
Immediate Effects of Acupuncture on Explosive Force Production and Stiffness in Male Knee Joint



Abstract
1. Introduction
2. Materials and Methods
2.1. Subjects
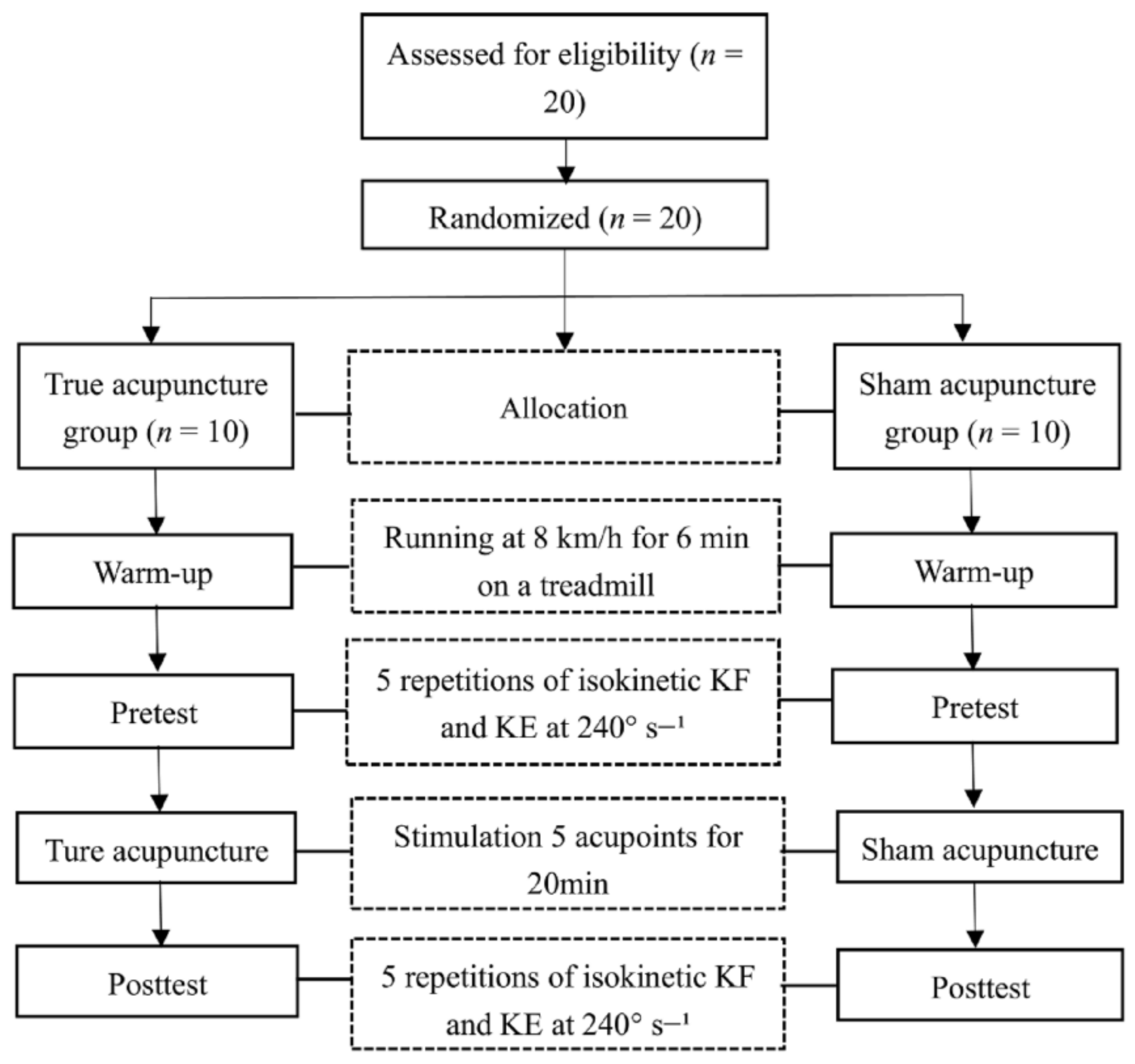
2.2. Study Design and Protocol
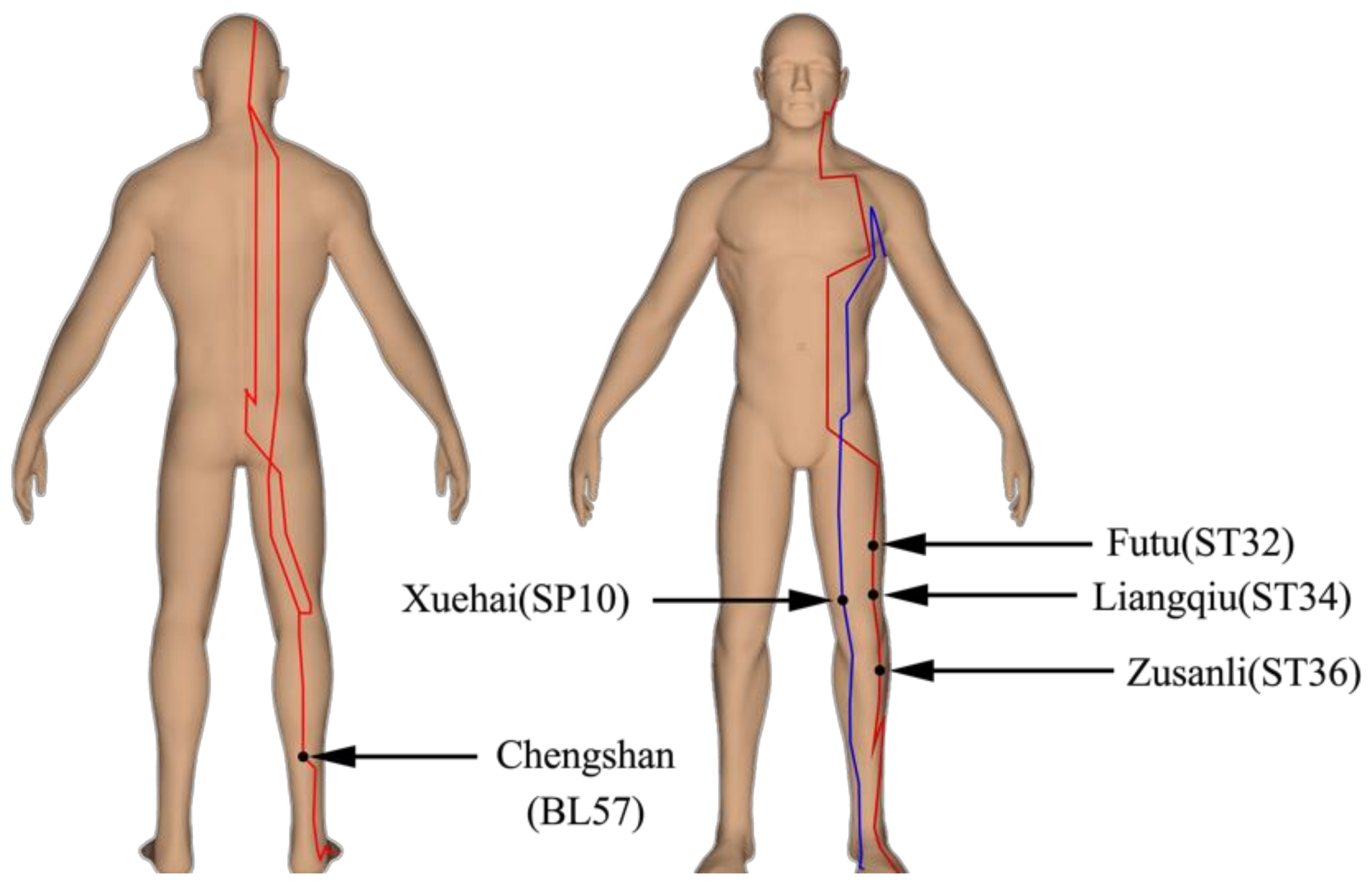
2.3. True Acupuncture and Sham Acupuncture Intervention
2.4. Measurement of Isokinetic Parameters
2.5. Reasons for Acupoints Selection
2.6. Data Analysis
2.7. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Tedesco, D.; Gori, D.; Desai, K.R.; Asch, S.; Carroll, I.R.; Curtin, C.; McDonald, K.M.; Fantini, M.P.; Hernandez-Boussard, T. Drug-free interventions to reduce pain or opioid consumption after total knee arthroplasty: A systematic review and meta-analysis. JAMA Surg. 2017, 152, e172872. [Google Scholar] [CrossRef]
- Hopton, A.; Curnoe, S.; Kanaan, M.; MacPherson, H. Acupuncture in practice: Mapping the providers, the patients and the settings in a national cross-sectional survey. BMJ Open 2012, 2. [Google Scholar] [CrossRef]
- Liu, S.Y.; Hsieh, C.L.; Wei, T.S.; Liu, P.T.; Chang, Y.J.; Li, T.C. Acupuncture stimulation improves balance function in stroke patients: A single-blinded controlled, randomized study. Am. J. Chin. Med. 2009, 37, 483–494. [Google Scholar] [CrossRef] [PubMed]
- Mikashima, Y.; Takagi, T.; Tomatsu, T.; Horikoshi, M.; Ikari, K.; Momohara, S. Efficacy of acupuncture during post-acute phase of rehabilitation after total knee arthroplasty. J. Tradit. Chin. Med. 2012, 32, 545–548. [Google Scholar] [CrossRef][Green Version]
- Hochberg, M.C.; Altman, R.D.; April, K.T.; Benkhalti, M.; Guyatt, G.; McGowan, J.; Towheed, T.; Welch, V.; Wells, G.; Tugwell, P. American College of Rheumatology 2012 recommendations for the use of nonpharmacologic and pharmacologic therapies in osteoarthritis of the hand, hip, and knee. Arthritis Care Res. (Hoboken) 2012, 64, 465–474. [Google Scholar] [CrossRef] [PubMed]
