
Meta-Analysis of the Association between Asbestos Exposure and Esophageal Cancer


 , ,
, ,
Abstract
1. Introduction
2. Materials and Methods
2.1. Protocol and Registration
2.2. Data Sources and Search Terms
2.3. Eligibility Criteria
2.4. Study Selection Process
2.5. Data Collection
2.6. Study Characteristics
2.7. Asbestos Exposure
2.8. Esophageal Cancer
2.9. Statistical Analysis
3. Results
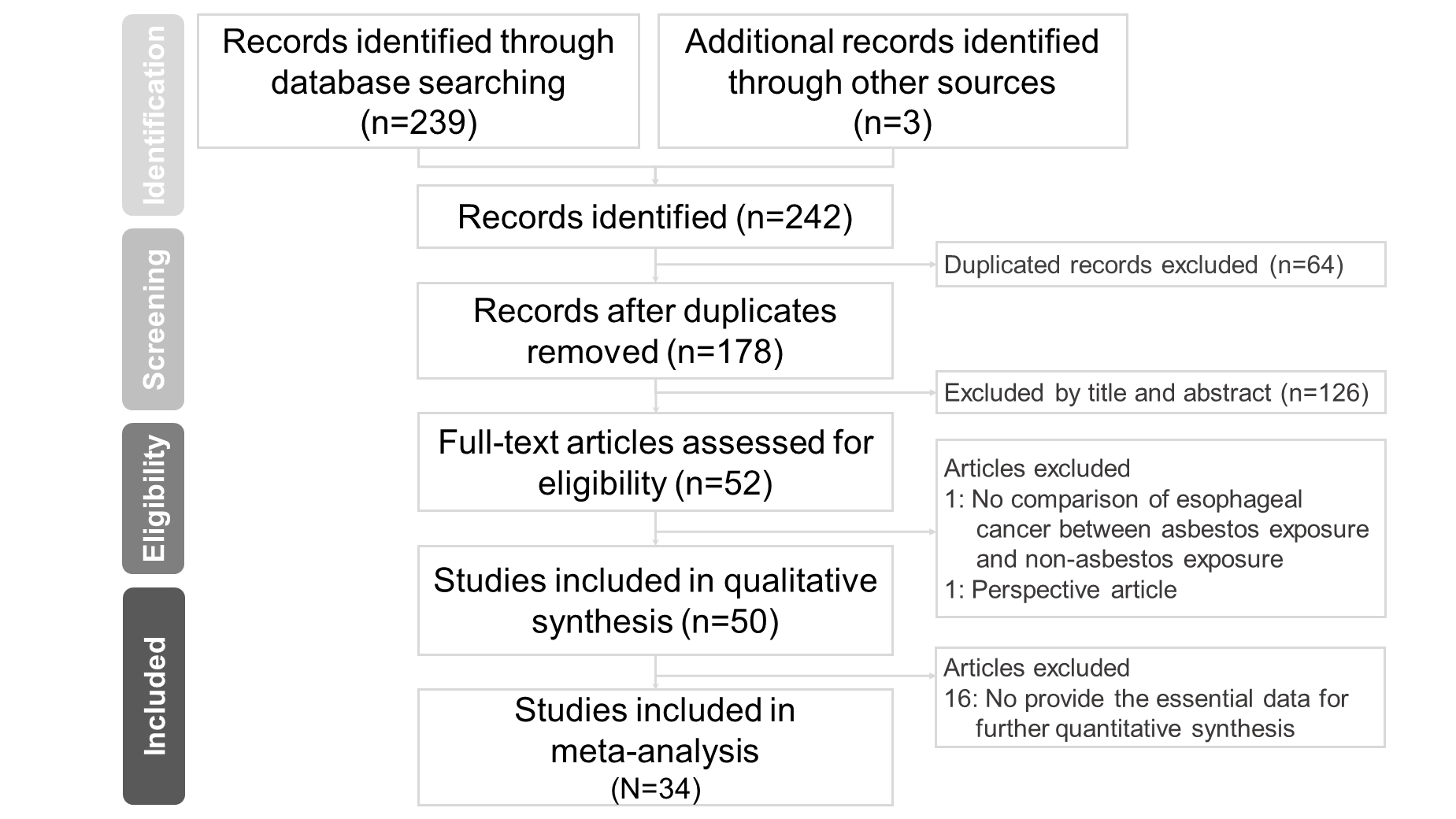
3.1. Selected Studies
3.2. Study Characteristics
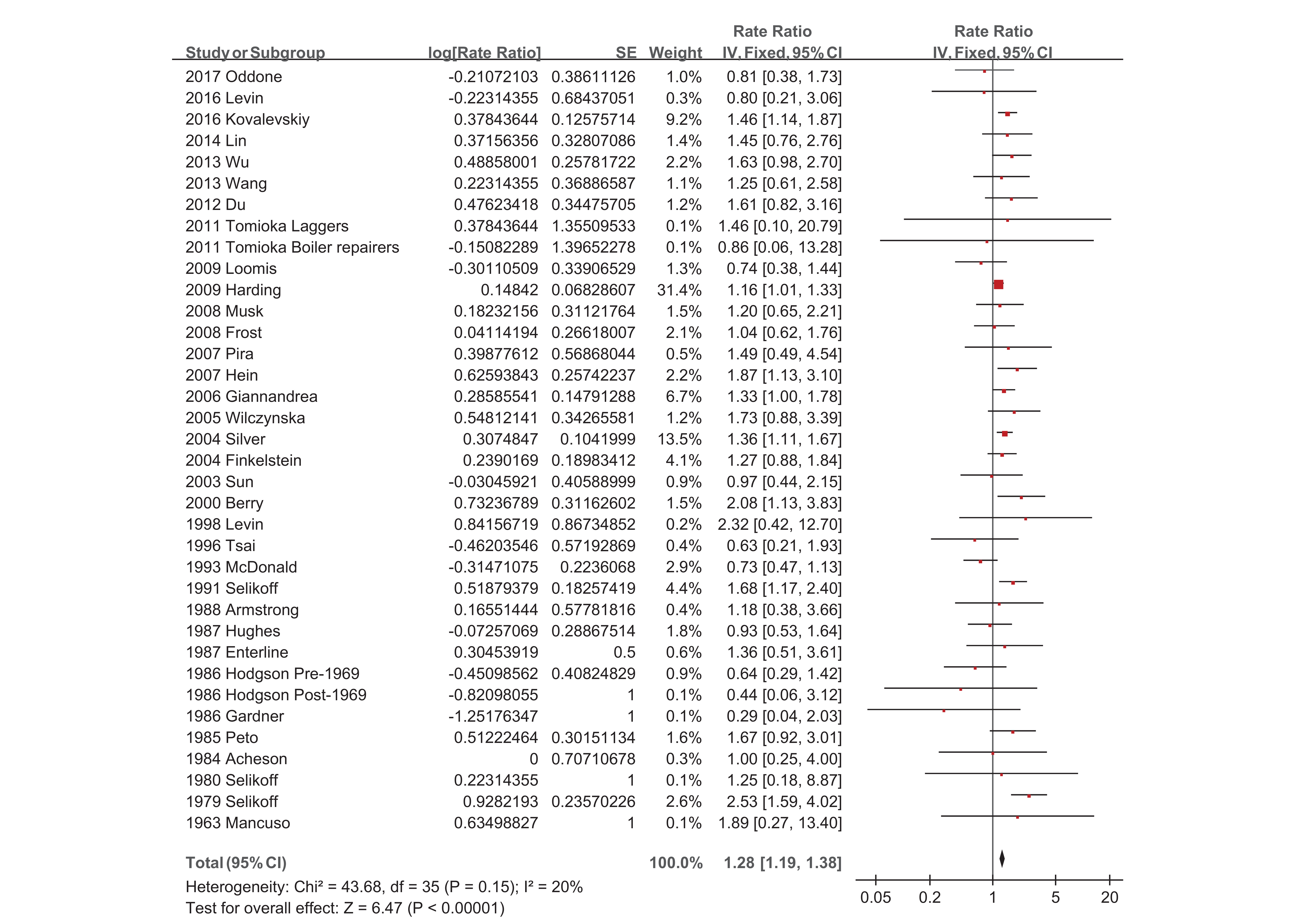
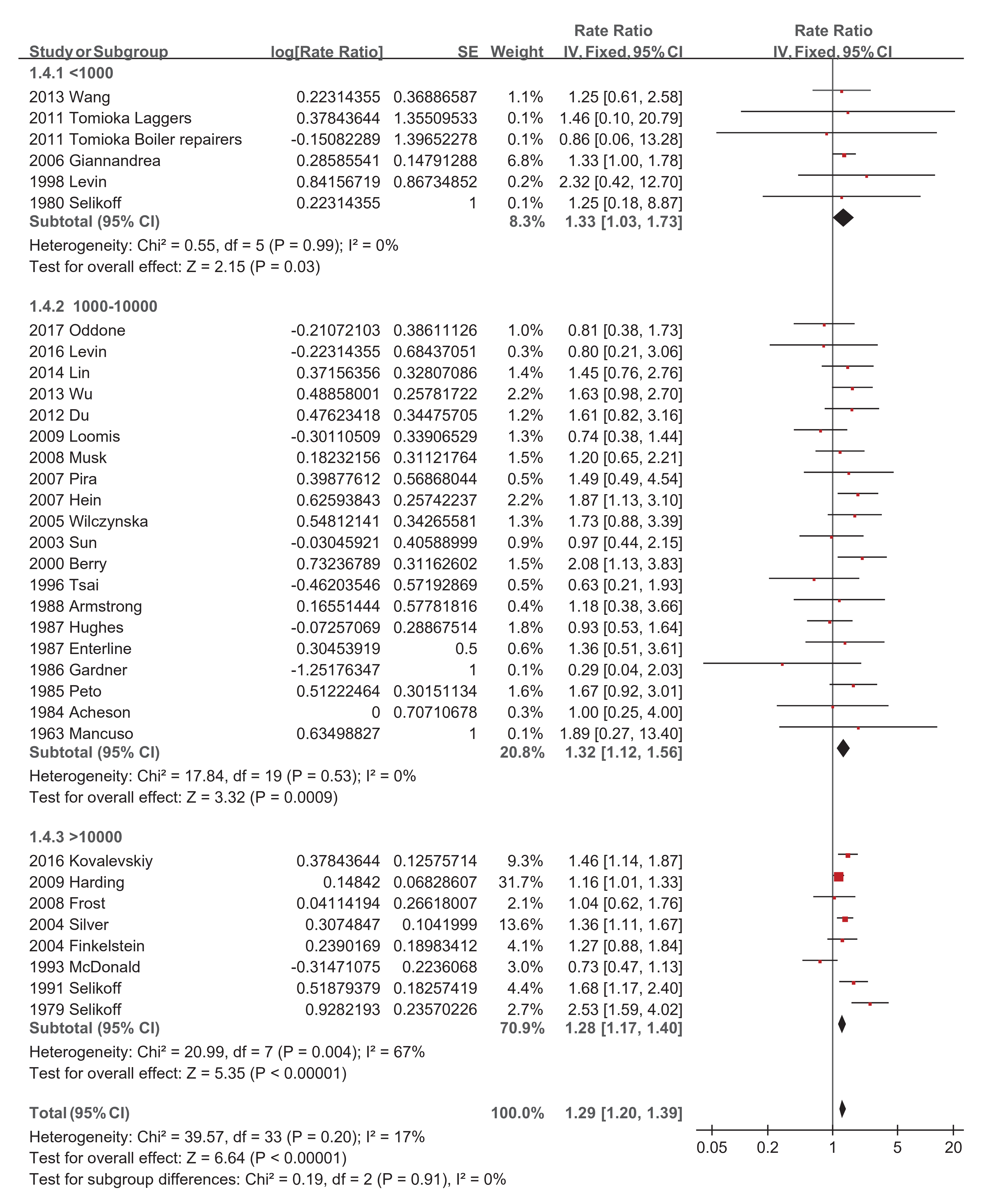
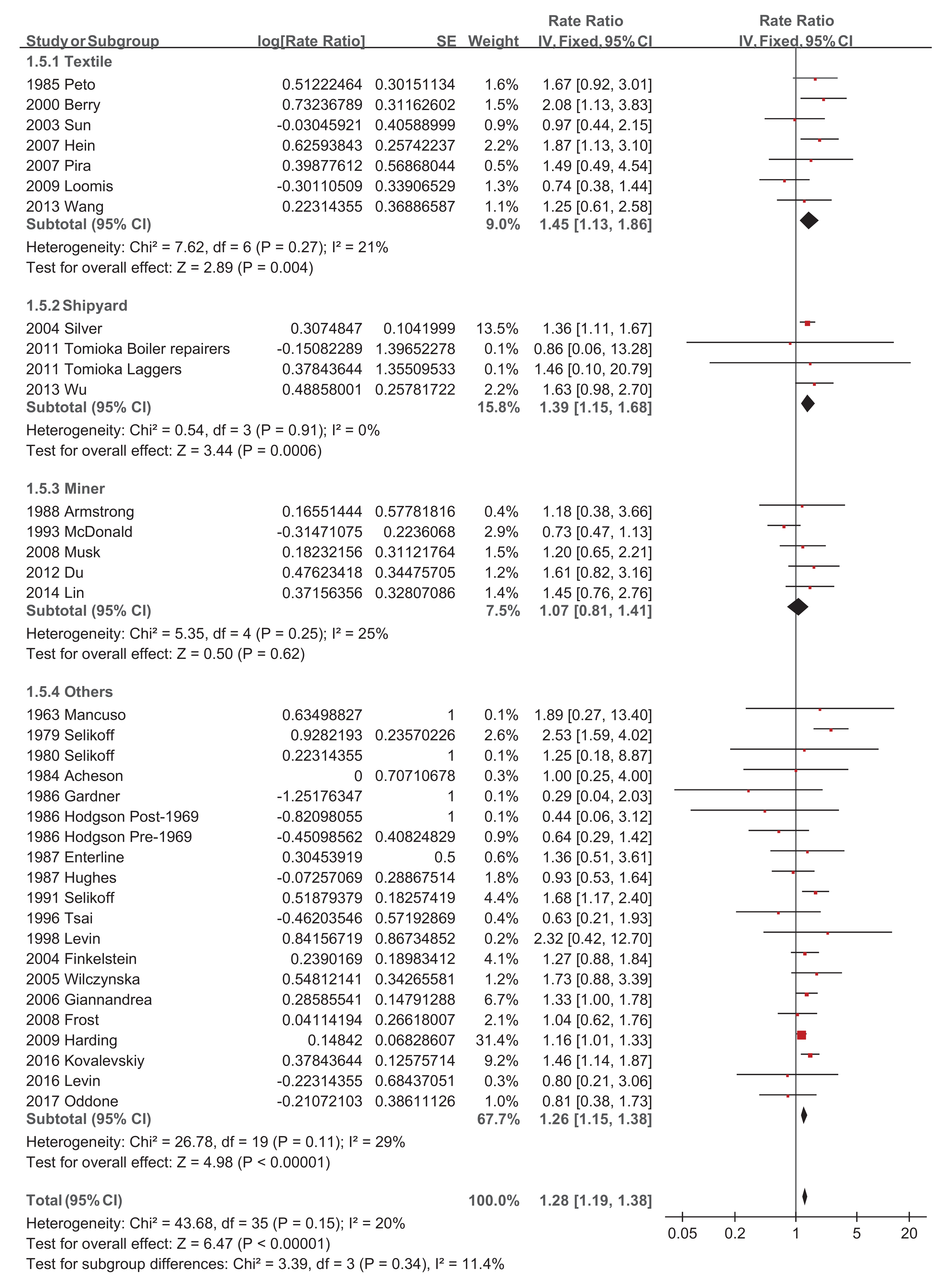
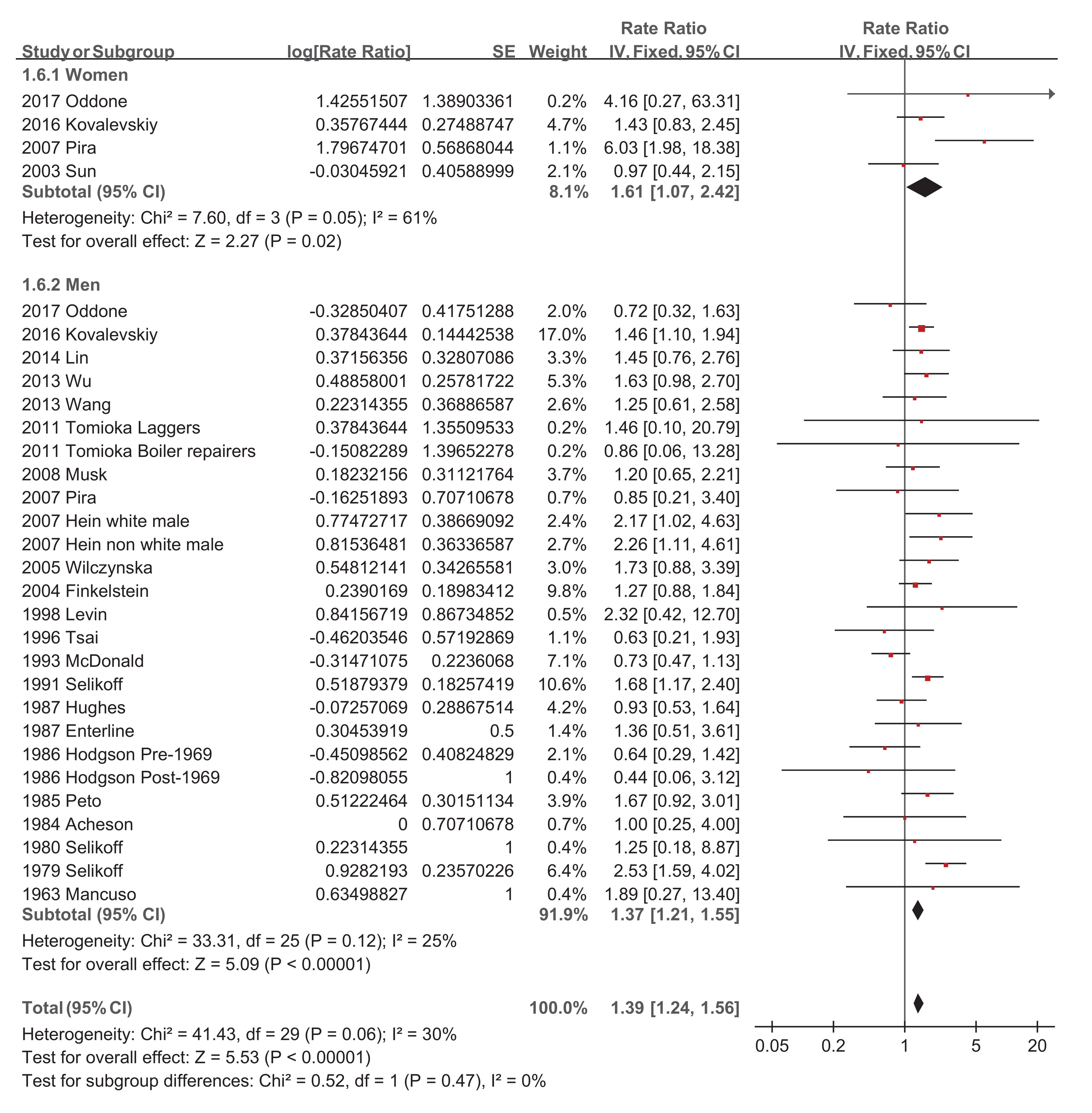
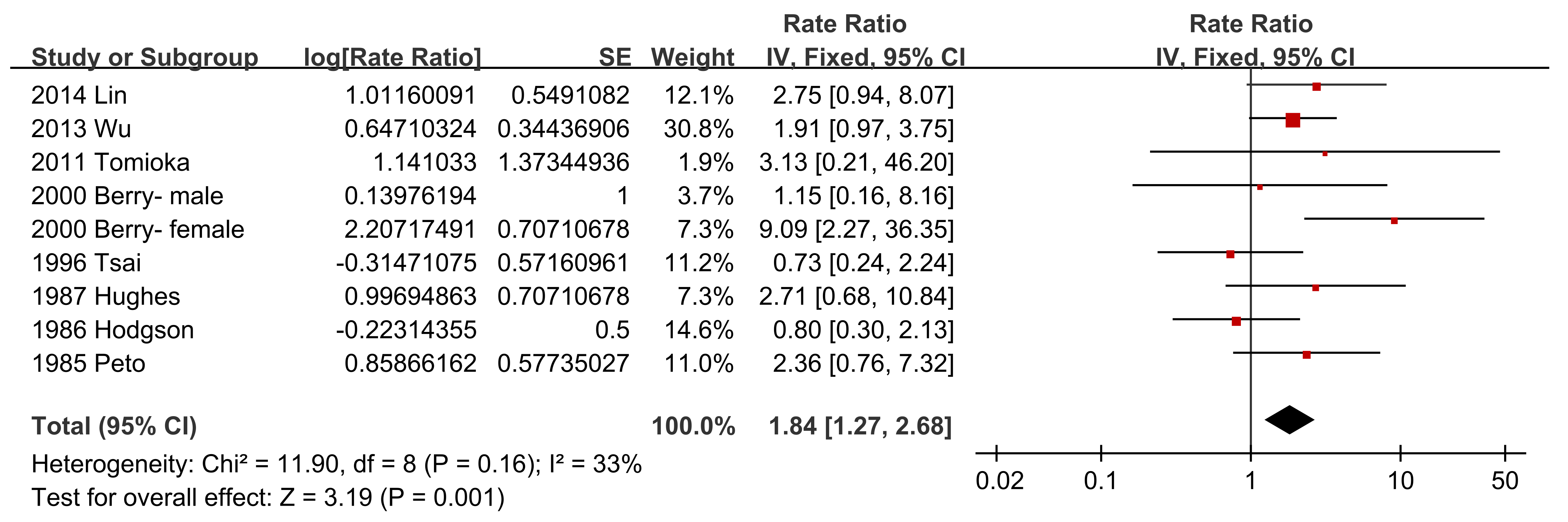
3.3. Meta-Analysis
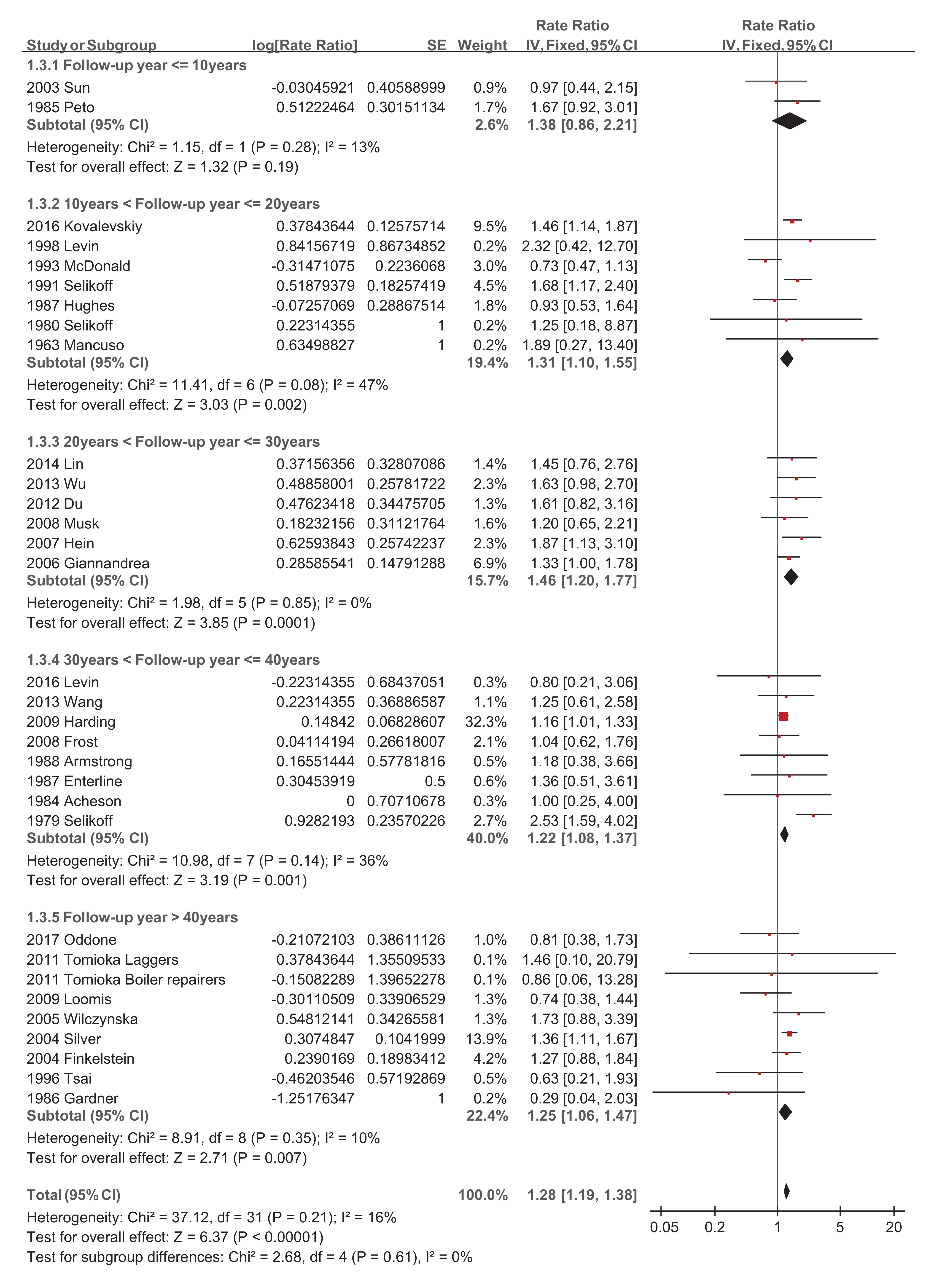
3.4. Subgroup Analysis
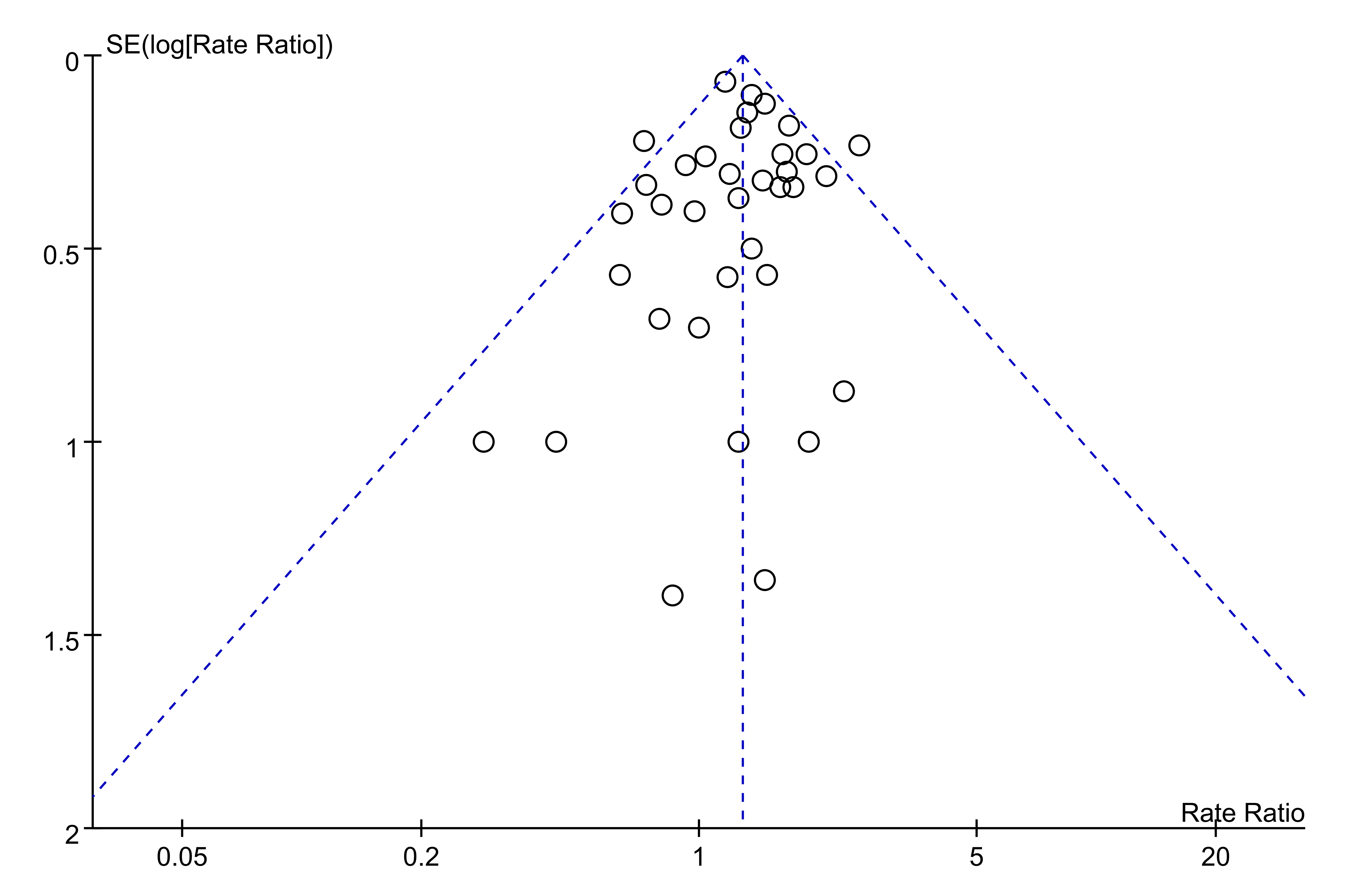
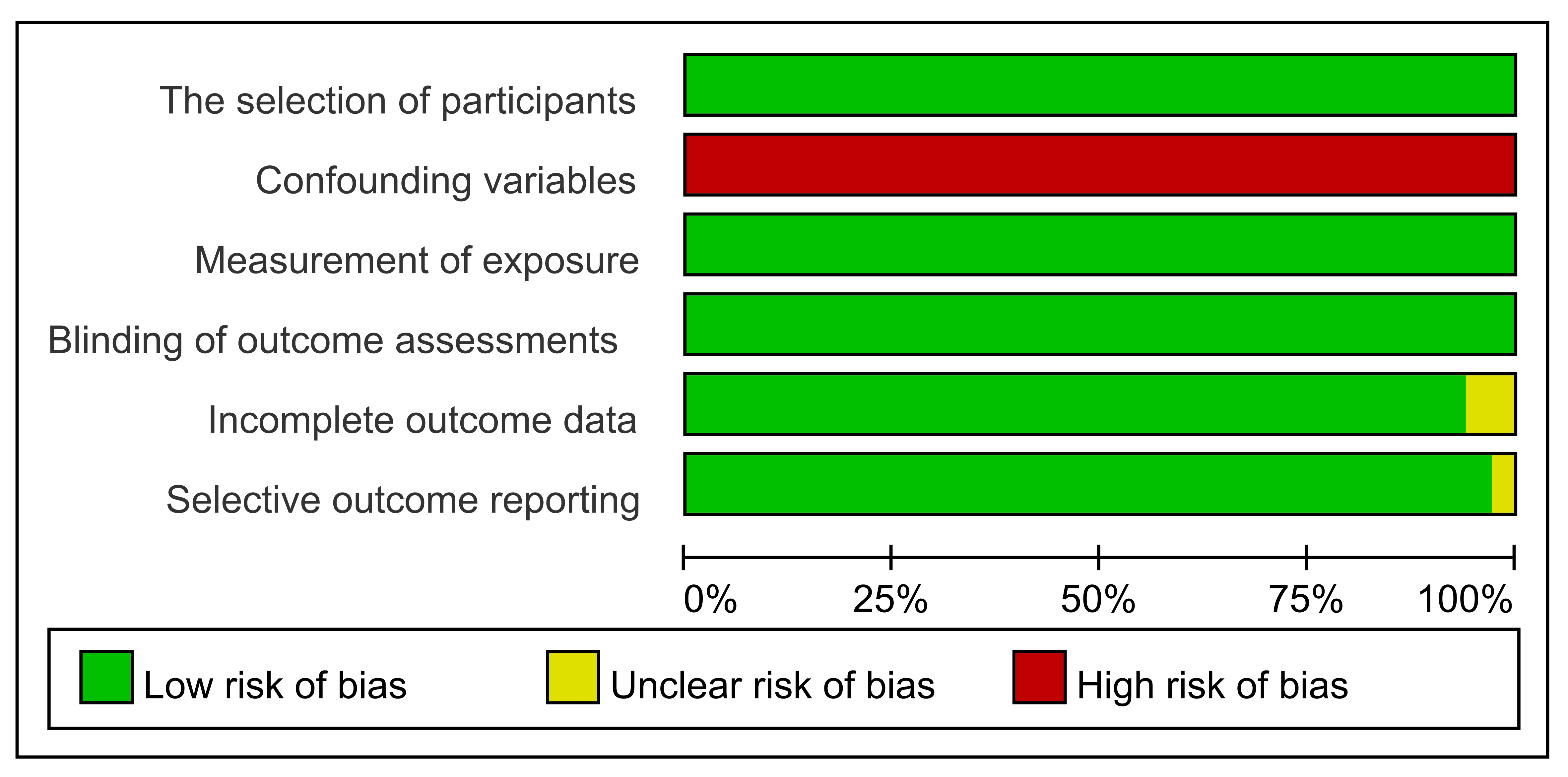
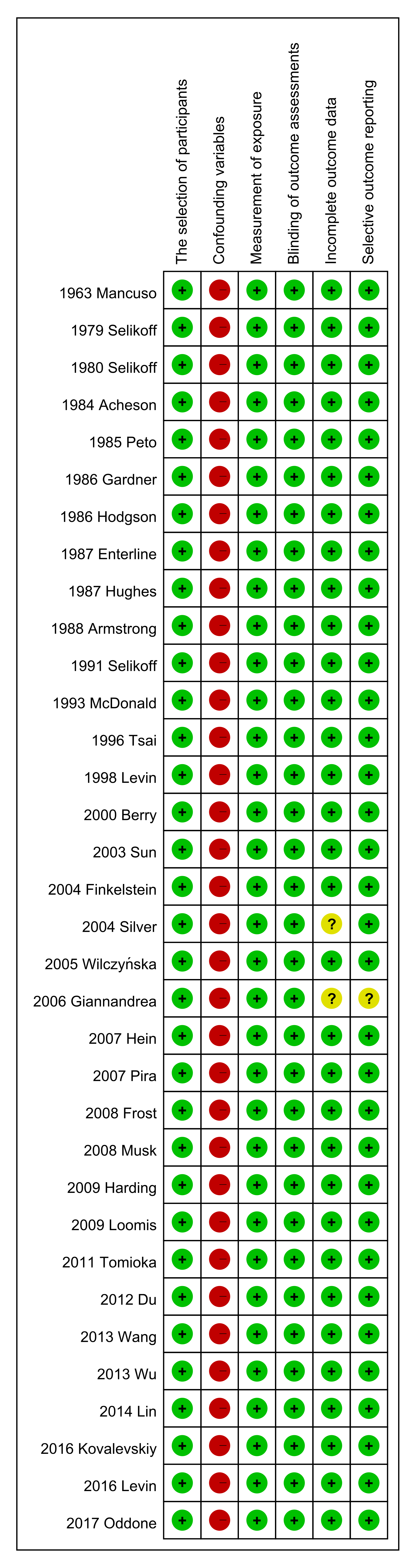
3.5. Risk of Bias Assessment
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- IARC Working Group on the Evaluation of Carcinogenic Risks to Humans. ASBESTOS (CHRYSOTILE, AMOSITE, CROCIDOLITE, TREMOLITE, ACTINOLITE AND ANTHOPHYLLITE). In IARC Monographs on the Evaluation of Carcinogenic Risks to Humans. Arsenic, Metals, Fibres and Dusts; International Agency for Research on Cancer, 2012; Volume 100 C. [Google Scholar]
- Albin, M.; Jakobsson, K.; Attewell, R.; Johansson, L.; Welinder, H. Mortality and cancer morbidity in cohorts of asbestos cement workers and referents. Br. J. Ind. Med. 1990, 47, 602–610. [Google Scholar] [CrossRef]
- Niklinski, J.; Niklinska, W.; Chyczewska, E.; Laudanski, J.; Naumnik, W.; Chyczewski, L.; Pluygers, E. The epidemiology of asbestos-related diseases. Lung Cancer 2004, 45 (Suppl. 1), S7–S15. [Google Scholar] [CrossRef]
- Gaudino, G.; Xue, J.; Yang, H. How asbestos and other fibers cause mesothelioma. Transl. Lung Cancer Res. 2020, 9, S39–S46. [Google Scholar] [CrossRef] [PubMed]
- Kratzke, P.; Kratzke, R.A. Asbestos-Related Disease. J. Radiol. Nurs. 2018, 37, 21–26. [Google Scholar] [CrossRef]
- Uhlenhopp, D.J.; Then, E.O.; Sunkara, T.; Gaduputi, V. Epidemiology of esophageal cancer: Update in global trends, etiology and risk factors. Clin. J. Gastroenterol. 2020, 13, 1010–1021. [Google Scholar] [CrossRef]
- Domper Arnal, M.J.; Ferrández Arenas, Á.; Lanas Arbeloa, Á. Esophageal cancer: Risk factors, screening and endoscopic treatment in Western and Eastern countries. World J. Gastroenterol. 2015, 21, 7933–7943. [Google Scholar] [CrossRef]
- Morgan, R.W.; Foliart, D.E.; Wong, O. Asbestos and gastrointestinal cancer. A review of the literature. West. J. Med. 1985, 143, 60–65. [Google Scholar] [PubMed]
- Offermans, N.S.; Vermeulen, R.; Burdorf, A.; Goldbohm, R.A.; Keszei, A.P.; Peters, S.; Kauppinen, T.; Kromhout, H.; van den Brandt, P.A. Occupational asbestos exposure and risk of esophageal, gastric and colorectal cancer in the prospective Netherlands Cohort Study. Int. J. Cancer 2014, 135, 1970–1977. [Google Scholar] [CrossRef] [PubMed]
