
Parkinson’s Disease and Deep Brain Stimulation Have an Impact on My Life: A Multimodal Study on the Experiences of Patients and Family Caregivers

Abstract
1. Introduction
2. Materials and Methods
2.1. Researcher Characteristics and Reflexivity
2.2. Recruitment and Collaborations
2.3. Study Population and Inclusion Criteria
2.4. Informed Consent Process
2.5. Data Collection
2.6. Data Analysis
2.7. Quality Assurance of Data
2.8. Ethical Concerns and Data Management
3. Results
3.1. Everyone’s Parkinson’s Is Different
3.1.1. Different Symptoms and Disease Progression
“I saw sand flowing from anywhere but in a closed circuit. It never stops (…) or I saw a black dog under the table at the hospital. There, I had a concentration of hallucinations from everyone. The doctors who came to see me at first that I was having these hallucinations, they had spaghetti hanging out”.(P44)
“Many people with Parkinson’s disease say that if they have psychological problems from the disease, either from or with or because of the disease, it is much worse than if they tremble and cannot walk well. And I think that too”.(P27)
“About 15 years ago, she made a mistake with our boat and hit a buoy at high speed. Then the water police came (…) She was trembling all over her body and I have never seen her like this. That frightened me very much and since then, it happens whenever she gets upset (…) When she is tense, she has such uncontrolled movements. I first noticed in 2004 that when she is very excited or scared or something, she trembles”.(FC13)
“In the beginning, I experienced the honeymoon, it went great, and the more the disease progressed, the more the uncontrolled movement I had. (…) I lost 10 kilos in half a year because I couldn’t sit quietly anymore”.(P9)
