
Eight-Year Retrospective Study of Young Adults in a Diabetes Transition Clinic




Abstract
:1. Introduction
2. Subjects and Methods
2.1. The Diabetes Transition Clinic
2.2. Data Collection
2.3. Statistical Analysis
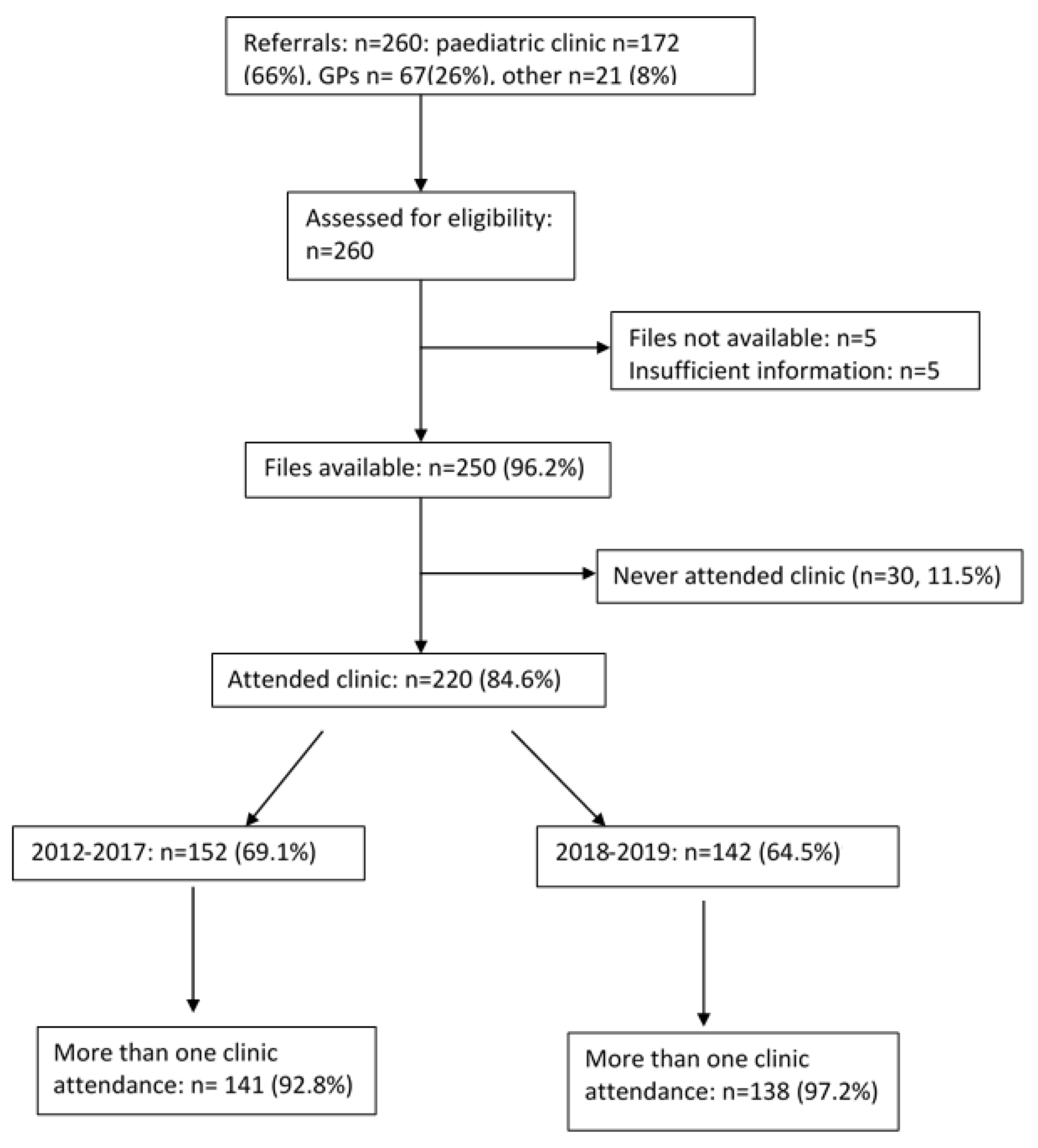
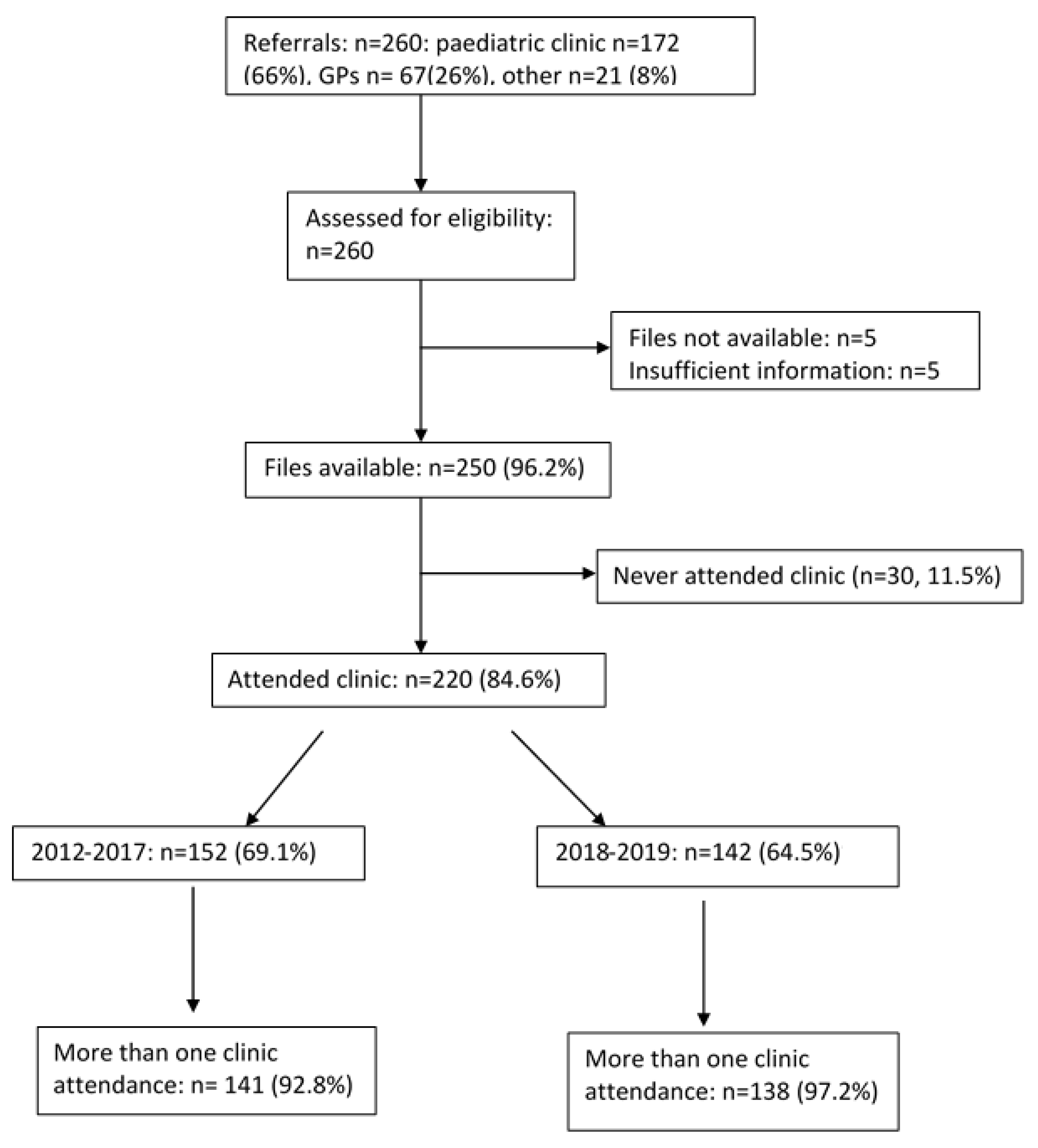
3. Results
3.1. Characteristics
3.2. Comparison of People with and without Mental Health Conditions
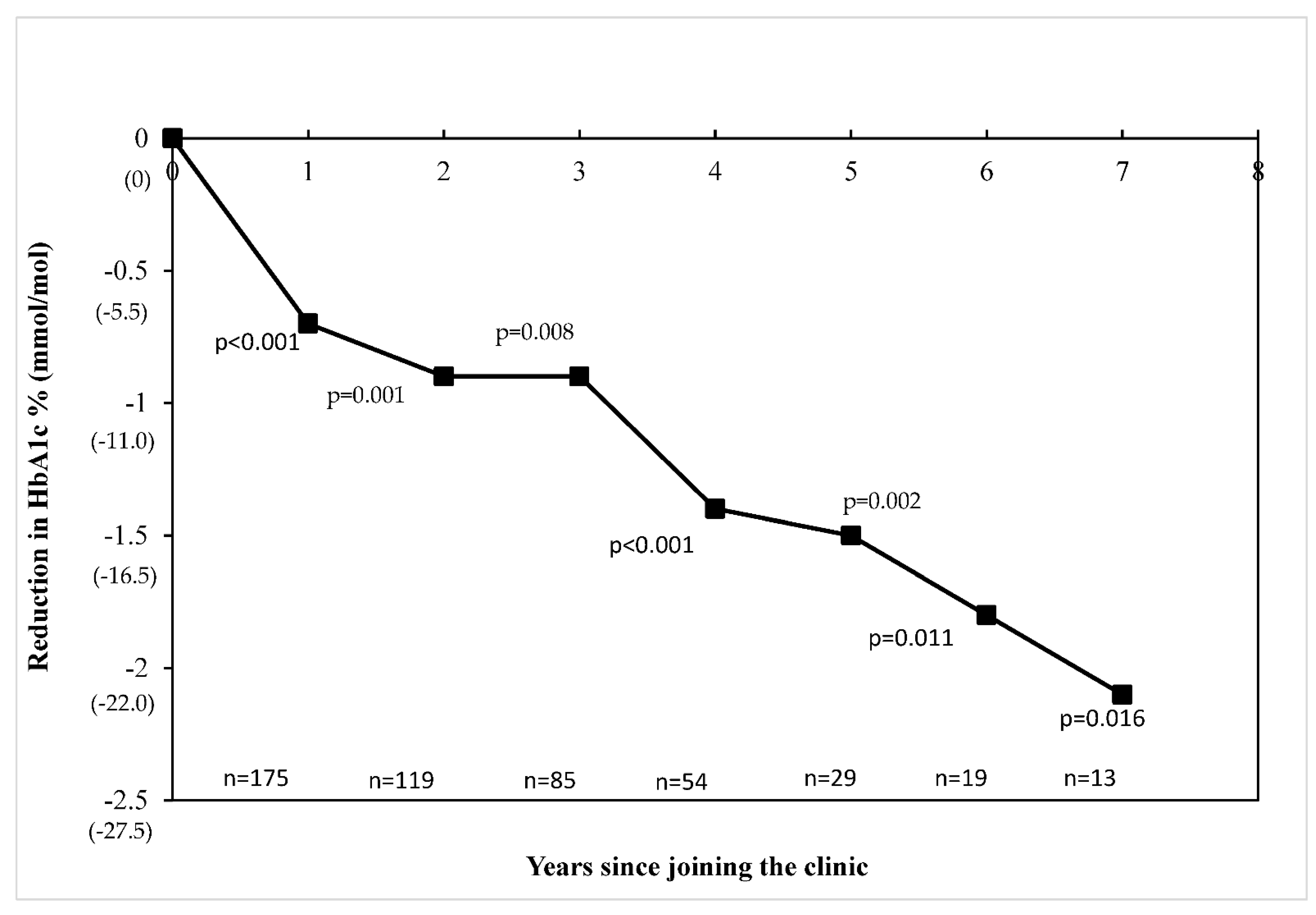
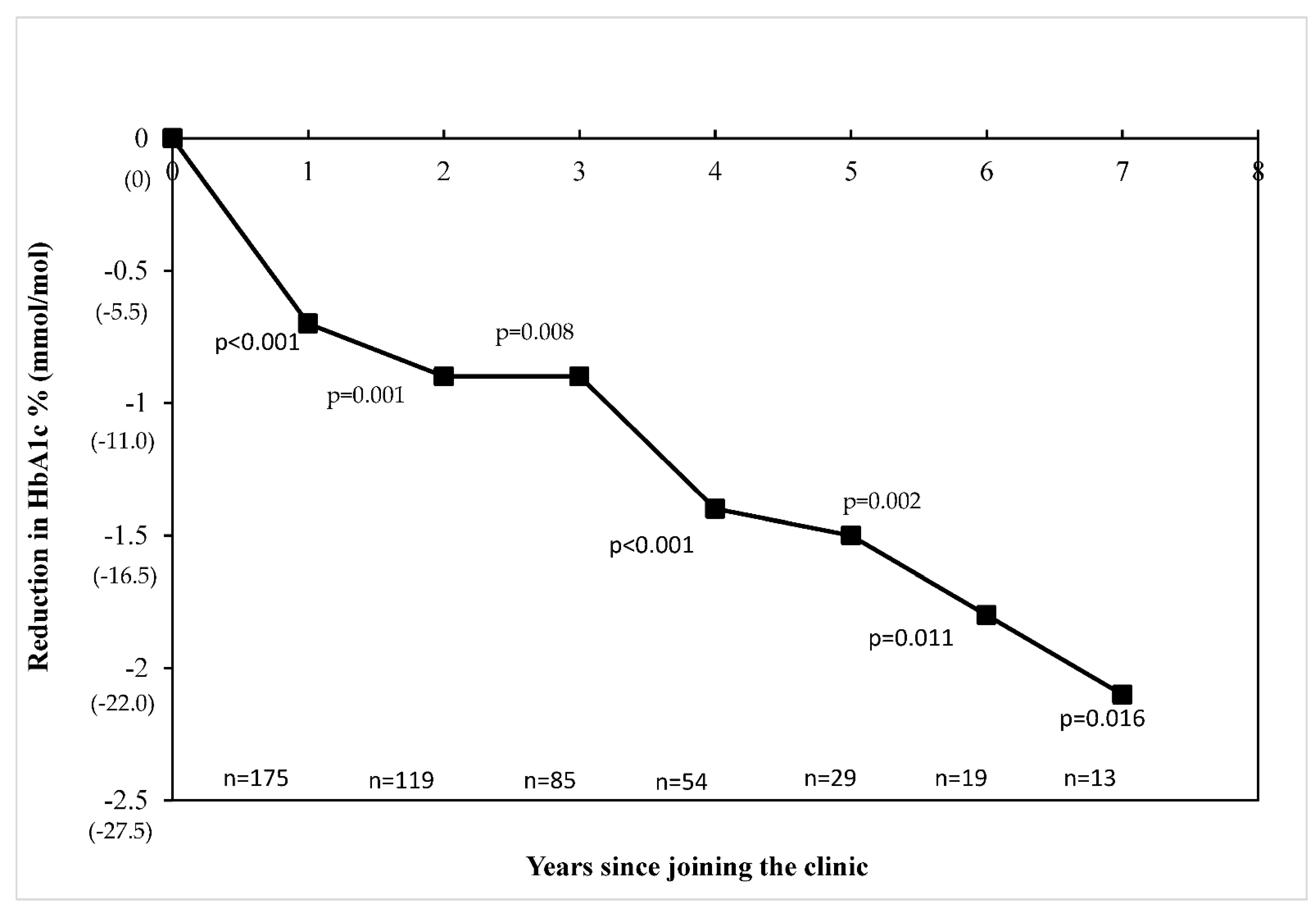
3.3. Glycaemic (HbA1c) Trend in the Clinic before and after Changes in Service Delivery
4. Discussion
Limitations and Strengths
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Conflicts of Interest
References
- Farrell, K.; Griffiths, R.; Fernandez, R. Factors determining diabetes care outcomes in patients with type 1 diabetes after transition from paediatric to adult health care: A systematic review—Protocol. JBI Libr. Syst. Rev. 2009, 7, 1–17. [Google Scholar]
