
A Systematic Review of Cross-Cultural Adaptation and Psychometric Properties of Oral Health Literacy Tools



Abstract
:1. Introduction
2. Materials and Methods
2.1. Eligibility Criteria
2.2. Information Source
2.3. Search Strategy
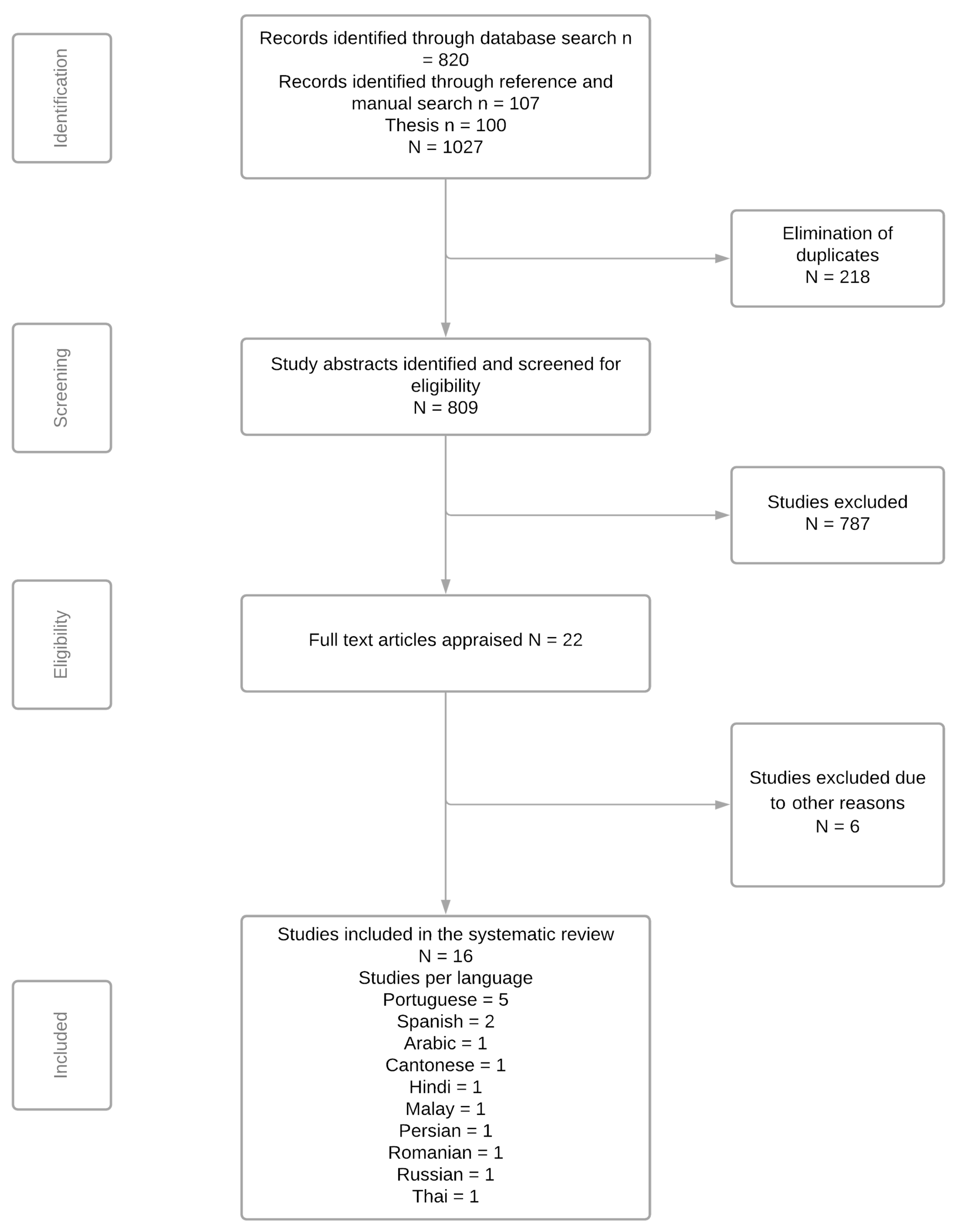
2.4. Study Selection
2.5. Data Extraction Process
2.6. Assessment of the Methodological Quality
- The Guidelines for the Process of Cross-Cultural Adaptations of Self-Report Measures [31], which states a cross-cultural adaptation, must include an initial translation, synthesis of translation, back-translation, reviews by the expert committee, and the pre-test version of the instrument. To assess the quality of the cross-cultural adaptation process, the tools were rated as + positive rating, - negative rating, 0 no information available, and unclear according to the criteria adapted from Costa and colleagues [44]. The steps of the cross-cultural adaptation process and the scoring system are described in Table S4.
- The COnsensus-based Standards for the selection of health Measurement INstruments (COSMIN) checklist [38] was used for evaluating the psychometric properties of the translated versions of the OHL tools. This standardized checklist consists of nine boxes on measurement properties, each consisting of 3 to 38 items. Each checklist item is ranked on a 4-point scale (inadequate, doubtful, adequate, and very good). An overall score of the methodological quality of a study was determined by taking the lowest rating of any items in a box (i.e., worst-score-counts method).
