
Is the Efficiency Score an Indicator for Incident Hypertension in the Community Population of Western China?


Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design and Population
2.2. Definitions
2.3. DEA Analysis
2.4. Statistical Analysis
3. Results
3.1. Baseline Characteristics
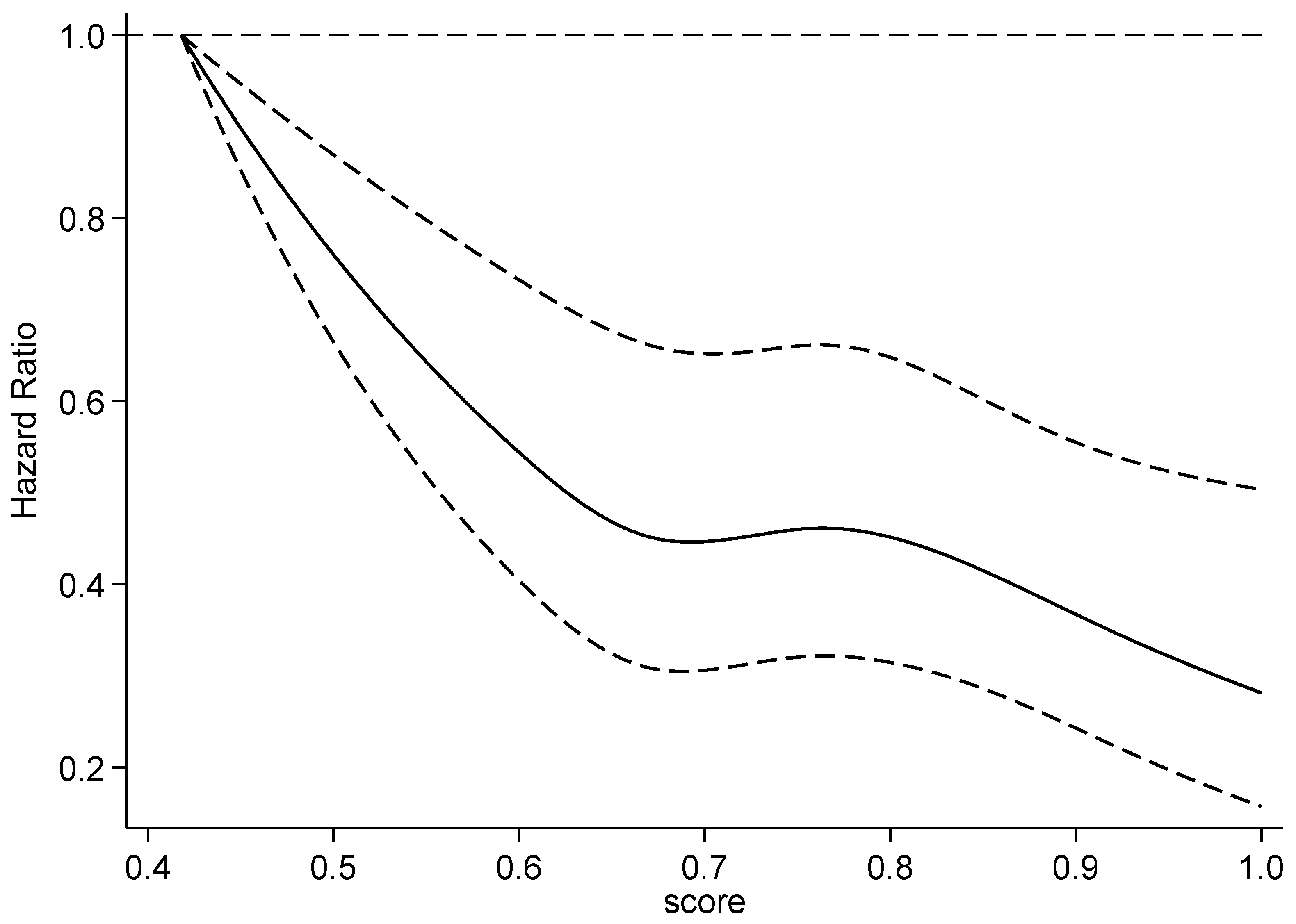
3.2. The Association between the Efficiency Score and Risk of Incident Hypertension
3.3. Quantile Regression between Efficiency Score and Systolic and Diastolic Blood Pressure in Follow-Up
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Lim, S.S.; Vos, T.; Flaxman, A.D.; Danaei, G.; Shibuya, K.; Adair-Rohani, H.; AlMazroa, M.A.; Amann, M.; Anderson, H.R.; Andrews, K.G.; et al. A comparative risk assessment of burden of disease and injury attributable to 67 risk factors and risk factor clus ters in 21 regions, 1990–2010: A systematic analysis for the Global Burden of Disease Study 2010. Lancet 2012, 380, 2224–2260. [Google Scholar] [CrossRef] [Green Version]
- GBD 2016 Risk Factors Collaborators. Global, regional, and national comparative risk assessment of 84 behavioural, environmental and occu pational, and metabolic risks or clusters of risks, 1990–2016: A systematic analysis for the Global Burden of Disease Study 2016. Lancet 2017, 390, 1345–1422. [Google Scholar] [CrossRef] [Green Version]
- Chronic and Non-communicable Disease Prevention and Control Center; Chinese Center for Disease Control and Prevention. Monitoring Report on Chronic Diseases and Risk Factors in China (2013); Military Medical Press: Beijing, China, 2016.
