
Development of the “National Asbestos Profile” to Eliminate Asbestos-Related Diseases in 195 Countries

 , ,
, ,  , and
, and
Abstract
1. Introduction
2. Materials and Methods
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Appendix A

{kind=link}
| Country | Reference |
|---|---|
| Australia | Asbestos Safety and Eradiation Agency. 2017. National Asbestos Profile for Australia. Available online: https://www.asbestossafety.gov.au/sites/default/files/documents/2017-12/ASEA_National_Asbestos_Profile_interactive_Nov17.pdf (accessed on 11 January 2021). [26] |
| Bangladesh | Bangladesh Occupational Safety, Health and Environment Foundation. 2016. National Asbestos Profile of Bangladesh. Obtained via personal communication: 20 April 2020. [27] |
| Bulgaria | Vangelova, K.; Dimitrova, S.; Dimitrova, I. 2015. National Asbestos Profile of Bulgaria. Available online: https://ncpha.government.bg/files/National%20Asbestos%20Profile_Bulgaria_2015-en.pdf (accessed on 11 January 2021). [28] |
| Cambodia | Ministry of Labor and Vocational Training. 2019. Cambodia National Asbestos Profile. Personal Communication, 2020. [29] |
| Germany | Federal Institute for Occupational Health and Safety. 2014. National Asbestos Profile for Germany. Available online: https://www.baua.de/EN/Service/Publications/Report/Gd80.pdf?__blob=publicationFile&v=8 (accessed on 11 January 2021). [30] |
| India | People’s Training & Research and Centre. 2017. India: National Asbestos Profile. Available online: https://amrc.org.hk/sites/default/files/NAP%20India.pdf (accessed on 11 January 2021). [31] |
| Indonesia | Indonesia Ban Asbestos Network. 2017. National Asbestos Profile Indonesia. Obtained via personal communication: 28 April 2020. [32] |
| Japan | Furuya, S.; Takahashi, K.; Mohaved, M.; Jiang, Y. 2013. National Asbestos Profile of Japan. Available online: https://www.researchgate.net/publication/237839114_National_Asbestos_Profile_of_Japan_-_Based_on_the_National_Asbestos_Profile_by_the_ILO_and_the_WHO (accessed on 11 January 2021) [33] |
| Laos | Laos Ministry of Industry and Commerce. 2017. National Asbestos Profile of Laos. Personal Communication, 2020. [34] |
| North Macedonia | Institute of Occupational Health of the Republic of Macedonia. 2014. National Asbestos Profile for the Republic of Macedonia. Personal Communication, 2020. [35] |
| Mongolia | Health Sciences University of Mongolia. 2012. National Asbestos Profile of Mongolia. Personal Communication, 2020. [36] |
| Nepal | Sah, R.C. 2016. National Asbestos Profile of Nepal. Available online: http://anroev.org/aban/wp-content/uploads/2016/10/National-Abestos-Profile-of-Nepal.pdf (accessed on 11 January 2021). [37] |
| Philippines | Republic of Philippines, Environmental and Occupational Health Office. 2013. National Asbestos Profile Philippines. Available online: https://www.informea.org/en/national-asbestos-profile-nap-philippines (accessed on 11 January 2021). [38] |
| Vietnam | Pham, V.H.; Tran, T.N.L.; Le, G.V.; Movahed, M.; Jiang, Y.; Pham, N.H.; Ogawa, H; Takahashi, K. Asbestos and asbestos-related diseases in Vietnam: In reference to the International Labor Organization/World Health Organization National Asbestos Profile. Saf. Health Work. 2013, 4, 117–121. doi:10.1016/j.shaw.2013.04.002. [39] |
| Asbestos Data | Disease Data | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Countries 1 | World Bank Income Group 2 | Asbestos Ban Status 3 | NAP Country Category 4 | Consumption of Raw Asbestos (USGS) 5 | Asbestos-Containing Material (UN Comtrade) 6 | Reported Mortality of Mesothelioma or Asbestosis (WHO MDB) 7 | Estimated Incidence of Mesothelioma (GBD) 8 | Estimated Mortality of Mesothelioma (WHO GHE) 9 | Reported or estimated Mortality of Mesothelioma (WHO GCO) 10 | |
| 1 | Afghanistan | LI | No-Ban | C | Yes | No | No | Yes | Yes | Yes |
| 2 | Albania | UMI | No-Ban | C | Yes | Yes | No | Yes | Yes | Yes |
| 3 | Algeria | LMI | Ban | C | Yes | Yes | No | Yes | Yes | Yes |
| 4 | Andorra | HI | No-Ban | C | No | Yes | No | Yes | No | No |
| 5 | Angola | LMI | No-Ban | D | Yes | Yes | No | Yes | Yes | Yes |
| 6 | Antigua and Barbuda | HI | No-Ban | D | Yes | Yes | No | Yes | No | No |
| 7 | Argentina | UMI | Ban | B | Yes | Yes | Yes | Yes | Yes | Yes |
| 8 | Armenia | UMI | No-Ban | D | Yes | Yes | Yes | Yes | Yes | Yes |