2.7. Assessment of Psychometric Properties
2.8. Data Synthesis
2.9. Measurement Properties
2.9.1. Reliability
- Internal consistency: The degree of inter-relatedness among the items, expressed by Cronbach’s alpha value [39].
- Reliability: The proportion of total variance in the measurements, which is because of true differences among patients, is represented by the Intraclass Correlation Coefficient (ICC) or weighted kappa [37].
- Measurement error: The systematic and random error of a patient’s score that is not attributed to the true change of the construct to be measured [49]. Measurement error is calculated as the smallest detectable change or limits of agreement, and its adequacy is determined by relating them to the minimal important change [50].
2.9.2. Validity
- Content validity: The degree to which the content of an instrument is an adequate reflection of the construct to be measured [39]. It is assessed by asking patients and professionals about the relevance, comprehensiveness, and comprehensibility of the items, response options, and instructions [51]. Content validity is only relevant for the development of original instruments [31], and therefore, not relevant to the scope of this review.
- Criterion validity: The extent to which scores of an instrument are an adequate reflection of a gold standard [39]. Since OHL tools do not have a gold standard for item selection, the domain criterion validity was not considered in this review.
- Construct validity: The degree to which the scores of an instrument are consistent with hypotheses (for instance, with regard to internal relationships, relationships to scores of other instruments, or differences between relevant groups) based on the assumption that the instrument validly measures the construct to be measured [39]. It has three important aspects:
- a.
- b.
- Hypothesis testing: The degree to which a particular measure relates to other measures in a way one would expect if it was validly measuring the supposed construct, i.e., in accordance with predefined hypotheses about the correlation or differences between the measures [39]. The following hypothesis was set for testing the construct validity:
- Correlation with scores of instruments measuring a similar construct or another OHL tool included in the pre-specified list will be highly or moderately to highly correlated.
- Correlation with scores of instruments measuring related but not the same constructs; for example, health-related quality of life measures will be either moderately to highly or moderately correlated.
- A weak to moderate correlation will be observed between scores of instruments included here and two different subgroups of patients.
- A weak correlation is defined as <0.30;
- A weak to moderate correlation is defined as >0.20 to <0.40;
- A moderate correlation is defined as >0.30 to <0.70;
- A moderate to high correlation is defined as >0.60 to <0.80;
- A high correlation is defined as >0.70.
- c.
- Cross-cultural validity: The degree to which the performance of items on a translated or culturally adapted instrument is an adequate reflection of the performance of items of the original version of the instrument [39]. This property is assessed by multi-group factor analysis or differential item functioning [53], using data from a population that completed the questionnaire in the original language, as well as data from a population that completed the questionnaire in the translated language.
2.10. Responsiveness
3. Results
3.1. Results of the Search
3.2. Characteristics of Oral Health Assessment Instruments
4. Discussion
4.1. Strengths and Limitations
4.2. Implications
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
| AREALD-30 | Arabic Rapid Estimate of Adult Literacy in Dentistry |
| Brazilian-HeLD | Brazilian-Portuguese version of Health Literacy in Dentistry scale |
| BOHLAT-P | Brazilian-Portuguese version of the Hong Kong OHL Assessment Task for Pediatric Dentistry |
| BREALD-30 | Brazilian version of the Rapid Estimate of Adult Literacy in Dentistry |
| BREALMD-20 | Brazilian version of 20-item Rapid Estimate Adult Literacy in Medicine and Dentistry |
| COSMIN | COnsensus-based Standards for the selection of health Measurement Instruments |
| CPI | Community Periodontal Index |
| DMFT | Decayed, Missing, and Filled Teeth |
| HKREALD-30 | Hong Kong Rapid Estimate of Adult Literacy in Dentistry |
| ICC | Intraclass Correlation Coefficient |
| IREALD-99 | Rapid Estimate of Adult Literacy in Dentistry-99 for Iranian population |
| MeSH | Medical Subject Headings |
| OHIP | Oral Health Impact Profile |
| OHIS | Oral Hygiene Index Simplified |
| OHL | Oral Health Literacy |
| OHLA-B | Oral Health Literacy Assessment-Brazilian |
| OHL-AQ-H | Oral Health Literacy Adult Questionnaire-Hindi Version |
| OHLI | Oral Health Literacy Instrument |
| OHLI-Cl | Chilean version of OHLI |
| OHLI-M | Oral health literacy instrument –Malay version |
| PICOS | the Population, Intervention, Comparator, Outcome, and Study Design |
| PRISMA | Preferred Reporting Items for Systematic Reviews and Meta-Analysis |
| PROSPERO | International Prospective Register of Systematic Reviews |
| REALD-30 | Rapid Estimate of Adult Literacy in Dentistry |
| R-OHLI | Russian version of Oral Health Literacy Instrument |
| RREALD-30 | Romanian version of Rapid Estimate of Adult Literacy in Dentistry-30 |
| SAHLSA | Short Assessment of Health Literacy for Spanish-speaking Adults |
| ToFHLiD | Test of Functional Health Literacy in Dentistry |
| ThREALD-30 | Thai version of Rapid Estimate of Adult Literacy in Dentistry-30 |
| TREALD-30 | Turkish version of Rapid Estimate of Adult Literacy in Dentistry-30 |
| WHO | World Health Organization |
References
- United Nations General Assembly. President. Political Declaration of the High-level Meeting of the General Assembly on the Prevention and Control of Non-communicable Diseases. Resolution A/66/L1. 2011. Available online: https://digitallibrary.un.org/record/710899/?ln=en (accessed on 3 November 2020).
