
A Scoping Review on Minimum Foot Clearance: An Exploration of Level-Ground Clearance in Individuals with Abnormal Gait


Abstract
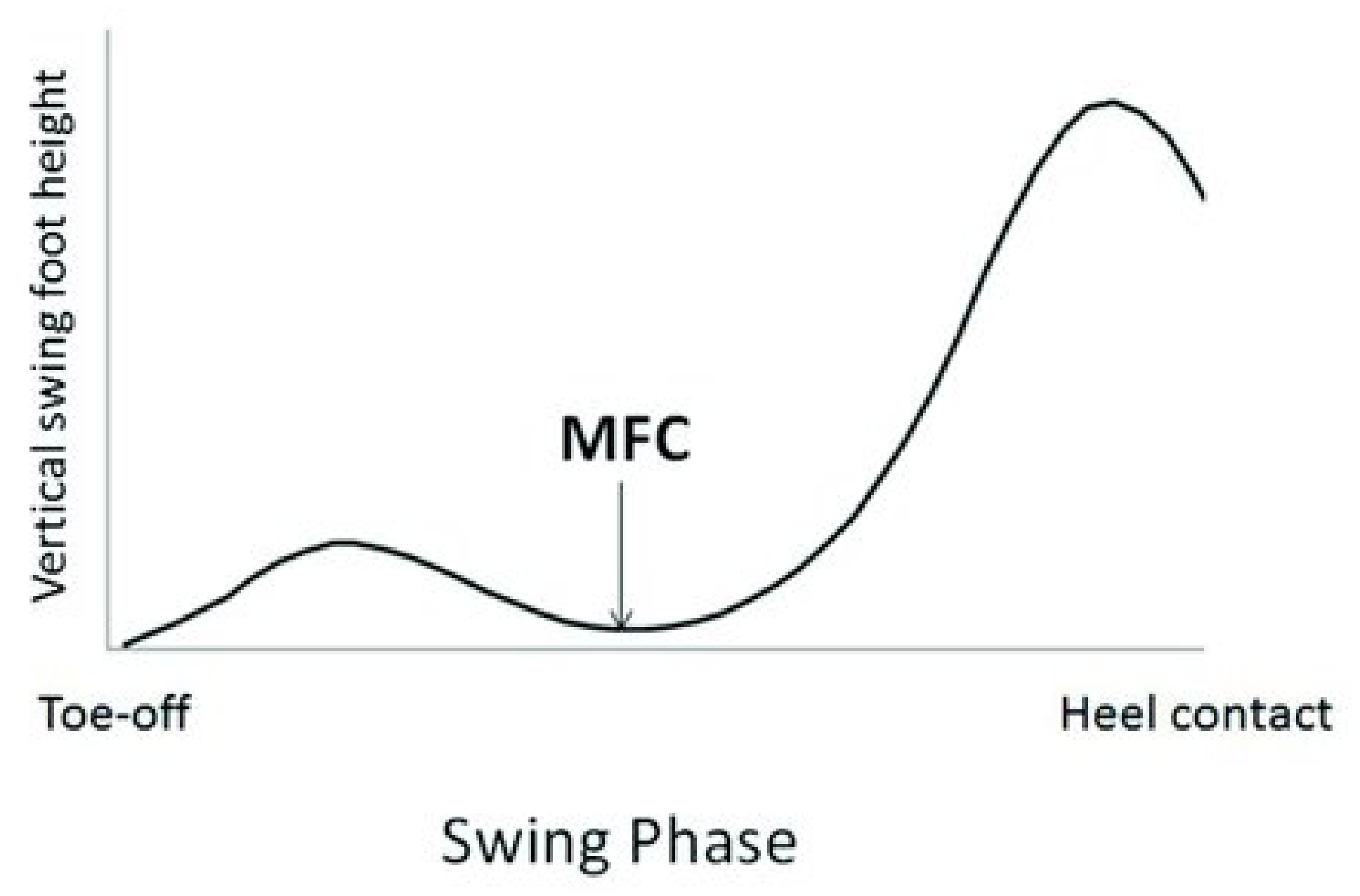
1. Introduction
2. Materials and Methods
2.1. Information Sources and Search Strategy
2.2. Eligibility Criteria
2.3. Selection of Papers
2.4. Data Charting and Analysis for RQ2
2.5. Critical Appraisal of the Studies
3. Results
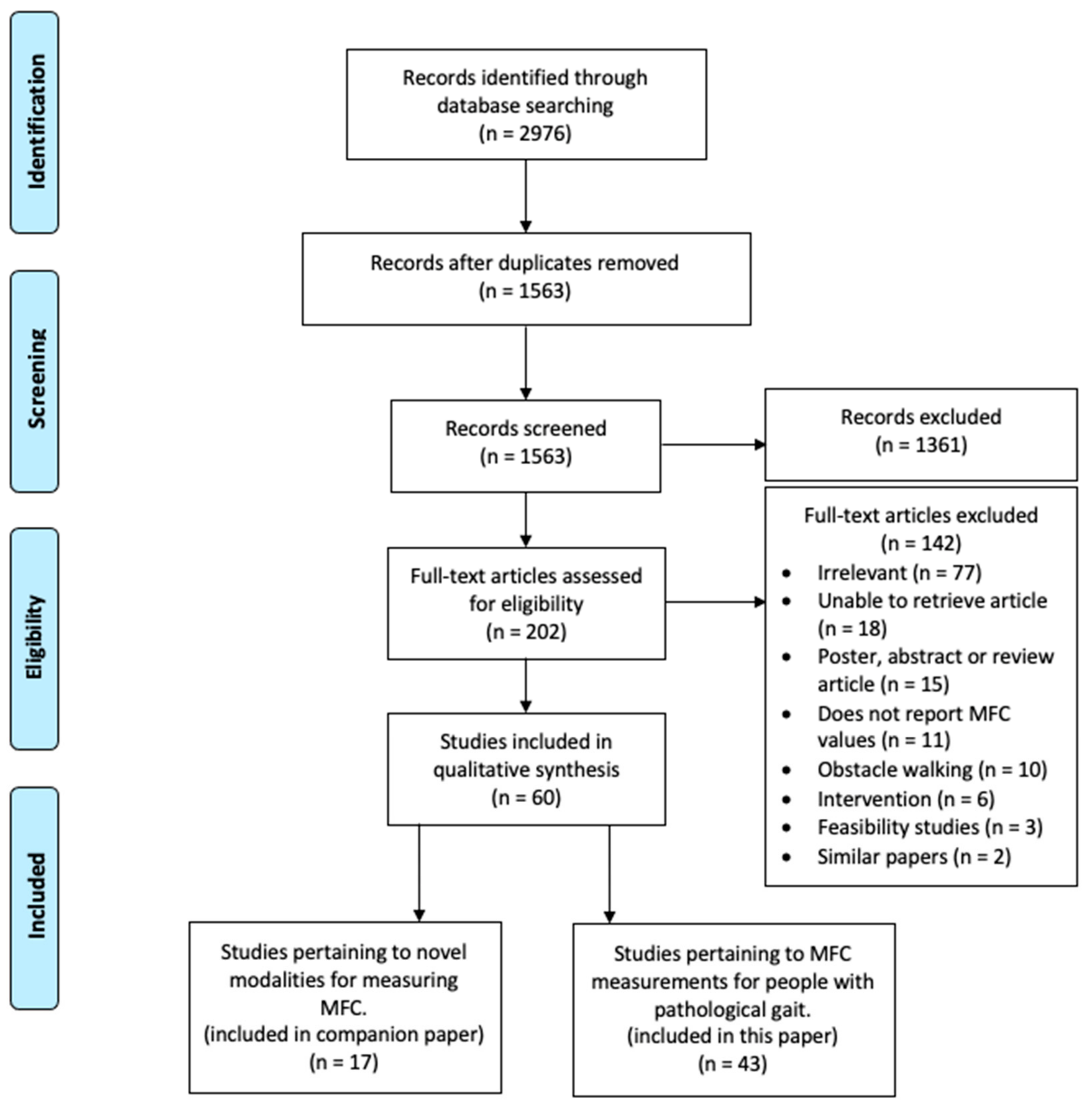
3.1. Search and Selection of Articles
3.2. Characteristics of Included Articles
3.2.1. Study Design Characteristics
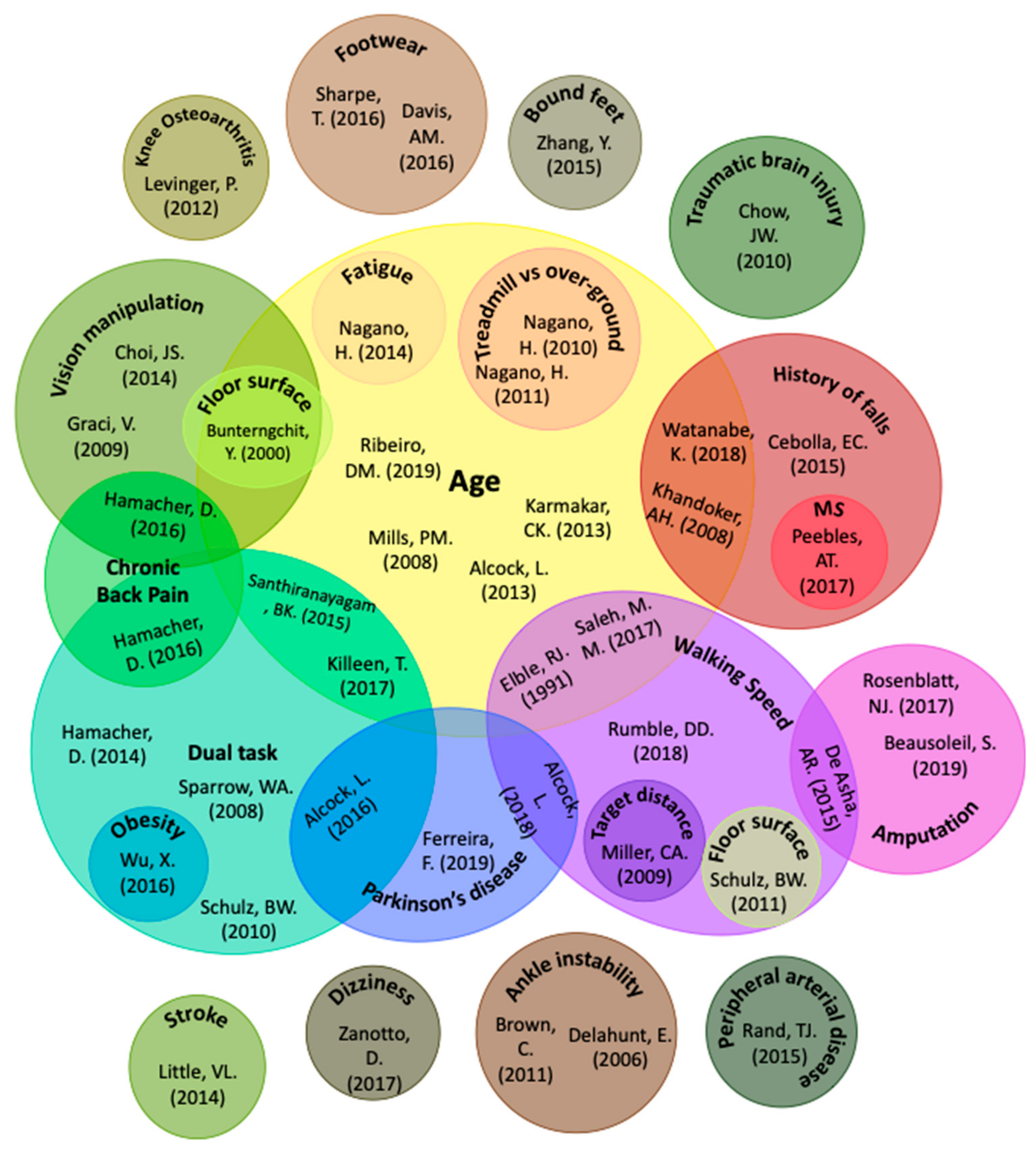
3.2.2. Areas of Research/Characteristics of Conditions Assessed
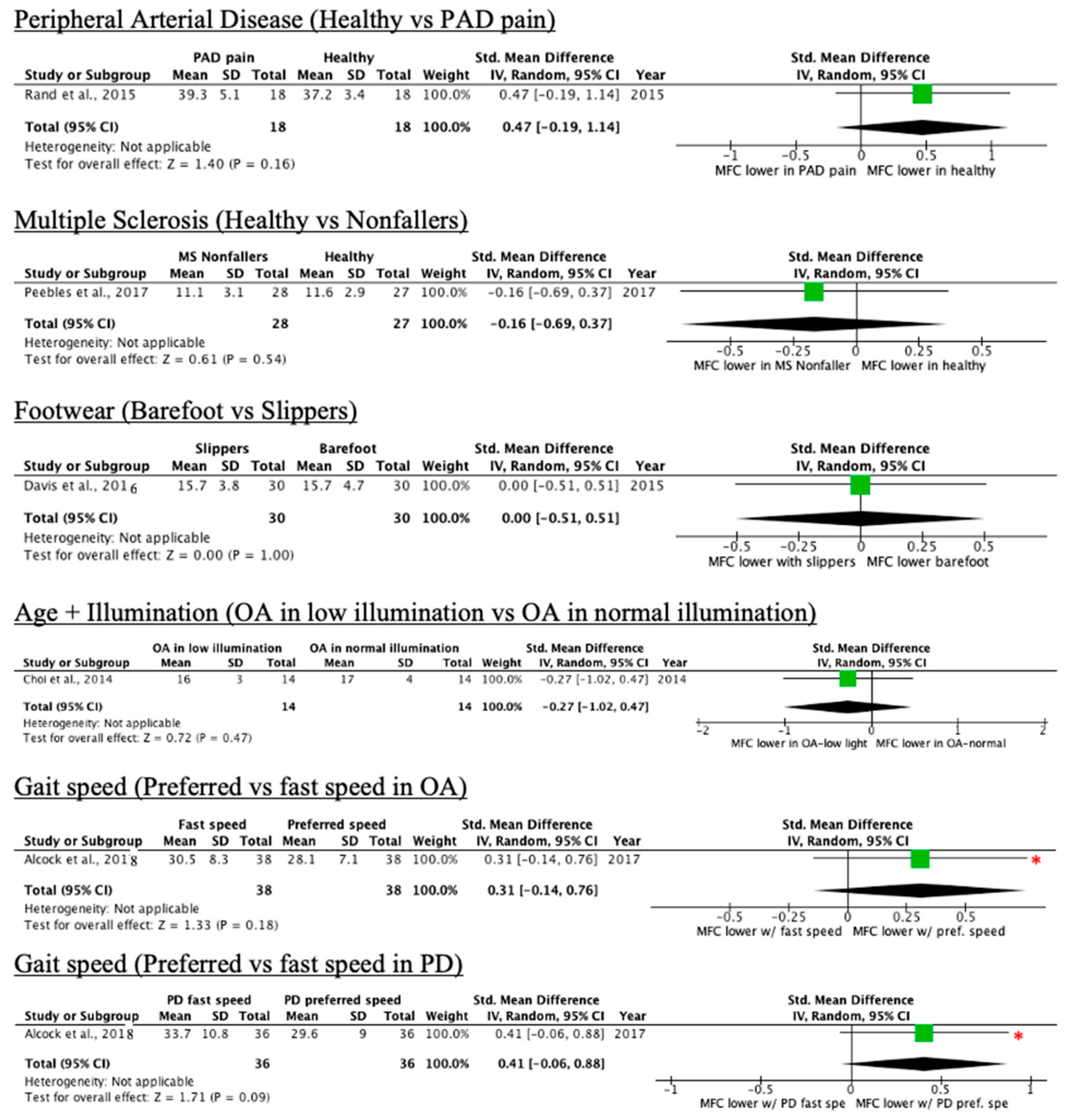
Conditions without an Impact on MFC Mean or Median
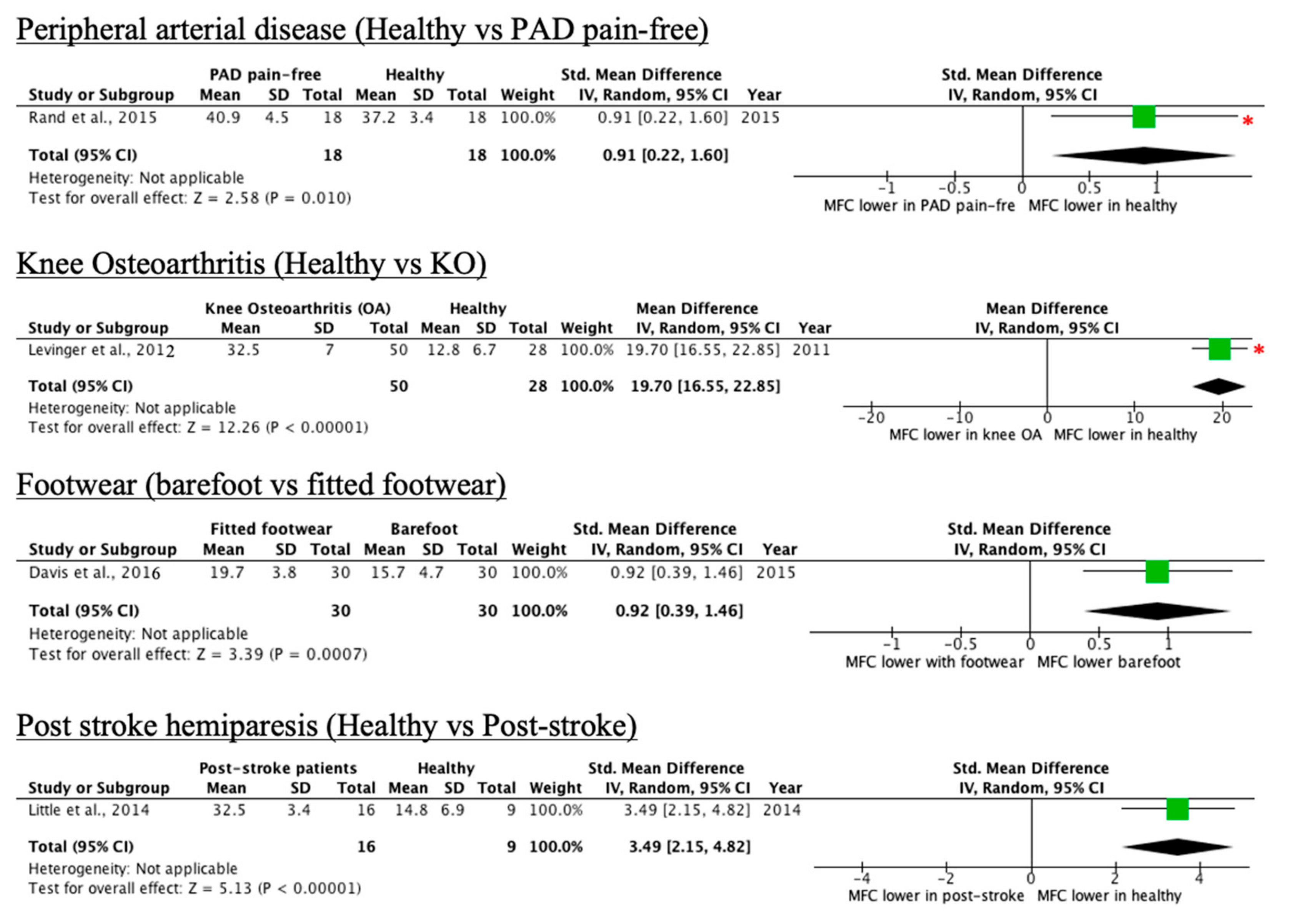
Conditions That Increase MFC Mean or Median
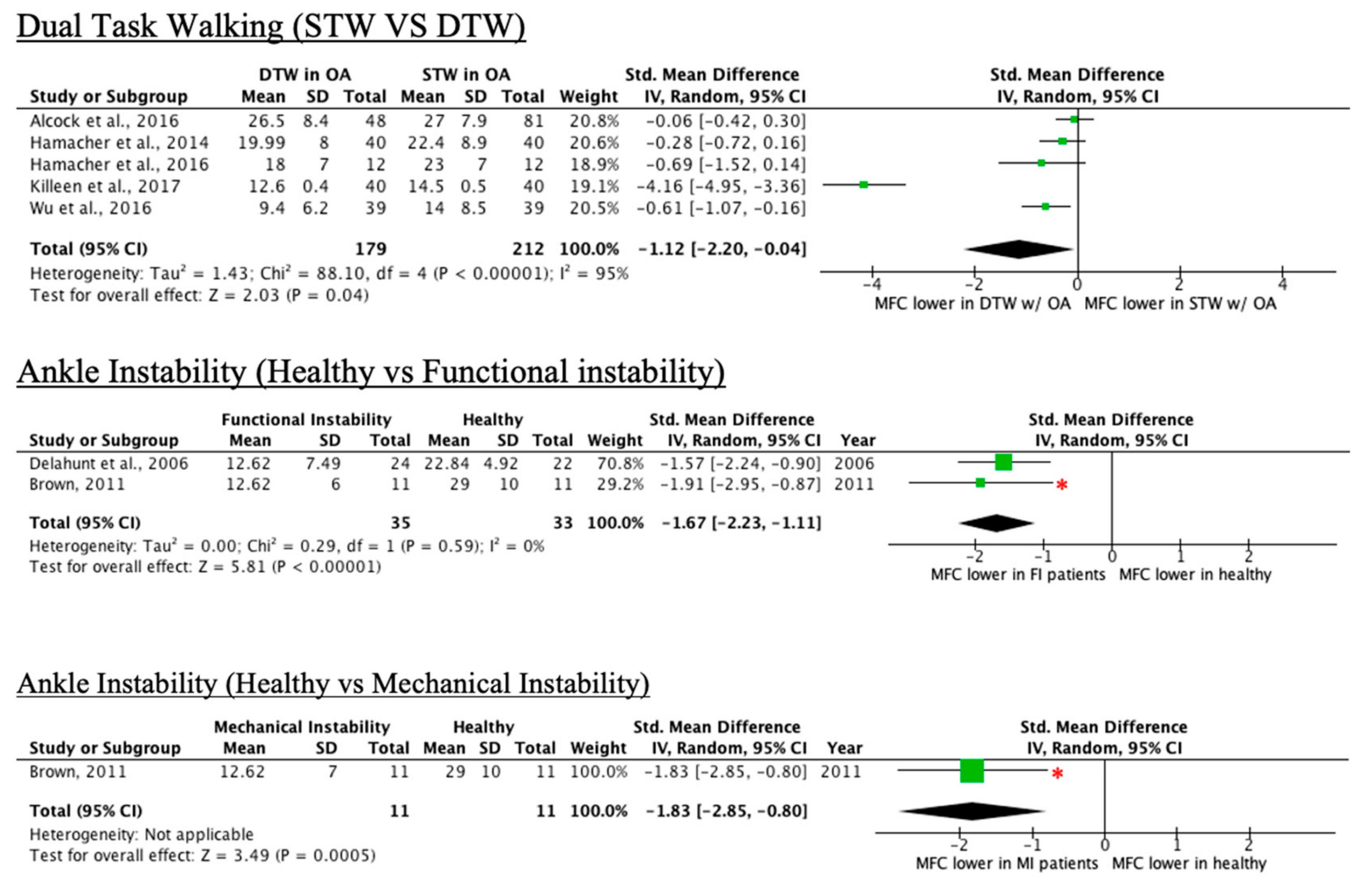
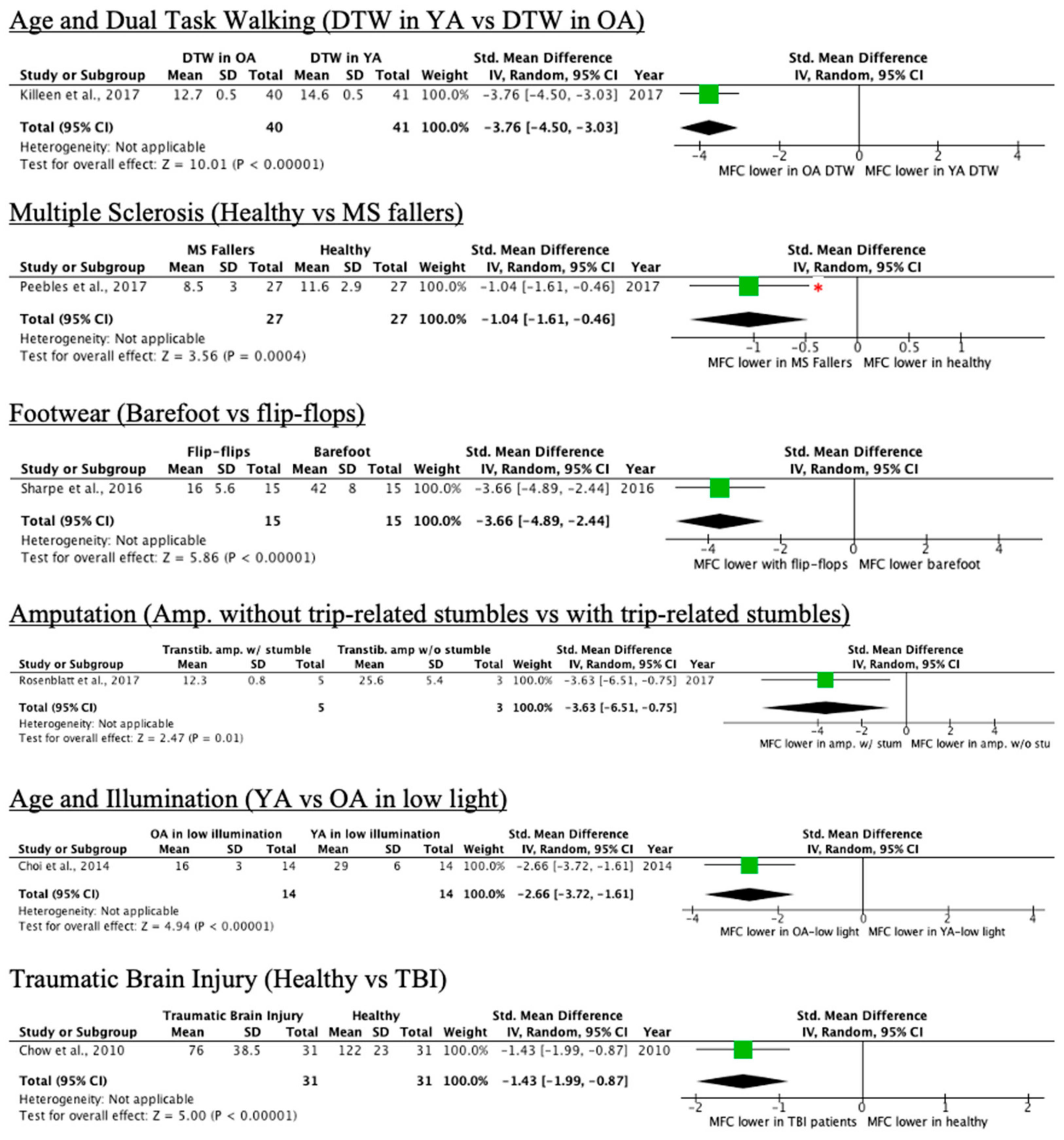
Conditions That Decrease MFC
Other Conditions
4. Discussion
4.1. Notable Conditions Assessed in Literature and their Limitations
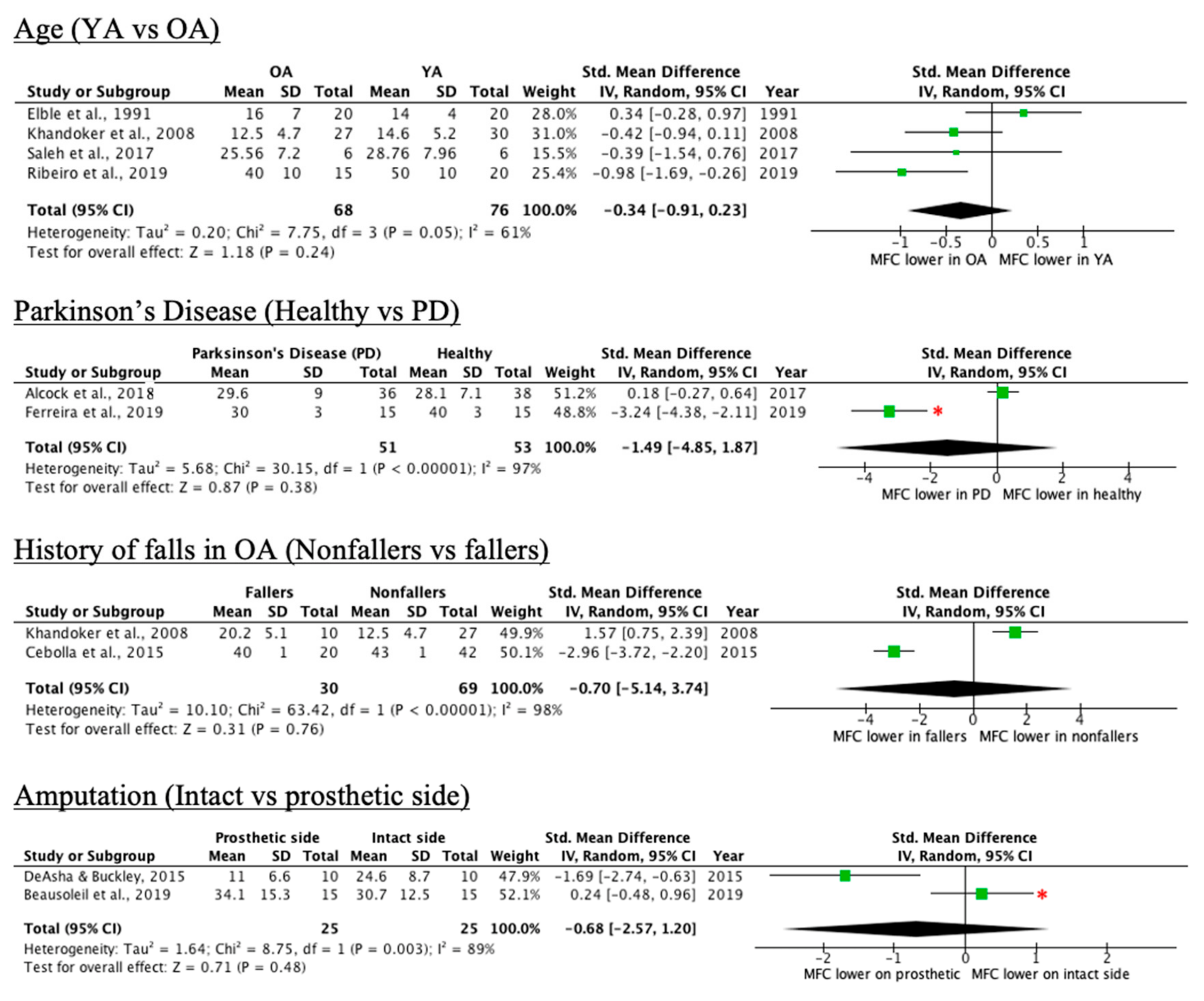
4.1.1. Age
4.1.2. History of Falls
4.1.3. Dual-Task Walking
4.1.4. Other Notable Conditions
4.2. Research Methods Used in Studies and General Limitations among all Conditions
4.3. Implications
4.4. Recommendations for Future Research
4.5. Limitations of this Scoping Review
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
References
- Johnson, S.; Kelly, S.; Rasali, D. Differences in fall injury hospitalization and related survival rates among older adults across age, sex, and areas of residence in Canada. Inj. Epidemiol. 2015, 2, 1–10. [Google Scholar] [CrossRef] [PubMed]
- Blake, A.J.; Morgan, K.; Bendall, M.J.; Dallosso, H.; Ebrahim, S.B.J.; Arie, T.H.D.; Fentem, P.H.; Bassey, E.J. Falls By Elderly People At Home: Prevalence And Associated Factors. Age Ageing 1988, 17, 365–372. [Google Scholar] [CrossRef] [PubMed]
- Li, W.; Keegan, T.H.; Sternfeld, B.; Sidney, S.; Quesenberry, C.P.; Kelsey, J.L. Outdoor falls among middle-aged and older adults: A neglected public health problem. Am. J. Public Health 2006, 96, 1192–1200. [Google Scholar] [CrossRef] [PubMed]
- Florence, C.S.; Bergen, G.; Atherly, A.; Burns, E.; Stevens, J.; Drake, C. Medical Costs of Fatal and Nonfatal Falls in Older Adults. J. Am. Geriatr. Soc. 2018, 66, 693–698. [Google Scholar] [CrossRef]
- Pai, Y.-C. Movement Termination and Stability in Standing. Exerc. Sport Sci. Rev. 2003, 31, 19–25. [Google Scholar] [CrossRef]
- Hanatsu, N.H.; Begg, R.K. Shoe-Insole Technology for Injury Prevention in Walking. Sensors 2018, 18, 1468. [Google Scholar] [CrossRef]
- Wang, W.; Adamczyk, P.G. Analyzing gait in the real world using wearable movement sensors and frequently repeated movement paths. Sensors 2019, 19, 1925. [Google Scholar] [CrossRef]
- Schulz, B.W.; Lloyd, J.; Lee, W.E., III. The effects of everyday concurrent tasks on overground minimum toe clearance and gait parameters. Gait Posture 2010, 32, 18–22. [Google Scholar] [CrossRef]
- Americans with Disabilities Act (ADA) Standards; U.S. Department of Labor: Washington, DC, USA, 1990.
- Toronto, C.O. Accessibility Design Guidelines; Diversity Management and Community Engagement Corporate Policy/Healthy City Office: Toronto, ON, Canada, 2004.
