
Factors Affecting Motivation among Key Populations to Engage with Tuberculosis Screening and Testing Services in Northwest Tanzania: A Mixed-Methods Analysis


 , ,
, ,  ,
,  and
and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Context
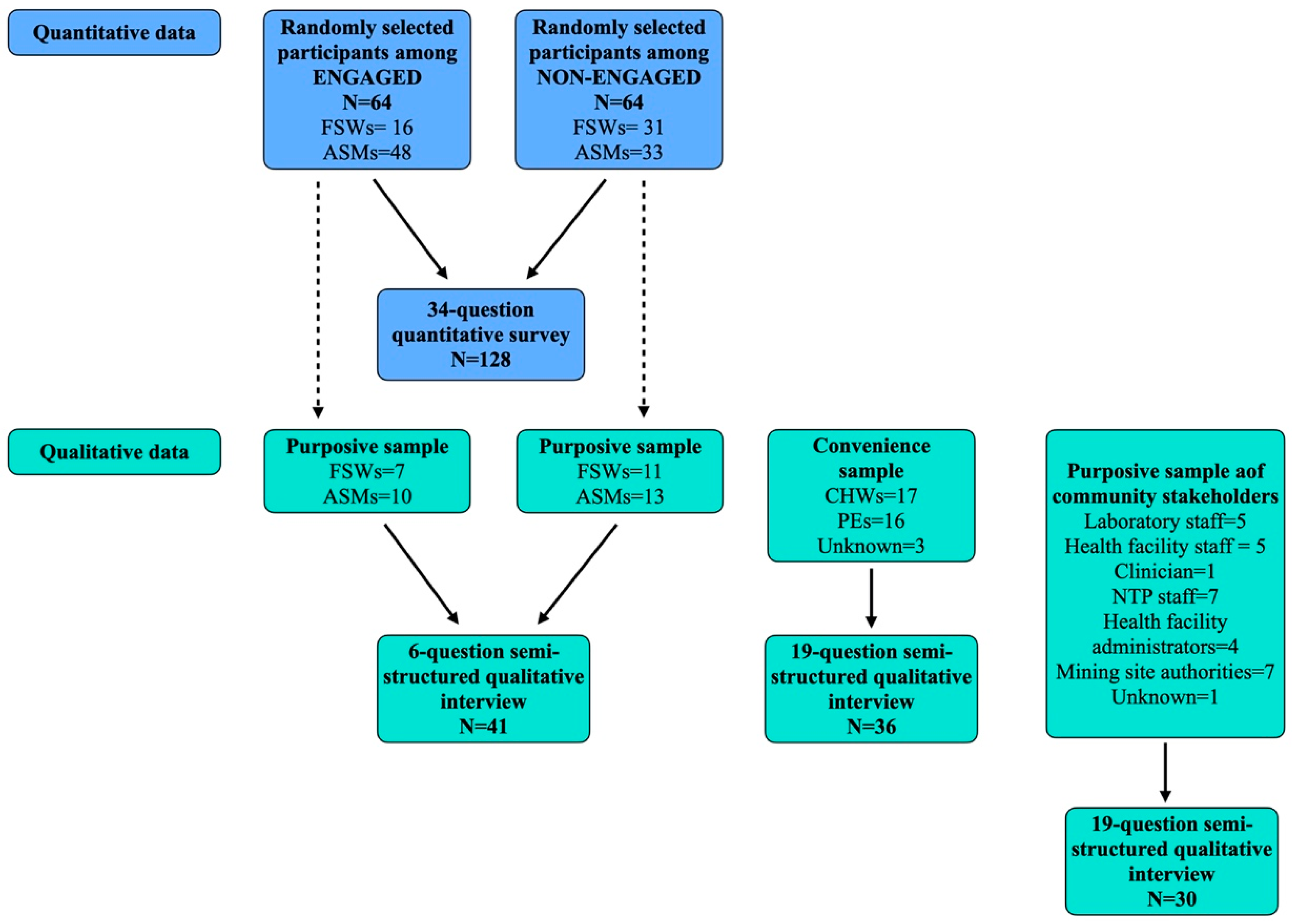
2.2. Study Design
2.3. Quantitative Data Collection and Analysis
2.4. Qualitative Data Collection and Analysis
3. Results
3.1. Quantitative Results
3.2. Qualitative Data
3.2.1. Factors Influencing Engagement of ASMs and FSWs by the Intervention
- a.
