
Effect of an Unsupervised Exercises-Based Athletics Injury Prevention Programme on Injury Complaints Leading to Participation Restriction in Athletics: A Cluster-Randomised Controlled Trial

 ,
, 
Abstract
:1. Introduction
2. Methods
2.1. Study Design and Overall Procedure
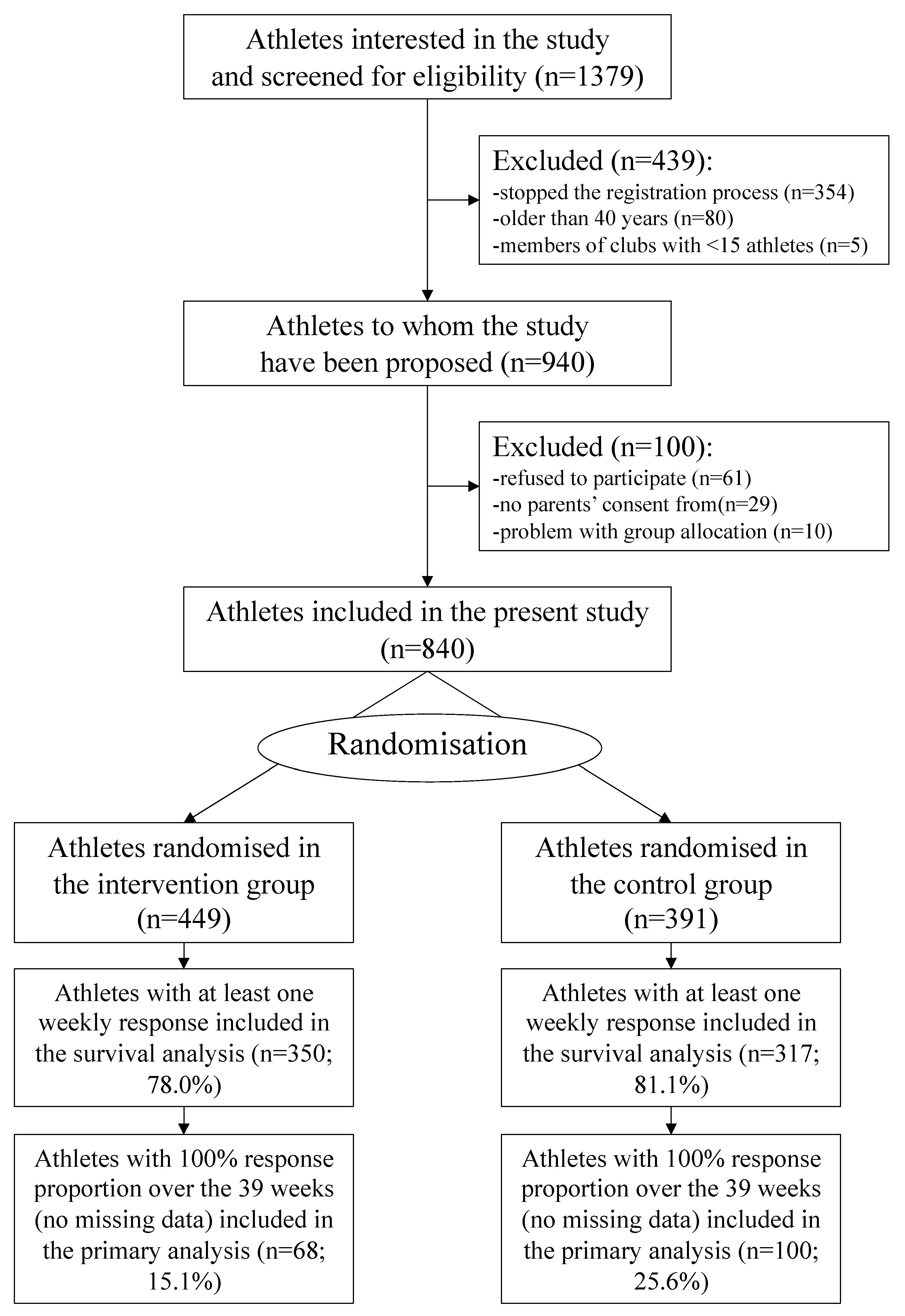
2.2. Population Recruitment and Inclusion/Exclusion Criteria
2.3. Randomisation
2.4. Interventions
2.5. Data Collection
2.6. Injury Definition
2.7. Compliance
2.8. Blinding
2.9. Sample Size
2.10. Study Outcomes
2.11. Statistical Methods
2.12. Deviations from the Protocol
3. Results
3.1. Population
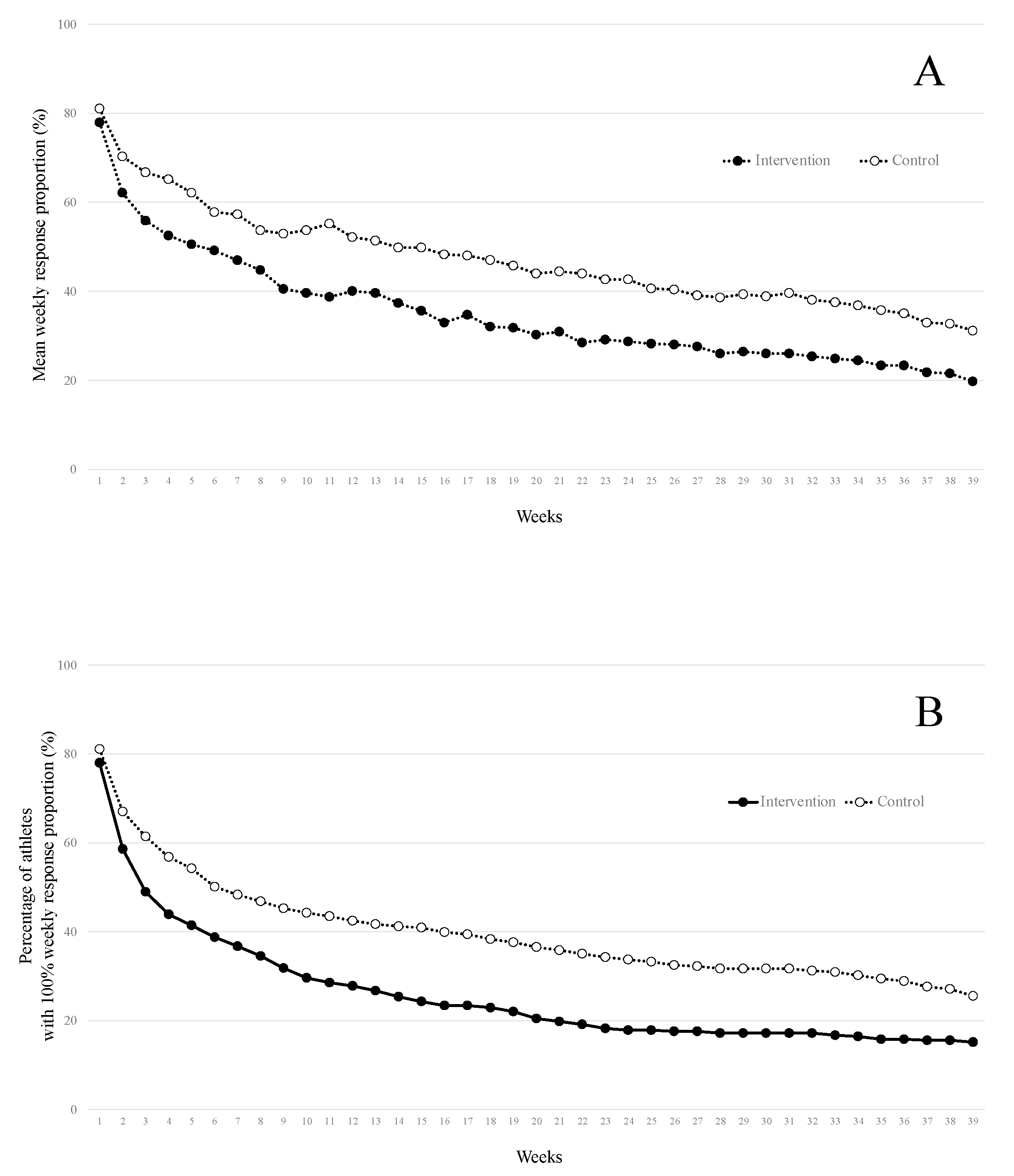
3.2. Response Proportions to the Weekly Questionnaire
3.3. Compliance with the AIPP and Adverse Effects
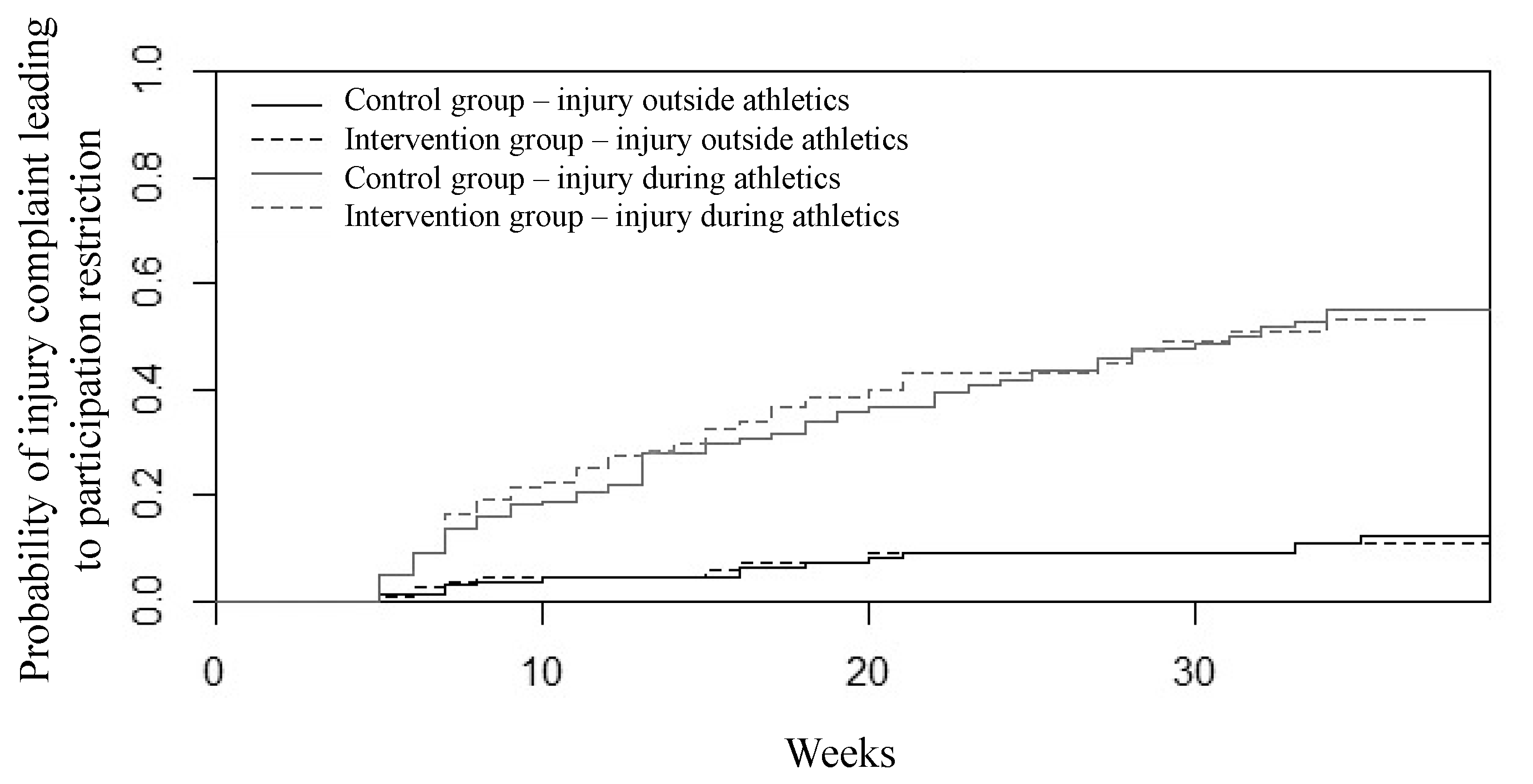
3.4. Primary Outcome Results
3.5. Secondary Outcome Results
4. Discussion
4.1. Challenge of Low Response Proportion to the Weekly Questionnaire
4.2. Challenge of Compliance with the Intervention
4.3. The Athletics Injury Prevention Programme
4.4. Strengths and Limitations
4.5. Practical Implications
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed consent statement
Data availability statement
Acknowledgments
Conflicts of Interest
References
- Edouard, P.; Alonso, J.M.; Jacobsson, J.; Depiesse, F.; Branco, P.; Timpka, T. Injury Prevention in Athletics: The Race Has Started and We Are on Track! New Stud. Athl. 2015, 30, 69–78. [Google Scholar]
- Jacobsson, J.; Timpka, T.; Kowalski, J.; Nilsson, S.; Ekberg, J.; Dahlström, Ö.; Renström, P.A. Injury patterns in Swedish elite athletics: Annual incidence, injury types and risk factors. Br. J. Sports Med. 2013, 47, 941–952. [Google Scholar] [CrossRef]
- Martínez-Silván, D.; Wik, E.H.; Alonso, J.M.; Jeanguyot, E.; Salcinovic, B.; Johnson, A.; Cardinale, M. Injury characteristics in male youth athletics: A five-season prospective study in a full-time sports academy. Br. J. Sports Med. 2020, 55, 954–960. [Google Scholar] [CrossRef] [PubMed]
- D’Souza, D. Track and field athletics injuries-a one-year survey. Br. J. Sports Med. 1994, 28, 197–202. [Google Scholar] [CrossRef] [Green Version]
- Bennell, K.L.; Crossley, K. Musculoskeletal injuries in track and field: Incidence, distribution and risk factors. Aust. J. Sci. Med. Sport 1996, 28, 69–75. [Google Scholar] [PubMed]