- Panero, E.; Digo, E.; Agostini, V.; Gastaldi, L. Comparison of Different Motion Capture Setups for Gait Analysis: Validation of spatio-temporal parameters estimation. In Proceedings of the 2018 IEEE International Symposium on Medical Measurements and Applications MeMeA, Rome, Italy, 11–13 June 2018; pp. 1–6. [Google Scholar] [CrossRef]
- Delfi, G.; Al Bochi, A.; Dutta, T. A scoping review on minimum foot clearance measurement: Sensing modalities. Int. J. Environ. Res. Public Health 2021. Submitted. [Google Scholar]
- Nagano, H.; Begg, R.; Sparrow, W.A. Controlling Swing Foot Center of Mass and Toe Trajectory to Minimize Tripping Risk; IEEE: Piscataway, NJ, USA, 2010; pp. 4854–4857. [Google Scholar] [CrossRef]
- Saleh, M.M.; Parasuraman, S.; Deisy, C.; Padmavathy, S.; Kingsly, D.; Singh, J.; Khan, M. Effects of Aging on Human Gait Stability; IEEE: Piscataway, NJ, USA, 2017; p. 5. [Google Scholar] [CrossRef]
- Nagano, H.; Begg, R.K.; Sparrow, W.A.; Taylor, S. Ageing and limb dominance effects on foot-ground clearance during treadmill and overground walking. Clin. Biomech. 2011, 26, 962–968. [Google Scholar] [CrossRef]
- Hamacher, D.; Hamacher, D.; Herold, F.; Schega, L. Are there differences in the dual-task walking variability of minimum toe clearance in chronic low back pain patients and healthy controls? Gait Posture 2016, 49, 97–101. [Google Scholar] [CrossRef]
- Peebles, A.T.; Bruetsch, A.P.; Lynch, S.G.; Huisinga, J.M. Dynamic balance in persons with multiple sclerosis who have a falls history is altered compared to non-fallers and to healthy controls. J. Biomech. 2017, 63, 158–163. [Google Scholar] [CrossRef]
- Beausoleil, S.; Miramand, L.; Turcot, K. Evolution of gait parameters in individuals with a lower-limb amputation during a six-minute walk test. Gait Posture 2019, 72, 40–45. [Google Scholar] [CrossRef]
- Ferreira, F.; Gago, M.F.; Bicho, E.; Carvalho, C.; Mollaei, N.; Rodrigues, L.; Sousa, N.; Rodrigues, P.P.; Ferreira, C.; Gama, J. Gait stride-to-stride variability and foot clearance pattern analysis in Idiopathic Parkinson’s Disease and Vascular Parkinsonism. J. Biomech. 2019, 92, 98–104. [Google Scholar] [CrossRef]
- Hamacher, D.; Hamacher, D.; Krowicki, M.; Schega, L. Gait Variability in Chronic Back Pain Sufferers with Experimentally Diminished Visual Feedback: A Pilot Study. J. Mot. Behav. 2015, 48, 205–208. [Google Scholar] [CrossRef]
- Hamacher, D.; Hamacher, D.; Schega, L. Towards the importance of minimum toe clearance in level ground walking in a healthy elderly population. Gait Posture 2014, 40, 727–729. [Google Scholar] [CrossRef] [PubMed]
- Brown, C. Foot clearance in walking and running in individuals with ankle instability. Am. J. Sports Med. 2011, 39, 1769–1776. [Google Scholar] [CrossRef] [PubMed]
- Mills, P.M.; Barrett, R.; Morrison, S. Toe clearance variability during walking in young and elderly men. Gait Posture 2008, 28, 101–107. [Google Scholar] [CrossRef] [PubMed]
- Alcock, L.; Galna, B.; Lord, S.; Rochester, L. Characterisation of foot clearance during gait in people with early Parkinsons disease: Deficits associated with a dual task. J. Biomech. 2016, 49, 2763–2769. [Google Scholar] [CrossRef] [PubMed]
