
Associations of COVID-19 Knowledge and Risk Perception with the Full Adoption of Preventive Behaviors in Seoul


Abstract
:1. Introduction
2. Methods
2.1. Study Design and Participants
2.2. Measures
2.3. Data Analysis
3. Results
3.1. Participants’ General Characteristics and Levels of COVID-19 Knowledge and Risk Perception
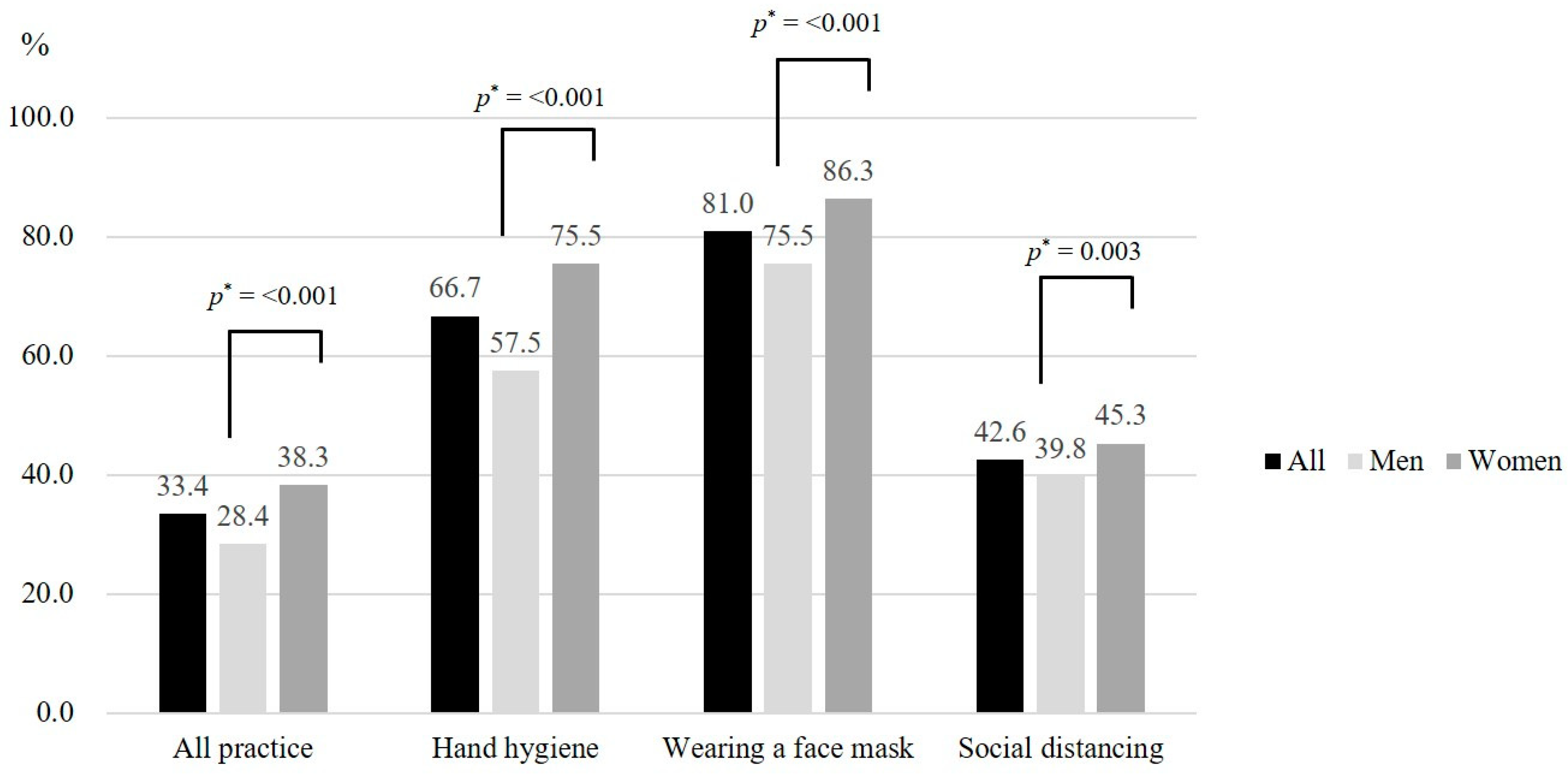
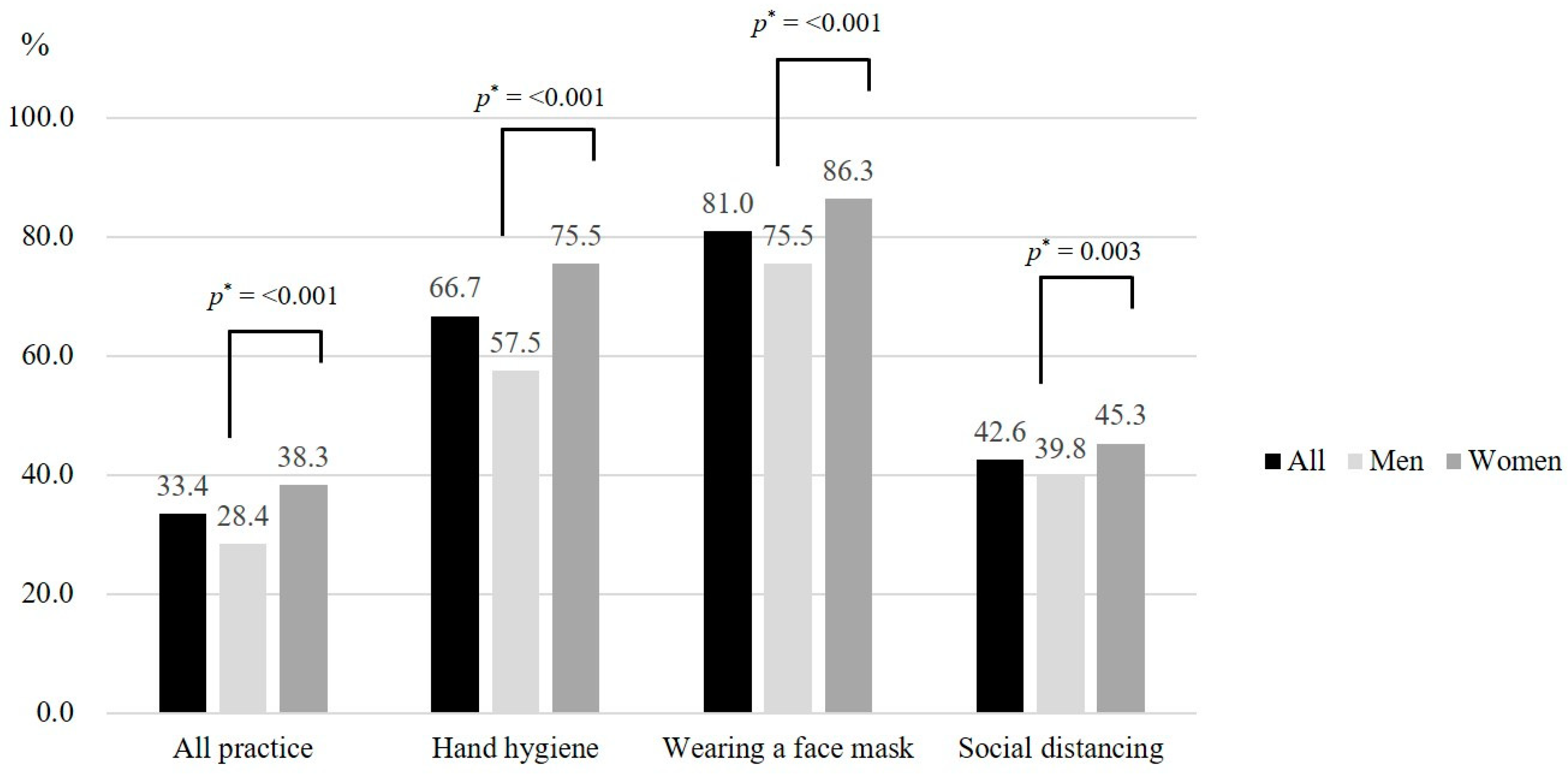
3.2. Full Adoption of Preventive Behaviors against COVID-19
3.3. Factors Associated with COVID-19 Knowledge and Risk Perception
3.4. Associations of the Full Adoption of COVID-19 Preventive Behaviors with General Characteristics, COVID-19 Knowledge, and Risk Perception
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- World Health Organization Statement on the Second Meeting of the International Health Regulations (2005) Emergency Committee Regarding the Outbreak of Novel Coronavirus (2019-nCoV). 2020. Available online: https://www.who.int/news/item/30-01-2020-statement-on-the-second-meeting-of-the-international-health-regulations-(2005)-emergency-committee-regarding-the-outbreak-of-novel-coronavirus-(2019-ncov) (accessed on 1 July 2020).
