
Physical Self-Concept Changes in Adults and Older Adults: Influence of Emotional Intelligence, Intrinsic Motivation and Sports Habits

 ,
, 
 ,
,  ,
,  , and
, and 
Abstract
1. Introduction
2. Materials and Methods
2.1. Design and Subjects
2.2. Instruments and Variables
2.3. Procedure
2.4. Analysis of Data
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Conflicts of Interest
References
- Population Division, Department of Economic and Social Affairs, United Nation. World Population Ageing 2017; United Nation: New York, NY, USA, 2017. [Google Scholar]
- Bhardwaj, R.; Amiri, S.; Buchwald, D.; Amram, O. Environmental correlates of reaching a centenarian age: Analysis of 144,665 deaths in Washington state for 2011–2015. Int. J. Environ. Res. Public Health 2020, 17, 2828. [Google Scholar] [CrossRef]
- Foscoloua, A.; Magriplisa, E.; Tyrovolasa, S.; Soulisa, G.; Bountzioukaa, V.; Mariolisc, A.; Piscopod, S.; Valacchie, G.; Anastasiouf, F.; Gotsisa, E.; et al. Lifestyle determinants of healthy ageing in a Mediterranean population: The multinational MEDIS study. Exp. Gerontol. 2018, 110, 35–41. [Google Scholar] [CrossRef]
- Hajat, C.; Selwyn, A.; Harris, M.; Yach, D. Preventive interventions for the second half of life: A systematic review. Am. J. Health Promot. 2018, 32, 1122–1139. [Google Scholar] [CrossRef]
- Sarabia-Cobo, C.M.; Pérez, V.; Hermosilla, C.; de Lorena, P. Retirement or no retirement? The decision’s effects on cognitive functioning, well-being, and quality of life. Behav. Sci. 2020, 10, 151. [Google Scholar] [CrossRef] [PubMed]
- Bangsbo, J.; Blackwell, J.; Boraxbekk, C.J.; Caserotti, P.; Dela, F.; Evans, A.B.; Jespersen, A.P.; Gliemann, L.; Kramer, A.F.; Lundbye-Jensen, J.; et al. Copenhagen consensus statement 2019: Physical activity and ageing. Br. J. Sports Med. 2019, 53, 856–858. [Google Scholar] [CrossRef] [PubMed]
- Calder, P.C.; Carding, S.R.; Christopher, G.; Kuh, D.; Langley-Evans, S.C. A holistic approach to healthy ageing: How can people live longer, healthier lives? J. Hum. Nutr. Diet. 2018, 31, 439–450. [Google Scholar] [CrossRef]
- Landi, F.; Calvani, R.; Picca, A.; Tosato, M.; Martone, A.M.; D’Angelo, M.; Serafini, E.; Bernabei, R.; Marzetti, E. Impact of habitual physical activity and type of exercise on physical performance across ages in community-living people. PLoS ONE 2018, 13, 0191820. [Google Scholar] [CrossRef] [PubMed]
- Parker, P.C.; Chipperfield, J.G.; Perry, R.P.; Hamm, J.M.; Hoppmann, C.A. Attributions for physical activity in very old adults: Predicting everyday physical activity and mortality risk. Psychol. Health 2019, 34, 216–231. [Google Scholar] [CrossRef]
- Saint-Maurice, P.F.; Coughlan, D.; Kelly, S.P.; Keadle, S.K.; Cook, M.B.; Carlson, S.A.; Fulton, J.E.; Matthews, C.E. Association of leisure-time physical activity across the adult life course with all-cause and cause-specific mortality. JAMA Netw. Open. 2019, 2, 190355. [Google Scholar] [CrossRef] [PubMed]
- Boulton, E.; Hawley-Hague, H.; French, D.P.; Mellone, S.; Zacchi, A.; Clemson, L.; Vereijken, B.; Todd, C. Implementing behaviour change theory and techniques to increase physical activity and prevent functional decline among adults aged 61–70: The PreventIT project. Prog. Cardiovasc. Dis. 2019, 62, 147–156. [Google Scholar] [CrossRef] [PubMed]
- Ensrud-Skraastad, O.K.; Haga, M. Associations between motor competence, physical self-perception and autonomous motivation for physical activity in children. Sports 2020, 8, 120. [Google Scholar] [CrossRef]
- Li, Y.C.; Chirico, D.; Graham, J.D.; Kwan, M.Y.W.; Cairney, J. Motor coordination and moderate-to-vigorous physical activity in emerging adults: Mediating effect of physical self-concept. International Int. J. Environ. Res. Public Health 2020, 17, 3748. [Google Scholar] [CrossRef]
