
Estimation of the Impact of Foodborne Salmonellosis on Consumer Well-Being in Hungary


Abstract
:1. Introduction
2. Materials and Methods
2.1. Data Collection and Sociodemographic Characteristics of the Samples
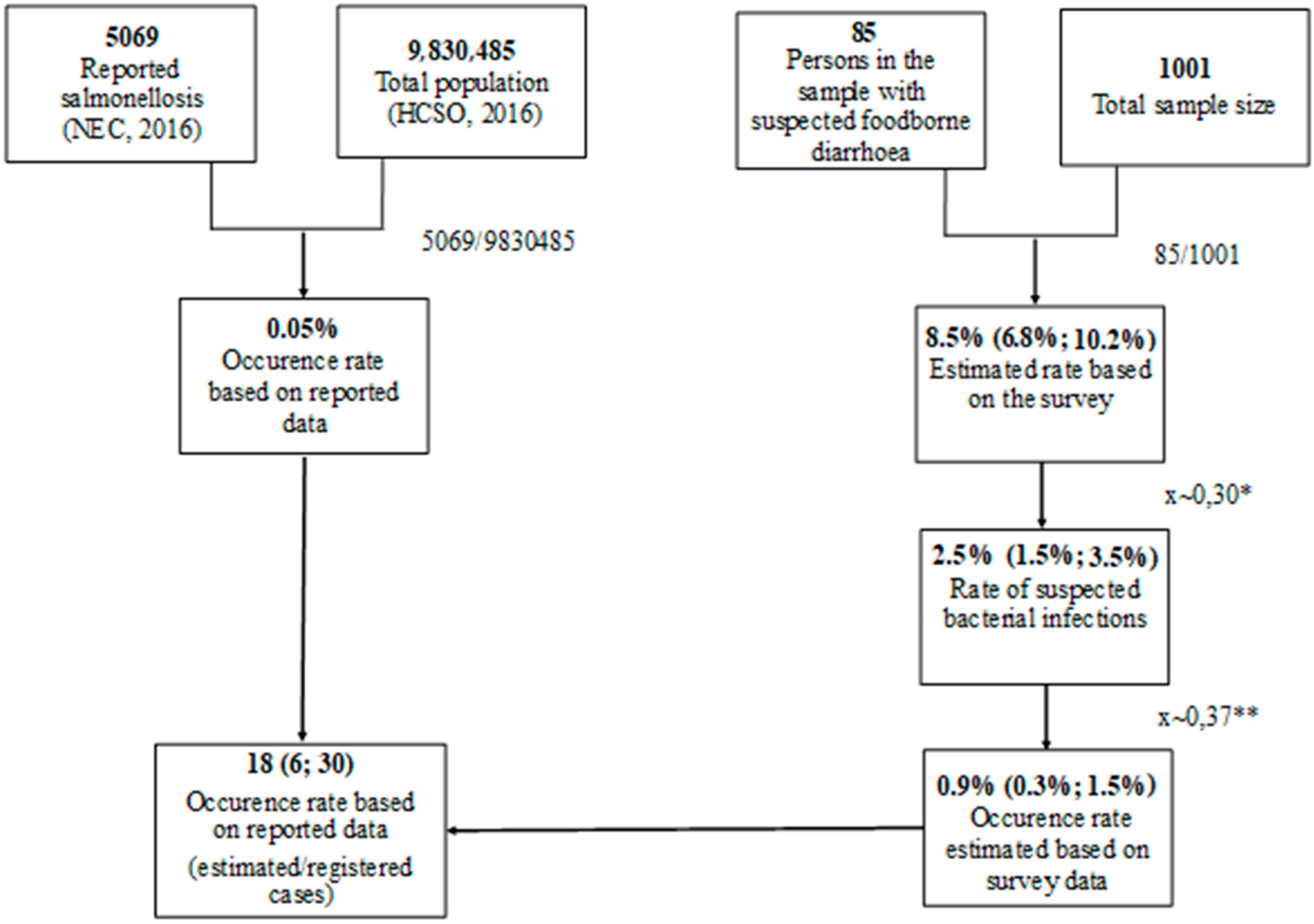
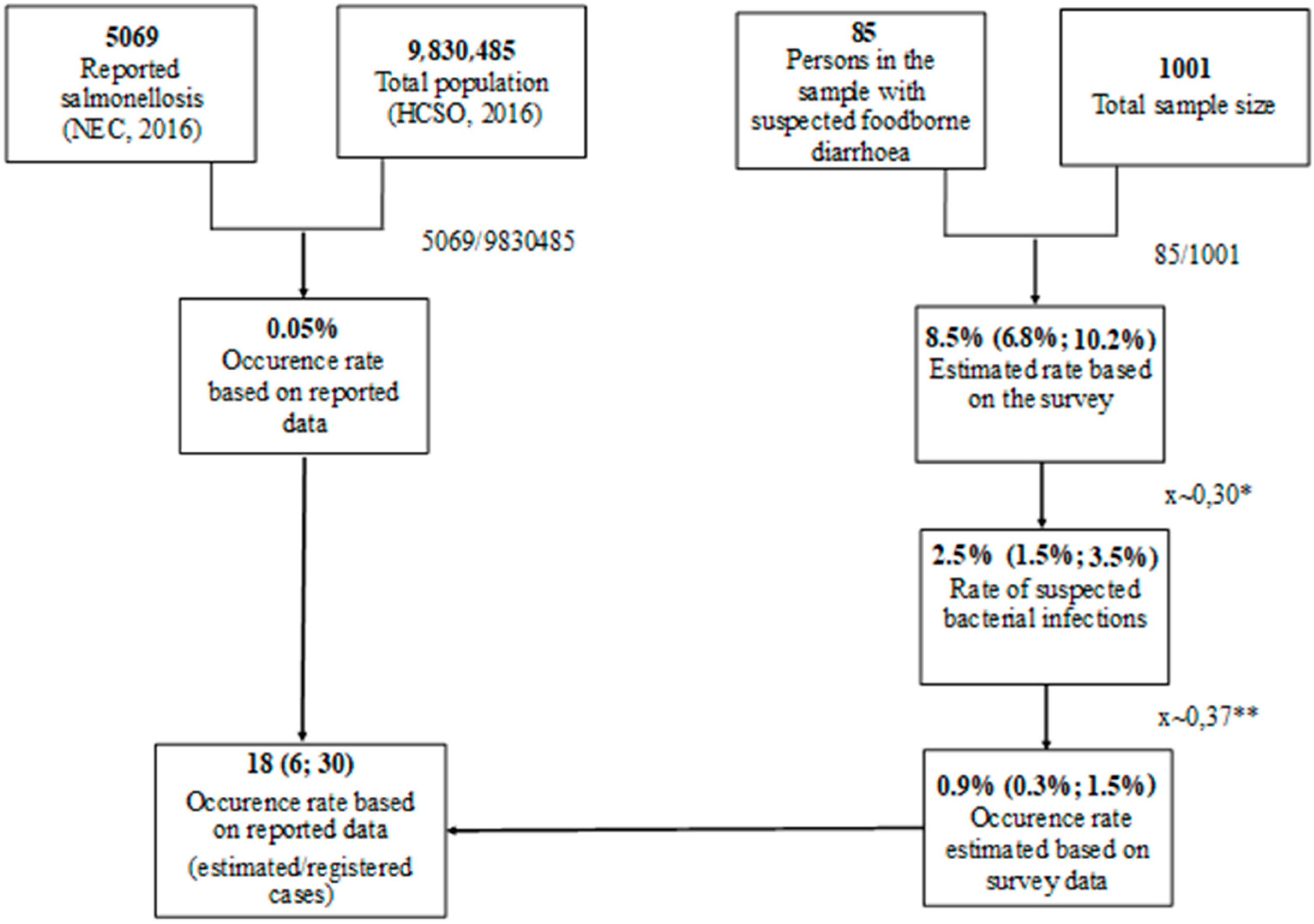
2.2. Multiplier Calculation
2.3. Estimation of Willingness to Pay
3. Results
3.1. Estimated Number of Foodborne Salmonellosis Cases
3.2. Hungarian Consumer WTP for Avoiding Foodborne Salmonellosis
3.3. Relationship between Demographic Parameters and WTP
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- European Food Safety Authority and European Centre for Disease Prevention and Control (EFSA and ECDC) (2018). The European Union One Health Zoonoses Report 2018. Available online: https://www.ecdc.europa.eu/sites/default/files/documents/zoonoses-EU-one-health-2018-report.pdf (accessed on 27 May 2021).
