
Eating Behaviour Changes during the COVID-19 Pandemic: A Systematic Review of Longitudinal Studies



Abstract
:1. Introduction
2. Materials and Methods
2.1. Search Strategy
2.2. Study Selection Process
3. Results
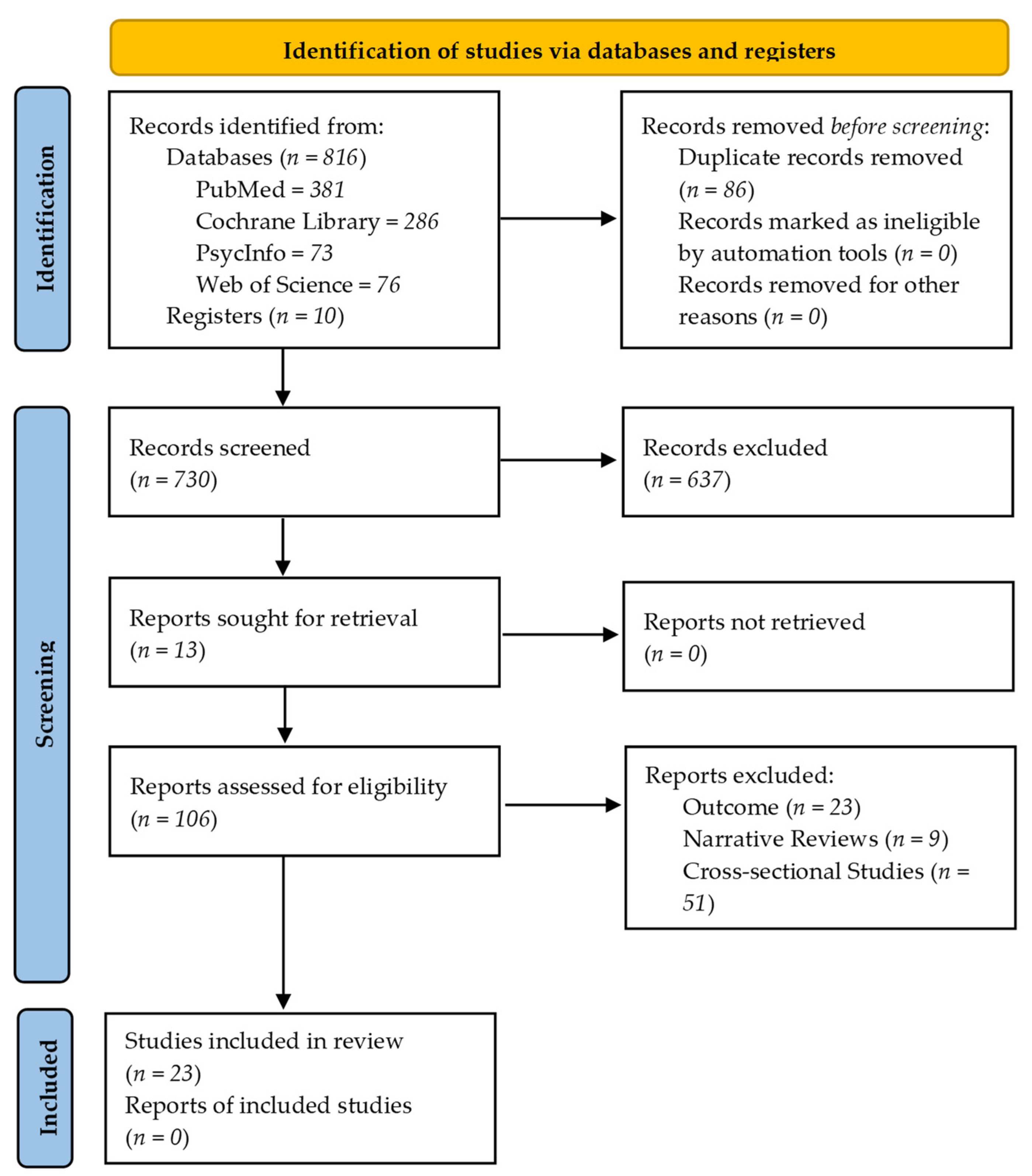
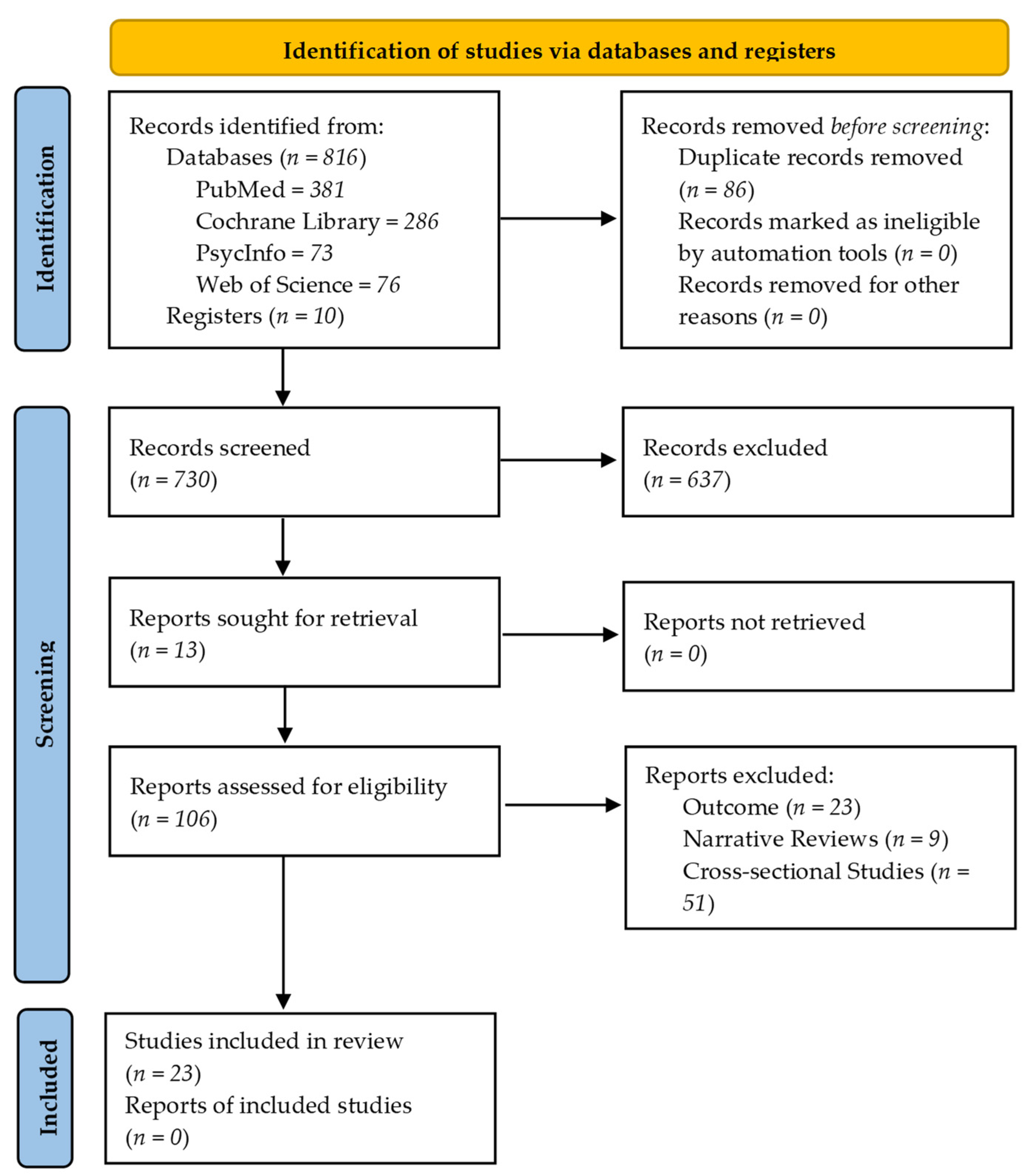
3.1. Study Selection
3.2. Study Characteristics
3.2.1. Country and Design of the Studies
3.2.2. Target Population
3.2.3. Sample Size
3.2.4. Assessment Tools
3.3. Objectives, Outcomes, and Results
3.3.1. Objectives
3.3.2. Outcomes
3.3.3. Results
3.4. Quality of Studies
4. Discussion
Implications for Government Policies in Nutrition
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Pérez Abreu, M.R.; Gómez Tejeda, J.J.; Dieguez Guach, R.A. Características clínico epidemiológicas de la COVID-19. Rev. Haban. Cienc. Méd. 2020, 19, e3254. [Google Scholar]
- Negrini, S.; Grabljevec, K.; Boldrini, P.; Kiekens, C.; Moslavac, S.; Zampolini, M.; Christodoulou, N. Up to 2.2 million people experiencing disability suffer collateral damage each day of COVID-19 lockdown in Europe. Eur. J. Phys. Rehabil. Med. 2020, 56, 361–365. [Google Scholar] [CrossRef]
- Parrado-González, A.; León-Jariego, J.C. Factores asociados al malestar emocional y morbilidad psíquica en población española [COVID-19: Factors associated with emotional distress and psychological morbidity in spanish population]. Rev. Esp. Salud Pública 2020, 94, e202006058. [Google Scholar]
- Ammar, A.; Brach, M.; Trabelsi, K.; Chtourou, H.; Boukhris, O.; Masmoudi, L.; Bouaziz, B.; Bentlage, E.; How, D.; Ahmed, M.; et al. Effects of COVID-19 Home Confinement on Eating Behaviour and Physical Activity: Results of the ECLB-COVID19 International Online Survey. Nutrients 2020, 12, 1583. [Google Scholar] [CrossRef]
- Balanzá–Martínez, V.; Atienza–Carbonell, B.; Kapczinski, F.; De Boni, R.B. Lifestyle behaviours during the COVID-19—Time to connect. Acta Psychiatr. Scand. 2020, 141, 399–400. [Google Scholar] [CrossRef]
- Campbell, H.; Wood, A.C. Challenges in Feeding Children Posed by the COVID-19 Pandemic: A Systematic Review of Changes in Dietary Intake Combined with a Dietitian’s Perspective. Curr. Nutr. Rep. 2021, 10, 155–165. [Google Scholar] [CrossRef]
- Abu Hatab, A.; Krautscheid, L.; Boqvist, S. COVID-19, livestock systems and food security in developing countries: A systematic review of an emerging literature. Pathogens 2021, 10, 586. [Google Scholar] [CrossRef]
- Scarmozzino, F.; Visioli, F. COVID-19 and the subsequent lockdown modified dietary habits of almost half the population in an Italian sample. Foods 2020, 9, 675. [Google Scholar] [CrossRef]
- Mason, T.B.; Heron, K.E.; Braitman, A.L.; Lewis, R.J. A daily diary study of perceived social isolation, dietary restraint, and negative affect in binge eating. Appetite 2016, 97, 94–100. [Google Scholar] [CrossRef]
- Moynihan, A.B.; van Tilburg, W.A.P.; Igou, E.R.; Wisman, A.; Donnelly, A.E.; Mulcaire, J.B. Eaten up by boredom: Consuming food to escape awareness of the bored self. Front. Psychol. 2015, 6, 369. [Google Scholar] [CrossRef]
- Rolland, B.; Haesebaert, F.; Zante, E.; Benyamina, A.; Haesebaert, J.; Franck, N. Global changes and factors of increase in caloric/salty food intake, screen use, and substance use during the early COVID-19 containment phase in the general population in France: Survey study. JMIR Public Health Surveill. 2020, 6, e19630. [Google Scholar] [CrossRef]
- Rothman, A.J.; Sheeran, P.; Wood, W. Reflective and automatic processes in the initiation and maintenance of dietary change. Ann. Behav. Med. 2009, 38 (Suppl. 1), S4–S17. [Google Scholar] [CrossRef]
- Zupo, R.; Castellana, F.; Sardone, R.; Sila, A.; Giagulli, V.A.; Triggiani, V.; Cincione, R.I.; Giannelli, G.; De Pergola, G. Preliminary trajectories in dietary behaviors during the COVID-19 pandemic: A public health call to action to face obesity. Int. J. Environ. Res. Public Health 2020, 17, 7073. [Google Scholar] [CrossRef]
- Ruiz-Roso, M.B.; Padilha, P.d.C.; Mantilla-Escalante, D.C.; Ulloa, N.; Brun, P.; Acevedo-Correa, D.; Peres, W.A.F.; Martorell, M.; Aires, M.T.; Cardoso, L.d.O.; et al. Confinamiento del COVID-19 y cambios en las tendencias alimentarias de los adolescentes en Italia, España, Chile, Colombia y Brasil. Nutrients 2020, 12, 1807. [Google Scholar] [CrossRef]
- Laguna, L.; Fiszman, S.; Puerta, P.; Chaya, C.; Tárrega, A. The impact of COVID-19 lockdown on food priorities. Results from a preliminary study using social media and an online survey with Spanish consumers. Food Qual. Prefer. 2020, 86, 104028. [Google Scholar] [CrossRef]
- Sidor, A.; Rzymski, P. Dietary choices and habits during COVID-19 lockdown: Experience from Poland. Nutrients 2020, 12, 1657. [Google Scholar] [CrossRef] [PubMed]
- Di Renzo, L.; Gualtieri, P.; Cinelli, G.; Bigioni, G.; Soldati, L.; Attinà, A.; Bianco, F.F.; Caparello, G.; Camodeca, V.; Carrano, E.; et al. Psychological aspects and eating habits during COVID-19 home confinement: Results of ehlc-COVID-19 italian online survey. Nutrients 2020, 12, 2152. [Google Scholar] [CrossRef]
- Hutton, G.B.; Brugulat-panés, A.; Bhagtani, D.; Maadjhou, C.M. A Systematic Scoping Review of the Impacts of Community Food Production Initiatives in Kenya, Cameroon, and South Africa. J. Glob. Health Rep. 2021, 5, e2021010. [Google Scholar] [PubMed]
- Chew, H.S.J.; Lopez, V. Global impact of COVID-19 on weight and weight-related behaviors in the adult population: A scoping review. Int. J. Environ. Res. Public Health 2021, 18, 1876. [Google Scholar] [CrossRef] [PubMed]