| 9 | Australia | HI | Ban | A | Yes | Yes | Yes | Yes | Yes | Yes |
| 10 | Austria | HI | Ban | B | Yes | Yes | Yes | Yes | Yes | Yes |
| 11 | Azerbaijan | UMI | No-Ban | C | Yes | Yes | No | Yes | Yes | Yes |
| 12 | Bahamas | HI | No-Ban | C | Yes | Yes | Yes | No | Yes | No |
| 13 | Bahrain | HI | Ban | B | No | Yes | Yes | Yes | Yes | Yes |
| 14 | Bangladesh | LMI | No-Ban | A | Yes | Yes | No | Yes | Yes | Yes |
| 15 | Barbados | HI | No-Ban | B | Yes | Yes | Yes | Yes | Yes | No |
| 16 | Belarus | UMI | No-Ban | D | Yes | Yes | No | Yes | Yes | Yes |
| 17 | Belgium | HI | Ban | B | Yes | Yes | Yes | Yes | Yes | Yes |
| 18 | Belize | UMI | No-Ban | D | Yes | Yes | Yes | Yes | Yes | No |
| 19 | Benin | LMI | No-Ban | D | Yes | Yes | No | Yes | Yes | Yes |
| 20 | Bhutan | LMI | No-Ban | C | Yes | Yes | No | Yes | Yes | No |
| 21 | Bolivia | LMI | No-Ban | B | Yes | Yes | Yes | Yes | Yes | Yes |
| 22 | Bosnia and Herzegovina | UMI | No-Ban | B | Yes | Yes | Yes | Yes | Yes | Yes |
| 23 | Botswana | UMI | No-Ban | C | Yes | Yes | No | Yes | Yes | No |
| 24 | Brazil | UMI | Ban | B | Yes | Yes | Yes | Yes | Yes | Yes |
| 25 | Brunei | HI | Ban | C | Yes | Yes | No | Yes | Yes | No |
| 26 | Bulgaria | UMI | Ban | A | Yes | Yes | Yes | Yes | Yes | Yes |
| 27 | Burkina Faso | LI | No-Ban | D | No | Yes | No | Yes | Yes | Yes |
| 28 | Burundi | LI | No-Ban | D | Yes | Yes | No | Yes | Yes | Yes |
| 29 | Cambodia | LMI | No-Ban | A | Yes | Yes | No | Yes | Yes | Yes |
| 30 | Cameroon | LMI | No-Ban | D | Yes | Yes | No | Yes | Yes | No |
| 31 | Canada | HI | Ban | B | Yes | Yes | Yes | Yes | Yes | Yes |
| 32 | Cape Verde | LMI | No-Ban | C | No | Yes | No | Yes | Yes | No |
| 33 | Central African Republic | LI | No-Ban | D | No | Yes | No | Yes | Yes | No |
| 34 | Chad | LI | No-Ban | C | Yes | No | No | Yes | Yes | No |
| 35 | Chile | HI | Ban | B | Yes | Yes | Yes | Yes | Yes | Yes |
| 36 | China | UMI | No-Ban | B | Yes | Yes | No | Yes | Yes | Yes |
| 37 | Colombia | UMI | Ban | B | Yes | Yes | Yes | Yes | Yes | Yes |
| 38 | Comoros | LMI | No-Ban | D | No | Yes | No | Yes | Yes | No |
| 39 | Congo–Brazzaville | LMI | No-Ban | D | Yes | Yes | No | Yes | Yes | Yes |
| 40 | Congo–Kinshasa (DR Congo) | LI | No-Ban | C | Yes | No | No | Yes | No | Yes |
| 41 | Costa Rica | UMI | No-Ban | B | Yes | Yes | Yes | Yes | Yes | No |
| 42 | Côte d’Ivoire | LMI | No-Ban | C | Yes | Yes | No | Yes | Yes | Yes |
| 43 | Croatia | HI | Ban | B | Yes | Yes | Yes | Yes | Yes | Yes |
| 44 | Cuba | UMI | No-Ban | C | Yes | Yes | Yes | Yes | Yes | Yes |
| 45 | Cyprus | HI | Ban | B | Yes | Yes | Yes | Yes | Yes | Yes |
| 46 | Czech Republic | HI | Ban | B | Yes | Yes | Yes | Yes | Yes | Yes |
| 47 | Denmark | HI | Ban | B | Yes | Yes | Yes | Yes | Yes | Yes |
| 48 | Djibouti | LMI | Ban | C | Yes | No | No | Yes | Yes | No |
| 49 | Dominica | UMI | No-Ban | D | Yes | Yes | No | Yes | Yes | No |
| 50 | Dominican Republic | UMI | No-Ban | D | Yes | Yes | Yes | Yes | Yes | Yes |
| 51 | Ecuador | UMI | No-Ban | B | Yes | Yes | Yes | Yes | Yes | Yes |
| 52 | Egypt | LMI | Ban | B | Yes | Yes | Yes | Yes | Yes | Yes |
| 53 | El Salvador | LMI | No-Ban | D | Yes | Yes | Yes | Yes | Yes | No |
| 54 | Equatorial Guinea | UMI | No-Ban | D | No | No | No | Yes | Yes | No |
| 55 | Eritrea | LI | No-Ban | D | Yes | No | No | Yes | Yes | Yes |
| 56 | Estonia | HI | Ban | B | Yes | Yes | Yes | Yes | Yes | Yes |
| 57 | Eswatini Swaziland | LMI | No-Ban | C | Yes | Yes | No | Yes | Yes | No |
| 58 | Ethiopia | LI | No-Ban | C | Yes | Yes | No | Yes | Yes | Yes |
| 59 | Fiji | UMI | No-Ban | B | Yes | Yes | Yes | Yes | No | No |
| 60 | Finland | HI | Ban | B | Yes | Yes | Yes | Yes | Yes | Yes |
| 61 | France | HI | Ban | B | Yes | Yes | Yes | Yes | Yes | Yes |
| 62 | Gabon | UMI | Ban | C | Yes | Yes | No | Yes | Yes | No |
| 63 | Gambia | LI | No-Ban | C | No | Yes | No | Yes | Yes | No |
| 64 | Georgia | UMI | No-Ban | C | Yes | Yes | Yes | Yes | Yes | Yes |
| 65 | Germany | HI | Ban | A | Yes | Yes | Yes | Yes | Yes | Yes |
| 66 | Ghana | LMI | No-Ban | B | Yes | Yes | No | Yes | Yes | Yes |
| 67 | Greece | HI | Ban | B | Yes | Yes | Yes | Yes | Yes | Yes |
| 68 | Grenada | UMI | No-Ban | C | No | Yes | Yes | Yes | No | No |
| 69 | Guatemala | UMI | No-Ban | C | Yes | Yes | Yes | Yes | Yes | No |
