
Kinesio Taping Relieves Pain and Improves Isokinetic Not Isometric Muscle Strength in Patients with Knee Osteoarthritis—A Systematic Review and Meta-Analysis



Abstract
:1. Introduction
2. Materials and Methods
2.1. Data Sources and Search Strategy
2.2. Inclusion Criteria
2.3. Exclusion Criteria
2.4. Screening
2.5. Data Collection and Meta-Analysis
3. Results
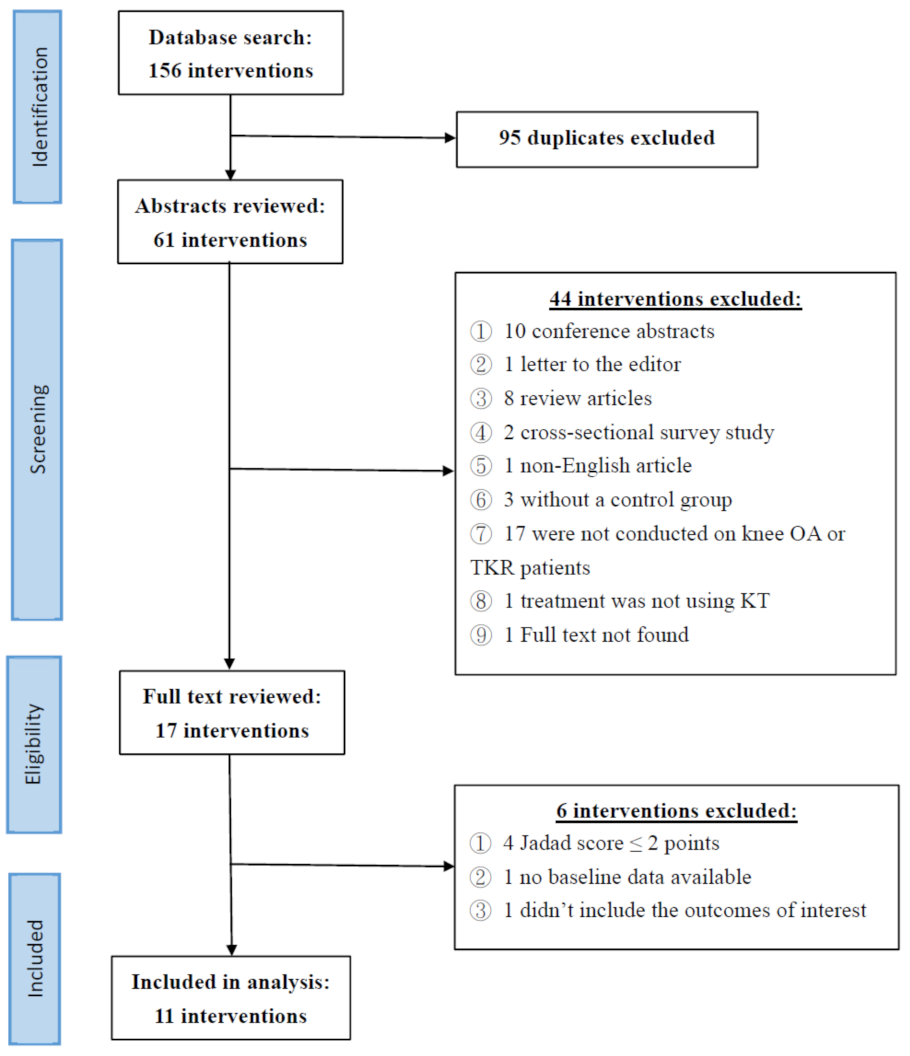
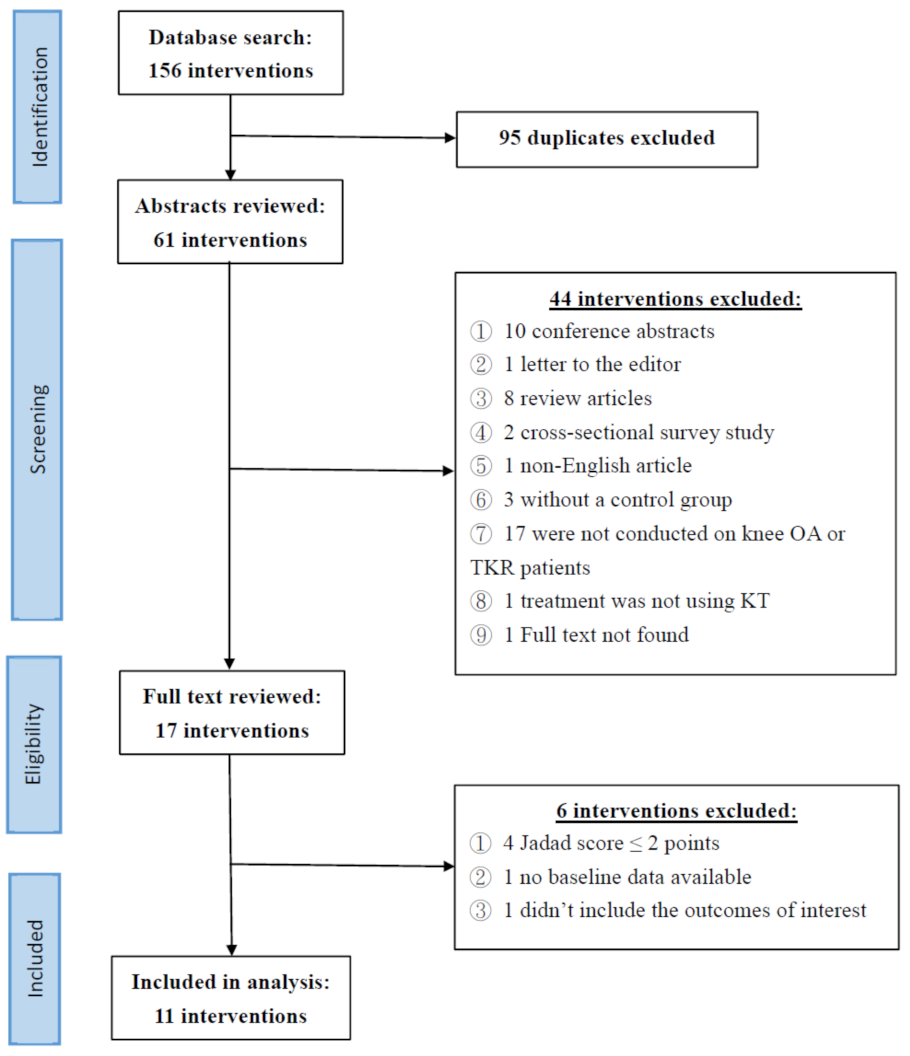
3.1. Search Results
3.2. Characteristics of Included Studies
3.3. Outcomes
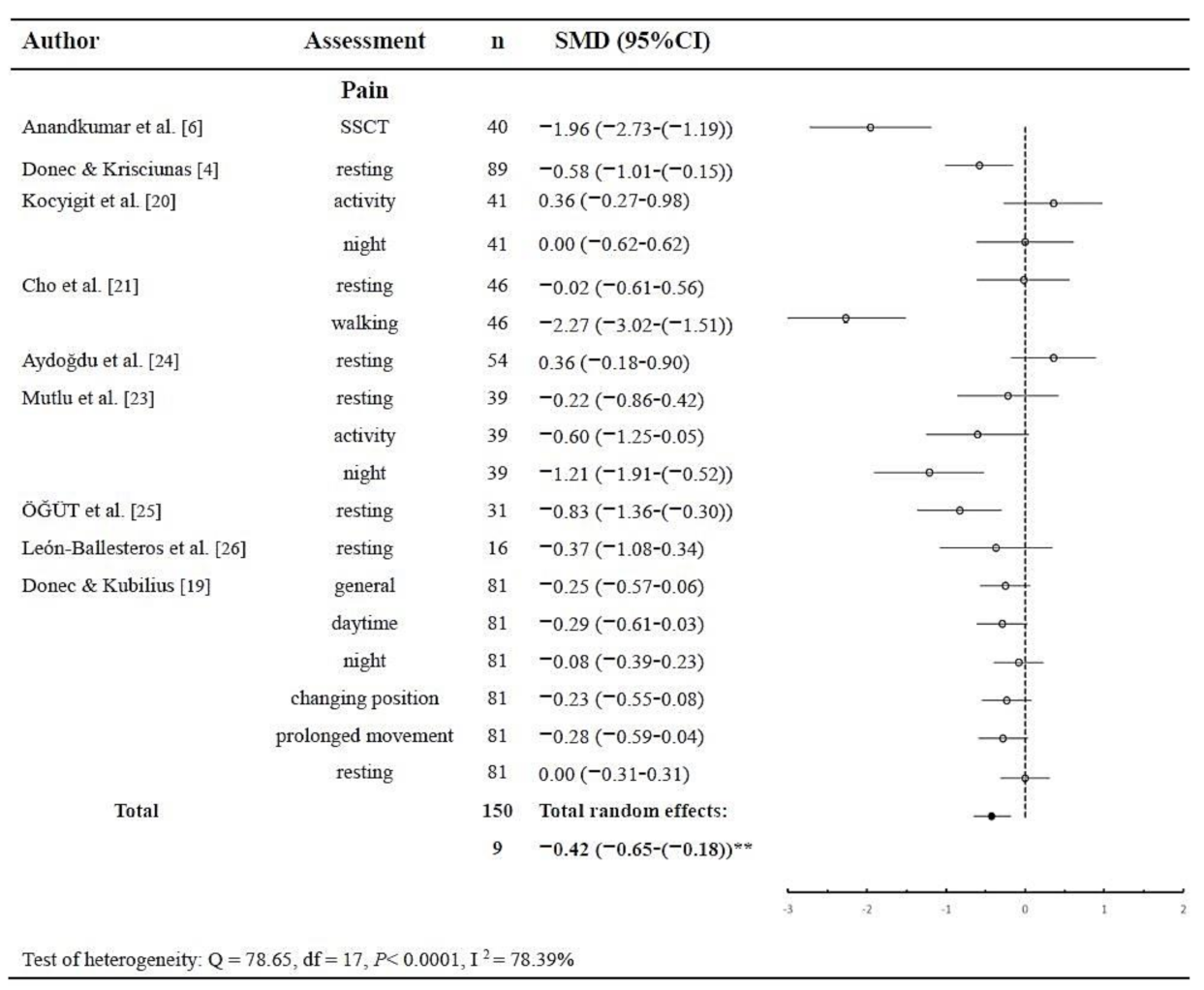
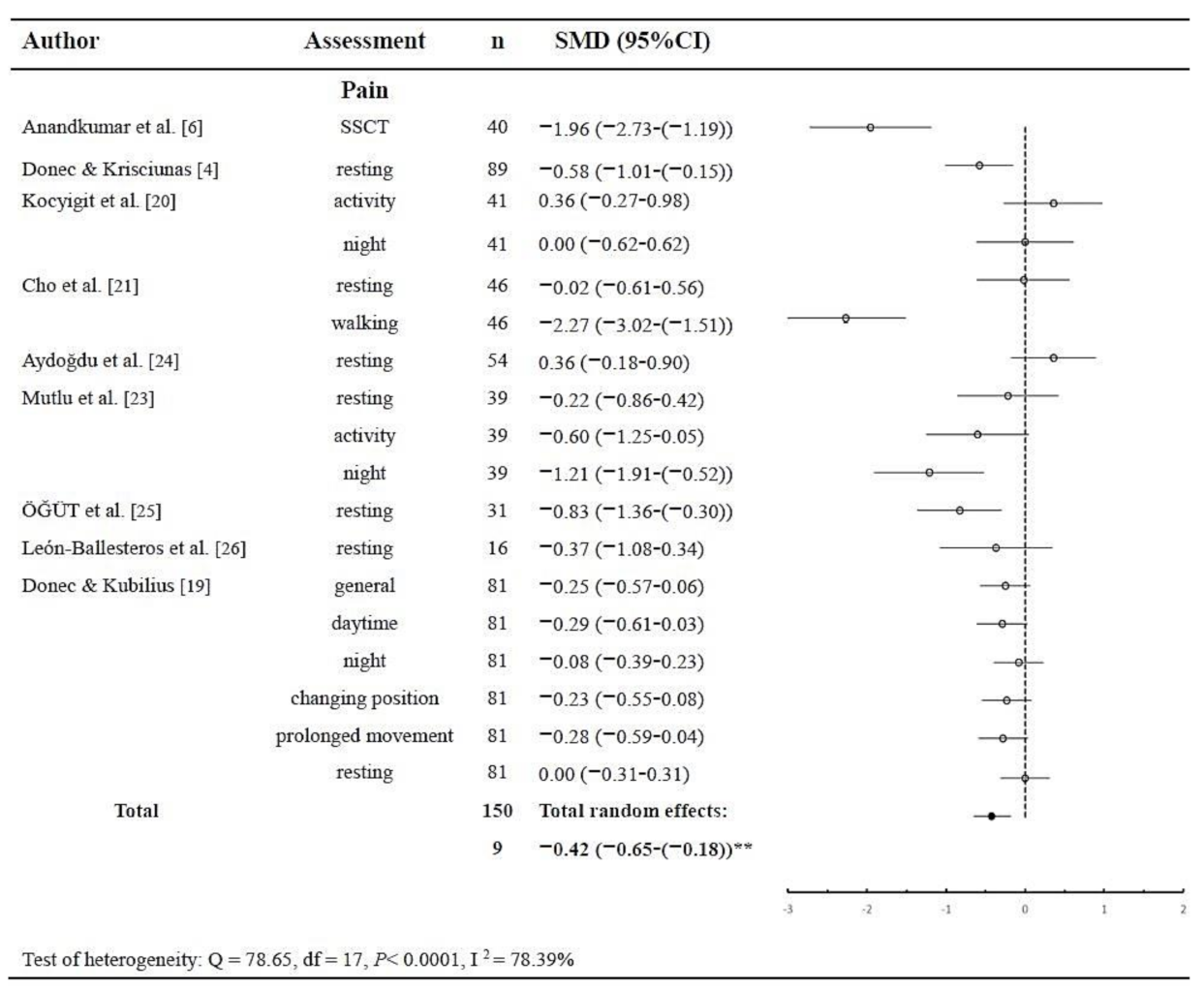
3.3.1. Pain
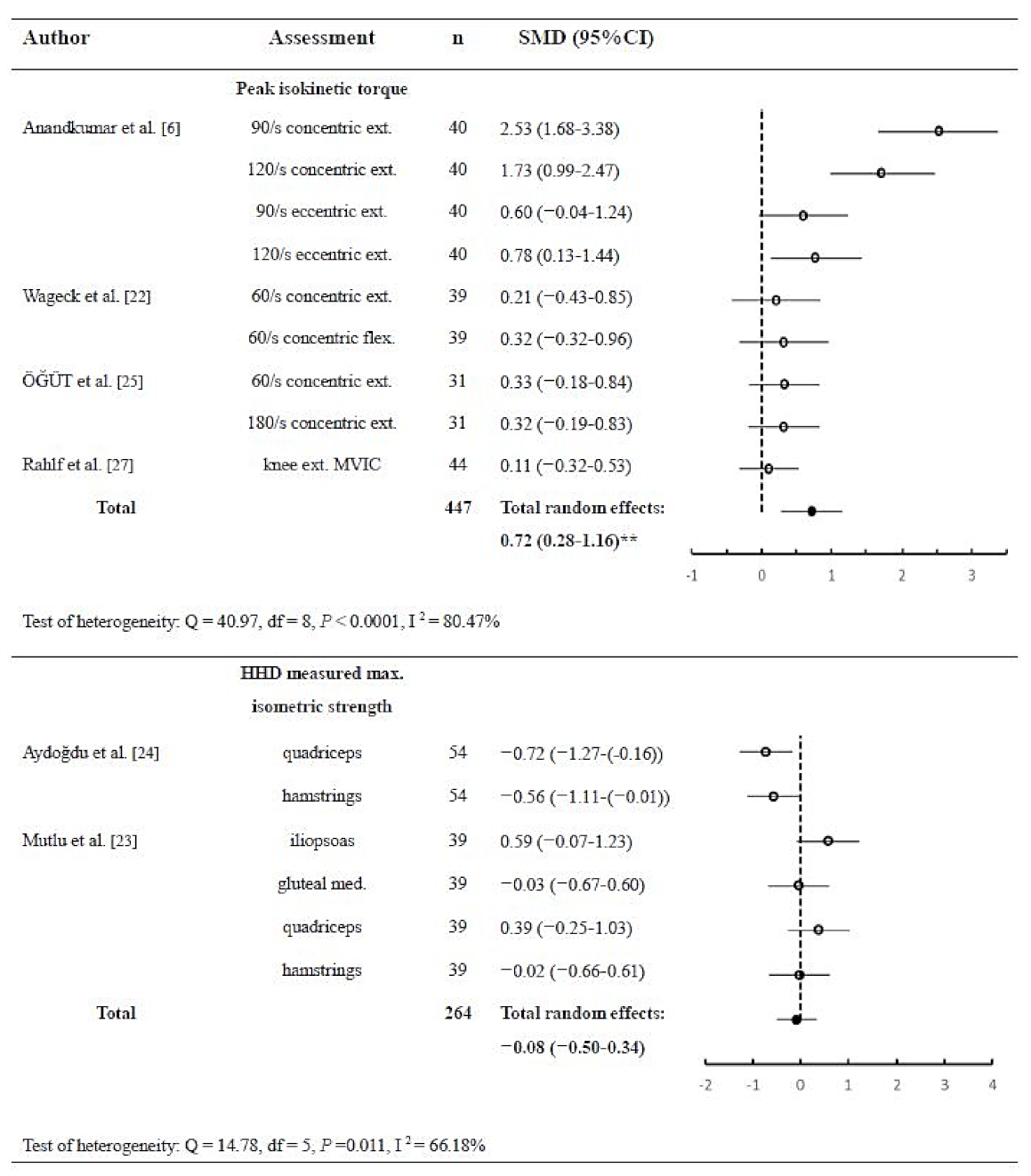
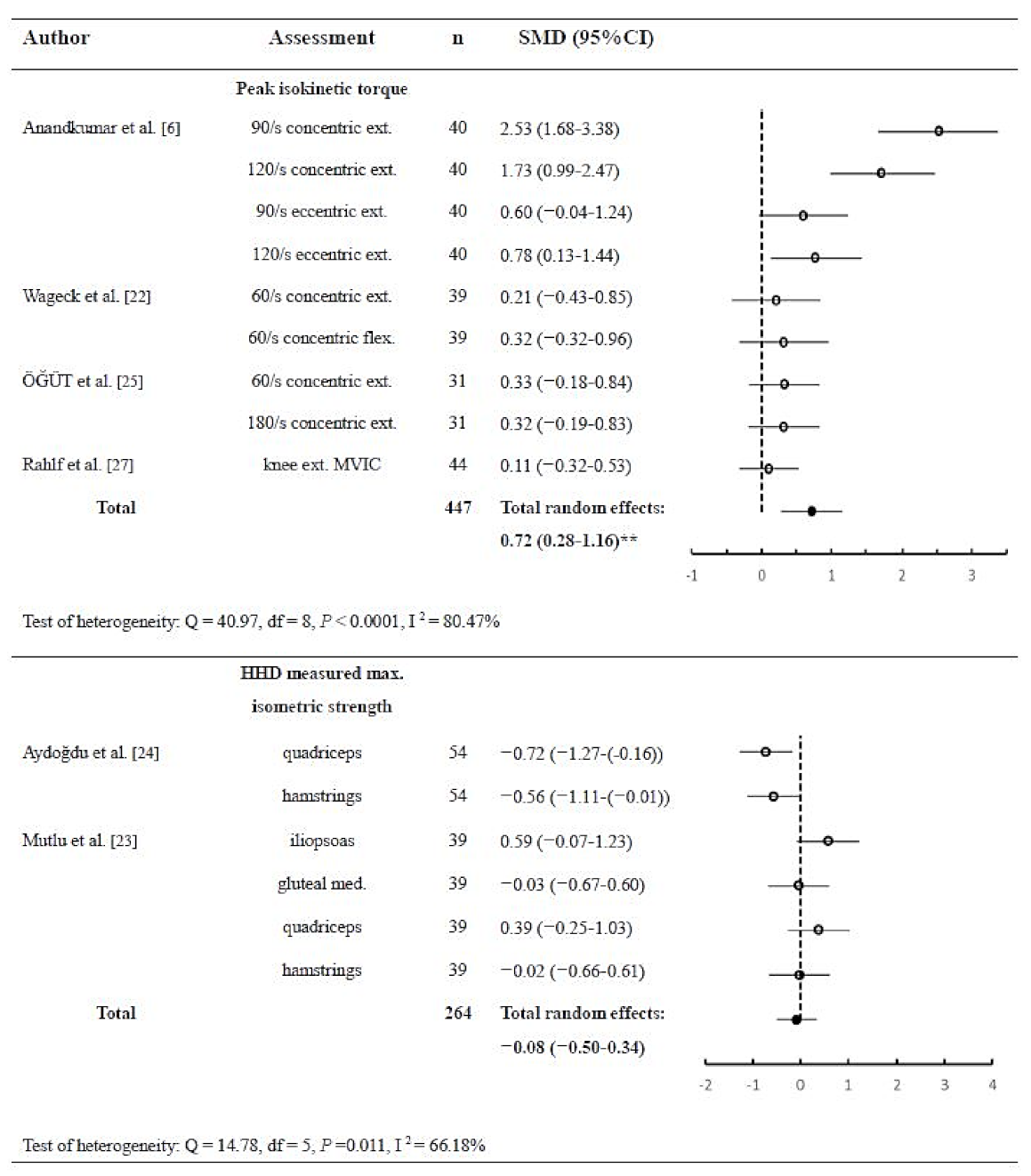
3.3.2. Muscle Strength
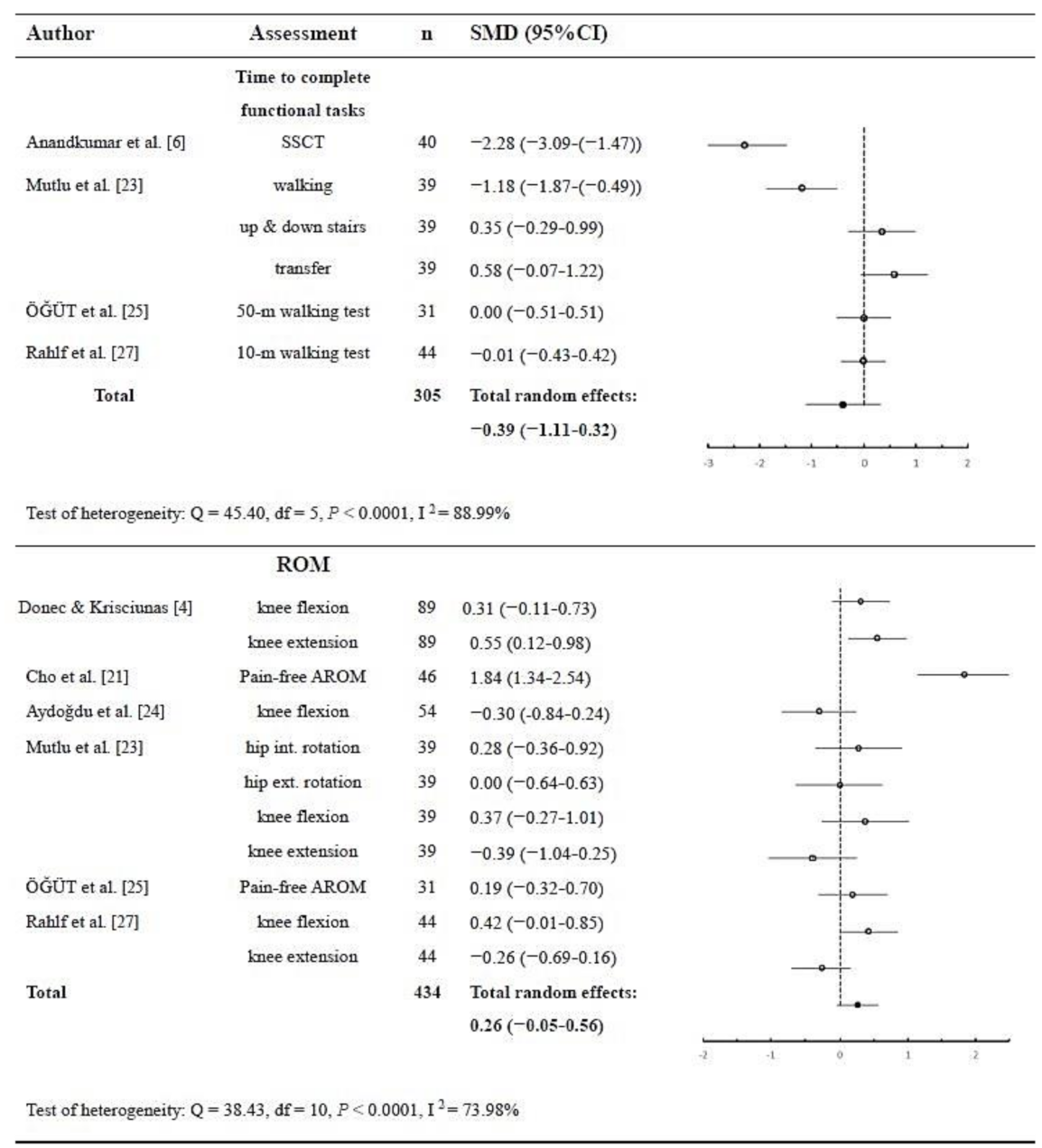
3.3.3. Function
3.3.4. ROM
4. Discussion
4.1. Significant Effect in Pain Relief
4.2. Significant Effect on Isokinetic Muscle Strength Improvement
4.3. Non-Significant Effect in Function and ROM
4.4. Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Fransen, M.; McConnell, S.; Bell, M.M. Exercise for osteoarthritis of the hip or knee. Cochrane Database Syst. Rev. 2001, 1–128. [Google Scholar] [CrossRef]
- Xie, F.; Kovic, B.; Jin, X.; He, X.; Wang, M.; Silvestre, C. Economic and humanistic burden of osteoarthritis: A systematic review of large sample studies. Pharmacoeconomics 2016, 34, 1087–1100. [Google Scholar] [CrossRef] [PubMed]
- Jongbloed, L.; van Twist, D.; Swart, N. Kinesio Taping Improves Pain, Range of Motion, and Proprioception in Older Patients With Knee Osteoarthritis. Am. J. Phys. Med. Rehabil. 2016, 95, e7. [Google Scholar] [CrossRef] [Green Version]
- Donec, V.; Kriščiūnas, A. The effectiveness of Kinesio Taping® after total knee replacement in early postoperative rehabilitation period. A randomized controlled trial. Eur. J. Phys. Rehabil. Med. 2014, 50, 363–371. [Google Scholar] [PubMed]
- Huang, C.-Y.; Hsieh, T.-H.; Lu, S.-C.; Su, F.-C. Effect of the Kinesio tape to muscle activity and vertical jump performance in healthy inactive people. Biomed. Eng. Online 2011, 10, 70. [Google Scholar] [CrossRef] [Green Version]
- Anandkumar, S.; Sudarshan, S.; Nagpal, P. Efficacy of kinesio taping on isokinetic quadriceps torque in knee osteoarthritis: A double blinded randomized controlled study. Physiother. Theory Pract. 2014, 30, 375–383. [Google Scholar] [CrossRef] [PubMed]
- Campolo, M.; Babu, J.; Dmochowska, K.; Scariah, S.; Varughese, J. A comparison of two taping techniques (kinesio and mcconnell) and their effect on anterior knee pain during functional activities. Int. J. Sports Phys. Ther. 2013, 2, 105–110. [Google Scholar]