- Neira, C.; Godinho, R.; Rincón, F.; Mardones, R.; Pedroso, J. Consequences of the COVID-19 syndemic for nutritional health: A systematic review. Nutrients 2021, 13, 1168. [Google Scholar] [CrossRef] [PubMed]
- Damayanthi, H.D.W.T.; Prabani, K.I.P. Nutritional determinants and COVID-19 outcomes of older patients with COVID-19: A systematic review. Arch. Gerontol. Geriatr. 2021, 95, 104411. [Google Scholar] [CrossRef]
- Huang, Y.; Yao, L.; Huang, Y.-M.; Wang, M.; Ling, W.; Sui, Y.; Zhao, H.-L. Obesity in patients with COVID-19: A systematic review and meta-analysis. Metab. Clin. Exp. 2020, 113, 154378. [Google Scholar] [CrossRef] [PubMed]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G.; Group, T.P. Preferred reporting items for systematic reviews and meta-analyses: The PRISMA statement. PLoS Med. 2009, 6, e1000097. [Google Scholar] [CrossRef] [Green Version]
- Higgins, J.P.T.; Green, S. Cochrane Handbook for Systematic Reviews of Interventions Version 5.1.0; The Cochrane Collaboration: London, UK, 2011; pp. 197–255. [Google Scholar]
- McHugh, M.L. Interrater reliability: The kappa statistic. Biochemia medica. Biochem. Medica 2012, 22, 276–282. [Google Scholar] [CrossRef]
- Khare, J.; Jindal, S. Observational study on Effect of Lock Down due to COVID 19 on glycemic control in patients with Diabetes: Experience from Central India. Diabetes Metab. Syndr. Clin. Res. Rev. 2020, 14, 1571–1574. [Google Scholar] [CrossRef]
- Munasinghe, S.; Sperandei, S.; Freebairn, L.; Conroy, E.; Jani, H.; Marjanovic, S.; Page, A. The Impact of Physical Distancing Policies During the COVID-19 Pandemic on Health and Well-Being Among Australian Adolescents. J. Adolesc. Health 2020, 67, 653–661. [Google Scholar] [CrossRef]
- Curtis, R.G.; Olds, T.; Ferguson, T.; Fraysse, F.; Dumuid, D.; Esterman, A.; Hendrie, G.A.; Brown, W.J.; Lagiseti, R.; Maher, C.A. Changes in diet, activity, weight, and wellbeing of parents during COVID-19 lockdown. PLoS ONE 2021, 16, e0248008. [Google Scholar] [CrossRef] [PubMed]
- Medrano, M.; Cadenas-Sanchez, C.; Oses, M.; Arenaza, L.; Amasene, M.; Labayen, I. Changes in lifestyle behaviours during the COVID-19 confinement in Spanish children: A longitudinal analysis from the MUGI project. Pediatr. Obes. 2021, 16, e12731. [Google Scholar] [CrossRef] [PubMed]
- Imaz-Aramburu, I.; Fraile-Bermúdez, A.B.; Martín-Gamboa, B.S.; Cepeda-Miguel, S.; Doncel-García, B.; Fernandez-Atutxa, A.; Irazusta, A.; Zarrazquin, I. Influence of the COVID-19 pandemic on the lifestyles of health sciences university students in spain: A longitudinal study. Nutrients 2021, 13, 1958. [Google Scholar] [CrossRef]
- Pietrobelli, A.; Pecoraro, L.; Ferruzzi, A.; Heo, M.; Faith, M.; Zoller, T.; Antoniazzi, F.; Piacentini, G.; Fearnbach, S.N.; Heymsfield, S.B. Effects of COVID-19 Lockdown on Lifestyle Behaviors in Children with Obesity Living in Verona, Italy: A Longitudinal Study. Obesity 2020, 28, 1382–1385. [Google Scholar] [CrossRef]
- Caruso, I.; Di Molfetta, S.; Guarini, F.; Giordano, F.; Cignarelli, A.; Natalicchio, A.; Perrini, S.; Leonardini, A.; Giorgino, F.; Laviola, L. Reduction of hypoglycaemia, lifestyle modifications and psychological distress during lockdown following SARS-CoV-2 outbreak in type 1 diabetes. Diabetes. Metab. Res. Rev. 2020, 37, e3404. [Google Scholar]
- Pellegrini, M.; Ponzo, V.; Rosato, R.; Scumaci, E.; Goitre, I.; Benso, A.; Belcastro, S.; Crespi, C.; De Michieli, F.; Ghigo, E.; et al. Changes in weight and nutritional habits in adults with obesity during the “lockdown” period caused by the COVID-19 virus emergency. Nutrients 2020, 12, 2016. [Google Scholar] [CrossRef]
- Segre, G.; Campi, R.; Scarpellini, F.; Clavenna, A.; Zanetti, M.; Cartabia, M.; Bonati, M. Interviewing children: The impact of the COVID-19 quarantine on children’s perceived psychological distress and changes in routine. BMC Pediatr. 2021, 21, 231. [Google Scholar] [CrossRef]
- Maffoni, S.; Brazzo, S.; De Giuseppe, R.; Biino, G.; Vietti, I.; Pallavicini, C.; Cena, H. Lifestyle changes and body mass index during COVID-19 pandemic lockdown: An Italian online-survey. Nutrients 2021, 13, 1117. [Google Scholar] [CrossRef] [PubMed]
- Martínez Steele, E.; Rauber, F.; dos Santos Costa, C.; Leite, M.A.; Gabe, K.T.; da Costa Louzada, M.L.; Levy, R.B.; Monteiro, C.A. Dietary changes in the NutriNet Brasil cohort during the COVID-19 pandemic. Rev. Saude Publica 2020, 54, 91. [Google Scholar] [CrossRef] [PubMed]
- Deschasaux-Tanguy, M.; Druesne-Pecollo, N.; Esseddik, Y.; De Edelenyi, F.S.; Allès, B.; Andreeva, V.A.; Baudry, J.; Charreire, H.; Deschamps, V.; Egnell, M.; et al. Diet and physical activity during the coronavirus disease 2019 (COVID-19) lockdown (March-May 2020): Results from the French NutriNet-Santé cohort study. Am. J. Clin. Nutr. 2021, 113, 924–938. [Google Scholar] [CrossRef] [PubMed]
- Zhang, J.; Zhao, A.; Ke, Y.; Huo, S.; Ma, Y.; Zhang, Y.; Ren, Z.; Li, Z.; Liu, K. Dietary behaviors in the post-lockdown period and its effects on dietary diversity: The second stage of a nutrition survey in a longitudinal chinese study in the COVID-19 era. Nutrients 2020, 12, 3269. [Google Scholar] [CrossRef] [PubMed]
- Yu, B.; Zhang, D.; Yu, W.; Luo, M.; Yang, S.; Jia, P. Impacts of lockdown on dietary patterns among youths in China: The COVID-19 Impact on Lifestyle Change Survey. Public Health Nutr. 2021, 24, 3221–3232. [Google Scholar] [CrossRef]