| 70 | Guinea | LI | No-Ban | D | Yes | Yes | No | Yes | Yes | No |
| 71 | Guinea-Bissau | LI | No-Ban | D | No | Yes | No | Yes | Yes | No |
| 72 | Guyana | UMI | No-Ban | C | Yes | Yes | Yes | Yes | Yes | No |
| 73 | Haiti | LI | No-Ban | C | Yes | No | No | Yes | Yes | Yes |
| 74 | Honduras | LMI | Ban | C | Yes | Yes | No | Yes | Yes | Yes |
| 75 | Hong Kong 1 | HI | No-Ban | B | Yes | Yes | Yes | No | No | No |
| 76 | Hungary | HI | Ban | B | Yes | Yes | Yes | Yes | Yes | Yes |
| 77 | Iceland | HI | Ban | B | Yes | Yes | Yes | Yes | Yes | Yes |
| 78 | India | LMI | No-Ban | A | Yes | Yes | No | Yes | Yes | Yes |
| 79 | Indonesia | UMI | No-Ban | A | Yes | Yes | No | Yes | Yes | Yes |
| 80 | Iran | UMI | No-Ban | B | Yes | Yes | Yes | Yes | Yes | Yes |
| 81 | Iraq | UMI | Ban | B | Yes | No | Yes | Yes | Yes | Yes |
| 82 | Ireland | HI | Ban | B | Yes | Yes | Yes | Yes | Yes | Yes |
| 83 | Israel | HI | Ban | B | Yes | Yes | Yes | Yes | Yes | Yes |
| 84 | Italy | HI | Ban | B | Yes | Yes | Yes | Yes | Yes | Yes |
| 85 | Jamaica | UMI | No-Ban | B | Yes | Yes | Yes | Yes | Yes | Yes |
| 86 | Japan | HI | Ban | A | Yes | Yes | Yes | Yes | Yes | Yes |
| 87 | Jordan | UMI | Ban | B | Yes | Yes | Yes | Yes | Yes | Yes |
| 88 | Kazakhstan | UMI | No-Ban | B | Yes | Yes | Yes | Yes | Yes | Yes |
| 89 | Kenya | LMI | No-Ban | B | Yes | Yes | No | Yes | Yes | Yes |
| 90 | Kiribati | LMI | No-Ban | B | No | Yes | No | Yes | Yes | No |
| 91 | Kuwait | HI | Ban | C | Yes | Yes | Yes | Yes | Yes | Yes |
| 92 | Kyrgyzstan | LMI | No-Ban | D | Yes | Yes | Yes | Yes | Yes | Yes |
| 93 | Laos | LMI | No-Ban | A | Yes | Yes | No | Yes | Yes | Yes |
| 94 | Latvia | HI | Ban | B | Yes | Yes | Yes | Yes | Yes | Yes |
| 95 | Lebanon | UMI | No-Ban | B | Yes | Yes | No | Yes | Yes | Yes |
| 96 | Lesotho | LMI | No-Ban | B | No | Yes | No | Yes | Yes | Yes |
| 97 | Liberia | LI | No-Ban | B | Yes | No | No | Yes | Yes | Yes |
| 98 | Libya | UMI | No-Ban | B | Yes | Yes | No | Yes | Yes | Yes |
| 99 | Liechtenstein | HI | Ban | B | No | No | No | No | No | No |
| 100 | Lithuania | HI | Ban | B | Yes | Yes | Yes | Yes | Yes | Yes |
| 101 | Luxembourg | HI | Ban | C | Yes | Yes | Yes | Yes | Yes | Yes |
| 102 | Madagascar | LI | No-Ban | C | Yes | Yes | No | Yes | Yes | Yes |
| 103 | Malawi | LI | No-Ban | C | Yes | Yes | No | Yes | Yes | No |
| 104 | Malaysia | UMI | No-Ban | B | Yes | Yes | No | Yes | Yes | Yes |
| 105 | Maldives | UMI | No-Ban | C | Yes | Yes | Yes | Yes | Yes | No |
| 106 | Mali | LI | No-Ban | D | Yes | Yes | No | Yes | Yes | Yes |
| 107 | Malta | HI | Ban | B | Yes | Yes | Yes | Yes | Yes | Yes |
| 108 | Marshall Islands | UMI | No-Ban | B | No | No | No | Yes | No | No |
| 109 | Mauritania | LMI | No-Ban | D | No | Yes | No | Yes | Yes | No |
| 110 | Mauritius | HI | Ban | B | Yes | Yes | Yes | Yes | No | No |
| 111 | Mexico | UMI | No-Ban | B | Yes | Yes | Yes | Yes | Yes | Yes |
| 112 | Micronesia | LMI | No-Ban | B | No | Yes | No | Yes | Yes | No |
| 113 | Moldova | LMI | No-Ban | C | Yes | Yes | Yes | Yes | Yes | Yes |
| 114 | Monaco | HI | Ban | B | No | No | No | No | No | No |
| 115 | Mongolia | LMI | No-Ban | A | Yes | Yes | Yes | Yes | Yes | Yes |
| 116 | Montenegro | UMI | No-Ban | C | Yes | Yes | Yes | Yes | Yes | No |
| 117 | Morocco | LMI | No-Ban | C | Yes | Yes | Yes | Yes | Yes | Yes |
| 118 | Mozambique | LI | Ban | B | Yes | Yes | No | Yes | Yes | Yes |
| 119 | Myanmar | LMI | No-Ban | D | Yes | Yes | No | Yes | Yes | Yes |
| 120 | Namibia | UMI | No-Ban | C | Yes | Yes | No | Yes | Yes | Yes |
| 121 | Nauru | HI | No-Ban | B | No | No | No | No | No | No |
| 122 | Nepal | LMI | No-Ban | A | Yes | Yes | No | Yes | Yes | Yes |
| 123 | Netherlands | HI | Ban | B | Yes | Yes | Yes | Yes | Yes | Yes |
| 124 | New Zealand | HI | Ban | B | Yes | Yes | Yes | Yes | Yes | Yes |
| 125 | Nicaragua | LMI | No-Ban | D | Yes | Yes | Yes | Yes | Yes | Yes |
| 126 | Niger | LI | No-Ban | D | Yes | Yes | No | Yes | Yes | No |
| 127 | Nigeria | LMI | No-Ban | B | Yes | Yes | No | Yes | Yes | Yes |
| 128 | North Korea | LI | No-Ban | D | Yes | No | No | Yes | Yes | Yes |
| 129 | North Macedonia | UMI | Ban | A | Yes | Yes | Yes | Yes | Yes | No |
| 130 | Norway | HI | Ban | B | Yes | Yes | Yes | Yes | Yes | Yes |
