
Post Discharge mHealth and Teach-Back Communication Effectiveness on Hospital Readmissions: A Systematic Review

 ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Search Strategies
2.2. Study Selection
2.3. Data Extraction and Management
2.4. Assessment of Quality of Studies
3. Results
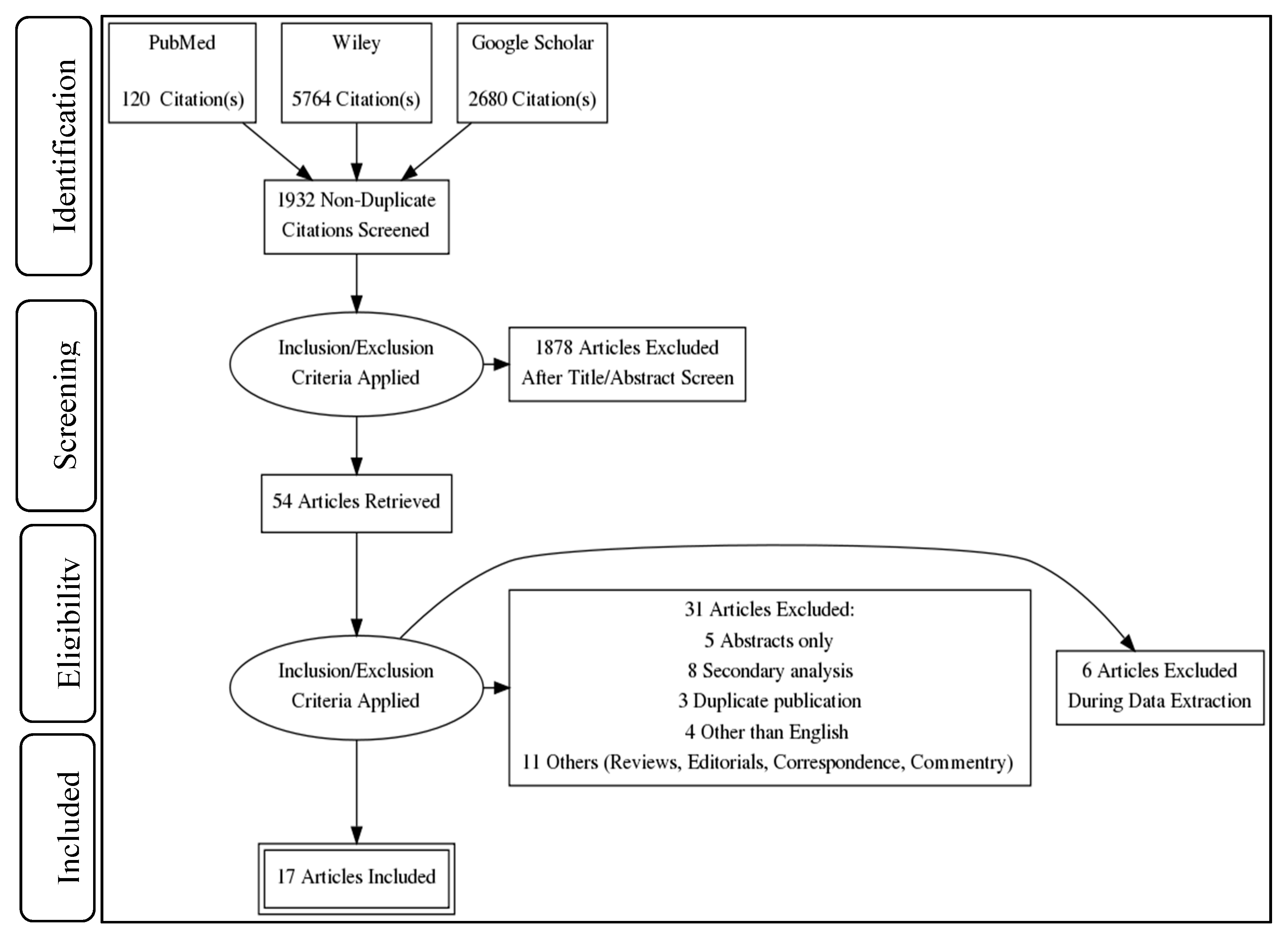
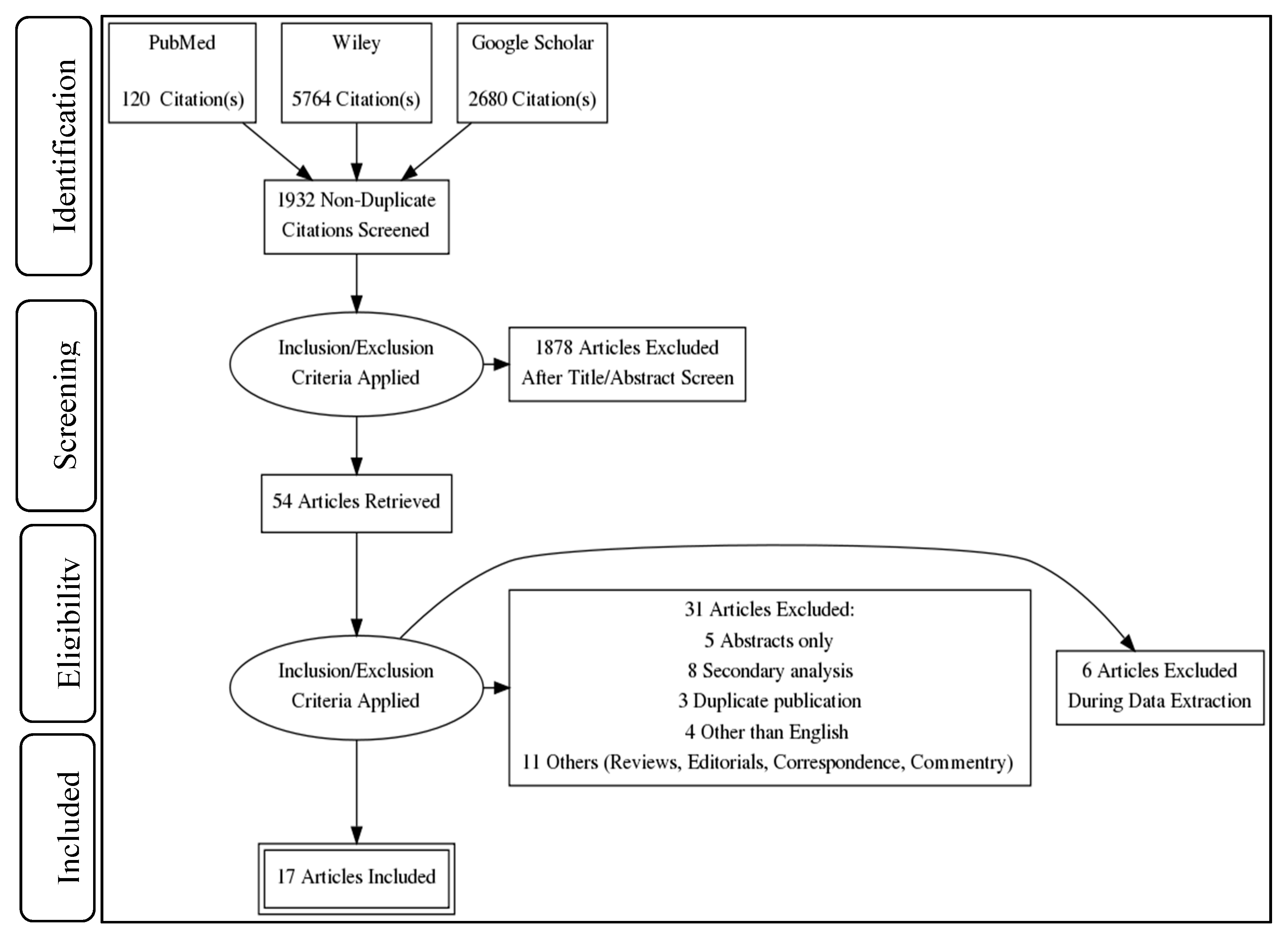
3.1. Search Strategy and Study Selection
3.2. Studies Characteristics
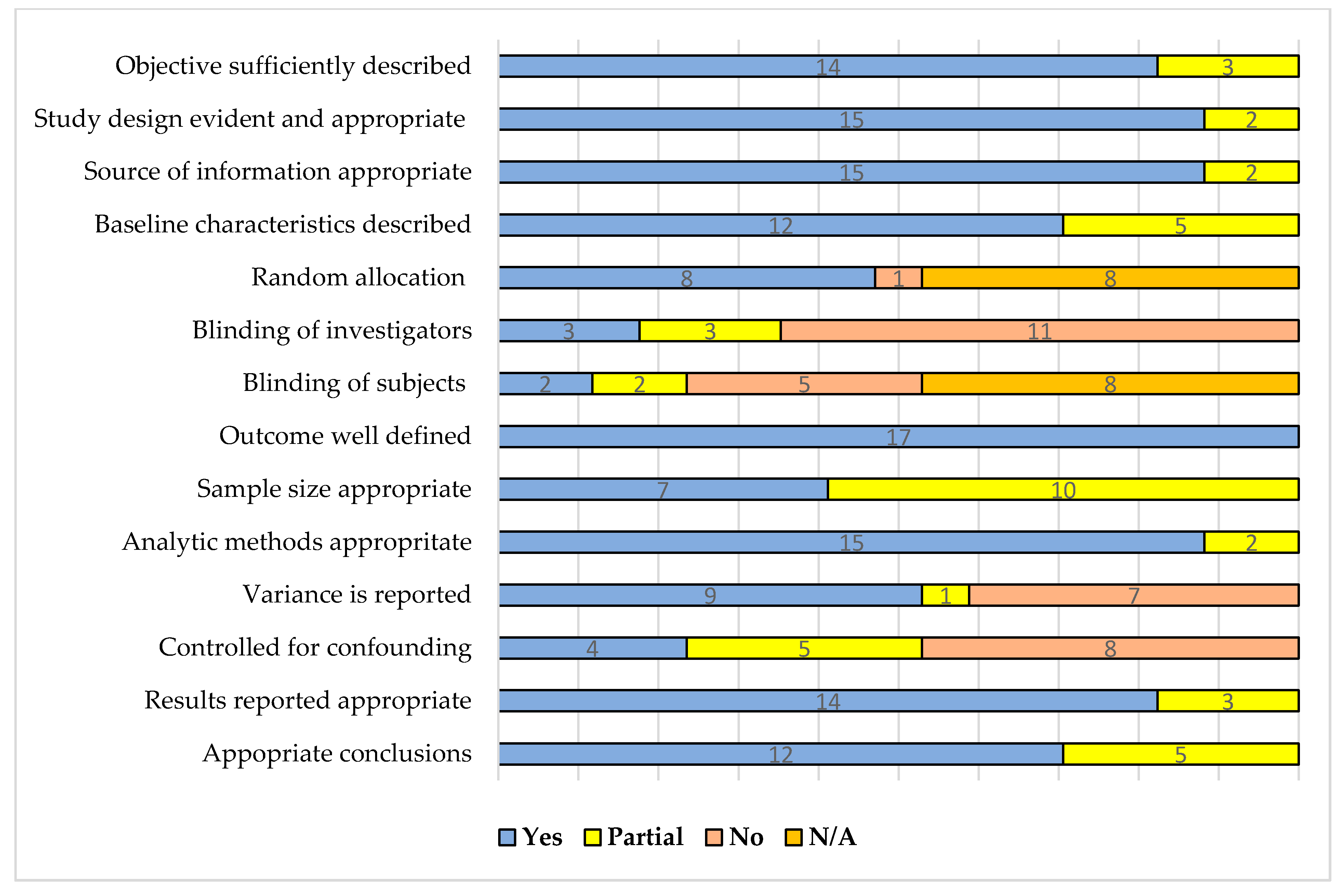
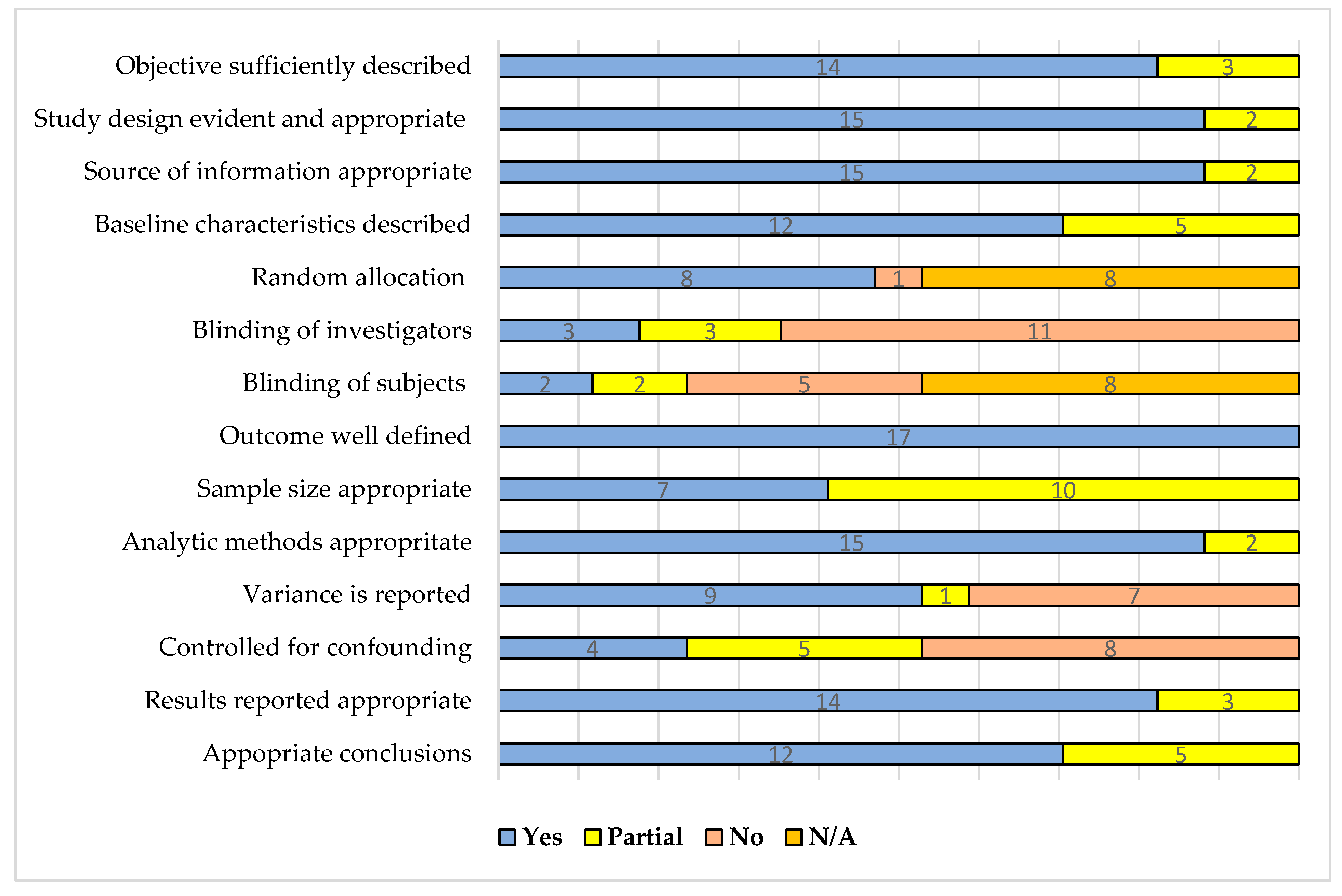
3.3. Studies Quality Assessment
4. Discussion
4.1. Health System Strategy and Policy Implications
4.2. Future Research Implications
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Appendix A
| Date: May 2021 | ||
| Keywords/Mesh Terms | Query | Items Found |
|---|---|---|
| Pubmed | ||
| 1. | (mHealth) OR (mobile health) OR (Telehealth) OR (Telecommunication) | 153,267 |
| 2. | (Teach-back ) OR (Teach-back experience) OR (Teach-back communication) OR (Closing the loop) OR (Discharge counselling) | 320 |
| 3. | (Hospital readmission reduction) OR (Hospital readmissions reduction) OR (Readmission reduction) OR (Frequent admissions reduction) OR (frequently admitted patients reduction) | 3851 |
| 4. | (((Teach-back ) OR (Teach-back experience) OR (Teach-back communication) OR (Closing the loop) OR (Discharge counselling)) OR ((mhealth) OR (mobile health) OR (Telehealth) OR (Telecommunication))) AND (((Hospital readmission reduction) OR (Hospital readmissions reduction) OR (Readmission reduction) OR (Frequent admissions reduction) OR (frequently admitted patients reduction))) | 120 |
| Wiley | ||
| 1. | (mhealth) OR (mobile health) OR (Telehealth) OR (Telecommunication) | 138 |
| 2. | (Teach-back ) OR (Teach-back experience) OR (Teach-back communication) OR (Closing the loop) OR (Discharge counselling) | 332,905 |
| 3. | (Hospital readmission reduction) OR (Hospital readmissions reduction) OR (Readmission reduction) OR (Frequent admissions reduction) OR (frequently admitted patients reduction) | 21,751 |
| 4. | (((Teach-back ) OR (Teach-back experience) OR (Teach-back communication) OR (Closing the loop) OR (Discharge counselling)) OR ((mhealth) OR (mobile health) OR (Telehealth) OR (Telecommunication))) AND (((Hospital readmission reduction) OR (Hospital readmissions reduction) OR (Readmission reduction) OR (Frequent admissions reduction) OR (frequently admitted patients reduction))) | 5764 |
| Google scholar | ||
| 1. | (mhealth) OR (mobile health) OR (Telehealth) OR (Telecommunication) | 3,940,000 |
| 2. | (Teach-back ) OR (Teach-back experience) OR (Teach-back communication) OR (Teach-back) OR (Teach-back communication) | 8960 |
| 3. | (Hospital readmission reduction) OR (Hospital readmissions reduction) OR (Readmission reduction) OR ( readmissions reduction) | 66,900 |
| 4. | (((Teach-back ) OR (Teach-back experience) OR (Teach-back communication) OR (Closing the loop) OR (Discharge counselling)) OR ((mhealth) OR (mobile health) OR (Telehealth) OR (Telecommunication))) AND (((Hospital readmission reduction) OR (Hospital readmissions reduction) OR (Readmission reduction) OR (Frequent admissions reduction) OR (frequently admitted patients reduction))) | 2680 |
| Grand Total | 8564 | |
Appendix B
| Serial | Questions for Quantitative Scoring | Yes (2) | Partial (1) | No (0) | N/A |
| 1. | Question/objective sufficiently described? | ||||
| 2. | Study design evident and appropriate? | ||||
| 3. | Method of subject/comparison group selection or source of information /input variables described and appropriate? | ||||
| 4. | Subject (and comparison group, if applicable) characteristics sufficiently described? | ||||
| 5. | If interventional and random allocation was possible, was it described? | ||||
| 6. | If interventional and blinding of investigators was possible, was it reported? | ||||
| 7. | If interventional and blinding of subjects was possible, was it reported? | ||||
| 8. | Outcome and (if applicable) exposure measure(s) well defined and robust to measurement/misclassification bias? Means of assessment reported? | ||||