- Liu, G.Q.; Rao, W.B.; Liu, Z.J.; Li, M.; Chu, Y.L. Prevalence and distribution of hypertension in population aged 15 years and over in Guizhou province. Zhonghua Liu Xing Bing Xue Za Zhi 2018, 39, 614–618. [Google Scholar] [PubMed]
- Egan, B.M.; Stevens-Fabry, S. Prehypertension-Prevalence, healthrisks, and management strategies. Nat. Rev. Cardiol. 2015, 12, 289–300. [Google Scholar] [CrossRef] [PubMed]
- Li, G.; Hu, R.; Zhang, X. The impact of the 2020 International Society of Hypertension global hypertension practice guidelines on the prevention and control of hypertension in China. Hypertens. Res. 2021, 44, 1040–1041. [Google Scholar] [CrossRef] [PubMed]
- Frohlich, K.L.; Potvin, L. Transcending the known in public health practice: The inequality paradox: The population approach and vulnerable populations. Am. J. Public Health 2008, 98, 216–221. [Google Scholar] [CrossRef] [PubMed]
- Nakamura, S.; Narimatsu, H.; Nakata, Y.; Sakaguchi, M.; Konta, T.; Watanabe, M.; Ueno, Y.; Ishizawa, K.; Yamashita, H.; Kayama, T.; et al. Efficiency score from data envelopment analysis can predict the future onset of hypertension and dyslipidemia: A cohort study. Sci. Rep. 2019, 9, 16309. [Google Scholar] [CrossRef] [PubMed]
- Mancia, G.; Fagard, R.; Narkiewicz, K.; Redon, J.; Zanchetti, A.; Böhm, M.; Christiaens, T.; Cifkova, R.; de Backer, G.; Dominiczak, A.; et al. 2013 ESH/ESC guidelines for the management of arterial hypertension: The task force for the management of arterial hypertension of the European society of hypertension (ESH) and of the European society of cardiology (ESC). Eur. Heart J. 2013, 34, 2159–2219. [Google Scholar] [PubMed] [Green Version]
- Huang, Y.; Gao, L.; Xie, X.; Tan, S.C. Epidemiology of dyslipidemia in Chinese adults: Meta-analysis of prevalence, awareness, treatment, and control. Popul. Health Metr. 2014, 12, 28. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rehm, J. How should prevalence of alcohol use disorders be assessed globally? Int. J. Methods Psychiatr. Res. 2016, 25, 79–85. [Google Scholar] [CrossRef] [PubMed]
- Mendes, M.A.; da Silva, I.; Ramires, V.; Reichert, F.; Martins, R.; Ferreira, R.; Tomasi, E. Metabolic equivalent of task (METs) thresholds as an indicator of physical activity intensity. PLoS ONE 2018, 7, e0200701. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- The IPAQ Group Guidelines for Data Processing and Analysis of the International Physical Activity Questionnaire. 2015. Available online: http://www.ipaq.ki.se (accessed on 22 September 2021).