| 131 | Oman | HI | Ban | B | Yes | Yes | Yes | Yes | Yes | Yes |
| 132 | Pakistan | LMI | No-Ban | B | Yes | Yes | No | Yes | Yes | Yes |
| 133 | Palau | HI | No-Ban | B | No | Yes | No | No | No | No |
| 134 | Panama | HI | No-Ban | C | Yes | Yes | Yes | Yes | Yes | Yes |
| 135 | Papua New Guinea | LMI | No-Ban | C | No | Yes | No | Yes | Yes | Yes |
| 136 | Paraguay | UMI | No-Ban | C | Yes | Yes | Yes | Yes | Yes | No |
| 137 | Peru | UMI | No-Ban | B | Yes | Yes | Yes | Yes | Yes | Yes |
| 138 | Philippines | LMI | No-Ban | A | Yes | Yes | Yes | Yes | Yes | Yes |
| 139 | Poland | HI | Ban | B | Yes | Yes | Yes | Yes | Yes | Yes |
| 140 | Portugal | HI | Ban | B | Yes | Yes | Yes | Yes | Yes | Yes |
| 141 | Qatar | HI | Ban | B | Yes | Yes | No | Yes | Yes | Yes |
| 142 | Romania | HI | Ban | B | Yes | Yes | Yes | Yes | Yes | Yes |
| 143 | Russia | UMI | No-Ban | B | Yes | Yes | No | Yes | Yes | Yes |
| 144 | Rwanda | LI | No-Ban | B | Yes | Yes | No | Yes | Yes | Yes |
| 145 | Saint Kitts and Nevis | HI | No-Ban | C | No | Yes | No | No | No | No |
| 146 | Saint Lucia | UMI | No-Ban | C | No | Yes | Yes | Yes | Yes | No |
| 147 | Saint Vincent and Grenadines | UMI | No-Ban | D | Yes | Yes | No | Yes | No | No |
| 148 | Samoa | UMI | No-Ban | B | Yes | Yes | No | Yes | Yes | No |
| 149 | San Marino | HI | No-Ban | B | No | Yes | No | No | No | No |
| 150 | São Tomé and Príncipe | LMI | No-Ban | C | No | Yes | No | Yes | Yes | No |
| 151 | Saudi Arabia | HI | Ban | B | Yes | Yes | Yes | Yes | Yes | Yes |
| 152 | Senegal | LMI | No-Ban | C | Yes | Yes | No | Yes | Yes | Yes |
| 153 | Serbia | UMI | Ban | B | Yes | Yes | Yes | Yes | Yes | Yes |
| 154 | Seychelles | HI | Ban | C | Yes | Yes | No | Yes | Yes | No |
| 155 | Sierra Leone | LI | No-Ban | D | Yes | Yes | No | Yes | Yes | No |
| 156 | Singapore | HI | No-Ban | B | Yes | Yes | Yes | Yes | Yes | Yes |
| 157 | Slovakia | HI | Ban | B | Yes | Yes | Yes | Yes | Yes | Yes |
| 158 | Slovenia | HI | Ban | B | Yes | Yes | Yes | Yes | Yes | Yes |
| 159 | Solomon Islands | LMI | No-Ban | B | No | Yes | No | Yes | Yes | No |
| 160 | Somalia | LI | No-Ban | D | No | No | No | Yes | Yes | Yes |
| 161 | South Africa | UMI | Ban | B | Yes | Yes | Yes | Yes | Yes | Yes |
| 162 | South Korea | HI | Ban | B | Yes | Yes | Yes | Yes | Yes | Yes |
| 163 | South Sudan | LI | No-Ban | B | No | Yes | No | Yes | Yes | Yes |
| 164 | Spain | HI | Ban | B | Yes | Yes | Yes | Yes | Yes | Yes |
| 165 | Sri Lanka | LMI | No-Ban | B | Yes | Yes | Yes | Yes | Yes | Yes |
| 166 | Sudan | LI | No-Ban | C | Yes | Yes | No | Yes | Yes | Yes |
| 167 | Suriname | UMI | No-Ban | D | Yes | Yes | Yes | Yes | Yes | No |
| 168 | Sweden | HI | Ban | B | Yes | Yes | Yes | Yes | Yes | Yes |
| 169 | Switzerland | HI | Ban | B | Yes | Yes | Yes | Yes | Yes | Yes |
| 170 | Syria | LI | No-Ban | C | Yes | Yes | No | Yes | Yes | Yes |
| 171 | Taiwan 1 | HI | Ban | B | Yes | No | No | Yes | No | No |
| 172 | Tajikistan | LI | No-Ban | B | Yes | Yes | No | Yes | Yes | No |
| 173 | Tanzania | LMI | No-Ban | C | Yes | Yes | No | Yes | Yes | No |
| 174 | Thailand | UMI | No-Ban | B | Yes | Yes | Yes | Yes | Yes | Yes |
| 175 | Timor-Leste | LMI | No-Ban | B | No | Yes | No | Yes | Yes | No |
| 176 | Togo | LI | No-Ban | C | Yes | Yes | No | Yes | Yes | Yes |
| 177 | Tonga | UMI | No-Ban | B | No | Yes | No | Yes | Yes | No |
| 178 | Trinidad and Tobago | HI | No-Ban | C | Yes | Yes | Yes | Yes | Yes | No |
| 179 | Tunisia | LMI | No-Ban | C | Yes | Yes | Yes | Yes | Yes | Yes |
| 180 | Turkey | UMI | Ban | B | Yes | Yes | Yes | Yes | Yes | Yes |
| 181 | Turkmenistan | UMI | No-Ban | D | Yes | Yes | No | Yes | Yes | Yes |
| 182 | Tuvalu | UMI | No-Ban | B | No | Yes | No | No | No | No |
| 183 | Uganda | LI | No-Ban | B | Yes | Yes | No | Yes | Yes | Yes |
| 184 | Ukraine | LMI | No-Ban | B | Yes | Yes | No | Yes | Yes | Yes |
| 185 | United Arab Emirates | HI | No-Ban | B | Yes | Yes | No | Yes | Yes | Yes |
| 186 | United Kingdom | HI | Ban | B | Yes | Yes | Yes | Yes | Yes | Yes |
| 187 | United States of America | HI | No-Ban | B | Yes | Yes | Yes | Yes | Yes | Yes |
| 188 | Uruguay | HI | Ban | C | Yes | Yes | Yes | Yes | Yes | Yes |
| 189 | Uzbekistan | LMI | No-Ban | C | Yes | Yes | Yes | Yes | Yes | Yes |
| 190 | Vanuatu | LMI | No-Ban | B | Yes | Yes | No | Yes | Yes | No |
