
Effectiveness of a Humor-Based Training for Reducing Employees’ Distress

 , ,
, ,
Abstract
:1. Introduction
Humor as a Stress Coping Mechanism
2. Materials and Methods
2.1. Procedure and Participants
2.2. Rationale and Content of the Training
2.3. Measures
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- American Psychological Association (APA). Stress in AmericaTM 2020 Report. 2020. Available online: https://www.apa.org/news/press/releases/stress/2020/report-october (accessed on 19 August 2021).
- Cosgrove, M.P.; Sargeant, L.A.; Caleyachetty, R.; Griffin, S.J. Work-related stress and Type 2 diabetes: Systematic review and meta-analysis. Occup. Med. (Lond.) 2012, 62, 167–173. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kivimäki, M.; Virtanen, M.; Elovainio, M.; Kouvonen, A.; Väänänen, A.; Vahtera, J. Work stress in the etiology of coronary heart disease—A meta-analysis. Scand. J. Work Environ. Health 2006, 431–442. [Google Scholar] [CrossRef]
- Li, J.; Zhang, M.; Loerbroks, A.; Angerer, P.; Siegrist, J. Work stress and the risk of recurrent coronary heart disease events: A systematic review and meta-analysis. Int. J. Occup. Med. Environ. Health 2014, 1–12. [Google Scholar] [CrossRef]
- Sui, H.; Sun, N.; Zhan, L.; Lu, X.; Chen, T.; Mao, X. Association between work-related stress and risk for type 2 diabetes: A systematic review and meta-analysis of prospective cohort studies. PLoS ONE 2016, 11, e0159978. [Google Scholar] [CrossRef]
- Hassard, J.; Teoh, K.R.; Visockaite, G.; Dewe, P.; Cox, T. The cost of work-related stress to society: A systematic review. J. Occup. Health Psychol. 2018, 23, 1. [Google Scholar] [CrossRef] [Green Version]
- Health and Safety Executive (HSE). Health and Safety at Work: Summary Statistics for Great Britain 2020. 2020. Available online: https://www.hse.gov.uk/statistics/overall/hssh1920.pdf (accessed on 19 August 2021).
- Krystal, J.H.; McNeil, R.L. Responding to the hidden pandemic for healthcare workers: Stress. Nat. Med. 2020, 26, 639. [Google Scholar] [CrossRef] [PubMed]
- Richardson, K.M.; Rothstein, H.R. Effects of occupational stress management intervention programs: A meta-analysis. J. Occup. Health Psychol. 2008, 13, 69. [Google Scholar] [CrossRef]
- Kröll, C.; Doebler, P.; Nüesch, S. Meta-analytic evidence of the effectiveness of stress management at work. Eur. J. Work Organ. Psychol. 2017, 26, 677–693. [Google Scholar] [CrossRef]
