
Successful Reboot of High-Performance Sporting Activities by Japanese National Women’s Handball Team in Tokyo, 2020 during the COVID-19 Pandemic: An Initiative Using the Japan Sports–Cyber Physical System (JS–CPS) of the Sports Research Innovation Project (SRIP)

 , , , , ,
, , , , ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Participant Information
2.2. History of Training Restrictions Due to Japan’s State of Emergency before Rebooting the National Team’s Training Camp
2.3. Details of the First Domestic Training Camp after Japan’s COVID-19 State of Emergency and “Stay-Home” Social Policy
2.4. Scientific Monitoring
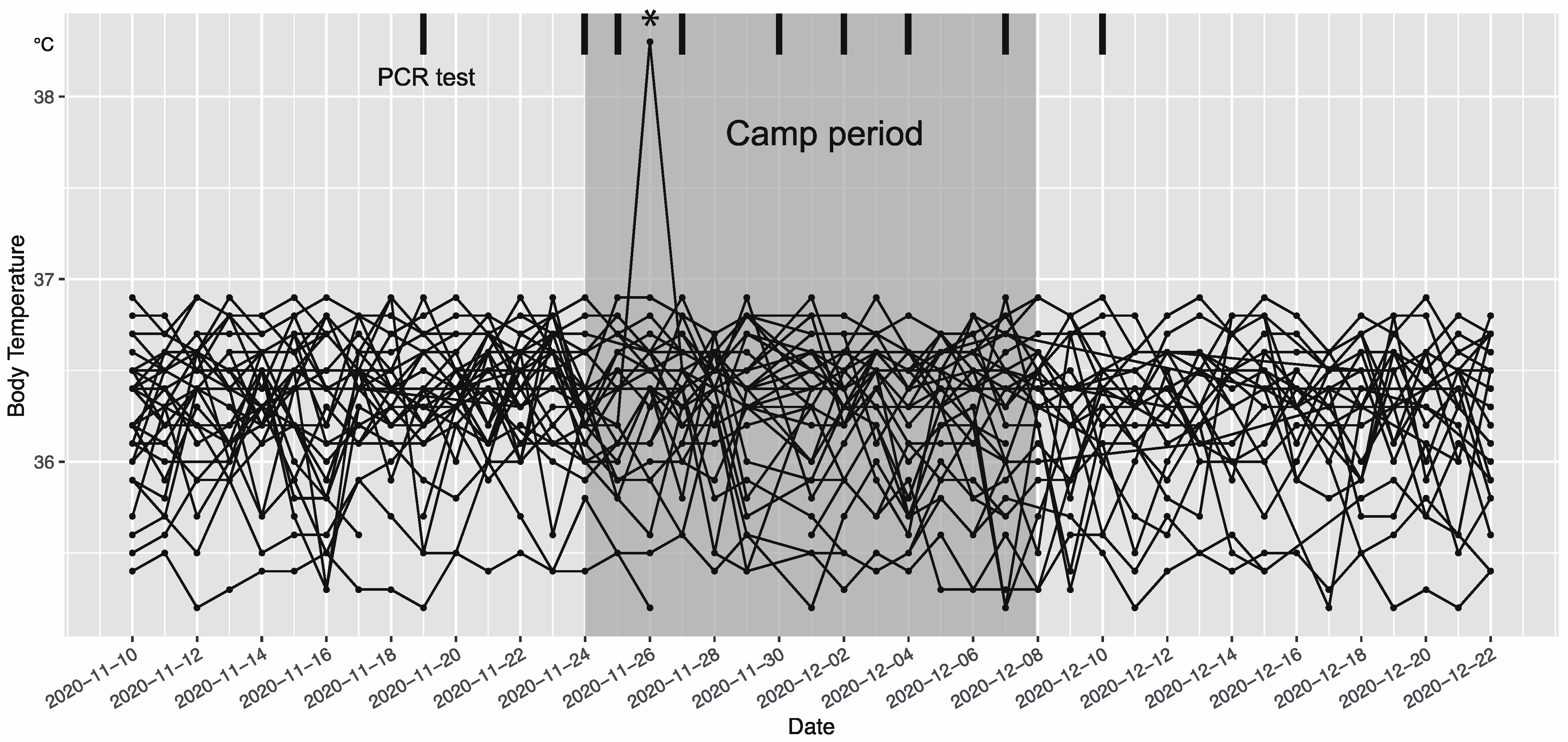
2.4.1. Web-Based Health Monitoring
2.4.2. Screening of SARS-CoV-2 with Frequent PCR Tests
- Precamp screening and postcamp verification.Each individual sampled their saliva (1 mL) at their residence under the online guidance of the researcher (I.O) on 19 November and 9 December, thereby providing pre- and postcamp samples, respectively. The centrifuge tube (primary packaging) containing saliva was wrapped with an absorbent sheet and tightly sealed in the biopouch (secondary packaging). The sample was then placed in a bio-mailer box (tertiary packaging) and sealed with a security sticker. Finally, the bio-mailer box was put into a quaternary packaging box. This box was then transported under the regulation of MHWL (Category B, UN3373) to the Group of Infection Control and Prevention (G-ICP) in Osaka University Hospital via Japan Post Co., Ltd., Tokyo, Japan. The results of pre- and postcamp PCR screening (all negative) were reported to JHA via email.