| 191 | Venezuela | UMI | No-Ban | B | Yes | Yes | Yes | Yes | Yes | Yes |
| 192 | Vietnam | LMI | No-Ban | A | Yes | Yes | No | Yes | Yes | Yes |
| 193 | Yemen | LI | No-Ban | D | Yes | Yes | No | Yes | Yes | Yes |
| 194 | Zambia | LMI | No-Ban | C | Yes | Yes | No | Yes | Yes | Yes |
| 195 | Zimbabwe | LMI | No-Ban | B | Yes | Yes | No | Yes | Yes | Yes |
| Total (Yes) | 165 | 179 | 96 | 186 | 178 | 134 | ||||
| Theme | Items of National Asbestos Profile | International Sources | National Sources, etc. | |||||
|---|---|---|---|---|---|---|---|---|
| Asbestos Data | Disease Data | |||||||
| Consumption of Raw Asbestos (USGS 1) | Asbestos-Containing Material (UN Comtrade 2) | Reported Mortality of Mesothelioma or Asbestosis (WHO MDB 3) | Estimated Incidence of Mesothelioma (GBD 4) | Estimated Mortality of Mesothelioma (WHO GHE 5) | Reported or estimated Mortality of Mesothelioma (WHO GCO 6) | |||
| Legislation | I-1. Current regulations on the different forms of asbestos I-15. National enforceable occupational exposure limits for chrysotile asbestos I-16. The system for inspection and enforcement of the exposure limits | I-1, I-15, I-16: Existing government laws and regulations | ||||||
| Asbestos | I-2. Import and consumption of asbestos per year (total and per major uses and forms) I-3. Import of asbestos-containing materials I-4. Domestic production of asbestos (if applicable) I-5. Domestic production of asbestos-containing materials | I-2, I-4 | I-3, I-5 | I-2, I-3: National trade statistics; I-4: National mining statistics; I-5: National manufacturing statistics | ||||
| Diseases | I-9. Estimate of the burden of diseases related to asbestos: disability adjusted life years and deaths attributable to asbestos exposure I-10. Prevalence of asbestosis – national data, a breakdown by industries if available I-11. Incidence of lung cancer among workers exposed to asbestos I-12. Incidence of mesothelioma I-17. Estimated economic losses due to asbestos-related diseases I-18. Major studies on epidemiology of asbestos-related diseases in the country | I-9 (reported deaths) | I-9, I-10, I-11, I-12 deaths, DALY) | I-9, I-12 (estimated | I-9, I-12 (reported a/o estimated deaths) | I-10: National compensation statistics; I-12: National/Regional Cancer Registry data; I-18: PUBMED | ||
| Risk Assessment | I-6. Estimated total number of workers exposed to asbestos in the country I-7. Full list of industries where exposure to asbestos is present in the country and list of industries with the largest numbers of workers potentially exposed to asbestos I-8. Industries with high risk of exposure (where overexposure is documented as exceeding occupational exposure limits) and estimated total number of workers at high risk I-13. Estimates on the percentage of house stock and vehicle fleet containing asbestos I-14. Total number of workers eligible for compensation for asbestos-related diseases, such as asbestosis, lung cancer and mesothelioma (per year) and the numbers of individuals compensated yearly | I-6, I-8: Industrial hygiene or occupational health data; I-7, I-13: Specific industry inventory; I-14: Occupational disease compensation data. | ||||||
References
- Institute for Health Metrics and Evaluation, Global Health Data Exchange. Global Burden of Disease Data. 2018. Available online: http://ghdx.healthdata.org/gbd-results-tool (accessed on 15 January 2021).
- World Health Organization. Elimination of Asbestos-Related Diseases. 2006. Available online: https://www.who.int/occupational_health/publications/asbestosrelateddiseases.pdf (accessed on 15 January 2021).
- International Labor Organization and World Health Organization. Outline for the Development of National Programs for Elimination of Asbestos-Related Diseases. 2007. Available online: https://www.who.int/occupational_health/publications/elim_asbestos_doc_en.pdf?ua=1 (accessed on 15 January 2021).
- International Labor Organization. Thirteenth Session of the Joint ILO/WHO Committee on Occupational Health. 2003. Available online: https://www.ilo.org/wcmsp5/groups/public/---ed_protect/---protrav/---safework/documents/publication/wcms_110478.pdf (accessed on 15 January 2021).
- Kazan-Allen, L. Current Asbestos Bans. 2019. Available online: http://www.ibasecretariat.org/alpha_ban_list.php (accessed on 15 January 2021).