- World Health Organization. Oral Health: Key Facts. Oral Health. 2020. Available online: https://www.who.int/news-room/fact-sheets/detail/oral-health (accessed on 1 November 2020).
- James, S.L.; Abate, D.; Abate, K.H.; Abay, S.M.; Abbafati, C.; Abbasi, N.; Abbastabar, H.; Abd-Allah, F.; Abdela, J.; Abdelalim, A.; et al. Global, regional, and national incidence, prevalence, and years lived with disability for 354 diseases and injuries for 195 countries and territories, 1990–2017: A systematic analysis for the Global Burden of Disease Study 2017. Lancet 2018, 392, 1789–1858. [Google Scholar] [CrossRef] [Green Version]
- Kassebaum, N.; Smith, A.G.C.; Bernabée, E.; Fleming, T.; Reynolds, A.; Vos, T.; Murray, C.J.L.; Marcenes, W.; GBD 2015 Oral Health Collaborators. Global, regional, and national prevalence, incidence, and disability-adjusted life years for oral conditions for 195 countries, 1990–2015: A systematic analysis for the global burden of diseases, injuries, and risk factors. J. Dent. Res. 2017, 96, 380–387. [Google Scholar] [CrossRef]
- Centers for Disease Control and Prevention. Oral Health Fast Facts 2020. Available online: https://www.cdc.gov/oralhealth/fast-facts/index.html (accessed on 1 November 2020).
- Peres, M.A.; Macpherson, L.M.; Weyant, R.J.; Daly, B.; Venturelli, R.; Mathur, M.R.; Listl, S.; Celeste, R.K.; Guarnizo-Herreño, C.C.; Kearns, C.; et al. Oral diseases: A global public health challenge. Lancet 2019, 394, 249–260. [Google Scholar] [CrossRef]
- Torppa-Saarinen, E.; Tolvanen, M.; Lahti, S.; Suominen, A.L. Changes and determinants of unmet oral health treatment need. Community Dent. Oral Epidemiol. 2020, 49, 158–165. [Google Scholar] [CrossRef] [PubMed]
- Watt, R.G. Social determinants of oral health inequalities: Implications for action. Community Dent. Oral Epidemiol. 2012, 40, 44–48. [Google Scholar] [CrossRef]
- Jamieson, L.; Gibson, B.; Thomson, W.M. Oral Health Inequalities and the Corporate Determinants of Health: A Commentary. Int. J. Environ. Res. Public Health 2020, 17, 6529. [Google Scholar] [CrossRef] [PubMed]
- Han, C. Oral health disparities: Racial, language and nativity effects. SSM-Popul. Health 2019, 8, 100436. [Google Scholar] [CrossRef]
- Liu, C.; Wang, D.; Liu, C.; Jiang, J.; Wang, X.; Chen, H.; Ju, X.; Zhang, X. What is the meaning of health literacy? A systematic review and qualitative synthesis. Fam. Med. Community Health 2020, 8, e000351. [Google Scholar] [CrossRef] [PubMed]
- US Department of Health and Human Services. Healthy People 2010: Understanding and Improving Health; US Department of Health and Human Services: Washington, DC, USA, 2000. [Google Scholar]
- Coleman, C.; Kurtz-Rossi, S.; McKinney, J.; Pleasant, A.; Rootman, I.; Shohet, L.; Calgary Charter on Health Literacy. Montreal: The Centre for Literacy; 2009. Available online: http://www.centreforliteracy.qc.ca/sites/default/files/CFL_Calgary_Charter_2011.pdf (accessed on 4 November 2020).
- Pleasant, A. Advancing health literacy measurement: A pathway to better health and health system performance. J. Health Commun. 2014, 19, 1481–1496. [Google Scholar] [CrossRef] [Green Version]
- Kickbusch, I.; Pelikan, J.; Apfel, F.; Tsouros, A. Health Literacy: The Solid Facts. 2013. World Health Organization, Regional Office for Europe. 2017. Available online: https://www.euro.who.int/__data/assets/pdf_file/0008/190655/e96854.pdf (accessed on 4 November 2020).