- Giannella, R.A. Salmonella. In Medical Microbiology, 4th ed.; Baron, S., Ed.; University of Texas Medical: Galveston, TX, USA, 1996; Chapter 21. [Google Scholar]
- Silva, C.; Calva, E.; Maloy, S. One Health and Food-Borne Disease: Salmonella Transmission between Humans, Animals, and Plants. In One Health, 1st ed.; Atlas, R.M., Maloy, S., Eds.; ASM Press: Washington, DC, USA, 2014; Chapter 9. [Google Scholar]
- Bauerfeind, R.; Von Graevenitz, A.; Kimmig, P.; Schiefer, H.G.; Schwarz, T.; Slenczka, W.; Zahner, H. Zoonoses: Infectious Diseases Transmissible from Animals and Humans, 4th ed.; ASM Press: Washington, DC, USA, 2016; pp. 257–261. [Google Scholar]
- Haapala, I.; Probart, C. Food Safety Knowledge, Perceptions, and Behaviors among Middle School Students. J. Nutr. Educ. Behav. 2004, 36, 71–76. [Google Scholar] [CrossRef]
- Byrd-Bredbenner, C.; Abbot, J.M.; Quick, V. Food Safety Knowledge and Beliefs of Middle School Children: Implications for Food Safety Educators. J. Food Sci. Educ. 2010, 9, 19–30. [Google Scholar] [CrossRef]
- Kiss, A.; Popp, J.; Oláh, J.; Lakner, Z. The Reform of School Catering in Hungary: Anatomy of a Health-Education Attempt. Nutrients 2019, 11, 716. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Santos-Ferreira, N.; Alves, Â.; Cardoso, M.J.; Langsrud, S.; Malheiro, A.R.; Fernandes, R.; Maia, R.; Truninger, M.; Junqueira, L.; Nicolau, A.I.; et al. Cross-contamination of lettuce with Campylobacter spp. via cooking salt during handling raw poultry. PLoS ONE 2021, 16, e0250980. [Google Scholar] [CrossRef] [PubMed]
- Syeda, R.; Lundgren, P.T.; Kasza, G.; Truninger, M.; Brown, C.; Lacroix-Hugues, V.; Izsó, T.; Teixeira, P.; Eley, C.; Ferré, N.; et al. Young People’s Views on Food Hygiene and Food Safety: A Multicentre Qualitative Study. Educ. Sci. 2021, 11, 261. [Google Scholar] [CrossRef]
- Møretrø, T.; Nguyen-The, C.; Didier, P.; Maître, I.; Izsó, T.; Kasza, G.; Skuland, S.E.; Cardoso, M.J.; Ferreira, V.B.; Teixeira, P.; et al. Consumer practices and prevalence of Campylobacter, Salmonella and norovirus in kitchens from six European countries. Int. J. Food Microbiol. 2021, 347, 109172. [Google Scholar] [CrossRef]
- Hungarian Central Statistical Office (HCSO). Number of major communicable diseases reported (2001–). 2020. Available online: https://www.ksh.hu/docs/hun/xstadat/xstadat_eves/i_feb001.html (accessed on 21 May 2021).