- Health-seeking practices
- b.
- Perception of the intervention
3.2.2. Perspectives of CHWs and PEs
- a.
- Motivations to occupy CHW/PE positions
- b.
- Role in the intervention and benefits to the community
“My community believe in the witchcraft and traditional healer so by giving them education [they] benefit from what I deliver to them.”(male, PE)
- c.
- Challenges experienced
“If I will not take precaution, [then] I am at greater risk of been infected with TB from the client [to] whom we provide services.”(male, PE)
- d.
- Recommendations
3.2.3. Community Stakeholder Perspectives on the Intervention
- a.
- Aspects to improve and recommendations
“[There] should be frequent supply of the medical equipment especially the sputum containers, there [was] a time [when] we faced [a] shortage of the sputum containers and by the helping of SHDEPHA [we got] containers from Shinyanga regional.”(female, NTP staff)
“It [is] hard for the ASM community to know if they have been infected with TB due to the nature of their work, [they] are exposed to dust, even if they show TB symptoms they do not take serious, they think it is because of the dust.”(male, mining site authority)
- b.
- Strengths and benefits to the community
“They managed to have so many indicators that serve the community, much determination in providing services to the community, having the CHW who contribute much to high notification.”(NTP staff, male)
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- World Health Organization. Global Tuberculosis Report 2020; World Health Organization: Geneva, Switzerland, 2020. [Google Scholar]
- World Health Organization. Tuberculosis Profile: United Republic of Tanzania 2021. Available online: https://worldhealthorg.shinyapps.io/tb_profiles/?_inputs_&entity_type=%22country%22&lan=%22EN%22&iso2=%22TZ%22 (accessed on 20 February 2021).
- Merket, H. Mapping Artisanal and Small-Scale Mining in Northwest Tanzania: A Survey on Its Nature, Scope and Impact 2019; IPIS: Antwerp, Belgium, 2019. [Google Scholar]
- Stuckler, D.; Basu, S.; McKee, M.; Lurie, M. Mining and Risk of Tuberculosis in Sub-Saharan Africa. Am. J. Public Health 2011, 101, 524–530. [Google Scholar] [CrossRef] [PubMed]
- Rees, D.; Murray, J. Silica, silicosis and tuberculosis. Int. J. Tuberc. Lung Dis. 2007, 11, 474–484. [Google Scholar] [PubMed]
- Auvert, B.; Ballard, R.; Campbell, C.; Caraël, M.; Carton, M.; Fehler, G.; Gouws, E.; MacPhail, C.; Taljaard, D.; Van Dam, J.; et al. HIV infection among youth in a South African mining town is associated with herpes simplex virus-2 seropositivity and sexual behaviour. AIDS 2001, 15, 885–898. [Google Scholar] [CrossRef] [PubMed]
- Llongo, I. Tuberculosis health belief gaps of tuberculosis and suspected tuberculosis cases in New York City. Int. J. Clin. Health Psychol. 2004, 4, 69–90. [Google Scholar]
- Glanz, K.; Rimer, B.K.; Viswanath, K. Health Behavior and Health Education: Theory, Research, and Practice; Wiley: Hoboken, NJ, USA, 2008. [Google Scholar]