“This has changed a lot, the disease. That is quite clear. Then, as you can see with the disease, where dyskinesia became more and more pronounced, comes the physiognomy change. I no longer knew my own wife by her face. It was so bad, the disfigurement that was caused by this illness that affects not only the movements but also the face”.(FC22)
3.1.2. Different Perception of the Disease
“This is the life before and after the disease and then you learn to live with it. It is true that I have done a lot of research to find out where we were heading to (…) We were told that there are as many symptoms as there are sick people. And this is how it is”.(P41)
“I had the impression that Parkinson’s itself does not exist and that it is a sum of factors that are individual. Therefore, they are really not understood, and they are mentioned below the name of Parkinson’s (…) If there would be a better understanding of the whole mechanisms, one could finally say that there are many versions of Parkinson’s, which are entirely related”.(P1)
“I can just say that my attitude to life is like this, I fight as long as I can, but it’s just getting harder and harder. It’s really getting more and more difficult. (…) This disease is also very interesting in terms of what you forget when it changes again afterwards”.(P12)
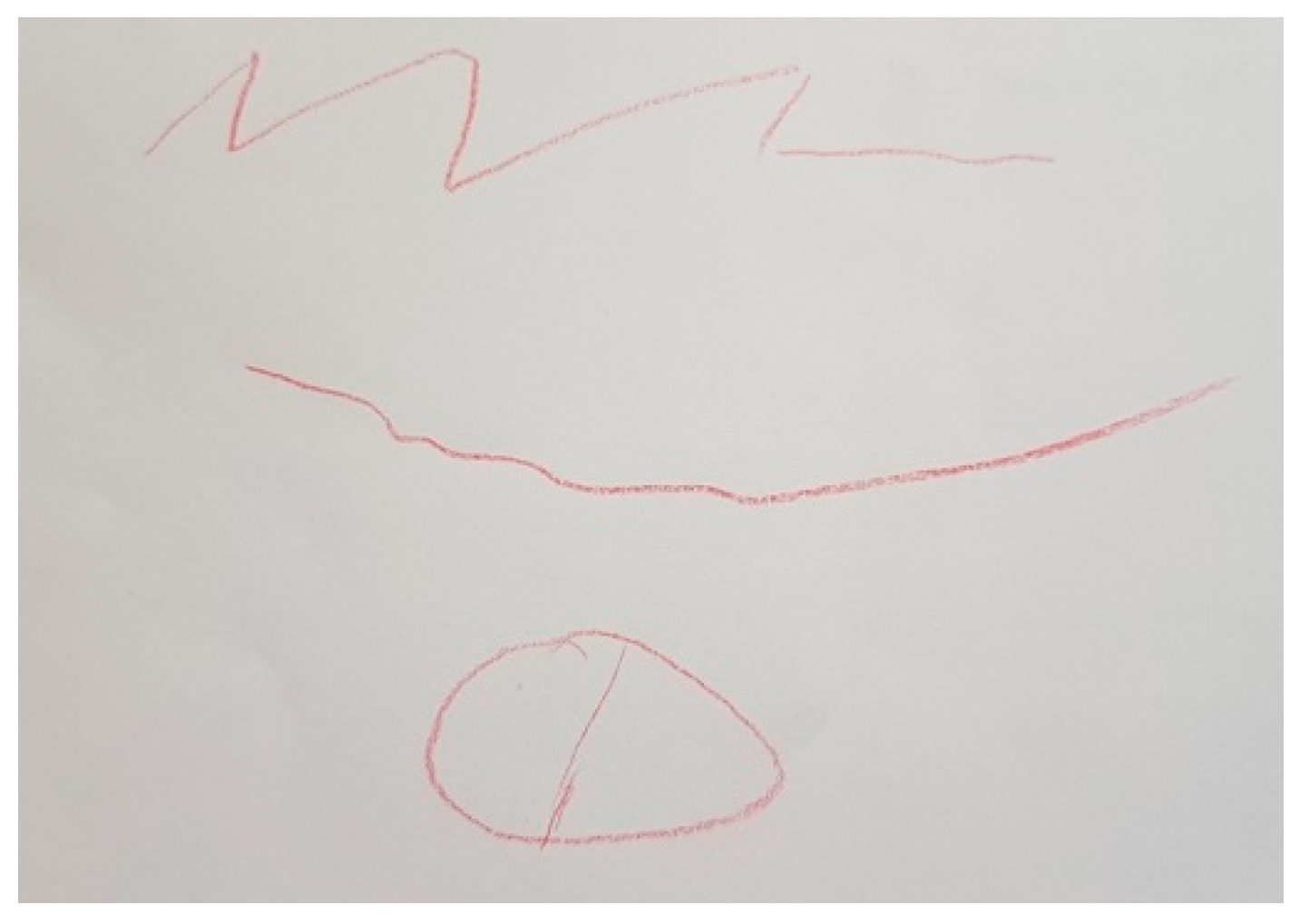
“What I drew is what concerns me the most and touches me negatively, which is the effect as if he would have a mask on his face (…). I always have to think when I talk to him or when I get in touch with him whether there’s something going on. He just looks glassy-eyed. It’s not that there’s something wrong or that something has happened (…) It is somehow difficult for him to express that he is there for the other person in an empathic way. And the connection is somehow interrupted. But maybe that has to do with me too. I react very personally”.