- Edouard, P.; Navarro, L.; Branco, P.; Gremeaux, V.; Timpka, T.; Junge, A. Injury frequency and characteristics (location, type, cause and severity) differed significantly among athletics (’track and field’) disciplines during 14 international championships (2007–2018): Implications for medical service planning. Br. J. Sports Med. 2020, 54, 159–167. [Google Scholar] [CrossRef] [PubMed]
- Raysmith, B.; Drew, M.K. Performance success or failure is influenced by weeks lost to injury and illness in elite Australian Track and Field athletes: A 5-year prospective study. J. Sci. Med. Sport 2016, 19, 778–783. [Google Scholar] [CrossRef] [PubMed]
- Edouard, P.; Navarro, L.; Pruvost, J.; Branco, P.; Junge, A. In-competition injuries and performance success in combined events during major international athletics championships. J. Sci. Med. Sport 2021, 24, 152–158. [Google Scholar] [CrossRef]
- Huxley, D.J.; O’Connor, D.; Healey, P.A. An examination of the training profiles and injuries in elite youth track and field athletes. Eur. J. Sport Sci. 2014, 14, 185–192. [Google Scholar] [CrossRef]
- Edouard, P.; Cugy, E.; Dolin, R.; Morel, N.; Serra, J.-M.; Depiesse, F.; Branco, P.; Steffen, K. The Athletics Injury Prevention Programme Can Help to Reduce the Occurrence at Short Term of Participation Restriction Injury Complaints in Athletics: A Prospective Cohort Study. Sports 2020, 8, 84. [Google Scholar] [CrossRef]
- Bahr, R.; Clarsen, B.; Derman, W.; Dvorak, J.; A Emery, C.; Finch, C.F.; Hägglund, M.; Junge, A.; Kemp, S.; Khan, K.M.; et al. International Olympic Committee consensus statement: Methods for recording and reporting of epidemiological data on injury and illness in sport 2020 (including STROBE Extension for Sport Injury and Illness Surveillance (STROBE-SIIS)). Br. J. Sports Med. 2020, 54, 372–389. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Campbell, M.K.; Piaggio, G.; Elbourne, D.R.; Altman, D.G. Consort 2010 statement: Extension to cluster. BMJ 2012, 345, e5661. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Alonso, J.M.; Jacobsson, J.; Timpka, T.; Ronsen, O.; Kajenienne, A.; Dahlström, Ö.; Spreco, A.; Edouard, P. Preparticipation injury complaint is a risk factor for injury: A prospective study of the Moscow 2013 IAAF Championships. Br. J. Sports Med. 2015, 49, 1118–1124. [Google Scholar] [CrossRef] [Green Version]