- de Knegt, L.V.; Pires, S.M.; Hald, T. Attributing foodborne salmonellosis in humans to animal reservoirs in the European Union using a multi-country stochastic model. Epidemiol. Infect. 2014, 143, 1175–1186. [Google Scholar] [CrossRef] [Green Version]
- Sockett, P. The economic implications of human salmonella infection. J. Appl. Bacteriol. 1991, 71, 289–295. [Google Scholar] [CrossRef]
- Vajda, Á.; Mohácsi-Farkas, C.; Ózsvári, L.; Kasza, G. Consumers’s willingness to pay for avoiding Salmonella infection. Acta Aliment. 2020, 49, 76–85. [Google Scholar] [CrossRef] [Green Version]
- Wertenbroch, K.; Skiera, B. Measuring Consumers’ Willingness to Pay at the Point of Purchase. J. Mark. Res. 2002, 39, 228–241. [Google Scholar] [CrossRef]
- Grunert, K.G.; Juhl, H.J.; Esbjerg, L.; Jensen, B.B.; Bech-Larsen, T.; Brunsø, K.; Madsen, C.Ø. Comparing methods for measuring consumer willingness to pay for a basic and an improved ready made soup product. Food Qual. Prefer. 2009, 20, 607–619. [Google Scholar] [CrossRef]
- Himmler, S.; Van Exel, J.; Perry-Duxbury, M.; Brouwer, W. Willingness to pay for an early warning system for infectious diseases. Eur. J. Health Econ. 2020, 21, 763–773. [Google Scholar] [CrossRef] [Green Version]
- Stroup, D.F.; Teutsch, S.M. Statistics in Public Health: Quantitative Approaches to Public Health Problems, 1st ed.; Oxford University Press: New York, NY, USA, 1998; pp. 39–56. [Google Scholar]
- 4a—Concepts of Health, Wellbeing and Illness, and the Aetiology of Illness. Available online: https://www.healthknowledge.org.uk/public-health-textbook/medical-sociology-policy-economics/4a-concepts-health-illness/section2/activity3 (accessed on 23 September 2021).
- Dolan, P.; Metcalfe, R. Measuring Subjective Wellbeing: Recommendations on Measures for use by National Governments. J. Soc. Policy 2012, 41, 409–427. [Google Scholar] [CrossRef] [Green Version]
- Hungarian Central Statistical Office (HCSO). Hungarian Census Data 2016. Available online: https://www.ksh.hu/mikrocenzus2016/kotet_3_demografiai_adatok (accessed on 27 May 2021).
- Wilcock, A.; Pun, M.; Khanona, J.; Aung, M. Consumer attitudes, knowledge and behaviour: A review of food safety issues. Trends Food Sci. Technol. 2004, 15, 56–66. [Google Scholar] [CrossRef]
- McCluskey, J.J.; Grimsrud, K.M.; Ouchi, H.; Wahl, T.I. Bovine spongiform encephalopathy in Japan: Consumers’ food safety perceptions and willingness to pay for tested beef. Aust. J. Agric. Resour. Econ. 2005, 49, 197–209. [Google Scholar] [CrossRef] [Green Version]
- Lobb, A.; Mazzocchi, M.; Traill, W. Modelling risk perception and trust in food safety information within the theory of planned behaviour. Food Qual. Prefer. 2007, 18, 384–395. [Google Scholar] [CrossRef]
- Cumming, R. Is probability sampling always better? A comparison of results from a quota and a probability sample survey. Community Health Stud. 2010, 14, 132–137. [Google Scholar] [CrossRef]
- Acharya, A.S.; Prakash, A.; Saxena, P.; Nigam, A. Sampling: Why and how of it? Indian J. Med Spéc. 2013, 4, 330–333. [Google Scholar] [CrossRef]
- Yang, K.; Banamah, A. Quota Sampling as an Alternative to Probability Sampling? An Experimental Study. Sociol. Res. Online 2014, 19, 56–66. [Google Scholar] [CrossRef] [Green Version]
- Hungarian National Bank (HNB). Exchange Rate—2019 Overview. Available online: http://www.mnbkozeparfolyam.hu/arfolyam-2019.html (accessed on 27 May 2021).