- Liu, Y.-H.; Wei, I.-P.; Wang, T.-M.; Lu, T.-W.; Lin, J.-G. Immediate effects of acupuncture treatment on intra-and inter-limb contributions to body support during gait in patients with bilateral medial knee osteoarthritis. Am. J. Chin. Med. 2017, 45, 23–35. [Google Scholar] [CrossRef]
- Hübscher, M.; Vogt, L.; Ziebart, T.; Banzer, W. Immediate effects of acupuncture on strength performance: A randomized, controlled crossover trial. Eur. J. Appl. Physiol. 2010, 110, 353–358. [Google Scholar] [CrossRef]
- Baudry, S.; Duchateau, J. Postactivation potentiation in a human muscle: Effect on the rate of torque development of tetanic and voluntary isometric contractions. J. Appl. Physiol. 2007, 102, 1394–1401. [Google Scholar] [CrossRef]
- Hamada, T.; Sale, D.G.; MacDougall, J.D.; Tarnopolsky, M.A. Postactivation potentiation, fiber type, and twitch contraction time in human knee extensor muscles. J. Appl. Physiol. 2000. [Google Scholar] [CrossRef]
- Mcbride, J.M.; Nimphius, S.; Erickson, T.M. The acute effects of heavy-load squats and loaded countermovement jumps on sprint performance. J. Strength Cond. Res. 2005, 19, 893–897. [Google Scholar]
- Turner, A.P.; Bellhouse, S.; Kilduff, L.P.; Russell, M. Postactivation potentiation of sprint acceleration performance using plyometric exercise. J. Strength Cond. Res. 2015, 29, 343–350. [Google Scholar] [CrossRef] [PubMed]
- Tillin, N.A.; Bishop, D. Factors modulating post-activation potentiation and its effect on performance of subsequent explosive activities. Sports Med. 2009, 39, 147–166. [Google Scholar] [CrossRef] [PubMed]
- Yang, X.-Y.; Shi, G.-X.; Li, Q.-Q.; Zhang, Z.-H.; Xu, Q.; Liu, C.-Z. Characterization of Deqi Sensation and Acupuncture Effect. Evid. Based Complementary Altern. Med. 2013, 2013, 319734. [Google Scholar] [CrossRef]