(FC6)
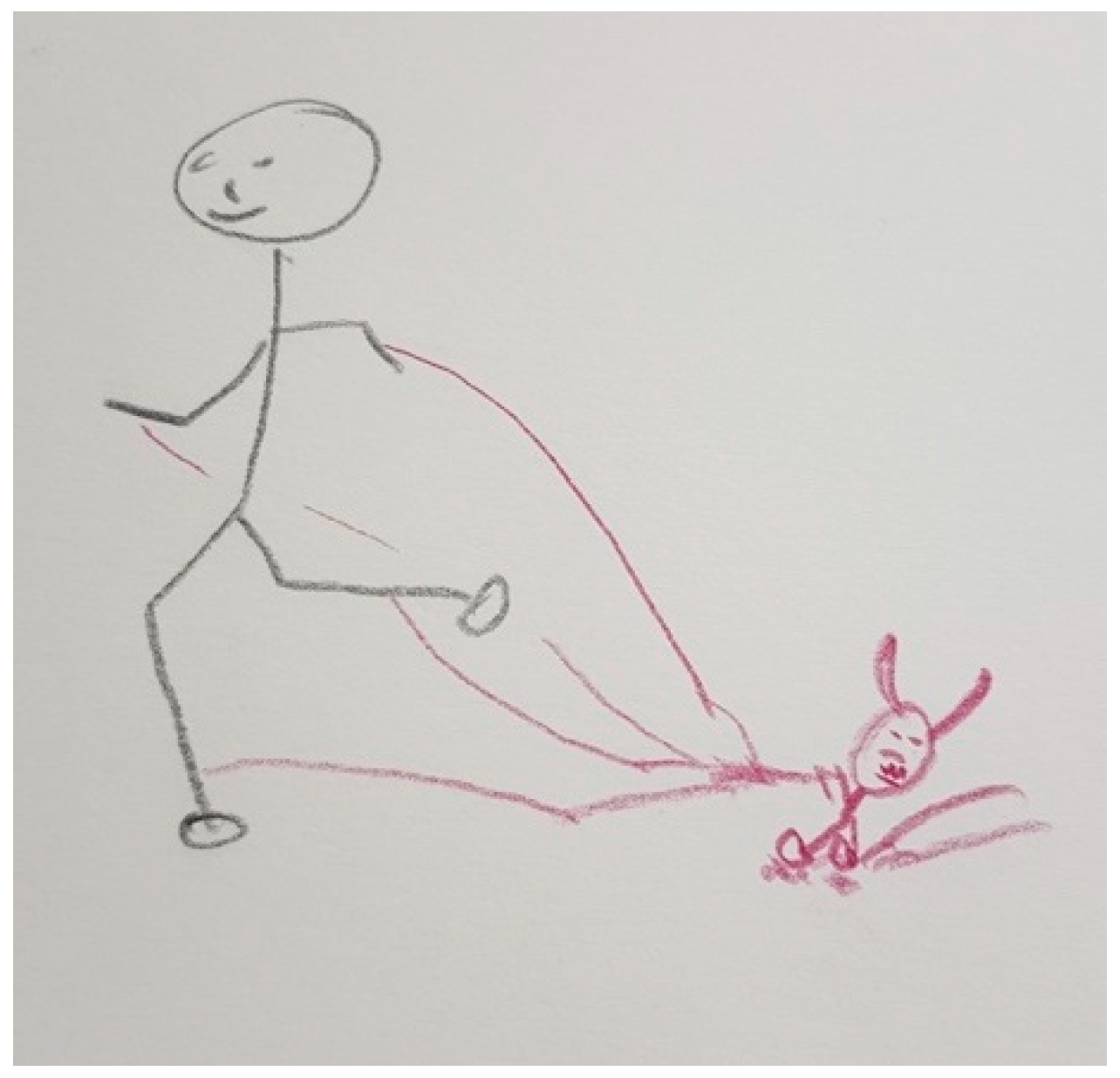
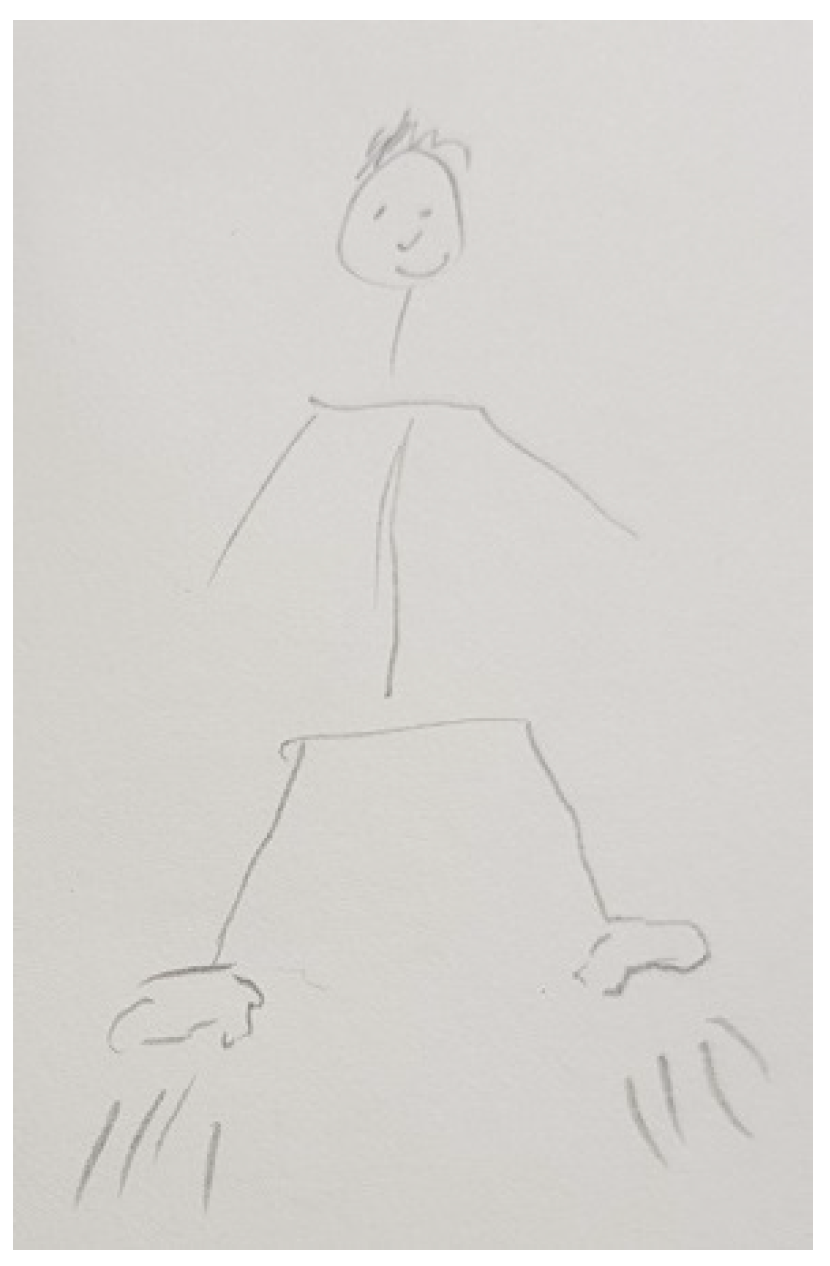
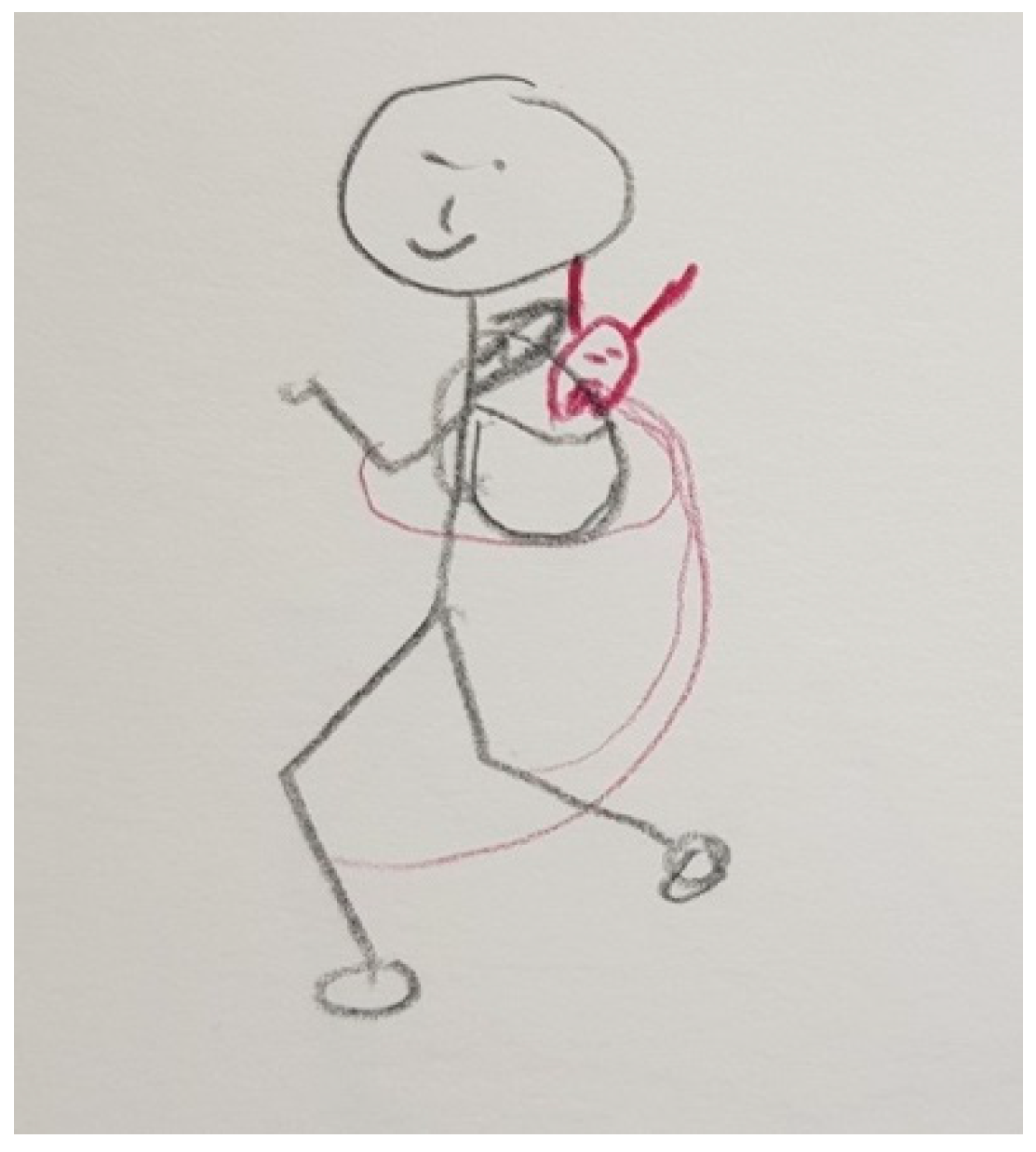
“That’s me. I have several ropes attached to my legs and arms and a little demon that holds me back. Then, my mobility is limited”.(P5)
“I think the disease itself is the devil on one side and the beautiful fairy on the other side. It is entirely day-dependent, time-dependent. Sometimes you could almost despair about the disease and other times, everything it’s quite normal and you can say to yourself that everyday life is actually quite normal. And then in the next half hour nothing works at all. What is also the problem is that we have to prepare every appointment very carefully”.(FC29)
“This is me, actually a satisfied person. And he has a shadow. And he doesn’t have an angry face, but he’s looking to see how I am (…) I’m actually happy when he stays behind me, when he doesn’t come in front of me (…) Whether I like it or not, he’s always there. I can’t turn him off”.(P35)
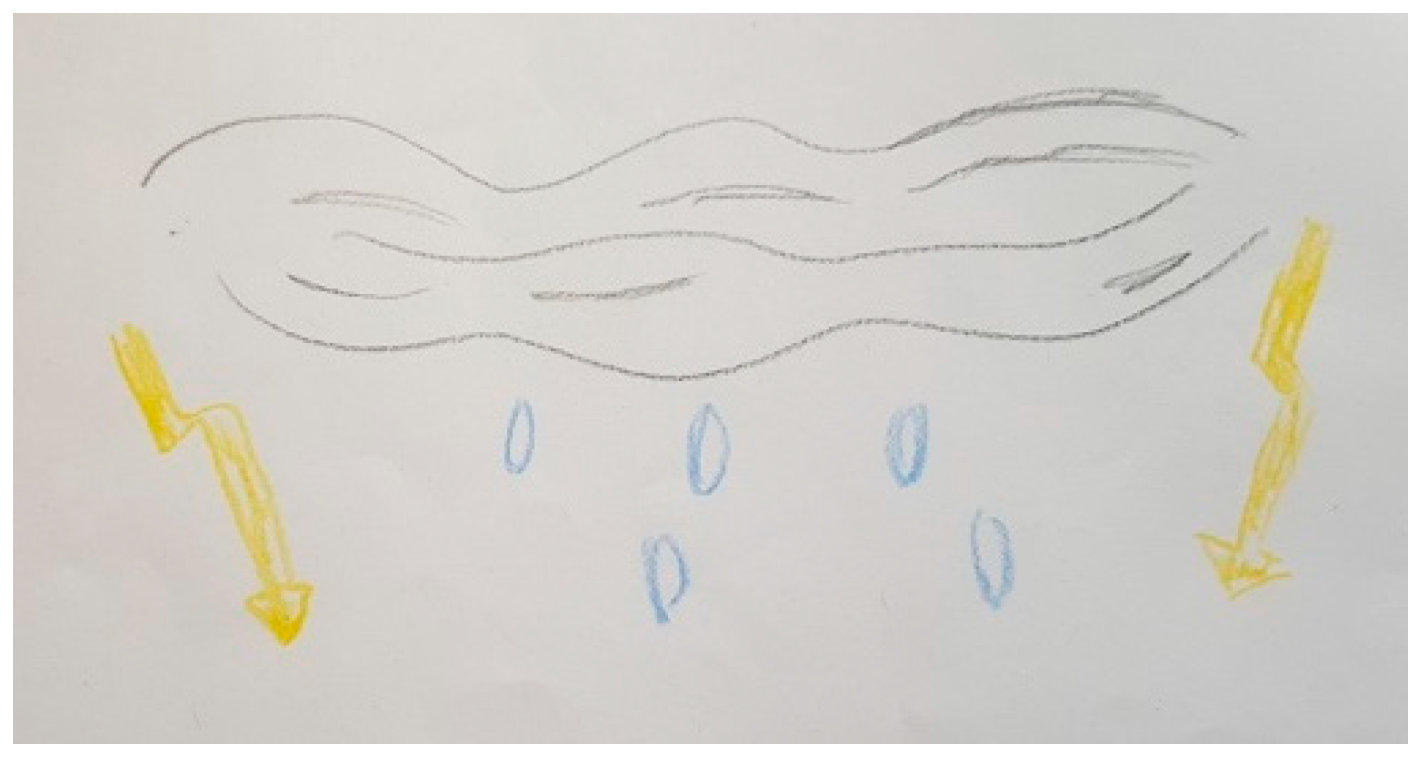
“It’s to explain the bad weather, the worst of the bad weather, for me. I was very active. I was really someone who was moving and all of sudden I had to stop because it was no longer possible, and my body wasn’t following”.(P40)
“It [PD] is autumn. Autumn. The leaves falling is not the end of life, but it’s the end of a life. It’s the end of the life before illness. So, it’s a time to mourn”.(FC41)