- World Health Organization Report of the WHO-China Joint Mission on Coronavirus Disease 2019 (COVID-19). 2020. Available online: https://www.who.int/publications/i/item/report-of-the-who-china-joint-mission-on-coronavirus-disease-2019-(covid-19) (accessed on 10 September 2020).
- Dong, E.; Du, H.; Gardner, L. An interactive web-based dashboard to track COVID-19 in real time. J. Lancet Infect. Dis. 2020, 20, 533–534. [Google Scholar] [CrossRef]
- Arslanca, T.; Fidan, C.; Daggez, M.; Dursun, P. Knowledge, preventive behaviors and risk perception of the COVID-19 pandemic: A cross-sectional study in Turkish health care workers. PLoS ONE 2021, 16, e0250017. [Google Scholar] [CrossRef] [PubMed]
- Noreen, Q.; Alexandra, L.; Neha, K.; Narue, W.-J.; Stephanie, D.; Matthew, B.; Carrie, R.; Amra, U. Community Mitigation Guidelines to Prevent Pandemic Influenza—United States, 2017; 66(No. RR-1); Centers for Disease Control and Prevention: Atlanta, GA, USA, 2017; pp. 1–34.
- Perra, N. Non-pharmaceutical interventions during the COVID-19 pandemic: A review. Phys. Rep. 2021, 913, 1–52. [Google Scholar] [CrossRef]
- Ferguson, N.; Laydon, D.; Nedjati Gilani, G.; Imai, N.; Ainslie, K.; Baguelin, M.; Bhatia, S.; Boonyasiri, A.; Perez, Z.C.; Cuomo-Dannenburg, G. Report 9: Impact of Non-Pharmaceutical Interventions (NPIs) to Reduce COVID19 Mortality and Healthcare Demand. Imperial College: London, UK, 2020. [Google Scholar]
- Shaw, R.; Kim, Y.-k.; Hua, J. Governance, technology and citizen behavior in pandemic: Lessons from COVID-19 in East Asia. Prog. Disaster Sci. 2020, 6, 100090. [Google Scholar] [CrossRef]
- Bults, M.; Beaujean, D.J.; de Zwart, O.; Kok, G.; van Empelen, P.; van Steenbergen, J.E.; Richardus, J.H.; Voeten, H.A. Perceived risk, anxiety, and behavioural responses of the general public during the early phase of the Influenza A (H1N1) pandemic in the Netherlands: Results of three consecutive online surveys. BMC Public Health 2011, 11, 1–13. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Choi, J.-S.; Kim, J.-S. Factors influencing preventive behavior against Middle East Respiratory Syndrome-Coronavirus among nursing students in South Korea. Nurse Educ. Today 2016, 40, 168–172. [Google Scholar] [CrossRef]
- Commodari, E.; La Rosa, V.L.; Coniglio, M.A. Health risk perceptions in the era of the new coronavirus: Are the Italian people ready for a novel virus? A cross-sectional study on perceived personal and comparative susceptibility for infectious diseases. Public Health 2020, 187, 8–14. [Google Scholar] [CrossRef] [PubMed]
- Azlan, A.A.; Hamzah, M.R.; Sern, T.J.; Ayub, S.H.; Mohamad, E. Public knowledge, attitudes and practices towards COVID-19: A cross-sectional study in Malaysia. PLoS ONE 2020, 15, e0233668. [Google Scholar] [CrossRef]
- Kim, J.S.; Choi, J.S. Middle East respiratory syndrome–related knowledge, preventive behaviours and risk perception among nursing students during outbreak. J. Clin. Nurs. 2016, 25, 2542–2549. [Google Scholar] [CrossRef]