- Wu, W.T.; Lin, Y.J.; Li, C.Y.; Tsai, P.J.; Yang, C.Y.; Liou, S.H.; Wu, T.N. Cancer Attributable to Asbestos Exposure in Shipbreaking Workers: A Matched-Cohort Study. PLoS ONE 2015, 10, e0133128. [Google Scholar] [CrossRef]
- Clin, B.; Morlais, F.; Dubois, B.; Guizard, A.V.; Desoubeaux, N.; Marquignon, M.F.; Raffaelli, C.; Paris, C.; Galateau-Salle, F.; Launoy, G.; et al. Occupational asbestos exposure and digestive cancers—A cohort study. Aliment. Pharmacol. Ther. 2009, 30, 364–374. [Google Scholar] [CrossRef]
- Reid, A.; Ambrosini, G.; de Klerk, N.; Fritschi, L.; Musk, B. Aerodigestive and gastrointestinal tract cancers and exposure to crocidolite (blue asbestos): Incidence and mortality among former crocidolite workers. Int. J. Cancer 2004, 111, 757–761. [Google Scholar] [CrossRef]
- De La Provôté, S.; Desoubeaux, N.; Paris, C.; Letourneux, M.; Raffaelli, C.; Galateau-Salle, F.; Gignoux, M.; Launoy, G. Incidence of digestive cancers and occupational exposure to asbestos. Eur. J. Cancer Prev. 2002, 11, 523–528. [Google Scholar] [CrossRef] [PubMed]
- Gustavsson, P.; Jakobsson, R.; Johansson, H.; Lewin, F.; Norell, S.; Rutkvist, L.E. Occupational exposures and squamous cell carcinoma of the oral cavity, pharynx, larynx, and oesophagus: A case-control study in Sweden. Occup. Environ. Med. 1998, 55, 393–400. [Google Scholar] [CrossRef] [PubMed]
- Parent, M.E.; Siemiatycki, J.; Fritschi, L. Workplace exposures and oesophageal cancer. Occup. Environ. Med. 2000, 57, 325–334. [Google Scholar] [CrossRef] [PubMed]
- Santibañez, M.; Vioque, J.; Alguacil, J.; Barber, X.; García de la Hera, M.; Kauppinen, T. Occupational exposures and risk of oesophageal cancer by histological type: A case-control study in eastern Spain. Occup. Environ. Med. 2008, 65, 774–781. [Google Scholar] [CrossRef] [PubMed]
- Rothman, K.J.; Greenland, S.; Lash, T.L. Modern Epidemiology; Wolters Kluwer Health/Lippincott Williams & Wilkins: Philadelphia, PE, USA, 2008; p. 665. [Google Scholar]
- Wang, B. Estimation of Standardized Mortality Ratio in Epidemiological Studies. Master’s Thesis, The University of Maine, Orono, ME, USA, 23 August 2002. [Google Scholar]
- Mancuso, T.F.; Coulter, E.J. Methodology in Industrial Health Studies. Arch. Environ. Health Int. J. 1963, 6, 210–226. [Google Scholar] [CrossRef]
- Selikoff, I.J.; Seidman, H.; Hammond, E.C. Mortality effects of cigarette smoking among amosite asbestos factory workers. J. Natl. Cancer Inst. 1980, 65, 507–513. [Google Scholar]
- Selikoff, I.J.; Hammond, E.C.; Seidman, H. Mortality experience of insulation workers in the United States and Canada, 1943—1976. Ann. NY Acad. Sci. 1979, 330, 91–116. [Google Scholar] [CrossRef]