- Utesch, T.; Dreiskämper, D.; Naul, R.; Geukes, K. Understanding physical (in-) activity, overweight, and obesity in childhood: Effects of congruence between physical self-concept and motor competence. Sci. Rep. 2018, 8, 1–10. [Google Scholar] [CrossRef]
- Babic, M.J.; Morgan, P.J.; Plotnikoff, R.C.; Lonsdale, C.; White, R.L.; Lubans, D.R. Physical activity and physical self-concept in youth: Systematic review and meta-analysis. Sports Med. 2014, 44, 1589–1601. [Google Scholar] [CrossRef]
- Berthelot, G.; Johnson, S.; Noirez, P.; Antero, J.; Marck, A.; Desgorces, F.D.; Pifferi, F.; Carter, P.A.; Spedding, M.; Mannoux, A.S.; et al. The age-performance relationship in the general population and strategies to delay age related decline in performance. Arch. Public Health 2019, 77, 1–9. [Google Scholar] [CrossRef]
- Hsu, Y.; Lu, F.J.H. Older adults’ physical exercise and health-related quality of life: The mediating role of physical self-concept. Educ. Gerontol. 2018, 44, 247–254. [Google Scholar] [CrossRef]
- Jodra, P.; Maté-Muñoz, J.L.; Domínguez, R. Percepción de salud, autoestima y autoconcepto físico en personas mayores en función de su actividad física. Rev. Psicol. Deporte 2019, 28, 127–134. [Google Scholar]
- Sweeney, A.M.; Wilson, D.K.; Van Horn, M.L. Longitudinal relationships between self-concept for physical activity and neighborhood social life as predictors of physical activity among older African American adults. Int. J. Behav. Nutr. Phy. 2017, 14, 1–12. [Google Scholar] [CrossRef] [PubMed]
- Shavelson, R.J.; Hubner, J.J.; Stanton, G.C. Self-concept: Validation of construct interpretations. Rev. Edu. Res. 1976, 4, 407–441. [Google Scholar] [CrossRef]
- Esnaola, I.; Sesé, A.; Antonio-Agirre, I.; Azpiazu, L. The development of multiple self-concept dimensions during adolescence. J. Res. Adolesc. 2020, 30, 100–114. [Google Scholar] [CrossRef] [PubMed]
- González-Valero, G.; Zurita-Ortega, F.; Ubago-Jiménez, J.L.; Puertas-Molero, P. Motivation, self-concept and discipline in young adolescents who practice rhythmic gymnastics. An intervention. Children 2020, 7, 135. [Google Scholar] [CrossRef] [PubMed]
- Fox, K.R.; Corbin, C.B. The physical self-perception profile: Development and preliminary validation. J. Sport Exerc. Psy. 1989, 11, 408–430. [Google Scholar] [CrossRef]
- Chrismas, B.C.R.; Majed, L.; Kneffel, Z. Physical fitness and physical self-concept of male and female young adults in Qatar. PLoS ONE 2019, 14, e0223359. [Google Scholar] [CrossRef]
- Garn, A.C.; Morin, A.J.S.; White, R.L.; Owen, K.B.; Donley, W.; Lonsdale, C. Moderate-to-vigorous physical activity as a predictor of changes in physical self-concept in adolescents. Health Psychol. 2020, 39, 190–198. [Google Scholar] [CrossRef]
- Jekauc, D.; Wagner, M.O.; Herrmann, C.; Hegazy, K.; Woll, A. Does physical self-concept mediate the relationship between motor abilities and physical activity in adolescents and young adults? PLoS ONE 2017, 12, 1–18. [Google Scholar] [CrossRef] [PubMed]
- Brown, D.M.Y.; Cairney, J. The synergistic effect of poor motor coordination, gender and age on self-concept in children: A longitudinal analysis. Res. Dev. Disabil. 2020, 98, 103576. [Google Scholar] [CrossRef]
- Klomsten, A.T.; Skaalvik, E.M.; Espnes, G.A. Physical self-concept and sports: Do gender differences still exist? Sex Roles 2004, 50, 119–127. [Google Scholar] [CrossRef]
- Trautwein, U.; Gerlach, E.; Lüdtke, O. Athletic classmates, physical self-concept, and free-time physical activity: A longitudinal study of frame of reference effects. J. Educ. Psychol. 2008, 100, 988–1001. [Google Scholar] [CrossRef]
- Amesberger, G.; Finkenzeller, T.; Müller, E.; Würth, S. Aging-related changes in the relationship between the physical self-concept and the physical fitness in elderly individuals. Scand. J. Med. Sci. Sports 2019, 29, 26–34. [Google Scholar] [CrossRef] [PubMed]