- Bartlett, L.; Martin, A.; Neil, A.L.; Memish, K.; Otahal, P.; Kilpatrick, M.; Sanderson, K.A. Systematic review and meta-analysis of workplace mindfulness training randomized controlled trials. J. Occup. Health Psychol. 2019, 24, 108. [Google Scholar] [CrossRef] [PubMed]
- Mills, M.J.; Fleck, C.R.; Kozikowski, A. Positive psychology at work: A conceptual review, state-of-practice assessment, and a look ahead. J. Posit. Psychol. 2013, 8, 153–164. [Google Scholar] [CrossRef]
- Meyers, M.C.; van Woerkom, M.; Bakker, A.B. The added value of the positive: A literature review of positive psychology interventions in organizations. Eur. J. Work. Organ. Psychol. 2013, 22, 618–632. [Google Scholar] [CrossRef]
- Donaldson, S.I.; Lee, J.Y.; Donaldson, S.I. Evaluating positive psychology interventions at work: A systematic review and meta-analysis. Int. J. Appl. Posit. Psychol. 2019, 4, 113–134. [Google Scholar] [CrossRef] [Green Version]
- Mesmer-Magnus, J.; Glew, D.J.; Viswesvaran, C. A meta-analysis of positive humor in the workplace. J. Manag. Psychol. 2012, 27, 155–190. [Google Scholar] [CrossRef]
- Martin, R.A. The Psychology of Humor: An Integrative Approach, 1st ed.; Elsevier Science: Burlington, MA, USA, 2007. [Google Scholar]
- Thorson, J.A. Powell, F.C. Development and validation of a multidimensional sense of humor scale. J. Clin. Psychol. 1993, 49, 3–23. [Google Scholar] [CrossRef]
- Thorson, J.A. Powell, F.C. Sense of humor scale and Dimensions of Personality. J. Clin. Psychol. 1993, 49, 799–808. [Google Scholar] [CrossRef]
- Dixon, N.F. Humor: A cognitive alternative to stress. In Stress and Anxiety; Sarason, I.G., Spielberger, C.D., Eds.; Hemisphere: Washington, DC, USA, 1980; Volume 7. [Google Scholar]
- Martin, R.A.; Lefcourt, H.M. Sense of humor as a moderator of the relation between stressors and moods. J. Personal. Soc. Psychol. 1983, 45, 1313. [Google Scholar] [CrossRef]
- García-Larrauri, B. Programa Para Mejorar el Sentido del Humor: ¡Porque la Vida con Buen Humor Merece la Pena! Pirámide: Madrid, Spain, 2006. [Google Scholar]
- Baisley, M.C.; Grunberg, N.E. Bringing humor theory into practice: An interdisciplinary approach to online humor training. New Ideas Psychol. 2019, 55, 24–34. [Google Scholar] [CrossRef]
- Ruch, W.; McGhee, P.E. Humor intervention programs. In The Wiley Blackwell Handbook of Positive Psychological Interventions; Parks, A.C., Schueller, S.M., Eds.; Wiley Blackwell: Hoboken, NJ, USA, 2014; pp. 179–193. [Google Scholar]
