Typologies of Family Functioning and 24-h Movement Behaviors

Abstract
1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Exposures
2.3. Outcomes
2.4. Statistical Analyses
3. Results
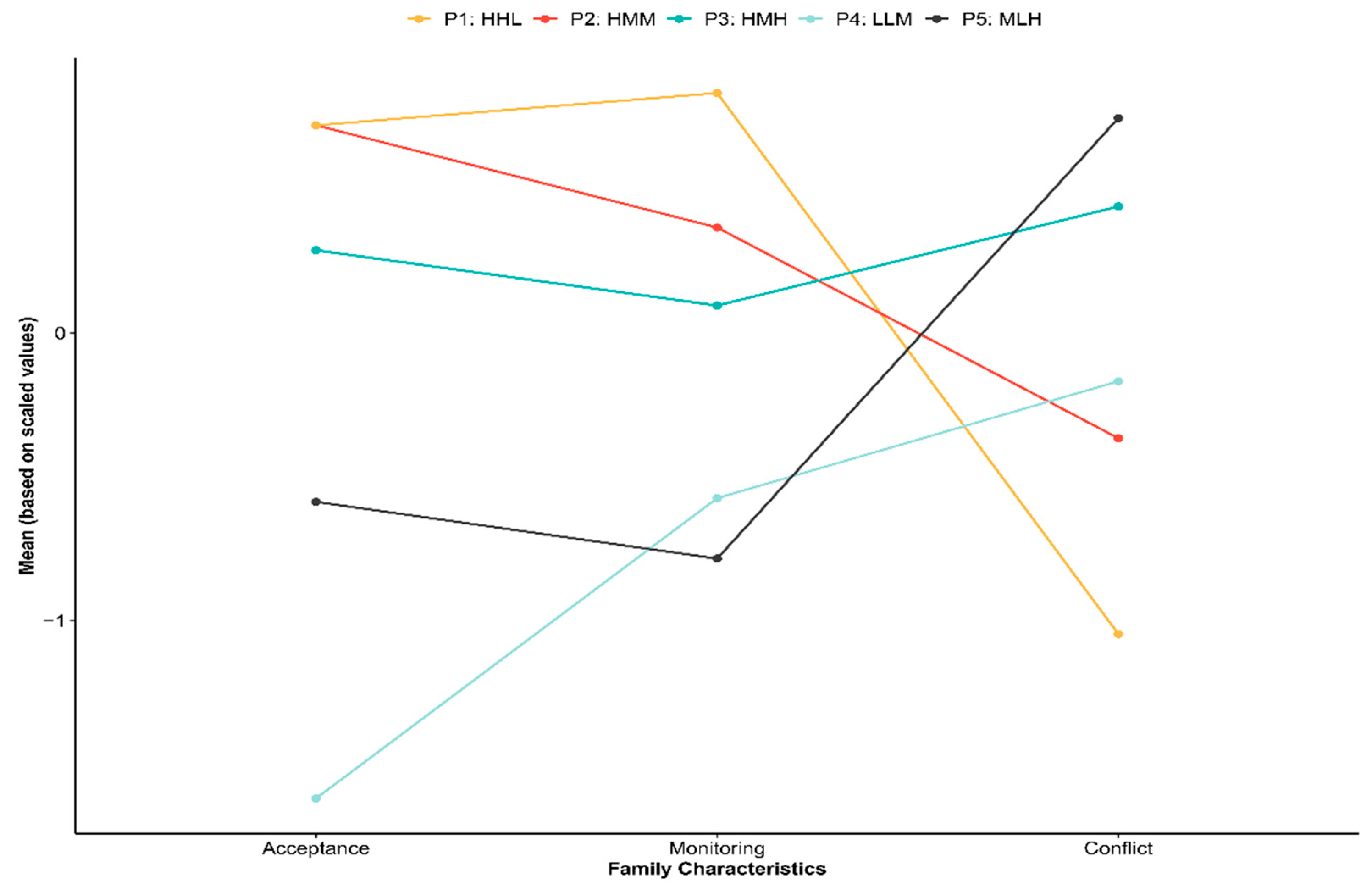
3.1. Latent Profiles
3.2. Association of Family Profiles with Number of Movement Behaviors Met
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Tremblay, M.S.; Carson, V.; Chaput, J.-P.; Gorber, S.C.; Dinh, T.; Duggan, M.; Faulkner, G.; Gray, C.E.; Gruber, R.; Janson, K.; et al. Canadian 24-Hour Movement Guidelines for Children and Youth: An Integration of Physical Activity, Sedentary Behaviour, and Sleep. Appl. Physiol. Nutr. Metab. 2016, 41, S311–S327. [Google Scholar] [CrossRef] [PubMed]
- Román-Viñas, B.; for the ISCOLE Research Group; Chaput, J.-P.; Katzmarzyk, P.T.; Fogelholm, M.; Lambert, E.V.; Maher, C.; Maia, J.; Olds, T.; Onywera, V.; et al. Proportion of children meeting recommendations for 24-h movement guidelines and associations with adiposity in a 12-country study. Int. J. Behav. Nutr. Phys. Act. 2016, 13, 1–10. [Google Scholar] [CrossRef]
- Lucas-De La Cruz, L.; Martínez-Vizcaíno, V.; García-Prieto, J.C.; Arias-Palencia, N.; Diez-Fernandez, A.; Milla-Tobarra, M.; Notario-Pacheco, B. Movement behaviors and cardiometabolic risk in schoolchildren. PLoS ONE 2018, 13, e0207300. [Google Scholar] [CrossRef] [PubMed]
- Lee, E.Y.; Spence, J.C.; Tremblay, M.S.; Carson, V. Meeting 24-Hour Movement Guidelines for Children and Youth and associations with psychological well-being among South Korean adolescents. Ment. Health Phys. Act. 2018, 14, 66–73. [Google Scholar] [CrossRef]
- Walsh, J.J.; Barnes, J.D.; Cameron, J.D.; Goldfield, G.S.; Chaput, J.-P.; Gunnell, K.E.; Ledoux, A.-A.; Zemek, R.L.; Tremblay, M.S. Associations between 24 h movement be-haviours and global cognition in US children: A cross-sectional observational study. Lancet Child. Adolesc. Health 2018, 2, 783–791. [Google Scholar] [CrossRef]
- Guerrero, M.D.; Barnes, J.D.; Walsh, J.J.; Chaput, J.-P.; Tremblay, M.S.; Goldfield, G.S. 24-Hour Movement Behaviors and Impulsivity. Pediatrics 2019, 144, e20190187. [Google Scholar] [CrossRef]
- Brown, D.; Kwan, M.; Arbour-Nicitopoulos, K.; Cairney, J. Identifying patterns of movement behaviours in relation to depres-sive symptoms during adolescence: A latent profile analysis approach. Prev. Med. 2021, 143, 106352. [Google Scholar] [CrossRef]
- Trost, S.G.; Sallis, J.F.; Pate, R.R.; Freedson, P.S.; Taylor, W.C.; Dowda, M. Evaluating a model of parental influence on youth physical activity. Am. J. Prev. Med. 2003, 25, 277–282. [Google Scholar] [CrossRef]
