
Adherence to an Injury Prevention Warm-Up Program in Children’s Soccer—A Secondary Analysis of a Randomized Controlled Trial

 , ,
, ,  , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
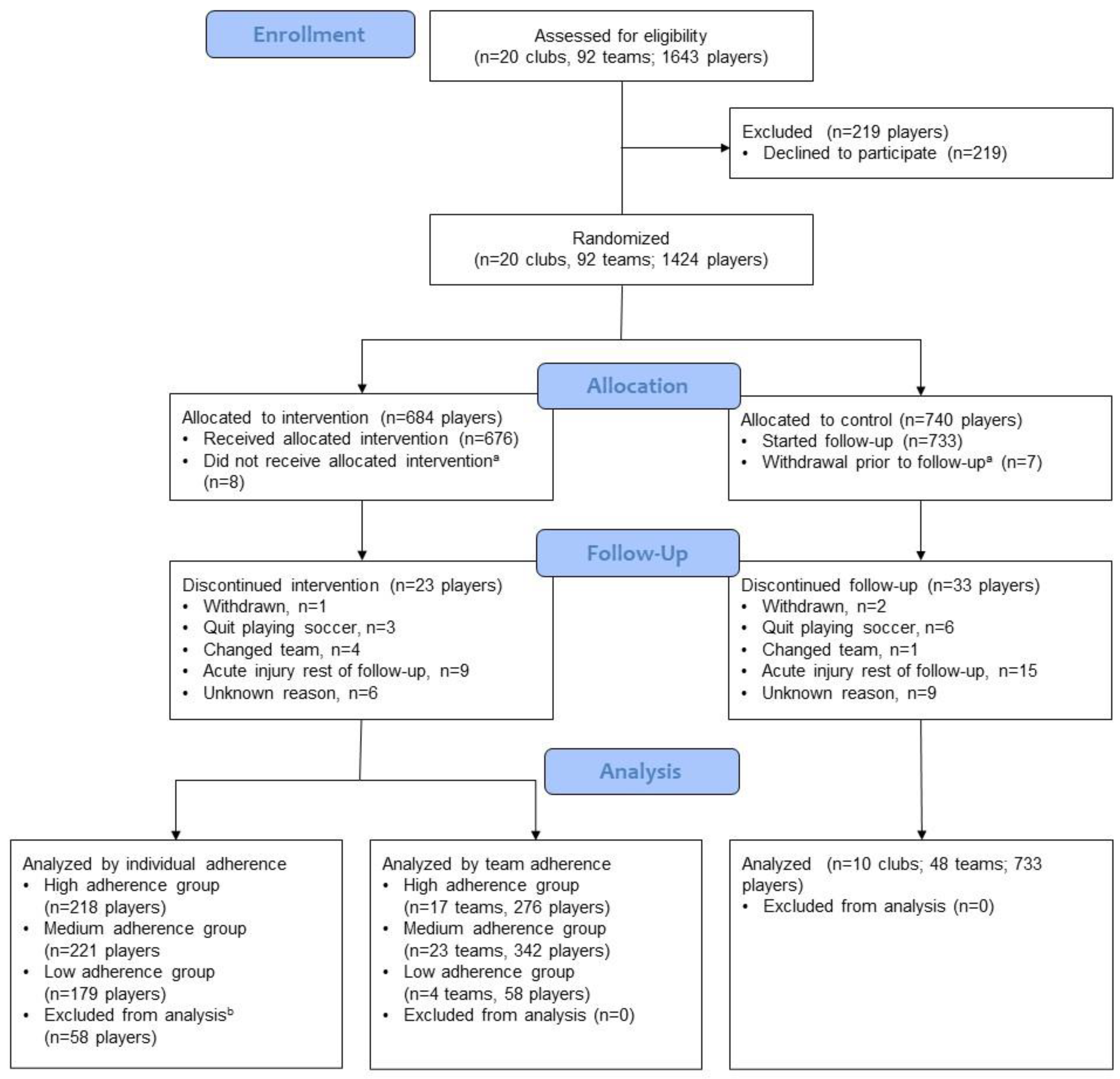
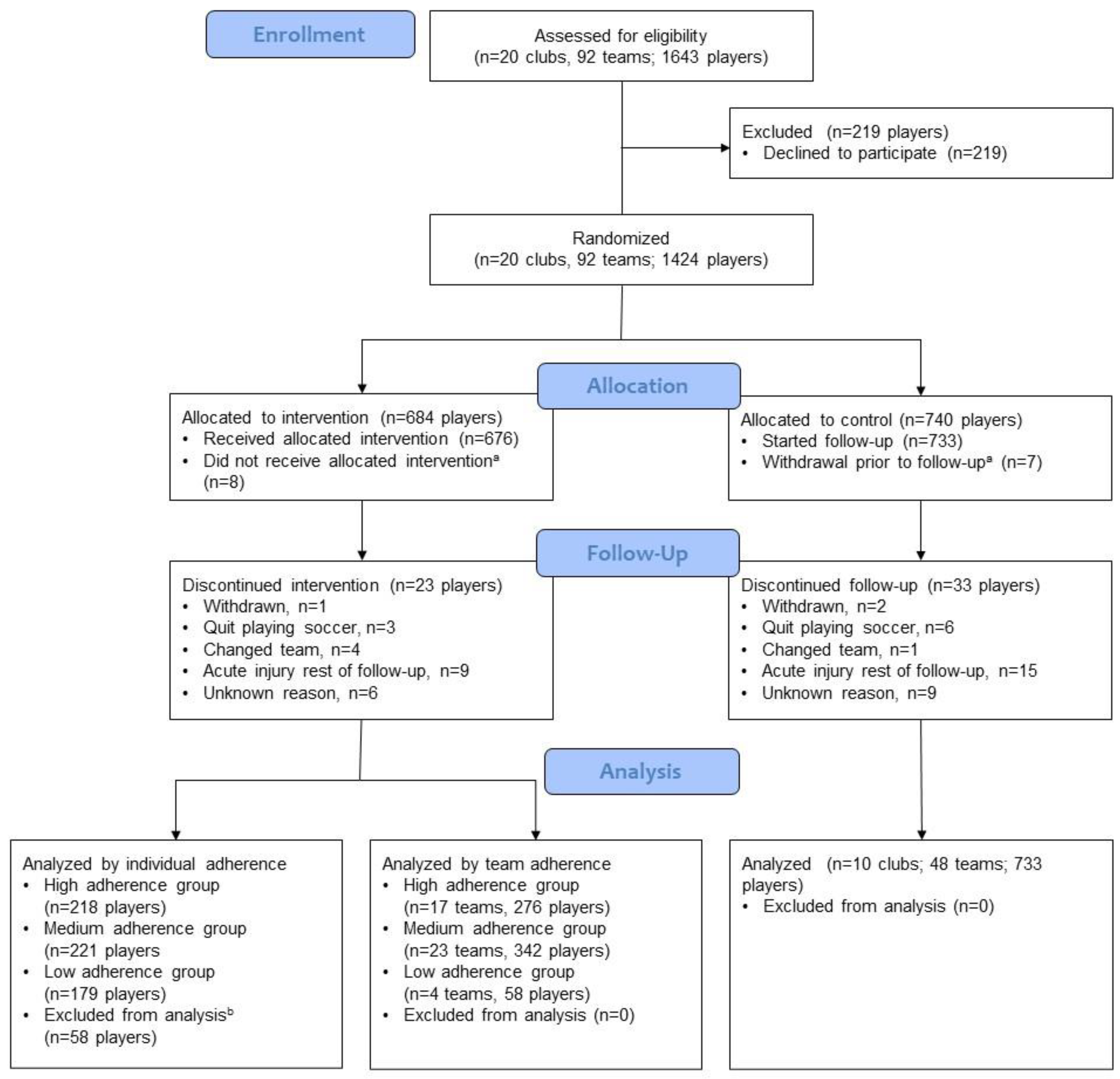
2.1. Participants and Randomization
2.2. Intervention
2.3. Team and Player Adherence
2.4. Injury and Exposure Recording
2.5. Coach Attitudes and Maintenance of the Program
2.6. Statistics
3. Results
3.1. Participants
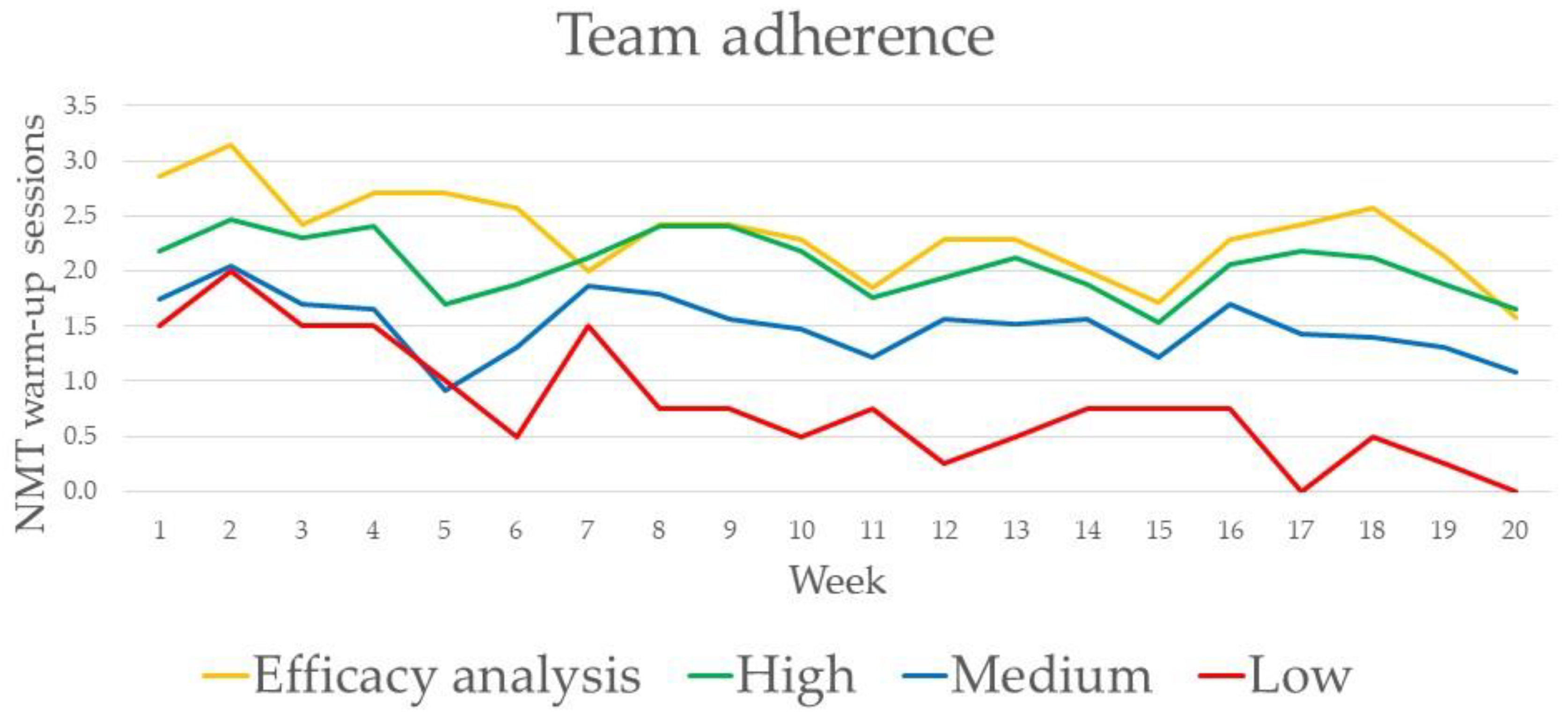
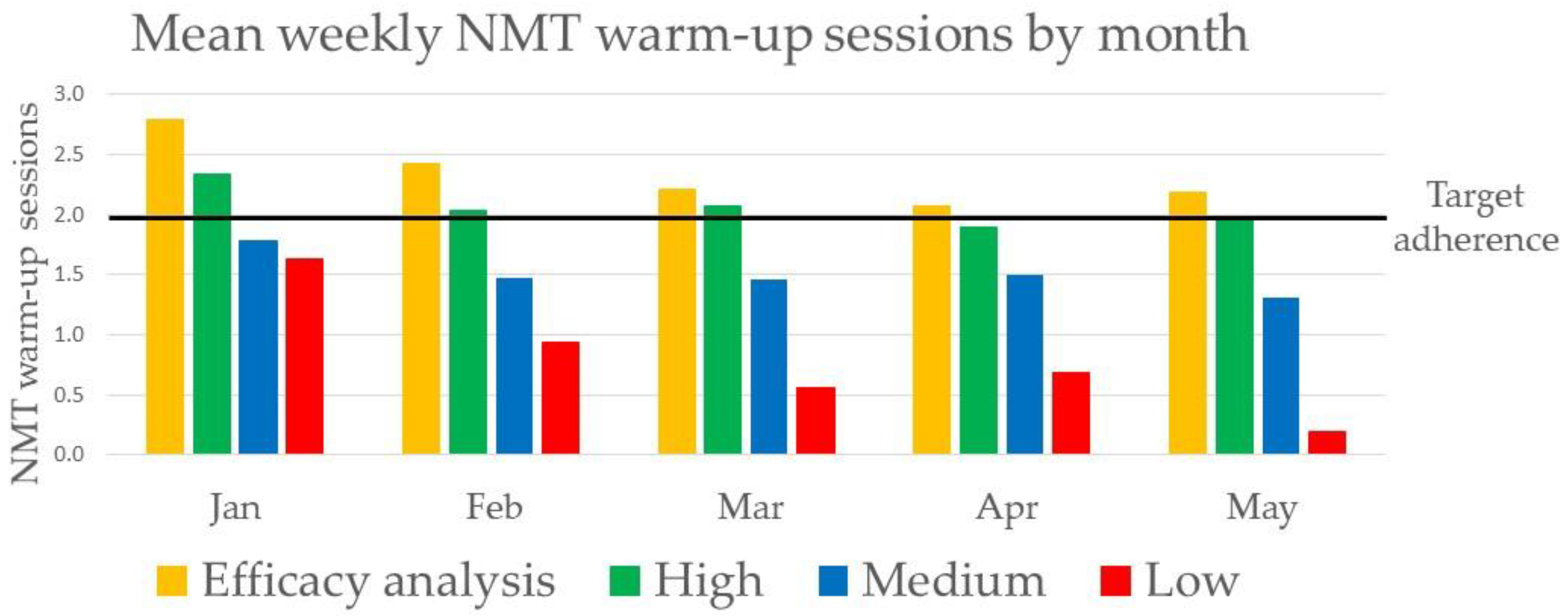
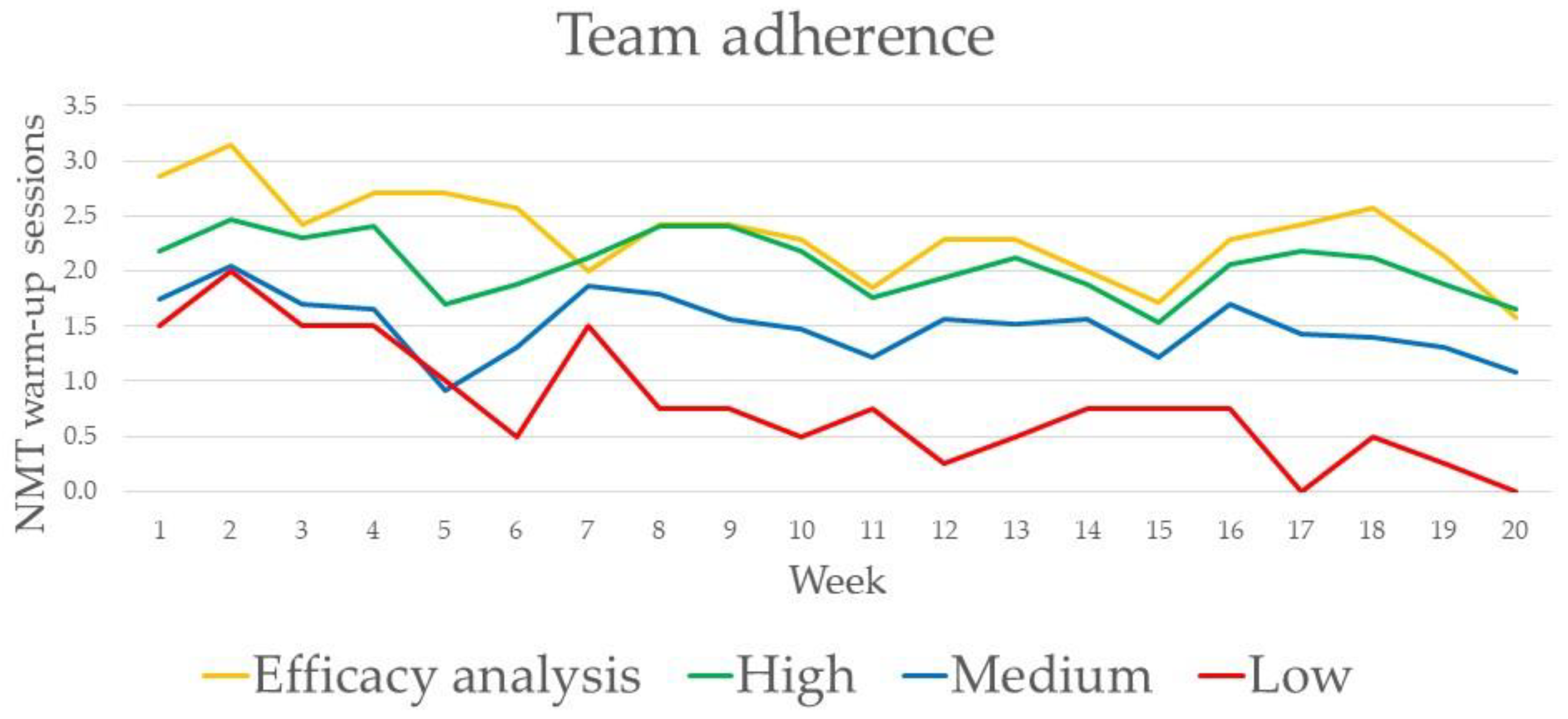
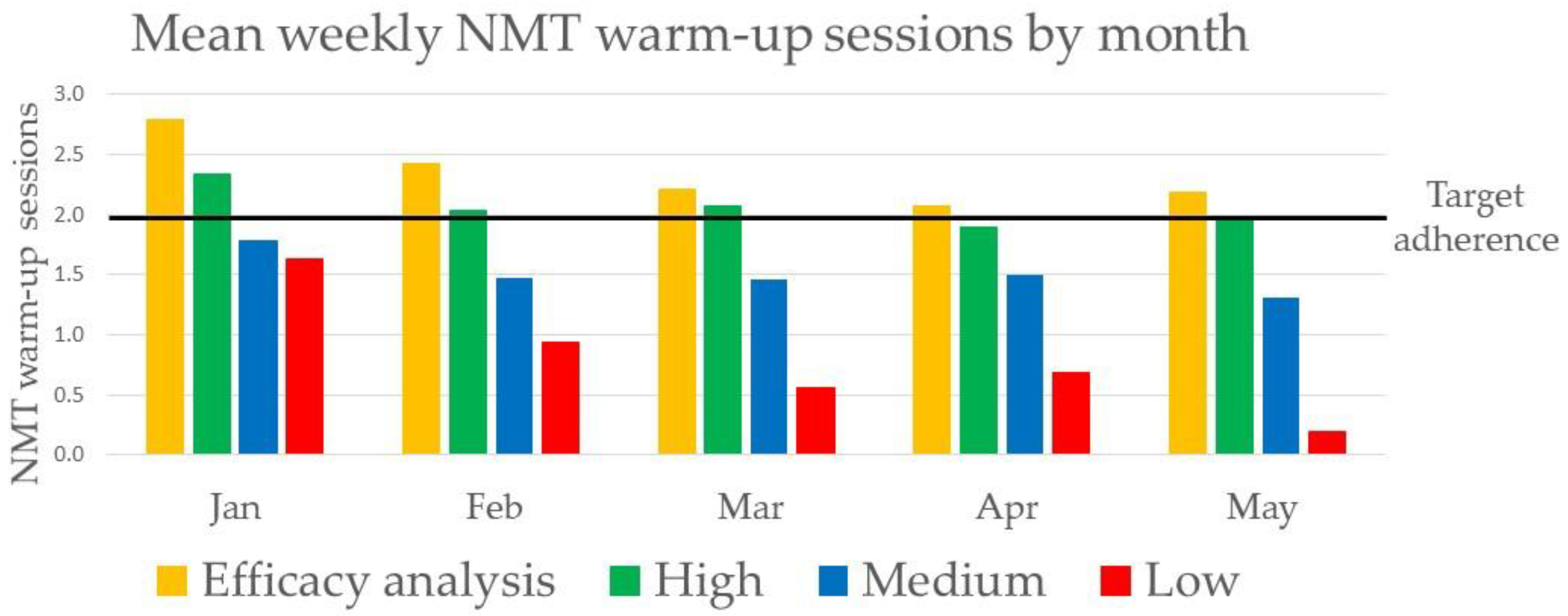
3.2. Adherence
3.3. Acute Injuries
3.4. Overuse Injuries
3.5. Efficacy Analysis
3.6. Coach Attitudes and Maintenance of the Program
- The warm-up was too long in duration. (n = 3)
- Overuse injury complaints were experienced to increase. (n = 2)
- The fidelity of performing the exercises varied between players. (n = 2)
- There were problems with limited spaces and limited time to do the warm-up properly. (n = 2)
- The involvement of ball skills in the warm-up was too little. (n = 1)
- Some exercises were too difficult for those under 12-years old. (n = 1)
- The warm-up was too demanding and tiring for the players in the beginning. (n = 1)
4. Discussion
4.1. Strengths and Limitations
4.2. Clinical Implementation
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Soligard, T.; Myklebust, G.; Steffen, K.; Holme, I.; Silvers, H.; Bizzini, M.; Junge, A.; Dvorak, J.; Bahr, R.; Andersen, E.A. Comprehensive warm-up programme to prevent injuries in young female footballers: Cluster randomised controlled trial. BMJ 2008, 337, a2469. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zarei, M.; Abbasi, H.; Namazi, P.; Asgari, M.; Rommers, N.; Rössler, R. The 11+ Kids warm-up programme to prevent injuries in young Iranian male high-level football (soccer) players: A cluster-randomised controlled trial. J. Sci. Med. Sport 2020, 23, 469–474. [Google Scholar] [CrossRef]