- Yusof, A.; Chia, Y.C.; Hasni, Y.M. Awareness and prevalence of mammography screening and its predictors--a cross sectional study in a primary care clinic in Malaysia. Asian Pac. J. Cancer Prev. 2014, 15, 8095–8099. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Karimy, M.; Azarpira, H.; Araban, M. Using Health Belief Model Constructs to Examine Differences in Adherence to Pap Test Recommendations among Iranian Women. Asian Pac. J. Cancer Prev. 2017, 18, 1389–1394. [Google Scholar] [CrossRef] [PubMed]
- Public Health Agency of Canada. Community Capacity Building Tool; Public Health Agency of Canada: Ottawa, ON, Canada, 2007. [Google Scholar]
- Lasater, M.E.; Grosso, A.; Ketende, S.; Lyons, C.; Pitche, V.P.; Tchalla, J.; Anato, S.; Sodji, D.; Nadedjo, F.; Baral, S. Characterising the relationship between migration and stigma affecting healthcare engagement among female sex workers in Lomé, Togo. Glob. Public Health 2019, 14, 1428–1441. [Google Scholar] [CrossRef] [PubMed]
- Phrasisombath, K.; Thomsen, S.; Sychareun, V.; Faxelid, E. Care seeking behaviour and barriers to accessing services for sexually transmitted infections among female sex workers in Laos: A cross-sectional study. BMC Health Serv. Res. 2012, 12, 37. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Colvin, C.; Mugyabuso, J.; Munuo, G.; Lyimo, J.; Oren, E.; Mkomwa, Z.; Makame, M.; Mwangomale, A.; Mahamba, V.; Mueller, L.; et al. Evaluation of community-based interventions to improve TB case detection in a rural district of Tanzania. Glob. Health Sci. Pract. 2014, 2, 219–225. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Verhagen, L.M.; Kapinga, R.; Van Rosmalen-Nooijens, K.A.W.L. Factors underlying diagnostic delay in tuberculosis patients in a rural area in Tanzania: A qualitative approach. Infection 2010, 38, 433–446. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rambiki, E.; Dimba, A.; Banda, P.; Ng’ambi, W.; Banda, K.; Girma, B. The prevalence of pulmonary tuberculosis among miners from the Karonga, Rumphi, Kasungu and Lilongwe Districts of Malawi in 2019. Malawi Med. J. 2020, 32, 184–191. [Google Scholar] [PubMed]
- Stuckler, D.; Steele, S.; Lurie, M.; Basu, S. Introduction: ’dying for gold’: The effects of mineral miningon HIV, tuberculosis, silicosis, and occupational diseases in southern Africa. Int. J. Health Serv. 2013, 43, 639–649. [Google Scholar] [CrossRef] [PubMed]
- Ohene, S.-A.; Bonsu, F.; Adusi-Poku, Y.; Dzata, F.; Bakker, M. Case finding of tuberculosis among mining communities in Ghana. PLoS ONE 2021, 16, e0248718. [Google Scholar] [CrossRef] [PubMed]
- Pande, T.; Vasquez, N.A.; Cazabon, D.; Creswell, J.; Brouwer, M.; Ramis, O. Finding the missing millions: Lessons from 10 ac-tive case finding interventions in high tuberculosis burden countries. BMJ Glob. Health 2020, 5, e003835. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Engaged * (%) | Non-Engaged ** (%) | Odds Ratio | p-Value | |
|---|---|---|---|---|
| Gender | ||||
| Female | 37 (58) | 32 (50) | 1 | |