- SARS-CoV-2 PCR testing protocol in the camp at ANTC.During the camp period (from 24 November to 8 December), SARS-CoV-2 PCR testing was conducted every Monday, Wednesday, and Friday (ideally every 48 h, excluding weekends) [16]. On the “test day”, each athlete and staff sampled their saliva around 8:00 am. The samples were then immediately transported to the semi-onsite PCR center held in the Toho University Medical School (about 1.0 h from ANTC) and tested by the staff of the Osaka University ICP team. The mean sample-to-answer (turnaround) time was 4.2 h (including 1.0 h of sample transportation time); therefore. the team staff could announce the results of the PCR tests at around 13:00 on every testing day, prior to the start of the afternoon training session (~15:30).
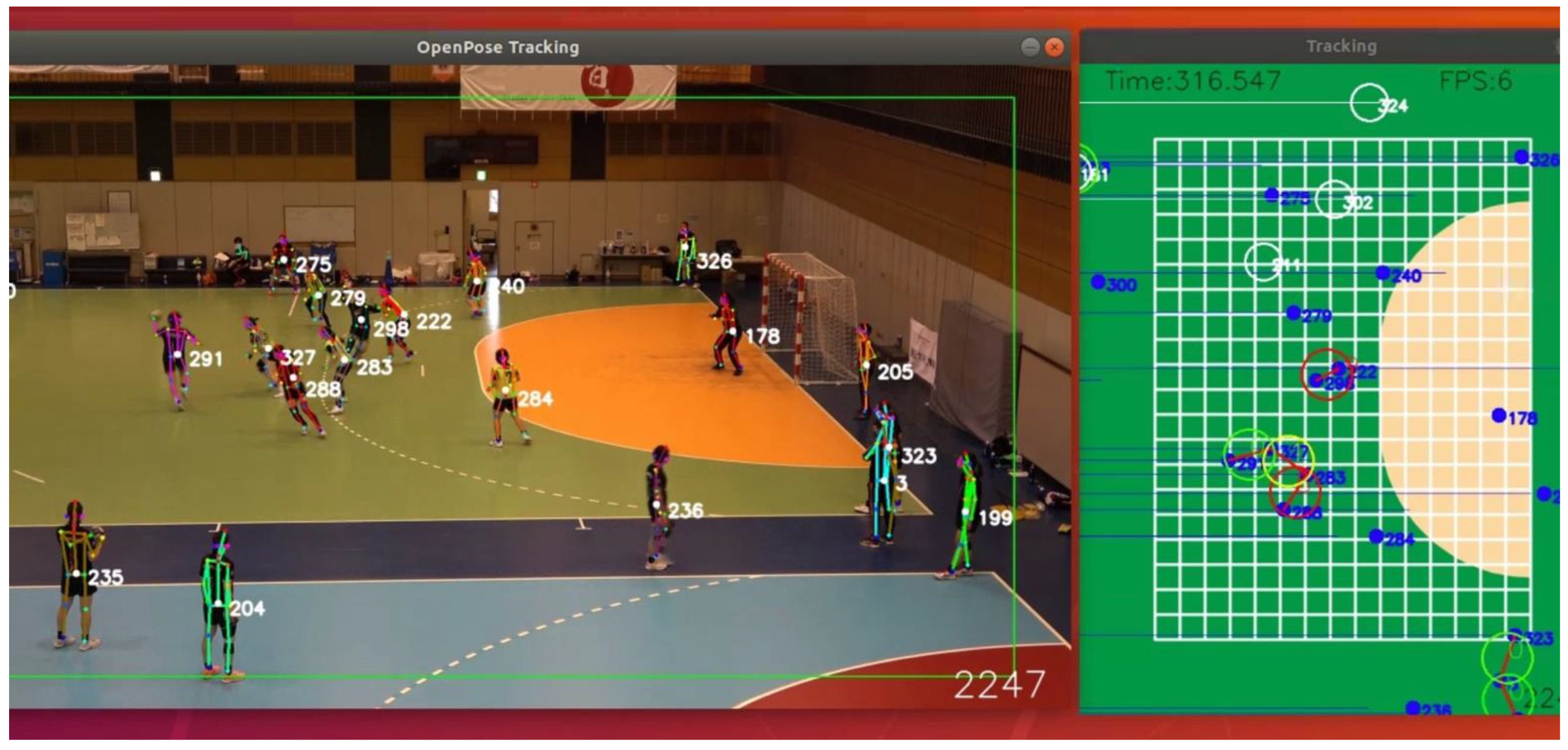
2.4.3. Real-Time Automated Quantitative Monitoring of Social Distancing with Motion Image-Based AI System
2.4.4. Heart Rate and Activity Monitoring with a Wearable Sensor Device
2.5. Data Analysis
3. Results
4. Discussion
4.1. Web-Based Health Monitoring
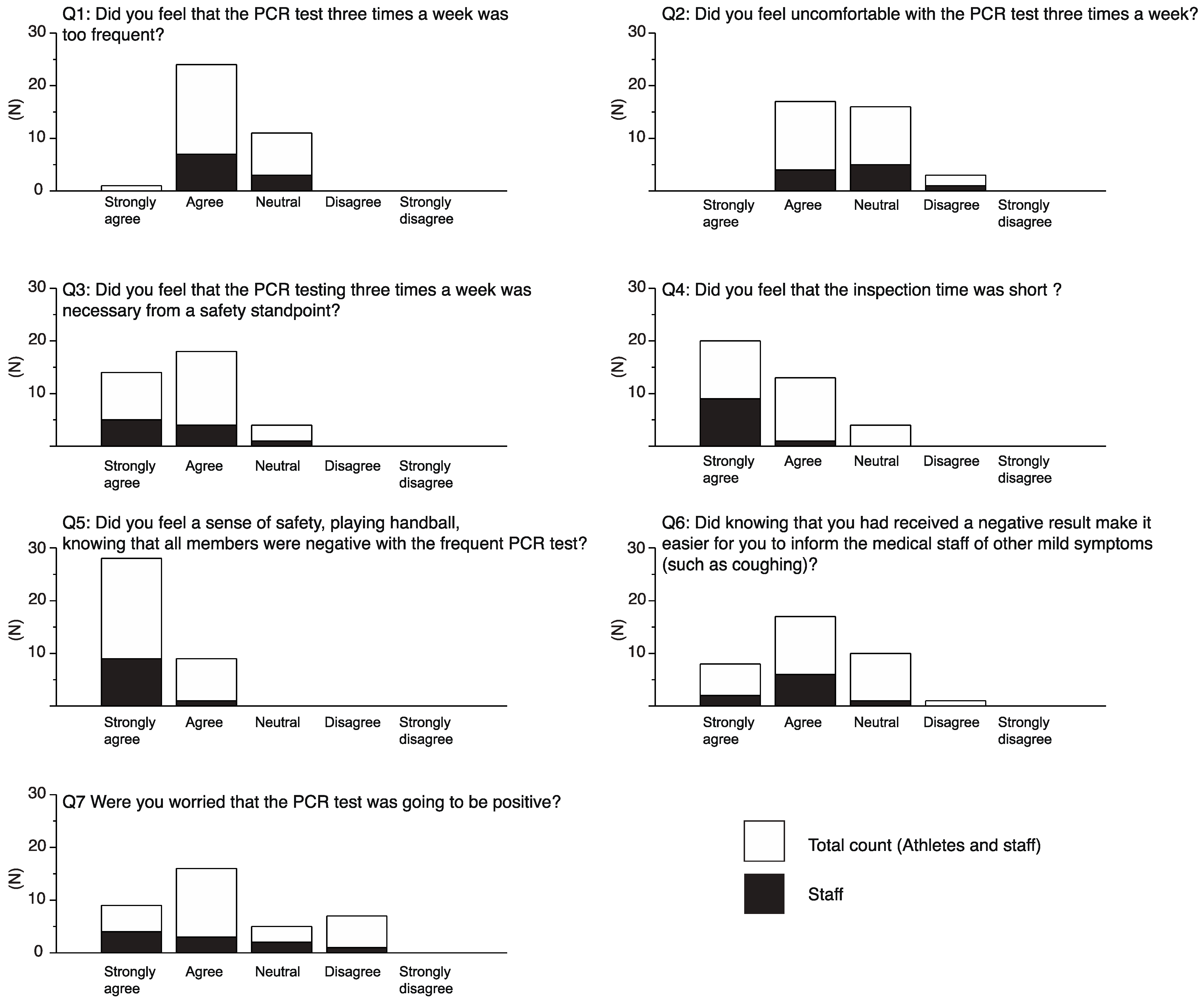
4.2. SARS-CoV-2 PCR Testing and Feedback
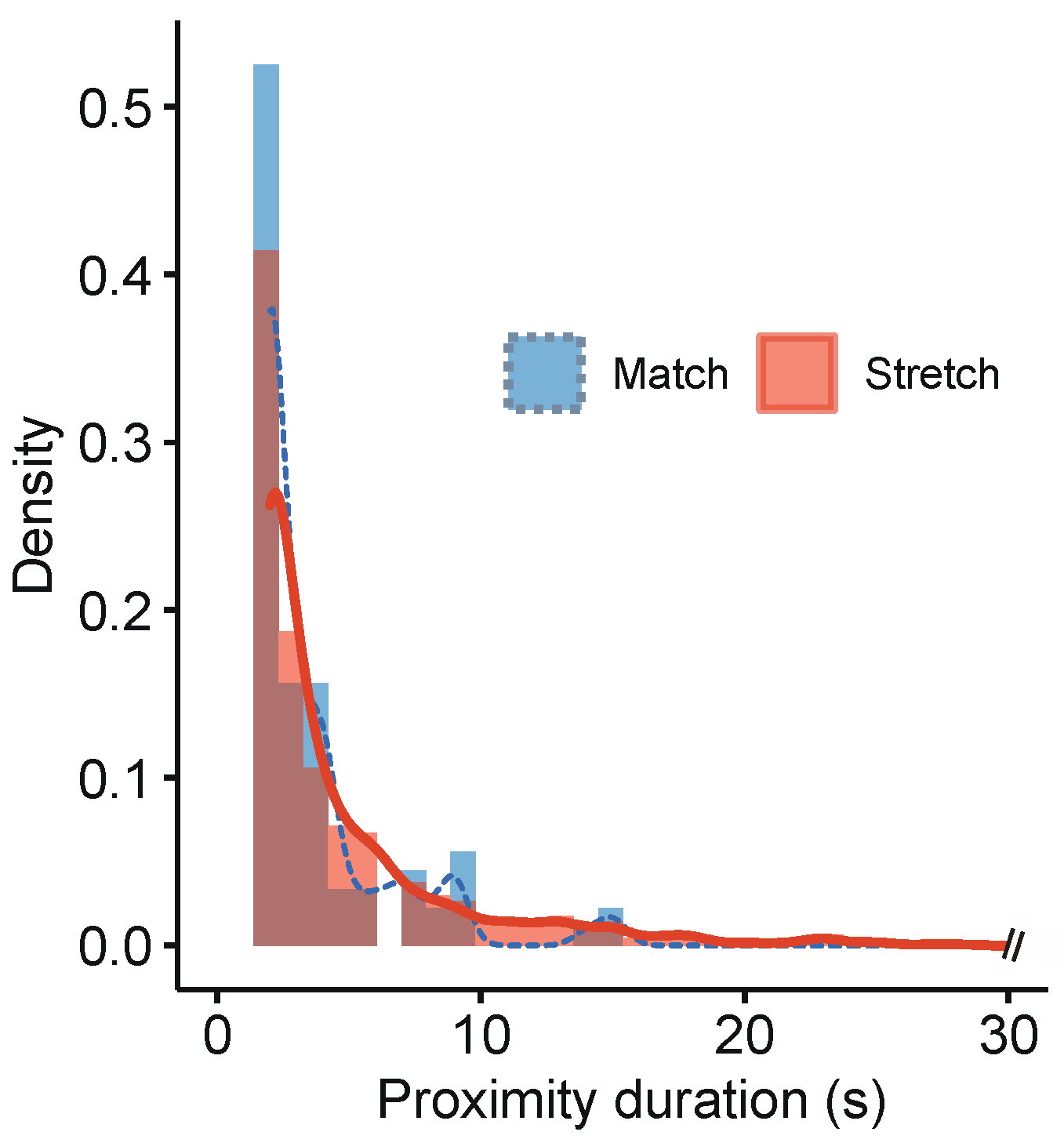
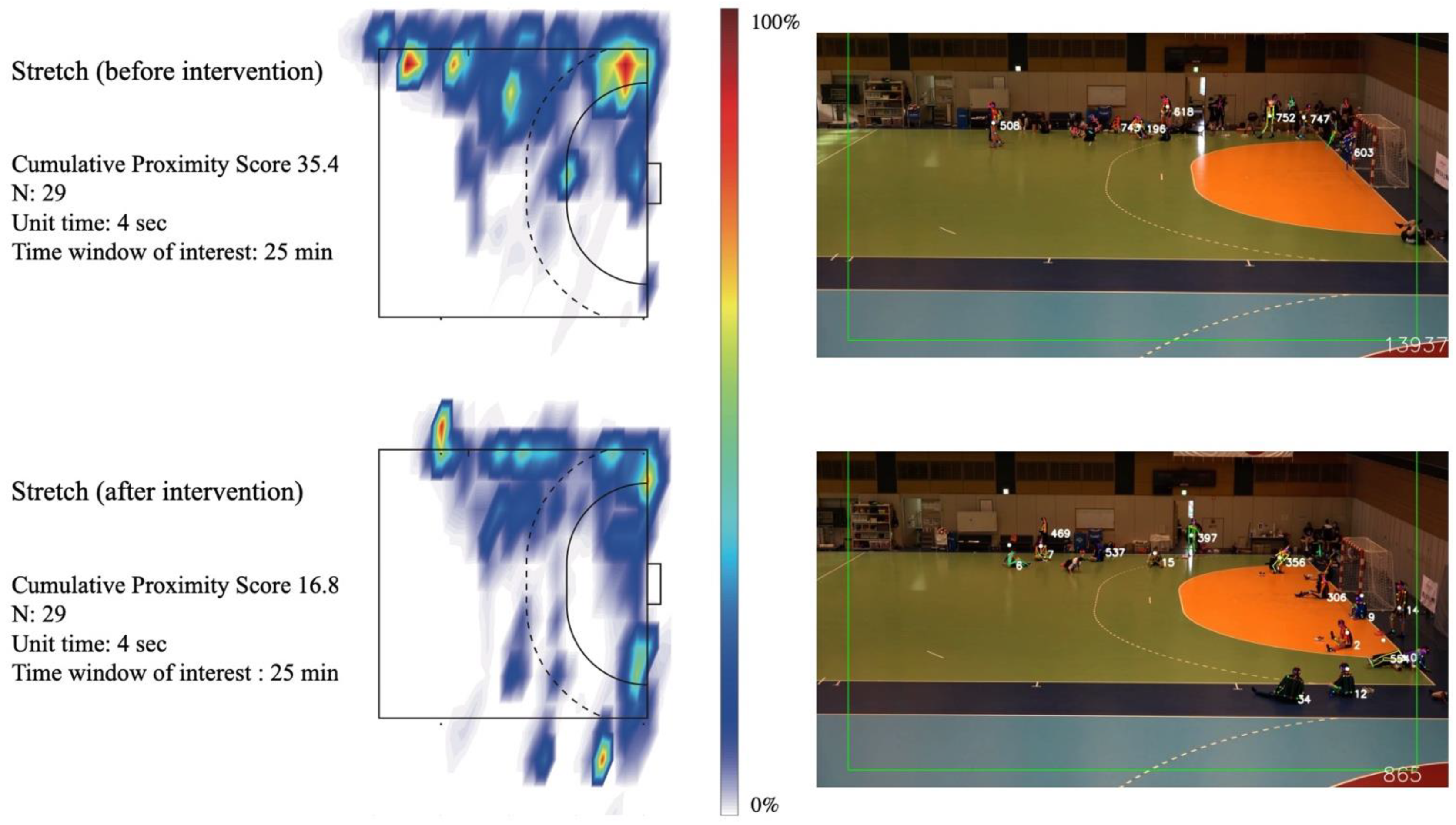
4.3. Real-Time Automated Qualitative Monitoring of Social Distancing on the Handball Court Using a Video-Based AI Algorithm
4.4. Heart Rate and Physical Intensity Evaluation Using the Wearable Sensor
4.5. Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
| SARS-CoV-2 | Severe acute respiratory syndrome coronavirus 2 |
| CPS | Cyber physical system |
| PCR | Polymerase chain reaction |
| AI | Artificial intelligence |
| JHA | Japan Handball Association |
| SRIP | Sports Research Innovation Project, Osaka University |
| ANTC | Ajinomoto National Training Center |
| JSA | Japan Sports Agency |
| JOC | Japan Olympic Committee |
| MHWL | Japanese Ministry of Health, Labor, and Welfare |
| G-ICP | Group of Infection Control and Prevention, Osaka University |
References