- Hui, K.K.; Nixon, E.E.; Vangel, M.G.; Liu, J.; Marina, O.; Napadow, V.; Hodge, S.M.; Rosen, B.R.; Makris, N.; Kennedy, D.N. Characterization of the" deqi" response in acupuncture. BMC Complement. Altern. Med. 2007, 7, 33. [Google Scholar] [CrossRef]
- Bai, L.; Cui, F.; Zou, Y.; Lao, L. Acupuncture de qi in stable somatosensory stroke patients: Relations with effective brain network for motor recovery. Evid.-Based Complementary Altern. Med. 2013, 2013, 9. [Google Scholar] [CrossRef]
- Kagitani, F.; Uchida, S.; Hotta, H. Afferent nerve fibers and acupuncture. J. Auton. Nerv. Syst. 2010, 157, 2–8. [Google Scholar] [CrossRef]
- Tsimachidis, C.; Patikas, D.; Galazoulas, C.; Bassa, E.; Kotzamanidis, C. The post-activation potentiation effect on sprint performance after combined resistance/sprint training in junior basketball players. J. Sports Sci. 2013, 31, 1117–1124. [Google Scholar] [CrossRef]
- Wang, I.-L.; Chen, Y.-M.; Wang, J.; Hu, R.; Zhang, K.-K.; Ho, C.-S. Effects of Acupuncture on Explosive Force Production by the Healthy Female Shoulder Joint. Evid. Based Complementary Altern. Med. 2020, 2020. [Google Scholar] [CrossRef] [PubMed]
- Folland, J.; Buckthorpe, M.; Hannah, R. Human capacity for explosive force production: Neural and contractile determinants. Scand. J. Med. Sci. Sports 2014, 24, 894–906. [Google Scholar] [CrossRef] [PubMed]
- Johnson, S.T.; Kipp, K.; Norcross, M.F.; Hoffman, M.A. Spinal and supraspinal motor control predictors of rate of torque development. Scand. J. Med. Sci. Sports 2015, 25, 623–629. [Google Scholar] [CrossRef] [PubMed]
- Fragoso, A.P.S.; Ferreira, A.S. Immediate effects of acupuncture on biceps brachii muscle function in healthy and post-stroke subjects. Chin. Med. 2012, 7, 1–9. [Google Scholar] [CrossRef]