- Acheson, E.D.; Gardner, M.J.; Winter, P.D.; Bennett, C. Cancer in a factory using amosite asbestos. Int. J. Epidemiol. 1984, 13, 3–10. [Google Scholar] [CrossRef]
- Peto, J.; Doll, R.; Hermon, C.; Binns, W.; Clayton, R.; Goffe, T. Relationship of mortality to measures of environmental asbestos pollution in an asbestos textile factory. Ann. Occup. Hyg. 1985, 29, 305–355. [Google Scholar] [CrossRef]
- Gardner, M.J.; Winter, P.D.; Pannett, B.; Powell, C.A. Follow up study of workers manufacturing chrysotile asbestos cement products. Br. J. Ind. Med. 1986, 43, 726–732. [Google Scholar] [CrossRef]
- Hodgson, J.T.; Jones, R.D. Mortality of asbestos workers in England and Wales 1971-81. Br. J. Ind. Med. 1986, 43, 158–164. [Google Scholar] [CrossRef]
- Enterline, P.E.; Hartley, J.; Henderson, V. Asbestos and cancer: A cohort followed up to death. Br. J. Ind. Med. 1987, 44, 396–401. [Google Scholar] [CrossRef]
- Hughes, J.M.; Weill, H.; Hammad, Y.Y. Mortality of workers employed in two asbestos cement manufacturing plants. Br. J. Ind. Med. 1987, 44, 161–174. [Google Scholar] [CrossRef] [PubMed]
- Armstrong, B.K.; de Klerk, N.H.; Musk, A.W.; Hobbs, M.S. Mortality in miners and millers of crocidolite in Western Australia. Br. J. Ind. Med. 1988, 45, 5–13. [Google Scholar] [CrossRef] [PubMed]
- Selikoff, I.J.; Seidman, H. Asbestos-associated deaths among insulation workers in the United States and Canada, 1967–1987. Ann. NY Acad. Sci. 1991, 643, 1–14. [Google Scholar] [CrossRef] [PubMed]
- McDonald, J.C.; Liddell, F.D.; Dufresne, A.; McDonald, A.D. The 1891–1920 birth cohort of Quebec chrysotile miners and millers: Mortality 1976-88. Br. J. Ind. Med. 1993, 50, 1073–1081. [Google Scholar] [CrossRef]
- Tsai, S.P.; Waddell, L.C.; Gilstrap, E.L.; Ransdell, J.D.; Ross, C.E. Mortality among maintenance employees potentially exposed to asbestos in a refinery and petrochemical plant. Am. J. Ind. Med. 1996, 29, 89–98. [Google Scholar] [CrossRef]
- Levin, J.L.; McLarty, J.W.; Hurst, G.A.; Smith, A.N.; Frank, A.L. Tyler asbestos workers: Mortality experience in a cohort exposed to amosite. Occup. Environ. Med. 1998, 55, 155–160. [Google Scholar] [CrossRef]
- Berry, G.; Newhouse, M.L.; Wagner, J.C. Mortality from all cancers of asbestos factory workers in east London 1933-80. Occup. Environ. Med. 2000, 57, 782–785. [Google Scholar] [CrossRef]
- Sun, T.; Li, L.; Shi, N.; Zhang, X. A 40-year cohort study on cancer mortality among female workers with manual spinning of chrysotile asbestos. Wei Sheng Yan Jiu 2003, 32, 511–513. [Google Scholar] [PubMed]
- Finkelstein, M.M.; Verma, D.K. A cohort study of mortality among Ontario pipe trades workers. Occup. Environ. Med. 2004, 61, 736–742. [Google Scholar] [CrossRef] [PubMed]
- Silver, S.R.; Daniels, R.D.; Taulbee, T.D.; Zaebst, D.D.; Kinnes, G.M.; Couch, J.R.; Kubale, T.L.; Yiin, J.H.; Schubauer-Berigan, M.K.; Chen, P.H. Differences in mortality by radiation monitoring status in an expanded cohort of Portsmouth Naval Shipyard workers. J. Occup. Environ. Med. 2004, 46, 677–690. [Google Scholar] [CrossRef] [PubMed]