- Hermassi, S.; Bouhafs, E.; Bragazzi, N.; Ichimura, S.; Alsharji, K.; Hayes, L.; Schwesig, R. Effects of Home Confinement on the Intensity of Physical Activity during the COVID-19 Outbreak in Team Handball According to Country, Gender, Competition Level, and Playing Position: A Worldwide Study. Int. J. Environ. Res. Public Health 2021, 18, 4050. [Google Scholar] [CrossRef]
- Maugeri, A.; Barchitta, M.; Agodi, A. A Clustering Approach to Classify Italian Regions and Provinces Based on Prevalence and Trend of SARS-CoV-2 Cases. Int. J. Environ. Res. Public Health 2020, 17, 5286. [Google Scholar] [CrossRef] [PubMed]
- Hermassi, S.; Sellami, M.; Salman, A.; Al-Mohannadi, A.; Bouhafs, E.; Hayes, L.; Schwesig, R. Effects of COVID-19 Lockdown on Physical Activity, Sedentary Behavior, and Satisfaction with Life in Qatar: A Preliminary Study. Int. J. Environ. Res. Public Health 2021, 18, 3093. [Google Scholar] [CrossRef] [PubMed]
- Fiorilli, G.; Grazioli, E.; Buonsenso, A.; Di Martino, G.; Despina, T.; Calcagno, G.; di Cagno, A. A national COVID-19 quarantine survey and its impact on the Italian sports community: Implications and recommendations. PLoS ONE 2021, 16, 0248345. [Google Scholar] [CrossRef] [PubMed]
- Di Cagno, A.; Buonsenso, A.; Baralla, F.; Grazioli, E.; Di Martino, G.; Lecce, E.; Calcagno, G.; Fiorilli, G. Psychological Impact of the Quarantine-Induced Stress during the Coronavirus (COVID-19) Outbreak among Italian Athletes. Int. J. Environ. Res. Public Health 2020, 17, 8867. [Google Scholar] [CrossRef]
- Håkansson, A.; Jönsson, C.; Kenttä, G. Psychological Distress and Problem Gambling in Elite Athletes during COVID-19 Restrictions—A Web Survey in Top Leagues of Three Sports during the Pandemic. Int. J. Environ. Res. Public Health 2020, 17, 6693. [Google Scholar] [CrossRef]
- Allegrante, J.P.; Auld, M.E.; Natarajan, S. Preventing COVID-19 and its sequela:“there is no magic bullet… it’s just behaviors”. Am. J. Prev. Med. 2020, 59, 288–292. [Google Scholar] [CrossRef] [PubMed]
- Pifarré, F.; Zabala, D.D.; Grazioli, G.; Maura, I.D.Y.I. COVID-19 and mask in sports. Apunt. Sports Med. 2020, 55, 143–145. [Google Scholar] [CrossRef]