- Kim, H.; Lee, B. The effects of kinesio tape on isokinetic muscular function of horse racing jockeys. J. Phys. Ther. Sci. 2013, 25, 1273–1277. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Serra, M.V.; Vieira, E.R.; Brunt, D.; Goethel, M.F.; Gonçalves, M.; Quemelo, P.R. Kinesio Taping effects on knee extension force among soccer players. Braz. J. Phys. Ther. 2015, 19, 152–158. [Google Scholar] [CrossRef] [Green Version]
- Murray, H. Effects of kinesio taping on muscle strength after ACL-repair. J. Orthop. Sports Phys. 2000, 30, 14. [Google Scholar]
- de Almeida Lins, C.A.; Neto, F.L.; de Amorim, A.B.C.; de Brito Macedo, L.; Brasileiro, J.S. Kinesio Taping® does not alter neuromuscular performance of femoral quadriceps or lower limb function in healthy subjects: Randomized, blind, controlled, clinical trial. Man. Ther. 2013, 18, 41–45. [Google Scholar] [CrossRef] [PubMed]
- Parreira, P.D.C.S.; Costa, L.D.C.M.; Junior, L.C.H.; Lopes, A.D.; Costa, L.O.P. Current evidence does not support the use of Kinesio Taping in clinical practice: A systematic review. J. Physiother. 2014, 60, 31–39. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Logan, C.A.; Bhashyam, A.R.; Tisosky, A.J.; Haber, D.B.; Jorgensen, A.; Roy, A.; Provencher, M.T. Systematic review of the effect of taping techniques on patellofemoral pain syndrome. Sports Health 2017, 9, 456–461. [Google Scholar] [CrossRef] [PubMed]
- Chang, W.-D.; Chen, F.-C.; Lee, C.-L.; Lin, H.-Y.; Lai, P.-T. Effects of Kinesio taping versus McConnell taping for patellofemoral pain syndrome: A systematic review and meta-analysis. Evid. Based Complement. Altern. Med. 2015, 2015, 471208. [Google Scholar] [CrossRef] [PubMed]
- Yam, M.L.; Yang, Z.; Zee, B.C.-Y.; Chong, K.C. Effects of Kinesio tape on lower limb muscle strength, hop test, and vertical jump performances: A meta-analysis. BMC Musculoskelet. Disord. 2019, 20, 212. [Google Scholar] [CrossRef] [PubMed]
- Lu, Z.; Li, X.; Chen, R.; Guo, C. Kinesio taping improves pain and function in patients with knee osteoarthritis: A meta-analysis of randomized controlled trials. Int. J. Surg. 2018, 59, 27–35. [Google Scholar] [CrossRef]
- Jadad, A.R.; Moore, R.A.; Carroll, D.; Jenkinson, C.; Reynolds D., J.; Gavaghan D., J.; McQuay, H.J. Assessing the quality of reports of randomized clinical trials: Is blinding necessary? Control Clin. Trials 1996, 17, 1–12. [Google Scholar] [CrossRef]