- Timpka, T.; Alonso, J.-M.; Jacobsson, J.; Junge, A.; Branco, P.; Clarsen, B.; Kowalski, J.; Mountjoy, M.; Nilsson, S.; Pluim, B.; et al. Injury and illness definitions and data collection procedures for use in epidemiological studies in Athletics (track and field): Consensus statement. Br. J. Sports Med. 2014, 48, 483–490. [Google Scholar] [CrossRef] [Green Version]
- Clarsen, B.; Rønsen, O.; Myklebust, G.; Flørenes, T.W.; Bahr, R. The Oslo Sports Trauma Research Center questionnaire on health problems: A new approach to prospective monitoring of illness and injury in elite athletes. Br. J. Sports Med. 2014, 48, 754–760. [Google Scholar] [CrossRef] [Green Version]
- Edouard, P.; Jacobsson, J.; Timpka, T.; Alonso, J.-M.; Kowalski, J.; Nilsson, S.; Karlsson, D.; Depiesse, F.; Branco, P. Extending in-competition Athletics injury and illness surveillance with pre-participation risk factor screening: A pilot study. Phys. Ther. Sport 2015, 16, 98–106. [Google Scholar] [CrossRef]
- Hosmer, D.W.; Lemeshow, S. Model-Building Strategies and Methods for Logistic Regression. In Applied Logistic Regression; John Wiley & Sons: Hoboken, NJ, USA, 2000; pp. 91–142. [Google Scholar] [CrossRef]
- Scrucca, L.; Santucci, A.; Aversa, F. Competing risk analysis using R: An easy guide for clinicians. Bone Marrow Transplant. 2007, 40, 381–387. [Google Scholar] [CrossRef] [Green Version]
- Clarsen, B.; Steffen, K.; Berge, H.M.; Bendiksen, F.; Fossan, B.; Fredriksen, H.; Gjelsvik, H.; Haugvad, L.; Kjelsberg, M.; Ronsen, O.; et al. Methods, challenges and benefits of a health monitoring programme for Norwegian Olympic and Paralympic athletes: The road from London 2012 to Tokyo 2020. Br. J. Sports Med 2021. [Google Scholar] [CrossRef]
- Dalen-Lorentsen, T.; Bjørneboe, J.; Clarsen, B.; Vagle, M.; Fagerland, M.W.; Andersen, T.E. Does load management using the acute:chronic workload ratio prevent health problems? A cluster randomised trial of 482 elite youth footballers of both sexes. Br. J. Sports Med. 2021, 55, 108–114. [Google Scholar] [CrossRef]