- Geboers, B.; Reijneveld, S.A.; Jansen, C.J.; de Winter, A.F. Health literacy is associated with health behaviors and social factors among older adults: Results from the LifeLines Cohort Study. J. Health Commun. 2016, 21, 45–53. [Google Scholar] [CrossRef]
- Mõttus, R.; Johnson, W.; Murray, C.; Wolf, M.S.; Starr, J.M.; Deary, I.J. Towards understanding the links between health literacy and physical health. Health Psychol. 2014, 33, 164. [Google Scholar] [CrossRef] [Green Version]
- Bostock, S.; Steptoe, A. Association between low functional health literacy and mortality in older adults: Longitudinal cohort study. BMJ 2012, 344, e1602. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Parker, E.J.; Jamieson, L.M. Associations between indigenous Australian oral health literacy and self-reported oral health outcomes. BMC Oral Health 2010, 10, 3. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mayo-Gamble, T.L.; Mouton, C. Examining the association between health literacy and medication adherence among older adults. Health Commun. 2018, 33, 1124–1130. [Google Scholar] [CrossRef] [PubMed]
- Kaur, N.; Kandelman, D.; Nimmon, L.; Potvin, L. Oral health literacy: Findings of a scoping review. EC Dent. Sci. 2015, 2, 293–306. [Google Scholar]
- Guo, Y.; Logan, H.L.; Dodd, V.J.; Muller, K.E.; Marks, J.G.; Riley, J.L., III. Health literacy: A pathway to better oral health. Am. J. Public Health 2014, 104, e85–e91. [Google Scholar] [CrossRef]
- Batista, M.J.; Lawrence, H.P.; de Sousa, M.d.L.R. Oral health literacy and oral health outcomes in an adult population in Brazil. BMC Public Health 2018, 18, 60. [Google Scholar] [CrossRef]
- Wehmeyer, M.M.H.; Corwin, C.L.; Guthmiller, J.M.; Lee, J.Y. The impact of oral health literacy on periodontal health status. J. Public Health Dent. 2014, 74, 80–87. [Google Scholar] [CrossRef] [Green Version]
- Department of Health and Human Services. National Institute of Dental and Craniofacial Research. The invisible barrier: Literacy and its relationship with oral health. A report of the workgroup sponsored by the National Institute of Dental and Craniofacial Research, National Institutes of Health, US Public Health Service. J. Public Health Dent. 2005, 65, 174–182. [Google Scholar]
- Lee, J.Y.; Rozier, R.G.; Lee, S.-Y.D.; Bender, D.; Ruiz, R.E. Development of a word recognition instrument to test health literacy in dentistry: The REALD-30–a brief communication. J. Public Health Dent. 2007, 67, 94–98. [Google Scholar] [CrossRef]
- Richman, J.A.; Lee, J.Y.; Rozier, R.G.; Gong, D.A.; Pahel, B.T.; Vann, W.F., Jr. Evaluation of a word recognition instrument to test health literacy in dentistry: The REALD-99. J. Public Health Dent. 2007, 67, 99–104. [Google Scholar] [CrossRef]
- Gong, D.A.; Lee, J.Y.; Rozier, R.G.; Pahel, B.T.; Richman, J.A.; Vann, W.F., Jr. Development and testing of the test of functional health literacy in dentistry (TOFHLiD). J. Public Health Dent. 2007, 67, 105–112. [Google Scholar] [CrossRef]
- Zhang, L.; Ding, D.; Fethney, J.; Neubeck, L.; Gallagher, R. Tools to measure health literacy among Chinese speakers: A systematic review. Patient Educ. Couns. 2020, 103, 888–897. [Google Scholar] [CrossRef] [PubMed]
- Rupareliya, D.A.; Shukla, Y.U. Need for Cross-Cultural Adaptation of Self-Reported Health Measures: Review Study. Indian J. Physiother. Occup. Ther. 2020, 14, 34–37. [Google Scholar]
- Beaton, D.E.; Bombardier, C.; Guillemin, F.; Ferraz, M.B. Guidelines for the process of cross-cultural adaptation of self-report measures. Spine J. 2000, 25, 3186–3191. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Guillemin, F. Cross-cultural Adaptation and Validation of Heatth Status Measures. Scand. J. Rheumatol. 2009, 24, 61–63. [Google Scholar] [CrossRef]
- Beaton, D.; Bombardier, C.; Guillemin, F.; Ferraz, M.B. Recommendations for the cross-cultural adaptation of the DASH & QuickDASH outcome measures. IWH 2007, 1, 1–45. [Google Scholar]
- Puga, V.O.; Lopes, A.D.; Costa, L.O. Assessment of cross-cultural adaptations and measurement properties of self-report outcome measures relevant to shoulder disability in Portuguese: A systematic review. Rev. Bras. Fisioter. 2012, 16, 85–93. [Google Scholar] [CrossRef] [Green Version]
- Maher, C.G.; Latimer, J.; Costa, L.O. The relevance of cross-cultural adaptation and clinimetrics for physical therapy instruments. Braz. J. Phys. Ther. 2007, 11, 245–252. [Google Scholar] [CrossRef] [Green Version]