- Manchado, C.; Tortosa-Martinez, J.; Vila, H.; Ferragut, C.; Platen, P. Performance Factors in Women’s Team Handball. J. Strength Cond. Res. 2013, 27, 1708–1719. [Google Scholar] [CrossRef] [Green Version]
- World Health Organization Headquarters. Considerations for Sports Federations/Sports Event Organizers When Planning Mass Gatherings in the Context of COVID-19; WHO/2019-nCoV/Mass_Gatherings_Sports/2020.1; WHO: Geneva, Switzerland, 2020. [Google Scholar]
- Shrivastava, S.R.; Shrivastava, P.S. Resuming international sporting events affected by coronavirus disease 2019 pandemic in a bio-secure bubble. Saudi J. Sports Med. 2020, 20, 55. [Google Scholar] [CrossRef]
- McHill, A.W.; Chinoy, E.D. Utilizing the National Basketball Association’s COVID-19 restart “bubble” to uncover the impact of travel and circadian disruption on athletic performance. Sci. Rep. 2020, 10, 1–7. [Google Scholar] [CrossRef] [PubMed]
- Jukic, I.; Calleja-González, J.; Cos, F.; Cuzzolin, F.; Olmo, J.; Terrados, N.; Njaradi, N.; Sassi, R.; Requena, B.; Milanovic, L.; et al. Strategies and Solutions for Team Sports Athletes in Isolation due to COVID-19. Sports 2020, 8, 56. [Google Scholar] [CrossRef]
- Toresdahl, B.G.; Asif, I.M. Coronavirus Disease 2019 (COVID-19): Considerations for the Competitive Athlete. Sports Health A Multidiscip. Approach 2020, 12, 221–224. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wilson, M.G.; Hull, J.H.; Rogers, J.; Pollock, N.; Dodd, M.; Haines, J.; Harris, S.; Loosemore, M.; Malhotra, A.; Pieles, G.; et al. Cardiorespiratory considerations for return-to-play in elite athletes after COVID-19 infection: A practical guide for sport and exercise medicine physicians. Br. J. Sports Med. 2020, 54, 1157–1161. [Google Scholar] [CrossRef] [PubMed]
- Larremore, D.B.; Wilder, B.; Lester, E.; Shehata, S.; Burke, J.M.; Hay, J.A.; Tambe, M.; Mina, M.J.; Parker, R. Test sensitivity is secondary to frequency and turnaround time for COVID-19 screening. Sci. Adv. 2021, 7, eabd5393. [Google Scholar] [CrossRef] [PubMed]