“There’s glue on your feet. You want to go somewhere, and you can’t. In your head you are already there, but your body cannot go there because your feet are sticky. The dopamine is missing”.(P21)
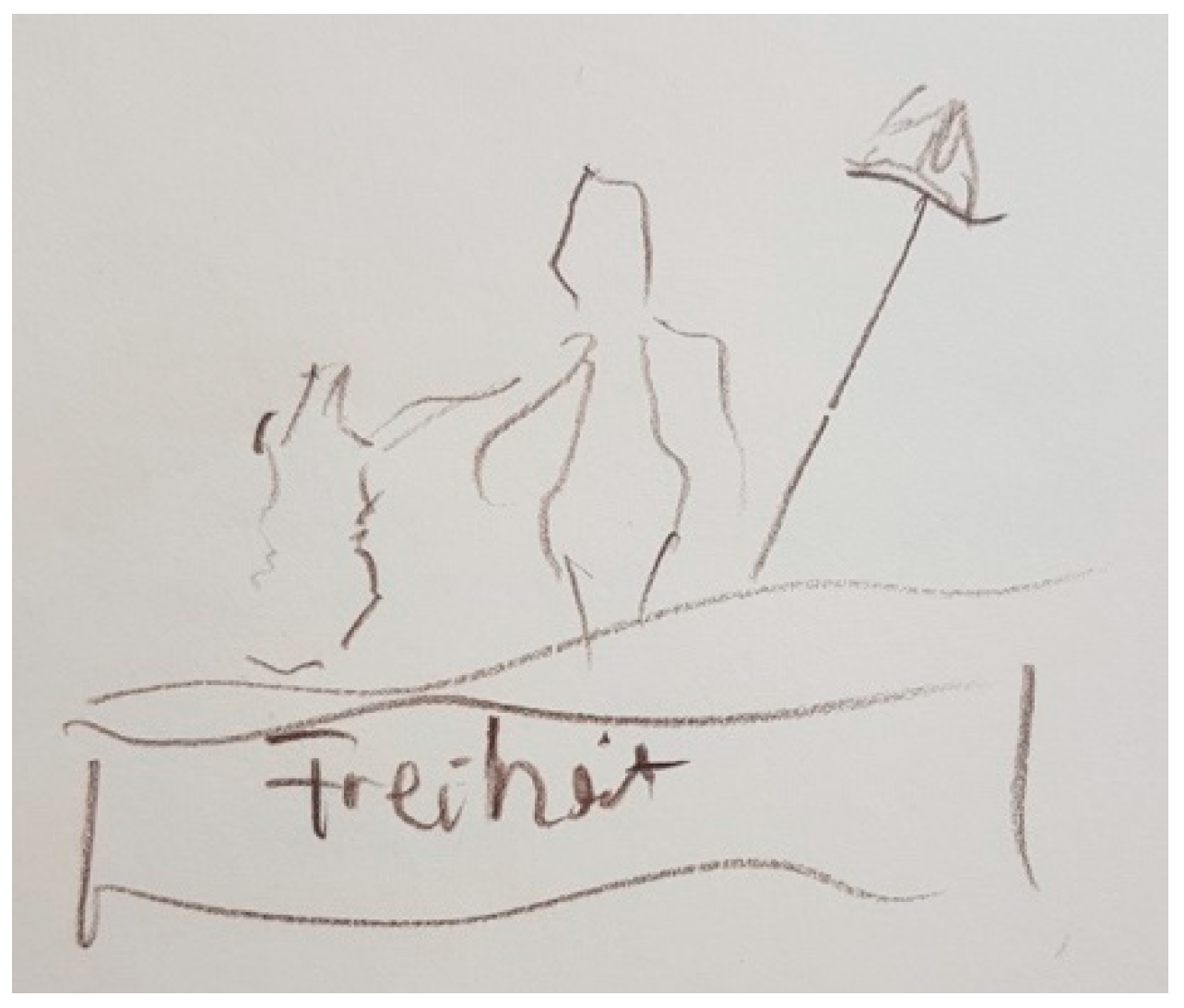
“This freedom, I don’t have it anymore, because I have Parkinson’s disease and I’ve lost my freedom. I find that very bad. I find it so sad (…) Now I simply have a good life, a good care, but I do not have freedom anymore”.(P8)
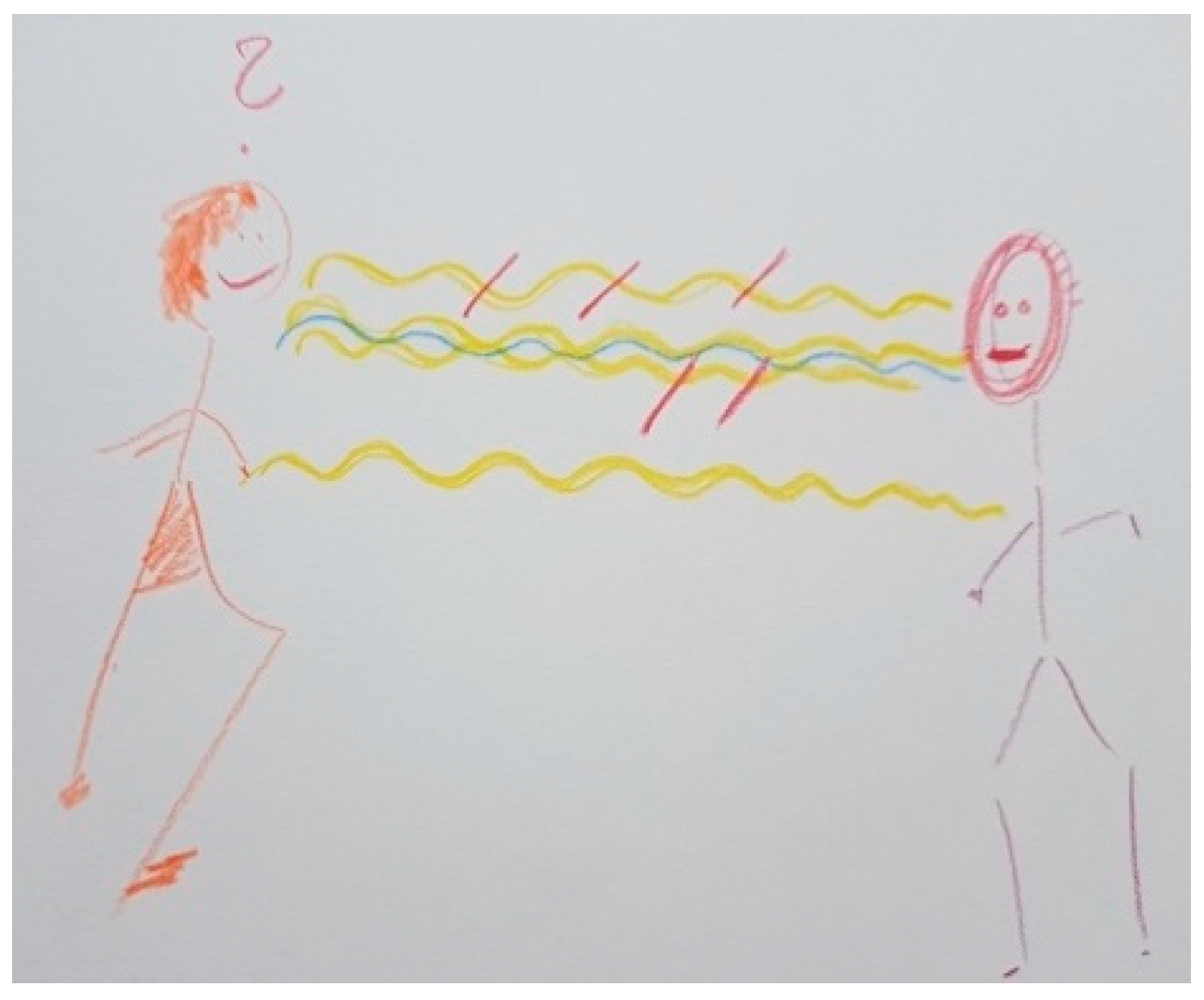
“Parkinson’s is like a cage for the person. The person is like in a cage for me and I can’t get into this cage”.(FC6)
3.1.3. Different Reaction to Drugs
“Our friends also noticed that he was so uninhibited and always restless. He always had to be stimulated and always had to listen to music. He also bought a lot of things like cars. He had a different behavior”.(FC2)
“The increased libido is a problem after all. People don’t talk about it so much, but it’s a side effect of the medication and it’s very demanding for the partner”.(P1)
“For example, when we were at the table with the children, he ate a lot and very quickly, and then stood up and went to his computer. And that’s difficult with children, when you try to educate the children and say: wait until everyone has finished and then you can get up and leave the table. And he, he had no concept of parenting anymore”.(FC2)
3.1.4. Different Difficulties and Changes That Led to Different Daily Routines
“People with Parkinson’s, they lose their sense of reality over time. For example, when she cooks something, it goes in slow motion. When I say: ‘can’t be done faster?’. She says: ‘yes, I do work fast’. Or also with movements, when people with Parkinson’s walk, it’s centimeter by centimeter and when you ask them about it and say: ‘why don’t you take bigger steps? It’s better’, she says: ‘yes, I do take big steps’. It’s as if reality slowly disappears”.(FC29)