| Male | 27 (42) | 32 (50) | 1.33 | 0.42 |
| Age | ||||
| 18–23 | 6 (9) | 7 (11) | 1 | |
| 24–30 | 17 (27) | 19 (30) | 1.04 | 0.95 |
| 31–40 | 24 (38) | 27 (42) | 1.03 | 0.95 |
| 41–50 | 17 (27) | 11 (17) | 1.80 | 0.38 |
| Residence | ||||
| Geita | 32 (50) | 31 (50) | 1 | |
| Shinyanga | 32 (50) | 31 (50) | 1 | 1 |
| Level of education | ||||
| Primary and lower level | 50 (79) | 51 (80) | 1 | |
| Secondary school level | 13 (21) | 11 (17) | 1.21 | 0.68 |
| Higher studies | 0 (0) | 2 (3) | – | |
| Type of work | ||||
| Female sex worker | 16 (25) | 31 (48) | 1 | |
| Drilling | 30 (47) | 26 (41) | 2.24 | 0.05 |
| Stone crushing | 18 (28) | 11 (7) | 4.98 | 0.003 |
| Income level | ||||
| Less than 2000 Tanzanian shillings per day | 48 (76) | 36 (56) | 1 | |
| More than 2000 Tanzanian shillings per day | 15 (24) | 28 (44) | 0.40 | 0.02 |
| Length of work in small-scale mining | ||||
| Less than 6 months | 2 (3) | 3 (5) | 1 | |
| 6 months–1 year | 16 (25) | 13 (20) | 1.85 | 0.64 |
| 1 year–3 years | 18 (29) | 17 (27) | 1.59 | 0.53 |
| More than 3 years | 27 (43) | 31 (48) | 1.31 | 0.78 |
| Length of work at current site | ||||
| Less than 6 months | 6 (10) | 7 (11) | 1 | |
| 6 months–1 year | 23 (37) | 19 (30) | 1.41 | 0.93 |
| 1 year–3 years | 17 (27) | 21 (33) | 0.94 | 0.59 |
| More than 3 years | 17 (27) | 17 (27) | 1.17 | 0.81 |
| Engaged | Non-Engaged | |||||
|---|---|---|---|---|---|---|
| Statement | Agree (%) | Undecided (%) | Disagree (%) | Agree (%) | Undecided (%) | Disagree (%) |
| Perceived susceptibility questions | ||||||
| TB is very contagious | 48 (75) | 6 (9) | 10 (16) | 41 (64) | 12 (19) | 11 (17) |
| Traditional healers can protect me from evil spirits including TB | 11 (17) | 5 (8) | 48 (75) | 9 (14) | 7 (11) | 48 (75) |
| Someone who is young and healthy can have TB | 46 (72) | 9 (14) | 9 (14) | 55 (86) | 3 (5) | 6 (9) |
| TB is a danger to me because of my work | 49 (77) | 9 (14) | 6 (9) | 54 (84) | 3 (5) | 7 (11) |
| Perceived severity questions | ||||||
| TB is more serious than most other diseases | 57 (89) | 3 (5) | 4 (6) | 52 (81) | 4 (6) | 8 (13) |
| TB can kill me | 61 (95) | 3 (5) | 0 (0) | 54 (84) | 4 (6) | 6 (9) |
| If I have TB, I cannot work | 53 (83) | 0 (0) | 11 (17) | 39 (61) | 5 (8) | 20 (31) |
| Perceived barriers questions | ||||||
| If you talk to the community health workers, everyone will think you have TB | 16 (25) | 10 (16) | 38 (59) | 21 (33) | 15 (23) | 28 (44) |
| Submitting sputum is embarrassing | 22 (34) | 1 (2) | 41 (64) | 20 (31) | 0 (0) | 44 (69) |
| Getting a TB test result is scary | 25 (39) | 0 (0) | 39 (61) | 14 (22) | 2 (3) | 48 (75) |
| If I have TB I might also have HIV | 37 (59) | 12 (19) | 14 (22) | 44 (69) | 7 (11) | 13 (20) |
| I cannot get to the health center–it is too far from the camp site | 28 (44) | 1 (2) | 35 (55) | 27 (42) | 2 (3) | 35 (55) |
| I would not want others to know that I have TB | 41 (64) | 1 (2) | 22 (34) | 23 (36) | 3 (5) | 38 (59) |
| If I have TB, I will get fired from my job | 23 (36) | 3 (5) | 38 (59) | 33 (52) | 3 (5) | 28 (44) |
