. 2009, 6, 1–55. [Google Scholar] [CrossRef]
- Treede, R.-D.; Rief, W.; Barke, A.; Aziz, Q.; Bennett, M.I.; Benoliel, R.; Cohen, M.; Evers, S.; Finnerup, N.B.; First, M.B.; et al. Chronic pain as a symptom or a disease: The IASP Classification of Chronic Pain for the International Classification of Diseases (ICD-11). Pain 2019, 160, 19–27. [Google Scholar] [CrossRef]
- Cohen, J. Statistical Power Analysis for the Behavioral Sciences, 2nd ed.; Lawrence Erlbaum Associates Inc.: Hillsdale, NJ, USA, 1988. [Google Scholar]
- Dowell, D.; Haegerich, T.; Chou, R. CDC Guidelines for Prescribing Opioids for Chronic Pain—United States, 2016. JAMA 2016, 315, 1624–1645. [Google Scholar] [CrossRef]
- Blanco, C.; Wall, M.M.; Okuda, M.; Wang, S.; Iza, M.; Olfson, M. Pain as a Predictor of Opioid Use Disorder in a Nationally Representative Sample. Am. J. Psychiatry 2016, 173, 1189–1195. [Google Scholar] [CrossRef]
- Novak, S.P.; Glasheen, C.; Roland, C.L. Prescription pain reliever misuse and levels of pain impairment: 3-year course in a nationally representative outpatient sample of US adults. Subst. Abuse Rehabil. 2016, 7, 87–98. [Google Scholar] [CrossRef]
- Martel, M.O.; Dolman, A.J.; Edwards, R.R.; Jamison, R.N.; Wasan, A.D. The association between negative affect and prescription opioid misuse in patients with chronic pain: The mediating role of opioid craving. J. Pain 2014, 15, 90–100. [Google Scholar] [CrossRef] [PubMed]
- Martel, M.O.; Finan, P.H.; McHugh, R.K.; Issa, M.; Edwards, R.R.; Jamison, R.N.; Wasan, A.D. Day-to-day pain symptoms are only weakly associated with opioid craving among patients with chronic pain prescribed opioid therapy. Drug Alcohol Depend. 2016, 162, 130–136. [Google Scholar] [CrossRef] [PubMed]
- Garland, E.L.; Brown, S.M.; Howard, M.O. Thought suppression as a mediator of the association between depressed mood and prescription opioid craving among chronic pain patients. J. Behav. Med. 2016, 39, 128–138. [Google Scholar] [CrossRef] [PubMed]
- Wasan, A.D.; Ross, E.L.; Michna, E.; Chibnik, L.; Greenfield, S.F.; Weiss, R.D.; Jamison, R.N. Craving of prescription opioids in patients with chronic pain: A longitudinal outcomes trial. J. Pain 2012, 13, 146–154. [Google Scholar] [CrossRef]
- Wasan, A.D.; Butler, S.F.; Budman, S.H.; Fernandez, K.; Weiss, R.D.; Greenfield, S.F.; Jamison, R.N. Does report of craving opioid medication predict aberrant drug behavior among chronic pain patients? Clin. J. Pain 2009, 25, 193–198. [Google Scholar] [CrossRef]
- Martel, M.O.; Edwards, R.R.; Jamison, R.N. The relative contribution of pain and psychological factors to opioid misuse: A 6-month observational study. Am. Psychol. 2020, 75, 772–783. [Google Scholar] [CrossRef]
- Edwards, R.R.; Wasan, A.D.; Michna, E.; Greenbaum, S.; Ross, E.; Jamison, R.N. Elevated pain sensitivity in chronic pain patients at risk for opioid misuse. J. Pain 2011, 12, 953–963. [Google Scholar] [CrossRef]
- Ferrari, R.; Capraro, M.; Visentin, M. Risk factors in opioid treatment of chronic noncancer pain: A multidisciplinary assessment. In Pain Management: Current Issues and Opinions; Gabor, B., Noe, C.E., Eds.; Intech: Rijeka, Croatia, 2012; pp. 419–459. [Google Scholar]
- Jamison, R.N.; Link, C.L.; Marceau, L.D. Do pain patients at high risk for substance misuse experience more pain? A longitudinal outcomes study. Pain Med. 2009, 10, 1084–1094. [Google Scholar] [CrossRef]
- Martel, M.O.; Wasan, A.D.; Jamison, R.N.; Edwards, R.R. Catastrophic thinking and increased risk for prescription opioid misuse in patients with chronic pain. Drug Alcohol Depend. 2013, 132, 335–341. [Google Scholar] [CrossRef]
- Morasco, B.J.; Dobscha, S.K. Prescription medication misuse and substance use disorder in VA primary care patients with chronic pain. Gen. Hosp. Psychiatry 2008, 30, 93–99. [Google Scholar] [CrossRef] [PubMed]
- Martel, M.O.; Jamison, R.N.; Wasan, A.D.; Edwards, R.R. The association between catastrophizing and craving in patients with chronic pain prescribed opioid therapy: A preliminary analysis. Pain Med. 2014, 15, 1757–1764. [Google Scholar] [CrossRef] [PubMed]