“I feel sometimes pressured because I make an appointment for her somewhere and calculate how long we need to get her ready and to be there. And then when we leave, it can happen that nothing works until we get to the station because it takes us a quarter of an hour to walk ten meters and then the train bye”.(FC29)
“One loses independence and of course is somewhat limited. You’re glad to have someone by your side to help you up, for example, on the edge of the bed to get up”.(P9)
“What comes next? How much should I work? Should I take this job or better this one? (…) How will it go financially and how will it go later? How many years will it take before he needs care? What will I do then? Can I care for someone at all? I’m not the caring type of person. I noticed that a long time ago. Then I thought, oh my God, how do I do that then? It was always like a sword of Damocles hanging over you and you have to think, what’s next?”(FC6)
3.1.5. Different Impact on Familial and Couple Relationships and on Social Life
“Something changed, I don’t know (…) Over time he became more of a patient and I became more of a caregiver, but I wouldn’t say from the beginning. It was over time, when more and more symptoms appeared (…) The illness has a strong influence on communication, because he often speaks very softly, because he speaks unclearly. Now, in the last few months, he is increasingly unable to express himself so well. The words don’t come out or he no longer knows what he wants to say, and his range of interests is simply more limited”.(FC17)
“She does not want to talk about it [PD] (…) My wife is not understanding as others can be. It’s always like that, an illness, it always affects both the relatives and the affected persons themselves (P7) (…) Would you say that your relationship with your wife changed after the diagnosis? (Researcher 1). “Yes, yes. I think it has. Yes, yes. She can’t help like that either, can she? (…) There are some people who really still have complaints and I also have complaints, but those who can no longer walk or are really old people. And with such problems my wife simply has problems. She doesn’t want to see them at all”.(P7)
“In our wedding day, she told me that you were limping (…) And then I went to the doctor, first to the general doctor and then to the neurologist. The second wife, she asked for divorce. I actually understood that, because she had already known my mother and seen how it is (…) And my second wife couldn’t stand that”.(P8)
“It’s just that for many couples it’s a big challenge. I see many who are trembling, and it’s easy, it wouldn’t work anymore if the partner didn’t have more patience. It’s tragic to see how that hurts you. There are so many different people. There are people who deal with it better and others who deal with it worse. You know, my son is washed up with it because he’s always had Parkinson’s around him. He experienced the grandfather yes. He came from school, he had to find the grandfather somewhere, he had to put him up again and bring him into the house. Then he experienced his father for 30 years. And now his partner and that is a lot for him at the moment and I think that often