- Finkenzeller, T.; Pötzelsberger, B.; Kösters, A.; Würth, S.; Amersberger, G.; Dela, F.; Müller, E. Aging in high functioning elderly persons: Study design and analyses of behavioral and psychological factors. Scand. J. Med. Sci. Sports 2019, 29, 7–16. [Google Scholar] [CrossRef] [PubMed]
- Esnaola, I. El autoconcepto físico durante el ciclo vital. Ann. Psychol. 2008, 24, 1–8. [Google Scholar]
- Infante, G.; Goñi, A.; Villarroel, J.D. Actividad física y autoconcepto, físico y general, a lo largo de la edad adulta. Rev. Psicol. Deporte 2011, 20, 429–444. [Google Scholar] [CrossRef][Green Version]
- Molero, D.; Zagalaz-Sánchez, M.L.; Cachón-Zagalaz, J. Estudio comparativo del autoconcepto físico a lo largo del ciclo vital. Rev. Psicol. Deporte 2013, 22, 135–142. [Google Scholar]
- Putnick, D.L.; Hahn, C.S.; Hendricks, C.; Bornstein, M.H. Developmental stability of scholastic, social, athletic, and physical appearance self-concepts from preschool to early adulthood. J. Child Psychol. Psyc. 2020, 61, 95–103. [Google Scholar] [CrossRef] [PubMed]
- Clancy, R.B.; Herring, M.P.; Campbell, M.J. Motivation measures in sport: A critical review and bibliometric análisis. Front. Psychol. 2017, 8, 348. [Google Scholar] [CrossRef]
- Bauman, A.E.; Reis, R.S.; Sallis, J.F.; Wells, J.C.; Loos, R.J.F.; Martin, B.W. Correlates of physical activity: Why are some people physically active and others not? Lancet 2012, 380, 258–271. [Google Scholar] [CrossRef]
- Derakhshanrad, S.A.; Piven, E.; Ghoochani, B.Z. A cross-sectional study to investigate motivation for physical activity in a sample of Iranian community-dwelling older adults. Health Promot. Perspect. 2020, 10, 135–141. [Google Scholar] [CrossRef]
- Lee, S.; Lee, C.; An, J. Psycho-social correlates of leisure-time physical activity (LTPA) among older adults: A multivariate analysis. Eur. Rev. Aging. Phys. Act. 2020, 17, 1–7. [Google Scholar] [CrossRef]
- Tang, M.; Wang, D.; Guerrien, A. A systematic review and meta-analysis on basic psychological need satisfaction, motivation, and well-being in later life: Contributions of self-determination theory. PsyCh J. 2020, 9, 5–33. [Google Scholar] [CrossRef]
- Lea, R.G.; Qualter, P.; Davis, S.K.; Pérez-González, J.C.; Bangee, M. Trait emotional intelligence and attentional bias for positive emotion: An eye tracking study. Pers. Indiv. Differ. 2018, 128, 88–93. [Google Scholar] [CrossRef]
- Szczygieł, D.; Mikolajczak, M. Why are people high in emotional intelligence happier? They make the most of their positive emotions. Pers. Indiv. Differ. 2017, 117, 177–181. [Google Scholar] [CrossRef]
- Petrides, K.V.; Pita, R.; Kokkinaki, F. The location of trait emotional intelligence in personality factor space. Br. J. Psychol. 2007, 98, 273–289. [Google Scholar] [CrossRef]
- Fiorilli, C.; Farina, E.; Buonomo, I.; Costa, S.; Romano, L.; Larcan, R.; Petrides, K.V. Trait Emotional Intelligence and School Burnout: The Mediating Role of Resilience and Academic Anxiety in High School. Int. J. Environ. Res. Public Health 2020, 17, 3058. [Google Scholar] [CrossRef] [PubMed]
- Cheshire, M.H.; Strickland, H.P.; Ewell, P.J. Measured emotional intelligence in Baccalaureate Nursing Education: A longitudinal study. Nurs. Educ. Perspect. 2020, 41, 103–105. [Google Scholar] [CrossRef] [PubMed]
- Dave, H.P.; Keefer, K.V.; Snetsinger, S.W.; Holden, R.R.; Parker, J.D.A. Stability and change in trait emotional intelligence in emerging adulthood: A four-year population-based study. J. Pers. Assess. 2021, 103, 57–66. [Google Scholar] [CrossRef] [PubMed]
- Foster, K.; Fethney, J.; McKenzie, H.; Fischer, M.; Harkness, E.; Kozlowski, D. Emotional intelligence increases over time: A longitudinal study of Australian pre-registration nursing students. Nurs. Educ. Today 2017, 55, 65–70. [Google Scholar] [CrossRef] [PubMed]