- Peters, A.; Laffel, L. Diabetes care for emerging adults: Recommendations for transition from pediatric to adult diabetes care systems: A position statement of the American Diabetes Association, with representation by the American College of Osteopathic Family Physicians, the American Academy of Pediatrics, the American Association of Clinical Endocrinologists, the American Osteopathic Association, the Centers for Disease Control and Prevention, Children with Diabetes, The Endocrine Society, the International Society for Pediatric and Adolescent Diabetes, Juvenile Diabetes Research Foundation International, the National Diabetes Education Program, and the Pediatric Endocrine Society (formerly Lawson Wilkins Pediatric Endocrine Society). Diabetes Care 2011, 34, 2477–2485. [Google Scholar] [CrossRef] [Green Version]
- Bernstein, C.M.; Stockwell, M.S.; Gallagher, M.P.; Rosenthal, S.L.; Soren, K. Mental health issues in adolescents and young adults with type 1 diabetes: Prevalence and impact on glycemic control. Clin. Pediatr. 2013, 52, 10–15. [Google Scholar] [CrossRef] [PubMed]
- Spaic, T.; Robinson, T.; Goldbloom, E.; Gallego, P.; Hramiak, I.; Lawson, M.; Malcolm, J.; Mahon, J.; Morrison, D.; Parikh, A.; et al. Closing the Gap: Results of the Multicenter Canadian Randomized Controlled Trial of Structured Transition in Young Adults With Type 1 Diabetes. Diabetes Care 2019, 42, 1018–1026. [Google Scholar] [CrossRef] [PubMed]
- Bridgett, M.; Abrahamson, G.; Ho, J. Transition, It’s More Than Just An Event: Supporting Young People With Type 1 Diabetes. J. Pediatr. Nurs. 2015, 30, e11–e14. [Google Scholar] [CrossRef]
- Gupta, A.; Taylor, F.; O’Sullivan, T.; Simmons, D. Characteristics of young adults with multiple episodes of diabetic ketoacidosis. Intern. Med. J. 2019, 49, 911–914. [Google Scholar] [CrossRef]