- Davis, A.M.; Galna, B.; Murphy, A.T.; Williams, C.M.; Haines, T.P. Effect of footwear on minimum foot clearance, heel slippage and spatiotemporal measures of gait in older women. Gait Posture 2016, 44, 43–47. [Google Scholar] [CrossRef]
- Alcock, L.; Galna, B.; Perkins, R.; Lord, S.; Rochester, L. Step length determines minimum toe clearance in older adults and people with Parkinson’s disease. J. Biomech. 2018, 71, 30–36. [Google Scholar] [CrossRef]
- Zanotto, D.; Mamuyac, E.M.; Chambers, A.R.; Nemer, J.S.; Stafford, J.A.; Agrawal, S.K.; Lalwani, A.K. Dizziness Handicap Inventory Score Is Highly Correlated With Markers of Gait Disturbance. Otol. Neurotol. Off. Publ. Am. Otol. Soc. Am. Neurotol. Soc. Eur. Acad. Otol. Neurotol. 2017, 38, 1490–1499. [Google Scholar] [CrossRef]
- Khandoker, A.H.; Taylor, S.B.; Karmakar, C.; Begg, R.K.; Palaniswami, M. Investigating scale invariant dynamics in minimum toe clearance variability of the young and elderly during treadmill walking. IEEE Trans. Neural Syst. Rehabil. Eng. 2008, 16, 380–389. [Google Scholar] [CrossRef]
- Elble, R.J.; Thomas, S.S.; Higgins, C.; Colliver, J. Stride-dependent changes in gait of older people. J. Neurol. 1991, 238, 1–5. [Google Scholar] [CrossRef]
- Ribeiro, D.M.; Buenoa, G.A.S.; Gervásio, F.M.; de Menezes, R.L. Foot-ground clearance characteristics in women: A comparison across different ages. Gait Posture 2019, 69, 121–125. [Google Scholar] [CrossRef]
- Alcock, L.; Vanicek, N.; O’Brien, T.D. Alterations in gait speed and age do not fully explain the changes in gait mechanics associated with healthy older women. Gait Posture 2013, 37, 586–592. [Google Scholar] [CrossRef]
- Cebolla, E.C.; Rodacki, A.; Bento, P.C.B. Balance, gait, functionality and strength: Comparison between elderly fallers and non-fallers. Braz. J. Phys. Ther. 2015, 19, 146–151. [Google Scholar] [CrossRef] [PubMed]
- Karmakar, C.; Khandoker, A.; Begg, R.; Palaniswami, M. Understanding ageing effects using complexity analysis of foot-ground clearance during walking. Comput. Methods Biomech. Biomed. Eng. 2013, 16, 554–564. [Google Scholar] [CrossRef] [PubMed]
- Watanabe, K. Relationship between Toe Clearance Strategy and Regional Regulation of Rectus Femoris Muscle During Swing Phase in Prolonged Walking in Young and Older Adults. Front. Physiol. 2018, 9, 1274. [Google Scholar] [CrossRef] [PubMed]
- De Asha, A.; Buckley, J.G. The effects of walking speed on minimum toe clearance and on the temporal relationship between minimum clearance and peak swing-foot velocity in unilateral trans-tibial amputees. Prosthet. Orthot. Int. 2015, 39, 120–125. [Google Scholar] [CrossRef] [PubMed]
- Rand, T.J.; Wurdeman, S.R.; Johanning, J.M.; Pipinos, I.I.; Myers, S.A. Increased minimum toe clearance variability in patients with peripheral arterial disease. Med. Eng. Phys. 2015, 37, 1141–1145. [Google Scholar] [CrossRef]
- Choi, J.-S.; Kang, D.-W.; Shin, Y.-H.; Tack, G.-R. Differences in gait pattern between the elderly and the young during level walking under low illumination. Acta Bioeng. Biomech. 2014, 16, 3–9. [Google Scholar] [PubMed]
- Rumble, D.D.; Hurt, C.P.; Brown, D.A. Step-by-step variability of swing phase trajectory area during steady state walking at a range of speeds. PLoS ONE 2018, 13, e0191247. [Google Scholar] [CrossRef] [PubMed]