- Meléndez, J.C.; Delhom, I.; Satorres, E. The power of emotional intelligence on older adults’ resilience. Ansiedad y Estrés 2019, 25, 14–19. [Google Scholar] [CrossRef]
- Fantini-Hauwel, C.; Mikolajczak, M. Factor structure, evolution, and predictive power of emotional competencies on physical and emotional health in the elderly. J. Aging. Health 2014, 26, 993–1014. [Google Scholar] [CrossRef]
- Navarro-Bravo, B.; Latorre, J.M.; Jiménez, A.; Cabello, R.; Fernández-Berrocal, P. Ability emotional intelligence in young people and older adults with and without depressive symptoms, considering gender and educational level. PeerJ 2019, 7, 6596. [Google Scholar] [CrossRef]
- Martín-Albo, J.; Núñez, J.L.; Domínguez, E.; León, J.; Tomás, J.M. Relationships between intrinsic motivation, physical self-concept and satisfaction with life: A longitudinal study. J. Sports Sci. 2012, 30, 337–347. [Google Scholar] [CrossRef]
- Padial-Ruz, R.; Pérez-Turpin, J.A.; Cepero-González, M.; Zurita-Ortega, F. Effects of physical self-concept, emotional isolation, and family functioning on attitudes towards physical education in adolescents: Structural equation analysis. Int. J. Environ. Res. Public Health 2020, 17, 94. [Google Scholar] [CrossRef] [PubMed]
- Fraguela-Vale, R.; Varela-Garrote, L.; Carretero-García, M.; Peralbo-Rubio, E.M. Basic psychological needs, physical self-concept, and physical activity among adolescents: Autonomy in focus. Front. Psychol. 2020, 11, 491. [Google Scholar] [CrossRef] [PubMed]
- Ramirez-Granizo, I.; Sánchez-Zafra, M.; Zurita-Ortega, F.; Puertas-Molero, P.; González-Valero, G.; Ubago-Jiménez, J.L. Multidimensional self-concept depending on levels of resilience and the motivational climate directed towards sport in schoolchildren. Int. J. Environ. Res. Public Health 2020, 17, 534. [Google Scholar] [CrossRef] [PubMed]
- Laborde, S.; Dosseville, F.; Allen, M.S. Emotional intelligence in sport and exercise: A systematic review. Scand. J. Med. Sci. Sports 2016, 26, 862–874. [Google Scholar] [CrossRef] [PubMed]
- Ubago-Jiménez, J.L.; González-Valero, G.; Puertas-Molero, P.; García-Martínez, I. Development of emotional intelligence through physical activity and sport practice. Behav. Sci. 2019, 9, 44. [Google Scholar] [CrossRef]
- Amado-Alonso, D.; León-del-Barco, B.; Mendo-Lázaro, S.; Sánchez-Miguel, P.A.; Iglesias Gallego, D. Emotional Intelligence and the Practice of Organized Physical-Sport Activity in Children. Sustainability 2019, 11, 1615. [Google Scholar] [CrossRef]
- Lamonte, M.J.; Buchner, D.M.; Rillamas-Sun, E.; Di, C.; Evenson, K.R.; Bellettiere, J.; Lewis, C.E.; Lee, I.; Tinker, L.F.; Seguin, R.; et al. Accelerometer-measured physical activity and mortality in women aged 63 to 99. J. Am. Geriatr. Soc. 2018, 66, 886–894. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. WHO Guidelines on Physical Activity and Sedentary Behaviour; World Health Organization: Geneva, Switzerland, 2020. [Google Scholar]
- Goñi, A.; Ruiz, S.; Liberal, I. Propiedades psicométricas de un nuevo cuestionario para la medida del autoconcepto físico. Rev. Psicol. Deporte 2004, 13, 195–213. [Google Scholar]
- Pelletier, L.; Tuson, K.M.; Fortier, M.; Vallerand, R.J. Toward a new measure of intrinsic motivation, extrinsic motivation, and amotivation in sports: The Sport Motivation Scale (SMS). J. Sport Exerc. Psy. 1995, 17, 35–53. [Google Scholar] [CrossRef]
- Balanguer, I.; Castillo, I.; Duda, J.L. Propiedades psicométricas de la escala de motivación deportiva en deportistas españoles. Rev. Mex. Psicol. 2007, 24, 197–207. [Google Scholar] [CrossRef]
- Salovey, P.; Mayer, J.D.; Goldman, S.L.; Turvey, C.; Palfai, T.P. Emotional attention, clarity, and repair: Exploring emotional intelligence using the Trait Meta-Mood Scale. In Emotion, Disclosure, and Health; Pennebaker, J.W., Ed.; American Psychological Association: Washington, DC, USA, 1995; pp. 125–154. [Google Scholar] [CrossRef]