- Barboza, S.D.; Bolling, C.S.; Nauta, J.; Van Mechelen, W.; Verhagen, E. Acceptability and perceptions of end-users towards an online sports-health surveillance system. BMJ Open Sport Exerc. Med. 2017, 3, 1–8. [Google Scholar] [CrossRef] [Green Version]
- Pas, H.I.M.F.L.; Pluim, B.M.; Kilic, O.; Verhagen, E.; Gouttebarge, V.; Holman, R.; Moen, M.H.; Kerkhoffs, G.M.; Tol, J.L. Effectiveness of an e-health tennis-specific injury prevention programme: Randomised controlled trial in adult recreational tennis players. Br. J. Sports Med. 2020, 54, 1036–1041. [Google Scholar] [CrossRef] [PubMed]
- Edouard, P.; Branco, P.; Alonso, J.M. Challenges in Athletics injury and illness prevention: Implementing prospective studies by standardised surveillance. Br. J. Sport Med. 2014, 48, 481–482. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nielsen, R.O.; Bertelsen, M.L.; Ramskov, D.; Damsted, C.; Verhagen, E.; Bredeweg, S.W.; Theisen, D.; Malisoux, L. Randomised controlled trials (RCTs) in sports injury research: Authors-Please report the compliance with the intervention. Br. J. Sports Med. 2020, 54, 51–57. [Google Scholar] [CrossRef] [Green Version]
- van Reijen, M.; Vriend, I.; van Mechelen, W.; Finch, C.F.; Verhagen, E.A. Compliance with Sport Injury Prevention Interventions in Randomised Controlled Trials: A Systematic Review. Sport Med. 2016, 46, 1125–1139. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bredeweg, S.W.; Zijlstra, S.; Bessem, B.; Buist, I. The effectiveness of a preconditioning programme on preventing running-related injuries in novice runners: A randomised controlled trial. Br. J. Sports Med. 2012, 46, 865–870. [Google Scholar] [CrossRef] [Green Version]
- Andersson, S.H.; Bahr, R.; Clarsen, B.; Myklebust, G. Preventing overuse shoulder injuries among throwing athletes: A cluster-randomised controlled trial in 660 elite handball players. Br. J. Sports Med. 2017, 51, 1073–1080. [Google Scholar] [CrossRef] [Green Version]
- Edouard, P.; Steffen, K.; Navarro, L.; Mansournia, M.A.; Nielsen, R.O. Methods matter: Instrumental variable analysis may be a complementary approach to intention-to-treat analysis and as treated analysis when analysing data from sports injury trials. Br. J. Sports Med. 2021, 55, 1006–1008. [Google Scholar] [CrossRef]