- Jia, P.; Liu, L.; Xie, X.; Yuan, C.; Chen, H.; Guo, B.; Zhou, J.; Yang, S. Changes in dietary patterns among youths in China during COVID-19 epidemic: The COVID-19 impact on lifestyle change survey (COINLICS). Appetite 2021, 158, 105015. [Google Scholar] [CrossRef]
- Dun, Y.; Ripley-Gonzalez, J.W.; Zhou, N.; You, B.; Li, Q.; Li, H.; Zhang, W.; Thomas, R.J.; Olson, T.P.; Liu, J.; et al. Weight gain in Chinese youth during a 4-month COVID-19 lockdown: A retrospective observational study. BMJ Open 2021, 11, e052451. [Google Scholar] [CrossRef]
- Barone Gibbs, B.; Kline, C.E.; Huber, K.A.; Paley, J.L.; Perera, S. COVID-19 shelter-at-home and work, lifestyle and well-being in desk workers. Occup. Med. 2021, 71, 86–94. [Google Scholar] [CrossRef]
- Lamarche, B.; Brassard, D.; Lapointe, A.; Laramée, C.; Kearney, M.; Côté, M.; Bélanger-Gravel, A.; Desroches, S.; Lemieux, S.; Plante, C. Changes in diet quality and food security among adults during the COVID-19-related early lockdown: Results from NutriQuébec. Am. J. Clin. Nutr. 2021, 113, 984–992. [Google Scholar] [CrossRef]
- Czenczek-Lewandowska, E.; Wyszyńska, J.; Leszczak, J.; Baran, J.; Weres, A.; Mazur, A.; Lewandowski, B. Health behaviours of young adults during the outbreak of the COVID-19 pandemic—A longitudinal study. BMC Public Health 2021, 21, 1038. [Google Scholar] [CrossRef] [PubMed]
- Naughton, F.; Ward, E.; Khondoker, M.; Belderson, P.; Marie Minihane, A.; Dainty, J.; Hanson, S.; Holland, R.; Brown, T.; Notley, C. Health behaviour change during the UK COVID-19 lockdown: Findings from the first wave of the C-19 health behaviour and well-being daily tracker study. Br. J. Health Psychol. 2021, 26, 624–643. [Google Scholar] [CrossRef] [PubMed]
- Herle, M.; Smith, A.D.; Bu, F.; Steptoe, A.; Fancourt, D. Trajectories of eating behavior during COVID-19 lockdown: Longitudinal analyses of 22,374 adults. Clin. Nutr. ESPEN 2021, 42, 158–165. [Google Scholar] [CrossRef]
- Hosomi, Y.; Munekawa, C.; Hashimoto, Y.; Okamura, T.; Takahashi, F.; Kawano, R.; Nakajima, H.; Majima, S.; Senmaru, T.; Nakanishi, N.; et al. The effect of COVID-19 pandemic on the lifestyle and glycemic control in patients with type 1 diabetes: A retrospective cohort study. Diabetol. Int. 2021, 1–6. [Google Scholar] [CrossRef]
- Sato, K.; Kobayashi, S.; Yamaguchi, M.; Sakata, R.; Sasaki, Y.; Murayama, C.; Kondo, N. Working from home and dietary changes during the COVID-19 pandemic: A longitudinal study of health app (CALO mama) users. Appetite 2021, 165, 105323. [Google Scholar] [CrossRef]
- Wells, G.; Brodsky, L.; O’Connell, D.; Shea, B.; Henry, D.; Mayank, S.; Tugwell, P. An evaluation of the Newcastle Ottawa Scale: An assessment tool for evaluating the quality of non-randomized studies. XI Cochrane Colloq. Evid. Health Care Cult. 2003, 26–31. Available online: https://cmr.cochrane.org/?CRGReportID=5100 (accessed on 1 October 2021).
- Lo, C.K.L.; Mertz, D.; Loeb, M. Newcastle-Ottawa Scale: Comparing reviewers’ to authors’ assessments. BMC Med. Res. Methodol. 2014, 14, 45. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Skotnicka, M.; Karwowska, K.; Kłobukowski, F.; Wasilewska, E.; Małgorzewicz, S. Dietary Habits before and during the COVID-19 Epidemic inSelected European Countries. Nutrients 2021, 1690, 1690. [Google Scholar] [CrossRef] [PubMed]
- Alsaffar, A.A. Sustainable diets: The interaction between food industry, nutrition, health and the environment. Food Sci. Technol. Int. 2016, 22, 102–111. [Google Scholar] [CrossRef]
- Mozaffarian, D.; Angell, S.Y.; Lang, T.; Rivera, J.A. Role of government policy in nutrition-barriers to and opportunities for healthier eating. BMJ 2018, 361, k2426. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Friel, S.; Hattersley, L.; Ford, L. Evidence Review: Addressing the Social Determinants of Inequities in Mental Wellbeing of Children and Adolescents; National Center for Epidemiology and Population Health: Canberra, ACT, Australia, 2013; Volume 62. [Google Scholar]
- Grosso, G.; Mateo, A.; Rangelov, N.; Buzeti, T.; Birt, C. Nutrition in the context of the Sustainable Development Goals. Eur. J. Public Health 2020, 30, I19–I23. [Google Scholar] [CrossRef] [PubMed]
- Meybeck, A.; Gitz, V. Conference on “Sustainable food consumption” Sustainable diets within sustainable food systems. Proc. Nutr. Soc. 2017, 76, 1–11. [Google Scholar] [CrossRef] [Green Version]
- Warren, J.M.; Smith, N.; Ashwell, M. A structured literature review on the role of mindfulness, mindful eating and intuitive eating in changing eating behaviours: Effectiveness and associated potential mechanisms. Nutr. Res. Rev. 2017, 30, 272–283. [Google Scholar] [CrossRef] [PubMed]
- Nelson, M.E.; Hamm, M.W.; Hu, F.B.; Abrams, S.A.; Griffin, T.S. Alignment of healthy dietary patterns and environmental sustainability: A systematic review. Adv. Nutr. 2016, 7, 1005–1025. [Google Scholar] [CrossRef] [Green Version]
- Drewnowski, A. Impact of nutrition interventions and dietary nutrient density on productivity in the workplace. Nutr. Rev. 2020, 78, 215–224. [Google Scholar] [CrossRef]
- Bérenger, V.; Verdier-Chouchane, A. Multidimensional Measures of Well-Being: Standard of Living and Quality of Life Across Countries. World Dev. 2007, 35, 1259–1276. [Google Scholar] [CrossRef]

{kind=link}
| Inclusion Criteria | Exclusion Criteria | |
|---|---|---|
| Participants | All participants | None |