- Takahashi, K.; Landrigan, P.J.; Ramazzini, C. The global health dimensions of asbestos and asbestos-related diseases. Ann. Glob. Health 2016, 82, 209–213. [Google Scholar] [CrossRef] [PubMed]
- Park, E.K.; Takahashi, K.; Hoshuyama, T.; Cheng, T.J.; Delgermaa, V.; Le, G.V.; Sorahan, T. Global magnitude of reported and unreported mesothelioma. Environ. Health Persp. 2011, 119, 514–518. [Google Scholar] [CrossRef] [PubMed]
- Lin, R.T.; Takahashi, K.; Karjalainen, A.; Hoshuyama, T.; Wilson, D.; Kameda, T.; Chan, C.C.; Wen, C.P.; Furuya, S.; Higashi, T.; et al. Ecological association between asbestos-related diseases and historical asbestos consumption: An international analysis. Lancet 2007, 369, 844–849. [Google Scholar] [CrossRef]
- Delgermaa, V.; Takahashi, K.; Park, E.K.; Le, G.V.; Hara, T.; Sorahan, T. Global mesothelioma deaths reported to the World Health Organization between 1994 and 2008. Bull. World Health Organ. 2011. [Google Scholar] [CrossRef] [PubMed]
- Chimed-Ochir, O.; Takahashi, K.; Sorahan, T.; Driscoll, T.; Fitzmaurice, C.; Yoko-o, M.; Sawanyawisuth, K.; Furuya, S.; Tanaka, F.; Horie, S.; et al. Estimation of the global burden of mesothelioma deaths from incomplete national mortality data. Occup. Environ. Med. 2017, 89, 716–724. [Google Scholar] [CrossRef]
- GBD 2016 Occupational Carcinogens Collaborators. Global and Regional Burden of Cancer in 2016 Arising from Occupational Exposure to Selected Carcinogens: A Systematic Analysis for the Global Burden of Disease Study 2016. Occup. Environ. Med. 2020, 77, 151–159. [Google Scholar] [CrossRef] [PubMed]
- Carbone, M.; Adusumilli, P.S.; Alexander, H.R., Jr.; Baas, P.; Bardelli, F.; Bononi, A.; Bueno, R.; Felley-Bosco, E.; Galateau-Salle, F.; Jablons, D.; et al. Mesothelioma: Scientific clues for prevention, diagnosis, and therapy. Cancer J. Clin. 2019, 69, 402–429. [Google Scholar] [CrossRef]
- United Nations. List of Member States. 2019. Available online: https://www.un.org/en/member-states/index.html (accessed on 15 January 2021).
- World Bank. World Bank Country and Lending Groups. Fiscal Year. 2021. Available online: https://datahelpdesk.worldbank.org/knowledgebase/articles/906519-world-bank-country-and-lending-groups (accessed on 15 January 2021).
- World Health Organization. List of WHO Member States. 2019. Available online: https://www.who.int/choice/demography/by_country/en/ (accessed on 15 January 2021).
- United States Geological Survey. Asbestos Statistics and Information, Minerals Yearbook 1920–2017 (Personal Communication Included). Available online: https://www.usgs.gov/centers/nmic/asbestos-statistics-and-information (accessed on 15 January 2021).
- United Nations Statistics Division. United Nations International Trade Statistics Database, UN Comtrade. Available online: https://comtrade.un.org/data/ (accessed on 15 January 2021).
- World Health Organization. WHO Mortality Database. 2019. Available online: https://www.who.int/data/data-collection-tools/who-mortality-database (accessed on 15 January 2021).
- World Health Organization. Global Health Estimates 2016: Deaths by Cause, Age, Sex, by Country and by Region, 2000–2016. Available online: https://www.who.int/healthinfo/global_burden_disease/en/ (accessed on 15 January 2021).
- World Health Organization. Global Cancer Observatory: Cancer Today. 2018. Available online: https://gco.iarc.fr/today (accessed on 15 January 2021).
- Wolff, H.; Vehmas, T.; Oksa, P.; Rantanen, J.; Vainio, H. Consensus Report: Asbestos, asbestosis, and cancer, the Helsinki criteria for diagnosis and attribution. Scand. J. Work. Environ. Health 2015, 41, 5–15. [Google Scholar] [CrossRef] [PubMed]
- Kameda, T.; Takahashi, K.; Kim, R.; Jiang, Y.; Movahed, M.; Park, E.K.; Rantanen, J. Asbestos: Use, bans and disease burden in Europe. Bull. World Health Organ. 2014, 92, 790–797. [Google Scholar] [CrossRef]
- Le, G.V.; Takahashi, K.; Park, E.K.; Delgermaa, V.; Oak, C.; Qureshi, A.M.; Aljunid, S.M. Asbestos use and asbestos-related diseases in Asia: Past, present and future. Respirology 2011, 16, 767–775. [Google Scholar] [CrossRef]
- World Health Organization Regional Office for Europe. Parma Declaration on Environment and Health. 2010. Available online: http://www.euro.who.int/__data/assets/pdf_file/0011/78608/E93618.pdf (accessed on 15 January 2021).
- National Institute for Occupational Safety and Health. Improving Workers’ Health across the Globe. 2016. Available online: https://www.cdc.gov/niosh/docs/2016-118/pdfs/success-stories_v01_nr04_n-compressed.pdf (accessed on 15 January 2021).
- Asbestos Safety and Eradiation Agency. National Asbestos Profile for Australia. 2017. Available online: https://www.asbestossafety.gov.au/sites/default/files/documents/2017-12/ASEA_National_Asbestos_Profile_interactive_Nov17.pdf (accessed on 11 January 2021).
- Bangladesh Occupational Safety, Health and Environment Foundation. 2016. National Asbestos Profile of Bangladesh. Per-sonal Communication. 2020.
- Vangelova, K.; Dimitrova, S.; Dimitrova, I. National Asbestos Profile of Bulgaria. 2015. Available online: https://ncpha.government.bg/files/National%20Asbestos%20Profile_Bulgaria_2015-en.pdf (accessed on 11 January 2021).
- Ministry of Labor and Vocational Training. 2019. Cambodia National Asbestos Profile. Obtained via personal communication: 04 May 2020.
- Federal Institute for Occupational Health and Safety. National Asbestos Profile for Germany. 2014. Available online: https://www.baua.de/EN/Service/Publications/Report/Gd80.pdf?__blob=publicationFile&v=8 (accessed on 11 January 2021).
- People’s Training & Research and Centre. India: National Asbestos Profile. 2017. Available online: https://amrc.org.hk/sites/default/files/NAP%20India.pdf (accessed on 11 January 2021).
- Indonesia Ban Asbestos Network. 2017. National Asbestos Profile Indonesia. Personal Communication, 2020.
- Furuya, S.; Takahashi, K.; Mohaved, M.; Jiang, Y. National Asbestos Profile of Japan. 2013. Available online: https://www.researchgate.net/publication/237839114_National_Asbestos_Profile_of_Japan_-_Based_on_the_National_Asbestos_Profile_by_the_ILO_and_the_WHO (accessed on 11 January 2021).
