
Fitting Assistive Technology for People with Hearing Loss: The Importance of Remote Microphone Systems′ Electroacoustic Verification

 , , and
, , and
Abstract
:1. Introduction
- (1)
- Does the RMS setting require adjustment to achieve transparency?
- (2)
- If the transparency is achieved without adjustments in the RMS setting, can it be associated with the degree of hearing loss, RMS’s and HA’s brand, or type of receiver?
2. Materials and Methods
2.1. Participants
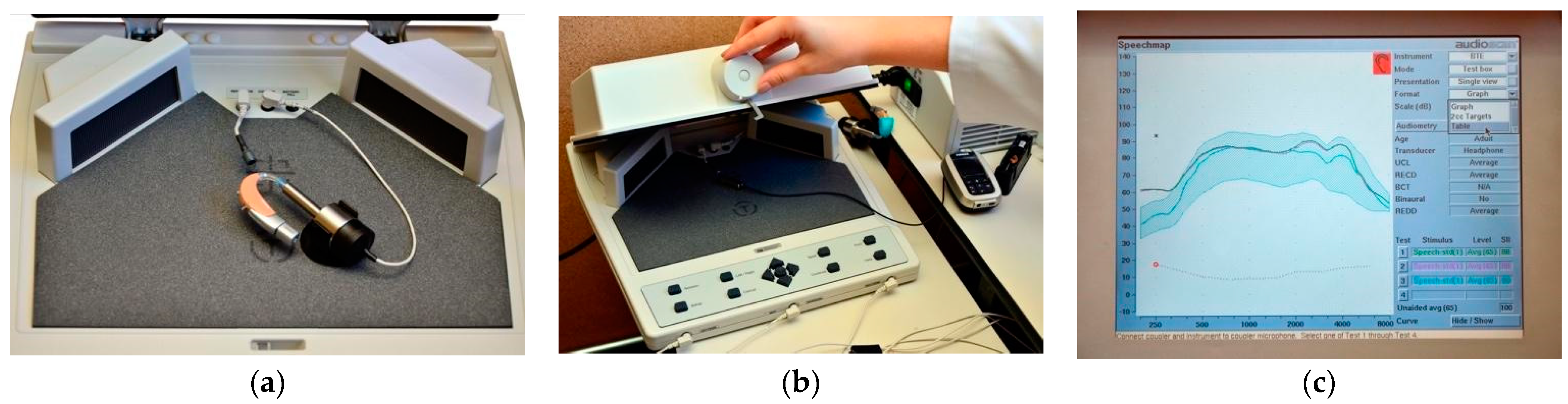
2.2. Procedure, Stimuli, and Equipment
3. Results
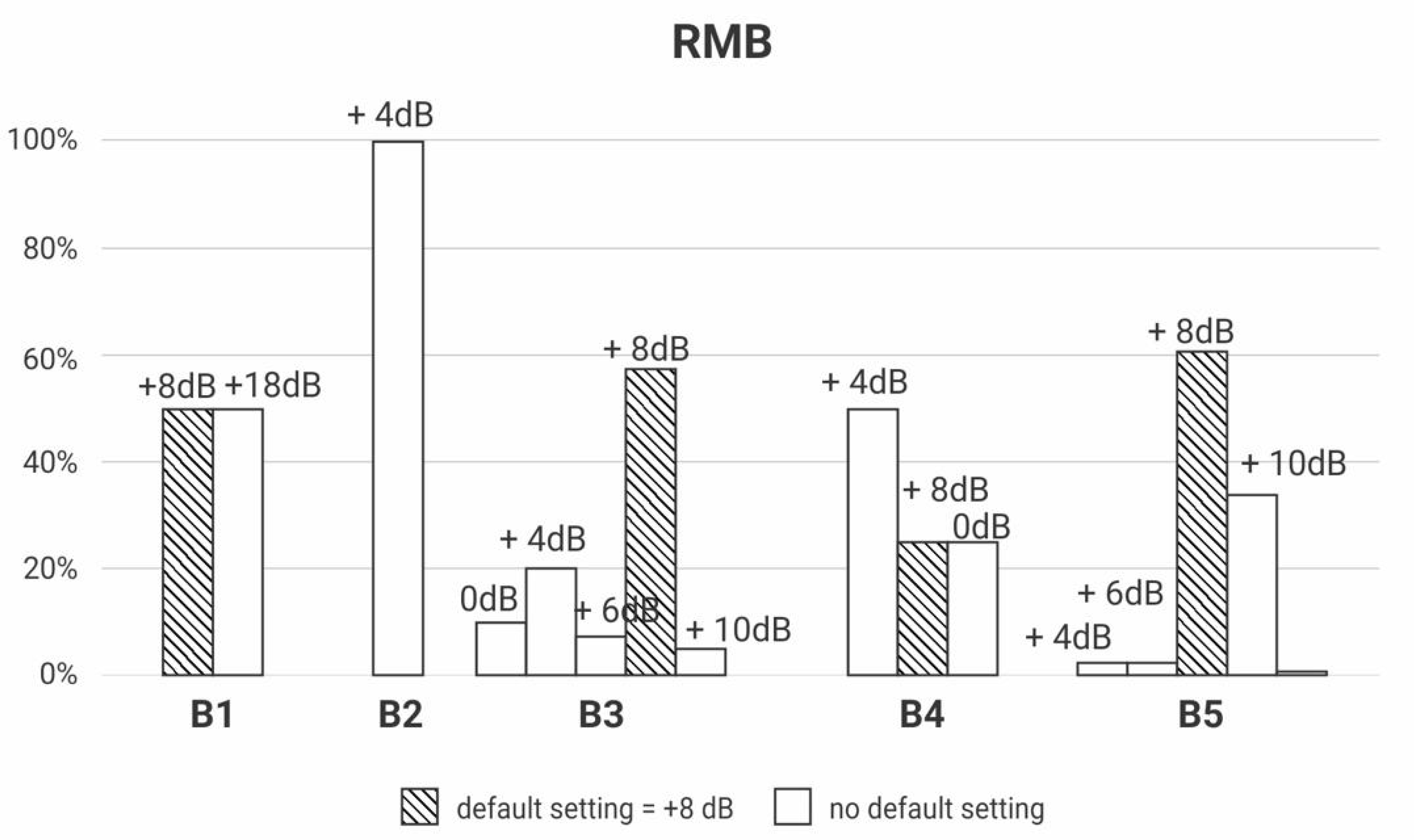
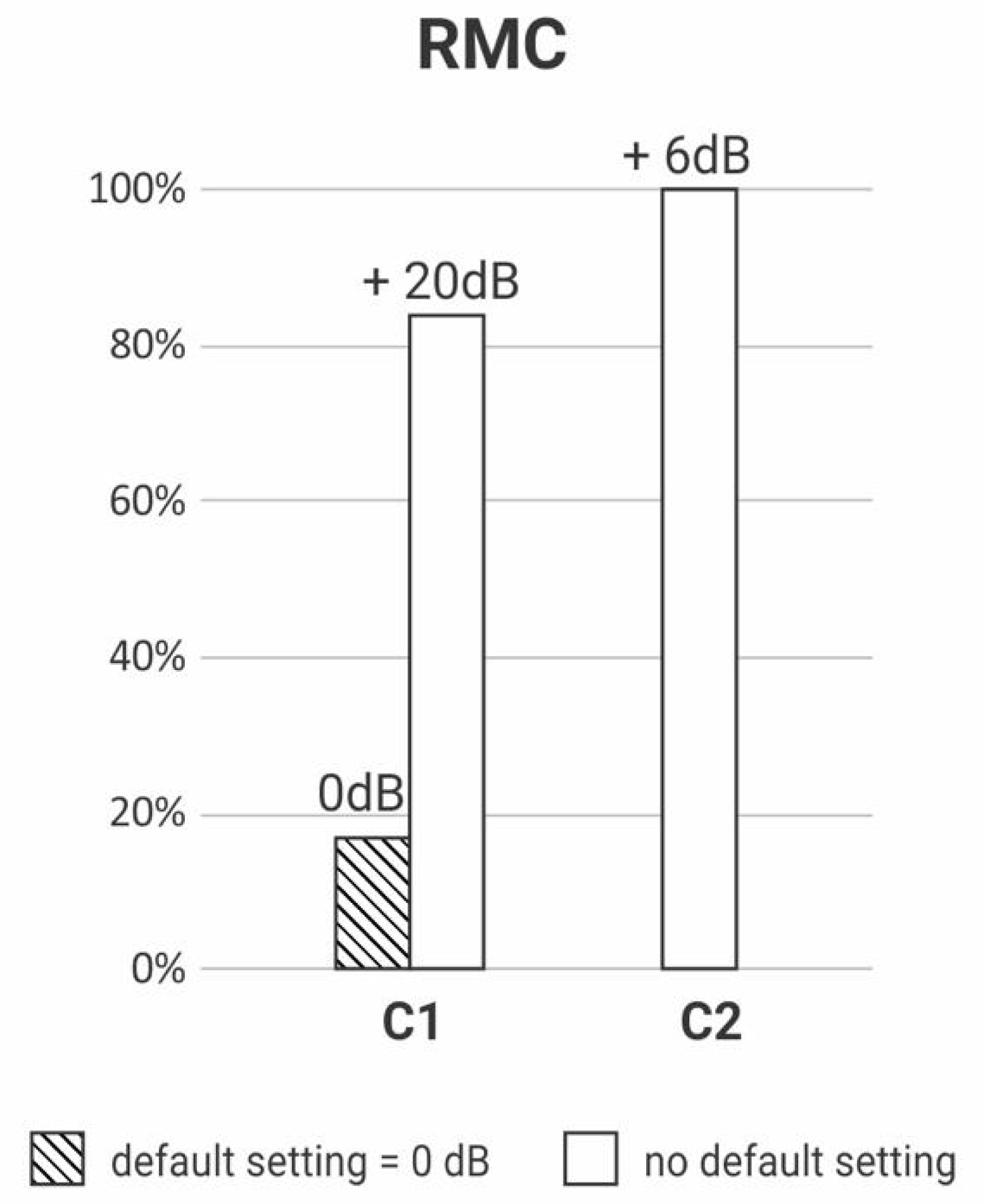
3.1. Does the RMS Setting Require Adjustment to Achieve Transparency?
3.2. If the Transparency Is Achieved without Adjustments in the RMS Setting, Can It Be Associated with the Degree of Hearing Loss, RMS’s and HA’s Brand, or Type of Receiver?
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Acknowledgments