| 9. | Sample size appropriate? | ||||
| 10. | Analytical methods described/justified and appropriate? | ||||
| 11. | Some estimate of variance is reported for the main results? | ||||
| 12. | Controlled for confounding? | ||||
| 13. | Results reported in sufficient detail? | ||||
| 14. | Conclusions supported by the results? |
Appendix C
| Total | Study 1 | Study 2 | Study 3 | Study 4 | Study 5 | Study 6 | Study 7 | Study 8 | Study 9 | Study 10 | Study 11 | Study 12 | Study 13 | Study 14 | Study 15 | Study 16 | Study 17 | ||||
| Criteria | Yes | Partial | No | NA | Celler B et al | Dastoon M et al | De Walt et al | Dinesen B et al | Estaban C et al | Frederix et al | Greenup EP et al | Howie-Esquivel J et al | Krumholz HM et al | Ong MK | Pinnock H et al | Rosen OZ et al | Rosnar BI et al | Sorknaes ED et al | Takahashi PY et al | Wang Y et al | White M et al |
| Objective sufficiently described | 14 | 3 | 0 | 0 | 2 | 2 | 1 | 1 | 1 | 2 | 2 | 2 | 2 | 2 | 2 | 2 | 2 | 2 | 2 | 2 | 2 |
| Study design evident and appropriate | 15 | 2 | 0 | 0 | 2 | 2 | 2 | 2 | 1 | 2 | 1 | 2 | 2 | 2 | 2 | 2 | 2 | 2 | 2 | 2 | 2 |
| Source of information appropriate | 15 | 2 | 0 | 0 | 2 | 2 | 2 | 2 | 2 | 1 | 1 | 2 | 2 | 2 | 2 | 2 | 2 | 2 | 2 | 2 | 2 |
| Baseline characteristics described | 12 | 5 | 0 | 0 | 2 | 2 | 2 | 2 | 2 | 1 | 1 | 2 | 2 | 2 | 2 | 2 | 2 | 1 | 1 | 1 | 2 |
| Random allocation | 8 | 1 | 8 | NA | 2 | 2 | 2 | NA | 2 | NA | NA | 2 | 2 | 2 | NA | NA | 0 | 2 | 2 | NA | |
| Blinding of investigators | 3 | 3 | 12 | 0 | NA | 2 | 2 | 2 | NA | 2 | NA | NA | 2 | 2 | 2 | NA | NA | 0 | 2 | 1 | NA |
| Blinding of subjects | 2 | 2 | 5 | 8 | NA | 1 | 1 | 2 | NA | 2 | NA | NA | 0 | 0 | 0 | NA | NA | 0 | 0 | 2 | NA |
| Outcome well defined | 17 | 0 | 0 | 0 | 2 | 2 | 2 | 2 | 2 | 2 | 2 | 2 | 2 | 2 | 2 | 2 | 2 | 2 | 2 | 2 | 2 |
| Sample size appropriate | 7 | 10 | 0 | 0 | 1 | 1 | 2 | 1 | 2 | 1 | 1 | 1 | 1 | 2 | 2 | 2 | 2 | 1 | 1 | 1 | 2 |
| Analytic methods appropriate | 15 | 2 | 0 | 0 | 2 | 2 | 2 | 1 | 2 | 1 | 2 | 2 | 2 | 2 | 2 | 2 | 2 | 2 | 2 | 2 | 2 |
| Variance is reported | 9 | 1 | 7 | 0 | 2 | 2 | 2 | 2 | 2 | 0 | 2 | 2 | 2 | 2 | 1 | 0 | 0 | 0 | 0 | 0 | 0 |
| Controlled for confounding | 4 | 5 | 8 | 0 | 2 | 0 | 1 | 0 | 0 | 0 | 1 | 1 | 2 | 2 | 1 | 2 | 1 | 0 | 0 | 0 | 0 |
| Results reported appropriate | 14 | 3 | 0 | 0 | 2 | 2 | 1 | 1 | 2 | 1 | 2 | 2 | 2 | 2 | 2 | 2 | 2 | 2 | 2 | 2 | 2 |
| Conclusions appropriate | 12 | 5 | 2 | 1 | 1 | 2 | 1 | 1 | 2 | 2 | 2 | 2 | 1 | 2 | 2 | 2 | 2 | 2 | 2 | ||
| Summary Score | - | - | - | - | 95 | 82 | 82 | 79 | 77 | 64 | 77 | 91 | 89 | 93 | 82 | 91 | 86 | 57 | 71 | 75 | 82 |
| Total score/Numerator | 147 | 43 | 33 | 16 | 21 | 23 | 23 | 22 | 17 | 18 | 17 | 20 | 25 | 26 | 23 | 20 | 19 | 16 | 20 | 21 | 18 |
| Denominator | 28 | 14 | 22 | 28 | 28 | 28 | 22 | 28 | 22 | 22 | 28 | 28 | 28 | 22 | 22 | 28 | 28 | 28 | 22 | ||
Appendix D
| Studies Included in the Systematic Review | Total Participants | SQS (%) | |
| Average | Range | ||
| All (n = 17) | 5713 | 81 | 57–95 |
| 3194 | 81 | 57–95 |
| 2519 | 81 | 71–93 |
| 2582 | 80 | 64–93 |
| 684 | 79 | 64–89 |
| 1898 | 82 | 71–93 |
| 3131 | 82 | 57–95 |
| 2510 | 83 | 57–95 |
| 621 | 80 | 77–82 |
| mHealth (n = 11) | 3708 | 78 | 57–95 |
| 1465 | 76 | 57–95 |
| 2243 | 81 | 71–93 |
| 2271 | 77 | 64–93 |
| 373 | 71 | 64–79 |
| 1898 | 82 | 71–93 |
| 1437 | 78 | 57–95 |
| 1092 | 79 | 77–95 |
| 906 | 77 | - |
| Teach—Back Communication (n = 6) | 2005 | 86 | 82–91 |
| 1729 | 87 | 82–91 |
| 276 | 82 | - |
| 311 | 84 | 82–89 |
| 1694 | 88 | 82–91 |
| 1418 | 91 | - |
| 276 | 82 | - |
References
- Gerhardt, G.; Yemane, A.; Hickman, P.; Oelschlaeger, A.; Rollins, E.; Brennan, N. Medicare Readmission Rates Showed Meaningful Decline in 2012. Medicare Medicaid Res. Rev. 2013, 3. [Google Scholar] [CrossRef] [Green Version]
- Almkuist, K.D. Using Teach-Back Method to Prevent 30-Day Readmissions in Patients with Heart Failure: A Systematic Review. MedSurg Nurs. 2017, 26, 5. [Google Scholar]