- Brug, J.; Aro, A.R.; Oenema, A.; De Zwart, O.; Richardus, J.H.; Bishop, G.D. SARS risk perception, knowledge, precautions, and information sources, the Netherlands. Emerg. Infect. Dis. 2004, 10, 1486. [Google Scholar] [CrossRef]
- Hussain, Z.A.; Hussain, S.A.; Hussain, F.A. Medical students’ knowledge, perceptions, and behavioral intentions towards the H1N1 influenza, swine flu, in Pakistan: A brief report. Am. J. Infect. Control. 2012, 40, e11–e13. [Google Scholar] [CrossRef] [PubMed]
- Alsoghair, M.; Almazyad, M.; Alburaykan, T.; Alsultan, A.; Alnughaymishi, A.; Almazyad, S.; Alharbi, M.; Alkassas, W.; Almadud, A.; Alsuhaibani, M. Medical Students and COVID-19: Knowledge, Preventive Behaviors, and Risk Perception. Int. J. Environ. Res. Public Health 2021, 18, 842. [Google Scholar] [CrossRef]
- Elhadi, M.; Msherghi, A.; Alsoufi, A.; Buzreg, A.; Bouhuwaish, A.; Khaled, A.; Alhadi, A.; Alameen, H.; Biala, M.; Elgherwi, A.; et al. Knowledge, preventive behavior and risk perception regarding COVID-19: A self-reported study on college students. Pan. Afr. Med. J. 2020, 35, 75. [Google Scholar] [CrossRef]
- Ibuka, Y.; Chapman, G.B.; Meyers, L.A.; Li, M.; Galvani, A.P. The dynamics of risk perceptions and precautionary behavior in response to 2009 (H1N1) pandemic influenza. BMC Infect. Dis. 2010, 10, 1–11. [Google Scholar] [CrossRef] [Green Version]
- Duan, T.; Jiang, H.; Deng, X.; Zhang, Q.; Wang, F. Government intervention, risk perception, and the adoption of protective action recommendations: Evidence from the COVID-19 prevention and control experience of China. Int. J. Environ. Res. Public Health 2020, 17, 3387. [Google Scholar] [CrossRef]
- Dryhurst, S.; Schneider, C.R.; Kerr, J.; Freeman, A.L.; Recchia, G.; Van Der Bles, A.M.; Spiegelhalter, D.; Van Der Linden, S. Risk perceptions of COVID-19 around the world. J. Risk Res. 2020, 23, 994–1006. [Google Scholar] [CrossRef]
- Roy, D.; Tripathy, S.; Kar, S.K.; Sharma, N.; Verma, S.K.; Kaushal, V. Study of knowledge, attitude, anxiety & perceived mental healthcare need in Indian population during COVID-19 pandemic. Asian J. Psychiatr. 2020, 51, 102083. [Google Scholar] [CrossRef]
- Kim, S.; Castro, M.C. Spatiotemporal pattern of COVID-19 and government response in South Korea (as of May 31, 2020). Int. J. Infect. Dis. 2020, 98, 328–333. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization Strengthening Preparedness for COVID-19 in Cities and Urban Settings: Interim Guidance for Local Authorities. 2020. Available online: https://www.who.int/publications/i/item/strengthening-preparedness-for-covid-19-in-cities-and-urban-settings (accessed on 15 September 2020).
- Kim, J.; You, M.; Shon, C. Impact of the COVID-19 pandemic on unmet healthcare needs in Seoul, South Korea: A cross-sectional study. BMJ Open 2021, 11, e045845. [Google Scholar] [CrossRef]
- Seoul Metropolitan Government Social Distancing Campaign: A Pause! 2021. Available online: https://news.seoul.go.kr/welfare/archives/514931 (accessed on 16 September 2021).