- Miller, C.A.; Feiveson, A.H.; Bloomberg, J.J. Effects of speed and visual-target distance on toe trajectory during the swing phase of treadmill walking. J. Appl. Biomech. 2009, 25, 32–42. [Google Scholar] [CrossRef] [PubMed]
- Schulz, B.W. Minimum toe clearance adaptations to floor surface irregularity and gait speed. J. Biomech. 2011, 44, 1277–1284. [Google Scholar] [CrossRef]
- Levinger, P.; Lai, D.; Menz, H.; Morrow, A.D.; Feller, J.A.; Bartlett, J.R.; Bergman, N.R.; Begg, R. Swing limb mechanics and minimum toe clearance in people with knee osteoarthritis. Gait Posture 2012, 35, 277–281. [Google Scholar] [CrossRef]
- Little, V.L.; McGuirk, T.E.; Patten, C. Impaired limb shortening following stroke: What’s in a name? PLoS ONE 2014, 9, e110140. [Google Scholar] [CrossRef]
- Graci, V.; Elliott, D.B.; Buckley, J.G. Peripheral visual cues affect minimum-foot-clearance during overground locomotion. Gait Posture 2009, 30, 370–374. [Google Scholar] [CrossRef]
- Santhiranayagam, B.K.; Lai, D.T.H.; Sparrow, W.A.; Begg, R.K. Minimum toe clearance events in divided attention treadmill walking in older and young adults: A cross-sectional study. J. Neuro. Eng. Rehabil. 2015, 12, 58. [Google Scholar] [CrossRef]
- Sparrow, W.A.; Begg, R.K.; Parker, S. Variability in the foot-ground clearance and step timing of young and older men during single-task and dual-task treadmill walking. Gait Posture 2008, 28, 563–567. [Google Scholar] [CrossRef]
- Killeen, T.; Easthope, C.S.; Demkó, L.; Filli, L.; Lőrincz, L.; Linnebank, M.; Curt, A.; Zörner, B.; Bolliger, M. Minimum toe clearance: Probing the neural control of locomotion. Sci. Rep. 2017, 7, 1922. [Google Scholar] [CrossRef]
- Wu, X.; Madigan, M.L.; Nussbaum, M.A. Executive Function and Measures of Fall Risk Among People With Obesity. Percept. Mot. Ski. 2016, 122, 825–839. [Google Scholar] [CrossRef] [PubMed]
- Delahunt, E.; Monaghan, K.; Caulfield, B. Altered neuromuscular control and ankle joint kinematics during walking in subjects with functional instability of the ankle joint. Am. J. Sports Med. 2006, 34, 1970–1976. [Google Scholar] [CrossRef] [PubMed]
- Sharpe, T.; Malone, A.; French, H.; Kiernan, D.; O’Brien, T. Effect of flip-flops on lower limb kinematics during walking: A cross-sectional study using three-dimensional gait analysis. Ir. J. Med. Sci. 2016, 185, 493–501. [Google Scholar] [CrossRef] [PubMed]
- Rosenblatt, N.J.; Bauer, A.; Grabiner, M.D. Relating minimum toe clearance to prospective, self-reported, trip-related stumbles in the community. Prosthet. Orthot. Int. 2017, 41, 387–392. [Google Scholar] [CrossRef]
- Chow, J.W.; Yablon, S.A.; Horn, T.S.; Stokic, D.S. Temporospatial characteristics of gait in patients with lower limb muscle hypertonia after traumatic brain injury. Brain Inj. 2010, 24, 1575–1584. [Google Scholar] [CrossRef]
- Nagano, H.; James, L.; Sparrow, W.A.; Begg, R.K. Effects of walking-induced fatigue on gait function and tripping risks in older adults. J. Neuroeng. Rehabil. 2014, 11, 155. [Google Scholar] [CrossRef]
- Bunterngchit, Y.; Lockhart, T.; Woldstad, J.C.; Smith, J.L. Age related effects of transitional floor surfaces and obstruction of view on gait characteristics related to slips and falls. Int. J. Ind. Ergon. 2000, 25, 223–232. [Google Scholar] [CrossRef][Green Version]