- Brentano, M.A.; Pinto, R.S. Adaptações neurais ao treinamento de força. Rev. Bras. Ativ. Física Saúde 2001, 6, 65–77. [Google Scholar]
- Mucha, D.; Ambroży, T.; Mucha, D. The effect of acupressure stimulation of ST-36–Zusanli, point on lower limbs explosive strength. Eur. J. Integr. Med. 2017, 11, 59–62. [Google Scholar] [CrossRef]
- Fan, Y.-z.; Gong, L.; Yan, J.-t.; Fang, M.; Sun, W.-q.; Wu, Y.-c. Clinical observation on treatment of knee osteoarthritis by acupuncture and tuina therapy. J. Acupunct. Tuina Sci. 2010, 8, 390–393. [Google Scholar] [CrossRef]
- Hannah, R.; Folland, J.P. Muscle-tendon unit stiffness does not independently affect voluntary explosive force production or muscle intrinsic contractile properties. Appl. Physiol. Nutr. Metab. 2015, 40, 87–95. [Google Scholar] [CrossRef]
- Tillin, N.A.; Jimenez-Reyes, P.; Pain, M.T.; Folland, J.P. Neuromuscular performance of explosive power athletes versus untrained individuals. Med. Sci. Sports Exerc. 2010, 42, 781–790. [Google Scholar] [CrossRef] [PubMed]
- Mikkola, J.S.; Rusko, H.K.; Nummela, A.T.; Paavolainen, L.M.; Häkkinen, K. Concurrent endurance and explosive type strength training increases activation and fast force production of leg extensor muscles in endurance athletes. J. Strength Cond. Res. 2007, 21, 613. [Google Scholar]
- Gorostiaga, E.; Izquierdo, M.; Ruesta, M.; Iribarren, J.; Gonzalez-Badillo, J.; Ibanez, J. Strength training effects on physical performance and serum hormones in young soccer players. Eur. J. Appl. Physiol. 2004, 91, 698–707. [Google Scholar] [CrossRef]
- Butler, R.J.; Crowell III, H.P.; Davis, I.M. Lower extremity stiffness: Implications for performance and injury. Clin. Biomech. (Bristol, Avon) 2003, 18, 511–517. [Google Scholar] [CrossRef]
- Huang, L.-P.; Zhou, S.; Ao, M.; Zhao, M.-L.; Zhang, L.-Q.; Cao, L.-J. Unilateral intramuscular needling can improve ankle dorsiflexor strength and muscle activation in both legs. J. Exerc. Sci. Fit. 2015, 13, 86–93. [Google Scholar] [CrossRef]