- Nakhla, M.; Daneman, D.; Frank, M.; Guttmann, A. Translating transition: A critical review of the diabetes literature. J. Pediatr. Endocrinol. Metab. 2008, 21, 507–516. [Google Scholar]
- Goldenring, J.M.; Rosen, D.S. Getting into adolescent heads: An essential update. Contemp. Pediatr. Montvale 2004, 21, 64–92. [Google Scholar]
- Wagner, D.V.; Ulrich, J.; Guttmann-Bauman, I.; Duke, D.C. The process of transition from pediatric to adult diabetes care: Recommendations for US healthcare systems. Diabetes Manag. 2015, 5, 379–391. [Google Scholar] [CrossRef]
- Cadario, F.; Prodam, F.; Bellone, S.; Trada, M.; Binotti, M.; Trada, M.; Allochis, G.; Baldelli, R.; Esposito, S.; Bona, G. Transition process of patients with type 1 diabetes (T1DM) from paediatric to the adult health care service: A hospital-based approach. Clin. Endocrinol. 2009, 71, 346–350. [Google Scholar] [CrossRef]
- Holmes-Walker, D.; Llewellyn, A.; Farrell, K. A transition care programme which improves diabetes control and reduces hospital admission rates in young adults with Type 1 diabetes aged 15–25 years. Diabet. Med. 2007, 24, 764–769. [Google Scholar] [CrossRef]
- Baxter, M.; Hudson, R.; Mahon, J.; Bartlett, C.; Samyshkin, Y.; Alexiou, D.; Hex, N. Estimating the impact of better management of glycaemic control in adults with type 1 and type 2 diabetes on the number of clinical complications and the associated financial benefit. Diabet. Med. 2016, 33, 1575–1581. [Google Scholar] [CrossRef] [PubMed]
- National Diabetes Service Scheme (NDSS). Diabetes Map. Available online: https://map.ndss.com.au/#!/ (accessed on 10 July 2021).
- Census QuickStats: Sydney—South West. 2016. Available online: https://quickstats.censusdata.abs.gov.au/census_services/getproduct/census/2016/quickstat/127?opendocument (accessed on 14 July 2020).