- Wilczyńska, U.; Szymczak, W.; Szeszenia-Dabrowska, N. Mortality from malignant neoplasms among workers of an asbestos processing plant in Poland: Results of prolonged observation. Int. J. Occup. Med. Environ. Health 2005, 18, 313–326. [Google Scholar]
- Giannandrea, F.; Binazzi, A.; Giordano, F.; Figà-Talamanca, I. Exposure to amphibolic fibres and cancer of the gastrointestinal tract: An epidemiological survey in Lagonegro district (Southern Italy). Giornale Italiano di Medicina del Lavoro ed Ergonomia 2006, 28, 334–335. [Google Scholar]
- Hein, M.J.; Stayner, L.T.; Lehman, E.; Dement, J.M. Follow-up study of chrysotile textile workers: Cohort mortality and exposure-response. Occup. Environ. Med. 2007, 64, 616–625. [Google Scholar] [CrossRef]
- Pira, E.; Pelucchi, C.; Piolatto, P.G.; Negri, E.; Discalzi, G.; La Vecchia, C. First and subsequent asbestos exposures in relation to mesothelioma and lung cancer mortality. Br. J. Cancer 2007, 97, 1300–1304. [Google Scholar] [CrossRef][Green Version]
- Frost, G.; Harding, A.H.; Darnton, A.; McElvenny, D.; Morgan, D. Occupational exposure to asbestos and mortality among asbestos removal workers: A Poisson regression analysis. Br. J. Cancer 2008, 99, 822–829. [Google Scholar] [CrossRef]
- Musk, A.W.; de Klerk, N.H.; Reid, A.; Ambrosini, G.L.; Fritschi, L.; Olsen, N.J.; Merler, E.; Hobbs, M.S.; Berry, G. Mortality of former crocidolite (blue asbestos) miners and millers at Wittenoom. Occup. Environ. Med. 2008, 65, 541–543. [Google Scholar] [CrossRef]
- Harding, A.H.; Darnton, A.; Wegerdt, J.; McElvenny, D. Mortality among British asbestos workers undergoing regular medical examinations (1971-2005). Occup. Environ. Med. 2009, 66, 487–495. [Google Scholar] [CrossRef]
- Loomis, D.; Dement, J.M.; Wolf, S.H.; Richardson, D.B. Lung cancer mortality and fibre exposures among North Carolina asbestos textile workers. Occup. Environ. Med. 2009, 66, 535–542. [Google Scholar] [CrossRef]
- Tomioka, K.; Natori, Y.; Kumagai, S.; Kurumatani, N. An updated historical cohort mortality study of workers exposed to asbestos in a refitting shipyard, 1947-2007. Int. Arch. Occup. Environ. Health 2011, 84, 959–967. [Google Scholar] [CrossRef] [PubMed]
- Du, L.; Wang, X.; Wang, M.; Lan, Y. Analysis of mortality in chrysotile asbestos miners in China. J. Huazhong Univ. Sci. Technol. Med. Sci. 2012, 32, 135–140. [Google Scholar] [CrossRef]
- Wang, X.; Lin, S.; Yu, I.; Qiu, H.; Lan, Y.; Yano, E. Cause-specific mortality in a Chinese chrysotile textile worker cohort. Cancer Sci. 2013, 104, 245–249. [Google Scholar] [CrossRef]
- Wu, W.T.; Lu, Y.H.; Lin, Y.J.; Yang, Y.H.; Shiue, H.S.; Hsu, J.H.; Li, C.Y.; Yang, C.Y.; Liou, S.H.; Wu, T.N. Mortality among shipbreaking workers in Taiwan—A retrospective cohort study from 1985 to 2008. Am. J. Ind. Med. 2013, 56, 701–708. [Google Scholar] [CrossRef]