- Ruch, W.F.; Hofmann, J.; Ruch, S.; Stolz, H. Training the sense of humor with the 7 Humor Habits Program and satisfaction with life. Humor 2018, 31, 287–309. [Google Scholar] [CrossRef] [Green Version]
- Wellenzohn, S.; Proyer, R.T.; Ruch, W. Who benefits from humor-based positive psychology interventions? The moderating effects of personality traits and sense of humor. Front. Psychol. 2018, 9, 821. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wellenzohn, S.; Proyer, R.T.; Ruch, W. Humor-based online positive psychology interventions: A randomized placebo-controlled long-term trial. J. Posit. Psychol. 2016, 11, 584–594. [Google Scholar] [CrossRef]
- Wellenzohn, S.; Proyer, R.T.; Ruch, W. How do positive psychology interventions work? A short-term placebo-controlled humor-based study on the role of the time focus. Pers. Individ. Differ. 2016, 96, 1–6. [Google Scholar] [CrossRef] [Green Version]
- Bartzik, M.; Bentrup, A.; Hill, S.; Bley, M.; von Hirschhausen, E.; Krause, G.; Peifer, C. Care for Joy: Evaluation of a Humor Intervention and Its Effects on Stress, Flow Experience, Work Enjoyment, and Meaningfulness of Work. Front. Public Health 2021, 9, 667821. [Google Scholar] [CrossRef] [PubMed]
- van Oortmerssen, L.A.; Caniëls, M.C.; van Assen, M.F. Coping with work stressors and paving the way for flow: Challenge and hindrance demands, humor, and cynicism. J. Happiness Stud. 2020, 21, 2257–2277. [Google Scholar] [CrossRef] [Green Version]
- Cann, A.; Etzel, K.C. Remembering and anticipating stressors: Positive personality mediates the relationship with sense of humor. Humor-Int. J. Humor Res. 2008, 21, 157–178. [Google Scholar] [CrossRef]
- Wanzer, M.; Booth-Butterfield, M.; Booth-Butterfield, S. “If we didn’t use humor, we’d cry”: Humorous coping communication in health care settings. J. Health Commun. 2005, 10, 105–125. [Google Scholar] [CrossRef]
- Sliter, M.; Kale, A.; Yuan, Z. Is humor the best medicine? The buffering effect of coping humor on traumatic stressors in firefighters. J. Organ. Behav. 2014, 35, 257–272. [Google Scholar] [CrossRef]
- Marziali, E.; McDonald, L.; Donahue, P. The role of coping humor in the physical and mental health of older adults. Aging Ment. Health 2008, 12, 713–718. [Google Scholar] [CrossRef]
- Fritz, H.L.; Russek, L.N.; Dillon, M.M. Humor use moderates the relation of stressful life events with psychological distress. Pers. Soc. Psychol. Bull. 2017, 43, 845–859. [Google Scholar] [CrossRef]