he just doesn’t have the energy anymore (…) She was very unwell before the operation and I just felt she had a nervous breakdown (…) I just notice that when she gets stressed, it comes through, and she needs another day [to recover]. And my son is allergic to it. He just almost can’t stand it. He didn’t want to be there today” (FC24). “Can I ask why?” (R1). “Something kind of broke” (FC24). “In the relationship you mean?” (R1). “Unfortunately. That hurts me a lot”.(FC24)
“At one point he was quite affected, and I asked him the question. I said, but what’s wrong? Then he looked to me in the eye and said: are you going to die daddy? I said no, but no, but no! It had nothing to do with it. In fact we hadn’t explained it to him because we thought we were protecting him and then we realized that he was still worried about it”.(P40)
“It’s quite difficult, it depends. My wife doesn’t have a problem, but she understands everything. She has given herself body and soul for me. But the children are not the same at all. It has changed (…) let’s just say that they don’t understand so much that you’re sick”.(P44)
“I didn’t want to show others this image of me, this image of the disease in fact” (P40). “So you didn’t go out anymore?” (R2). “Very little (…) I have the impression that some people think that we are not the same because we are sick. I think there are many who think that because maybe I’m a little slower, I have more difficulty in talking, that inside we’re not the same, whereas inside, when I think, I think very quickly”.(P40)
3.1.6. Different Personal Coping Strategies
“In fact, I preferred not to know anything (…) I told myself that if I didn’t know anything, I wouldn’t have symptoms that could happen later”.(P40)