- Lin, S.; Wang, X.; Yano, E.; Yu, I.; Lan, Y.; Courtice, M.N.; Christiani, D.C. Exposure to chrysotile mining dust and digestive cancer mortality in a Chinese miner/miller cohort. Occup. Environ. Med. 2014, 71, 323–328. [Google Scholar] [CrossRef]
- Kovalevskiy, E.V.; Schonfeld, S.J.; Feletto, E.; Moissonnier, M.; Kashanskiy, S.V.; Bukhtiyarov, I.V.; Schüz, J. Comparison of mortality in Asbest city and the Sverdlovsk region in the Russian Federation: 1997–2010. Environ. Health 2016, 15, 42. [Google Scholar] [CrossRef][Green Version]
- Levin, J.L.; Rouk, A.; Shepherd, S.; Hurst, G.A.; McLarty, J.W. Tyler asbestos workers: A mortality update in a cohort exposed to amosite. J. Toxicol. Environ. Health B Crit. Rev. 2016, 19, 190–200. [Google Scholar] [CrossRef] [PubMed]
- Oddone, E.; Ferrante, D.; Tunesi, S.; Magnani, C. Mortality in asbestos cement workers in Pavia, Italy: A cohort study. Am. J. Ind. Med. 2017, 60, 852–866. [Google Scholar] [CrossRef] [PubMed]
- Kim, S.Y.; Park, J.E.; Lee, Y.J.; Seo, H.J.; Sheen, S.S.; Hahn, S.; Jang, B.H.; Son, H.J. Testing a tool for assessing the risk of bias for nonrandomized studies showed moderate reliability and promising validity. J. Clin. Epidemiol. 2013, 66, 408–414. [Google Scholar] [CrossRef]
- Institute of Medicine Committee on Asbestos: Selected Health Effects. The National Academies Collection: Reports funded by National Institutes of Health. In Asbestos: Selected Cancers; National Academies Press (US) Copyright © 2021, National Academy of Sciences: Washington, DC, USA, 2006. [Google Scholar] [CrossRef]
- Li, B.; Tang, S.P.; Wang, K.Z. Esophagus cancer and occupational exposure to asbestos: Results from a meta-analysis of epidemiology studies. Dis. Esophagus 2016, 29, 421–428. [Google Scholar] [CrossRef]
- Peterson, M.K.; Mohar, I.; Lam, T.; Cook, T.J.; Engel, A.M.; Lynch, H. Critical review of the evidence for a causal association between exposure to asbestos and esophageal cancer. Crit. Rev. Toxicol. 2019, 49, 597–613. [Google Scholar] [CrossRef]
- Møller, P.; Danielsen, P.H.; Jantzen, K.; Roursgaard, M.; Loft, S. Oxidatively damaged DNA in animals exposed to particles. Crit. Rev. Toxicol. 2013, 43, 96–118. [Google Scholar] [CrossRef]
- Wronkiewicz, S.K.; Roggli, V.L.; Hinrichs, B.H.; Kendler, A.; Butler, R.A.; Christensen, B.C.; Marsit, C.J.; Nelson, H.H.; McClean, M.D.; Kelsey, K.T.; et al. Chrysotile fibers in tissue adjacent to laryngeal squamous cell carcinoma in cases with a history of occupational asbestos exposure. Mod. Pathol. Off. J. US Can. Acad. Pathol. 2020, 33, 228–234. [Google Scholar] [CrossRef]
- Uguen, M.; Dewitte, J.D.; Marcorelles, P.; Loddé, B.; Pougnet, R.; Saliou, P.; De Braekeleer, M.; Uguen, A. Asbestos-related lung cancers: A retrospective clinical and pathological study. Mol. Clin. Oncol. 2017, 7, 135–139. [Google Scholar] [CrossRef]