| Outcome | Eating behaviour changes during the COVID-19 pandemic. | Those studies which do not assess pre/post-records of data among participants. |
| Type of study | Longitudinal studies (prospective and retrospective) | Cross-sectional studies, reviews, letters to the editor, recommendations. |
| Language | All languages | None |
| Setting | All settings | None |
| Search Strategy |
|---|
| ((((((“COVID-19”[MeSH Terms]) OR “coronavirus”[MeSH Terms]) OR “quarantine”[MeSH Terms]) OR “coronavirus pandemic”[Title/Abstract]”) OR 2019-nCov”[Title/Abstract]) OR “confinement”[Title/Abstract]) OR “lockdown”[Title/Abstract]) AND (((((((((“feeding behavior”[MeSH Terms]) OR “diet, healthy”[MeSH Terms]) OR “diet*” [MeSH Terms]) “Diet, Food, and Nutrition”[MeSH Terms]) OR “healthy eating”[Title/Abstract]) OR “diet*”[Title/Abstract]) OR “dietary pattern”[Title/Abstract]) OR “food intake”[Title/Abstract]) OR “nutrit*”[Title/Abstract]) OR “diet change”[Title/Abstract] AND ((cohort [Title/Abstract]) OR (longitudinal [Title/Abstract]) OR (follow-up [Title/Abstract]) OR (prospective [Title/Abstract]) OR (retrospective [Title/Abstract]) OR (observational [Title/Abstract])) |
| First Author/Year/ Region (Country) | Design (Study Type) | Length of Follow-Up (Weeks) | Target Population (Age) | Inclusion Criteria | Exclusion Criteria | Sample Size at Baseline (Total n/Female (%)) | Assessment Tool | Target Lifestyles | Sample Size at Follow-Up (Total n/Female (%)) | Statistical Technique/s |
|---|---|---|---|---|---|---|---|---|---|---|
| Khare, (2020) Bhopal (India) | PS | 3 weeks | Patients aged 18–65 years old with a diagnose of type 2 diabetes mellitus | Adult patients with previously diagnosed type 2 diabetes mellitus on treatment, and willing to participate in the study | Sick patient, patients with established microvascular or macrovascular complication of diabetes, pregnancy, and not willing to participate in the study | n = 143 Female = 36.36% (n = 52) | Questionnaire designed for this study | Diet, exercise, sleep, glycaemic control | n = 143 Female = 36.36% (n = 52) | Descriptive analysis (paired t-test) |
| Munasinghe, (2020) New South Wales (Australia) | PS | 22 weeks | Adolescents aged 13–19 years of a Sydney population catchment | (1) Age 13–19 years old (2) living in Sidney | No | n = 1298 Female = 80.5% (n = 1045) | Self-reported dietary behaviour was measured using questions validated for adolescents by the NSW Centre for Public Health Nutrition | Physical activity, sedentary behaviour, dietary behaviour, screen time | n = 582 Female = 79.89% (n = 465) | Multivariate multilevel mixed-effect logistic regression models |
| Medrano, (2020) All regions (Spain) | PS | 6 weeks | Spanish children aged 10–14 years old | Children and adolescents who were enrolled in a participating school were eligible for inclusion | Pupils with an intellectual or a physical disability that prevents response to the lifestyle questionnaires were initially excluded from the MUGI project | n = 291 Female = 47.8% (n = 139) | The Mediterranean Diet Quality Index for children and teenagers (KIDMED) | Physical activity, sleep, screen time and diet | n = 113 Female = 48.7% (n = 55) | (1) Dependent t-test (continuous variables) and (2) analysis of covariances (ANCOVA) |
| Pietrobelli, (2020) Verona (Italy) | RS | 11 weeks | Children and adolescents aged 6–18 years old | Children and adolescents with overweight and obesity | No | n = 41 Female = 46.34% (n = 19) | 12 items lifestyle questionnaire (sports activity participation, screen time, sleep behaviour, and eating habits, focusing on servings of red meat, pasta, snacks, fruits, and vegetables) | Physical activity, screen time, sleep behaviour and eating habits | n = 41 Female = 46.34% (n = 19) | (1) Descriptive statistics of the participant’s baseline, (2) paired t-tests, (3) correlation analysis, (4) independent two-sample t-tests |
| Caruso, (2020) Bari (Italy) | RS | 2 weeks before and 2 weeks after lockdown | People ≥18 years old with a diagnose of type 1 diabetes mellitus | Both males and females older than 18 years old diagnosed with diabetes mellitus type 1 for at least 1 year. Being on an intensive insulin regimen for at least 6 months and Having their glucose data uploaded to the Libreview platform | History of acute myocardial infarction, stroke and percutaneous or surgical revascularization within the last 30 days. (2) Active neoplasia within the last 6 months and (3) Any other concomitant medical or psychological condition | n = 48 Female = 47.9% (n = 23) | Changes in dietary habits were assessed on a semi-quantitative basis (higher/lower/same frequency) with an ad hoc questionnaire | Physical activity and diet | n = 48 Female = 47.9% (n = 23) | (1) Two-tailed paired Student’s t-test (2) Wilcoxon matched-pairs signed-rank test, and (3) chi-square test |
| Pellegrini, (2020) Nothern Italy (Italy) | RS | 4 weeks | Patients aged 18–75 years old | Patients of the Obesity Unit of the Diabetes and Metabolic Diseases Clinic of the Città dela Salute e della Scienza Hospital of Torino | Dropouts | n = 150 Female = 77.33% (n = 116) | A 12-question multiple-choice questionnaire | Physical activity and diet | n = 150 Female = 77.33% (n = 116) | (1) T-test for paired samples, (2) Mann-Whitney test (2 groups), (3) Kruskal-Wallis test (3 groups), (4) multiple regression model, and (6) regression path model |