- Cao, Z.; Hidalgo Martinez, G.; Simon, T.; Wei, S.-E.; Sheikh, Y.A. OpenPose: Realtime Multi-Person 2D Pose Estimation using Part Affinity Fields. IEEE Trans. Pattern Anal. Mach. Intell. 2018, 43, 172–186. [Google Scholar] [CrossRef] [Green Version]
- Córdova, A.; Latasa, I. Respiratory flows as a method for safely preventing the coronavirus transmission (COVID-19). Apunt. Sports Med. 2020, 55, 81–85. [Google Scholar] [CrossRef]
- Scholkmann, F.; Wolf, U. The Pulse-Respiration Quotient: A Powerful but Untapped Parameter for Modern Studies about Human Physiology and Pathophysiology. Front. Physiol. 2019, 10, 371. [Google Scholar] [CrossRef] [Green Version]
- Manchado, C.; Pers, J.; Navarro, F.; Han, A.; Sung, E.; Platen, P. Time-motion analysis in women’s team handball: Importance of aerobic performance. J. Hum. Sport Exerc. 2013, 8, 376–390. [Google Scholar] [CrossRef] [Green Version]
- Infectious Disease Surveillance Center; National Institute of Infectious Diseases. Guidelines for Active Epidemiological Investigation in Patients with Novel Coronavirus Infection (Tentative Version). 2020. Available online: https://www.niid.go.jp/niid/images/epi/corona/2019nCoV-02-200206-en.pdf (accessed on 1 February 2020).
- Knudsen, N.S.; Thomasen, M.M.; Andersen, T.B. Spread of Virus during Soccer Matches. medRxiv 2020. [Google Scholar] [CrossRef]
- Póvoas, S.C.; Seabra, A.F.; Ascensão, A.A.; Magalhães, J.; Soares, J.M.; Rebelo, A.N. Physical and Physiological Demands of Elite Team Handball. J. Strength Cond. Res. 2012, 26, 3365–3375. [Google Scholar] [CrossRef] [PubMed]
- Kniubaite, A.; Skarbalius, A.; Clemente, F.M.; Conte, D. Quantification of external and internal match loads in elite female team handball. Biol. Sport 2019, 36, 311–316. [Google Scholar] [CrossRef] [PubMed]
- Freire, L.D.A.; Tannure, M.; Sampaio, M.; Slimani, M.; Znazen, H.; Bragazzi, N.L.; Aedo-Muñoz, E.; Soto, D.A.S.; Brito, C.J.; Miarka, B. COVID-19-Related Restrictions and Quarantine COVID-19: Effects on Cardiovascular and Yo-Yo Test Performance in Professional Soccer Players. Front. Psychol. 2020, 11, 589543. [Google Scholar] [CrossRef] [PubMed]