- Cuello-Garcia, C.; Pérez-Gaxiola, G.; van Amelsvoort, L. Social media can have an impact on how we manage and investigate the COVID-19 pandemic. J. Clin. Epidemiol. 2020, 127, 198. [Google Scholar] [CrossRef] [PubMed]
- Ning, L.; Niu, J.; Bi, X.; Yang, C.; Liu, Z.; Wu, Q.; Ning, N.; Liang, L.; Liu, A.; Hao, Y. The impacts of knowledge, risk perception, emotion and information on citizens’ protective behaviors during the outbreak of COVID-19: A cross-sectional study in China. BMC Public Health 2020, 20, 1–12. [Google Scholar] [CrossRef] [PubMed]
- Rattay, P.; Michalski, N.; Domanska, O.M.; Kaltwasser, A.; De Bock, F.; Wieler, L.H.; Jordan, S. Differences in risk perception, knowledge and protective behaviour regarding COVID-19 by education level among women and men in Germany. Results from the COVID-19 Snapshot Monitoring (COSMO) study. PLoS ONE 2021, 16, e0251694. [Google Scholar] [CrossRef]
- Expert Group on Health Promotion for the Seoul Metropolitan Government. Executive Summary Report: Person-Centered and Customized Information Campaign for Seoul Citizens—On A Basis of A Survey on the Knowledge and Risk Perception of Seoul Citizens for a Campaign to Practice COVID-19 Preventive Actions; Seoul Metropolitan Govenment and Expert Group on Health Promotion for the Seoul Metropolitan Government: Seoul, Korea, 2021.
- Seoul Metropolitan Government COVID-19 Dashboard: Trend of COVID-19 Occurence. 2020. Available online: https://www.seoul.go.kr/coronaV/coronaStatus.do (accessed on 3 November 2020).
- Ministry of Health and Welfare Criteria Median Income and Livelihood/Medical Benefit Selection Criteria and Minimum Level of Coverage. 2021. Available online: http://www.mohw.go.kr/upload/viewer/skin/doc.html?fn=1596776679207_20200807140439.hwp&rs=/upload/viewer/result/202109/ (accessed on 1 July 2021).
- Taghrir, M.H.; Borazjani, R.; Shiraly, R. COVID-19 and Iranian medical students; A survey on their related-knowledge, preventive behaviors and risk perception. Arch. Iran. Med. 2020, 23, 249–254. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hwang, Y.; Jeong, S.H. Misinformation Exposure and Acceptance: The Role of Information Seeking and Processing. Health Commun. 2021, 11, 1–9. [Google Scholar] [CrossRef]
- Tomczyk, S.; Rahn, M.; Schmidt, S. Social distancing and stigma: Association between compliance with behavioral recommendations, risk perception, and stigmatizing attitudes during the COVID-19 outbreak. Front. Psychol. 2020, 11, 1821. [Google Scholar] [CrossRef] [PubMed]
- Abdelhafiz, A.S.; Mohammed, Z.; Ibrahim, M.E.; Ziady, H.H.; Alorabi, M.; Ayyad, M.; Sultan, E.A. Knowledge, perceptions, and attitude of Egyptians towards the novel coronavirus disease (COVID-19). J. Community Health 2020, 45, 881–890. [Google Scholar] [CrossRef]
- Hussain, A.; Garima, T.; Singh, B.M.; Ram, R.; Tripti, R.P. Knowledge, attitudes, and practices towards COVID-19 among Nepalese Residents: A quick online cross-sectional survey. Asian J. Med. Sci. 2020, 11, 6–11. [Google Scholar] [CrossRef]
- Haque, T.; Hossain, K.M.; Bhuiyan, M.M.R.; Ananna, S.A.; Chowdhury, S.H.; Islam, M.R.; Ahmed, A.; Rahman, M.M. Knowledge, attitude and practices (KAP) towards COVID-19 and assessment of risks of infection by SARS-CoV-2 among the Bangladeshi population: An online cross sectional survey. PLoS ONE 2020, 15, e0239254. [Google Scholar] [CrossRef]
- Seoul Metropolitan Government and The Seoul Institute Seoul at A Glance 2015. 2016. Available online: https://opengov.seoul.go.kr/analysis/8461972 (accessed on 30 September 2016).