- Cheng, D.; Chan, X.W.; Amarnani, R.K.; Farivar, F. Finding humor in work–life conflict: Distinguishing the effects of individual and co-worker humor. J. Vocat. Behav. 2021, 125, 103538. [Google Scholar] [CrossRef]
- van der Wal, C.N.; Kok, R.N. Laughter-inducing therapies: Systematic review and meta-analysis. Soc. Sci. Med. 2019, 232, 473–488. [Google Scholar] [CrossRef]
- Zhao, J.; Yin, H.; Zhang, G.; Li, G.; Shang, B.; Wang, C.; Chen, L. A meta-analysis of randomized controlled trials of laughter and humour interventions on depression, anxiety and sleep quality in adults. J. Adv. Nurs. 2019, 75, 2435–2448. [Google Scholar] [CrossRef]
- Romero, E.; Pescosolido, A. Humor and group effectiveness. Hum. Relat. 2008, 61, 395–418. [Google Scholar] [CrossRef]
- Jarzabkowski, P.A.; Lê, J.K. We have to do this and that? You must be joking: Constructing and responding to paradox through humor. Organ. Stud. 2017, 38, 433–462. [Google Scholar] [CrossRef] [Green Version]
- Vecchio, R.P.; Justin, J.E.; Pearce, C.L. The influence of leader humor on relationships between leader behavior and follower outcomes. J. Manag. Issues 2009, 171–194. [Google Scholar]
- Pundt, A.; Herrmann, F. Affiliative and aggressive humour in leadership and their relationship to leader–member exchange. J. Occup. Organ. Psychol. 2015, 88, 108–125. [Google Scholar] [CrossRef]
- Yam, K.C.; Christian, M.S.; Wei, W.; Liao, Z.; Nai, J. The mixed blessing of leader sense of humor: Examining costs and benefits. Acad. Manage. J. 2018, 61, 348–369. [Google Scholar] [CrossRef]
- Dyck, K.T.; Holtzman, S. Understanding humor styles and well-being: The importance of social relationships and gender. Pers. Individ. Differ. 2013, 55, 53–58. [Google Scholar] [CrossRef]
- Martin, R.A.; Puhlik-Doris, P.; Larsen, G.; Gray, J.; Weir, K. Individual differences in uses of humor and their relation to psychological well-being: Development of the Humor Styles Questionnaire. J. Res. Pers. 2003, 37, 48–75. [Google Scholar] [CrossRef]
- Guenter, H.; Schreurs, B.; Van Emmerik, I.H.; Gijsbers, W.; Van Iterson, A. How adaptive and maladaptive humor influence well-being at work: A diary study. Humor 2013, 26, 573–594. [Google Scholar] [CrossRef]
- Cantero-Sánchez, F.J.; León-Rubio, J.M.; Medina-Anzano, S.; Gómez-Delgado, T. Evaluación y entrenamiento de las habilidades sociales. In Psicología Social: Orientaciones Teóricas y Ejercicios Prácticas; León-Rubio, J.M., Barriga, S., Gómez-Delgado, T., González-Gabaldón, B., Medina-Anzano, S., Cantero-Sánchez, F.J., Eds.; McGraw-Hill: Madrid, Spain, 1998; pp. 433–452. [Google Scholar]