- Faraone, S.V. Interpreting estimates of treatment effects: Implications for managed care. Pharm. Ther. 2008, 33, 700–711. [Google Scholar]
- Donec, V.; Kubilius, R. The effectiveness of Kinesio Taping(R) for pain management in knee osteoarthritis: A randomized, double-blind, controlled clinical trial. Adv. Musculoskelet. Dis. 2019, 11, 1759720X19869135. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kocyigit, F.; Turkmen, M.B.; Acar, M.; Guldane, N.; Kose, T.; Kuyucu, E.; Erdil, M. Kinesio taping or sham taping in knee osteoarthritis? A randomized, double-blind, sham-controlled trial. Complement. Clin. Pract. 2015, 21, 262–267. [Google Scholar] [CrossRef]
- Cho, H.Y.; Kim, E.H.; Kim, J.; Yoon, Y.W. Kinesio taping improves pain, range of motion, and proprioception in older patients with knee osteoarthritis: A randomized controlled trial. Am. J. Phys. Med. Rehabil. 2015, 94, 192–200. [Google Scholar] [CrossRef]
- Wageck, B.; Nunes, G.S.; Bohlen, N.B.; Santos, G.M.; de Noronha, M. Kinesio Taping does not improve the symptoms or function of older people with knee osteoarthritis: A randomised trial. J. Physiother. 2016, 62, 153–158. [Google Scholar] [CrossRef] [Green Version]
- Mutlu, E.K.; Mustafaoglu, R.; Birinci, T.; Ozdincler, A.R. Does kinesio taping of the knee improve pain and functionality in patients with knee osteoarthritis?: A randomized controlled clinical trial. Am. J. Phys. Med. Rehabil. 2017, 96, 25–33. [Google Scholar] [CrossRef] [PubMed]
- Aydogdu, O.; Sari, Z.; Yurdalan, S.U.; Polat, M.G. Clinical outcomes of kinesio taping applied in patients with knee osteoarthritis: A randomized controlled trial. J. Back Musculoskelet. Rehabil. 2017, 30, 1045–1051. [Google Scholar] [CrossRef] [PubMed]
- Öğüt, H.; Güler, H.; Yildizgören, M.T.; Velioğlu, O.; Turhanoğlu, A.D. Does kinesiology taping improve muscle strength and function in knee osteoarthritis? A single-blind, randomized and controlled study. Arch. Rheumatol. 2018, 33, 335–343. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- León-Ballesteros, S.; Espinosa-Morales, R.; Clark-Peralta, P.; Gómez-Pineda, A.G.; Guadarrama-Becerril, J.H. Kinesiotape and quadriceps strengthening with elastic band in women with knee osteoarthritis and overweight or obesity. A randomized clinical trial. Reumatol. Clín. (Engl. Ed.) 2020, 16, 11–16. [Google Scholar]
- Rahlf, A.L.; Braumann, K.M.; Zech, A. Kinesio Taping Improves Perceptions of Pain and Function of Patients With Knee Osteoarthritis: A Randomized, Controlled Trial. J. Sport Rehabil. 2019, 28, 481–487. [Google Scholar] [CrossRef] [Green Version]