| Perceived benefits questions | ||||||
| TB medicines can cure TB | 59 (92) | 5 (8) | 0 (0) | 55 (86) | 3 (5) | 6 (9) |
| TB medication will help someone with TB to be stronger and continue to work | 60 (94) | 4 (6) | 0 (0) | 52 (81) | 6 (9) | 6 (9) |
| If I have TB I can get regular checkups | 61 (95) | 0 (0) | 3 (5) | 56 (88) | 3 (5) | 5 (8) |
| It is important to tell others in my community about TB | 57 (89) | 0 (0) | 7 (11) | 58 (91) | 1 (2) | 5 (8) |
| It is important to tell others to seek medical help if I think they have TB | 60 (94) | 3 (5) | 1 (2) | 61 (95) | 1 (2) | 2 (3) |
| It is important to get tested for HIV | 61 (95) | 3 (5) | 0 (0) | 60 (94) | 0 (0) | 4 (6) |
| If I have HIV, I can get medications and live a healthy life | 59 (92) | 3 (5) | 2 (3) | 58 (91) | 2 (3) | 4 (6) |
| Score | Threshold for Agreement | Engaged Mean Score (Sd) | Non-Engaged Mean Score (Sd) | p-Value |
|---|---|---|---|---|
| Perceived susceptibility | 8 | 9.8 (1.2) | 9.9 (1.5) | 0.45 |
| Perceived severity | 6 | 8.4 (1.2) | 7.7 (1.6) | 0.01 |
| Perceived barriers | 14 | 13.4 (2.5) | 13.2 (3.0) | 0.62 |
| Perceived benefits | 14 | 20.3 (1.4) | 19.8 (1.94) | 0.07 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Khaji, R.A.; Kabwebwe, V.M.; Mringo, A.G.; Nkwabi, T.F.; Bigio, J.; Mergenthaler, C.; Aguilera Vasquez, N.; Pande, T.; Rahman, M.T.; Haraka, F. Factors Affecting Motivation among Key Populations to Engage with Tuberculosis Screening and Testing Services in Northwest Tanzania: A Mixed-Methods Analysis. Int. J. Environ. Res. Public Health 2021, 18, 9654. https://doi.org/10.3390/ijerph18189654
Khaji RA, Kabwebwe VM, Mringo AG, Nkwabi TF, Bigio J, Mergenthaler C, Aguilera Vasquez N, Pande T, Rahman MT, Haraka F. Factors Affecting Motivation among Key Populations to Engage with Tuberculosis Screening and Testing Services in Northwest Tanzania: A Mixed-Methods Analysis. International Journal of Environmental Research and Public Health. 2021; 18(18):9654. https://doi.org/10.3390/ijerph18189654
Chicago/Turabian StyleKhaji, Rabia Abeid, Venance Muzuka Kabwebwe, Annasia Goodluck Mringo, Thomas Faustine Nkwabi, Jacob Bigio, Christina Mergenthaler, Nathaly Aguilera Vasquez, Tripti Pande, Md Toufiq Rahman, and Fredrick Haraka. 2021. "Factors Affecting Motivation among Key Populations to Engage with Tuberculosis Screening and Testing Services in Northwest Tanzania: A Mixed-Methods Analysis" International Journal of Environmental Research and Public Health 18, no. 18: 9654. https://doi.org/10.3390/ijerph18189654
APA StyleKhaji, R. A., Kabwebwe, V. M., Mringo, A. G., Nkwabi, T. F., Bigio, J., Mergenthaler, C., Aguilera Vasquez, N., Pande, T., Rahman, M. T., & Haraka, F. (2021). Factors Affecting Motivation among Key Populations to Engage with Tuberculosis Screening and Testing Services in Northwest Tanzania: A Mixed-Methods Analysis. International Journal of Environmental Research and Public Health, 18(18), 9654. https://doi.org/10.3390/ijerph18189654