- Assefi, N.P.; Sherman, K.J.; Jacobsen, C.; Goldberg, J.; Smith, W.R.; Buchwald, D. A randomized clinical trial of acupuncture compared with sham acupuncture in fibromyalgia. Ann. Intern. Med. 2005, 143, 10–19. [Google Scholar] [CrossRef]
- de Carvalho, A.O.; Cabral, L.; Rubini, E. Acupuncture improves flexibility: Acute effect of acupuncture before a static stretch of hip adductors. Med. Acupunct. 2011, 23, 27–33. [Google Scholar] [CrossRef]
- Stival, R.S.M.; Cavalheiro, P.R.; Stasiak, C.; Galdino, D.T.; Hoekstra, B.E.; Schafranski, M.D. Acupuncture in fibromyalgia: A randomized, controlled study addressing the immediate pain response. Rev. Bras. Reumatol. Engl. Ed. 2014, 54, 431–436. [Google Scholar]
- Maioli, C.; Falciati, L.; Marangon, M.; Perini, S.; Losio, A. Short- and long-term modulation of upper limb motor-evoked potentials induced by acupuncture. Eur. J. Neurosci. 2006, 23, 1931–1938. [Google Scholar] [CrossRef] [PubMed]
- Connelly, D.M.; Vandervoort, A.A. Effects of isokinetic strength training on concentric and eccentric torque development in the ankle dorsiflexors of older adults. J. Gerontol. Ser. A: Biol. Sci. Med. Sci. 2000, 55, B465–B472. [Google Scholar] [CrossRef]
- Hodgson, M.; Docherty, D.; Robbins, D. Post-activation potentiation. Sports Med. 2005, 35, 585–595. [Google Scholar] [CrossRef]
- Farup, J.; Sørensen, H.J.T.J.o.S.; Research, C. Postactivation potentiation: Upper body force development changes after maximal force intervention. J. Strength Cond. Res. 2010, 24, 1874–1879. [Google Scholar] [CrossRef]
- Ozerkan, K.N.; Bayraktar, B.; Sahinkaya, T.; Goksu, O.C.; Yucesir, I.; Yildiz, S. Comparison of the effectiveness of the traditional acupuncture point, ST. 36 and Omura’s ST. 36 Point (True ST. 36) needling on the isokinetic knee extension & flexion strength of young soccer players. Acupunct. Electro-Ther. Res. 2007, 32, 71–79. [Google Scholar]