- Srikanth, V.K.; Fryer, J.L.; Zhai, G.; Winzenberg, T.M.; Hosmer, D.; Jones, G. A meta-analysis of sex differences prevalence, incidence and severity of osteoarthritis. Osteoarthr. Cartil. 2005, 13, 769–781. [Google Scholar] [CrossRef] [Green Version]
- Balki, S.; Göktaş, H.E.; Öztemur, Z. Kinesio taping as a treatment method in the acute phase of ACL reconstruction: A double-blind, placebo-controlled study. Acta Orthop. Traumatol. Turc. 2016, 50, 628–634. [Google Scholar] [CrossRef] [Green Version]
- Hart, J.M.; Pietrosimone, B.; Hertel, J.; Ingersoll, C.D. Quadriceps activation following knee injuries: A systematic review. J. Athl. Train. 2010, 45, 87–97. [Google Scholar] [CrossRef] [Green Version]
- Hassan, B.; Doherty, S.; Mockett, S.; Doherty, M. Effect of pain reduction on postural sway, proprioception, and quadriceps strength in subjects with knee osteoarthritis. Ann. Rheum. Dis. 2002, 61, 422–428. [Google Scholar] [CrossRef]
- Kim, W.K.; Kim, D.-K.; Seo, K.M.; Kang, S.H. Reliability and validity of isometric knee extensor strength test with hand-held dynamometer depending on its fixation: A pilot study. Ann. Rehabil. Med. 2014, 38, 84–93. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zapparoli, F.Y.; Riberto, M. Isokinetic evaluation of the hip flexor and extensor muscles: A systematic review. J. Sport Rehabil. 2017, 26, 556–566. [Google Scholar] [CrossRef] [PubMed]
- Pamuk, U.; Yucesoy, C.A. MRI analyses show that kinesio taping affects much more than just the targeted superficial tissues and causes heterogeneous deformations within the whole limb. J. Biomech. 2015, 48, 4262–4270. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Author (Year) | Study Design | Participants | Intervention | Outcome Measures | Evaluation Time | Results | Jadad Score |
|---|---|---|---|---|---|---|---|
| Anandkumar et al. [6] (2014) | RCT | 40 subjects (17 males; 23 females) with knee OA randomly allocated to experimental group (n = 20) or control group (n = 20) | Experimental group: Three I-shaped KT strips applied from origins of the RF, VL and VM muscles to insertions with 50~70% tension. Control group: Same as the experimental group but with no tension. | 1. Pain during SSCT (VAS) 2. Peak isokinetic quadriceps torque 3. Functional task: SSCT 4. ROM: N/A 5. Other: N/A | Before tx, 30 min after KT application | A large effect sizewith significant improvements in pain, peak quadriceps torque, and SSCT was obtained in the experimental group compared to the control group immediately after KT application. | 5 |