- Simoes de Araujo, E.A.; Ferreira Xavier Ribeiro, M.J.; Sá Rodrigues, M.D.; León Rubio, J.M. Habilidades sociais e empreendedorismo. In Habilidades Sociais. Diálogos e Intercâmbios Sobre Pesquisa e Práctica; Del Prette, Z.A.P., Benevides-Soares, A., de Sousa Pereira-Guizzo, C., Fortes-Wagner, M., Romera-Leme, V.B., Eds.; Sinopsys: Sao Paulo, Brazil, 2015; pp. 425–444. [Google Scholar]
- Sá Rodrigues, M.D.; Simoes de Araujo, E.A.; Ferreira Xavier Ribeiro, M.J.; León-Rubio, J.M. Habilidades interpessoais nas competências gerenciais e de liderança. In Habilidades Sociais. Diálogos e Intercâmbios Sobre Pesquisa e Práctica; Del Prette, Z.A.P., Benevides-Soares, A., de Sousa Pereira-Guizzo, C., Fortes-Wagner, M., Romera-Leme, V.B., Eds.; Sinopsys: Sao Paulo, Brazil, 2015; pp. 462–496. [Google Scholar]
- Cantero-Sánchez, F.J.; León-Rubio, J.M.; Vázquez-Morejón, R.; León-Pérez, J.M. Evaluation of an assertiveness training based on the Social Learning Theory for Occupational Health, Safety, and Environment practitioners. Sustainability 2021, 13, 11504. [Google Scholar] [CrossRef]
- Carbelo Baquero, B. Estudio del Sentido del Humor: Validación de un Instrumento para Medir el Sentido del Humor, Análisis del Cuestionario y su Relación con el Estrés; Universidad de Alcalá: Alcalá de Henares, Spain, 2005. [Google Scholar]
- Tapia-Villanueva, L.; Armijo, I.; Pereira, X.; Molina, M.E. Chilean Spanish version of the State Trait Cheerfulness Inventory (STCI-T-60, trait form): Individual and couple forms. Humor 2014, 27, 481–498. [Google Scholar] [CrossRef]
- Lobo, A.; Pérez-Echeverría, M.J.; Artal, J. Validity of the scaled version of the General Health Questionnaire (GHQ-28) in a Spanish population. Psychol. Med. 1986, 16, 135–140. [Google Scholar] [CrossRef] [PubMed]
- Fritz, C.O.; Morris, P.E.; Richler, J.J. Effect size estimates: Current use, calculations, and interpretation. J. Exp. Pyschol. Gen. 2012, 141, 2–18. [Google Scholar] [CrossRef] [Green Version]
- Berry, S. Humor me on this one. The healing role of humor in EMS. JEMS 2003, 28, 66–79. [Google Scholar] [PubMed]
- Rosenberg, L. A qualitative investigation of the use of humor by emergency personnel as a strategy for coping with stress. J. Emerg. Nurs. 1991, 17, 197–202. [Google Scholar] [PubMed]