- Emery, C.A.; Meeuwisse, W.H. The effectiveness of a neuromuscular prevention strategy to reduce injuries in youth soccer: A cluster-randomised controlled trial. Br. J. Sports Med. 2010, 44, 555–562. [Google Scholar] [CrossRef]
- Rössler, R.; Junge, A.; Bizzini, M.; Verhagen, E.; Chomiak, J.; aus der Funten, K.; Meyer, T.; Dvorak, J.; Lichtenstein, E.; Beaudouin, F.; et al. A Multinational Cluster Randomised Controlled Trial to Assess the Efficacy of ‘11+ Kids’: A Warm-Up Programme to Prevent Injuries in Children’s Football. Sports Med. 2018, 48, 1493–1504. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Finch, C.F. A new framework for research leading to sports injury prevention. J. Sci. Med. Sport 2006, 9, 3–9. [Google Scholar] [CrossRef] [PubMed]
- Finch, C.F.; Donaldson, A. A sports setting matrix for understanding the implementation context for community sport. Br. J. Sports Med. 2010, 44, 973–978. [Google Scholar] [CrossRef]
- Verhagen, E.A.; Hupperets, M.D.W.; Finch, C.F.; van Mechelen, W. The impact of adherence on sports injury prevention effect estimates in randomised controlled trials: Looking beyond the CONSORT statement. J. Sci. Med. Sport 2011, 14, 287–292. [Google Scholar] [CrossRef] [PubMed]
- Mckay, C.D.; Merrett, C.K.; Emery, C.A. Predictors of FIFA 11+ Implementation Intention in Female Adolescent Soccer: An Application of the Health Action Process Approach (HAPA) Model. Int. J. Environ. Res. Public Health 2016, 13, 657. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Owoeye, O.B.A.; Mckay, C.D.; Verhagen, E.A.; Emery, C.A. Advancing adherence research in sport injury prevention. Br. J. Sports Med. 2018, 52, 1078. [Google Scholar] [CrossRef] [PubMed]