| Donec and Krisciunas [4] (2014) | RCT | 89 post-TKR patients (13 males; 76 females) randomized to experimental group (n = 40) or control group (n = 49) | Experimental group: Postop rehabilitation program and KT, including lymphatic correction, Y strip for RF facilitation (paper-off tension) and I strip for medial knee ligaments. Control group: Only postop rehabilitation program. | 1. Postop pain (NPRS) 2. Muscle strength: N/A 3. Functional task: N/A 4. ROM 5. Other: Edema (leg circumference at 4 standardized points) | Before tx and 2nd, 8th, 16th, 24th, and 28th days postop | In both groups, postop pain decreased significantly; however, less pain was found in the KT group from the 2nd week. Knee extension was better in the experimental group on the 28th day postop. Edema was less intense and subsided more quickly in the KT group. | 3 |
| Donec & Kubilius [19] (2019) | RCT | 157 patients (33 males; 124 females) with knee OA randomized to KT group (n = 81) or control group (n = 76) | Experimental group: Two Y strips with paper-off tension, one applied from RF toward the patella, the other from the tibial tuberosity to VM and VL. Two I strips with 75–100% tension, applied on the patella tendon and the collateral ligamnets. Control group: Sham tape applied transversely over the thigh, calf, medial, and lateral sides of the knee joint. | 1. Pain (NPRS) 2. Muscle strength: N/A 3. Function: N/A 4. ROM: N/A 5. Other: PPT, KOOS | Before tx, 1 month (immediately after tx), 1 further month after tx (follow-up) | All self-reported improvement remained at the 1-month follow up. Significantly higher and clinically meaningful reduction of pain intensity was found in the KT group after the treatment month, in comparison with the control group. More pain reduction was reported in the daytime for participants in the KT group at the follow up. | 5 |
| Kocyigit et al. [20] (2015) | RCT | 41 patients (13 males; 28 females) with knee OA randomized to experimental group (n = 21) or control group (n = 20) | Experimental group: Y-shaped KT applied from the RF, with ends around the patellae (25% tension). Y-shaped KT from the tibial tuberosity, with ends around the patellae (25% tension). I-strip KT applied mediolaterally to the patella. Control group: Sham taping with 5 cm surgical hypoallergenic flexible tape with no tension. | 1. Activity & nocturnal pain (VAS) 2. Muscle strength: N/A 3. Functional task: N/A 4. ROM: N/A 5. Other: Lequesne index, QOL (NHP score). | Before tx, after 12 days of tx | In both groups, VAS for activity pain, VAS for nocturnal pain, Lequesne index score, and NHP score decreased significantly. NHP energy scores were significantly different between the groups in favor of sham taping. | 5 |