- van Wormer, K.; Boes, M. Humor in the emergency room: A social work perspective. Health. Soc. Work 1997, 22, 87–92. [Google Scholar] [CrossRef] [PubMed]
- Piotrowski, A.; Makarowski, R.; Predoiu, R.; Predoiu, A.; Boe, O. Resilience and Subjectively Experienced Stress Among Paramedics Prior to and During the COVID-19 Pandemic. Front. Psychol. 2021, 12, 664540. [Google Scholar] [CrossRef] [PubMed]
- Rose, S.; Hartnett, J.; Pillai, S. Healthcare worker’s emotions, perceived stressors and coping mechanisms during the COVID-19 pandemic. PLoS ONE 2021, 16, e0254252. [Google Scholar] [CrossRef]
- Caudill, A.; Woodzicka, J. Funny business: Using humor for good in the workplace. Humor-Int. J. Humor Res. 2017, 30, 43–62. [Google Scholar] [CrossRef]
- Fang, X.H.; Wu, L.; Lu, L.S.; Kan, X.H.; Wang, H.; Xiong, Y.J.; Ma, D.C.; Wu, G.C. Mental health problems and social supports in the COVID-19 healthcare workers: A Chinese explanatory study. BMC Psychiatry 2021, 21, 34. [Google Scholar] [CrossRef]
- Fritz, H.L. Why are humor styles associated with well-being, and does social competence matter? Examining relations to psychological and physical well-being, reappraisal, and social support. Pers. Individ. Differ. 2020, 154, 109641. [Google Scholar] [CrossRef]
- Avison, W.R.; Pearlin, L.I. Advances in the Conceptualization of the Stress Process: Essays in Honor of Leonard I. Pearlin; Springer: New York, NY, USA, 2010; pp. 261–269. [Google Scholar]
- Briñol, P.; Petty, R.E.; Gandarillas, B.; Moreno, L. Are positive interventions always beneficial? Span. J. Psychol. 2020, 23, E23. [Google Scholar] [CrossRef] [PubMed]
- Bakker, A.B.; Rodriguez-Munoz, A.; Derks, D. The emergence of positive occupational health psychology. Psicothema 2012, 24, 66–72. [Google Scholar]
- Salanova, M.; Llorens, S.; Martínez, I.M. Contributions from positive organizational psychology to develop healthy and resilient organizations. Papeles del Psicol. 2016, 37, 177–184. [Google Scholar]

{kind=link}
{kind=link}
| Content | Sessions | Objectives and Activities |
|---|---|---|
| Welcome | 0 | Sending welcome email with training schedule and a participation letter that explained the study. |
| Introduction | 1 | Conducting pre-training data collection. Understanding the sense of humor from a scientific perspective and the benefits of using positive humor at work (vs. other types of humor). |
| Humor appreciation | 2–4 | Exploring the factors that facilitate good mood and the use of positive humor at work. Being more tolerant with oneself. |