- Biddle, S.J.H.; Atkin, A.J.; Cavill, N.; Foster, C. Correlates of physical activity in youth: A review of quantitative systematic re-views. Int. Rev. Sport Exerc. Psychol. 2011, 4, 294–298. [Google Scholar] [CrossRef]
- Schaefer, E.S. Children’s Reports of Parental Behavior: An Inventory. Child Dev. 1965, 36, 413. [Google Scholar] [CrossRef]
- Khaleque, A.; Rohner, R.P. Perceived Parental Acceptance-Rejection and Psychological Adjustment: A Meta-Analysis of Cross-Cultural and Intracultural Studies. J. Marriage Fam. 2002, 64, 54–64. [Google Scholar] [CrossRef]
- Rhodes, R.E.; Guerrero, M.D.; Vanderloo, L.M.; Barbeau, K.; Birken, C.S.; Chaput, J.-P.; Faulkner, G.; Janssen, I.; Madigan, S.; Mâsse, L.C.; et al. Development of a consensus statement on the role of the family in the physical activity, sedentary, and sleep behaviours of children and youth. Int. J. Behav. Nutr. Phys. Act. 2020, 17, 1–31. [Google Scholar] [CrossRef] [PubMed]
- Sterdt, E.; Liersch, S.; Walter, U. Correlates of physical activity of children and adolescents: A systematic review of reviews. Health Educ. J. 2013, 73, 72–89. [Google Scholar] [CrossRef]
- Langer, S.L.; Crain, A.L.; Senso, M.M.; Levy, R.L.; Sherwood, N.E. Predicting child physical activity and screen time: Parental sup-port for physical activity and general parenting styles. J. Pediatr. Psychol. 2014, 39, 633–642. [Google Scholar] [CrossRef] [PubMed]
- Gunn, H.E.; O’Rourke, F.; Dahl, R.E.; Goldstein, T.R.; Rofey, D.L.; Forbes, E.E.; Shaw, D.S. Young adolescent sleep is associated with parental monitoring. Sleep Health 2019, 5, 58–63. [Google Scholar] [CrossRef]
- Arredondo, E.; Elder, J.P.; Ayala, G.X.; Campbell, N.; Baquero, B.; Duerksen, S. Is parenting style related to children’s healthy eating and physical activity in Latino families? Health Educ. Res. 2006, 21, 862–871. [Google Scholar] [CrossRef]
- Gentile, D.A.; Reimer, R.A.; Nathanson, A.I.; Walsh, D.A.; Eisenmann, J.C. Protective effects of parental monitoring of children’s media use a prospective study. JAMA Pediatr. 2014, 168, 479–484. [Google Scholar] [CrossRef]
- Machado, A.K.F.; Wendt, A.; Ricardo, L.I.; Marmitt, L.P.; Martins, R.C. Are parental monitoring and support related with loneliness and problems to sleep in adolescents? Results from the Brazilian School-based Health Survey. Child. Youth Serv. Rev. 2020, 119, 105682. [Google Scholar] [CrossRef]
- Moos, R.H.; Moos, B.S. Family Environment Scale Manual: Development, Applications, Research, 3rd ed.; Consulting Psychologist Press: Palo Alta, CA, USA, 1994. [Google Scholar]