- Karanicolas, P.J.; Bhandari, M.; Kreder, H.; Moroni, A.; Richardson, M.; Walter, S.D.; Norman, G.R.; Guyatt, G.H. Evaluating agreement: Conducting a reliability study. J. Bone Joint Surg.Am. 2009, 91, 99–106. [Google Scholar] [CrossRef]
- Prinsen, C.A.C.; Mokkink, L.B.; Bouter, L.M.; Alonso, J.; Patrick, D.L.; de Vet, H.C.; Terwee, C.B. COSMIN guideline for systematic reviews of patient-reported outcome measures. Qual. Life Res. 2018, 27, 1147–1157. [Google Scholar] [CrossRef] [Green Version]
- Mokkink, L.B.; De Vet, H.C.; Prinsen, C.A.; Patrick, D.L.; Alonso, J.; Bouter, L.M.; Terwee, C.B. COSMIN risk of bias checklist for systematic reviews of patient-reported outcome measures. Qual. Life Res. 2018, 27, 1171–1179. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mokkink, L.B.; Prinsen, C.; Patrick, D.L.; Alonso, J.; Bouter, L.M.; de Vet, H.; Terwee, C.B. COSMIN methodology for systematic reviews of patient-reported outcome measures (PROMs). User Manual. 2018, 78, 1. [Google Scholar]
- Parthasarathy, D.S.; McGrath, C.; Bridges, S.M.; Wong, H.M.; Yiu, C.; Au, T. Efficacy of instruments measuring oral health literacy: A systematic review. Oral Health Prev. Dent. 2014, 12, 2233–2243. [Google Scholar]
- Ghaffari, M.; Rakhshanderou, S.; Ramezankhani, A.; Mehrabi, Y.; Safari-Moradabadi, A. Systematic review of the tools of oral and dental health literacy: Assessment of conceptual dimensions and psychometric properties. BMC Oral Health 2020, 20, 186. [Google Scholar] [CrossRef]
- Dickson-Swift, V.; Kenny, A.; Farmer, J.; Gussy, M.; Larkins, S. Measuring oral health literacy: A scoping review of existing tools. BMC Oral Health 2014, 14, 148. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kanchan, S.; Sagarkar, A.R.; Ranadheer, R. Critically appraisal of tools to measure using the cosmin checklist. Indian J. Public Health Res. Dev. 2020, 11, 666–670. [Google Scholar] [CrossRef]
- Costa, L.d.C.M.; Maher, C.G.; McAuley, J.H.; Costa, L.O.P. Systematic review of cross-cultural adaptations of McGill Pain Questionnaire reveals a paucity of clinimetric testing. J. Clin. Epidemiol. 2009, 62, 934–943. [Google Scholar] [CrossRef]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G.; Group, P. Preferred reporting items for systematic reviews and meta-analyses: The PRISMA statement. PLoS Med. 2009, 6, e1000097. [Google Scholar] [CrossRef] [Green Version]
- Booth, A.; Clarke, M.; Dooley, G.; Ghersi, D.; Moher, D.; Petticrew, M.; Stewart, L. The nuts and bolts of PROSPERO: An international prospective register of systematic reviews. Syst. Rev. 2012, 1, 2. [Google Scholar] [CrossRef] [Green Version]
- Costantino, G.; Montano, N.; Casazza, G. When should we change our clinical practice based on the results of a clinical study? The hierarchy of evidence. Intern. Emerg. Med. 2015, 10, 745–747. [Google Scholar] [CrossRef]
- Clarivate Analytics. EndNote X9.1.1; Clarivate Analytics: San Francisco, CA, USA, 2019. [Google Scholar]
- Mokkink, L.B.; Prinsen, C.A.C.; Bouter, L.M.; de Vet, H.C.W.; Terwee, C.B. The COnsensus-based Standards for the selection of health Measurement INstruments (COSMIN) and how to select an outcome measurement instrument. Braz. J. Phys. Ther. 2016, 20, 105–113. [Google Scholar] [CrossRef] [Green Version]
- Terwee, C.B.; Bot, S.D.; de Boer, M.R.; van der Windt, D.A.; Knol, D.L.; Dekker, J.; Bouter, L.; de Vet, H.C. Quality criteria were proposed for measurement properties of health status questionnaires. J. Clin. Epidemiol. 2007, 60, 34–42. [Google Scholar] [CrossRef] [Green Version]
- Terwee, C.B.; Prinsen, C.A.C.; Chiarotto, A.; Westerman, M.J.; Patrick, D.L.; Alonso, J.; Bouter, L.; De Vet, H.C.W.; Mokkink, L.B. COSMIN methodology for evaluating the content validity of patient-reported outcome measures: A Delphi study. Qual. Life Res. 2018, 27, 1159–1170. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Abma, I.L.; Rovers, M.; van der Wees, P.J. Appraising convergent validity of patient-reported outcome measures in systematic reviews: Constructing hypotheses and interpreting outcomes. BMC Res. Notes 2016, 9, 26. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gadermann, A.M.; Chen, M.Y.; Emerson, S.D.; Zumbo, B.D. Examining Validity Evidence of Self-Report Measures Using Differential Item Functioning. Methodology 2018, 14, 165–176. [Google Scholar] [CrossRef]