| Humor creation | 5–7 | Improving creativity and flexible thinking in order to intentionally create positive humor. |
| Humor as coping | 8–10 | Anticipating adverse conditions at work and coping with adversity in a more flexible and positive way. How to use positive humor under stressful situations. |
| Positive exchanges | 11–12 | Developing an assertive communication style in which positive humor can play a pivotal role. |
| Follow-up | 13 | Monitoring the training and conducting post-training data collection. |
| Variables | Post-Training | |||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Pre-Training | Mean a | SD a | 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | 9 | 10 | 11 | 12 |
| 1. Sense of humor | 2.43 | 0.47 | 0.90 ** | 0.82 ** | 0.72 ** | 0.58 ** | 0.62 ** | 0.21 | 0.46 ** | −0.39 ** | −0.34 ** | −0.39 ** | −0.46 ** | −0.21 |
| 2. Humor generation | 2.50 | 0.61 | 0.59 ** | 0.53 ** | 0.52 ** | 0.31 * | 0.42 ** | −0.13 | 0.47 ** | −0.22 | −0.12 | −0.26 | −0.26 * | −0.15 |
| 3. Coping through humor | 2.53 | 0.54 | 0.72 ** | 0.67 ** | 0.58 ** | 0.43 ** | 0.50 ** | 0.23 | 0.24 | −0.28 * | −0.28 * | −0.30 * | −0.37 ** | −0.05 |
| 4. Appreciation of humor | 3.50 | 0.84 | 0.49 ** | 0.46 ** | 0.37 ** | 0.33 * | 0.33 * | −0.14 | 0.38 ** | −0.18 | −0.11 | −0.20 | −0.27 * | −0.04 |
| 5. Attit. towards humor | 1.52 | 1.28 | 0.52 ** | 0.49 ** | 0.35 ** | 0.46 ** | 0.35 ** | 0.50 ** | 0.11 | −0.31 * | −0.35 ** | −0.25 | −0.30 * | −0.22 |
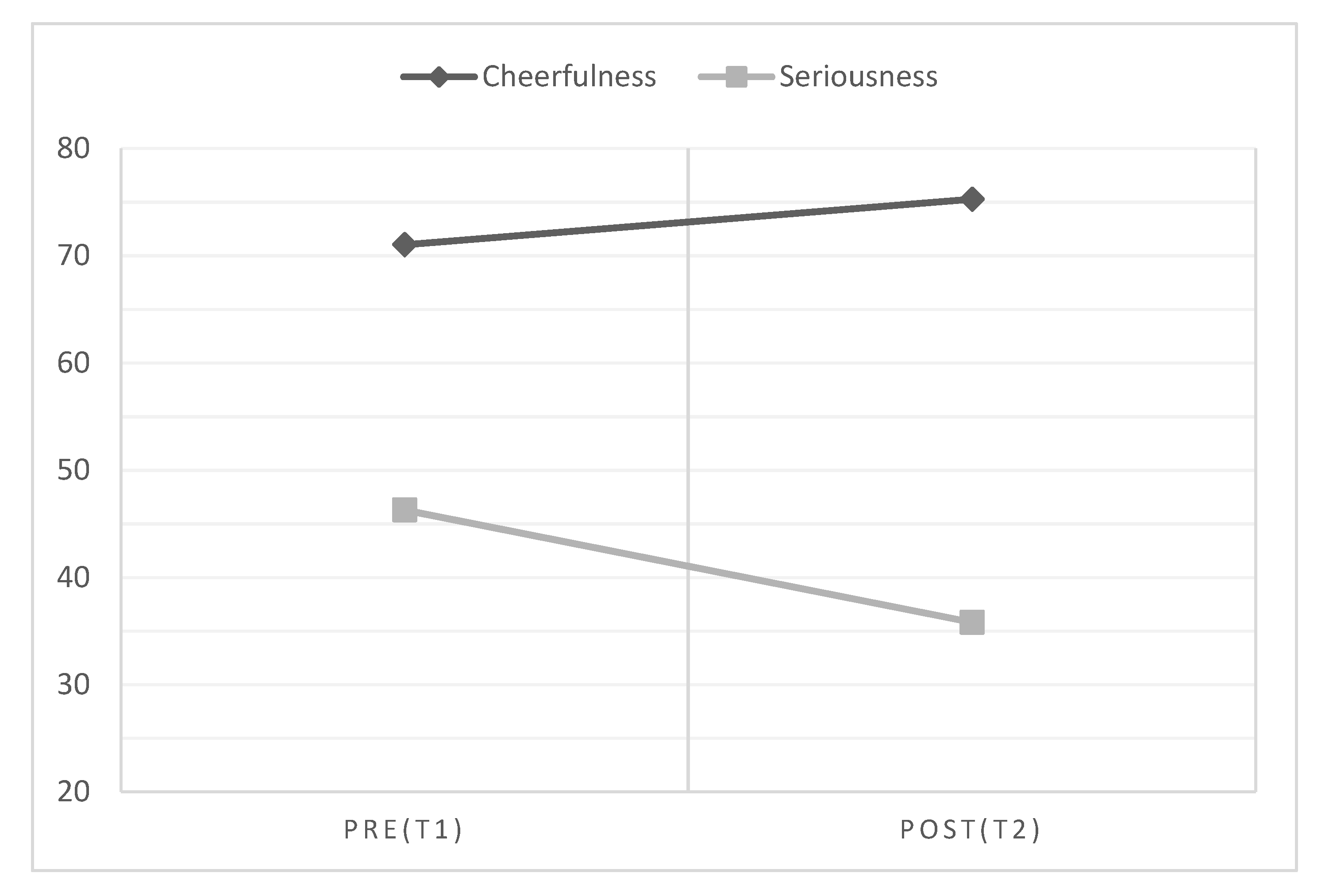
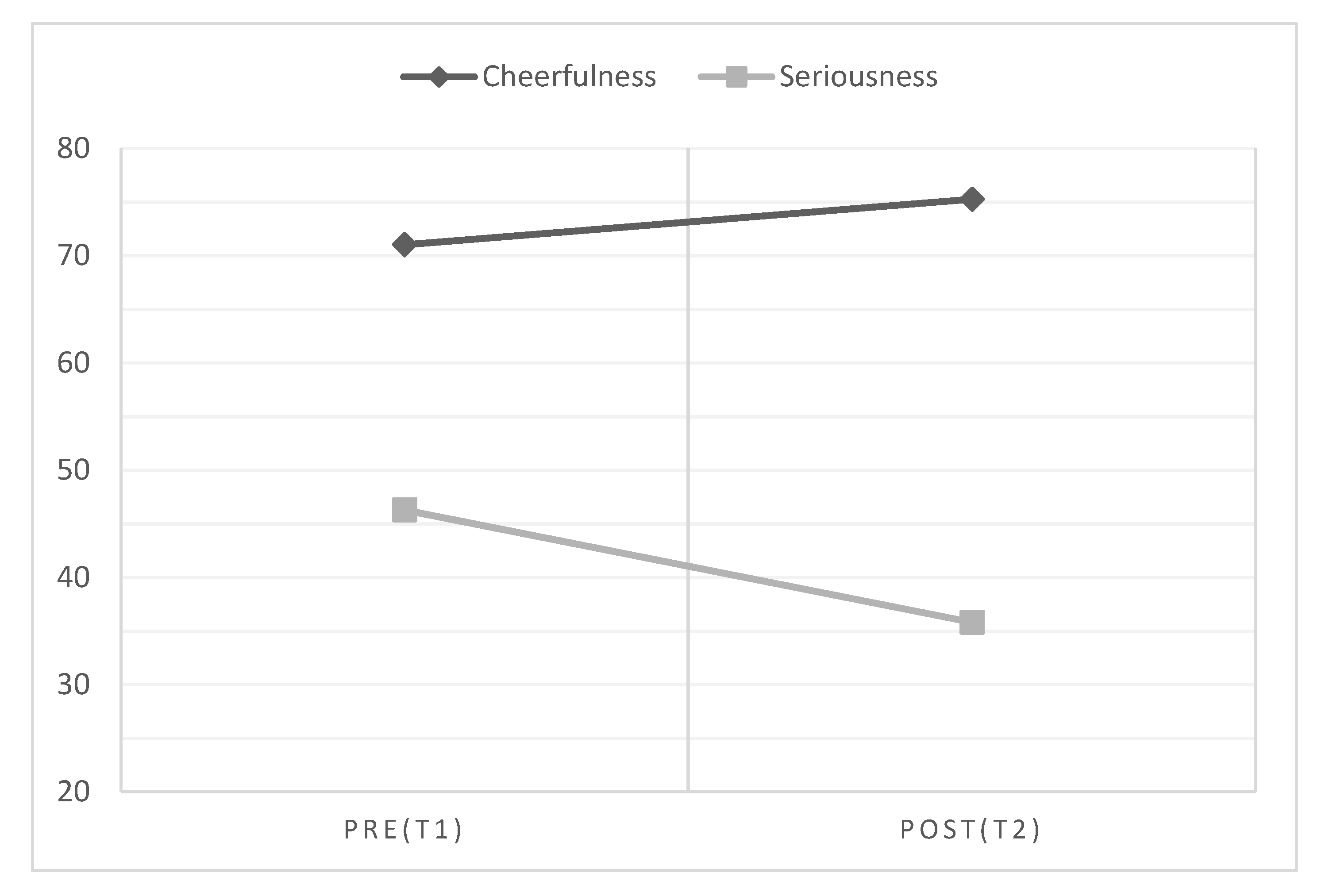
| 6. Seriousness | 46.29 | 21.44 | 0.47 ** | 0.45 ** | 0.29 * | 0.43 ** | 0.30 * | 0.55 ** | 0.07 | −0.28 * | −0.33 * | −0.21 | −0.27 * | −0.17 |
| 7. Cheerfulness | 71.03 | 8.34 | 0.60 ** | 0.54 ** | 0.52 ** | 0.33 * | 0.42 ** | −0.18 | 0.45 ** | −0.25 | −0.16 | −0.31 * | −0.28 * | −0.13 |
| 8. Psychol. distress (PD) | 8.24 | 6.26 | −0.39 ** | −0.30 * | −0.33 * | −0.43 ** | −0.27 * | 0.09 | −0.12 | 0.92 ** | 0.81 ** | 0.80 ** | 0.82 ** | 0.82 ** |
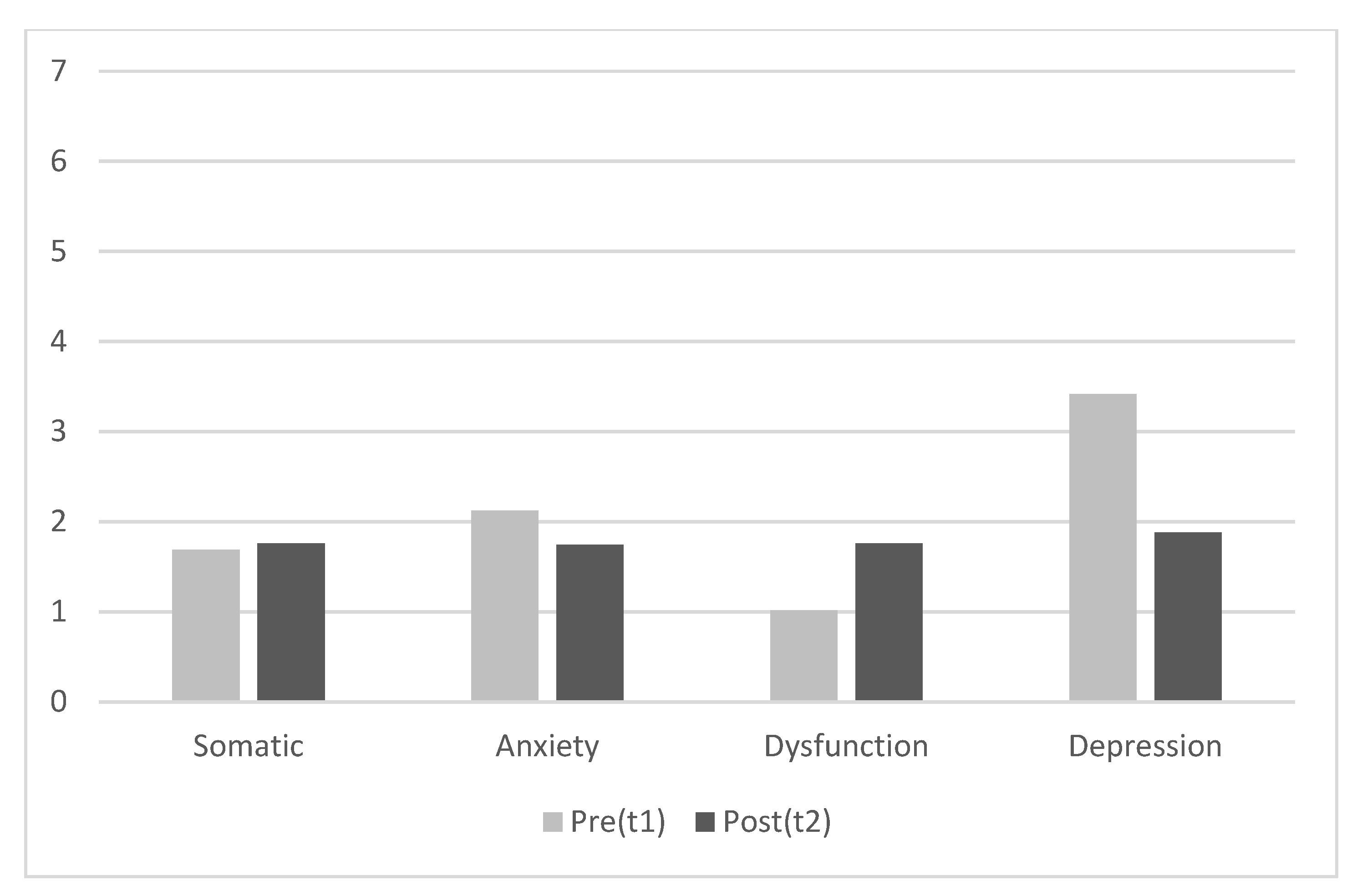
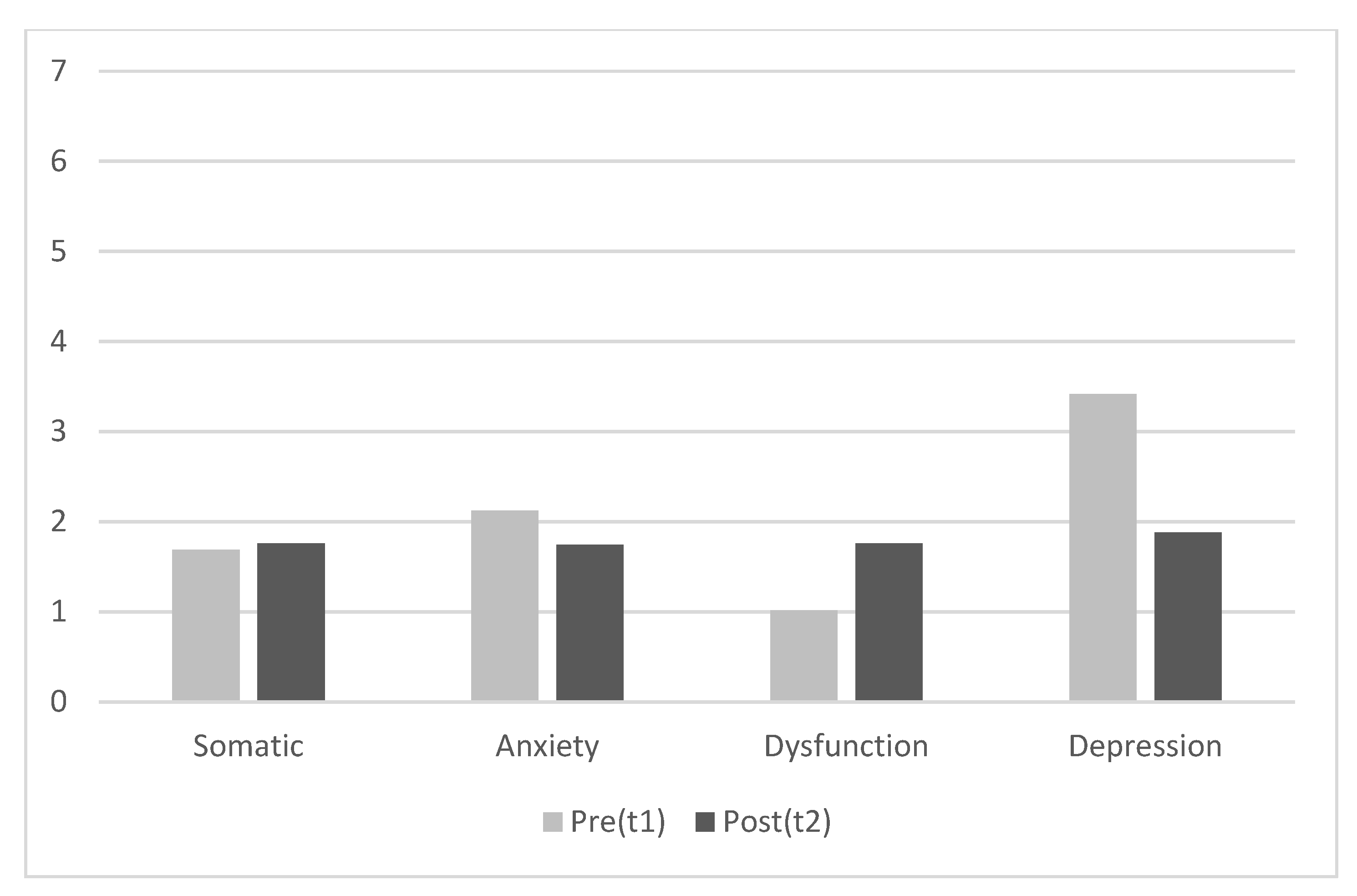
| 9. PD-Somatic symptoms | 1.69 | 1.99 | −0.24 | −0.16 | −0.27 * | −0.24 | −0.12 | 0.29* | −0.11 | 0.68 ** | 0.56 ** | 0.62 ** | 0.66 ** | 0.55 ** |
| 10. PD-Anxiety/insomnia | 2.12 | 2.29 | −0.29 * | −0.21 | −0.24 | −0.37 ** | −0.20 | 0.11 | −0.18 | 0.81 ** | 0.72 ** | 0.78 ** | 0.70 ** | 0.67 ** |
| 11. PD-Social dysfunction | 1.01 | 1.61 | 0.08 | 0.13 | 0.08 | −0.11 | 0.02 | 0.01 | 0.08 | 0.34 * | 0.22 | 0.31 * | 0.21 | 0.47 ** |