- Fernandez-Berrocal, P.; Extremera, N.; Ramos, N. Validity and reliability of the spanish modified version of the trait meta-mood scale. Psychol. Rep. 2004, 94, 751–755. [Google Scholar] [CrossRef] [PubMed]
- Marsh, H.W. Age and gender effects in physical self-concepts for adolescent elite athletes and nonathletes: A multicohort-multioccasion. J. Sport Exerc. Psychol. 1998, 20, 237–259. [Google Scholar] [CrossRef]
- Martin, A.J.; Liem, G.A.; Coffey, L.; Martínez, C.; Parker, P.P.; Marsh, H.W.; Jackson, S.A. What happens to physical activity behavior, motivation, self-concept, and flow after completing school? A longitudinal study. J. Appl. Sport Psychol. 2010, 22, 437–457. [Google Scholar] [CrossRef]
- Clark, B.C. Neuromuscular changes with aging and sarcopenia. J. Frailty Aging 2019, 8, 7–9. [Google Scholar] [CrossRef]
- Larsson, L.; Degens, H.; Li, M.; Salviati, L.; Lee, Y.; Thompson, W.; Kirkland, J.L.; Sandri, M. Sarcopenia: Aging-related loss of muscle mass and function. Physiol. Rev. 2019, 99, 427–511. [Google Scholar] [CrossRef] [PubMed]
- Schwaba, T.; Bleidorn, W. Personality trait development across the transition to retirement. J. Pers. Soc. Psychol. 2019, 116, 651–665. [Google Scholar] [CrossRef] [PubMed]
- Alemany-Arrebola, I.; Cortijo-Cantos, A.; Granda-Vera, J. La cultura, la edad y el sexo como mediadores del autoconcepto físico. Rev. Int. de Med. y Cienc. de la Act. Física y del Deporte 2020, 20, 353–368. [Google Scholar] [CrossRef]
- Li, G.S.F.; Lu, F.J.H.; Wang, A.H.H. Exploring the relationships of physical activity, emotional intelligence and health in Taiwan college students. J. Exerc. Sci. Fit. 2009, 7, 55–63. [Google Scholar] [CrossRef]
- Zysberg, L.; Hemmel, R. Emotional Intelligence and Physical Activity. J. Phys. Act. Health 2017, 15, 53–56. [Google Scholar] [CrossRef]
- Castro-Sánchez, M.; Zurita-Ortega, F.; Chacón-Cuberos, R.; López-Gutiérrez, C.J.; Zafra-Santos, E. Emotional intelligence, motivational climate and levels of anxiety in athletes from different categories of sports: Analysis through structural equations. Int. J. Environ. Res. Public Health 2018, 15, 894. [Google Scholar] [CrossRef] [PubMed]
- Tsaousis, I.; Smaragda, K. Factorial invariance and latent mean differences of scores on trait emotional intelligence across gender and age. Pers. Indiv. Differ. 2013, 54, 169–173. [Google Scholar] [CrossRef]
- Clevinger, K.; Petrie, T.; Martin, S.; Greenleaf, C. The relationship of sport involvement and gender to physical fitness, self-efficacy, and self-concept in middle school students. Phys. Educ. 2020, 77, 9228. [Google Scholar] [CrossRef]
- Kay, A.B.; Wilson, E.L.; White, T.W.; Morris, D.S.; Majercik, S. Age is just a number: A look at “elderly” sport-related traumatic injuries at a level I trauma center. Am. J. Surg. 2019, 217, 1121–1125. [Google Scholar] [CrossRef] [PubMed]
- Chacón-Cuberos, R.; Zurita-Ortega, F.; García-Mármol, E.; Castro-Sánchez, M. Multidimensional self-concept depending on sport practice in university students of Physical Education from Andalucía. Retos 2020, 37, 174–180. [Google Scholar]




{kind=link}
{kind=link}
{kind=link}
| n = 520 | 41–50 (n = 116) | 51–60 (n = 225) | 61–70 (n = 135) | 71–80 (n = 44) | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| M | W | psex * | M | W | psex* | M | W | psex * | M | W | psex * | pgroup ** | ||
| Distribution | n | 66 | 50 | - | 173 | 52 | - | 102 | 33 | - | 28 | 16 | - | - |
| % | 56.89 | 43.10 | 0.167 | 76.88 | 23.11 | 0.001 | 75.55 | 24.44 | 0.001 | 63.63 | 36.36 | 0.006 | 0.005 | |
| Age (years) | M | 45.58 | 45.50 | 0.952 | 55.69 | 55.29 | 0.461 | 63.21 | 63.39 | 0.688 | 73.86 | 71.81 | 0.007 | 0.001 |