Conflicts of Interest
References
- Thibodeau, L. Comparison of speech recognition with adaptive digital and FM remote microphone hearing assistance technology by listeners who use hearing aids. Am. J. Audiol. 2014, 23, 201–210. [Google Scholar] [CrossRef] [PubMed]
- American Speech-Language-Hearing Association. Guidelines for Fitting and Monitoring FM Systems. In American Speech-Language-Hearing Association, Desk Reference; American Speech-Language-Hearing Association: Rockville, MD, USA, 2002; Available online: https://www.asha.org/policy/gl2002-00010/ (accessed on 10 November 2020).
- Eiten, L.R.; Lewis, D.E. Verifying Frequency-Modulated System Performance: It’s the Right Thing To Do. Semin. Hear. 2010, 31, 233–240. Available online: https://doi.org/10.1055/s-0030-1262328 (accessed on 10 November 2020). [CrossRef]
- American Academy of Audiology. Remote Microphone Hearing Assistance Technologies for Children and Youth from Birth to 21 Years (Includes Supplement A). In American Academy of Audiology, Clinical Practice Guidelines; American Academy of Audiology: Reston, VA, USA, 2008; Updated 2011; Available online: http://www.audiology.org/resources/documentlibrary/Documents/HATGuideline.pdf. (accessed on 10 November 2020).
- International Bureau for Audiophonology. Recommendation 06/16–07/7. In Management of Hearing Assistive Technology (HAT)–FM/RF; International Bureau for Audiophonology: Valencia, Spain, 2017; Available online: https://www.biap.org/de/recommandations/recommendations/tc-06-hearing-aids/228-rec-06-16-07-7-en-management-of-hearing-assistive-technology/file (accessed on 10 November 2020).
- National Deaf Children’s Society, UK Children’s Radio Aid Working Group. Quality Standards for Use of Personal Radio Aids; National Deaf Children’s Society: London, UK, 2017; Available online: http://www.fmworkinggroup.org.uk (accessed on 12 July 2017).