- Demarie, S.; Galvani, C.; Billat, V.L. Horse-Riding Competitions Pre and Post COVID-19: Effect of Anxiety, sRPE and HR on Performance in Eventing. Int. J. Environ. Res. Public Health 2020, 17, 8648. [Google Scholar] [CrossRef]
- Fikenzer, S.; Fikenzer, K.; Laufs, U.; Falz, R.; Pietrek, H.; Hepp, P. Impact of COVID-19 lockdown on endurance capacity of elite handball players. J. Sports Med. Phys. Fitness 2020. [Google Scholar] [CrossRef]
- Althubaiti, A. Information bias in health research: Definition, pitfalls, and adjustment methods. J. Multidiscip. Healthc. 2016, 9, 211–217. [Google Scholar] [CrossRef] [Green Version]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Athletes | Staff | |
|---|---|---|
| Number of participant (female, male) | 29 (29, 0) | 24 (4, 20) |
| Mean age (SD) | 28.4 (4.1) y | 40.2 (14.2) y |
| Mean height (SD) | 163.8 (18.8) cm | 171.2 (11.1) cm |
| Mean weight (SD) | 66.7 (8.3) kg | 70.7 (13.2) kg |
| Mean training hours per week during camp | 18 h per week | |
| History of COVID-19 infection before camp | None | None |
| COVID-19 infections after camp | None | None |
| Date | Schedule | Samples: Athletes | Samples: Staff | Results | Sample-to-Answer Time * | Note |
|---|---|---|---|---|---|---|
| 20 November | Precamp | 28 | 21 | Negative | — | All athletes and staff transported their saliva samples to Osaka University from their home teams. Based on these results, the JHA recruited all athletes and staff. |
| 24 November | In-camp, start up | 28 | 11 | Negative | 5.5 h | |
| 25 November | In-camp, regular | 28 | 10 | Negative | 3 h | |
| 25 November | In-camp, irregular | 1 | 0 | Negative | 3 h | One additional athlete was invited. |
| 26 November | In-camp, irregular | 4 | 0 | Negative | 3 h | One athlete recorded a fever on the morning of 26 November. This athlete and three other athletes from the same home team were tested for screening purposes. |