- Bizzini, M.; Dvorak, J. FIFA 11+: An effective programme to prevent football injuries in various player groups worldwide—a narrative review. Br. J. Sports Med. 2015, 49, 577–579. [Google Scholar] [CrossRef] [PubMed]
- Steffen, K.; Myklebust, G.; Olsen, O.E.; Holme, I.; Bahr, R. Preventing injuries in female youth football—A cluster-randomized controlled trial. Scand. J. Med. Sci. Sports 2008, 18, 605–614. [Google Scholar] [CrossRef] [PubMed]
- Soligard, T.; Nilstad, A.; Steffen, K.; Myklebust, G.; Holme, I.; Dvorak, J.; Bahr, R.; Andersen, T.E. Compliance with a comprehensive warm-up programme to prevent injuries in youth football. Br. J. Sports Med. 2010, 44, 787–793. [Google Scholar] [CrossRef] [PubMed]
- Steffen, K.; Emery, C.A.; Romiti, M.; Kang, J.; Bizzini, M.; Dvorak, J.; Finch, C.F.; Meeuwisse, W.H. High adherence to a neuromuscular injury prevention programme (FIFA 11+) improves functional balance and reduces injury risk in Canadian youth female football players: A cluster randomised trial. Br. J. Sports Med. 2013, 47, 794–802. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hägglund, M.; Atroshi, I.; Wagner, P.; Waldén, M. Superior compliance with a neuromuscular training programme is associated with fewer ACL injuries and fewer acute knee injuries in female adolescent football players: Secondary analysis of an RCT. Br. J. Sports Med. 2013, 47, 974–979. [Google Scholar] [CrossRef]
- Pasanen, K.; Parkkari, J.; Pasanen, M.; Hiilloskorpi, H.; Mäkinen, T.; Järvinen, M.; Kannus, P. Neuromuscular training and the risk of leg injuries in female floorball players: Cluster randomised controlled study. BMJ 2008, 337, a295. [Google Scholar] [CrossRef] [Green Version]
- Campbell, M.K.; Piaggio, G.; Elbourne, D.R.; Altman, D.G.; CONSORT Group. Consort 2010 statement: Extension to cluster randomised trials. BMJ 2012, 345, e5661. [Google Scholar] [CrossRef] [Green Version]