| SD | 2.55 | 2.74 | - | 2.68 | 2.87 | - | 2.73 | 2.83 | - | 2.90 | 2.83 | - | - | |
| Me | 46 | 46 | - | 56 | 56 | - | 62.5 | 63 | - | 73 | 70.5 | - | - | |
| IQR | 4.75 | 4.00 | - | 4.00 | 4.25 | - | 5 | 6 | - | 4.25 | 2.25 | - | - | |
| Height (m) | M | 1.77 | 1.64 | 0.001 | 1.74 | 1.60 | 0.001 | 1.73 | 1.60 | 0.001 | 1.70 | 1.58 | 0.001 | 0.004 |
| SD | 7.66 | 7.31 | - | 7.51 | 9.60 | - | 7.77 | 6.31 | - | 7.21 | 4.76 | - | - | |
| Me | 1.78 | 1.64 | - | 1.76 | 1.60 | - | 1.75 | 1.62 | - | 1.70 | 1.60 | - | - | |
| IQR | 10.5 | 9.5 | - | 9.00 | 9.25 | - | 10.0 | 8.5 | - | 7.5 | 5.5 | - | - | |
| Weight (kg) | M | 82.69 | 62.8 | 0.001 | 81.46 | 62.52 | 0.001 | 79.69 | 67.1 | 0.001 | 75.78 | 69.09 | 0.100 | 0.149 |
| SD | 12.55 | 15.13 | - | 12.13 | 9.19 | - | 10.82 | 14.64 | - | 8.00 | 12.31 | - | - | |
| Me | 79.0 | 59.5 | - | 80.0 | 60.0 | - | 78.0 | 63.0 | - | 77.0 | 68.0 | - | - | |
| IQR | 15.50 | 9.75 | - | 16.75 | 12.00 | - | 15.00 | 12.00 | - | 9.5 | 13.5 | - | - | |
| BMI (kg/m2) | M | 26.31 | 23.30 | 0.001 | 26.72 | 24.52 | 0.001 | 26.69 | 26.00 | 0.175 | 26.23 | 27.71 | 0.537 | 0.002 |
| SD | 4.19 | 5.46 | - | 4.36 | 4.23 | - | 4.33 | 5.55 | - | 3.22 | 5.34 | - | - | |
| Me | 25.76 | 21.82 | - | 26.07 | 22.96 | - | 25.71 | 25.31 | - | 25.14 | 27.09 | - | - | |
| IQR | 5.00 | 2.93 | - | 4.41 | 4.43 | - | 4.38 | 4.54 | - | 4.14 | 6.25 | - | - | |
| Variable | 41–50 | 51–60 | 61–70 | 71–80 | X2 | |||||
|---|---|---|---|---|---|---|---|---|---|---|
| n | % | n | % | n | % | n | % | p | V Cramer | |
| Sports initiation | 0.001 | 0.171 | ||||||||
| Childhood | 74 | 63.79 | 113 | 50.22 | 57 | 42.22 | 16 | 36.36 | - | - |
| Adolescence | 20 | 17.24 | 64 | 28.44 | 42 | 31.11 | 12 | 27.27 | - | - |
| Adult | 22 | 18.97 | 35 | 15.56 | 30 | 22.22 | 9 | 20.45 | - | - |
| Not practice | 0 | 0.00 | 13 | 5.78 | 6 | 4.44 | 7 | 15.91 | - | - |
| PA level | 0.001 | 0.219 | ||||||||
| Not active | 7 | 6.03 | 45 | 20.00 | 22 | 16.30 | 13 | 29.55 | - | - |
| Active | 109 | 93.97 | 180 | 80.00 | 113 | 83.70 | 31 | 70.45 | - | - |
| Number of sports practiced | 0.001 | 0.188 | ||||||||
| None | 0 | 0.00 | 13 | 5.78 | 6 | 4.44 | 7 | 15.91 | - | - |
| 1 | 11 | 9.48 | 35 | 15.56 | 26 | 19.26 | 11 | 25.00 | - | - |
| 2 | 41 | 35.34 | 100 | 44.44 | 47 | 34.81 | 15 | 34.09 | - | - |
| 3 or more | 64 | 55.17 | 77 | 34.22 | 56 | 41.48 | 11 | 25.00 | - | - |
| Sports | ||||||||||
| Outdoor | 87 | 75.00 | 160 | 71.11 | 94 | 69.63 | 28 | 63.64 | 0.366 | 0.089 |
| Fitness | 68 | 58.62 | 95 | 42.22 | 67 | 49.63 | 18 | 40.91 | 0.046 | 0.141 |
| Opponent | 31 | 26.72 | 39 | 17.33 | 22 | 16.30 | 2 | 4.55 | 0.001 | 0.213 |
| Variable | 41–50 | 51–60 | 61–70 | 71–80 | Levene’s Test | Means’s Test | Effect Size | ||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| M(SD) | M(SD) | M(SD) | M(SD) | F | p | X2 | p | η2 | IC 95% | ||
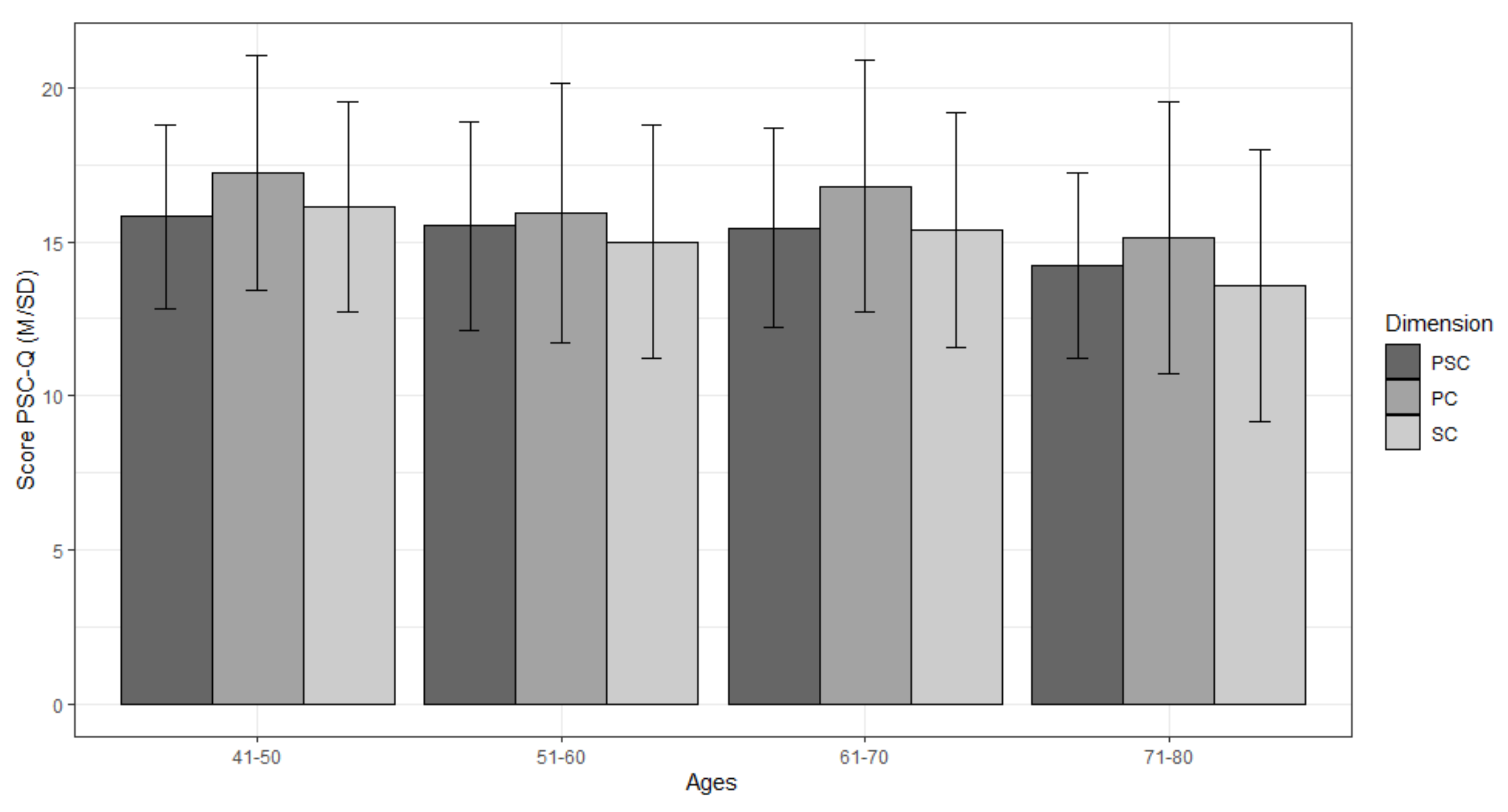
| PSC-Q | PSC | 15.81(2.97) | 15.51(3.40) | 15.45(3.24) | 14.22(3.01) | 0.775 | 0.508 | 9.571 | 0.022 | 0.02 | (0.00, 0.04) |
| PC | 17.25(3.80) | 15.94(4.21) | 16.80(4.07) | 15.13(4.42) | 1.117 | 0.341 | 13.326 | 0.001 | 0.03 | (0.00, 005) | |
| AT | 21.93(5.05) | 22.31(4.72) | 22.82(4.79) | 22.04(3.71) | 2.225 | 0.084 | 2.955 | 0.398 | 0.00 | (0.00, 0.01) | |
| SC | 16.13(3.43) | 15.00(3.80) | 15.40(3.81) | 13.59(4.40) | 2.239 | 0.084 | 16.344 | 0.001 | 0.03 | (0.01, 005) | |
| ST | 14.25(2.76) | 14.12(3.08) | 14.10(3.38) | 13.79(3.23) | 1.265 | 0.285 | 1.300 | 0.279 | 0.00 | (0.00, 0.00) | |
| TMMS24 | EA | 23.99(6.86) | 23.96(6.88) | 23.00(6.66) | 23.20(7.66) | 0.476 | 0.698 | 2.343 | 0.504 | 0.00 | (0.00, 0.00) |
| EU | 26.19(6.88) | 27.57(6.46) | 26.52(5.73) | 25.54(6.09) | 1.878 | 0.132 | 4.485 | 0.213 | 0.01 | (0.00, 0.03) | |
| ER | 28.12(6.10) | 28.67(6.48) | 27.34(6.44) | 27.45(6.58) | 0.729 | 0.535 | 4.245 | 0.236 | 0.01 | (0.00, 002) | |