| Martínez-Steele, (2020) All regions (Brazil) | PS | 15 weeks | People ≥18 years old | People older than 18 years old residing in Brazil | No | n = 10,116 Female = 78% (n = 7895) | A simplified questionnaire about diet | Diet | n = 10,116 Female = 78% (n = 7895) | (1) Chi square, and (2) t-test |
| Deschasaux-Tanguy. (2020) All regions (France) | PS | 24 weeks | French people ≥18 years old | Adults aged ≥18 years old living in France | No | n = 37,252 Female = 52.3% (n = 19.483) | Web-based 24-h dietary records | Food-related practices, physical activity, and body weight | n = 37,252 Female = 52.3% (n = 19.483) | (1) The Alternative Healthy Eating Index (AHEI)-2010 score, (2) NOVA classification, (3) multiple correspondence analysis, (4) ANCOVA models for variations in continuous variables, and (5) multivariable logistic regression models |
| Zhang (2020) All regions (China) | RS | 20 weeks | Adults living in China aged 18–80 years old | Adults 18–80 years old living in mainland China | No | n = 1994 Female = 62.79% (n = 1252) | (1) A standardized survey, (2) the Household Dietary Diversity Score (HDDS), and (3) a series of questions regarding changes in dietary behaviours | Diet | n = 1994 Female = 62.79% (n = 1252) | (1) Univariate analysis, (2) A linear regression model, (3) K-means clustering analysis, and (4) Multivariable analysis |
| Yu. (2020) All regions (China) | RS | 4 weeks | People from China aged 17–22 years old | Youth people under three educational attachments (i.e., high school, college or graduate) in China | No | n = 10,082 Female = 72.39% (n = 7298) | COVID-19 Impact on Lifestyle Change Survey (COINLICS) | Diet | n = 10,082 Female = 72.39% (n = 7298) | (1) Descriptive statistics to summarise characteristics of participants, (2) Pair t-test to compare the differences in frequency of food and beverage consumption, and (3) A factor analysis with orthogonal rotation to derive main dietary patterns before-after the pandemic |
| Barone, (2021) Pennsylvania (USA) | PS | 54 weeks | Desk workers ≥18 years old | Participants in the RESET BP trial | No | n = 112 Female = 69% (n = 77) | Diet Screener Questionnaire | Sedentary behaviour, physical activity, sleep quality, and diet | n = 112 Female = 69% (n = 77) | (1) Paired samples, (2) McNemar tests, and (3) Bowker’s tests |
| Curtis, (2021) Adelaide (Australia) | PS | 54 weeks | Healthy adults aged 18–65 years old | Adults residing in greater metropolitan Adelaide, having access to a Bluetooth-enabled mobile device or computer and home internet, proficiency in English, and ambulant | Pregnancy, having an implanted electronical medical device, or experiencing or receiving treatment for any life-threatening condition impacting daily lifestyle and health | n = 61 Female = 65.6% (n = 40) | Dietary Questionnaire for Epidemiological Studies (DQUES and diet v3.2; Cancer Council Victoria) | Physical activity, and diet | n = 61 Female = 65.6% (n = 40) | Mixed effects models |
| Jia, (2021) All regions (China) | RS | 20 weeks | Chinese youth aged 15–28 years old | No | No | n = 10,082 female = 71.7% (n = 7320) | (1) Food frequency questionnaire, and (2) Beverages Diet frequency questionnaire | Diet | n = 10,082 Female = 71.7% (n = 7320) | (1) Chi square, and (2) T-test |
| Lamarche, (2021) Quebec (Canada) | PS | 20 weeks | Adults living in Quebec ≥18 years old | Adults aged ≥18 years old with a residential address in the province of Quebec | Not being able to read and understand French or English. Not having access to the Internet (with a phone, tablet or computer), and not having an active email address. Living outside of the province of Quebec | n = 853 female = 87.2% (n = 744) | Self-administered web-based 24-h time dietary recall | Smoking, screen time, physical activity, and diet | n = 853 Female = 87.2% (n = 744) | Linear mixed regression models |
| Czenczek-Lewandowska. (2021) South-east Poland (Poland) | RS | 5 weeks | Polish people in early adulthood aged 18–34 years old | People aged from 18 to 34 years of Polish nationality resident in south-east Poland throughout the pandemic period | No | n = 506 Female = 70.2% (n = 355) | The modified Food Frequency Questionnaire (FFQ-6) | Diet, physical activity and sedentary behaviour, and sleep quality | n = 506 Female = 70.2% (n = 355) | |
| Naughton. (2021) High deprivation areas of all regions (United Kigndom) | PS | 12 weeks | Adult-vulnerable people from the United Kingdom ≥18 years old | Adults living in the United Kingdom. Those with a physical high-risk health condition for COVID-19 (in line with the UK National Health Service definitions), those living in a high deprivation area, and those with a self-reported mental health issue. | People without access to a smartphone | n = 1044 Female = 72.7% (n = 747) * Other = 0.2% (n = 2) | (1) An online survey, and (2) Daily health behaviour monitoring | Diet, physical activity, alcohol, smoking and vaping, and substance use behaviours | n = 1044 Female = 72.7% (n = 747) * Other = 0.2% (n = 2) | (1) Descriptive analyses for all health behaviour measures, (2) Multivariable regression models, and (3) Covariates |
| Imaz-Aramburu. (2021) Basque Country (Spain) | PS | 48 weeks | Students from Spain ≥19 years old | Nursing and medical students at the beginning of the second year of their degree and a physiotherapy student at the beginning of the third year at the Faculty of Medicine and Nursing, University of the Basque Country, Spain | No | n = 267 Female = 76% (n = 203) | (1) An ad hoc self-administered questionnaire, (2) the Mediterranean diet (MedDiet) questionnaire | Diet, and physical activity | n = 267 Female = 76% (n = 203) | (1) Kolmogorov–Smirnov test, (2) a Wilcoxon signed-rank test to analyze the difference between MedDiet scores, moderate and intense physical activity, and eating habits, (3) Paired t-tests, and (4) a McNemar test to compare proportions between adherence to the Mediterranean Diet and physical activity frequency |