- Schultz, A.T.; Smaldone, A. Components of interventions that improve transitions to adult care for adolescents with type 1 diabetes. J. Adolesc. Health 2017, 60, 133–146. [Google Scholar] [CrossRef]
- Yue, D.K.; Colagiuri, S.; McElduff, A.; Silink, M. Diabetes Control and Complications Trial Position statment of the Australian Diabetes Society. Med. J. Aust. 1993, 159, 803–804. [Google Scholar] [CrossRef] [PubMed]
- ABS. National survey of mental health and wellbeing: Summary of results. In Statistics on Key Mental Health Issues Including the Prevalence of Mental Disorders, the Associated Disability, and the Use of Services; Australian Bureau of Statistics: Canberra, Australia, 2007. [Google Scholar]
- Ducat, L.; Philipson, L.H.; Anderson, B.J. The mental health comorbidities of diabetes. JAMA 2014, 312, 691–692. [Google Scholar] [CrossRef]
- Goodwin, J.; Savage, E.; Horgan, A. Adolescents’ and young Adults’ beliefs about mental health services and care: A systematic review. Arch. Psychiatr. Nurs. 2016, 30, 636–644. [Google Scholar] [CrossRef]
- Penninx, B.W.J.H.; Lange, S.M.M. Metabolic syndrome in psychiatric patients: Overview, mechanisms, and implications. Dialogues Clin. Neurosci. 2018, 20, 63–73. [Google Scholar] [CrossRef] [PubMed]
- Mendelsohn, C.P.; Kirby, D.P.; Castle, D.J. Smoking and mental illness. An update for psychiatrists. Australas. Psychiatry 2015, 23, 37–43. [Google Scholar] [CrossRef] [PubMed]
- Cooper, J.; Mancuso, S.G.; Borland, R.; Slade, T.; Galletly, C.; Castle, D. Tobacco smoking among people living with a psychotic illness: The second Australian Survey of Psychosis. Aust. N. Z. J. Psychiatry 2012, 46, 851–863. [Google Scholar] [CrossRef]
- Williams, J.M.; Steinberg, M.L.; Griffiths, K.G.; Cooperman, N. Smokers with behavioral health comorbidity should be designated a tobacco use disparity group. Am. J. Public Health 2013, 103, 1549–1555. [Google Scholar] [CrossRef]
- Greenhalgh, E.; Stillman, S.; Ford, C. 7.12 Smoking and Mental Health; Cancer Council Victoria: Melbourne, Australia, 2018. [Google Scholar]
- Forman–Hoffman, V.L.; Hedden, S.L.; Glasheen, C.; Davies, C.; Colpe, L.J. The role of mental illness on cigarette dependence and successful quitting in a nationally representative, household-based sample of US adults. Ann. Epidemiol. 2016, 26, 447–454. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shah, V.N.; Taylor, D.D.; Foster, N.C.; Beck, R.O.Y.; Akturk, H.K.; Kinney, G.L. 836-P: Cannabis Use in Adults with Type 1 Diabetes (T1D) Is Associated with Poor Glycemic Control and Increased Risk for Diabetic Ketoacidosis (DKA). Diabetes 2019, 68. [Google Scholar] [CrossRef]
- Ali, K.; Farrer, L.; Gulliver, A.; Griffiths, K.M. Online peer-to-peer support for young people with mental health problems: A systematic review. JMIR Ment. Health 2015, 2, e4418. [Google Scholar] [CrossRef] [PubMed] [Green Version]

{kind=link}
{kind=link}
| Variables | All |
|---|---|
| N (%) | 220 |
| Period | |