- Finch, C. A new framework for research leading to sports injury prevention. J. Sci. Med. Sport 2006, 9, 3–9. [Google Scholar] [CrossRef]
- Donaldson, A.; Finch, C.F. Planning for implementation and translation: Seek first to understand the end-users’ perspectives. Br. J. Sports Med. 2012, 46, 306–307. [Google Scholar] [CrossRef]
- Owoeye, O.B.A.; McKay, C.; Verhagen, E.A.L.M.; A Emery, C. Advancing adherence research in sport injury prevention. Br. J. Sports Med. 2018, 52, 5–7. [Google Scholar] [CrossRef]
- Steib, S.; Rahlf, A.L.; Pfeifer, K.; Zech, A. Dose-Response Relationship of Neuromuscular Training for Injury Prevention in Youth Athletes: A Meta-Analysis. Front. Physiol. 2017, 8, 920. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kok, G.; Gottlieb, N.H.; Peters, G.-J.; Mullen, P.D.; Parcel, G.S.; Ruiter, R.A.; Fernández, M.E.; Markham, C.M.; Bartholomew, L.K. A taxonomy of behaviour change methods: An Intervention Mapping approach A taxonomy of behaviour change methods: An Intervention. Health Psychol. Rev. 2016, 10, 297–312. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
{kind=link}
{kind=link}
| Exercises | Repetitions | Bonus (If It Is Too Easy, Athlete Can Increase Difficulty) |
|---|---|---|
| Core stability—the plank (4 sides: prone position, lateral, supine position, lateral): | ||
| Level 1: both legs | 15 sec. per side for 3 min | 4 × 30 sec. for 6 min, then for 12 min |
| Level 2: alternate legs | ||
| Level 3: unstable support | ||
| Single leg balance: | ||
| Level 1: static | 3 × 15 sec. (each side) | 3 × 30 sec. each side |
| Level 2: unstable support | ||
| Level 3: throwing ball with partner, then on unstable support | ||
| Pelvis strengthening: | ||
| Lunges | 3 × 10 rep. | 6 × 10 rep., then 6 × 10 rep. with medicine ball |
| Hip abductor strengthening—Level 1: leg empty | 3 × 10 rep. (each side) | 6 × 10 rep. (each side), then unstable support |
| Hip abductor strengthening—Level 2: with elastic | 3 × 10 rep. (each side) | 6 × 10 rep. (each side), then unstable support |
| Hamstring exercises: | ||
| Hamstring stretching (different positions) | 3 × 15 sec. | |
| Hamstring strengthening | ||
| Level 1: isometric contraction on two legs | 6 × 6 sec. | 10 × 10 sec. |