| Segre. (2021) Milan (Italy) | RS | 3 weeks | Italian children and adolescents aged 6–14 years old | Primary or middle school students living in Milan | Not being able to attend Zoom Meetings | n = 82 Female = 46.3% (n = 38) | 10–20 min-structured interviews | Distance learning, eating, and sleeping habits | n = 82 Female = 46.3% (n = 38) | Chi-square and Fisher’s exact test. |
| Maffoni. (2021) All regions (Italy) | RS | 2 weeks | Italian people ≥18 years old | Adults >18 years residing in Italy | No | n = 1304 Female = 74.62% (n = 973) | (1) A 38 multiple-choice web-form survey in Google Forms, and (2) 10 multiple-choice items | Water intake, alcohol consumption, physical activity, diet | n = 1304 Female = 74.62% (n = 973) | (1) T-test, and (2) Multiple Regression Analyses |
| Hosomi. (2021) Kyoto (Japan) | RS | 2 weeks | Patients diagnosed with Type 1 Diabetes Mellitus, aged 16–75 years old | Patients with Type 1 Diabetes Mellitus who visited the Department of Endocrinology and Metabolism of the Kyoto Prefectural University of Medicine | Patients with missing data | n = 34 Female = 67.65% (n = 23) | A self-administered questionnaire related to stress and lifestyle factors | Stress levels, sleep time, exercise intensity levels, total diet, snack, and prepared food intake. | n = 34 Female = 67.65% (n = 23) | (1) Descriptive analyses, (2) Spearman’s correlation, (3) and Pair t-test to evaluate differences before and after the pandemic |
| Herle. (2021) All regions (United Kingdom) | PS | 5 weeks | Adults ≥18 years old | Adults living in the UK during the COVID-19 pandemic | No | n = 22,374 Female = 76% (n = 16,984) | Self-reported eating changes | Eating behaviour, mental health, physical health and body weight | n = 22,374 Female = 76% (n = 16,984) | (1) Descriptive statistics, and (2) Latent class growth analysis to derive trajectories of change in eating across lockdown |
| Dun. (2021) Zhejiang and Hunan (China) | RS | 3 weeks | Chinese students aged 17–27 years old | Students from Hunan Traditional Chinese Medical College (Hunan, China) and from the Medical College of Jinhua Polytechnic (Zhejiang, China) who were free of chronic diseases and had measured body weight at the universities before the lockdown | No | n = 12,889 Female = 80.22% (n = 10,340) | An 81-item-online follow-up questionnaire | Perceptions of COVID-19, physical activity, sedentary time, meal frequency, alcohol consumption, and mental health | n = 12,889 Female = 80.22% (n = 10,340) | (1) Paired t-test and Wilcoxon signed-rank test, (2) A baseline body weight-adjusted linear regression for associations with dietary habits, and (3) A multivariate linear regression |
| Sato. (2021) All regions (Japan) | PS | 19 weeks | Adults ≥18 years old | Adults living in Japan | No | n = 5929 Female = 69% (n = 4087) | CALO mama health app | Diet and physical activity | n = 5929 Female = 69% (n = 4087) | (1) Generalized linear mixed models, (2) A Poisson distribution was to the count of intake of the food groups, and (3) A negative binomial distribution was to the count of drinking alcohol |
| Authors | Objective | Outcome | Results |
|---|---|---|---|
| Khare et al. (2020) | To study the effect of lockdown on glycaemic control in diabetic patients and possible factors responsible for this | Dietary changes (secondary outcome) | Dietary changes were observed as a change in the type of diet, change in timing of meals, change in frequency of meals and change in the amount of diet. |
| Munasinghe et al. (2020) | To investigate changes in physical activity, dietary behaviours, and well-being during the early period of physical distancing policies | Dietary behaviour (primary outcome) | There were declines in fast food consumption following implementation of physical distancing but no substantial changes in fruit and vegetable consumption. |
| Medrano et al. (2020) | To examine the effects of the COVID-19 confinement on lifestyle behaviours and to assess the influence of social vulnerabilities on changes in lifestyle behaviours | Adherence to the Mediterranean Diet (primary outcome) | Children worsened their lifestyle behaviours during the COVID-19 confinement, specifically their adherence to the Mediterranean Diet. No significant differences were found behaviours between primary and secondary students. |
| Pietrobelli et al. (2020) | To test the hypothesis that factors contributing to weight gain among children and adolescents with overweight and obesity are exacerbated during a pandemic associated lockdown | (1) Number of meals eaten per day, (2) changes in vegetable and fruit intake (3) potato chips intake, (4) red meat intake and (5) sugary drinks (primary outcomes) | The number of meals eaten per day got increased. There were no changes in vegetable intake, and fruit intake increased. There was an increased consumptions of potato chips, red meat, and sugary drinks during the lockdown. |