- Lee, J.; Kim, K.; Park, G.; Cha, N. The role of online news and social media in preventive action in times of infodemic from a social capital perspective: The case of the COVID-19 pandemic in South Korea. Telemat. Inf. 2021, 64, 101691. [Google Scholar] [CrossRef]
- Levkovich, I.; Shinan-Altman, S. The impact of gender on emotional reactions, perceived susceptibility and perceived knowledge about COVID-19 among the Israeli public. Int. Health 2021, 15, ihaa 101. [Google Scholar] [CrossRef]
- Gao, H.; Hu, R.; Yin, L.; Yuan, X.; Tang, H.; Luo, L.; Chen, M.; Huang, D.; Wang, Y.; Yu, A. Knowledge, attitudes and practices of the Chinese public with respect to coronavirus disease (COVID-19): An online cross-sectional survey. BMC Public Health 2020, 20, 1–8. [Google Scholar] [CrossRef]
- Geldsetzer, P. Knowledge and perceptions of COVID-19 among the general public in the United States and the United Kingdom: A cross-sectional online survey. Ann. Intern. Med. 2020, 173, 157–160. [Google Scholar] [CrossRef] [Green Version]
- Central Disaster and Safety Countermeasures Headquarters Updates on COVID-19 in Republic of Korea 2020. 2020. Available online: http://ncov.mohw.go.kr/tcmBoardView.do?brdId=&brdGubun=&dataGubun=&ncvContSeq=360241&contSeq=360241&board_id=&gubun=ALL (accessed on 17 October 2020).
- Seoul Metropolitan Government Social Distancing Phase 1, What Is the Change of Quarantine Rule in Seoul? 2020. Available online: https://mediahub.seoul.go.kr/archives/1302547 (accessed on 16 October 2020).
- Chan, E.Y.Y.; Huang, Z.; Lo, E.S.K.; Hung, K.K.C.; Wong, E.L.Y.; Wong, S.Y.S. Sociodemographic Predictors of Health Risk Perception, Attitude and Behavior Practices Associated with Health-Emergency Disaster Risk Management for Biological Hazards: The Case of COVID-19 Pandemic in Hong Kong, SAR China. Int. J. Environ. Res. Public Health 2020, 17, 3869. [Google Scholar] [CrossRef]
- Lv, G.; Yuan, J.; Hsieh, S.; Shao, R.; Li, M. Knowledge and Determinants of Behavioral Responses to the Pandemic of COVID-19. Front. Med. 2021, 8, 673187. [Google Scholar] [CrossRef]
- Chua, C.E.; Kew, G.S.; Demutska, A.; Quek, S.; Loo, E.X.L.; Gui, H.; Wong, S.; Lau, H.X.; Low, E.X.S.; Loh, T.L. Factors associated with high compliance behaviour against COVID-19 in the early phase of pandemic: A cross-sectional study in 12 Asian countries. BMJ Open 2021, 11, e046310. [Google Scholar] [CrossRef]
- Kim, Y.; Yoon, T.; Son, A. Effects of COVID-19 knowledge, risk perception, subjective norms, and perceived behavioral control on preventive action intentions and preventive action practices in college students. J. Korean Soc. Health Educ. Promot. 2021, 38, 25–36. [Google Scholar] [CrossRef]
- Marschalko, E.E.; Kotta, I.; Kalcza-Janosi, K.; Szabo, K.; Jancso-Farcas, S. Psychological predictors of COVID-19 prevention behavior in Hungarian women across different generations. Front. Psychol. 2021, 12, 10. [Google Scholar] [CrossRef] [PubMed]
- Qutob, N.; Awartani, F. Knowledge, attitudes and practices (KAP) towards COVID-19 among Palestinians during the COVID-19 outbreak: A cross-sectional survey. PLoS ONE 2021, 16, e0244925. [Google Scholar] [CrossRef]
- Rana, I.A.; Bhatti, S.S.; Aslam, A.B.; Jamshed, A.; Ahmad, J.; Shah, A.A. COVID-19 risk perception and coping mechanisms: Does gender make a difference? Int. J. Disaster Risk Reduct. IJDRR 2021, 55, 102096. [Google Scholar] [CrossRef] [PubMed]