- Feng, Y.; Yu, X.; Chiu, Y.; Lin, T. Energy Efficiency and Health Efficiency of Old and New EU Member States. Front. Public Health 2020, 8, 168. [Google Scholar] [CrossRef] [PubMed]
- Bouland, D.L.; Fink, E.; Dehaan, C.; Fontanesi, J. Data envelopment analysis: Dynamic possibilities in an academic medical center application. J. Med. Pract. Manag. 2012, 28, 109–115. [Google Scholar]
- Zheng, W.; Sun, H.; Zhang, P.; Zhou, G.; Jin, Q.; Lu, X. A four-stage DEA-based efficiency evaluation of public hospitals in China after the implementation of new medical reforms. PLoS ONE 2018, 10, e0203780. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Adler, N.; Friedmanb, L.; Sinuany-Sternbc, Z. Review of ranking methods in the data envelopment analysis context. Eur. J. Oper. Res. 2002, 140, 249–265. [Google Scholar] [CrossRef]
- Narimatsu, H.; Nakata, Y.; Nakamura, S.; Sato, H.; Sho, R.; Otani, K.; Kawasaki, R.; Kubota, I.; Ueno, Y.; Kato, T.; et al. Applying data envelopment analysis to preventive medicine: A novel method for constructing a personalized risk model of obesity. PLoS ONE 2015, 10, e0126443. [Google Scholar] [CrossRef] [PubMed]
- Wang, B.Y.; Liu, Y.; Sun, X.Z.; Yin, Z.; Li, H.H.; Ren, Y.C.; Zhao, Y.; Zhang, R.Y.; Zhang, M.; Hu, D.S. Prediction model and assessment of probability of incident hypertension: The Rural Chinese Cohort Study. J. Human Hypertens. 2021, 35, 74–84. [Google Scholar] [CrossRef] [PubMed]
- Kanegae, H.; Suzuki, K.; Fukatani, K.; Ito, T.; Harada, N.; Kario, K. Highly precise risk prediction model for new-onset hypertension using artificial intelligence techniques. J. Clin. Hypertens. (Greenwich Conn.) 2020, 22, 445–450. [Google Scholar] [CrossRef] [PubMed] [Green Version]

{kind=link}
| Characteristics | Total (n = 2412) | Hypertension (n = 857) | Non-Hypertension (n = 1555) | t/Χ2 Value | p Value |
|---|---|---|---|---|---|
| Gender | 11.070 | 0.001 | |||
| Male | 1056 (43.8) | 414 (48.3) | 642 (41.3) | ||
| Female | 1356 (56.2) | 443 (51.7) | 913 (58.7) | ||
| Age | 51.83 ± 9.15 | 52.38 ± 9.46 | 51.52 ± 8.96 | 2.193 | 0.028 |
| Smoking | 4.012 | 0.045 | |||
| Yes | 614 (26.8) | 234 (29.3) | 380 (25.4) | ||
| No | 1681 (73.2) | 565 (70.7) | 1116 (74.6) | ||
| Alcohol use | 4.127 | 0.127 | |||
| Yes, abuse | 63 (2.6) | 30 (10.1) | 33 (6.3) | ||
| Yes, non-abuse | 756 (31.3) | 266 (89.9) | 490 (93.7) | ||
| No | 1593 (66.0) | 561 (65.5) | 1032 (66.4) | ||
| METs | 7655.02 ± 157.49 | 7452.45 ± 256.73 | 7766.68 ± 199.15 | 0.955 | 0.340 |
| Salt intake (g/d) | 11.98 ± 0.16 | 11.35 ± 0.21 | 12.32 ± 0.21 | 2.986 | 0.003 |
| Grain and cereal intake (g/d) | 428.45 ± 4.58 | 430.47 ± 9.08 | 427.33 ± 5.03 | 0.328 | 0.743 |
| Meat intake (g/d) | 93.38 ± 2.12 | 82.37 ± 3.27 | 99.44 ± 2.74 | 3.870 | <0.001 |
| Vegetable and fruit intake (g/d) | 397.87 ± 4.61 | 384.79 ± 208.47 | 405.09 ± 235.11 | 2.112 | 0.035 |
| BMI (kg/m2) | 22.74 ± 0.06 | 22.62 ± 0.10 | 22.81 ± 0.08 | 1.469 | 0.142 |