| SMS | IM | 5.71(1.09) | 5.48(1.42) | 5.24(1.47) | 4.39(1.79) | 4.803 | 0.002 | 5.999 | 0.001 | 0.06 | (0.02, 0.09) |
| EM | 3.82(1.08) | 3.89(1.19) | 3.76(1.35) | 3.72(1.42) | 8.647 | 0.034 | 0.687 | 0.529 | 0.04 | (0.01, 0.07) | |
| NM | 2.15(1.13) | 2.08(1.08) | 2.45(1.24) | 2.88(1.47) | 3.692 | 0.011 | 5.717 | 0.001 | 0.04 | (0.01, 0.07) | |
| Dimension | PSC | ST | SC | AT | PC | EA | EU | ER | IM | EM | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| ST | 0.54 | ** | 1 | |||||||||||||||||
| (0.47, 0.60) | ||||||||||||||||||||
| SC | 0.58 | ** | 0.60 | ** | 1 | |||||||||||||||
| (0.52, 0.63) | (0.54, 0.65) | |||||||||||||||||||
| AT | 0.56 | ** | 0.57 | ** | 0.49 | 1 | ||||||||||||||
| (0.50, 0.63) | (0.51, 0.63) | (0.43, 0.56) | ||||||||||||||||||
| PC | 0.51 | ** | 0.64 | ** | 0.70 | ** | 0.60 | ** | 1 | |||||||||||
| (0.45, 0.57) | (0.58, 0.69) | (0.65, 0.74) | (0.55, 0.65) | |||||||||||||||||
| EA | 0.02 | 0.06 | 0.02 | 0.01 | 0.06 | 1 | ||||||||||||||
| (−0.06, 0.11) | (−0.03, 0.15) | (−0.07, 0.11) | (−0.08, 0.09) | (−0.03, 0.15) | ||||||||||||||||
| EU | 0.15 | ** | 0.19 | ** | 0.16 | ** | 0.11 | * | 0.16 | ** | 0.33 | ** | 1 | |||||||
| (0.07, 0.24) | (0.10, 0.27) | (0.08, 0.24) | (0.02, 0.19) | (0.08, 0.24) | (0.25, 0.40) | |||||||||||||||
| ER | 0.31 | ** | 0.30 | ** | 0.29 | ** | 0.25 | ** | 0.31 | ** | 0.21 | ** | 0.48 | ** | 1 | |||||
| (0.23, 0.38) | (0.22, 0.38) | (0.21, 0.36) | (0.17, 0.33) | (0.23, 0.38) | (0.13, 0.29) | (0.41, 0.54) | ||||||||||||||
| IM | 0.38 | ** | 0.35 | ** | 0.54 | ** | 0.26 | ** | 0.45 | ** | 0.16 | ** | 0.29 | ** | 0.35 | ** | 1 | |||
| (0.30, 0.45) | (0.28, 0.43) | (0.48, 0.60) | (0.18, 0.34) | (0.38, 0.52) | (0.08, 0.24) | (0.21, 0.36) | (0.27, 0.42) | |||||||||||||
| EM | 0.14 | ** | 0.16 | 0.38 | ** | 0.13 | ** | 0.32 | ** | 0.14 | ** | 0.08 | 0.17 | ** | 0.48 | ** | 1 | |||
| (0.05, 0.22) | (0.07, 0.24) | (0.31, 0.46) | (0.05, 0.21) | (0.24, 0.39) | (0.06, 0.22) | (−0.01, 0.16) | (0.08, 0.25) | (0.41, 0.54) | ||||||||||||
| NM | −0.38 | ** | −0.26 | ** | −0.28 | ** | −0.27 | ** | −0.28 | ** | 0.00 | −0.25 | ** | −0.25 | ** | −0.36 | ** | 0.07 | ** | |
| (−0.45, −0.31) | (−0.34, −0.26) | (0.36, −0.20) | (−0.35, −0.19) | (−0.36, −0,20) | (0.09, 0.08) | (−0.33, −0.16) | (−0.33, −0.17) | (−0.44, 0.29) | (0.01, 0.07) | |||||||||||
| Dimension | 41–50 Years | 51–60 Years | 61–70 Years | 71–80 Years | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| r | IC | p | r | IC | p | r | IC | p | r | IC | p | |
| ST | 0.51 | (0.36, 0.51) | 0.001 | 0.54 | (0.44, 0.63) | 0.001 | 0.56 | (0.43, 0.67) | 0.001 | 0.40 | (0.12, 0.63) | 0.010 |
| SC | 0.58 | (0.44, 0,69) | 0.001 | 0.62 | (0.53, 0.69) | 0.001 | 0.57 | (0.45, 0.68) | 0.001 | 0.20 | (−0.10, 0.47) | 0.190 |
| AT | 0.50 | (0.35, 0.63) | 0.001 | 0.58 | 0.49, 0.66) | 0.001 | 0.64 | (0.53, 0.73) | 0.001 | 0.28 | (−0.02, 0.53) | 0.060 |
| PC | 0.51 | (0.36, 0.51) | 0.001 | 0.52 | (0.42, 0.61) | 0.001 | 0.60 | (0.48, 0.70) | 0.001 | 0.23 | (−0.07, 0.49) | 0.140 |
| EA | −0.21 | (−0.38, −0.21) | 0.020 | 0.05 | (−0.08, 0.18) | 0.430 | 0.09 | (−0.08, 0.26) | 0.280 | 0.13 | (−0.18, 0.41) | 0.420 |
| EU | 0.17 | (−0.02, 0.17) | 0.070 | 0.16 | (0.03, 0.28) | 0.001 | 0.07 | (−0.10, 0.24) | 0.420 | 0.22 | (−0.08, 0.49) | 0.140 |
| ER | 0.26 | (0.08, 0.42) | 0.010 | 0.37 | (0.25, 0.48) | 0.001 | 0.22 | (0.06, 0.38) | 0.010 | 0.30 | (0.01, 0.55) | 0.050 |
| IM | 0.26 | (0.08, 0.42) | 0.001 | 0.46 | (0.35, 0.56) | 0.001 | 0.34 | (0.18, 0.48) | 0.001 | 0.25 | (−0.05, 0.51) | 0.100 |
| EM | 0.12 | (−0.02, 0.34) | 0.190 | 0.21 | (0.08, 0.33) | 0.001 | 0.06 | (−0.11, 0.23) | 0.500 | 0.07 | (−0.23, 0.36) | 0.650 |
| NM | −0.42 | (0.56, −0.25) | 0.001 | −0.39 | (−0.50, −0.28) | 0.001 | −0.32 | (−0.46, −0.32) | 0.001 | −0.34 | (−0.58, −0.05) | 0.020 |