- Hilska, M.; Leppänen, M.; Vasankari, T.; Clarsen, B.; Aaltonen, S.; Bahr, R.; Haapasalo, H.; Parkkari, J.; Kannus, P.; Pasanen, K. Neuromuscular training warm-up in the prevention of overuse lower extremity injuries in children’s football: A cluster-randomized controlled trial. Transl. Sports Med. 2021, 00, 1–10. [Google Scholar] [CrossRef]
- Hilska, M.; Leppänen, M.; Vasankari, T.; Aaltonen, S.; Kannus, P.; Parkkari, J.; Steffen, K.; Kujala, U.M.; Konttinen, N.; Räisänen, A.M.; et al. Neuromuscular Training Warm-up Prevents Acute Noncontact Lower Extremity Injuries in Children’s Soccer: A Cluster Randomized Controlled Trial. Orthop. J. Sports Med. 2021, 9. [Google Scholar] [CrossRef]
- Fuller, C.W.; Ekstrand, J.; Junge, A.; Andersen, T.E.; Bahr, R.; Dvorak, J.; Hägglund, M.; McCrory, P.; Meeuwisse, W.H. Consensus statement on injury definitions and data collection procedures in studies of football (soccer) injuries. Br. J. Sports Med. 2006, 40, 193–201. [Google Scholar] [CrossRef] [PubMed]
- Clarsen, B.; Myklebust, G.; Bahr, R. Development and validation of a new method for the registration of overuse injuries in sports injury epidemiology: The Oslo Sports Trauma Research Centre (OSTRC) Overuse Injury Questionnaire. Br. J. Sports Med. 2013, 47, 495–502. [Google Scholar] [CrossRef] [Green Version]
- Lindblom, H.; Waldén, M.; Carlfjord, S.; Hägglund, M. Implementation of a neuromuscular training programme in female adolescent football: 3-year follow-up study after a randomised controlled trial. Br. J. Sports Med. 2014, 48, 1425–1430. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Emery, C.A.; Hagel, B.; Morrongiello, B.A. Injury Prevention in Child and Adolescent Sport: Whose Responsibility Is It? Clin. J. Sport Med. 2006, 16, 514–521. [Google Scholar] [CrossRef]