- Shahnazi, H.; Ahmadi-Livani, M.; Pahlavanzadeh, B.; Rajabi, A.; Hamrah, M.S.; Charkazi, A. Assessing preventive health behaviors from COVID-19: A cross sectional study with health belief model in Golestan Province, Northern of Iran. Infect. Dis. Poverty 2020, 9, 1–9. [Google Scholar] [CrossRef]
- Al-Hanawi, M.K.; Angawi, K.; Alshareef, N.; Qattan, A.; Helmy, H.Z.; Abudawood, Y.; Alqurashi, M.; Kattan, W.M.; Kadasah, N.A.; Chirwa, G.C. Knowledge, attitude and practice toward COVID-19 among the public in the Kingdom of Saudi Arabia: A cross-sectional study. Front. Public Health 2020, 8, 217. [Google Scholar] [CrossRef] [PubMed]
- Siu, J.Y. Qualitative study on the shifting sociocultural meanings of the facemask in Hong Kong since the severe acute respiratory syndrome (SARS) outbreak: Implications for infection control in the post-SARS era. Int. J. Equity Health 2016, 15, 1–16. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Feng, S.; Shen, C.; Xia, N.; Song, W.; Fan, M.; Cowling, B.J. Rational use of face masks in the COVID-19 pandemic. Lancet Respir. Med. 2020, 8, 434–436. [Google Scholar] [CrossRef]
- Xie, K.; Liang, B.; Dulebenets, M.A.; Mei, Y. The impact of risk perception on social distancing during the COVID-19 pandemic in China. Int. J. Environ. Res. Public Health 2020, 17, 6256. [Google Scholar] [CrossRef]
- Schneider, C.R.; Dryhurst, S.; Kerr, J.; Freeman, A.L.J.; Recchia, G.; Spiegelhalter, D.; van der Linden, S. COVID-19 risk perception: A longitudinal analysis of its predictors and associations with health protective behaviours in the United Kingdom. J. Risk Res. 2021, 24, 294–313. [Google Scholar] [CrossRef]
- Chen, Y.; Feng, J.; Chen, A.; Lee, J.E.; An, L. Risk perception of COVID-19: A comparative analysis of China and South Korea. Int. J. Disaster Risk Reduct. IJDRR 2021, 61, 102373. [Google Scholar] [CrossRef]
- Man, S.S.; Chan, A.H.S.; Alabdulkarim, S. Quantification of risk perception: Development and validation of the construction worker risk perception (CoWoRP) scale. J. Saf. Res. 2019, 71, 25–39. [Google Scholar] [CrossRef]

{kind=link}
| Variables | n (%) or Mean (SD) | p | |||
|---|---|---|---|---|---|
| n | All | Men (n = 1463) | Women (n = 1537) | ||
| Age, years | 3000 | 43.6 (14.0) | 43.5 (14.1) | 43.7 (13.92) | 0.779 a |
| 19–29 | 640 (21.3) | 310 (21.2) | 330 (21.5) | 0.802 a | |
| 30–49 | 1229 (41.0) | 611 (41.8) | 618 (40.2) | ||
| 50–64 | 914 (30.5) | 441 (30.1) | 473 (30.8) | ||
| ≥65 | 217 (7.2) | 101 (6.9) | 116 (7.5) | ||
| Education | 3000 | 0.008 a | |||
| >College | 2512 (83.7) | 1138 (77.8) | 1132 (73.6) | ||
| ≤High school | 488 (16.3) | 325 (22.2) | 405 (26.4) | ||
| Household income, won | 2939 | 0.083 a | |||
| >5,000,000 | 1360 (46.3) | 858 (58.6) | 949 (61.7) | ||
| ≤5,000,000 | 1579 (53.7) | 605 (41.4) | 588 (38.3) | ||
| Employed | 2931 | <0.001 a | |||
| Yes | 2118 (72.3) | 1151 (78.7) | 967 (62.9) | ||
| No | 813 (27.7) | 312 (21.3) | 570 (37.1) | ||
| Knowledge (0–100) d | 3000 | 84.6 (13.52) | 84.0 (14.517) | 85.1 (12.48) | 0.444 b |
| Low | 66.4 (11.77) | 64.8 (13.12) | 68.0 (10.04) | ||
| Middle | 85.8 (2.90) | 85.8 (2.90) | 85.8 (2.90) | ||
| High | 96.3 (2.84) | 96.3 (2.84) | 96.3 (2.85) | ||