- Tadakamadla, S.K.; Quadri, M.F.A.; Pakpour, A.H.; Zailai, A.M.; Sayed, M.E.; Mashyakhy, M.; Inamdar, A.S.; Tadakamadla, J. Reliability and validity of Arabic rapid estimate of adult literacy in dentistry (AREALD-30) in Saudi Arabia. BMC Oral Health 2014, 14, 120. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Junkes, M.C.; Fraiz, F.C.; Sardenberg, F.; Lee, J.Y.; Paiva, S.M.; Ferreira, F.M. Validity and reliability of the Brazilian version of the Rapid Estimate of Adult Literacy in Dentistry—BREALD-30. PLoS ONE 2015, 10, e0131600. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cruvinel, A.F.P.; Méndez, D.A.C.; Oliveira, J.G.; Gutierres, E.; Lotto, M.; Machado, M.A.A.; Oliveira, T.M.; Cruvinel, T. The Brazilian version of the 20-item rapid estimate of adult literacy in medicine and dentistry. PeerJ 2017, 5, e3744. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wong, H.M.; Bridges, S.M.; Yiu, C.K.; McGrath, C.P.; Au, T.K.; Parthasarathy, D.S. Development and validation of Hong Kong rapid estimate of adult literacy in dentistry. J. Investig. Clin. Dent. 2012, 3, 118–127. [Google Scholar] [CrossRef] [PubMed]
- Pakpour, A.H.; Lawson, D.M.; Tadakamadla, S.K.; Fridlund, B. Validation of Persian rapid estimate of adult literacy in dentistry. J. Investig. Clin. Dent. 2016, 7, 198–206. [Google Scholar] [CrossRef]
- Cartes-Velásquez, R.; Luengo-Machucaa, L. Adaptation and Validation of the Rapid Estimate of Adult Literacy in Dentistry for Chilean Population. P. R. Health Sci. J. 2018, 37, 52–54. [Google Scholar] [PubMed]
- Sfeatcu, R.; Lie, S.A.; Funieru, C.; Åström, A.N.; Virtanen, J.I. The reliability and validity of the Romanian rapid estimate of adult literacy in dentistry (RREALD-30). Acta Odontol. Scand. 2020, 79, 132–138. [Google Scholar] [CrossRef] [PubMed]
- Mialhe, F.L.; Tenani, C.F.; De Checchi, M.H.R.; Jamieson, L.; Ju, X. Psychometric properties of Health Literacy in Dentistry scale in an elderly Brazilian population. Braz. Oral Res. 2020, 34, e021. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Firmino, R.T.; Granville-Garcia, A.F.; McGrath, C.P.; Bendo, C.B.; Ferreira, F.M.; Paiva, S.M. Validation for Brazilian Portuguese language of the Hong Kong Oral Health Literacy Assessment Task for Paediatric Dentistry (BOHLAT-P). Int. J. Paediatr. Dent. 2020, 30, 234–243. [Google Scholar] [CrossRef]
- Bado, F.M.R.; Ferreira, F.M.; de Souza Barbosa, T.; Mialhe, F.L. Translation and cross-cultural adaptation of the oral health literacy assessment-Spanish to Brazilian portuguese. Pesqui. Bras. Clin. Integr. 2017, 17, 1–10. [Google Scholar] [CrossRef]
- Vyas, S.; Nagarajappa, S.; Dasar, P.L.; Mishra, P. Linguistic adaptation and psychometric evaluation of original Oral Health Literacy-Adult Questionnaire (OHL-AQ). J. Adv. Med. Educ. Prof. 2016, 4, 163–169. [Google Scholar]
- Ramlay, M.Z.; Saddki, N.; Tin-Oo, M.M.; Arifin, W.N. Cross-Cultural Adaptation and Validation of Oral Health Literacy Instrument (OHLI) for Malaysian Adults. Int. J. Environ. Res. Public Health 2020, 17, 5407. [Google Scholar] [CrossRef]
- Cartes-Velásquez, R.A.; Machuca, L.L. Adaptation and validation of the oral health literacy instrument for the Chilean population. Int. Dent. J. 2017, 67, 215–220. [Google Scholar] [CrossRef]
- Blizniuk, A.; Ueno, M.; Furukawa, S.; Kawaguchi, Y. Evaluation of a Russian version of the oral health literacy instrument (OHLI). BMC Oral Health 2014, 14, 141. [Google Scholar] [CrossRef] [Green Version]
- Deeraksa, S.; Chaichit, R.; Muktabhant, B.; Udompanich, S. Reliability and Validity of the Thai Version of Rapid Estimate of Adult Literacy in Dentistry. J. Int. Oral Health 2019, 11, 132. [Google Scholar]
- Peker, K.; Köse, T.E.; Güray, B.; Uysal, Ö.; Erdem, T.L. Reliability and validity of the Turkish version of the Rapid Estimate of Adult Literacy in Dentistry (TREALD-30). Acta Odontol. Scand. 2017, 75, 198–207. [Google Scholar] [CrossRef] [PubMed]
- Flynn, P.M.; John, M.T.; Naik, A.; Kohli, N.; VanWormer, J.; Self, K. Psychometric properties of the English version of the Oral Health Literacy Adults Questionnaire-OHL-AQ. Community Dent. Health 2016, 33, 274–280. [Google Scholar]