- Bradley, E.H.; Curry, L.; Horwitz, L.I.; Sipsma, H.; Thompson, J.W.; Elma, M.; Walsh, M.N.; Krumholz, H.M. Contemporary evidence about hospital strategies for reducing 30-day readmissions: A national study. J. Am. Coll. Cardiol. 2012, 60, 607–614. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Al-Damluji, M.S.; Dzara, K.; Hodshon, B.; Punnanithinont, N.; Krumholz, H.M.; Chaudhry, S.I.; Horwitz, L.I. Association of Discharge Summary Quality with Readmission Risk for Patients Hospitalized with Heart Failure Exacerbation. Circ. Cardiovasc. Qual. Outcomes 2015, 8, 109–111. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fernandez-Lazaro, C.I.; García-González, J.M.; Adams, D.P.; Fernandez-Lazaro, D.; Mielgo-Ayuso, J.; Caballero-Garcia, A.; Racionero, F.M.; Córdova, A.; Miron-Canelo, J.A. Adherence to treatment and related factors among patients with chronic conditions in primary care: A cross-sectional study. BMC Fam. Pract. 2019, 20, 1–12. [Google Scholar] [CrossRef]
- Farris, C. The Teach Back Method. Home Healthc. Now 2015, 33, 344–345. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jager, A.J.; Wynia, M.K. Who Gets a Teach-Back? Patient-Reported Incidence of Experiencing a Teach-Back. J. Health Commun. 2012, 17, 294–302. [Google Scholar] [CrossRef]
- Smith, A. Smartphone Ownership-2013 Update; Pew Research Center: Washington, DC, USA, 2013; Volume 12. [Google Scholar]
- Hamine, S.; Gerth-Guyette, E.; Faulx, D.; Green, B.B.; Ginsburg, A.S. Impact of mHealth Chronic Disease Management on Treatment Adherence and Patient Outcomes: A Systematic Review. J. Med Internet Res. 2015, 17, e52. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Boutwell, A. Reduced readmissions: Reform’s low-hanging fruit. Healthc. Exec. 2011, 26, 86–89. [Google Scholar]
- Mansukhani, R.P.; Bridgeman, M.; Candelario, D.; Eckert, L.J. Exploring Transitional Care: Evidence-Based Strategies for Improving Provider Communication and Reducing Readmissions. Formul. Manag. 2015, 40, 690–694. [Google Scholar]
- Mahmoudi, S.; Taghipour, H.R.; Javadzadeh, H.R.; Ghane, M.R.; Goodarzi, H.; Motamedi, M.H.K. Hospital Readmission Through the Emergency Department. Trauma Mon. 2016, 21, 21. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Azuhairi, A.; Arshad, J. Clients’experience and satisfaction of utilizing healthcare services in a community-based health insurance program in lahore, pakistan. Int. J. Public Health Clin. Sci. 2020, 7, 97–112. [Google Scholar]
- Ghimire, P.; Sapkota, V.P.; Poudyal, A.K. Factors Associated with Enrolment of Households in Nepal’s National Health Insurance Program. Int. J. Health Policy Manag. 2019, 8, 636–645. [Google Scholar] [CrossRef] [PubMed]
- Ahmed, S.; Ahmed, M.W.; Hasan, M.; Mehdi, G.G.; Islam, Z.; Rehnberg, C.; Niessen, L.; Khan, J. Assessing the incidence of catastrophic health expenditure and impoverishment from out-of-pocket payments and their determinants in Bangladesh: Evidence from the nationwide Household Income and Expenditure Survey 2016. Int. Health 2021, 15, 1–13. [Google Scholar]
- Bali, A.S.; Ramesh, M. Governing healthcare in India: A policy capacity perspective. Int. Rev. Adm. Sci. 2021, 87, 275–293. [Google Scholar] [CrossRef]
- Karunaratna, S.; Ranasinghe, T.; Chandraratne, N.; De Silva, A. The Social Health Insurance Scheme for Public Sector Employees in Sri Lanka and Its Effect on Reducing the Financial Burden of Illness. Asia Pac. J. Public Health 2019, 31, 584–593. [Google Scholar] [CrossRef]
- Reshmi, B.; Unnikrishnan, B.; Parsekar, S.S.; Rajwar, E.; Vijayamma, R.; Venkatesh, B.T. Health insurance awareness and its uptake in India: A systematic review protocol. BMJ Open 2021, 11, e043122. [Google Scholar] [CrossRef]
- Hayden, D.M.; Pinzon, M.M.; Francescatti, A.B.; Edquist, S.C.; Malczewski, M.R.; Jolley, J.M.; Brand, M.I.; Saclarides, T.J. Hospital Readmission for Fluid and Electrolyte Abnormalities Following Ileostomy Construction: Preventable or Unpredictable? J. Gastrointest. Surg. 2013, 17, 298–303. [Google Scholar] [CrossRef] [PubMed]