- Zhang, Y.; Feng, N.; Hu, N.; Gu, Y. A pilot study on gait kinematics of old women with bound feet. Appl. Bionics Biomech. 2015, 2015, 589709. [Google Scholar] [CrossRef]
- Shi, L.; Duan, F.; Yang, Y.; Sun, Z. The Effect of Treadmill Walking on Gait and Upper Trunk through Linear and Nonlinear Analysis Methods. Sensors 2019, 19, 2204. [Google Scholar] [CrossRef]
- Hamacher, D.; Hamacher, D.; Krowicki, M.; Schega, L. Between-day test-retest reliability of gait variability in older individuals improves with a familiarization trial. Aging Clin. Exp. Res. 2017, 29, 327–329. [Google Scholar] [CrossRef] [PubMed]
- Meyer, C.; Killeen, T.; Easthope, C.S.; Curt, A.; Bolliger, M.; Linnebank, M.; Zörner, B.; Filli, L. Familiarization with treadmill walking: How much is enough? Sci. Rep. 2019, 9, 5232. [Google Scholar] [CrossRef] [PubMed]
- Telonio, A.; Blanchet, S.; Maganaris, C.; Baltzopoulos, V.; McFadyen, B. The detailed measurement of foot clearance by young adults during stair descent. J. Biomech. 2013, 46, 1400–1402. [Google Scholar] [CrossRef]









{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Parameter | Value |
|---|---|
| Mean total # of participants | 41.4 |
| Mean male to female ratio | 1.071 |
| Use of treadmill | 34.9% |
| Indoors setting | 100.0% |
| Participants wearing shoes | 79.0% |
| Equipment used | 30 motion capture, 6 IMU, 2 electromagnetic system, 5 combination of systems |
| MTC to MFC | 74.4% to 25.6% |
| Condition/IV Assessed | Control vs. Intervention | Article | MFC Mean/ Median | Impact of Condition on MFC/MTC Mean/Median | Impact of Condition on MFC Variability | MFC: Control Group (mm) | MFC: Intervention Group (mm) |
|---|---|---|---|---|---|---|---|
| Age | YA vs. OA | [14] | Mean | No sig. mean MFC diff | Sig greater in OA | 28.76 ± 7.96 | 25.56 ± 7.20 |
| [28] | Mean | No sig. mean MFC diff | Sig greater in OA | 14.6 ± 5.2 | 12.5 ± 4.7 | ||
| Median | No sig. median MFC diff | Sig greater in OA | 14.4 ± 5.2 | 12.1 ± 4.7 | |||
| [29] | Mean | No sig. mean MFC diff | Not reported | 14 ± 4 | 16 ± 7 | ||
| [23] | Median | No sig. median MFC diff | Sig greater in OA | 14.9 ± 1.6 | 13.8 ± 2.1 | ||
| [30] | Mean | Sig. lower mean MFC in OA | N/A | 50 ± 10 | 40 ± 10 | ||
| [31] | Mean | Decreases in MFC of 0.2 cm/year of age | N.R. | N.R. | N.R. | ||
| Parkinson’s disease | Healthy vs. idiopathic PD | [19] | Mean | No sig. mean MFC diff | No sig. diff | 40 ± 3 | 30 ± 3 |
| Healthy vs. vascular PD | No sig. mean MFC diff | No sig. diff | 40 ± 3 | 30 ± 2 | |||
| Healthy vs. PD (at preferred speed) | [26] | Mean | N.R. | N/A | 28.1 ± 7.1 | 29.6 ± 9 | |
| Healthy vs. PD (at fast speed) | N.R. | 30.5 ± 8.3 | 33.7 ± 10.8 | ||||
| History of Falls in OA | Non-fallers vs. fallers | [32] | Mean | Sig. lower mean MFC in Fallers | N.R. | 43 ± 1 | 40 ± 1 |
| [28] | Mean | Sig. lower mean MFC in Non-fallers | Sig. greater in fallers | 12.5 ± 4.7 | 20.2 ± 5.1 | ||
| [33] | Median | Sig. lower median MFC in Non-fallers | Sig. greater in fallers | 12.1 ± 4.7 | 20 ± 5.1 | ||
| Falls and time: MTC at 5–10 min vs. MTC at 15–20 min in OA | [34] | Mean | Sig. lower MTC with time in OA w/o history of falls, but not in those with one or in YA | Sig. greater MTC variability in OA than YA | Graph | Graph | |