- Zhu, S.P.; Luo, L.; Zhang, L.; Shen, S.X.; Ren, X.X.; Guo, M.W.; Yang, J.M.; Shen, X.Y.; Xu, Y.S.; Ji, B.; et al. Acupuncture De-qi: From Characterization to Underlying Mechanism. Evid. Based Complementary Altern. Med. 2013, 2013, 518784. [Google Scholar] [CrossRef]
- Sun, Z.G.; Pi, Y.L.; Zhang, J.; Wang, M.; Zou, J.; Wu, W. Effect of acupuncture at ST36 on motor cortical excitation and inhibition. Brain Behav. 2019, 9, e01370. [Google Scholar] [CrossRef]
- Ahmedov, S.J.T.J.o.S.; Research, C. Ergogenic effect of acupuncture in sport and exercise: A brief review. J. Strength Cond. Res. 2010, 24, 1421–1427. [Google Scholar] [CrossRef] [PubMed]
- Spaeth, R.B.; Camhi, S.; Hashmi, J.A.; Vangel, M.; Wasan, A.D.; Edwards, R.R.; Gollub, R.L.; Kong, J. A longitudinal study of the reliability of acupuncture deqi sensations in knee osteoarthritis. Evid. Based Complementary Altern. Med. 2013, 2013, 12. [Google Scholar] [CrossRef] [PubMed]
- Scaglioni, G.; Ferri, A.; Minetti, A.E.; Martin, A.; Van Hoecke, J.; Capodaglio, P.; Sartorio, A.; Narici, M.V. Plantar flexor activation capacity and H reflex in older adults: Adaptations to strength training. J. Appl. Physiol. 2002, 92, 2292–2302. [Google Scholar] [CrossRef] [PubMed]
- Napadow, V.; Makris, N.; Liu, J.; Kettner, N.W.; Kwong, K.K.; Hui, K.K. Effects of electroacupuncture versus manual acupuncture on the human brain as measured by fMRI. Hum. Brain Mapp. 2005, 24, 193–205. [Google Scholar] [CrossRef]
- Fink, M.; Rollnik, J.D.; Bijak, M.; Borstädt, C.; Däuper, J.; Guergueltcheva, V.; Dengler, R.; Karst, M. Needle acupuncture in chronic poststroke leg spasticity. Arch. Phys. Med. Rehabil. 2004, 85, 667–672. [Google Scholar] [CrossRef] [PubMed]