- Conger, R.D.; Ge, X.; Elder, G.H.; O Lorenz, F.; Simons, R.L. Economic stress, coercive family process, and developmental problems of adolescents. Child. Dev. 1994, 65, 541–561. [Google Scholar] [CrossRef]
- Sadeh, A. Consequences of Sleep Loss or Sleep Disruption in Children. Sleep Med. Clin. 2007, 2, 513–520. [Google Scholar] [CrossRef]
- Khor, S.P.; Anne, M.; Aldridge, G.; Bei, B.; Yap, M.B.H. Modifiable parental factors in adolescent sleep: A systematic review and meta-analysis. Sleep Med. Rev. 2021, 56, 101408. [Google Scholar] [CrossRef] [PubMed]
- Gregory, A.M.; Caspi, A.; Moffitt, T.E.; Poulton, R. Family Conflict in Childhood: A Predictor of Later Insomnia. Sleep 2006, 29, 1063–1067. [Google Scholar] [CrossRef] [PubMed]
- El-Sheikh, M.; Buckhalt, J.A.; Mize, J.; Acebo, C. Marital Conflict and Disruption of Children’s Sleep. Child Dev. 2006, 77, 31–43. [Google Scholar] [CrossRef] [PubMed]
- Sadeh, A. Stress, Trauma, and Sleep in Children. Child Adolesc. Psychiatr. Clin. 1996, 5, 685–700. [Google Scholar] [CrossRef]
- Rosenblatt, P.C.; Cunningham, M.R. Television Watching and Family Tensions. J. Marriage Fam. 1976, 38, 105. [Google Scholar] [CrossRef]
- Vandewater, E.A.; Lee, J.H.; Shim, M.-S. Family Conflict and Violent Electronic Media Use in School-Aged Children. Media Psychol. 2005, 7, 73–86. [Google Scholar] [CrossRef]
- Schaefer, E.S. A configurational analysis of children’s reports of parent behavior. J. Consult. Psychol. 2006, 29, 552–557. [Google Scholar] [CrossRef]
- Brener, N.D.; Kann, L.; McManus, T.; Kinchen, S.A.; Sundberg, E.C.; Ross, J.G. Reliability of the 1999 Youth Risk Behavior Survey questionnaire. J. Adolesc. Health 2002, 31, 336–342. [Google Scholar] [CrossRef]
- Barch, D.M.; Albaugh, M.D.; Avenevoli, S.; Chang, L.; Clark, D.B.; Glantz, M.D.; Hudziak, J.J.; Jernigan, T.L.; Tapert, S.F.; Yurgelun-Todd, D.; et al. Demographic, physical and mental health as-sessments in the adolescent brain and cognitive development study: Rationale and description. Dev. Cogn. Neurosci. 2018, 32, 55–66. [Google Scholar] [CrossRef]
- Bruni, O.; Ottaviano, S.; Guidetti, V.; Romoli, M.; Innocenzi, M.; Cortesi, F.; Giannotti, F. The Sleep Disturbance Scale for Children (SDSC) Construct ion and validation of an instrument to evaluate sleep disturbances in childhood and adolescence. J. Sleep Res. 1996, 5, 251–261. [Google Scholar] [CrossRef]
- Scrucca, L.; Fop, M.; Murphy, T.B.; Raftery, A.E. mclust 5: Clustering, Classification and Density Estimation Using Gaussian Finite Mixture Models. R J. 2016, 8, 289–317. [Google Scholar] [CrossRef] [PubMed]