- Keusch, G.T.; Fontaine, O.; Bhargava, A.; Boschi-Pinto, C.; Bhutta, Z.A.; Gotuzzo, E.; Rivera, J.; Chow, J.; Shahid-Salles, S.; Laxminarayan, R. Diarrheal Diseases. In Disease Control Priorities in Developing Countries, 2nd ed.; Jamison, D.T., Breman, J.G., Measham, A.R., Alleyene, G., Claeson, M., Evans, D.B., Jha, P., Mills, A., Musgrove, P., Eds.; Oxford University Press: New York, NY, USA, 2006; pp. 371–387. [Google Scholar]
- Ogoina, D. Fever, fever patterns and diseases called ‘fever’—A review. J. Infect. Public Health 2011, 4, 108–124. [Google Scholar] [CrossRef] [Green Version]
- World Health Organization (WHO). The Burden of Foodborne Diseases in the WHO European Region. Available online: https://www.euro.who.int/__data/assets/pdf_file/0005/402989/50607-WHO-Food-Safety-publicationV4_Web.pdf (accessed on 27 May 2021).
- McDonald, J.H. Kruskal–Wallis test. In Handbook of Biological Statistics, 2nd ed.; McDonald, J.H., Ed.; Sparky House Publishing: Baltimore, MD, USA, 2009; pp. 165–172. [Google Scholar]
- National Epidemiological Center (NEC). Reported Infectious Diseases in Hungary, 2012–2016. Available online: http://www.oek.hu/oek.web?to=2475,2465&nid=509&pid=1&lang=hun (accessed on 27 May 2021).
- Bresee, J.S.; Widdowson, M.-A.; Monroe, S.S.; Glass, R.I.; Acheson, D. Foodborne Viral Gastroenteritis: Challenges and Opportunities. Clin. Infect. Dis. 2002, 35, 748–753. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fonseca, J.M.; Ravishankar, S. Safer Salads. Am. Sci. 2007, 95, 494. [Google Scholar] [CrossRef]
- National Public Health Center (NPHC). Reported Infectious Diseases in Hungary, 2015–2019. National Public Health Center. Available online: https://www.antsz.hu/data/cms96760/OSAP_Fertozo_2019_honlapra.pdf (accessed on 27 May 2021).
- Országh, E.; Pitter, J.G.; Kaló, Z.; Vokó, Z.; Józwiak, Á. Retrospective cost-utility analysis of the Non-typhoidal Salmonella control programme in Hungary. Food Control. 2021, 120, 107529. [Google Scholar] [CrossRef]
- Havelaar, A.H.; Ivarsson, S.; Löfdahl, M.; Nauta, M.J. Estimating the true incidence of campylobacteriosis and salmonellosis in the European Union, 2009. Epidemiol. Infect. 2012, 141, 293–302. [Google Scholar] [CrossRef]
- De Jong, B.; Ekdahl, K. The comparative burden of salmonellosis in the European Union member states, associated and candidate countries. BMC Public Health 2006, 6, 4. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- European Food Safety Authority; European Centre for Disease Prevention and Control. Trends and Sources of Zoonoses and Zoonotic agents in the European Union in 2009. EFSA J. 2011, 9, 2090. [Google Scholar]
- Gortva-Vajda, Á. The Social Cost of Foodborne Salmonellosis in Hungary. Master’s Thesis, Szent Istvan University, Budapest, Hungary, 2021. Available online: https://uni-mate.hu/sites/default/files/gortva-vajda_agnes-thesis.pdf (accessed on 15 September 2021).