| 27 November | In-camp, regular | 29 | 12 | Negative | 5.5 h | |
| 30 November | In-camp, regular | 29 | 12 | Negative | 5 h | |
| 2 December | In-camp, regular | 28 | 11 | Negative | 5 h | One athlete retired because of injury. |
| 4 December | In-camp, regular | 28 | 10 | Negative | 4 h | |
| 7 December | In-camp, regular | 28 | 11 | Negative | 4 h | |
| 10 December | Postcamp | 29 | 6 | Negative | — | All athletes and staff transported their saliva samples to Osaka University from their home teams. Based on these results, the JHA allowed them to return to their regular practices and jobs. |
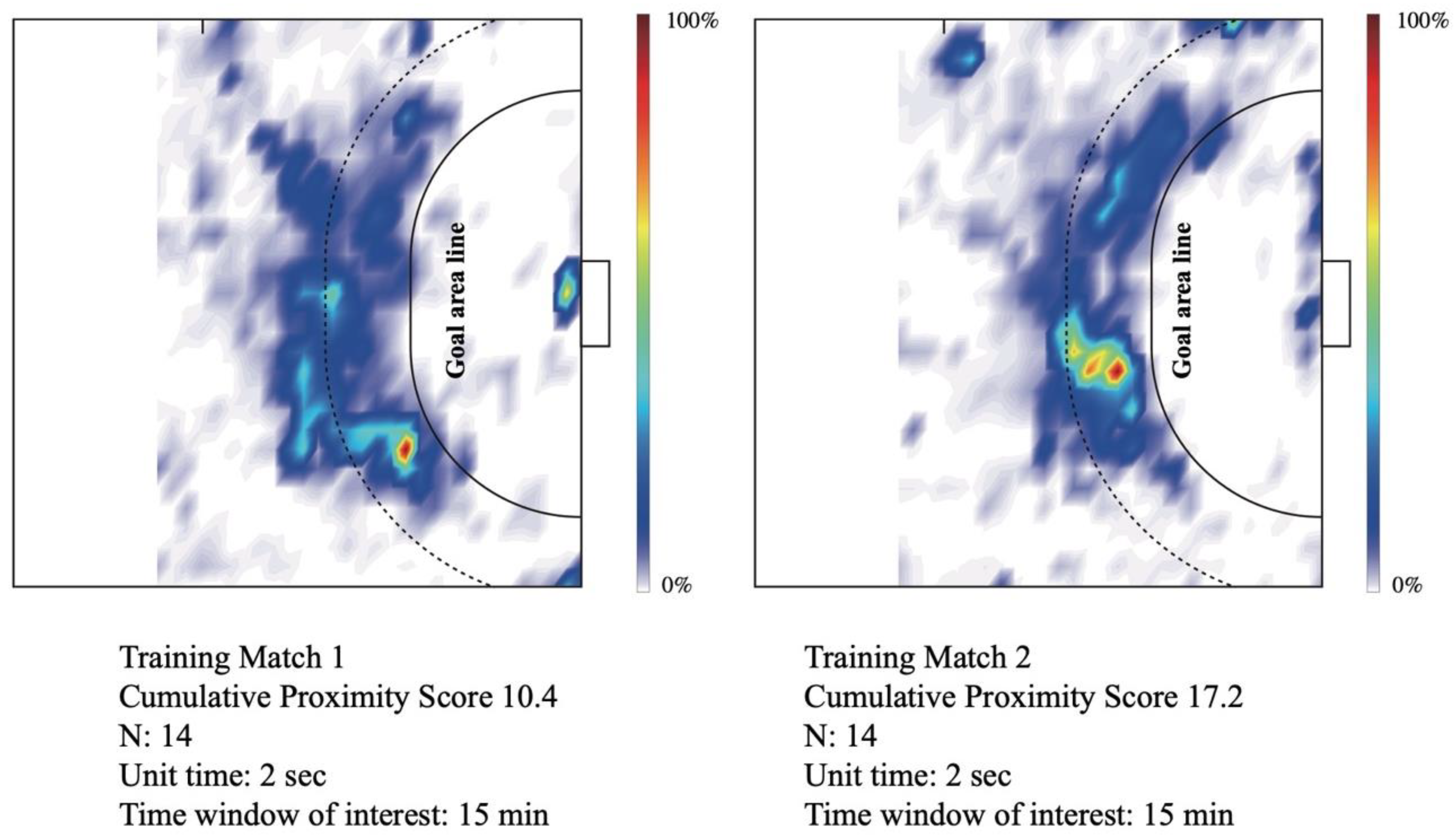
| Cumulative Proximity Score (UT Adjusted) | Unit Time (s) | Maximum Proximity Duration (s) | Averaged Proximity Duration (s) | Time Window of Interest (min) | Number of Athletes in Video ROI | |
|---|---|---|---|---|---|---|
| Training Match 1 | 10.4 | 2 | 21 | 2.4 | 15 | 14 |
| Training Match 2 | 17.2 | 2 | 31 | 2.5 | 15 | 14 |
| Stretch (before feedback) | 35.4 | 4 | 56 | 3.9 | 25 | 29 |
| Stretch (after feedback) | 16.8 | 4 | 60 | 2.5 | 25 | 29 |
| Position | At Rest (SD) | 3000 m Run (SD) | Max in Match (%3000 m) | Average in Match (%3000 m) |
|---|---|---|---|---|
| BP | 58.8 (13.4) | 186.6 (8.5) | 191.9 (104.0%) | 155.9 (84.5%) |
| PV | 61.0 (4.2) | 186.0 (10.7) | 194.9 (105.1%) | 144.9 (81.9%) |
| WG | 64.9 (9.1) | 184.0 (7.3) | 182.7 (99.4%) | 148.4 (80.7%) |
| GK | 67.3 (6.4) | 185.3 (8.5) | 169.7 (87.5%) | 144.9 (74.7%) |
| Zone 1 (%) | Zone 2 (%) | Zone 3 (%) | Zone 4 (%) | Zone 5 (%) | |
|---|---|---|---|---|---|
| BP | 16.5 ± 8.8 | 19.2 ± 9.1 | 24.7 ± 11.1 | 23.2 ± 11.8 | 15.7 ± 18.0 |
| PV | 22.3 ± 10.8 | 16.5 ± 5.3 | 22.2 ± 7.0 | 30.2 ± 5.7 | 8.3 ± 6.7 |
| WG | 18.5 ± 12.1 | 33.2 ± 12.5 | 26.8 ± 9.6 | 15.8 ± 9.2 | 5.3 ± 6.2 |