- Borrelli, E.P.; McGladrigan, C.G. A Review of Pharmacologic Management in the Treatment of Mesothelioma. Curr. Treat. Options Oncol. 2021, 22, 14. [Google Scholar] [CrossRef]
- Wang, X.; Lin, S.; Yano, E.; Yu, I.T.; Courtice, M.; Lan, Y.; Christiani, D.C. Exposure-specific lung cancer risks in Chinese chrysotile textile workers and mining workers. Lung Cancer 2014, 85, 119–124. [Google Scholar] [CrossRef]
- Berman, D.W. Comparing milled fiber, Quebec ore, and textile factory dust: Has another piece of the asbestos puzzle fallen into place? Crit. Rev. Toxicol. 2010, 40, 151–188. [Google Scholar] [CrossRef]












{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Study (Year) | Country | N | Follow-up Period | Study Population | Asbestos type | Comparison | Observed/Expected of EC | SMR (95%CI) | Reference Population |
|---|---|---|---|---|---|---|---|---|---|
| 1. Oddone (2017) | Italy | 1818 males and females | 1932–1992 | asbestos-cement workers in the largest plant in Lombardy | Mixed asbestos | Overall Male Female | 8/9.92 7/9.68 1/0.24 | 0.81 (0.35–1.59) 0.72 (0.29–1.49) 4.16 (0.10–23.16) | the National Institute of Health based on mortality |
| 2. Kovalevskiy (2016) | Russian | 16,596 males and females | 1997–2010 | Population-based | Chrysotile | Overall Male Female | 66/45.21 51/34.93 15/10.49 | 1.46 (1.13–1.85) 1.46 (1.09–1.92) 1.43 (0.80–2.35) | Sverdlovsk resion |
| 3. Levin (2016) | USA | 1130 male and female | 1979–2013 | Tyler asbestos plant | Amosite | Overall | 3/3.75 | 0.80 (0.16–2.34) | Life Table Analysis System, CDC, USA |
| 4. Lin (2014) | China | 1539 males | 1981–2006 | Chrysotile asbestos miners | Chrysolite | Overall (male) | 9/6.22 | 1.45 (0.76–2.75) | Chinese national data |
| 5. Wang (2013) | China | 586 males and 279 females | 1972–2008 | Chrysolite textile factory | Primarily chrysotile | Male | 7/5.59 | 1.25 (0.61–2.59) | Chinese nationwide data |
| 6. Wu (2013) | Taiwan | 4926 males and females | 1985–2008 | Ship breaks | Mixed asbestos | Male Male flame cutters Male lifters | 17/10.4 13/5.8 4/2.2 | 1.63 (0.95–2.61) 2.24 (1.19–3.84) 1.82 (0.49–4.66) | General population of Taiwan |
| 7. Du (2012) | China | 1932 males and females | 1981–2010 | Chrysotile asbestos miners | Chrysolite | Overall | 9/5.59 | 1.61 (0.73–2.82) | Chinese national death rate |
| 8. Tomioka (2011) | Japan | 90 male laggers159 male boiler repairers | 1947–2007 | Refitting shipyard | Mixed asbestos | Male laggers Male boiler repairers | 1/0.68 1/1.16 | 1.46 (0.04–8.11) 0.86 (0.02–4.77) | Japanese male population |
| 9. Harding (2009) | UK | 98,117 males and females | 1971–2006 | British asbestos workers | Mixed asbestos | Overall | 220/189.66 | 1.16 (1.01–1.32) | Great Britain |