| 2012–2016 | 78 (35.5) |
| 2019–2019 | 68 (30.9) |
| 2012–2019 | 74 (33.6) |
| Socio-demography | |
| Current age, mean (SD) | 22.6 (3.1) |
| Age at first assessment, mean (SD) | 18.6 (2.0) |
| Female, n (%) | 92 (44.5) |
| Place of Birth—Australia | 205 (93.2) |
| Aboriginal or Torres Strait Island | 6 (2.7) |
| Smoking, n (%) | 44 (20.0) |
| Alcohol, n (%) | 108 (49.1) |
| Diabetes type | |
| Type 1 diabetes | 184 (83.6) |
| Type 2 diabetes/Other | 36(16.4) |
| Glycaemia, mean (SD) | |
| HbA1c at entry, % (mmol/mol) | 9.9 ± 2.6 (84 ± 29) |
| Mean HbA1c | 9.2 ± 2.0 (77 ± 22) |
| HbA1c at last visit, % (mmol/mol) | 8.9 ± 2.3 (74 ± 25) |
| Reduction in HbA1c since first attendance, %(mmol/mol) | 0.9 ± 2.8 (10.1 ± 29.8) |
| Driving requirement compliance, n (%) | 89 (40.5) |
| Age of diagnosis (years), mean (SD) | 12.2 ± 5.9 |
| Diabetes duration (years), mean (SD) | 9.8 ± 6.3 |
| Number of clinic check ins, mean (SD) | 6.1 ± 5.0 |
| Number of years in clinic, mean (SD) | 2.2 ± 1.7 |
| Variables | All |
|---|---|
| Metabolic outcomes, mean (standard deviation) | |
| Lipids (mmol/L) | |
| Mean total cholesterol | 4.7 ± 1.1 |
| Mean TAGs | 1.8 ± 1.8 |
| Mean HDL | 1.4 ± 0.4 |
| Mean LDL | 2.7 ± 0.8 |
| Blood pressures (mmHg) | |
| Mean of mean sBP | 124 ± 11 |
| Mean of mean dBP | 75 ± 7 |
| BMI (kg/m2) | 28.0 ± 7.7 |
| Treatment, n (%) | |
| Insulin only | 169 (76.8) |
| Insulin and oral/GLP1 | 35 (15.9) |
| Oral/GLP1 only a | 18 (50.0) |
| Complications, n (%) | |
| Neuropathy | 17 (7.7) |
| Nephropathy † | 34 (15.5) |
| Retinopathy | 11 (5.0) |
| Any long-term complication, n (%) | 34 (15.5) |
| Hypertension, n (%) | 77 (35.0) |
| Mental health condition, n (%) | 89 (40.5) |
| DKA †, n (%) | 110 (50.0) |
| Multiple DKA episodes, n (%) | 46 (21.1) |
| Hypoglycaemia admissions, n (%) | 24 (10.9) |
| Multiple hypo episodes, n (%) | 6 (2.8) |
| Any long-term complication, n (%) | 34 (15.5) |
| Hypertension, n (%) | 77 (35.0) |
| Target achieved, n (%) | |
| sBP < 130 mm Hg | 142 (71.4) |
| dBP < 80 mmHg | 148 (74.4) |
| HbA1c ** | 23 (10.7) |
| Total cholesterol < 5.0 mmol/L | 106 (66.7) |
| Total TAGs < 2.0 mmol/L | 122 (76.7) |
| Total HDL > 1.0 mmol/L | 116 (81.7) |
| Total LDL < 2.5 mmol/L | 61 (43.9) |
| Variables | Mental Health Conditions (n = 89) | No Mental Health Conditions (n = 131) | p Value |
|---|---|---|---|
| Current age, mean (± SD) years | 22.8 (2.8) | 22.5 (3.2) | 0.816 |
| Age at first assessment, mean (± SD) years | 18.7 (1.96) | 18.6 (2.0) | 0.816 |
| Gender Male, n (%) Female, n (%) | 45 (50.6) 44 (49.4) | 77 (59.2) 53 (40.8) | 0.205 |
| Type of Diabetes 1, n (%) 2/other, n (%) | 74 (83.1) 15 (16.9) | 109 (83.8) 21 (16.2) | 0.891 |
| Aboriginal or Torres Strait Islander status, n (%) | 5 (5.6) | 1 (0.8) | 0.031 |
| DKA, n (%) | 54 (60.7) | 56 (42.7) | 0.009 |
| Multiple DKA, n (%) | 25 (28.4) | 21 (16.0) | 0.031 |
| Hypoglycaemia admissions, n (%) | 12 (13.5) | 12 (9.2) | 0.313 |