- Keats, M.R.; Emery, C.A.; Finch, C.F. Are We Having Fun Yet? Fostering Adherence to Injury Preventive Exercise Recommendations in Young Athletes. Sports Med. 2012, 42, 175–184. [Google Scholar] [CrossRef]
- Räisänen, A.M.; Owoeye, O.B.A.; Befus, K.; van den Berg, C.; Pasanen, K.; Emery, C.A. Warm-Ups and Coaches’ Perceptions: Searching for Clues to Improve Injury Prevention in Youth Basketball. Front. Sports Act. Living 2021, 3, 619291. [Google Scholar] [CrossRef] [PubMed]
- Norcross, M.F.; Johnson, S.T.; Bovbjerg, V.E.; Koester, M.C.; Hoffman, M.A. Factors influencing high school coaches’ adoption of injury prevention programs. J. Sci. Med. Sport 2016, 19, 299–304. [Google Scholar] [CrossRef] [PubMed]
- O’Brien, J.; Young, W.; Finch, C.F. The delivery of injury prevention exercise programmes in professional youth soccer: Comparison to the FIFA 11+. J. Sci. Med. Sport 2016, 20, 26–31. [Google Scholar] [CrossRef] [PubMed]
- Eckard, T.; Padua, D.A.; Hearn, D.W.; Pexa, B.S.; Frank, B.S. The Relationship Between Training Load and Injury in Athletes: A Systematic Review. Sports Med. 2018, 48, 1929–1961. [Google Scholar] [CrossRef] [PubMed]
- Drew, M.K.; Finch, C.F. The Relationship Between Training Load and Injury, Illness and Soreness: A Systematic and Literature Review. Sports Med. 2016, 46, 861–883. [Google Scholar] [CrossRef] [PubMed]
- Owoeye, O.B.A.; Emery, C.A.; Befus, K.; Palacios-Derflingher, L.; Pasanen, K. How much, how often, how well? Adherence to a neuromuscular training warm-up injury prevention program in youth basketball. J. Sports Sci. 2020, 38, 2329–2337. [Google Scholar] [CrossRef] [PubMed]
- Perera, N.K.P.; Hägglund, M. We have the injury prevention exercise programme, but how well do youth follow it? J. Sci. Med. Sport 2020, 23, 463–468. [Google Scholar] [CrossRef] [Green Version]

{kind=link}
{kind=link}
{kind=link}
| High | Medium | Low | Control | p-Value 1 | |
|---|---|---|---|---|---|