- Hekmatpou, D.; Mohammadi, E.; Ahmadi, F. Barriers of readmission control among patients with congestive heart failure: A qualitative study. J. Arak Univ. Med Sci. 2008, 11, 49–58. [Google Scholar]
- Coffey, A.; Leahy-Warren, P.; Savage, E.; Hegarty, J.; Cornally, N.; Day, M.R.; Sahm, L.; O’Connor, K.; O’Doherty, J.; Liew, A.; et al. Interventions to Promote Early Discharge and Avoid Inappropriate Hospital (Re)Admission: A Systematic Review. Int. J. Environ. Res. Public Health 2019, 16, 2457. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sansano-Nadal, O.; Giné-Garriga, M.; Brach, J.S.; Wert, D.M.; Jerez-Roig, J.; Guerra-Balic, M.; Oviedo, G.; Fortuño, J.; Gómara-Toldrà, N.; Soto-Bagaria, L.; et al. Exercise-Based Interventions to Enhance Long-Term Sustainability of Physical Activity in Older Adults: A Systematic Review and Meta-Analysis of Randomized Clinical Trials. Int. J. Environ. Res. Public Health 2019, 16, 2527. [Google Scholar] [CrossRef] [Green Version]
- Sooknarine-Rajpatty, J.; Auyeung, A.B.; Doyle, F. A Systematic Review Protocol of the Barriers to Both Physical Activity and Obesity Counselling in the Secondary Care Setting as Reported by Healthcare Providers. Int. J. Environ. Res. Public Health 2020, 17, 1195. [Google Scholar] [CrossRef] [Green Version]
- Georgiou, M.; Morison, G.; Smith, N.; Tieges, Z.; Chastin, S. Mechanisms of Impact of Blue Spaces on Human Health: A Systematic Literature Review and Meta-Analysis. Int. J. Environ. Res. Public Health 2021, 18, 2486. [Google Scholar] [CrossRef] [PubMed]
- Kmet, L.M.; Cook, L.S.; Lee, R.C. Standard Quality Assessment Criteria for Evaluating Primary Research Papers from a Variety of Fields; Health Technology Assessment, Unit Alberta Heritage Foundation for Medical Research: Edmonton, AB, Canada, 2004; pp. 1–22. [Google Scholar]
- Celler, B.; Varnfield, M.; Nepal, S.; Sparks, R.; Li, J.; Jayasena, R.; Agboola, S.; Bergmo, T. Impact of At-Home Telemonitoring on Health Services Expenditure and Hospital Admissions in Patients with Chronic Conditions: Before and After Control Intervention Analysis. JMIR Med. Inform. 2017, 5, e29. [Google Scholar] [CrossRef] [Green Version]
- Dinesen, B.; Haesum, L.K.; Soerensen, N.; Nielsen, C.; Grann, O.; Hejlesen, O.; Toft, E.; Ehlers, L.H. Using preventive home monitoring to reduce hospital admission rates and reduce costs: A case study of telehealth among chronic obstructive pulmonary disease patients. J. Telemed. Telecare 2012, 18, 221–225. [Google Scholar] [CrossRef] [PubMed]
- Esteban, C.; Moraza, J.; Iriberri, M.; Aguirre, U.; Goiria, B.; Quintana, J.M.; Aburto, M.; Capelastegui, A. Outcomes of a telemonitoring-based program (telEPOC) in frequently hospitalized COPD patients. Int. J. Chronic Obstr. Pulm. Dis. 2016, 11, 2919–2930.e4. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rosner, B.I.; Gottlieb, M.; Anderson, W.N. Effectiveness of an Automated Digital Remote Guidance and Telemonitoring Platform on Costs, Readmissions, and Complications After Hip and Knee Arthroplasties. J. Arthroplast. 2018, 33, 988–996. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sorknæs, A.D.; Madsen, H.; Hallas, J.; Jest, P.; Hansen-Nord, M. Nurse tele-consultations with discharged COPD patients reduce early readmissions–an interventional study. Clin. Respir. J. 2011, 5, 26–34. [Google Scholar] [CrossRef]
- Wang, Y.; Li, M.; Zhao, X.; Pan, X.; Lu, M.; Lu, J.; Hu, Y. Effects of continuous care for patients with type 2 diabetes using mobile health application: A randomised controlled trial. Int. J. Health Plan. Manag. 2019, 34, 1025–1035. [Google Scholar] [CrossRef]
- Frederix, I.; Vanderlinden, L.; Verboven, A.-S.; Welten, M.; Wouters, D.; De Keulenaer, G.; Ector, B.; Elegeert, I.; Troisfontaines, P.; Weytjens, C.; et al. Long-term impact of a six-month telemedical care programme on mortality, heart failure readmissions and healthcare costs in patients with chronic heart failure. J. Telemed. Telecare 2019, 25, 286–293. [Google Scholar] [CrossRef]