- Hah, J.M.; Sturgeon, J.A.; Zocca, J.; Sharifzadeh, Y.; Mackey, S.C. Factors associated with prescription opioid misuse in a cross-sectional cohort of patients with chronic non-cancer pain. J. Pain Res. 2017, 10, 979. [Google Scholar] [CrossRef] [PubMed]
- Sullivan, M.J.L.; Bishop, S.R.; Pivik, J. The Pain Catastrophizing Scale: Development and validation. Psychol. Assess. 1995, 7, 524–532. [Google Scholar] [CrossRef]
- Lai, H.M.X.; Cleary, M.; Sitharthan, T.; Hunt, G.E. Prevalence of comorbid substance use, anxiety and mood disorders in epidemiological surveys, 1990–2014: A systematic review and meta-analysis. Drug Alcohol Depend. 2015, 154, 1–13. [Google Scholar] [CrossRef] [PubMed]
- Martins, S.S.; Fenton, M.C.; Keyes, K.M.; Blanco, C.; Zhu, H.; Storr, C.L. Mood and anxiety disorders and their association with non-medical prescription opioid use and prescription opioid-use disorder: Longitudinal evidence from the National Epidemiologic Study on Alcohol and Related Conditions. Psychol. Med. 2012, 42, 1261–1272. [Google Scholar] [CrossRef]
- Goldner, E.M.; Lusted, A.; Roerecke, M.; Rehm, J.; Fischer, B. Prevalence of Axis-1 psychiatric (with focus on depression and anxiety) disorder and symptomatology among non-medical prescription opioid users in substance use treatment: Systematic review and meta-analyses. Addict. Behav. 2014, 39, 520–531. [Google Scholar] [CrossRef]
- de Heer, E.W.; Gerrits, M.M.J.G.; Beekman, A.T.F.; Dekker, J.; van Marwijk, H.W.J.; de Waal, M.W.M.; Spinhoven, P.; Penninx, B.W.J.H.; van der Feltz-Cornelis, C.M. The association of depression and anxiety with pain: A study from NESDA. PLoS ONE 2014, 9, e106907. [Google Scholar] [CrossRef]
- Grattan, A.; Sullivan, M.D.; Saunders, K.W.; Campbell, C.I.; Von Korff, M.R. Depression and prescription opioid misuse among chronic opioid therapy recipients with no history of substance abuse. Ann. Fam. Med. 2012, 10, 304–311. [Google Scholar] [CrossRef] [PubMed]
- Gros, D.F.; Milanak, M.E.; Brady, K.T.; Back, S.E. Frequency and severity of comorbid mood and anxiety disorders in prescription opioid dependence. Am. J. Addict. 2013, 22, 261–265. [Google Scholar] [CrossRef] [PubMed]
- Feingold, D.; Brill, S.; Goor-Aryeh, I.; Delayahu, Y.; Lev-Ran, S. Misuse of prescription opioids among chronic pain patients suffering from anxiety: A cross-sectional analysis. Gen. Hosp. Psychiatry 2017, 47, 36–42. [Google Scholar] [CrossRef]
- Feingold, D.; Brill, S.; Goor-Aryeh, I.; Delayahu, Y.; Lev-Ran, S. The association between severity of depression and prescription opioid misuse among chronic pain patients with and without anxiety: A cross-sectional study. J. Affect. Disord. 2018, 235, 293–302. [Google Scholar] [CrossRef]
- Rogers, A.H.; Bakhshaie, J.; Lam, H.; Langdon, K.J.; Ditre, J.W.; Zvolensky, M.J. Pain-related anxiety and opioid misuse in a racially/ethnically diverse young adult sample with moderate/severe pain. Cog. Behav. Ther. 2018, 47, 372–382. [Google Scholar] [CrossRef]
- Van Rijswijk, S.M.; van Beek, M.H.C.T.; Schoof, G.M.; Schene, A.H.; Steegers, M.; Schellekens, A.F. Iatrogenic opioid use disorder, chronic pain and psychiatric comorbidity: A systematic review. Gen. Hosp. Psychiatry 2019, 59, 37–50. [Google Scholar] [CrossRef]
- Baker, T.B.; Piper, M.E.; McCarthy, D.E.; Majeskie, M.R.; Fiore, M.C. Addiction motivation reformulated: An affective processing model of negative reinforcement. Psychol. Rev. 2004, 111, 33. [Google Scholar] [CrossRef] [PubMed]
- McCarthy, D.E.; Curtin, J.J.; Piper, M.E.; Baker, T.B. Negative Reinforcement: Possible Clinical Implications of an Integrative Model. In Substance Abuse and Emotion; Kassel, K.D., Ed.; American Psychological Association: Washington, DC, USA, 2010; pp. 15–42. [Google Scholar] [CrossRef]
- Evans, C.J.; Cahill, C.M. Neurobiology of opioid dependence in creating addiction vulnerability. F1000Research 2016, 5, 1748. [Google Scholar] [CrossRef]