- Dhaher, Y.Y.; Tsoumanis, A.D.; Houle, T.T.; Rymer, W.Z. Neuromuscular reflexes contribute to knee stiffness during valgus loading. J. Neurophysiol. 2005, 93, 2698–2709. [Google Scholar] [CrossRef] [PubMed]
- Fuglevand, A.J.; Winter, D.A.; Patla, A.E. Models of recruitment and rate coding organization in motor-unit pools. J. Neurophysiol. 1993, 70, 2470–2488. [Google Scholar] [CrossRef]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Characteristic | Treatment | Pre | Post | p Values | ||
|---|---|---|---|---|---|---|
| Main Effects (Time) | Main Effects (Group) | Interaction (Time × Group) | ||||
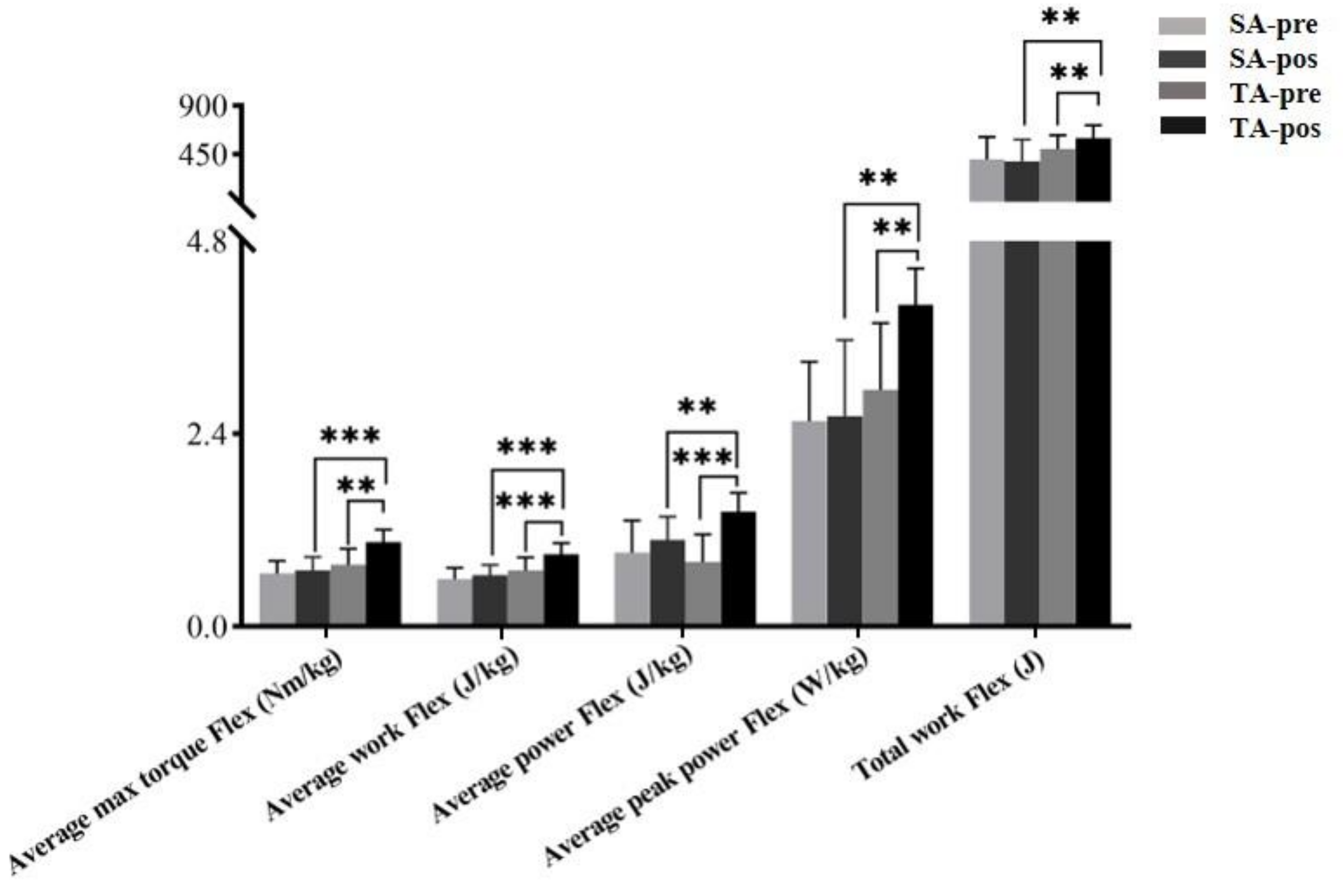
| Average max torque Flex/kg (Nm/kg) | SA | 0.66 ± 0.16 | 0.70 ± 0.17 | <0.001 | 0.004 | 0.002 * |
| TA | 0.77 ± 0.20 | 1.05 ± 0.16 | ||||
| Average work Flex/kg (J/kg) | SA | 0.58 ± 0.14 | 0.64 ± 0.13 | <0.001 | 0.005 | 0.008 * |
| TA | 0.71 ± 0.16 | 0.90 ± 0.14 | ||||
| Average power Flex/kg (J/kg) | SA | 0.92 ± 0.40 | 1.08 ± 0.29 | <0.001 | 0.365 | 0.008 * |
| TA | 0.80 ± 0.35 | 1.43 ± 0.24 | ||||
| Average peak power Flex/kg (W/kg) | SA | 2.56 ± 0.74 | 2.62 ± 0.95 | 0.015 | 0.024 | 0.027 * |
| TA | 2.95 ± 0.83 | 4.01 ± 0.45 | ||||
| Total work Flex/kg (J) | SA | 401.63 ± 212.40 | 384.41 ± 204.35 | 0.010 | 0.052 | 0.001 * |
| TA | 499.96 ± 129.86 | 600.44 ± 121.66 | ||||
| Stiffness Flex/kg (Nm/Kg*deg) | SA | 0.002 ± 0.002 | 0.001 ± 0.001 | 0.015 | <0.001 | 0.001 * |
| TA | 0.002 ± 0.001 | 0.004 ± 0.001 | ||||
| Characteristic | Treatment | Pre | Post | P values | ||
|---|---|---|---|---|---|---|
| Main Effects (Time) | Main Effects (Group) | Interaction (Time × Group) | ||||
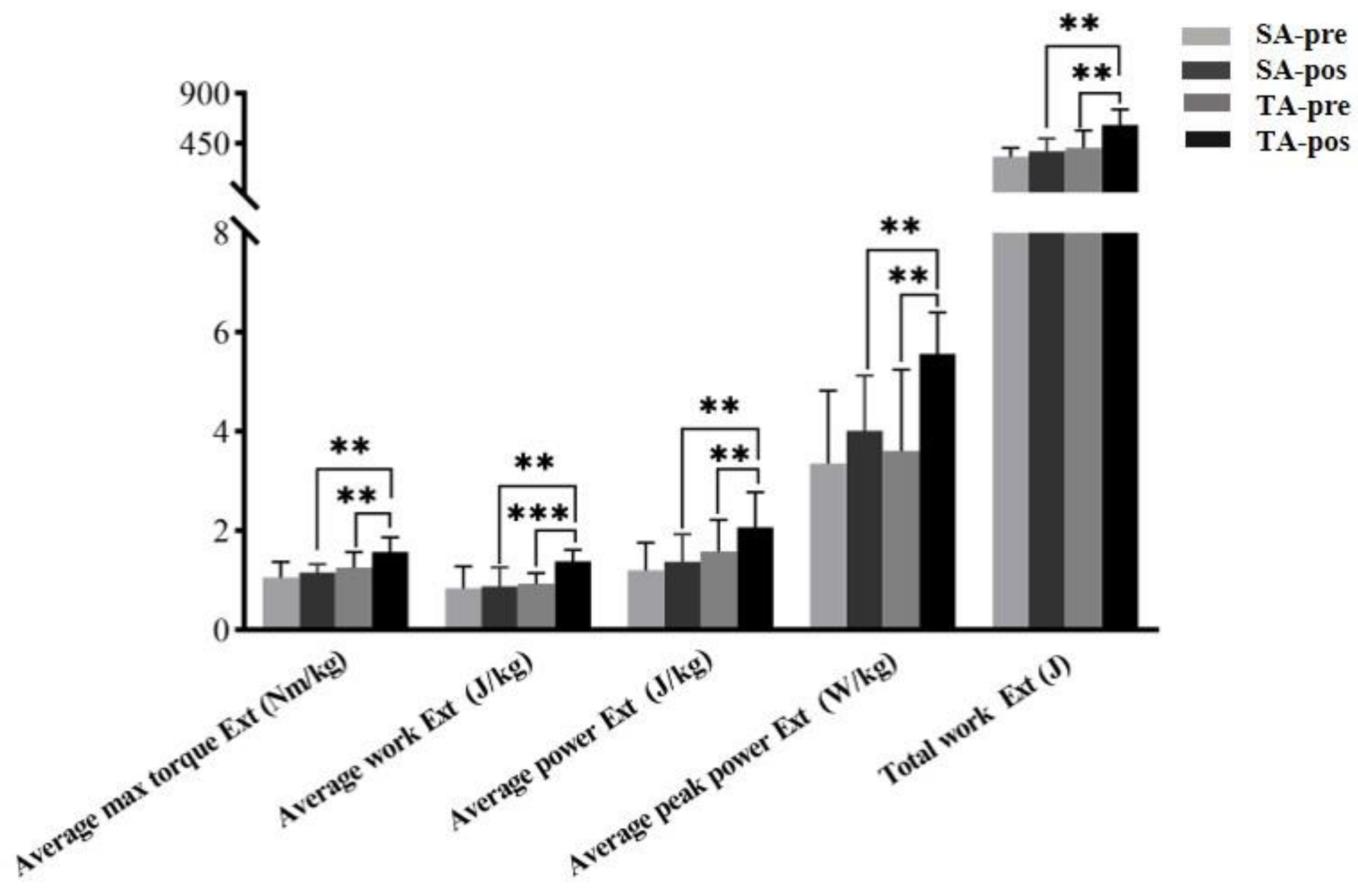
| Average max torque Ext/kg (Nm/kg) | SA | 1.06 ± 0.31 | 1.16 ± 0.22 | <0.001 | 0.020 | 0.027 * |
| TA | 1.26 ± 0.31 | 1.57 ± 0.30 | ||||