- Greenup, E.P.; McCusker, M.; Potts, B.A.; Bryett, A. The Efficacy of Telemedicine-Supported Discharge Within an In-Home Model of Care. Telemed. e-Health 2017, 23, 763–765. [Google Scholar] [CrossRef] [PubMed]
- Ong, M.K.; Romano, P.S.; Edgington, S.; Aronow, H.U.; Auerbach, A.D.; Black, J.T.; De Marco, T.; Escarce, J.J.; Evangelista, L.S.; Hanna, B. Effectiveness of remote patient monitoring after discharge of hospitalized patients with heart failure: The better effectiveness after transition–heart failure (BEAT-HF) randomized clinical trial. JAMA Intern. Med. 2016, 176, 310–318. [Google Scholar] [CrossRef]
- Pinnock, H.; Hanley, J.; McCloughan, L.; Todd, A.; Krishan, A.; Lewis, S.; Stoddart, A.; Van Der Pol, M.; MacNee, W.; Sheikh, A.; et al. Effectiveness of telemonitoring integrated into existing clinical services on hospital admission for exacerbation of chronic obstructive pulmonary disease: Researcher blind, multicentre, randomised controlled trial. BMJ 2013, 347, f6070. [Google Scholar] [CrossRef] [Green Version]
- Takahashi, P.Y.; Pecina, J.L.; Upatising, B.; Chaudhry, R.; Shah, N.D.; Van Houten, H.; Cha, S.; Croghan, I.; Naessens, J.M.; Hanson, G.J. A Randomized Controlled Trial of Telemonitoring in Older Adults with Multiple Health Issues to Prevent Hospitalizations and Emergency Department Visits. Arch. Intern. Med. 2012, 172, 773–779. [Google Scholar] [CrossRef] [Green Version]
- Dastoom, M.; Elahi, N.; Baraz, S.; Latifi, S.M. The Effects of Group Education with the Teach-Back Method on Hospital Readmission Rates of Heart Failure Patients. Jundishapur J. Chronic Dis. Care 2016, 5, 5. [Google Scholar] [CrossRef] [Green Version]
- De Walt, D.; Malone, R.M.; Bryant, M.; Kosnar, M.C.; Corr, K.; Rothman, R.L.; Sueta, C.; Pignone, M.P. A heart failure self-management program for patients of all literacy levels: A randomized, controlled trial [ISRCTN11535170]. BMC Health Serv. Res. 2006, 6, 30. [Google Scholar] [CrossRef] [Green Version]
- Howie-Esquivel, J.; Spicer, J.G. Association of Partner Status and Disposition with Rehospitalization in Heart Failure Patients. Am. J. Crit. Care 2012, 21, e65–e73. [Google Scholar] [CrossRef]
- Krumholz, H.M.; Amatruda, J.; Smith, G.; Mattera, J.; Roumanis, S.; Radford, M.J.; Crombie, P.; Vaccarino, V. Randomized trial of an education and support intervention to prevent readmission of patients with heart failure. J. Am. Coll. Cardiol. 2002, 39, 83–89. [Google Scholar] [CrossRef] [Green Version]
- Rosen, O.Z.; Fridman, R.; Rosen, B.T.; Shane, R.; Pevnick, J.M. Medication adherence as a predictor of 30-day hospital readmissions. Patient Prefer. Adherence 2017, 11, 801–810. [Google Scholar] [CrossRef] [Green Version]
- White, M.; Garbez, R.; Carroll, M.; Brinker, E.; Howie-Esquivel, J. Is “Teach-Back” Associated with Knowledge Retention and Hospital Readmission in Hospitalized Heart Failure Patients? J. Cardiovasc. Nurs. 2013, 28, 137–146. [Google Scholar] [CrossRef]
- Dinh, T.T.H.; Bonner, A.; Clark, R.; Ramsbotham, J.; Hines, S. The effectiveness of the teach-back method on adherence and self-management in health education for people with chronic disease: A systematic review. JBI Evid. Synth. 2016, 14, 210–247. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Holt, H.D. The Readmission Difference: Examining the Negative Impact of Hospital Readmissions on Financial Performance. Int. J. Health Sci. 2017, 5, 31–41. [Google Scholar]
- Graham, K.L.; Auerbach, A.; Schnipper, J.L.; Flanders, S.A.; Kim, C.S.; Robinson, E.; Ruhnke, G.W.; Thomas, L.R.; Kripalani, S.; Vasilevskis, E.E.; et al. Preventability of Early Versus Late Hospital Readmissions in a National Cohort of General Medicine Patients. Ann. Intern. Med. 2018, 168, 766–774. [Google Scholar] [CrossRef]
- Kansagara, D.; Chiovaro, J.C.; Kagen, D.; Jencks, S.; Rhyne, K.; O’Neil, M.; Kondo, K.; Relevo, R.; Motu’apuaka, M.; Freeman, M.; et al. Transitions of Care from Hospital to Home: An Overview of Systematic Reviews and Recommendations for Improving Transitional Care in the Veterans Health Administration; VA-ESP Project #05-225; Evidence-based Synthesis Program (ESP) Center Portland VA Medical Center: Portland, OR, USA, 2015; pp. 1–62. [Google Scholar]