| Amputation | Non-amputated limb vs. amputated limb | [18] | Mean | Sig. higher mean MTC on amputated limb | N.R. | 30.7 ± 12.5 | 34.1 ± 15.3 |
| Intact vs. prosthetic side | [35] | Mean | Sig. lower MTC on prosthetic side (no increase in MTC with increasing gait speed on prosthetic side) | N.R. | 24.6 ± 8.7 | 11.0 ± 6.6 | |
| Peripheral Arterial Disease with pain | Healthy vs. PAD pain | [36] | Mean | No sig. mean MFC diff | Sig higher MTC variability diff in PAD pain patients | 37.2 ± 3.4 | 39.3 ± 5.1 |
| Non-fallers with Multiple Sclerosis (MS) | Healthy Control vs. MS Non-fallers | [17] | Mean | N.R. | N.R. | 11.6 ± 2.9 | 11.1 ± 3.1 |
| Slippers | Barefoot vs. slippers | [25] | Mean | No sig. mean MFC diff | N.R. | 15.7 ± 4.7 | 15.7 ± 3.8 |
| Age + Illumination | OA in normal conditions vs. OA in low illumination conditions | [37] | Mean | No sig. MTC diff b/w illumination conditions in OA (sig diff for younger group) | N.R. | 17 ± 4 | 16 ± 3 |
| Gait Speed | Gait Speed in OA | [26] | Mean | Higher mean MTC with increasing speed and longer step length | N/A | 28.1 ± 7.1 | 30.5 ± 8.3 |
| [38] | Mean | Sig. higher mean MTC with increasing speed | No sig. diff in variability with increasing speed | N/A | N/A | ||
| Gait Speed in Healthy YA | [39] | Mean | Sig lower mean MTC with increasing treadmill speed (Graph) | N.R. | N/A | N/A | |
| [40] | Mean | Sig. higher mean MTC with increasing gait speed; Sig higher mean MTC from no obstacle to visible obstacle, and from visible to hidden obstacle | No sig changes in variability across obstacle conditions | N/A | N/A | ||
| PD preferred speed vs PD fast speed | [26] | Mean | Sig. higher mean MTC at faster speed | N/A | 29.6 ± 9 | 33.7 ± 10.8 |
| Condition/IV Assessed | Control vs. Intervention | Article | MFC Mean/ Median | Impact of Condition on MFC/MTC Mean/Median | Impact of Condition on MFC Variability | MFC: Control Group (mm) | MFC: Intervention Group (mm) |
|---|---|---|---|---|---|---|---|
| Peripheral Arterial Disease without pain | Healthy vs. PAD pain-free | [36] | Mean | No sig. diff | Sig higher MTC variability diff in PAD pain-free patients | 37.2 ± 3.4 | 40.9 ± 4.5 |
| Knee Osteoarthritis | Healthy vs. KO | [41] | Mean | No sig. diff | N.R. | 12.8 ± 6.7 | 32.5 ± 7 |
| Fitted footwear | Barefoot vs. fitted footwear | [25] | Mean | Sig. lower MFC in barefoot walking | N.R. | 15.7 ± 4.7 | 19.7 ± 3.8 |
| Post-stroke hemiparesis | Healthy vs. post-stoke patients | [42] | Mean | Sig. higher MTC in Post-Stroke patients | N.R. | 14.8 ± 6.9 | 32.5 ± 3.4 |
| Vision obstruction | FV (full vision) vs. CPO (circumferential-peripheral occlusion), UO (upper occlusion), LO (lower occlusion) | [43] | Median | Sig. higher MFC with CPO compared to rest | N.R. | N/A | N/A |
| Condition/IV Assessed | Control vs. Intervention | Article | MFC Mean/ Median | Impact of Condition on MFC/MTC Mean/Median | Impact of Condition on MFC Variability | MFC: Control Group (mm) | MFC: Intervention Group (mm) |
|---|---|---|---|---|---|---|---|
| Dual Task Walking (DTW) | Single Task Walking (STW) vs. DTW in OA | [44] | Mean | No sig. mean MFC diff (GRAPH) | Sig. greater variability in preferred speed single task walking group | N/A | N/A |
| [21] | Mean | No sig. mean MFC diff | No sig variability diff | 22.4 ± 8.9 | 19.99 ± 8 | ||