| SBP (mmHg) | 118.80 ± 11.51 | 120.64 ± 11.04 | 117.81 ± 11.64 | 5.771 | <0.001 |
| DBP (mmHg) | 74.60 ± 7.80 | 75.17 ± 7.54 | 74.29 ± 7.92 | 2.650 | 0.008 |
| TC | 4.82 ± 1.29 | 4.81 ± 1.22 | 4.82 ± 1.34 | 0.220 | 0.826 |
| TG | 1.76 ± 1.78 | 1.76 ± 1.61 | 1.75 ± 1.86 | 0.172 | 0.864 |
| HDL-C | 1.46 ± 0.59 | 1.47 ± 0.57 | 1.46 ± 0.59 | 0.314 | 0.754 |
| LDL-C | 2.68 ± 1.14 | 2.65 ± 1.14 | 2.69 ± 1.15 | 0.902 | 0.367 |
| Efficiency score | 0.69 ± 0.11 | 0.67 ± 0.11 | 0.70 ± 0.12 | 6.810 | <0.001 |
| Hazard Ratio (95% Confidence Interval) | |||
|---|---|---|---|
| Model 1 | Model 2 | Model 3 | |
| Efficiency score (per 0.1 increase) | 0.34 (0.18, 0.63) ** | 0.36 (0.19, 0.66) ** | 0.20 (0.09, 0.42) * |
| Subgroup analysis | |||
| Gender | |||
| Male | 0.22 (0.09, 0.55) ** | 0.23 (0.09, 0.56) ** | 0.15 (0.05, 0.44) ** |
| Female | 0.46 (0.20, 1.07) | 0.54 (0.23, 1.24) | 0.28 (0.10, 0.78) ** |
| Age, years | |||
| <60 | 0.49 (0.24, 1.00) | 0.47 (0.23, 0.95) * | 0.26 (0.11, 0.62) ** |
| ≥60 | 0.16 (0.05, 0.57) ** | 0.16 (0.05, 0.57) ** | 0.07 (0.01, 0.35) ** |
| Percentile of Efficiency Score | Coefficient of SBP(95%CI) | Coefficient of DBP(95%CI) |
|---|---|---|
| 10 | −17.88 (−37.45, 1.687) | 0.03 (−9.94, 9.99) |
| 20 | −13.39 (−26.61, −0.17) * | −3.39 (−15.90, 9.12) |
| 30 | −13.91 (−22.93, −4.90) ** | −2.84 (−14.67, 8.99) |
| 40 | −16.81 (−28.43, −5.19) ** | −4.19 (−13.35, 4.98) |
| 50 | −19.75 (−32.09, −7.42) ** | −4.00 (−10.85, 2.86) |
| 60 | −21.88 (−38.54, −5.21) * | −7.36 (−14.14, −0.58) * |
| 70 | −24.83 (−44.69, −4.96) * | −6.70 (−15.85, 2.44) |
| 80 | −19.63 (−34.33, −4.93) ** | −11.35 (−19.99, −2.71) * |
| 90 | −30.92 (−65.79, 3.95) | −16.50 (−27.54, −5.45) ** |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Yu, Y.; Chen, Y.; Wang, Y.; Yu, L.; Liu, T.; Fu, C. Is the Efficiency Score an Indicator for Incident Hypertension in the Community Population of Western China? Int. J. Environ. Res. Public Health 2021, 18, 10132. https://doi.org/10.3390/ijerph181910132
Yu Y, Chen Y, Wang Y, Yu L, Liu T, Fu C. Is the Efficiency Score an Indicator for Incident Hypertension in the Community Population of Western China? International Journal of Environmental Research and Public Health. 2021; 18(19):10132. https://doi.org/10.3390/ijerph181910132
Chicago/Turabian StyleYu, Yangwen, Yun Chen, Yiying Wang, Lisha Yu, Tao Liu, and Chaowei Fu. 2021. "Is the Efficiency Score an Indicator for Incident Hypertension in the Community Population of Western China?" International Journal of Environmental Research and Public Health 18, no. 19: 10132. https://doi.org/10.3390/ijerph181910132
APA StyleYu, Y., Chen, Y., Wang, Y., Yu, L., Liu, T., & Fu, C. (2021). Is the Efficiency Score an Indicator for Incident Hypertension in the Community Population of Western China? International Journal of Environmental Research and Public Health, 18(19), 10132. https://doi.org/10.3390/ijerph181910132