| 10. Loomis (2009) | USA | 5770 males and females | 1950–2003 | Asbestos textile factories | Chrysolite | Overall | 10/13.49 | 0.74 (0.36–1.36) | National population, USA |
| 11. Frost (2008) | UK | 31,302 males and females | 1971–2005 | Stripping/removal workers | Mixed asbestos | Overall | 16/15.36 | 1.042 (0.596–1.692) | England, Wales and Scotlant |
| 12. Musk (2008) | Australia | 6943 males | 1979–2001 | Crocidolite mine | Crocidolite | Overall (male) | 12/10 | 1.20 (0.62–2.10) | Western Australian male population |
| 13. Hein (2007) | USA | 3072 males and females | 1979–2001 | Asbestos textile plant | Chrysolite | Overall White males Nonwhite males | 17/9.1 8/3.69 9/3.98 | 1.87 (1.09–2.99) 2.17 (0.94–4.28) 2.26 (1.03–4.28) | USA and South Carolina |
| 14. Pira (2007) | Italy | 1966 males and females | Up to 2004 | Asbestos (mainly textile) company | Mixed asbestos | Overall Male Female | 4/2.7 2/2.4 2/0.3 | 1.49 (0.41–3.81) 0.85 (NR) 6.03 (NR) | Italian National Institute of Statistics, and WHO |
| 15. Giannandrea (2006) | Italy | 427 deaths for gastrointestinal cancer | 1980–2001 | Population-based | Tremolite | Overall | NR | 1.3309 (0.98–1.75) | Basilicata region |
| 16. Wilczyńska (2005) | Poland | 4497 males and females | 1945–1999 | Asbestos plant | Mixed asbestos | Male | 10/5.78 | 1.73 (0.83–3.18) | General Poland population |
| 17. Finkelstein (2004) | USA and Canada | 25,285 males | 1950–1999 | Pipe trade workers | Not specified | Overall (male) | 30/23.62 | 1.27 (0.86–1.81) | Ontario male population |
| 18. Silver (2004) | USA | 37,853 males and females | 1952–1996 | Portsmouth Naval Shipyard | Not specified | Overall | 97/71.32 | 1.36 (1.11–1.67) | NIOSH personal computer Life Tabale Analysis System |
| 19. Sun (2003) | China | 5681 females | 1990–2000 | Manual spinning workers | Chrysotile | Overall (female) | 6/6.18 | 0.97 (0.44–2.16) | Cixi City female population |
| 20. Berry (2000) | UK | 5100 males and females (12 cases) | Up to 1980 | Textile and prefabricated cement pipes | Mixed asbestos | Overall | 12/5.78 | 2.08 (0.44–2.16) | England and Wales |
| 21. Levin (1998) | USA | 753 males | 1954–1972 | Manufacture of asbestos pipe insulation materials | Amosite | Overall (male) | 2/0.9 | 2.32 (0.28–8.39) | Empolys mortality and population data system, University of Pittsburgh, USA |
| 22. Tsai (1996) | USA | 2504 males | 1948–1989 | Refinery and petrochemical plant, Texas | Mixed asbestos | Overall (male) | 4/6.4 | 0.63 (0.17–1.60) | Harris County, Texas |
| 23. McDonald (1993) | Canada | 11,000 males | 1976–1988 | Chrysotile miners and millers | Chrysotile | Overall (male) | 20/27.39 | 0.73 (NR) | General population of Ouebec |
| 24. Selikoff (1991) | USA and Canada | 17,800 males | 1967–1986 | Asbestos insulation workers | Not specified | Overall (male) | 30/17.80 | 1.68 (NR) | US National Center for Health Statistics |