| Variable | 41–50 Years | 51–60 Years | 61–70 Years | 71–80 Years | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| p | η2 | IC | p | η2 | IC | p | η2 | IC | p | η2 | IC | |
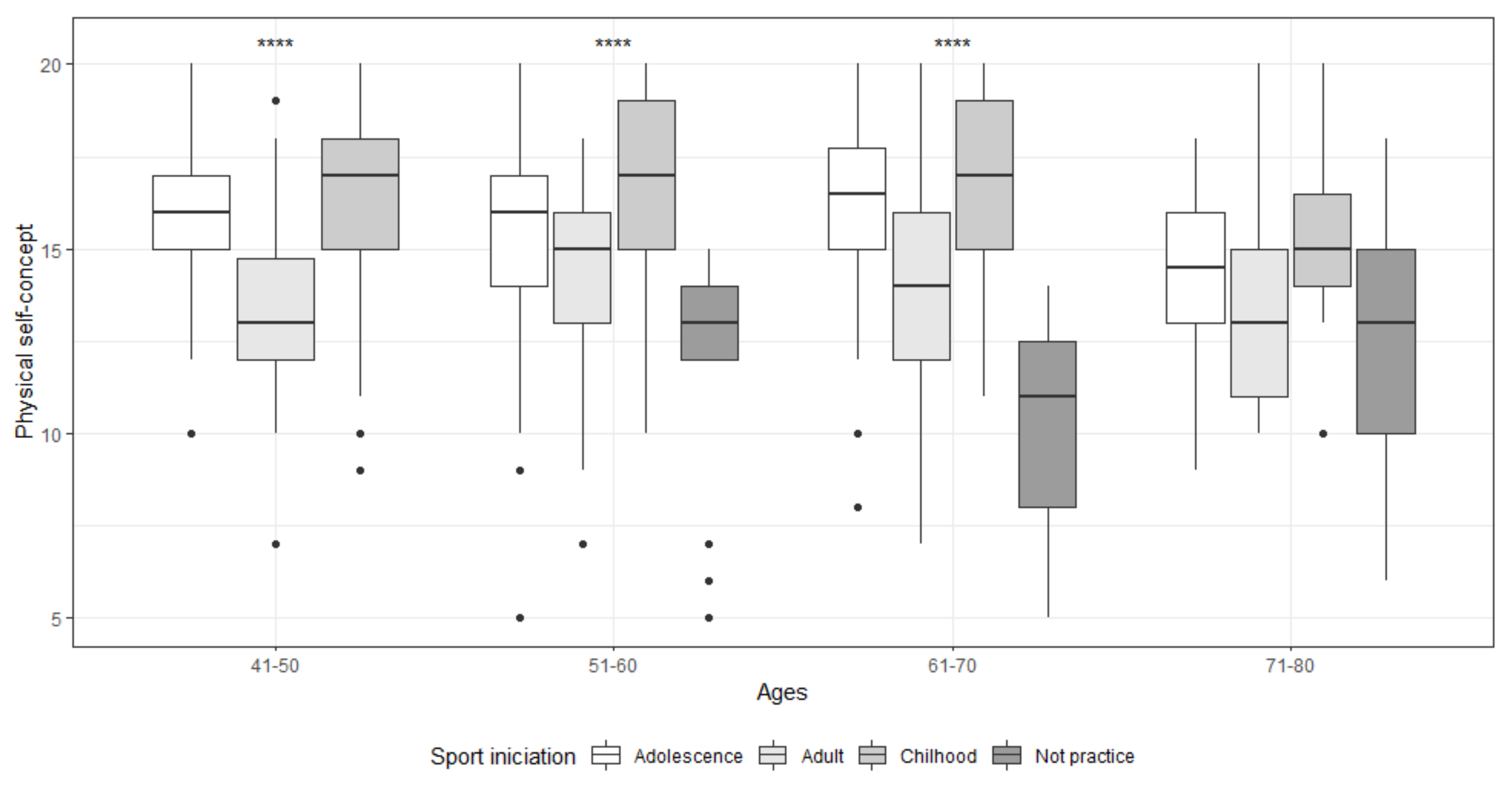
| Sportsinitiation | 0.001 | 0.19 | (0.08, 0.29) | 0.001 | 0.19 | (0.11, 0.26) | 0.001 | 0.23 | (0.13, 0.32) | 0.180 | 0.12 | (0.00, 0.26) |
| M | SD | M | SD | M | SD | M | SD | |||||
| Not practice | - | - | 11.62 | 3.33 | 10.17 | 3.49 | 12.43 | 4.20 | ||||
| Childhood | 16.53 | 2.46 | 16.53 | 2.46 | 16.53 | 2.44 | 15.38 | 2.71 | ||||
| Adolescence | 15.80 | 2.59 | 15.23 | 3.13 | 15.98 | 2.82 | 14.25 | 2.45 | ||||
| Adult | 13.41 | 2.68 | 14.20 | 2.46 | 13.77 | 3.13 | 13.56 | 3.09 | ||||
| PA level | p | d | IC | p | d | IC | p | d | IC | p | d | IC |
| 0.362 | 0.20 | (0.56, 0.96) | 0.001 | 0.50 | (0.17, 0.83) | 0.005 | 0.73 | (0.26, 1.19) | 0.262 | 0.51 | (0.15, 1.17) | |
| M | SD | M | SD | M | SD | M | SD | |||||
| Not active | 15.28 | 1.97 | 14.33 | 2.91 | 13.54 | 3.77 | 13.15 | 3.33 | ||||
| Active | 15.84 | 2.81 | 15.81 | 2.94 | 15.83 | 3.01 | 14.67 | 2.80 | ||||
| Number of sports | p | η2 | IC | p | η2 | IC | p | η2 | IC | p | η2 | IC |
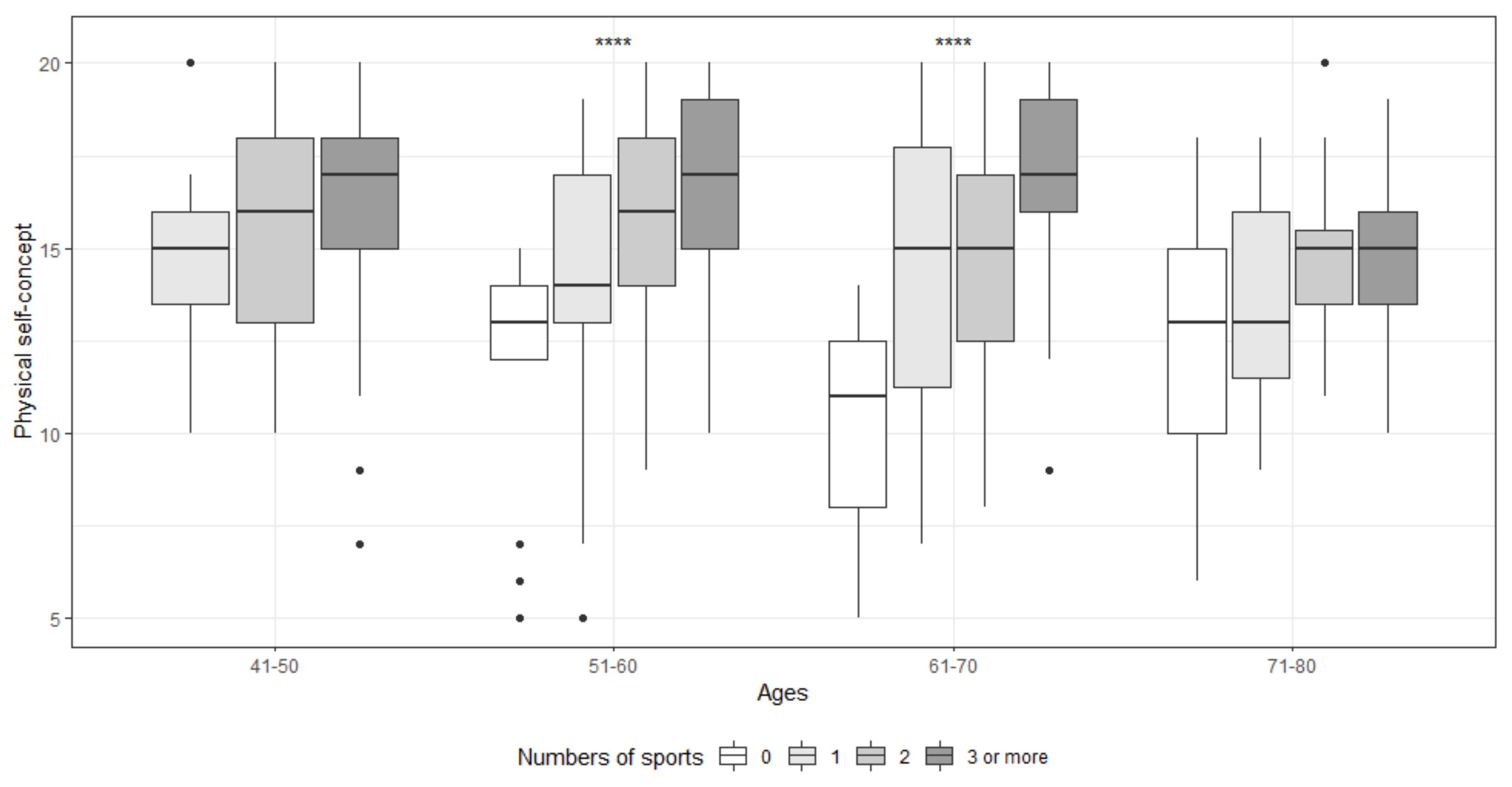
| 0.173 | 0.02 | (0.00, 0.07) | 0.001 | 0.17 | (0.09, 0.24) | 0.001 | 0.24 | (0.13, 0.33) | 0.401 | 0.10 | (0.00, 0.22) | |
| M | SD | M | SD | M | SD | M | SD | |||||
| None | - | - | 11.62 | 3.33 | 10.17 | 3.49 | 12.43 | 4.20 | ||||
| 1 | 14.82 | 2.79 | 14.37 | 3.21 | 14.58 | 3.78 | 13.73 | 3.10 | ||||
| 2 | 15.59 | 2.79 | 15.58 | 2.63 | 14.81 | 2.74 | 15.07 | 2.55 | ||||
| 3 or more | 16.12 | 2.75 | 16.61 | 2.55 | 16.98 | 2.39 | 14.73 | 2.45 | ||||
| Sports | p | η2 | IC | p | η2 | IC | p | η2 | IC | p | η2 | IC |
| 0.531 | 0.01 | (0.00, 0.03) | 0.543 | 0.19 | (0.00, 0.01) | 0.914 | 0.00 | (0.00, 0.01) | 0.666 | 0.02 | (0.00, 0.10) | |
| M | SD | M | SD | M | SD | M | SD | |||||
| Outdoors | 15.28 | 2.93 | 15.91 | 2.66 | 16.02 | 2.86 | 14.96 | 2.47 | ||||
| Fitness | 15.72 | 2.90 | 16.17 | 2.88 | 16.19 | 2.83 | 14.39 | 2.89 | ||||
| Opponent | 16.39 | 2.62 | 15.87 | 2.93 | 16.00 | 3.01 | 13.50 | 2.12 | ||||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Conde-Pipó, J.; Melguizo-Ibáñez, E.; Mariscal-Arcas, M.; Zurita-Ortega, F.; Ubago-Jiménez, J.L.; Ramírez-Granizo, I.; González-Valero, G. Physical Self-Concept Changes in Adults and Older Adults: Influence of Emotional Intelligence, Intrinsic Motivation and Sports Habits. Int. J. Environ. Res. Public Health 2021, 18, 1711. https://doi.org/10.3390/ijerph18041711
Conde-Pipó J, Melguizo-Ibáñez E, Mariscal-Arcas M, Zurita-Ortega F, Ubago-Jiménez JL, Ramírez-Granizo I, González-Valero G. Physical Self-Concept Changes in Adults and Older Adults: Influence of Emotional Intelligence, Intrinsic Motivation and Sports Habits. International Journal of Environmental Research and Public Health. 2021; 18(4):1711. https://doi.org/10.3390/ijerph18041711
Chicago/Turabian StyleConde-Pipó, Javier, Eduardo Melguizo-Ibáñez, Miguel Mariscal-Arcas, Félix Zurita-Ortega, Jose Luis Ubago-Jiménez, Irwin Ramírez-Granizo, and Gabriel González-Valero. 2021. "Physical Self-Concept Changes in Adults and Older Adults: Influence of Emotional Intelligence, Intrinsic Motivation and Sports Habits" International Journal of Environmental Research and Public Health 18, no. 4: 1711. https://doi.org/10.3390/ijerph18041711
APA StyleConde-Pipó, J., Melguizo-Ibáñez, E., Mariscal-Arcas, M., Zurita-Ortega, F., Ubago-Jiménez, J. L., Ramírez-Granizo, I., & González-Valero, G. (2021). Physical Self-Concept Changes in Adults and Older Adults: Influence of Emotional Intelligence, Intrinsic Motivation and Sports Habits. International Journal of Environmental Research and Public Health, 18(4), 1711. https://doi.org/10.3390/ijerph18041711