| Level 1: heel to buttock with elastic | 3 × 6 sec. (each side) | 5 × 10 sec. (each side) |
| Level 2: isometric contraction on one leg | 6 × 6 sec. (each side) | 10 × 10 sec. (each side) |
| Level 2: heel to buttock with elastic | 3 × 6 sec. (each side) | 5 × 10 sec. (each side) |
| Level 3: Nordic hamstring with help of upper arms | 1 × 5 rep., then 3 × 5 rep., then 6 × 6 rep. | |
| Level 4: Nordic hamstring | 1 × 5 rep., then 3 × 5 rep., then 6 × 6 rep. | |
| Level 5: Pliometric | 1 × 5 rep., then 3 × 5 rep., then 6 × 6 rep. | |
| Lower leg exercises: | ||
| Lower leg stretching | 3 × 15 sec. (each side) | |
| Lower leg strengthening—Level 1: down to the ground | 3 × 8 rep. (each side) | 3 × 10 rep., then 5 × 10 rep. each side and then increase load |
| Lower leg strengthening—Level 2: down to the void | 3 × 8 rep. (each side) | 3 × 10 rep., then 5 × 10 rep. each side, and then increase loads |
| Total Included Athletes (n = 840) | Athletes with 100% Response Proportion over the 39 Weeks (n = 168) | Athletes Included in the Survival Analysis with at Least One Weekly Response (n = 667) | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Intervention (n = 449) | Control (n = 391) | Intervention (n = 68) | Control (n = 100) | Intervention (n = 350) | Control (n = 317) | |||||||
| Sex: | ||||||||||||
| Female athletes | 201 | (44.8) | 149 | (38.1) | 28 | (41.2) | 29 | (29.0) | 155 | (44.3) | 115 | (36.3) |
| Male athletes | 248 | (55.2) | 242 | (61.9) | 40 | (58.8) | 71 | (71.0) | 195 | (55.7) | 202 | (63.7) |
| Age (years) | 30.1 | (6.7) | 30.2 | (6.6) | 32.4 | (6.1) | 30.9 | (6.5) | 30.4 | (6.7) | 30.5 | (6.4) |
| Height (cm) * | 172.5 | (8.7) | 173.0 | (8.1) | 173.5 | (8.6) | 175.3 | (8.2) | 172.5 | (8.9) | 173.3 | (8.1) |
| Body mass (kg) * | 63.2 | (10.1) | 64.3 | (11.6) | 63.2 | (9.3) | 64.3 | (9.2) | 63.1 | (10.3) | 64.7 | (11.6) |
| Disciplines: * | ||||||||||||
| Endurance | 347 | (77.3) | 305 | (78.0) | 60 | (88.2) | 79 | (79.0) | 279 | (79.7) | 248 | (78.2) |
| Road running | 185 | (41.2) | 162 | (41.4) | 30 | (44.1) | 38 | (38.0) | 144 | (41.1) | 130 | (41.0) |
| Middle and long distances running (track) | 83 | (18.5) | 60 | (15.3) | 15 | (22.1) | 19 | (19.0) | 71 | (20.3) | 49 | (15.5) |