- Sabbahi, D.A.; Lawrence, H.P.; Limeback, H.; Rootman, I. Development and evaluation of an oral health literacy instrument for adults. Community Dent. Oral Epidemiol. 2009, 37, 451–462. [Google Scholar] [CrossRef] [PubMed]
- Gironda, M.; Der-Martirosian, C.; Messadi, D.; Holtzman, J.; Atchison, K. A brief 20-item dental/medical health literacy screen (REALMD-20). J. Public Health Dent. 2013, 73, 50–55. [Google Scholar] [CrossRef] [Green Version]
- Lee, J.; Stucky, B.; Rozier, G.; Lee, S.Y.; Zeldin, L.P. Oral Health Literacy Assessment: Development of an oral health literacy instrument for Spanish speakers. J. Public Health Dent. 2013, 73, 1–8. [Google Scholar] [CrossRef] [Green Version]
- Wong, H.M.; Bridges, S.M.; Yiu, C.K.; McGrath, C.P.; Au, T.K.; Parthasarathy, D.S. Validation of the Hong Kong oral health literacy assessment task for paediatric dentistry (HKOHLAT-P). Int. J. Paediatr. Dent. 2013, 23, 366–375. [Google Scholar] [CrossRef]
- Jones, K.; Parker, E.; Mills, H.; Brennan, D.; Jamieson, L. Development and psychometric validation of a Health Literacy in Dentistry scale (HeLD). Community Dent. Health 2014, 31, 37–43. [Google Scholar]
- Assessment, Q.O.L. The World Health Organization quality of life assessment (WHOQOL): Position paper from the World Health Organization. Soc Sci Med. 1995, 41, 1403–1409. [Google Scholar] [CrossRef]
- Swami, V.; Barron, D. Translation and validation of body image instruments: Challenges, good practice guidelines, and reporting recommendations for test adaptation. Body Image 2019, 31, 204–220. [Google Scholar] [CrossRef]
- Hall, D.A.; Domingo, S.Z.; Hamdache, L.Z.; Manchaiah, V.; Thammaiah, S.; Evans, C.; Wong, L.L.N. A good practice guide for translating and adapting hearing-related questionnaires for different languages and cultures. Int. J. Audiol. 2018, 57, 161–175. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gjersing, L.; Caplehorn, J.R.; Clausen, T. Cross-cultural adaptation of research instruments: Language, setting, time and statistical considerations. BMC Med. Res. Methodol. 2010, 10, 13. [Google Scholar] [CrossRef] [Green Version]
- Winser, S.J.; Smith, C.M.; Hale, L.A.; Claydon, L.S.; Whitney, S.L.; Mehta, P. COSMIN for quality rating systematic reviews on psychometric properties. Phys. Ther. Rev. 2015, 20, 132–134. [Google Scholar] [CrossRef]
- Merom, D.; John, J.R. Measurement Issues in Quantitative Research. Handbook of Research Methods in Health Social Sciences; Springer Singapore: Singapore, 2018; pp. 1–20. [Google Scholar]
- Sharma, M.; Petosa, R.L. Measurement and Evaluation for Health Educators; Jones & Bartlett Publishers: Burlington, MA, USA, 2014. [Google Scholar]
- Koo, T.K.; Li, M.Y. A guideline of selecting and reporting intraclass correlation coefficients for reliability research. J. Chiropr. Med. 2016, 15, 155–163. [Google Scholar] [CrossRef] [Green Version]
- Reichenheim, M.E.; Hökerberg, Y.H.M.; de Moraes, C.L. Assessing construct structural validity of epidemiological measurement tools: A seven-step roadmap. Cad. Saúde. Pública. 2014, 30, 927–939. [Google Scholar] [CrossRef] [Green Version]
- Yong, A.G.; Pearce, S. A beginner’s guide to factor analysis: Focusing on exploratory factor analysis. Tutor. Quant. Methods Psychology. 2013, 9, 79–94. [Google Scholar] [CrossRef]
- Sierevelt, I.N.; Van Eekeren, I.C.M.; Haverkamp, D.; Reilingh, M.L.; Terwee, C.B.; Kerkhoffs, G.M.M.J. Evaluation of the Dutch version of the Foot and Ankle Outcome Score (FAOS): Responsiveness and minimally important change. Knee Surg. Sports Traumatol. Arthrosc. 2016, 24, 1339–1347. [Google Scholar] [CrossRef]
- Terwee, C.B.; Mokkink, L.B.; Knol, D.L.; Ostelo, R.W.; Bouter, L.M.; de Vet, H.C. Rating the methodological quality in systematic reviews of studies on measurement properties: A scoring system for the COSMIN checklist. Qual. Life Res. 2012, 21, 651–657. [Google Scholar] [CrossRef] [Green Version]
- Singleton, K.; Krause, E. Understanding cultural and linguistic barriers to health literacy. OJIN Online J. Issues Nurs. 2009, 14, 4. [Google Scholar]
- Whiting, P.F.; Rutjes, A.W.; Westwood, M.E.; Mallett, S.; Deeks, J.J.; Reitsma, J.B.; Leeflang, M.M.; Sterne, J.A.; Bossuyt, P.M. QUADAS-2: A revised tool for the quality assessment of diagnostic accuracy studies. Ann. Intern. Med. 2011, 155, 529–536. [Google Scholar] [CrossRef]