| Teams, n | 17 | 23 | 4 | 48 | - |
| Players, n | 276 | 342 | 58 | 733 | - |
| Females, % | 15 | 21 | 5 | 22 | 0.002 |
| Age, mean (SD) | 12.2 (1.3) | 12.0 (1.1) | 13.2 (0.8) | 12.3 (1.1) | <0.001 |
| Previous injuries (yes/no) 2, yes n (%) | 124 (45) | 141 (41) | 34 (59) | 291 (40) | 0.002 |
| Weekly exposure hours, mean (SD) | 5.1 (1.5) | 5.4 (1.2) | 7.2 (1.2) | 4.5 (0.9) | <0.001 |
| NMT warm-up sessions per week, mean (SD) | 2.1 (0.3) | 1.5 (0.2) | 0.8 (0.5) | - | <0.001 |
| Team Adherence | Player Adherence | ||||||
|---|---|---|---|---|---|---|---|
| Injury Incidence per 1000 h (95% CI) | Crude 1 IRR (95% CI) | Adjusted 2 IRR (95% CI) | Injury Incidence per 1000 h | Crude 1 IRR (95% CI) | Adjusted 2 IRR (95% CI) | ||
| LE Injuries | |||||||
| High | 4.77 (4.01 to 5.64) | 0.87 (0.71 to 1.08) | 0.88 (0.71 to 1.10) | High | 4.15 (3.37 to 5.06) | 0.76 (0.60 to 0.96) | 0.77 (0.61 to 0.96) |
| Medium | 4.17 (3.54 to 4.88) | 0.77 (0.54 to 1.09) | 0.78 (0.57 to 1.08) | Medium | 5.14 (4.29 to 6.12) | 0.96 (0.72 to 1.27) | 0.97 (0.73 to 1.28) |
| Low | 3.50 (2.35 to 5.02) | 0.66 (0.48 to 0.90) | 0.66 (0.45 to 0.96) | Low | 4.23 (3.38 to 5.23) | 0.78 (0.55 to 1.11) | 0.79 (0.57 to 1.11) |
| Control | 5.48 (4.93 to 6.08) | 1 (reference) | 1 (reference) | Control | 5.48 (4.93 to 6.08) | 1 (reference) | 1 (reference) |
| Noncontact LE Injuries | |||||||
| High | 1.87 (1.41 to 2.43) | 0.67 (0.48 to 0.94) | 0.69 (0.49 to 0.97) | High | 1.87 (1.37 to 2.51) | 0.67 (0.51 to 0.89) | 0.68 (0.51 to 0.91) |
| Medium | 1.83 (1.43 to 2.32) | 0.67 (0.42 to 1.07) | 0.69 (0.46 to 1.02) | Medium | 2.09 (1.57 to 2.73) | 0.77 (0.47 to 1.24) | 0.79 (0.49 to 1.25) |
| Low | 1.43 (0.75 to 2.48) | 0.52 (0.34 to 0.79) | 0.53 (0.36 to 0.77) | Low | 1.67 (1.16 to 2.33) | 0.61 (0.34 to 1.08) | 0.63 (0.37 to 1.05) |