| 25. Armstrong (1988) | Australia | 6916 males and females | 1943–1980 | Crocidolite mining and milling | Crocidolite | Overall | 3/2.54 | 1.18 (0.38–3.66) | Western Australia |
| 26. Enterline (1987) | USA | 1074 males | 1941–1980 | Asbestos company | Not specified | Overall (male) | 4/2.95 | 1.356 (NR) | US white men |
| 27. Hughes (1987) | USA | 6931 males | 1970–1982 | New Orleans asbestos cement plants | Primarily chrysotile | Overall (male) | 12/12.9 | 0.93 (NR) | Louisiana mortality |
| 28. Gardner (1986) | UK | 2167 male and female | 1941–1983 | Asbestos cement factory | Mainly chrysotile, but some amosite | Overall | 1/3.5 | 0.286 (NR) | England and Wales |
| 29. Hodgson (1986) | UK | 31,150 males | Up to 1981 | British asbestos workers | Not specified | Pre-1969 Post-1969 | 6/9.4 1/2.3 | 0.637 (NR) 0.44 (NR) | England and Wales |
| 30. Peto (1985) | UK | 3211 males | 1969–1973 | Rochdale asbestos textile factory workers | Mainly chrysotile, but some crocidolite | Overall (male) | 11/6.59 | 1.669 (NR) | England and Wales |
| 31. Acheson (1984) | UK | 5969 males | 1947–1979 | A manufacture factory | Amosite | Overall (male) | 2/2 | 1.00 (NR) | England and Wales |
| 32. Selikoff (1980) | USA | 582 males | 1961–1977 | Amosite factory workers | Amosite | Overall (male) | 1/0.8 | 1.25 (NR) | New Jersy white males |
| 33. Selikoff (1979) | USA | 17,800 males | 1943–1976 | US and Canada asbestos insulation workers | Not specified | Overall (male) | 18/7.1 | 2.53 (NR) | US white male |
| 34. Mancuso (1963) | USA | 1495 males and females | 1940–1960 | An asbestos company | Not specified | Overall (male) | 1/0.53 | 1.887 (NR) | Ohio State general population |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Wu, C.-W.; Chuang, H.-Y.; Tsai, D.-L.; Kuo, T.-Y.; Yang, C.-C.; Chen, H.-C.; Kuo, C.-H. Meta-Analysis of the Association between Asbestos Exposure and Esophageal Cancer. Int. J. Environ. Res. Public Health 2021, 18, 11088. https://doi.org/10.3390/ijerph182111088
Wu C-W, Chuang H-Y, Tsai D-L, Kuo T-Y, Yang C-C, Chen H-C, Kuo C-H. Meta-Analysis of the Association between Asbestos Exposure and Esophageal Cancer. International Journal of Environmental Research and Public Health. 2021; 18(21):11088. https://doi.org/10.3390/ijerph182111088
Chicago/Turabian StyleWu, Chih-Wei, Hung-Yi Chuang, Dong-Lin Tsai, Tzu-Yu Kuo, Chen-Cheng Yang, Huang-Chi Chen, and Chao-Hung Kuo. 2021. "Meta-Analysis of the Association between Asbestos Exposure and Esophageal Cancer" International Journal of Environmental Research and Public Health 18, no. 21: 11088. https://doi.org/10.3390/ijerph182111088
APA StyleWu, C.-W., Chuang, H.-Y., Tsai, D.-L., Kuo, T.-Y., Yang, C.-C., Chen, H.-C., & Kuo, C.-H. (2021). Meta-Analysis of the Association between Asbestos Exposure and Esophageal Cancer. International Journal of Environmental Research and Public Health, 18(21), 11088. https://doi.org/10.3390/ijerph182111088