| Cho et al. [21] (2015) | RCT | 46 patients (13 males; 33 females) with knee OA randomized to experimental group (n = 23) or control group (n = 23) | Experimental group: Y-shaped KT starting from the originof RF to the insertion with 15–25% tension. Control group: Placebo KT applied in the same way with no tension. | 1. Pain (VAS) 2. Muscle strength: N/A 3. Functional task: N/A 4. Pain-free AROM 5. Other: PPT (midportion of the quadriceps and TA), Proprioception. | Before tx, 1 hour after KT application | The experimental group showed attenuation of pain during walking, decreased PPT, and significantly improved AROM and proprioception. There were significant differences in pain during walking and PPT between the 2 groups. | 5 |
| Wageck et al. [22] (2016) | RCT | 39 patients (5 males; 34 females) with knee OA randomized to experimental group (n = 19) or control group (n = 20) | Experimental group: 3 KT application techniques, including drainage, quadriceps relaxation with paper-off tension (Y strip), and pain relief (star application). Control group: Sham taping with two I-shaped KT strips applied without tension across the quadriceps. | 1. Pain: N/A 2. Knee extensor and flexor isokinetic torque 3. Functional task: N/A 4. ROM: N/A 5. Other: PPT, Volumetry, Perimetry, Lysholm score, WOMAC. | Before tx, after 4 days of tx, 19 days after tx (follow-up) | On day 4 and 19, there were no significant between-group differences in knee extensor/flexor muscle strength, PPT at any measured point, volumetry, perimetry, Lysholm score, or WOMAC score. | 5 |
| Mutlu et al. [23] (2017) | RCT | 39 patients (6 males; 33 females) with knee OA randomized to experimental group (n = 20) or control group (n = 19) | Experimental group: Two Y-shaped KT strips applied to the RF and hamstring muscles from origin to insertion with 25% tension. Control group: Placebo KT applied transversely to the muscle groups of the quadriceps and hamstrings at 2 levels. | 1. Pain (VAS)2. Isometric muscle strength (HHD) 3. Functional task: ALF (walking 8m; up &down 7 steps; transferring) 4. Active ROM 5. Other: WOMAC. | Before tx, immediately after tx, 6–9 days after tx, 1-month follow-up | The KT group had a large decrease in VAS activity and walking task scores from the initial taping application to 6–9 days after tx to the 1-month follow-up compared with the control group. No significant difference in outcome measures for ROM and muscle strength between groups. | 5 |