- Laos Ministry of Industry and Commerce. 2017. National Asbestos Profile of Laos. Personal Communication, 2020.
- Institute of Occupational Health of the Republic of Macedonia. 2014. National Asbestos Profile for the Republic of Macedonia. Obtained via personal communication: 15 July 2020.
- Health Sciences University of Mongolia. 2012. National Asbestos Profile of Mongolia. Personal Communication. 2020.
- Sah, R.C. National Asbestos Profile of Nepal. 2016. Available online: http://anroev.org/aban/wp-content/uploads/2016/10/National-Abestos-Profile-of-Nepal.pdf (accessed on 11 January 2021).
- Republic of Philippines, Environmental and Occupational Health Office. National Asbestos Profile Philippines. 2013. Available online: https://www.informea.org/en/national-asbestos-profile-nap-philippines (accessed on 11 January 2021).
- Pham, V.H.; Tran, T.N.L.; Le, G.V.; Movahed, M.; Jiang, Y.; Pham, N.H.; Ogawa, H.; Takahashi, K. Asbestos and asbestos-related diseases in Vietnam: In reference to the International Labor Organization/World Health Organization National Asbestos Profile. Saf. Health Work 2013, 4, 117–121. [Google Scholar] [CrossRef] [PubMed][Green Version]

| Country Category | Document Category | Document Description |
|---|---|---|
| A | “bona fide NAP” | a single document that describes the national situation of asbestos and asbestos-related diseases (ARDs) in adherence to the NAP format published by the WHO/ILO3 |
| B | “proxy NAP” | a single document or multiple documents that describe the national situation of asbestos and ARDs but does (do) not satisfy the criterion for a bona fide NAP; * includes government statements and/or decrees, scientific articles and third-party organization reports |
| C | “relevant published information” | information that does not satisfy the criteria for a bona fide or proxy NAP but refers to asbestos and/or ARDs; includes online information on asbestos as part of wider occupational health and safety policies, toxic chemical waste management policies, ARD case studies and media releases on asbestos and/or ARDs |
| D | “no relevant information” | status that lacked any of the above |
| Country Category | Number of Countries | Income Category 1 | Region | Status of Asbestos Ban | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| HI | UMI | LMI | LI | Western Pacific | South East Asia | Europe | Americas | Africa | East Mediterranean | Banned | No-Ban | ||
| A: Countries that have bona fide NAP 2 | 14 | 3 | 3 | 8 | 0 | 7 | 4 | 3 | 0 | 0 | 0 | 5 | 9 |
| (7%) | (5%) | (6%) | (16%) | (0%) | (28%) | (36%) | (6%) | (0%) | (0%) | (0%) | (8%) | (7%) | |
| B: Countries that do not have bona fide NAP but have proxy NAP 3 | 98 | 49 | 28 | 15 | 6 | 17 | 4 | 39 | 14 | 12 | 12 | 51 | 47 |
| (50%) | (78%) | (52%) | (31%) | (21%) | (68%) | (36%) | (72%) | (40%) | (26%) | (57%) | (78%) | (36%) | |
| C: Countries that have neither bona fide or proxy NAP but have other relevant published information | 51 | 10 | 14 | 16 | 11 | 2 | 2 | 8 | 13 | 19 | 7 | 9 | 42 |
| (26%) | (16%) | (26%) | (33%) | (38%) | (8%) | (18%) | (15%) | (37%) | (40%) | (33%) | (14%) | (32%) | |
| D: Countries with no relevant published information | 32 | 1 | 9 | 10 | 12 | 1 | 1 | 4 | 8 | 16 | 2 | 0 | 32 |
| (16%) | (2%) | (17%) | (20%) | (41%) | (4%) | (9%) | (7%) | (23%) | (34%) | (10%) | (0%) | (25%) | |
| All countries | 195 | 63 | 54 | 49 | 29 | 27 | 11 | 54 | 35 | 47 | 21 | 65 | 130 |