| [16] | Mean | No sig. mean MFC diff | No sig variability diff | 23 ± 7 | 18 ± 7 | ||
| [24] | Mean | No sig. mean MFC diff | No sig variability diff | 27 ± 7.9 | 26.5 ± 8.4 | ||
| [45] | Mean and Median | No Dual Task effects; Right foot MFC sig greater than left foot for YA and OA | Sig. higher MFC variability in OA for right-foot only | Graph | Graph | ||
| [8] | Mean | MTC changes dependent on task (↑ for carrying basket, ↓ for answering questions, and unchanged for carrying water on tray) | N.R. | Graph | Graph | ||
| [46] | Mean | Incongruent Stroop Task: Sig lower mean MFC in DTW | No sig. variability diff | 14.5 ± 0.5 | 12.7 ± 0.5 | ||
| Congruent Stroop Task: Sig. lower mean MFC in DTW | No sig. variability diff | 14.5 ± 0.5 | 12.6 ± 0.4 | ||||
| STW vs DTW in obese and comparison groups (combined data) | [47] | Mean | Sig. lower mean MTC in DT | N.R. | 14 ± 8.5 | 9.4 ± 6.2 | |
| Age + Dual Task Walking (DTW) | DTW in YA vs DTW in OA | [44] | Mean | No sig. mean MFC diff (GRAPH) | No sig variability diff | N/A | N/A |
| [46] | Mean | Incongruent Stroop Task: Sig. lower mean MFC in OA | Sig. greater variability in OA | 14.6 ± 0.5 | 12.7 ± 0.5 | ||
| Congruent Stroop Task: No sig. diff (values not given) | Sig. greater variability in OA | N/A | N/A | ||||
| Ankle instability | Functional instability (FI) (Control vs. FI Patients) | [48] | Mean | Sig. lower mean MFC in FI individuals | N.R. | 22.84 ± 4.92 | 12.62 ± 7.49 |
| [22] | Mean | No sig. mean MFC diff | N.R. | 29 ± 10 | 12.62 ± 6 | ||
| Mechanical instability (MI) (Control vs. MI Patients) | No sig. mean MFC diff | Sig. increased variability in MI group | 29 ± 10 | 12.62 ± 7 | |||
| Fallers with Multiple Sclerosis (MS) | Healthy Control vs. MS Fallers | [17] | Mean | Sig. lower MTC in MS Fallers | No sig variability diff | 11.6 ± 2.9 | 8.5 ± 3 |
| Flip-flops | Barefoot vs flip-flops | [49] | Mean | Sig. lower mean MFC in flip-flops | N.R. | 42 ± 8 | 16 ± 5.6 |
| Transtibial Amputation + Trip-related stumbles | No history of trip-related stumbles (TS) vs. trip-related stumbles (TS) | [50] | Mean | Sig. lower MTC (prosthetic side) for individuals that report TS | N.R. | 25.6 ± 5.4 | 12.3 ± 0.8 |
| Age + Illumination | YA vs. OA in low illumination conditions | [37] | Mean | Sig. lower MTC in OA | N.R. | 29 ± 6 | 16 ± 3 |
| Traumatic Brain injury (TBI) | Healthy (slow speed) vs. TBI (preferred speed) | [51] | Mean | Sig. lower mean MTC in TBI patients (regardless of walking speed) | N.R. | 122 ± 23 | 76 ± 38.5 |
| Fatigue | Non-fatigued vs. fatigued OA | [52] | Mean | Sig. lower mean MFC in fatigued OA | Sig. reduced in fatigued OA (graph) | N/A | N/A |
| Age + Treadmill/Overground | Overground vs. Treadmill | [15] | Median | Sig. lower median MFC in treadmill walking; non-dominant foot MFC greater than dominant foot on treadmill; no ageing effects | Lower variability on treadmill (nonsig.) | Graph | Graph |
| [13] | N.R. | Sig. lower MTC in treadmill walking; greater assymetry in OA; no ageing effect | N.R. | 17.5 | 12.1 | ||
| Age + Floor surface + Vision Obstruction | YA vs. OA with and without load (i.e vision obstruction) | [53] | Mean | Age × Load: Sig. lower mean MFC in OA carrying load (i.e. w/ vision obstruction) | N.R. | Graph | Graph |