| Average work Ext/kg (J/kg) | SA | 0.84 ± 0.44 | 0.88 ± 0.39 | 0.019 | 0.025 | 0.043 * |
| TA | 0.93 ± 0.22 | 1.38 ± 0.24 | ||||
| Average power Ext/kg (J/kg) | SA | 1.20 ± 0.56 | 1.37 ± 0.56 | 0.002 | 0.041 | 0.013 * |
| TA | 1.58 ± 0.64 | 2.07 ± 0.71 | ||||
| Average peak power Ext/kg (W/kg) | SA | 3.63 ± 1.46 | 4.01 ± 1.12 | <0.001 | 0.178 | 0.008 * |
| TA | 3.61 ± 1.64 | 5.56 ± 0.84 | ||||
| Total work Ext/kg (J) | SA | 332.87 ± 78.60 | 378.72 ± 116.28 | <0.001 | 0.003 | 0.021 * |
| TA | 410.89 ± 158.12 | 617.70 ± 140.73 | ||||
| Stiffness Flex/kg (Nm/Kg*deg) | SA | 0.002 ± 0.002 | 0.002 ± 0.002 | 0.002 | <0.001 | <0.001 * |
| TA | 0.004 ± 0.002 | 0.007 ± 0.002 | ||||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Wang, J.; Wang, I.-L.; Hu, R.; Yao, S.; Su, Y.; Zhou, S.; Chen, C.-H. Immediate Effects of Acupuncture on Explosive Force Production and Stiffness in Male Knee Joint. Int. J. Environ. Res. Public Health 2021, 18, 9518. https://doi.org/10.3390/ijerph18189518
Wang J, Wang I-L, Hu R, Yao S, Su Y, Zhou S, Chen C-H. Immediate Effects of Acupuncture on Explosive Force Production and Stiffness in Male Knee Joint. International Journal of Environmental Research and Public Health. 2021; 18(18):9518. https://doi.org/10.3390/ijerph18189518
Chicago/Turabian StyleWang, Jun, I-Lin Wang, Rui Hu, Shun Yao, Yu Su, Shu Zhou, and Che-Hsiu Chen. 2021. "Immediate Effects of Acupuncture on Explosive Force Production and Stiffness in Male Knee Joint" International Journal of Environmental Research and Public Health 18, no. 18: 9518. https://doi.org/10.3390/ijerph18189518
APA StyleWang, J., Wang, I.-L., Hu, R., Yao, S., Su, Y., Zhou, S., & Chen, C.-H. (2021). Immediate Effects of Acupuncture on Explosive Force Production and Stiffness in Male Knee Joint. International Journal of Environmental Research and Public Health, 18(18), 9518. https://doi.org/10.3390/ijerph18189518