| (100%) | (100%) | (100%) | (100%) | (100%) | (100%) | (100%) | (100%) | (100%) | (100%) | (100%) | (100%) | (100%) | |
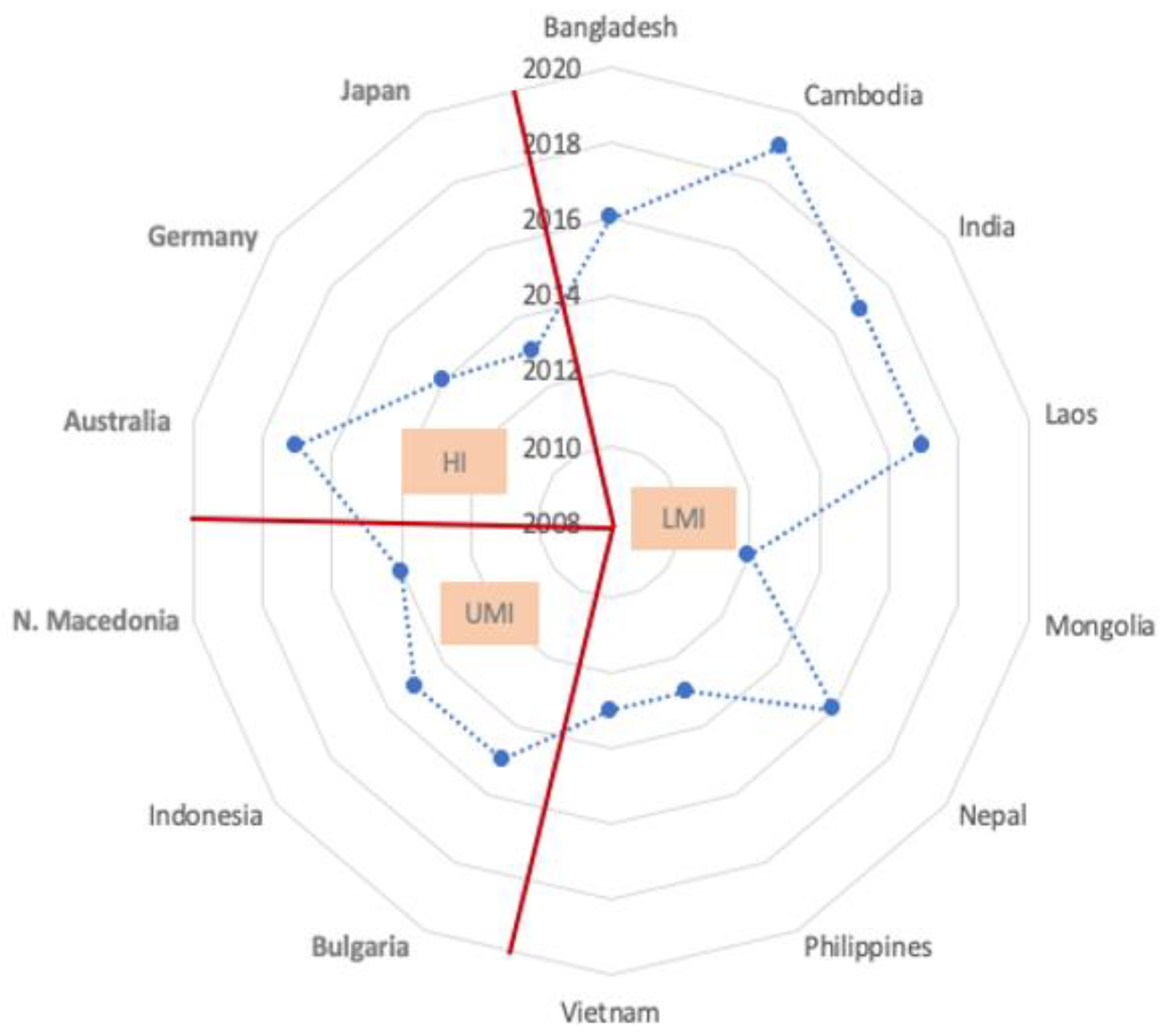
| Country | NAP Publication Year | National Income Category 1 | Region 2 | Asbestos Ban | Authors 3 |
|---|---|---|---|---|---|
| Australia | 2017 | HI | WP | 2003 | G |
| Bangladesh | 2016 | LMI | SEA | No-ban | NG |
| Bulgaria | 2015 | UMI | EUR | 2005 | G |
| Cambodia | 2019 | LMI | WP | No-ban | G, MS |
| Germany | 2014 | HI | EUR | 2005 | G |
| India | 2017 | LMI | SEA | No-ban | NG |
| Indonesia | 2015 | UMI | SEA | No-ban | NG, MS |
| Japan | 2013 | HI | WP | 2007 | NG, MS |
| Laos | 2017 | LMI | WP | No-ban | G, MS |
| North Macedonia | 2014 | UMI | EUR | 2014 | NG, MS |
| Mongolia | 2012 | LMI | WP | No-ban | G, MS |
| Nepal | 2016 | LMI | SEA | No-ban | NG, MS |
| Philippines | 2013 | LMI | WP | No-ban | G, MS |
| Vietnam | 2013 | LMI | WP | No-ban | G, MS |
| Country Category | Data Availability | |||||
|---|---|---|---|---|---|---|
| Asbestos Data | Disease Data | |||||
| Consumption of Raw Asbestos < USGS 1 > (Row %) | Asbestos-Containing Material, Cement, Textiles or Friction Material < UN Comtrade 2 > (row %) | Reported Mortality of Mesothelioma or Asbestosis 3 < WHO MDB 3 > (Row%) | Estimated Incidence of Mesothelioma < GBD 4 > (Row %) | Estimated Mortality of Mesothelioma < WHO GHE 5 > (Row %) | Reported or Estimated Mortality of Mesothelioma < WHO GCO 6 > (Row%) | |
| A (n = 14) | 14 (100%) | 14 (100%) | 7 (50%) | 14 (100%) | 14 (100%) | 13 (93%) |
| B (n = 98) | 83 (85%) | 91 (93%) | 63 (64%) | 91 (93%) | 87 (89%) | 77 (79%) |
| C (n = 51) | 43 (84%) | 46 (90%) | 19 (37%) | 49 (96%) | 47 (92%) | 27 (53%) |
| D (n = 32) | 25 (78%) | 28 (88%) | 7 (22%) | 32 (100%) | 30 (94%) | 17 (53%) |
| All countries (n = 195) | 165 (85%) | 179 (92%) | 96 (49%) | 186 (95%) | 178 (91%) | 134 (69%) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Arachi, D.; Furuya, S.; David, A.; Mangwiro, A.; Chimed-Ochir, O.; Lee, K.; Tighe, P.; Takala, J.; Driscoll, T.; Takahashi, K. Development of the “National Asbestos Profile” to Eliminate Asbestos-Related Diseases in 195 Countries. Int. J. Environ. Res. Public Health 2021, 18, 1804. https://doi.org/10.3390/ijerph18041804
Arachi D, Furuya S, David A, Mangwiro A, Chimed-Ochir O, Lee K, Tighe P, Takala J, Driscoll T, Takahashi K. Development of the “National Asbestos Profile” to Eliminate Asbestos-Related Diseases in 195 Countries. International Journal of Environmental Research and Public Health. 2021; 18(4):1804. https://doi.org/10.3390/ijerph18041804
Chicago/Turabian StyleArachi, Diana, Sugio Furuya, Annette David, Alexander Mangwiro, Odgerel Chimed-Ochir, Kenneth Lee, Peter Tighe, Jukka Takala, Tim Driscoll, and Ken Takahashi. 2021. "Development of the “National Asbestos Profile” to Eliminate Asbestos-Related Diseases in 195 Countries" International Journal of Environmental Research and Public Health 18, no. 4: 1804. https://doi.org/10.3390/ijerph18041804
APA StyleArachi, D., Furuya, S., David, A., Mangwiro, A., Chimed-Ochir, O., Lee, K., Tighe, P., Takala, J., Driscoll, T., & Takahashi, K. (2021). Development of the “National Asbestos Profile” to Eliminate Asbestos-Related Diseases in 195 Countries. International Journal of Environmental Research and Public Health, 18(4), 1804. https://doi.org/10.3390/ijerph18041804