| Aydogdu et al. [24] (2017) | RCT | 54 patients (8 males; 46 females) with knee OA randomized to experimental group (n = 28) or control group (n = 26) | Experimental group: Conventional tx and Y-shaped KT strips applied to the RF and hamstring muscles from origin to insertion with 50–70% tension. Control group: Conventional tx including physical agents (hot pack, USD, TENS) and supervised exercises (stretching and strengthening exercises). | 1. Pain (VAS) 2. Isometric muscle strength (HHD) 3. Functional task: N/A 4. ROM 5. Other: KOOS. | Before tx, 1 hour after taping in first tx session, 3 weeks after tx started | Significant differences were observed in pain, ROM, and functional status (KOOS) between pre-tx and post-taping in the experimental group. | 3 |
| ÖĞÜT et al. [25] (2018) | RCT | 61 patients (females) with knee OA randomized to experimental group (n = 31) or control group (n = 30) | Experimental group: Conventional tx and 3 Y-shaped KT strips applied to the RF (paper-off tension), VL (full stretching at the ends), and VM (full stretching at the ends) from origin to insertion for facilitation.Control group: Conventional tx (hot pack, USD, TENS) and sham taping (I strip applied transversely over quadriceps muscle). | 1. Pain (VAS) 2. Knee extensor isokinetic torque 3. Functional task: 50-m walking time 4. ROM 5. Other: WOMAC | Before tx, immediately after tx, 1-month follow-up, 3-month follow-up | In the KT group, the WOMAC pain and WOMAC total scores decreased significantly after treatment compared to the sham-KT group. In both groups; VAS, WOMAC pain, stiffness, physical function, and total values decreased significantly after treatment. In both groups, isokinetic quadriceps peak torque measurements were increased after treatment. | 5 |
| León-Ballesteros et al. [26] (2018) | RCT | 32 patients (females) with knee OA randomized to experimental group (n = 16) or control group (n = 16) | Experimental group: Quadriceps strengthening exercise program and 2 KT strips (I and Y-shape) applied from 15 cm above the interarticular line to below with no tension.Control group: Quadriceps strengthening exercise program and sham tape (I strip with >50% tension). | 1. Pain (VAS) 2. Muscle strength: N/A 3. Functional task: N/A 4. ROM: N/A 5. Other: WOMAC | Before tx, end of the weeks 2, 4, and 6 (end of tx). | At the end of the tx, there were no significant differences in pain between the groups. Both groups had a difference of 2.7 points with respect to the baseline measurement, change percentage of 32.2% and31.1% for placebo and experimental respectively. | 5 |