| Control | 2.76 (2.38 to 3.20) | 1 (reference) | 1 (reference) | Control | 2.76 (2.38 to 3.20) | 1 (reference) | 1 (reference) |
| Team Adherence | Player Adherence | |||||||
|---|---|---|---|---|---|---|---|---|
| Mean Weekly Injury Prevalence % (95% CI) | Crude 1 OR (95% CI) | Adjusted 2 OR | Mean Weekly Injury Prevalence % (95% CI) | Crude 1 OR (95% CI) | Adjusted 2 OR | |||
| LE Injuries | ||||||||
| High | 12.5 (11.6 to 13.5) | 1.01 (0.98 to 1.04) | 1.01 (0.98 to 1.04) | High | 8.9 (8.0 to 9.8) | 1.01 (0.98 to 1.05) | 1.01 (0.98 to 1.05) | |
| Medium | 10.2 (9.4 to 11.0) | 1.01 (0.98 to 1.04) | 1.01 (0.98 to 1.04) | Medium | 9.3 (8.4 to 10.2) | 1.00 (0.97 to 1.03) | 1.00 (0.97 to 1.03) | |
| Low | 15.5 (13.2 to 18.0) | 1.01 (0.96 to 1.07) | 1.01 (0.96 to 1.07) | Low | 15.5 (14.3 to 16.9) | 1.02 (0.99 to 1.05) | 1.02 (0.99 to 1.05) | |
| Control | 11.3 (10.7 to 11.9) | 1 (reference) | 1 (reference) | Control | 11.3 (10.7 to 11.9) | 1 (reference) | 1 (reference) | |
| Substantial LE Injuries | ||||||||
| High | 6.1 (5.5 to 6.8) | 1.00 (0.96 to 1.04) | 1.00 (0.96 to 1.04) | High | 3.4 (2.9 to 4.0) | 1.00 (0.95 to 1.05) | 1.00 (0.95 to 1.05) | |
| Medium | 5.5 (4.9 to 6.1) | 0.99 (0.96 to 1.03) | 0.99 (0.96 to 1.03) | Medium | 4.6 (4.0 to 5.3) | 0.99 (0.94 to 1.03) | 0.99 (0.94 to 1.03) | |
| Low | 9.2 (7.5 to 11.2) | 1.00 (0.94 to 1.07) | 1.01 (0.94 to 1.08) | Low | 8.6 (7.7 to 9.6) | 1.01 (0.97 to 1.05) | 1.01 (0.97 to 1.05) | |
| Control | 5.0 (4.7 to 5.4) | 1 (reference) | 1 (reference) | Control | 5.0 (4.7 to 5.4) | 1 (reference) | 1 (reference) | |
| Acute Injuries | Injury Incidence per 1000 h (95% CI) | Crude 1 IRR (95% CI) | Adjusted 2 IRR (95% CI) |
| LE injuries | 4.72 (3.56 to 6.14) | 0.87 (0.57 to 1.34) | 0.87 (0.59 to 1.29) |
| Noncontact LE injuries | 1.45 (0.86 to 2.31) | 0.52 (0.28 to 1.001) | 0.53 (0.29 to 0.97) |
| Overuse Injuries | Mean Weekly Injury Prevalence % (95% CI) | Crude 3 OR (95% CI) | Adjusted 4 OR (95% CI) |