| Caruso et al. (2020) | To assess lockdown-related changes in glucose control and variability and their association with psychological distress and lifestyle changes in type 1 diabetes mellitus patients | (1) Meals per day, (2) starchy foods, (3) sweets, (4) whole grains and (5) vegetables (secondary outcomes) | Patients increased the frequency of starchy foods and sweets consumption, respectively. |
| Pellegrini et al. (2020) | To evaluate the changes in weight and dietary habits in a sample of individuals with obesity after 1 month of enforced lockdown | Changes in dietary habits (primary outcome) | There was an increased consumption of snacks, cereals, and sweets. |
| Martínez-Steele et al. (2020) | To describe the dietary characteristic of a cohort immediately before and during the pandemic | Changes in dietary characteristics (primary outcome) | The consumption of vegetables, fruits and legumes increased on daily diet. There was a pattern of stability in the consumption of ultra-processed food, although the number of people who consumed it increased. |
| Deschasaux-Tanguy. (2020) | To explore potential changes in dietary intake, physical activity, body weight and food supply during the COVID-19 lockdown and how these differed according to individual characteristics | Determinants of nutrition-related behaviour (primary outcome) | Diet-related practices during COVID-19 lockdown were modified. Trouble to keep a regular mealtime schedule, more frequent snaking (at least 3 times a day, every day) and a decreased consumption of fresh food was reported. Ultra-processed food consumption increased. |
| Zhang. (2020) | To explore post-lockdown dietary behaviours and their effects on dietary diversity. | Dietary behaviour (primary outcome) | An increased consumption of seafood and dietary supplements was found. Also, frozen food and raw food consumption decreased, whereas a higher alcohol and vinegar intake was registered. |
| Yu. (2020) | To assess changes in dietary patterns among youths in China after COVID-19 lockdown | Dietary patterns (primary outcome) | Significant changes in the weekly frequency of major food intake after lockdown was reported. There was a decrease in rice intake while an increase consumption of other staple food such as fish, eggs, fresh vegetables, preserved vegetables, fresh fruit and dairy products was recorded. There was an increased consumption of wheat products and a decrease in the frequency of beverages intake. |
| Barone. (2021) | To study the longitudinal impact of COVID-19 on work practices, lifestyle and well-being among desk workers during COVID-19 lockdown | Dietary habits (primary outcome) | No changes in dietary habits were found, except for a reduced frequency of red meat consumption. |
| Curtis. (2021) | To examine changes in activity patterns, recreational physical activities, diet, weight and wellbeing from before to during COVID-19 restrictions | Dietary intake (primary outcome) | Total energy intake did not change, but a slightly lower percentage of energy from protein and a greater percentage of energy from alcohol were recorded. |
| Jia. (2021) | To measure changes in diet patterns during the COVID-19 lockdown among youths in China | Diet patterns (primary outcome) | Significant changes in diet patterns associated with more frequent consumption of wheat products, other staple foods, preserved vegetables, and tea and less frequent consumption of rice, meat, poultry, fresh vegetables and fruit, soybean and dairy products and sugar-sweetened beverages were found. |
| Lamarche. (2021) | To document the change in diet quality and in food insecurity observed during the COVID-19–related early lockdown | Diet quality (primary outcome) | There were small but significant increases in the following components: whole grains, greens and beans, refined grains (reduced consumption), total vegetables, total dairy, seafood and plant proteins, added sugar (reduced consumption), and total proteins. The overall diet quality slightly improved. |
| Czenczek-Lewandowska. (2021) | To assess whether and to what extent the outbreak of the COVID-19 pandemic influenced the health-promoting behaviours of young adults in terms of eating habits, physical activity, sedentary behaviours and sleep. | Eating habits (primary outcome) | Average consumption of sweets, snacks, cereal products increased. A significant higher intake of alcohol and fats was recorded. |
| Naughton. (2021) | To provide baseline cohort descriptives and assess change in health behaviours since the UK COVID-19 lockdown | Dietary behaviour (primary outcome) | There were reductions in the mean reported number of daily portions of vegetables and fruit but no change in reported portions of high sugar food consumed. In the case of alcohol consumption, there was an increase in the average intake per month. |
| Imaz-Aramburu. (2021) | To understand the influence that the pandemic exerted on the lifestyles of university students, in particular those enrolled in health sciences programs | Eating habits (secondary outcome) | There was a greater adherence to the Mediterranean Diet. The consumption of vegetables increased significantly during the pandemic whereas the consumption of fatty meats tended to increase. An increased consumption of nuts was recorded. |
| Segre. (2021) | To analyse the impact of the quarantine on students’ life in Milan, one of the Italian cities most affected by COVID-19 | Eating habits (primary outcome) | The amount of food eaten increased, with a higher consumption of junk food, snacks and sweets. |