| Race Walking | 2 | (0.4) | 7 | (1.8) | 1 | (1.5) | 2 | (2.0) | 2 | (0.6) | 5 | (1.6) |
| Trail | 77 | (17.1) | 76 | (19.4) | 14 | (20.6) | 20 | (20.0) | 62 | (17.7) | 64 | (20.2) |
| Explosive | 97 | (21.6) | 84 | (21.5) | 8 | (11.8) | 21 | (21.0) | 70 | (20.0) | 67 | (21.1) |
| Sprints | 44 | (9.8) | 30 | (7.7) | 4 | (5.9) | 4 | (4.0) | 37 | (10.6) | 22 | (6.9) |
| Hurdles | 13 | (2.9) | 12 | (3.1) | 1 | (1.5) | 4 | (4.0) | 9 | (2.6)) | 9 | (2.8) |
| Jumps | 19 | (4.2) | 16 | (4.1) | 2 | (2.9) | 4 | (4.0) | 13 | (3.7) | 14 | (4.4) |
| Throws | 14 | (3.1) | 14 | (3.6) | 0 | (0.0) | 2 | (2.0) | 8 | (2.3) | 10 | (3.2) |
| Combined events | 7 | (1.6) | 12 | (3.1) | 1 | (1.5) | 7 | (7.0) | 3 | (0.9) | 12 | (3.8) |
| Weekly athletics training (hours) * | 5.4 | (2.5) | 5.7 | (2.9) | 5.3 | (2.1) | 5.3 | (2.4) | 5.3 | (2.4) | 5.6 | (2.7) |
| Week sport practice expect athletics (hours) * | 2.8 | (3.0) | 2.5 | (2.7) | 2.5 | (2.9) | 2.2 | (2.5) | 2.7 | (2.9) | 2.4 | (2.6) |
| History of ICPR during the preceding season: * | ||||||||||||
| No | 140 | (52.0) | 142 | (54.4) | 36 | (52.9) | 53 | (53.0) | 124 | (52.5) | 132 | (54.3) |
| Yes | 129 | (48.0) | 119 | (45.6) | 32 | (47.1) | 47 | (47.0) | 112 | (47.5) | 111 | (45.7) |
| Outcome | Percentage (No) | Adjusted Odds Ratio (95% CI) * | ||
|---|---|---|---|---|
| Intervention Group (n = 68) | Control Group (n = 100) | |||
| Proportion of athletes who presented at least one ICPR over 39 weeks (n = 168) | 64.7% (n = 44) | 65.0% (n = 65) | 0.81 (0.36 to 1.85) | |
| Low compliance ** (n = 36 of 68) | 63.9% (n = 23 of 36) | 0.85 (0.37 to 1.97) | ||
| Moderate compliance ** (n = 26 of 68) | 69.2% (n = 18 of 26) | 1.13 (0.45 to 3.04) | ||
| Good compliance ** (n = 6 of 68) | 50.0% (n = 3 of 6) | 0.75 (0.12 to 4.82) | ||
| Outcome | Intervention Group (n = 68) (Mean (SD) | Control Group (n = 100) (Mean (SD) | Adjusted Difference * (95% CI) | |
|---|---|---|---|---|
| Injury burden (days lost per 1000 h of exposure) over 39 weeks (n = 168) | 343.3 (817.8) | 285.6 (619.6) | 11.3 (−322.5 to 172.9 | |
| Low compliance ** (n = 36 of 68) | 307.1 (513.2) | 19.9 (−207.5 to 247.3) | ||
| Moderate compliance ** (n = 26 of 68) | 449.6 (1180.2) | 134.2 (−200.3 to 468.8) | ||