{kind=link}
| Public Sector Costs | |
|---|---|
| Costs of Health Care | Costs of Investigation and Testing |
| –Physician visits | –Disease surveillance cost |
| –Laboratory cost | –Research |
| –Hospitalisation, medications | –Outbreak cost |
| –Ambulance or travel cost | –Other considerations |
| Costs of Households and Society | |
| –Direct cost of illness to households (e.g., caretaker for ill person) | |
| –Pain and other psychological suffering, risk aversion | |
| –Cost attributable to loss of productive activity | |
| –Cost attributable to pain, suffering and death | |
| –Cost to industry (e.g., extra cleaning/cooking time cost; extra cost of refrigerator, freezer, etc.) | |
| –Increased food cost (willingness to pay for more expensive but safer food), etc. | |
| Sociodemographic Categories | Sample 2017 (n = 1001) | Sample 2019 (n = 1001) | Population * | |
|---|---|---|---|---|
| Sex | Female | 52.55 | 53.45 | 53.07 |
| Male | 47.45 | 46.55 | 46.93 | |
| Age group | 18–29 | 16.68 | 17.88 | 17.59 |
| 30–39 | 19.78 | 16.88 | 17.04 | |
| 40–59 | 34.07 | 33.57 | 33.83 | |
| >60 | 29.46 | 31.67 | 31.54 | |
| Geographical distribution (NUTS-2) | Central Hungary | 30.07 | 31.17 | 30.75 |
| Central Transdanubia | 11.49 | 11.09 | 10.80 | |
| Western Transdanubia | 10.59 | 10.39 | 10.03 | |
| Southern Transdanubia | 8.69 | 8.29 | 9.13 | |
| Northern Hungary | 11.99 | 11.79 | 11.62 | |
| Northern Great Plain | 14.88 | 14.58 | 14.90 | |
| Southern Great Plain | 12.29 | 12.69 | 12.78 | |
| Sociodemographic Categories | WTP Sample (n = 456) | |
|---|---|---|
| Sex | Female | 53.8 |
| Male | 46.2 | |
| Age group | 18–44 | 57.5 |
| 45–64 | 27.9 | |
| >65 | 14.9 | |
| Geographical distribution (NUTS-2) | Central Hungary | 31.2 |
| Central Transdanubia | 10.4 | |
| Western Transdanubia | 11.9 | |
| Southern Transdanubia | 9.7 | |
| Northern Hungary | 10.0 | |
| Northern Great Plain | 12.6 | |
| Southern Great Plain | 14.2 | |
| Type of residence | Capital (Budapest) | 22.8 |
| City | 64.0 | |
| Village | 13.2 | |
| Number of persons in the household | 1 person | 13.2 |
| 2 persons | 32.4 | |
| 3 persons | 21.5 | |
| 4 persons | 21.5 | |
| >4 persons | 11.4 | |
| Children under the age of 15 in the household | Yes | 23.4 |
| No | 76.6 | |
| Responsible for food shopping | Respondent themselves | 35.6 |
| Together with a family member | 53.0 | |
| Other person | 11.4 | |
| Level of income | Low | 0.7 |
| Below average | 12.1 | |
| Average | 61.2 | |
| Above average | 24.3 | |
| High | 1.8 | |
| Economic status | Employeed | 55.4 |
| Self-employed | 7.0 | |
| Pensioner, disability pensoner | 17.5 | |
| Job seeker | 0.7 | |
| Homemaker | 1.3 | |
| Student | 18.2 | |
| Level of education | Primary school | 2.2 |
| Vocational school | 5.1 | |
| Secondary school | 33.5 | |
| University, college | 59.2 | |
| Scientific studies/background | Yes | 26.0 |
| No | 74.0 | |
| Occupation related to food production | Yes | 12.8 |
| No | 87.2 | |
| Special diet | Yes | 19.8 |
| No | 80.2 | |
| WTP Answers, HUF (EUR) | Number of Respondents | Percentage (%) |
|---|---|---|
| 250,001–500,000 (768.4–1536.6) | 7 | 1.5 |
| 200,001–250,000 (614.7–768.3) | 1 | 0.2 |
| 150,001–200,000 (461.1–614.6) | 1 | 0.2 |
| 50,001–150,000 (153.8–461.0) | 46 | 10.1 |