| LE injuries | 13.2 (11.8 to 14.7) | 0.99 (0.95 to 1.03) | 0.99 (0.95 to 1.03) |
| Substantial LE injuries | 6.3 (5.4 to 7.4) | 0.98 (0.93 to 1.03) | 0.98 (0.93 to 1.03) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Hilska, M.; Leppänen, M.; Vasankari, T.; Aaltonen, S.; Raitanen, J.; Räisänen, A.M.; Steffen, K.; Forsman, H.; Konttinen, N.; Kujala, U.M.; et al. Adherence to an Injury Prevention Warm-Up Program in Children’s Soccer—A Secondary Analysis of a Randomized Controlled Trial. Int. J. Environ. Res. Public Health 2021, 18, 13134. https://doi.org/10.3390/ijerph182413134
Hilska M, Leppänen M, Vasankari T, Aaltonen S, Raitanen J, Räisänen AM, Steffen K, Forsman H, Konttinen N, Kujala UM, et al. Adherence to an Injury Prevention Warm-Up Program in Children’s Soccer—A Secondary Analysis of a Randomized Controlled Trial. International Journal of Environmental Research and Public Health. 2021; 18(24):13134. https://doi.org/10.3390/ijerph182413134
Chicago/Turabian StyleHilska, Matias, Mari Leppänen, Tommi Vasankari, Sari Aaltonen, Jani Raitanen, Anu M. Räisänen, Kathrin Steffen, Hannele Forsman, Niilo Konttinen, Urho M. Kujala, and et al. 2021. "Adherence to an Injury Prevention Warm-Up Program in Children’s Soccer—A Secondary Analysis of a Randomized Controlled Trial" International Journal of Environmental Research and Public Health 18, no. 24: 13134. https://doi.org/10.3390/ijerph182413134
APA StyleHilska, M., Leppänen, M., Vasankari, T., Aaltonen, S., Raitanen, J., Räisänen, A. M., Steffen, K., Forsman, H., Konttinen, N., Kujala, U. M., & Pasanen, K. (2021). Adherence to an Injury Prevention Warm-Up Program in Children’s Soccer—A Secondary Analysis of a Randomized Controlled Trial. International Journal of Environmental Research and Public Health, 18(24), 13134. https://doi.org/10.3390/ijerph182413134