- Cruz, A.D.; Jacob, R.T.S.; Fidêncio, V.L.D.; Ferreira, K.; Moret, A.L.M.; Lopes, N.B.F.; Morettin-Zupelari, M.; Costa Filho, O.A. Procedures characterization for fitting FM Systems in Audiological Publics Services. In Proceedings of the 32° Encontro Internacional de Audiologia, Gramado, Brazil, 21 April 2017. [Google Scholar]
- Symington, L.; De Conde Johnson, C. Using electroacoustic FM verification measures to assess the cross-compatibility of FM system components. In Proceedings of the A Sound Foundation Through Early Amplification, Chicago, IL, USA, 8–10 November 2010; Phonak: Stäfa, Switzerland, 2010. [Google Scholar]
- Thibodeau, L.M.; Wallace, S. Guidelines and Standards for Wireless Technology for Individuals with Hearing Loss. Semin. Hear. 2014, 35, 159–167. [Google Scholar]
- Norrix, L.W.; Camarota, K.; Harris, F.P.; Dean, J. The Effects of FM and Hearing Aid Microphone Settings, FM Gain, and Ambient Noise Levels on SNR. J. Am. Acad. Audiol. 2016, 27, 117–125. [Google Scholar] [CrossRef] [PubMed]
- Mulla, I. Pre-School Use of FM Amplification Technology. Ph.D. Thesis, University of Manchester, Manchester, NH, UK, 2011. Available online: https://www.escholar.manchester.ac.uk/api/datastream?publicationPid=uk-ac-man-scw:138160&datastreamId=FULL-TEXT.PDF (accessed on 10 November 2020).
- American National Standards Institute. American National Standard for the Specification of Hearing Aid Characteristics; ANSI S3.22-1976; American National Standards Institute: Melville, NY, USA, 1976. [Google Scholar]
- American National Standards Institute. American National Standard for the Specification of Hearing Aid Characteristics; ANSI S3.22-1982; American National Standards Institute: Melville, NY, USA, 1982. [Google Scholar]
- Schafer, E.C.; Thibodeau, L.M.; Whalen, H.S.; Overson, G.J. Electroacoustic evaluation of frequency-modulated receivers interfaced with personal hearing aids. Lang. Speech Hear. Serv. Sch. 2007, 38, 315–326. [Google Scholar] [CrossRef]
- American Speech-Language-Hearing Association. Guidelines for Fitting and Monitoring FM Systems. In American Speech-Language-Hearing Association, Desk Reference; American Speech-Language-Hearing Association: Rockville, MD, USA, 1994; (Suppl. 12). [Google Scholar]
- American Speech-Language-Hearing Association. Guidelines for Fitting and Monitoring FM Systems. In American Speech-Language-Hearing Association, Desk Reference, 2nd ed.; American Speech-Language-Hearing Association: Rockville, MD, USA, 1999. [Google Scholar]
- Phonak. iPOP Phonak Dynamic FM Offset Protocol; Phonak Sonova AG: Stäfa, Switzerland, 2009; Available online: https://www.yumpu.com/en/document/read/25302938/ipop-a-phonak-dynamic-offset-protocol (accessed on 10 November 2020).
- Phonak. Roger Verification Guide, Roger Offset Protocol for Roger (02) Receivers; Phonak Sonova AG: Stäfa, Switzerland, 2016; Available online: https://www.phonakpro.com/content/dam/phonakpro/gc_hq/de/products_solutions/wireless_accessories/roger_touchscreen_mic/documents/verification_guide_phonak_offset_protocol_roger.pdf (accessed on 10 November 2020).