- Kitsiou, S.; Paré, G.; Jaana, M.; Gerber, B. Effectiveness of mHealth interventions for patients with diabetes: An overview of systematic reviews. PLoS ONE 2017, 12, e0173160. [Google Scholar] [CrossRef] [Green Version]
- Kitsiou, S.; Vatani, H.; Paré, G.; Gerber, B.S.; Buchholz, S.W.; Kansal, M.M.; Leigh, J.; Creber, R.M.M. Effectiveness of Mobile Health Technology Interventions for Patients with Heart Failure: Systematic Review and Meta-analysis. Can. J. Cardiol. 2021, 37, 1248–1259. [Google Scholar] [CrossRef] [PubMed]
- Artetxe, A.; Beristain, A.; Graña, M. Predictive models for hospital readmission risk: A systematic review of methods. Comput. Methods Programs Biomed. 2018, 164, 49–64. [Google Scholar] [CrossRef] [PubMed]
- Lavenberg, J.G.; Leas, B.; Umscheid, C.A.; Williams, K.; Goldmann, D.R.; Kripalani, S. Assessing preventability in the quest to reduce hospital readmissions. J. Hosp. Med. 2014, 9, 598–603. [Google Scholar] [CrossRef] [Green Version]
- Walsh, E.G.; Wiener, J.M.; Haber, S.; Bragg, A.; Freiman, M.; Ouslander, J.G. Potentially avoidable hospitalizations of dually eligible Medicare and Medicaid beneficiaries from nursing facility and home-and community-based services waiver programs. J. Am. Geriatr. Soc. 2012, 60, 821–829. [Google Scholar] [CrossRef]
- Pavic, M.; Klaas, V.; Theile, G.; Kraft, J.; Tröster, G.; Blum, D.; Guckenberger, M. Mobile Health Technologies for Continuous Monitoring of Cancer Patients in Palliative Care Aiming to Predict Health Status Deterioration: A Feasibility Study. J. Palliat. Med. 2020, 23, 678–685. [Google Scholar] [CrossRef]
- Piette, J.D.; List, J.; Rana, G.K.; Townsend, W.; Striplin, D.; Heisler, M. Mobile Health Devices as Tools for Worldwide Cardiovascular Risk Reduction and Disease Management. Circulation 2015, 132, 2012–2027. [Google Scholar] [CrossRef] [Green Version]
- Kripalani, S.; Weiss, B.D. Teaching about health literacy and clear communication. J. Gen. Intern. Med. 2006, 21, 888–890. [Google Scholar] [CrossRef] [PubMed]
- Talevski, J.; Shee, A.W.; Rasmussen, B.; Kemp, G.; Beauchamp, A. Teach-back: A systematic review of implementation and impacts. PLoS ONE 2020, 15, e0231350. [Google Scholar] [CrossRef] [PubMed]
- Ulrich, L.; Welty, M.; Henderson, A.; Allen, E. Quality improvement approach to increasing respiratory therapist driven teach back style asthma education. J. Asthma 2021, 1–6. [Google Scholar] [CrossRef] [PubMed]
- Catalyst, N. Hospital readmissions reduction program (HRRP). NEJM Catalyst 2018.
- Hansen, L.O.; Young, R.S.; Hinami, K.; Leung, A.; Williams, M.V. Interventions to Reduce 30-Day Rehospitalization: A Systematic Review. Ann. Intern. Med. 2011, 155, 520–528. [Google Scholar] [CrossRef]
- Gire, N.; Farooq, S.; Naeem, F.; Duxbury, J.; McKeown, M.; Kundi, P.S.; Chaudhry, I.B.; Husain, N. mHealth based interventions for the assessment and treatment of psychotic disorders: A systematic review. mHealth 2017, 3, 33. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Alluhaidan, A.; Lee, E.; Alnosayan, N.; Chatterjee, S.; Houston-Feenstra, L.; Dysinger, W.; Kagoda, M. Designing Patient-Centered mHealth Technology Intervention to Reduce Hospital Readmission for Heart-Failure Patients. In Proceedings of the 2015 48th Hawaii International Conference on System Sciences, Kauai, HI, USA, 5–8 January 2015; pp. 2886–2895. [Google Scholar]

{kind=link}
{kind=link}
| Population | |
|---|---|
| Age | >20 years of age |
| Gender | Both genders |
| Disease status | Patients with non-communicable diseases (NCDs) |
| Location | Any country and region |
| Intervention/Exposure | |
| mHealth/telemedicine/telehealth | Mobile health communication through telephone and/or short text messages and/or Delivery of health services via remote telecommunications |
| Teach-back communication | Patient education and (or) information about discharge instructions allowing them to restate the instructions in their own words. |