| 12. PD-Depression | 3.41 | 3.19 | −0.45 ** | −0.39 ** | −0.34 ** | −0.37 ** | −0.32 * | −0.10 | −0.07 | 0.62 ** | 0.61 ** | 0.47 ** | 0.59 ** | 0.54 ** |
| Mean b | - | - | 2.47 | 2.50 | 2.43 | 2.36 | 2.49 | 35.81 | 75.28 | 7.14 | 1.76 | 1.74 | 1.76 | 1.88 |
| SD b | - | - | 0.56 | 0.61 | 0.63 | 1.08 | 0.80 | 12.15 | 4.19 | 6.09 | 1.76 | 1.72 | 1.66 | 1.72 |
| Variable | Mean Rank Positives | Mean Rank Negatives | Z | p | r |
|---|---|---|---|---|---|
| Sense of humor | 30.63 | 25.28 | −0.73 | 0.462 | 0.07 |
| Generation of humor | 25.52 | 29.98 | −0.20 | 0.843 | 0.02 |
| Coping through humor | 21.71 | 29.81 | −1.33 | 0.182 | 0.12 |
| Appreciation of humor | 10.50 | 25.26 | −5.55 | 0.001 | 0.51 |
| Attitudes toward humor | 33.19 | 12.70 | −4.76 | 0.001 | 0.44 |
| Cheerfulness | 30.50 | 13.66 | −3.93 | 0.001 | 0.36 |
| Seriousness | 15.50 | 36.40 | −3.32 | 0.001 | 0.31 |
| Psychol. Distress (PD) | 18.60 | 22.41 | −3.35 | 0.001 | 0.31 |
| PD-somatic complaints | 22.23 | 20.70 | −0.48 | 0.634 | 0.04 |
| PD-anxiety and insomnia | 16.46 | 18.80 | −1.96 | 0.050 | 0.18 |
| PD-social dysfunction | 22.91 | 21.27 | −3.09 | 0.002 | 0.29 |
| PD-depression | 12.18 | 24.23 | −3.86 | 0.001 | 0.36 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
León-Pérez, J.M.; Cantero-Sánchez, F.J.; Fernández-Canseco, Á.; León-Rubio, J.M. Effectiveness of a Humor-Based Training for Reducing Employees’ Distress. Int. J. Environ. Res. Public Health 2021, 18, 11177. https://doi.org/10.3390/ijerph182111177
León-Pérez JM, Cantero-Sánchez FJ, Fernández-Canseco Á, León-Rubio JM. Effectiveness of a Humor-Based Training for Reducing Employees’ Distress. International Journal of Environmental Research and Public Health. 2021; 18(21):11177. https://doi.org/10.3390/ijerph182111177
Chicago/Turabian StyleLeón-Pérez, Jose M., Francisco J. Cantero-Sánchez, Ángela Fernández-Canseco, and José M. León-Rubio. 2021. "Effectiveness of a Humor-Based Training for Reducing Employees’ Distress" International Journal of Environmental Research and Public Health 18, no. 21: 11177. https://doi.org/10.3390/ijerph182111177
APA StyleLeón-Pérez, J. M., Cantero-Sánchez, F. J., Fernández-Canseco, Á., & León-Rubio, J. M. (2021). Effectiveness of a Humor-Based Training for Reducing Employees’ Distress. International Journal of Environmental Research and Public Health, 18(21), 11177. https://doi.org/10.3390/ijerph182111177