| GK | 44.4 ± 25.9 | 53.3 ± 24.1 | 2.3 ± 1.8 | 0.0 ± 0.0 | 0.0 ± 0.0 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ogasawara, I.; Hamaguchi, S.; Hasegawa, R.; Akeda, Y.; Ota, N.; Revankar, G.S.; Konda, S.; Taguchi, T.; Takanouchi, T.; Imoto, K.; et al. Successful Reboot of High-Performance Sporting Activities by Japanese National Women’s Handball Team in Tokyo, 2020 during the COVID-19 Pandemic: An Initiative Using the Japan Sports–Cyber Physical System (JS–CPS) of the Sports Research Innovation Project (SRIP). Int. J. Environ. Res. Public Health 2021, 18, 9865. https://doi.org/10.3390/ijerph18189865
Ogasawara I, Hamaguchi S, Hasegawa R, Akeda Y, Ota N, Revankar GS, Konda S, Taguchi T, Takanouchi T, Imoto K, et al. Successful Reboot of High-Performance Sporting Activities by Japanese National Women’s Handball Team in Tokyo, 2020 during the COVID-19 Pandemic: An Initiative Using the Japan Sports–Cyber Physical System (JS–CPS) of the Sports Research Innovation Project (SRIP). International Journal of Environmental Research and Public Health. 2021; 18(18):9865. https://doi.org/10.3390/ijerph18189865
Chicago/Turabian StyleOgasawara, Issei, Shigeto Hamaguchi, Ryosuke Hasegawa, Yukihiro Akeda, Naoki Ota, Gajanan S. Revankar, Shoji Konda, Takashi Taguchi, Toshiya Takanouchi, Kojiro Imoto, and et al. 2021. "Successful Reboot of High-Performance Sporting Activities by Japanese National Women’s Handball Team in Tokyo, 2020 during the COVID-19 Pandemic: An Initiative Using the Japan Sports–Cyber Physical System (JS–CPS) of the Sports Research Innovation Project (SRIP)" International Journal of Environmental Research and Public Health 18, no. 18: 9865. https://doi.org/10.3390/ijerph18189865
APA StyleOgasawara, I., Hamaguchi, S., Hasegawa, R., Akeda, Y., Ota, N., Revankar, G. S., Konda, S., Taguchi, T., Takanouchi, T., Imoto, K., Okimoto, N., Sakuma, K., Uchiyama, A., Yamasaki, K., Higashino, T., Tomono, K., & Nakata, K. (2021). Successful Reboot of High-Performance Sporting Activities by Japanese National Women’s Handball Team in Tokyo, 2020 during the COVID-19 Pandemic: An Initiative Using the Japan Sports–Cyber Physical System (JS–CPS) of the Sports Research Innovation Project (SRIP). International Journal of Environmental Research and Public Health, 18(18), 9865. https://doi.org/10.3390/ijerph18189865