| Good compliance ** (n = 6 of 68) | 99.9 (125.3) | −159.2 (−670.2 to 351.8) | ||
| Outcome | Intervention Group (n = 350) (Mean (SD) | Control Group (n = 317) (Mean (SD) | Adjusted Hazard Ratio * (95% CI) | |
|---|---|---|---|---|
| Time to the first ICPR during athletics practice (in weeks) (n = 667) | 6.62 (9.64) | 7.58 (8.94) | 1.02 (0.76 to 1.37) | |
| Low compliance ** (n = 231 of 350) | 5.62 (8.94) | 0.96 (0.65 to 1.40) | ||
| Moderate compliance ** (n = 76 of 350) | 9.34 (11.41) | 1.06 (0.60 to 1.89) | ||
| Good compliance ** (n = 43 of 350) | 7.19 (9.11) | 0.90 (0.43 to 1.90) | ||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Edouard, P.; Steffen, K.; Peuriere, M.; Gardet, P.; Navarro, L.; Blanco, D. Effect of an Unsupervised Exercises-Based Athletics Injury Prevention Programme on Injury Complaints Leading to Participation Restriction in Athletics: A Cluster-Randomised Controlled Trial. Int. J. Environ. Res. Public Health 2021, 18, 11334. https://doi.org/10.3390/ijerph182111334
Edouard P, Steffen K, Peuriere M, Gardet P, Navarro L, Blanco D. Effect of an Unsupervised Exercises-Based Athletics Injury Prevention Programme on Injury Complaints Leading to Participation Restriction in Athletics: A Cluster-Randomised Controlled Trial. International Journal of Environmental Research and Public Health. 2021; 18(21):11334. https://doi.org/10.3390/ijerph182111334
Chicago/Turabian StyleEdouard, Pascal, Kathrin Steffen, Marie Peuriere, Pierre Gardet, Laurent Navarro, and David Blanco. 2021. "Effect of an Unsupervised Exercises-Based Athletics Injury Prevention Programme on Injury Complaints Leading to Participation Restriction in Athletics: A Cluster-Randomised Controlled Trial" International Journal of Environmental Research and Public Health 18, no. 21: 11334. https://doi.org/10.3390/ijerph182111334
APA StyleEdouard, P., Steffen, K., Peuriere, M., Gardet, P., Navarro, L., & Blanco, D. (2021). Effect of an Unsupervised Exercises-Based Athletics Injury Prevention Programme on Injury Complaints Leading to Participation Restriction in Athletics: A Cluster-Randomised Controlled Trial. International Journal of Environmental Research and Public Health, 18(21), 11334. https://doi.org/10.3390/ijerph182111334