| Maffoni. (2021) | To investigate lifestyle habits and eating behaviours modifications in a sample of Italian adults during “Phase 1” COVID-19 pandemic home confinement | Eating behaviours (primary outcome) | Negative changes in eating behaviour were found. These included an increased consumption of desserts or sweets at lunch. Craving or eating between meals was reported as well as the higher consumption of unhealthy snacks, beverages and ultra-processed food. |
| Hosomi. (2021) | To investigate the effects of the COVID-19 pandemic on the glycaemic control and changes in stress levels and lifestyle in patients with T1D. | Diet (primary outcome) | Average amount of food intake got increased. The consumption of snacks and prepared food were also considerably increased. |
| Herle. (2021) | To describe how people’s eating behaviour (eating more, eating less, eating the same) changed over 8 weeks of lockdown in the UK | Eating behaviour (primary outcome) | Many individuals did experience changes to their food intake as well as lower adherence to healthy eating patterns |
| Dun. (2021) | To observe weight change in Chinese youth during a 4-month lockdown and the associations between weight change and COVID-19-related stress, anxiety, depression, physical activity, sedentary time and dietary habits. | Dietary habits (secondary outcome) | A higher alcohol consumption was found in particular among men. Daily snack frequency also increased. |
| Sato. (2021) | To study dietary changes during the pandemic while considering changes in work and life patterns | Dietary changes (primary outcome) | Working people tended to consume less fruits and dairy products but more meats and alcohol compared with non-workers. In particular, irregular workers consumed less vegetables, mushrooms and fish. The average daily number of self-made meals increased among all participants. |
| Study ID | Selection | Comparability | Outcome | Total | Score | |||||
|---|---|---|---|---|---|---|---|---|---|---|
| Representativeness of the Exposed Cohort | Selection of the Non-Exposed Cohort | Ascertainment of Exposure | Demonstration That the Outcome of Interest Was Not Present at the Start of the Study | Comparability of Cohorts on the Basis of the Design or Analysis | Assessment of Outcome | Was Follow-Up Long Enough for Outcomes to Occur | Adequacy of the Follow-Up | |||
| Khare et al. (2020) | ☆ | ☆ | ☆ | ☆ | ☆☆ | ☆ | ☆ | ☆ | 9 | Low risk of bias |
| Munasinghe et al. (2020) | ☆ | ☆ | ☆ | ☆ | ☆ | ☆ | ☆ | 7 | Low risk of bias | |
| Caruso et al. (2020) | ☆ | ☆ | ☆ | ☆ | ☆☆ | ☆ ☆ | ☆ | 9 | Low risk of bias | |
| Medrano et al. (2020) | ☆ | ☆ | ☆ | ☆ | ☆ | ☆ ☆ | ☆ | ☆ | 9 | Low risk of bias |
| Pietrobelli et al. (2020) | ☆ | ☆ | ☆ | ☆ | ☆ | ☆ | ☆ | 7 | Low risk of bias | |
| Pellegrini et al. (2020) | ☆ | ☆ | ☆ | ☆ | ☆ | ☆ | ☆ | ☆ | 8 | Low risk of bias |
| Martínez-Steele et al. (2020) | ☆ | ☆ | ☆ | ☆ | ☆ | ☆ | ☆ | ☆ | 8 | Low risk of bias |
| Deschasaux-Tanguy et al. (2020) | ☆ | ☆ | ☆ | ☆ | ☆ | ☆ | ☆ | 7 | Low risk of bias | |
| Zhang et al. (2020) | ☆ | ☆ | ☆ | ☆ | ☆ | ☆ ☆ | ☆ | ☆ | 9 | Low risk of bias |
| Yu et al. (2020) | ☆ | ☆ | ☆ | ☆ | ☆ | ☆ | ☆ | 7 | Low risk of bias | |
| Barone et al. (2021) | ☆ | ☆ | ☆ | ☆ | ☆ | ☆ ☆ | ☆ | 8 | Low risk of bias | |
| Curtis et al. (2021) | ☆ | ☆ | ☆ | ☆ | ☆ ☆ | ☆ | ☆ | 8 | Low risk of bias | |
| Jia et al. (2021) | ☆ | ☆ | ☆ | ☆ ☆ | ☆ | ☆ | 7 | Low risk of bias | ||
| Lamarche et al. (2021) | ☆ | ☆ | ☆ | ☆ | ☆ | ☆ ☆ | ☆ | ☆ | 9 | Low risk of bias |
| Czenczek-Lewandowska et al. (2021) | ☆ | ☆ | ☆ | ☆ | ☆ | ☆ | ☆ | 7 | Low risk of bias | |
| Naughton et al. (2021) | ☆ | ☆ | ☆ | ☆ | ☆ | ☆ ☆ | ☆ | ☆ | 9 | Low risk of bias |
| Imaz-Aramburu et al. (2021) | ☆ | ☆ | ☆ | ☆ | ☆ ☆ | ☆ | ☆ | 8 | Low risk of bias | |
| Segre et al. (2021) | ☆ | ☆ | ☆ | ☆ | ☆ | ☆ | ☆ | 7 | Low risk of bias | |
| Maffoni et al. (2021) | ☆ | ☆ | ☆ | ☆ | ☆ | ☆ | ☆ | 7 | Low risk of bias | |
| Hosomi et al. (2021) | ☆ | ☆ | ☆ | ☆ | ☆ | ☆ | ☆ | 7 | Low risk of bias | |
| Herle et al. (2021) | ☆ | ☆ | ☆ | ☆ | ☆ | ☆ | ☆ | 7 | Low risk of bias | |
| Dun et al. (2021) | ☆ | ☆ | ☆ | ☆ | ☆ | ☆ | ☆ | 7 | Low risk of bias | |
| Sato et al. (2021) | ☆ | ☆ | ☆ | ☆ | ☆ ☆ | ☆ | ☆ | 8 | Low risk of bias | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
González-Monroy, C.; Gómez-Gómez, I.; Olarte-Sánchez, C.M.; Motrico, E. Eating Behaviour Changes during the COVID-19 Pandemic: A Systematic Review of Longitudinal Studies. Int. J. Environ. Res. Public Health 2021, 18, 11130. https://doi.org/10.3390/ijerph182111130
González-Monroy C, Gómez-Gómez I, Olarte-Sánchez CM, Motrico E. Eating Behaviour Changes during the COVID-19 Pandemic: A Systematic Review of Longitudinal Studies. International Journal of Environmental Research and Public Health. 2021; 18(21):11130. https://doi.org/10.3390/ijerph182111130
Chicago/Turabian StyleGonzález-Monroy, Cristina, Irene Gómez-Gómez, Cristian M. Olarte-Sánchez, and Emma Motrico. 2021. "Eating Behaviour Changes during the COVID-19 Pandemic: A Systematic Review of Longitudinal Studies" International Journal of Environmental Research and Public Health 18, no. 21: 11130. https://doi.org/10.3390/ijerph182111130
APA StyleGonzález-Monroy, C., Gómez-Gómez, I., Olarte-Sánchez, C. M., & Motrico, E. (2021). Eating Behaviour Changes during the COVID-19 Pandemic: A Systematic Review of Longitudinal Studies. International Journal of Environmental Research and Public Health, 18(21), 11130. https://doi.org/10.3390/ijerph182111130