- Koob, G.F. Neurobiology of opioid addiction: Opponent process, hyperkatifeia, and negative reinforcement. Biol. Psychiatry 2020, 87, 44–53. [Google Scholar] [CrossRef] [PubMed]
- Langdon, K.J.; Dove, K.; Ramsey, S. Comorbidity of opioid-related and anxiety-related symptoms and disorders. Curr. Opin. Psychol. 2019, 30, 17–23. [Google Scholar] [CrossRef]
- Rogers, A.H.; Garey, L.; Bakhshaie, J.; Viana, A.G.; Ditre, J.W.; Zvolensky, M.J. Anxiety, depression, and opioid misuse among adults with chronic pain: The role of anxiety sensitivity. Clin. J. Pain 2020, 36, 862–867. [Google Scholar] [CrossRef]
- Rogers, A.H.; Orr, M.F.; Shepherd, J.M.; Bakhshaie, J.; Ditre, J.W.; Buckner, J.D.; Zvolensky, M.J. Anxiety, depression, and opioid misuse among adults with chronic pain: The role of emotion dysregulation. J. Behav. Med. 2021, 44, 66–73. [Google Scholar] [CrossRef] [PubMed]
- Kathryn McHugh, R.; Otto, M.W. Profiles of distress intolerance in a substance-dependent sample. Am J Drug Alcohol Abuse 2012, 38, 161–165. [Google Scholar] [CrossRef] [PubMed]
- Ramírez-Maestre, C.; Reyes-Pérez, A.; Esteve, R.; López-Martínez, A.E.; Bernardes, S.; Jensen, M.P. Opioid Pain Medication Prescription for Chronic Pain in Primary Care Centers: The Roles of Pain Acceptance, Pain Intensity, Depressive Symptoms, Pain Catastrophizing, Sex, and Age. Int. J. Environ. Res. Public Health 2020, 17, 6428. [Google Scholar] [CrossRef] [PubMed]
- McCracken, L.M.; Vowles, K.E. Acceptance and commitment therapy and mindfulness for chronic pain: Model, process, and progress. Am. Psychol. 2014, 69, 178. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| M | SD | Range | 1 | 2 | 3 | 4 | 5 | 6 | |
|---|---|---|---|---|---|---|---|---|---|
| 1. Pain acceptance | 17.39 | 13.78 | 0–46 | 1 | |||||
| 2. Anxiety | 19.80 | 5.77 | 7–28 | −0.37 ** | 1 | ||||
| 3. Depression | 15.77 | 5.08 | 7–27 | −0.55 ** | 0.55 ** | 1 | |||
| 4. Catastrophizing | 5.47 | 2.18 | 2–8 | −0.48 ** | 0.46 ** | 0.62 ** | 1 | ||
| 5. Pain intensity | 6.94 | 1.67 | 0–10 | −0.35 ** | 0.20 * | 0.27 ** | 0.29 ** | 1 | |
| 6. Opioid misuse | 15.55 | 8.64 | 0–39 | −0.28** | 0.57 ** | 0.52 ** | 0.44 ** | 0.16 | 1 |
| Pain Acceptance | Opioid Misuse | |
|---|---|---|
| γ | β | |
| Pain intensity | −0.27 * | 0.06 |
| Pain catastrophizing | −0.36 * | 0.12 |
| Anxiety | −0.40 * | 0.36 * |
| Depression | −0.51 * | 0.25 * |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Esteve, R.; Marcos, E.; Reyes-Pérez, Á.; López-Martínez, A.E.; Ramírez-Maestre, C. Pain Acceptance Creates an Emotional Context That Protects against the Misuse of Prescription Opioids: A Study in a Sample of Patients with Chronic Noncancer Pain. Int. J. Environ. Res. Public Health 2021, 18, 3054. https://doi.org/10.3390/ijerph18063054
Esteve R, Marcos E, Reyes-Pérez Á, López-Martínez AE, Ramírez-Maestre C. Pain Acceptance Creates an Emotional Context That Protects against the Misuse of Prescription Opioids: A Study in a Sample of Patients with Chronic Noncancer Pain. International Journal of Environmental Research and Public Health. 2021; 18(6):3054. https://doi.org/10.3390/ijerph18063054
Chicago/Turabian StyleEsteve, Rosa, Estefanía Marcos, Ángela Reyes-Pérez, Alicia E. López-Martínez, and Carmen Ramírez-Maestre. 2021. "Pain Acceptance Creates an Emotional Context That Protects against the Misuse of Prescription Opioids: A Study in a Sample of Patients with Chronic Noncancer Pain" International Journal of Environmental Research and Public Health 18, no. 6: 3054. https://doi.org/10.3390/ijerph18063054
APA StyleEsteve, R., Marcos, E., Reyes-Pérez, Á., López-Martínez, A. E., & Ramírez-Maestre, C. (2021). Pain Acceptance Creates an Emotional Context That Protects against the Misuse of Prescription Opioids: A Study in a Sample of Patients with Chronic Noncancer Pain. International Journal of Environmental Research and Public Health, 18(6), 3054. https://doi.org/10.3390/ijerph18063054