| Multiple hypoglycaemia events, n (%) | 4 (4.5) | 2 (1.5) | 0.185 |
| Neuropathy, n (%) | 8 (9.0) | 9 (6.9) | 0.564 |
| Nephropathy †, n (%) | 6 (6.7) | 4 (3.1) | 0.197 |
| Retinopathy, n (%) | 8 (9.0) | 3 (2.3) | 0.025 |
| Any long-term complication, n (%) | 20 (22.5) | 15 (11.5) | 0.028 |
| Hypertension, n (%) | 32 (36) | 45 (34.6) | 0.838 |
| Smoking, n (%) | 27 (30.3) | 17 (13.1) | 0.005 |
| Alcohol, n (%) | 41 (46.1) | 67 (51.5) | 0.460 |
| Driving requirement compliance, n (%) | 33 (37.1) | 56 (42.1) | 0.071 |
| HbA1c at entry, % (mmol/mol) | 10.2 ± 2.6 (89 ± 29) | 9.6 ± 2.6 (82 ± 29) | 0.083 |
| Last HbA1c, % (mmol/mol) | 9.4 ± 2.4 (79 ± 27) | 8.7 ± 2.2 (71 ± 24) | 0.027 |
| Target HDL, n (%) | 41 (46.1) | 75 (57.3) | 0.046 |
| Age at diagnosis, years | 11.3 ± 5.8 | 12.1 ± 5.9 | 0.060 |
| Diabetes duration, years | 10.7 ± 6.4 | 9.1 ± 6.2 | 0.056 |
| Number of clinic check ins | 5.6 ± 4.0 | 6.6 ± 5.3 | 0.229 |
| Number of years in clinic | 1.8 ± 1.5 | 2.1 ± 2.0 | 0.389 |
| Model 1 | Model 2 | |||||
|---|---|---|---|---|---|---|
| Variables | OR | aOR [95%CI] | p-value | OR | aOR [95%CI] | p-value |
| Gender (1) | 0.185 | 1.20 [0.67, 2.15] | 0.533 | 0.162 | 1.18 [0.66, 2.08] | 0.58 |
| Type of Diabetes (1) | 0.386 | 1.47 [0.56, 3.87] | 0.434 | 0.389 | 1.48 [0.57, 3.82] | 0.423 |
| Age (/year) | −0.011 | 0.99 [0.89, 1.10] | 0.832 | −0.013 | 0.99 [0.89, 1.10] | 0.808 |
| Diabetes Duration (/year) | 0.037 | 1.04 [0.98, 1.10] | 0.194 | 0.032 | 1.03[0.98, 1.09] | 0.249 |
| HbA1c (1) | 0.704 | 2.02 [1.10, 3.70] | 0.023 | - | - | - |
| DKA (1) | 0.592 | 1.81 [0.93, 3.50] | 0.079 | 0.764 | 2.15 [1.13, 4.07] | 0.019 |
| Hypoglycaemia (1) | 0.212 | 1.24 [0.48, 3.19] | 0.662 | 0.131 | 1.14 [0.45, 2.92] | 0.784 |
| Any microvascular complication (1) | 0.487 | 1.63 [0.72, 3.66] | 0.239 | 0.702 | 2.02 [0.92, 4.43] | 0.08 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Sritharan, A.; Osuagwu, U.L.; Ratnaweera, M.; Simmons, D. Eight-Year Retrospective Study of Young Adults in a Diabetes Transition Clinic. Int. J. Environ. Res. Public Health 2021, 18, 12667. https://doi.org/10.3390/ijerph182312667
Sritharan A, Osuagwu UL, Ratnaweera M, Simmons D. Eight-Year Retrospective Study of Young Adults in a Diabetes Transition Clinic. International Journal of Environmental Research and Public Health. 2021; 18(23):12667. https://doi.org/10.3390/ijerph182312667
Chicago/Turabian StyleSritharan, Aarooran, Uchechukwu L. Osuagwu, Manjula Ratnaweera, and David Simmons. 2021. "Eight-Year Retrospective Study of Young Adults in a Diabetes Transition Clinic" International Journal of Environmental Research and Public Health 18, no. 23: 12667. https://doi.org/10.3390/ijerph182312667
APA StyleSritharan, A., Osuagwu, U. L., Ratnaweera, M., & Simmons, D. (2021). Eight-Year Retrospective Study of Young Adults in a Diabetes Transition Clinic. International Journal of Environmental Research and Public Health, 18(23), 12667. https://doi.org/10.3390/ijerph182312667