- Repetti, R.L.; Taylor, S.E.; Seeman, T.E. Risky families: Family social environments and the mental and physical health of off-spring. Psychol. Bull. 2002, 128, 330–366. [Google Scholar] [CrossRef] [PubMed]
- Rothbart, M.K.; Ahadi, S.A.; Hershey, K.L.; Fisher, P. Investigations of temperament at three to seven years: The children’s behav-ior questionnaire. Child. Dev. 2001, 72, 1394–1408. [Google Scholar] [CrossRef]
- Jago, R.; Zahra, J.; Edwards, M.J.; Kesten, J.; Solomon-Moore, E.L.; Thompson, J.; Sebire, S.J. Managing the screen-viewing behaviours of children aged 5–6 years: A qualitative analysis of parental strategies: Table 1. BMJ Open 2016, 6, e010355. [Google Scholar] [CrossRef] [PubMed]
- Evans, C.A.; Jordan, A.B.; Horner, J. Only two hours? A qualitative study of the challenges parents perceive in restricting child television time. J. Fam. Issues 2011, 32, 1223–1244. [Google Scholar] [CrossRef]
- Padilla-Walker, L.M.; Nelson, L.J. Black hawk down?: Establishing helicopter parenting as a distinct construct from other forms of parental control during emerging adulthood. J. Adolesc. 2012, 35, 1177–1190. [Google Scholar] [CrossRef]
- Hong, J.-C.; Hwang, M.-Y.; Kuo, Y.-C.; Hsu, W.-Y. Parental monitoring and helicopter parenting relevant to vocational student’s procrastination and self-regulated learning. Learn. Individ. Differ. 2015, 42, 139–146. [Google Scholar] [CrossRef]


{kind=link}
| Solutions | BIC | CAIC | SABIC | BLRT p-Value | Entropy |
|---|---|---|---|---|---|
| 1-Profile | 97,839.01 | 97848.01 | 97810.41 | - | 1.00 |
| 2-Profile | 88,667.48 | 88684.48 | 88613.46 | 0.001 | 0.745 |
| 3-Profile | 84,198.61 | 84223.61 | 84119.16 | 0.001 | 0.820 |
| 4-Profile | 81,853.51 | 81886.51 | 81748.64 | 0.001 | 0.737 |
| 5-Profile | 79,035.78 | 79076.78 | 78905.48 | 0.001 | 0.843 |
| Profile | Acceptance | Monitoring | Conflict | |||
|---|---|---|---|---|---|---|
| M | SD | M | SD | M | SD | |
| P1: H-Acceptance, H-Monitoring, L-Conflict (n = 1462) | 15.00 | 0.00 | 24.07 | 0.80 | 0.00 | 0.00 |
| P2: H-Acceptance, M-Monitoring, M-Conflict (n = 3095) | 15.00 | 0.00 | 22.87 | 1.67 | 1.33 | 0.87 |
| P3: H-Acceptance, M-Monitoring, H-Conflict (n = 3357) | 14.34 | 0.47 | 22.17 | 1.93 | 2.90 | 2.07 |
| P4: L-Acceptance, L-Monitoring, M-Conflict (n = 1895) | 11.45 | 1.62 | 20.44 | 2.98 | 1.72 | 1.73 |
| P5: M-Acceptance, L-Monitoring, H-Conflict (n = 2020) | 13.02 | 1.10 | 19.89 | 2.98 | 3.50 | 2.01 |
| ≥1 Recommendation | ≥2 Recommendations | 3 Recommendations | |||||||
|---|---|---|---|---|---|---|---|---|---|