| OA w/o load vs w/load while transitioning from carpet to vinyl | Age × Load × Floor: Sig lower mean MFC in OA when carrying load and transitioning (i.e. w/vision obstruction) | N.R. | Graph | Graph |
| Condition/IV Assessed | Control vs. Intervention | Article | MFC Mean/ Median | Impact of Condition on MFC/MTC Mean/Median | Impact of Condition on MFC Variability | MFC: Control Group (mm) | MFC: Intervention Group (mm) |
|---|---|---|---|---|---|---|---|
| Chronic back pain | Healthy vs chronic lower back pain (no vision obstruction) | [20] | N/A | MTC data not provided (Assessed variability) | No sig difference in coefficient of variation | N/A | N/A |
| Healthy vs chronic lower back pain (LBP) (impairment goggles) | Sig higher CV of MFC for chronic LBP patients | N/A | N/A | ||||
| Chronic LBP patients with vs without visual obstruction (i.e. impairment goggles) | Sig higher CV of MFC for chronic LBP patients with visual obstruction | N/A | N/A | ||||
| Bound feet | Control vs patients with bound feet | [54] | Mean | Continuous increase in MTC; MHC increased at 20% of swing phase then decreased | N.R. | N/A | N/A |
| Dizziness | Mean Foot clearance of cohort with a range of DHI-S scores | [27] | Mean | MTC data not provided | N.R. | N/A | 32.5 |
| Effect on MFC | Conditions |
|---|---|
| Decrease | Dual-task walking, age and dual-task walking, ankle instability, fallers with multiple sclerosis, flip-flops, transtibial amputation + trip-related stumbles (variability ↓), age and illumination, traumatic brain injury, fatigue (variability ↓ in fatigued older adults), age and treadmill/over ground, age and floor surface and vision obstruction. |
| No effect | Age (variability ↑), Parkinson’s disease, history of falls in older adults, amputation, peripheral arterial disease with pain (variability ↑), non-fallers with multiple sclerosis, slippers, age and illumination, gait speed |
| Increase | Peripheral arterial disease without pain, knee osteoarthritis, fitted footwear, post-stroke hemiparesis, vision obstruction |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Al Bochi, A.; Delfi, G.; Dutta, T. A Scoping Review on Minimum Foot Clearance: An Exploration of Level-Ground Clearance in Individuals with Abnormal Gait. Int. J. Environ. Res. Public Health 2021, 18, 10289. https://doi.org/10.3390/ijerph181910289
Al Bochi A, Delfi G, Dutta T. A Scoping Review on Minimum Foot Clearance: An Exploration of Level-Ground Clearance in Individuals with Abnormal Gait. International Journal of Environmental Research and Public Health. 2021; 18(19):10289. https://doi.org/10.3390/ijerph181910289
Chicago/Turabian StyleAl Bochi, Abdulrahman, Ghazaleh Delfi, and Tilak Dutta. 2021. "A Scoping Review on Minimum Foot Clearance: An Exploration of Level-Ground Clearance in Individuals with Abnormal Gait" International Journal of Environmental Research and Public Health 18, no. 19: 10289. https://doi.org/10.3390/ijerph181910289
APA StyleAl Bochi, A., Delfi, G., & Dutta, T. (2021). A Scoping Review on Minimum Foot Clearance: An Exploration of Level-Ground Clearance in Individuals with Abnormal Gait. International Journal of Environmental Research and Public Health, 18(19), 10289. https://doi.org/10.3390/ijerph181910289