- Lucas, N.P.; Macaskill, P.; Irwig, L.; Bogduk, N. The development of a quality appraisal tool for studies of diagnostic reliability (QAREL). J. Clin. Epidemiol. 2010, 63, 854–861. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
| Abbreviation | Name of Instrument | Year | Country | Authors | Type of Tool |
|---|---|---|---|---|---|
| AREALD-30 [54] | Arabic Rapid Estimate of Adult Literacy in Dentistry | 2014 | Saudi Arabia | Tadakamadla et al. | 30-item word recognition tool |
| Brazilian-HeLD [61] | Brazilian-Portuguese version of Health Literacy in Dentistry (HeLD) scale | 2020 | Brazil | Mialhe et al. | 29-item (HeLD-29) and 14-item (HeLD-14) tools assessing access, support, understanding, use, economic barriers, receptivity, and communication |
| BOHLAT-P [62] | Brazilian-Portuguese version of the Hong Kong OHL Assessment Task for Pediatric Dentistry (HKOHLAT-P) | 2020 | Brazil | Firmino et al. | 49-item tool assessing oral health knowledge, numeracy test and comprehensive |
| BREALD-30 [55] | Brazilian version of the Rapid Estimate of Adult Literacy in Dentistry | 2015 | Brazil | Junkes et al. | 30-item word recognition tool |
| BREALMD-20 [56] | Brazilian version of 20-item Rapid Estimate Adult Literacy in Medicine and Dentistry | 2017 | Brazi | Cruvinel et al. | 20-item word recognition tool |
| HKREALD-30 [57] | Hong Kong Rapid Estimate of Adult Literacy in Dentistry | 2012 | Hong Kong | Wong et al. | 30-item word recognition tool |
| IREALD-99 [58] | Rapid Estimate of Adult Literacy in Dentistry-99 for Iranian population | 2016 | Iran | Pakpour et al. | 99-item word recognition tool |
| OHLA-B [63] | Oral Health Literacy Assessment—Brazilian | 2017 | Brazil | Bado et al. | 30-item word recognition and comprehension tool |
| OHL-AQ-H [64] | Oral Health Literacy Adult Questionnaire—Hindi Version | 2016 | India | Vyas et al. | 17-item tool encompassing comprehension, numeracy test, listening, and decision-making domains |
| OHLI-Cl [66] | Chilean version of OHLI | 2017 | Chile | Cartes-Velásquez and Luengo-Machucaa | 57-item functional health literacy tool (38 items for reading comprehension and 19 items for numeracy test) |
| OHLI-M [65] | Oral health literacy instrument—Malay version | 2020 | Malaysia | Ramlay et al. | 57-item functional health literacy tool (38 items for reading comprehension and 19 items for numeracy test) |
| REALD-30 for Chilean population [59] | Rapid Estimate of Adult Literacy in Dentistry for Chilean population | 2018 | Chile | Cartes- Velásquez and Luengo-Machucaa | 30-item word recognition tool |
| R-OHLI [67] | Russian version of the OHLI | 2014 | Belarus | Blizniuk et al. | 57-item functional health literacy tool containing 38 items for reading comprehension and 19 items for a numeracy test |
| RREALD-30 [60] | Romanian rapid estimate of adult literacy in dentistry | 2020 | Romania | Sfeatcu et al. | 30-item word recognition tool |
| ThREALD-30 [68] | Thai version of Rapid Estimate of Adult Literacy in Dentistry | 2019 | Thailand | Deeraksa et al. | 30-item word recognition tool |
| TREALD-30 [69] | Turkish version of Rapid Estimate of Adult Literacy in Dentistry-30 | 2017 | Turkey | Peker et al. | 30-item word recognition tool |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Praveen, S.; Parmar, J.; Chandio, N.; Arora, A. A Systematic Review of Cross-Cultural Adaptation and Psychometric Properties of Oral Health Literacy Tools. Int. J. Environ. Res. Public Health 2021, 18, 10422. https://doi.org/10.3390/ijerph181910422
Praveen S, Parmar J, Chandio N, Arora A. A Systematic Review of Cross-Cultural Adaptation and Psychometric Properties of Oral Health Literacy Tools. International Journal of Environmental Research and Public Health. 2021; 18(19):10422. https://doi.org/10.3390/ijerph181910422
Chicago/Turabian StylePraveen, Sobiya, Jinal Parmar, Navira Chandio, and Amit Arora. 2021. "A Systematic Review of Cross-Cultural Adaptation and Psychometric Properties of Oral Health Literacy Tools" International Journal of Environmental Research and Public Health 18, no. 19: 10422. https://doi.org/10.3390/ijerph181910422
APA StylePraveen, S., Parmar, J., Chandio, N., & Arora, A. (2021). A Systematic Review of Cross-Cultural Adaptation and Psychometric Properties of Oral Health Literacy Tools. International Journal of Environmental Research and Public Health, 18(19), 10422. https://doi.org/10.3390/ijerph181910422