| Risk perception (1–7) d | 3000 | 4.24 (0.82) | 4.21 (0.83) | 4.26 (0.81) | 0.079 c |
| Low | 3.90 (3.36) | 3.90 (3.33) | 3.90 (3.40) | ||
| Middle | 4.60 (4.24) | 4.60 (4.24) | 4.60 (4.25) | ||
| High | 7.00 (5.14) | 6.67 (5.14) | 7.00 (5.15) | ||
| Variables | OR (95% CI) a | ||
|---|---|---|---|
| High COVID-19 Knowledge | High COVID-19 Risk Perception | ||
| Model 1 | Model 2 | ||
| Age | 1.01 (1.000–1.011) | 0.99 (0.980–0.990) | 0.99 (0.980–0.990) |
| Women | 1.02 (0.873–1.188) | 1.08 (0.926–1.251) | 1.08 (0.925–1.249) |
| College-educated | 1.43 (1.143–1.779) | 0.81 (0.658–0.989) | 0.80 (0.650–0.989) |
| Employed | 1.10 (0.918–1.305) | 1.18 (0.992–1.395) | 1.18 (0.992–1.394) |
| Household income > 5,000,000 won | 1.18 (1.012–1.376) | 1.01 (0.869–1.173) | 1.00 (0.862–1.166) |
| COVID-19 knowledge | |||
| Low | - | - | ref. |
| Middle | - | - | 1.10 (0.912–1.335) |
| High | - | - | 1.13 (0.937–1.365) |
| Variables | OR (95% CI) | |||
|---|---|---|---|---|
| Full Adoption of Preventive Behaviors | ||||
| All Three Behaviors | Hand Hygiene | Face Mask Wearing | Social Distancing | |
| General characteristics | ||||
| Age | 1.01 (1.007–1.019) | 1.00 (0.991–1.003) | 0.99 (0.986–1.000) | 1.01 (1.009–1.020) |
| Women | 1.52 (1.295–1.789) | 2.29 (1.942–2.690) | 1.94 (1.591–2.354) | 1.20 (1.031–1.401) |
| College-educated | 0.95 (0.767–1.189) | 1.03 (0.823–1.292) | 0.77 (0.582–1.026) | 0.86 (0.693–1.056) |
| Employed | 0.79 (0.659–0.942) | 0.89 (0.737–1.071) | 0.74 (0.590–0.941) | 0.78 (0.658–0.929) |
| Household income > 5,000,000 won | 0.96 (0.819–1.130) | 1.01 (0.854–1.183) | 0.96 (0.788–1.161) | 0.91 (0.784–1.067) |
| COVID-19 knowledge | ||||
| Low | ref. | ref. | ref. | ref. |
| Middle | 1.07 (0.868–1.314) | 1.32 (1.082–1.619) | 1.39 (1.101–1.759) | 0.96 (0.789–1.166) |
| High | 1.32 (1.082–1.621) | 1.47 (1.201–1.793) | 1.65 (1.302–2.089) | 1.21 (0.998–1.466) |
| COVID-19 risk perception | ||||
| Low | ref. | ref. | ref. | ref. |
| Middle | 0.94 (0.776–1.145) | 1.01 (0.837–1.228) | 1.00 (0.798–1.258) | 0.97 (0.804–1.162) |
| High | 1.35 (1.111–1.638) | 1.17 (0.956–1.421) | 1.09 (0.858–1.375) | 1.50 (1.247–1.810) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Choo, J.; Park, S.; Noh, S. Associations of COVID-19 Knowledge and Risk Perception with the Full Adoption of Preventive Behaviors in Seoul. Int. J. Environ. Res. Public Health 2021, 18, 12102. https://doi.org/10.3390/ijerph182212102
Choo J, Park S, Noh S. Associations of COVID-19 Knowledge and Risk Perception with the Full Adoption of Preventive Behaviors in Seoul. International Journal of Environmental Research and Public Health. 2021; 18(22):12102. https://doi.org/10.3390/ijerph182212102
Chicago/Turabian StyleChoo, Jina, Sooyeon Park, and Songwhi Noh. 2021. "Associations of COVID-19 Knowledge and Risk Perception with the Full Adoption of Preventive Behaviors in Seoul" International Journal of Environmental Research and Public Health 18, no. 22: 12102. https://doi.org/10.3390/ijerph182212102
APA StyleChoo, J., Park, S., & Noh, S. (2021). Associations of COVID-19 Knowledge and Risk Perception with the Full Adoption of Preventive Behaviors in Seoul. International Journal of Environmental Research and Public Health, 18(22), 12102. https://doi.org/10.3390/ijerph182212102