- Nelson, J.A. Coupling FM systems to high-technology digital hearing aids. J. Educ. Audiol 2001, 9, 13–20. [Google Scholar]
- Nelson, J.A. Achieving Hearing Aid and FM System Transparency. Hear. Rev. 2002, 9, 14–20. [Google Scholar]
- Platz, R. SNR advantage, FM advantage, and FM fitting. Access: Achieving Clear Communication Employing Sound Solutions. In Proceedings of the First International Conference, Chicago, IL, USA, November 2003; Fabry, D., Ed.; Phonak: Stäfa, Switzerland, 2004; pp. 147–154. [Google Scholar]
- Thibodeau, L.; Mccaffrey, H.; Abrahamson, J. Effects of coupling hearing aids to FM systems via neckloops. J. Acad. Rehabil. Audiol 1998, 21, 49–56. [Google Scholar]
- Auriemmo, J.; Keenan, D.; Passerieux, D.; Kuk, F. Assessing FM transparency, FM/HA ratio with digital aids. Hear. J. 2005, 58, 30–42. [Google Scholar] [CrossRef]
- Blair, R.C.; Taylor, R.A. Bioestatística Para Ciências da Saúde; Pearson Education do Brasil: São Paulo, Brazil, 2013. [Google Scholar]
- Barreiros, A.G.E.; Mendes, B.C.A.; Ficker, L.B.; Novaes, B.C.A.C. Auditory rehabilitation: Family’s role in adherence to the use of wireless transmission system in school. Distúrb. Comum. 2016, 28, 718–729. [Google Scholar]
- Esturaro, G.T.; Novaes, B.C.D.A.C.; Deperon, T.M.; Martinez, M.A.N.; Mendes, B.D.C.A. Use of wireless transmission system and performance of hearing impaired students from the perspective of teachers. Distúrb. Comun. 2016, 28, 730–742. [Google Scholar]
- Schafer, E.C.; Musgrave, E.; Momin, S.; Sandrock, C.; Romine, D. A proposed electroacoustic test protocol for personal FM receivers coupled to cochlear implant sound processors. J. Am. Acad. Audiol. 2013, 24, 941–954. [Google Scholar] [CrossRef] [PubMed]
- Ward, Y. A Critical Evaluation of “AutoConnect” Using the Phonak MLxi Dynamic FM Receiver; MSc Audiology, University of Manchester: Manchester, UK, 2010. [Google Scholar]
- Bondurant, L.; Thibodeau, L. Behavioral verification of programmable FM advantage settings. J. Educ. Audiol. 2011, 17, 11–22. [Google Scholar]
- Salehi, H.; Parsa, V.; Folkeard, P. Electroacoustic assessment of wireless remote microphone systems. Audiol. Res. 2018, 8, 204. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Naeve-Velguth, S.; Miller, T.J.; Kujawa, S.K. Effect of MicroMLxS Designated Programmable Audio Input (DPAI) and Switch Settings on FM- and Muted-FM Transparency for Six DPAI Hearing Instruments. J. Educ. Audiol. 2009, 15, 53–62. [Google Scholar]
- Dijkstra, E.; Mülder, H.E. The Evolution of Wireless Systems in Pediatric Settings. In A Sound Foundation Through Early Amplification, Proceedings of the 7th Phonak International Pediatric Audiology Conference, Atlanta, GA, USA, 2–5 October 2016; Tharpe, A.M., Bagatto, M., Eds.; Phonak Sonova AG: Stäfa, Switzerland, 2016; Chapter 8; pp. 1–7. Available online: https://www.phonakpro.com/content/dam/phonakpro/gc_hq/en/events/2016/international_pediatric_audiology_conference_atlanta/chapter_08_dijkstra_draft.pdf (accessed on 10 November 2020).
- Feilner, M.; Rich, S.; Jones, C. Automatic and Directional for Kids, Scientific Background and Implementation of Pediatric Optimized Automatic Functions. In Phonak Insight; Phonak: Stäfa, Switzerland, 2016. [Google Scholar]
- Allen, S.; Mulla, I.; Ng, Z.Y.; Archbold, S.; Gregory, M. Using Radio Aids with Pre-School Deaf Children; National Deaf Children’s Society, The Ear Foundation: Londres, UK, 2017; Available online: https://www.ndcs.org.uk/media/1822/ear_foundation_using_radio_aids_with_preschool_deaf_children.pdf (accessed on 10 November 2020).