| Setting | Outpatient department, admitted cases, or both |
| Control | |
| Standard care | Patients with routine/usual care |
| Outcome | |
| Primary outcome | Hospital readmissions or frequent hospitalizations reduction |
| Period of observation | 30–180 days after index discharge |
| Study Design | |
| Study design included | Quantitative study design |
| Time Period | |
| Searched till | June 2020 |
| Exclusion Criteria | Duplicate publication |
| Articles not specifying hospital readmission reduction | |
| Where full-text articles could not be recovered. | |
| Studies that were neither available in English nor could be translated | |
| Studies that have utilized secondary data analysis | |
| Qualitative studies, opinion pieces, theoretical papers, non-peer-reviewed manuscripts, abstracts, reviews, editorials, commentaries, correspondence. | |
| Author, Publication Year | Country | Design | Condition | Sample Size (n) | Intervention | Key Findings |
|---|---|---|---|---|---|---|
| Celler B et al. 2017 [26] | Australia | BACI | Multiple chronic conditions | 237 | mHealth | Intervention group showed a 53.2% reduction in the rate of predicted unscheduled readmission to hospital (p = 0.02) and a reduction in mortality between 41.3% and 44.5% as compared to the controls. Statistical tests: Chi-square test, Fisher exact test for categorical variables, the two-sample t-test for continuous variables, Wilcoxon rank-sum test for skewed variables. Quality score: 95% |
| Dastoon M et al. 2016 [37] | Iran | RCT | HF | 100 | Teach-back communication | Greater time spent in teach-back communication significantly reduced hospital readmissions by 56.2% in the intervention group (44 vs. 21, p = 0.04). Statistical tests: Man–Whitney U and Chi-square tests Quality score: 82% |
| De Walt DA et al. 2006 [38] | USA | RCT | HF | 123 | Teach-back communication | Intervention group had a decreased rate of hospitalization [adjusted incidence rate ratios (IRR)] = 0.53; CI 0.32, 0.89). Statistical technique: Multivariate regression analysis Quality score: 82% |
| Dinesen B et al. 2012 [27] | Denmark | RCT | COPD | 111 | mHealth | Intervention group demonstrated a significantly reduced (p = 0.04) requirement of hospitalization and 30-day readmissions. Statistical tests: Kaplan–Meier survival analysis, log rank test Quality score: 79% |
| Estaban C et al. 2016 [28] | Spain | NR-OS | COPD | 197 | mHealth | Intervention group had significantly lower rates of 30 days readmission (OR = 0.46, 95% CI = 0.29–0.74; p < 0.001). Statistical tests: Chi-square test for qualitative variables and a two-sampled Wilcoxon test for continuous variables. Quality score: 77% |
| Frederix I et al. 2018 [32] | Belgium | Multicenter prospective RCT | HF | 142 | mHealth | The number of days lost due to readmissions was significantly lower in the intervention group (p = 0.04). Statistical tests: Independent t-tests (parametric) or Mann–Whitney U tests (nonparametric) for continuous variables and Chi-square test for categorical variables, Cox regression model for hazards ratio Quality score: 64% |
| Greenup EP et al. 2017 [33] | Australia | Clinical trial (non-randomized) | Multiple chronic conditions | 345 | mHealth | No significant difference in rates of readmission in intervention group. Statistical tests: Chi-square test, binary logistic regression model. Quality score: 77% |
| Howie-Esquivel J et al. 2015 [39] | USA | Cross-sectional | HF | 1033 | Teach-back communication | Usual care group was 1.5 times more likely to be hospitalized (95% CI: 1.2–1.9; p = 0.001) compared to intervention group. Statistical technique: Multiple logistic regression. Quality score: 91% |
| Krumholz HM et al. 2002 [40] | USA | RCT | HF | 88 | Teach-back communication | After adjusting for clinical and demographic characteristics, the intervention group had a significantly lower risk of readmission as compared with the control group (Hazard ratio = 0.56, 95% CI: 0.32, 0.96; p = 0.03) Statistical tests: Mantel–Haenszel chi-square, Cox proportional hazards model. Quality score: 89% |