| Rahlf et al. [27] (2018) | RCT | 141 patients (67 males; 74 females) with knee OA randomized to KT group (tx group) (n = 47) or sham tape group (control group) (n = 47), and no tape group (n = 47). | Experimental group: One I strip over the patella from the tibial tuberosity to the lower third of the quadriceps with max. tension. 2 I strips over medial and lateral collateral ligaments, respectively. Control group: Sham tape applied transversely distal to the knee with no tension. | 1. Pain: N/A 2. MVIC measured by isokinetic dynamometer 3. Functional task: 10 meter walk test 4. ROM 5. Other: WOMAC, BESS | Before tx, immediately after tx (tape applied for 3 consecutive days) | Significant effects were found for WOMAC pain (tape vs. sham; tape vs. control, stiffness (tape vs. sham; tape vs. control), and physical function (tape vs. sham; tape vs. control). No interactions were found for balance, muscle strength, walking speed, or active range of motion. | 5 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Mao, H.-Y.; Hu, M.-T.; Yen, Y.-Y.; Lan, S.-J.; Lee, S.-D. Kinesio Taping Relieves Pain and Improves Isokinetic Not Isometric Muscle Strength in Patients with Knee Osteoarthritis—A Systematic Review and Meta-Analysis. Int. J. Environ. Res. Public Health 2021, 18, 10440. https://doi.org/10.3390/ijerph181910440
Mao H-Y, Hu M-T, Yen Y-Y, Lan S-J, Lee S-D. Kinesio Taping Relieves Pain and Improves Isokinetic Not Isometric Muscle Strength in Patients with Knee Osteoarthritis—A Systematic Review and Meta-Analysis. International Journal of Environmental Research and Public Health. 2021; 18(19):10440. https://doi.org/10.3390/ijerph181910440
Chicago/Turabian StyleMao, Hsin-Yu, Meng-Tzu Hu, Yea-Yin Yen, Shou-Jen Lan, and Shin-Da Lee. 2021. "Kinesio Taping Relieves Pain and Improves Isokinetic Not Isometric Muscle Strength in Patients with Knee Osteoarthritis—A Systematic Review and Meta-Analysis" International Journal of Environmental Research and Public Health 18, no. 19: 10440. https://doi.org/10.3390/ijerph181910440
APA StyleMao, H.-Y., Hu, M.-T., Yen, Y.-Y., Lan, S.-J., & Lee, S.-D. (2021). Kinesio Taping Relieves Pain and Improves Isokinetic Not Isometric Muscle Strength in Patients with Knee Osteoarthritis—A Systematic Review and Meta-Analysis. International Journal of Environmental Research and Public Health, 18(19), 10440. https://doi.org/10.3390/ijerph181910440