| 20,001–50,000 (6.9–153.7) | 59 | 12.9 |
| 10,001–20,000 (30.8–61.8) | 58 | 12.7 |
| 1-10,000 (<30.7) | 225 | 49.3 |
| 0 | 59 | 12.9 |
| 456 | 100.0 |
| Sociodemographic Categories | WTP Mean Values (HUF) | p | df | H | |
|---|---|---|---|---|---|
| Sex | Female | 23,789 | 0.26 | 1 | 1.28 |
| Male | 32,208 | ||||
| Age group | 18–44 | 32,279 | <0.0001 | 3 | 15.73 |
| 45–64 | 26,545 | ||||
| >65 | 18,557 | ||||
| Geographical distribution (NUTS-2) | Central Hungary | 41,092 | 0.01 | 6 | 16.27 |
| Central Transdanubia | 23,183 | ||||
| Western Transdanubia | 19,810 | ||||
| Southern Transdanubia | 24,789 | ||||
| Northern Hungary | 10,456 | ||||
| Northern Great Plain | 32,568 | ||||
| Southern Great Plain | 22,305 | ||||
| Type of residence | Capital (Budapest) | 15,321 | 0.21 | 2 | 3.17 |
| City | 26,663 | ||||
| Village | 39,462 | ||||
| Number of persons in the household | 1 person | 20,941 | 0.08 | 7 | 12.79 |
| 2 persons | 31,034 | ||||
| 3 persons | 26,648 | ||||
| 4 persons | 32,112 | ||||
| >4 persons | 25,504 | ||||
| Children under the age of 15 in the household | Yes | 36,987 | 0.01 | 1 | 6.51 |
| No | 25,502 | ||||
| Responsible for food shopping | Respondent themselves | 21,962 | 0.38 | 2 | 1.95 |
| Together with a family member | 33,058 | ||||
| Other person | 26,760 | ||||
| Level of income | Low | 1,667 | <0.0001 | 4 | 39.04 |
| Below average | 11,822 | ||||
| Average | 24,755 | ||||
| Above average | 36,599 | ||||
| High | 96,250 | ||||
| Economic status | Employeed | 33,436 | <0.0001 | 5 | 18.51 |
| Self-employed | 36,623 | ||||
| Pensioner, disability pensoner | 18,591 | ||||
| Job seeker | 41,667 | ||||
| Homemaker | 22,083 | ||||
| Student | 20,665 | ||||
| Level of education | Primary school | 5160 | 0.05 | 3 | 8.04 |
| Vocational school | 22,596 | ||||
| Secondary school | 24,147 | ||||
| University, college | 28,393 | ||||
| Scientific studies/background | Yes | 37,175 | 0.07 | 1 | 3.32 |
| No | 30,667 | ||||
| Occupation related to food production | Yes | 20,556 | 0.75 | 1 | 0.10 |
| No | 29,778 | ||||
| Special diet | Yes | 26,880 | 0.15 | 1 | 2.06 |
| No | 28,906 | ||||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Vajda, Á.; Ózsvári, L.; Szakos, D.; Kasza, G. Estimation of the Impact of Foodborne Salmonellosis on Consumer Well-Being in Hungary. Int. J. Environ. Res. Public Health 2021, 18, 10131. https://doi.org/10.3390/ijerph181910131
Vajda Á, Ózsvári L, Szakos D, Kasza G. Estimation of the Impact of Foodborne Salmonellosis on Consumer Well-Being in Hungary. International Journal of Environmental Research and Public Health. 2021; 18(19):10131. https://doi.org/10.3390/ijerph181910131
Chicago/Turabian StyleVajda, Ágnes, László Ózsvári, Dávid Szakos, and Gyula Kasza. 2021. "Estimation of the Impact of Foodborne Salmonellosis on Consumer Well-Being in Hungary" International Journal of Environmental Research and Public Health 18, no. 19: 10131. https://doi.org/10.3390/ijerph181910131
APA StyleVajda, Á., Ózsvári, L., Szakos, D., & Kasza, G. (2021). Estimation of the Impact of Foodborne Salmonellosis on Consumer Well-Being in Hungary. International Journal of Environmental Research and Public Health, 18(19), 10131. https://doi.org/10.3390/ijerph181910131