| Ong MK 2016 [34] | USA | RCT | HF | 1437 | mHealth | Telephone calls and TM did not reduce 180-day readmissions. Statistical technique: Multivariate logistic regression. Quality score: 93% |
|
Pinnock H et al. 2013 [35] | UK | RCT | COPD | 256 | mHealth | TM was not effective in postponing hospital readmission for patients with ECOPD. Statistical technique: Kaplan–Meier survival analysis, using Cox proportional hazards model. Quality Score: 82% |
|
Rosen OZ et al. 2017 [41] | USA | CS | Multiple chronic conditions | 385 | Teach-back communication | Patients with combined low and intermediate adherence had readmission rates of 2% compared to 9.3% for patients with high adherence (p = 0.05) Statistical tests: Wilcoxon rank-sum test and Chi-square test Quality score: 91% |
|
Rosnar BI et al. 2018 [29] | USA | Multicenter CS | Hip and knee arthroplasties | 558 | mHealth | A statistically significant reduction in readmission rate in the mHealth arm (3.4%; 95% CI, 0.1–6.7%) vs the control (12.2%; 95% CI, 6.4–18.0%) (p = 0.01). Statistical tests: Fisher’s exact test and t-test Quality score: 86% |
| Sorknaes AD et al. 2011 [30] | Denmark | Clinical trial (non-randomized) | COPD | 100 | mHealth | In intervention group TM consultation resulted in 12% readmissions vs 22% in control group, days of readmission were reduced by about 20 days. Statistical Tests: Kaplan–Meier survival analysis and multivariate Cox regression analysis Quality score: 57% |
| Takahashi PY et al. 2012 [36] | USA | RCT | Multiple chronic conditions | 205 | mHealth | No statistical difference was noted in hospitalizations and ER visits between the TM group (63.7%) and the group receiving usual care (57.3%) (p = 0.345) Statistical tests: Wilcoxon rank sum test, two-sample t-test and Chi- squared test Quality score: 71% |
|
Wang Y et al. 2019 [31] | China | RCT | Type 2 diabetes | 120 | mHealth | Intervention significantly (p < 0.05) reduced hospitalization in the intervention group. Statistical tests: Chi-squared tests for categorical variables and independent sample t-tests for continuous variables Quality score: 75% |
|
White M et al. 2013 [42] | USA | CS | HF | 276 | Teach-back communication | No statistical significance (p = 0.775 and 0.609) was observed either in patients who answered teach-back questions correctly or in the reduction of 30-day hospital readmission rates. Statistical Tests: Chi-squared test for categorical data; Fisher exact test for dichotomous data, and Student t-test to compare quantitative data Quality score: 82% |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Mashhadi, S.F.; Hisam, A.; Sikander, S.; Rathore, M.A.; Rifaq, F.; Khan, S.A.; Hafeez, A. Post Discharge mHealth and Teach-Back Communication Effectiveness on Hospital Readmissions: A Systematic Review. Int. J. Environ. Res. Public Health 2021, 18, 10442. https://doi.org/10.3390/ijerph181910442
Mashhadi SF, Hisam A, Sikander S, Rathore MA, Rifaq F, Khan SA, Hafeez A. Post Discharge mHealth and Teach-Back Communication Effectiveness on Hospital Readmissions: A Systematic Review. International Journal of Environmental Research and Public Health. 2021; 18(19):10442. https://doi.org/10.3390/ijerph181910442
Chicago/Turabian StyleMashhadi, Syed Fawad, Aliya Hisam, Siham Sikander, Mommana Ali Rathore, Faisal Rifaq, Shahzad Ali Khan, and Assad Hafeez. 2021. "Post Discharge mHealth and Teach-Back Communication Effectiveness on Hospital Readmissions: A Systematic Review" International Journal of Environmental Research and Public Health 18, no. 19: 10442. https://doi.org/10.3390/ijerph181910442
APA StyleMashhadi, S. F., Hisam, A., Sikander, S., Rathore, M. A., Rifaq, F., Khan, S. A., & Hafeez, A. (2021). Post Discharge mHealth and Teach-Back Communication Effectiveness on Hospital Readmissions: A Systematic Review. International Journal of Environmental Research and Public Health, 18(19), 10442. https://doi.org/10.3390/ijerph181910442