| Predictors | OR | 95% CI | p | OR | 95% CI | p | OR | 95% CI | p |
| (Intercept) | 70.73 | 30.20, 165.67 | <0.001 | 40.96 | 13.58, 123.51 | <0.001 | 1.58 | 0.18, 13.76 | 0.677 |
| Age (decimal years) | 0.71 | 0.66, 0.77 | <0.001 | 0.63 | 0.57, 0.69 | <0.001 | 0.66 | 0.55, 0.79 | <0.001 |
| Sex (ref: girls, n = 5142) | 1.20 | 1.10, 1.31 | <0.001 | 1.43 | 1.27, 1.61 | <0.001 | 1.18 | 0.94, 1.49 | 0.148 |
| Ethnicity: African Americans a (n = 1503) | 0.27 | 0.18, 0.41 | <0.001 | 0.17 | 0.10, 0.27 | <0.001 | 0.19 | 0.06, 0.58 | 0.004 |
| Ethnicity: Caucasians a (n = 5861) | 0.65 | 0.44, 0.96 | 0.032 | 0.72 | 0.46, 1.12 | 0.145 | 1.40 | 0.55, 3.55 | 0.477 |
| Ethnicity: Hispanics a (n = 1765) | 0.36 | 0.24, 0.54 | <0.001 | 0.31 | 0.20, 0.50 | <0.001 | 0.29 | 0.10, 0.79 | 0.015 |
| Ethnicity: Multiracial a (n = 1367) | 0.43 | 0.29, 0.64 | <0.001 | 0.43 | 0.27, 0.69 | <0.001 | 0.61 | 0.23, 1.61 | 0.318 |
| Family income (1–10 scale, M = 7.24, SD = 2.42) | 1.14 | 1.12, 1.16 | <0.001 | 1.28 | 1.24, 1.32 | <0.001 | 1.41 | 1.31, 1.53 | <0.001 |
| Family typology: P2 b | 0.81 | 0.69, 0.95 | 0.012 | 0.77 | 0.63, 0.94 | 0.012 | 0.54 | 0.39, 0.76 | <0.001 |
| Family typology: P3 b | 0.62 | 0.53, 0.73 | <0.001 | 0.49 | 0.40, 0.59 | <0.001 | 0.28 | 0.20, 0.40 | <0.001 |
| Family typology: P4 b | 0.54 | 0.45, 0.64 | <0.001 | 0.42 | 0.33, 0.52 | <0.001 | 0.24 | 0.16, 0.36 | <0.001 |
| Family typology: P5 b | 0.54 | 0.45, 0.64 | <0.001 | 0.35 | 0.28, 0.44 | <0.001 | 0.19 | 0.12, 0.29 | <0.001 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Guerrero, M.D.; Barnes, J.D.; Tremblay, M.S.; Pulkki-Råback, L. Typologies of Family Functioning and 24-h Movement Behaviors. Int. J. Environ. Res. Public Health 2021, 18, 699. https://doi.org/10.3390/ijerph18020699
Guerrero MD, Barnes JD, Tremblay MS, Pulkki-Råback L. Typologies of Family Functioning and 24-h Movement Behaviors. International Journal of Environmental Research and Public Health. 2021; 18(2):699. https://doi.org/10.3390/ijerph18020699
Chicago/Turabian StyleGuerrero, Michelle D., Joel D. Barnes, Mark S. Tremblay, and Laura Pulkki-Råback. 2021. "Typologies of Family Functioning and 24-h Movement Behaviors" International Journal of Environmental Research and Public Health 18, no. 2: 699. https://doi.org/10.3390/ijerph18020699
APA StyleGuerrero, M. D., Barnes, J. D., Tremblay, M. S., & Pulkki-Råback, L. (2021). Typologies of Family Functioning and 24-h Movement Behaviors. International Journal of Environmental Research and Public Health, 18(2), 699. https://doi.org/10.3390/ijerph18020699