- Benítez-Barrera, C.; Angley, G.; Tharpe, A.M. Remote microphone use in the homes of children with hearing loss: Impact on parent and child language production. J. Speech Lang. Hear. Res. 2018, 61, 399–409. [Google Scholar] [CrossRef] [PubMed]
- Benítez-Barrera, C.; Thompson, E.; Angley, G.; Woynaroski, T.; Tharpe, A.M. Remote microphone use at home: Impact on child-directed speech. J. Speech Lang. Hear. Res. 2019, 62, 2002–2008. [Google Scholar] [CrossRef] [PubMed]
- Thompson, E.; Benítez-Barrera, C.R.; Angley, G.; Woynaroski, T.; Tharpe., A.M. Remote Microphone System Use in the Homes of Children with Hearing Loss: Impact on Caregiver Communication and Child Vocalizations. J. Speech Lang. Hear. Res. 2020, 63, 633–642. [Google Scholar] [CrossRef] [PubMed]
- Thompson, E.C.; Benítez-Barrera, C.R.; Tharpe, A.M. Home Use of Remote Microphone Systems by Children with Hearing Loss. Hear. J. 2020, 73, 34–36. [Google Scholar] [CrossRef]
- American National Standards Institute. American National Standard Specification of Performance Measurement of Hearing Assistance Devices/Systems; ANSI/ASA S3.47; American National Standards Institute: Washington, DC, USA, 2014. [Google Scholar]



{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variable | Category | Default Setting | p-Value | OR | CI 95% | p-Value | ||
|---|---|---|---|---|---|---|---|---|
| Yes | No | |||||||
| Degree of hearing loss | Mild | n | 6 | 10 | 0.264 | |||
| % | 4.1 | 7.6 | ||||||
| Moderate | n | 59 | 47 | 0.48 | 0.16–1.41 | 0.180 | ||
| % | 40.4 | 35.8 | ||||||
| Severe | n | 52 | 39 | 0.45 | 0.15–1.34 | 0.180 | ||
| % | 35.6 | 29.7 | ||||||
| Profound | n | 29 | 35 | 0.72 | 0.23–2.23 | 0.570 | ||
| % | 19.8 | 26.7 | ||||||
| Transmitter/receiver brand | RMB | n | 104 | 79 | 0.005 * | |||
| % | 71.2 | 60.3 | ||||||
| RMA | n | 40 | 40 | 1.32 | 0.78–2.23 | 0.310 | ||
| % | 27.4 | 30.5 | ||||||
| RMC | n | 2 | 12 | 7.90 | 1.72–36.32 | 0.002 * | ||
| % | 1.3 | 9.1 | ||||||
| Receiver | Design-dedicated | n | 110 | 97 | 0.053 | |||
| % | 75.3 | 74.0 | ||||||
| Universal | n | 32 | 22 | 0.78 | 0.42–1.43 | 0.030 * | ||
| % | 21.9 | 16.7 | ||||||
| Neckloop | n | 4 | 12 | 3.40 | 1.06 to 10.90 | 0.420 | ||
| % | 2.7 | 9.1 | ||||||
| Receiver | Design-dedicated | n | 110 | 97 | 0.421 | |||
| % | 77.4 | 81.5 | ||||||
| Universal | n | 32 | 22 | 0.78 | 0.24–2.50 | 0.420 | ||
| % | 21.9 | 16.7 | ||||||
| Receiver | Neckloop | n | 4 | 12 | 0.022 * | |||
| % | 2.7 | 9.1 | ||||||
| Universal and design-dedicated | n | 142 | 119 | 0.28 | 0.09–0.89 | 0.020 * | ||
| % | 97.2 | 90.8 | ||||||
| HA | RMB | n | 79 | 65 | 0.241 | |||
| % | 54.1 | 49.6 | ||||||
| RMA | n | 47 | 38 | 0.98 | 0.57–1.68 | 0.940 | ||
| % | 32.1 | 29 | ||||||
| Other | n | 20 | 28 | 1.70 | 0.88–3.30 | 0.110 | ||
| % | 13.7 | 21.3 | ||||||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Jacob, R.T.d.S.; Paccola, E.C.M.; Bucuvic, É.C.; Salgado, M.H. Fitting Assistive Technology for People with Hearing Loss: The Importance of Remote Microphone Systems′ Electroacoustic Verification. Int. J. Environ. Res. Public Health 2021, 18, 13251. https://doi.org/10.3390/ijerph182413251
Jacob RTdS, Paccola ECM, Bucuvic ÉC, Salgado MH. Fitting Assistive Technology for People with Hearing Loss: The Importance of Remote Microphone Systems′ Electroacoustic Verification. International Journal of Environmental Research and Public Health. 2021; 18(24):13251. https://doi.org/10.3390/ijerph182413251
Chicago/Turabian StyleJacob, Regina Tangerino de Souza, Elaine Cristina Moreto Paccola, Érika Cristina Bucuvic, and Manoel Henrique Salgado. 2021. "Fitting Assistive Technology for People with Hearing Loss: The Importance of Remote Microphone Systems′ Electroacoustic Verification" International Journal of Environmental Research and Public Health 18, no. 24: 13251. https://doi.org/10.3390/ijerph182413251
APA StyleJacob, R. T. d. S., Paccola, E. C. M., Bucuvic, É. C., & Salgado, M. H. (2021). Fitting Assistive Technology for People with Hearing Loss: The Importance of Remote Microphone Systems′ Electroacoustic Verification. International Journal of Environmental Research and Public Health, 18(24), 13251. https://doi.org/10.3390/ijerph182413251