“That is also the purpose of this self-help group, because people meet there who know what it means to have experienced this operation, but also what it means to have survived it. And what it means when other people think you are healthy again”.(P12)
“In my opinion, too much is said about the sick person in our self-help group and not about oneself in the relatives’ group. So, I always bring that up there (…) I ask: ‘how are you doing’ and now they are starting to talk a bit more about themselves. (…) It helps to talk to people who have similar experiences. So, it’s also like not being alone. Talking about it with other people is always a bit difficult if they judge how it should be (…) But with those who have the same experiences, you only say I do it this way or I do it differently. And, um, yes, you also have to look after yourself”.(FC17)
“He had the impression that we were seeing something [PD symptoms], when it wasn’t at all (…) But he could see that, and he had the impression that everyone was paying attention to it. So, he didn’t want to talk about it too much, and I was the opposite. For me, to talk about it was a way of trivializing this illness. It was like saying I have the flu, yes, he has Parkinson’s, and then there you go. Then I talked a lot about it. It’s true, I pushed him to do it because it’s not keeping things inside that’s going to help”.(FC41)
3.2. Going through PD Together
“I do everything for my partner. Doctor talks, everything, and I’m there and I want to know what’s being done and yes. That’s everything for me. And that’s why, we manage, we do everything. It works”.(FC14)
“I think I wouldn’t have made it without her”(P44)
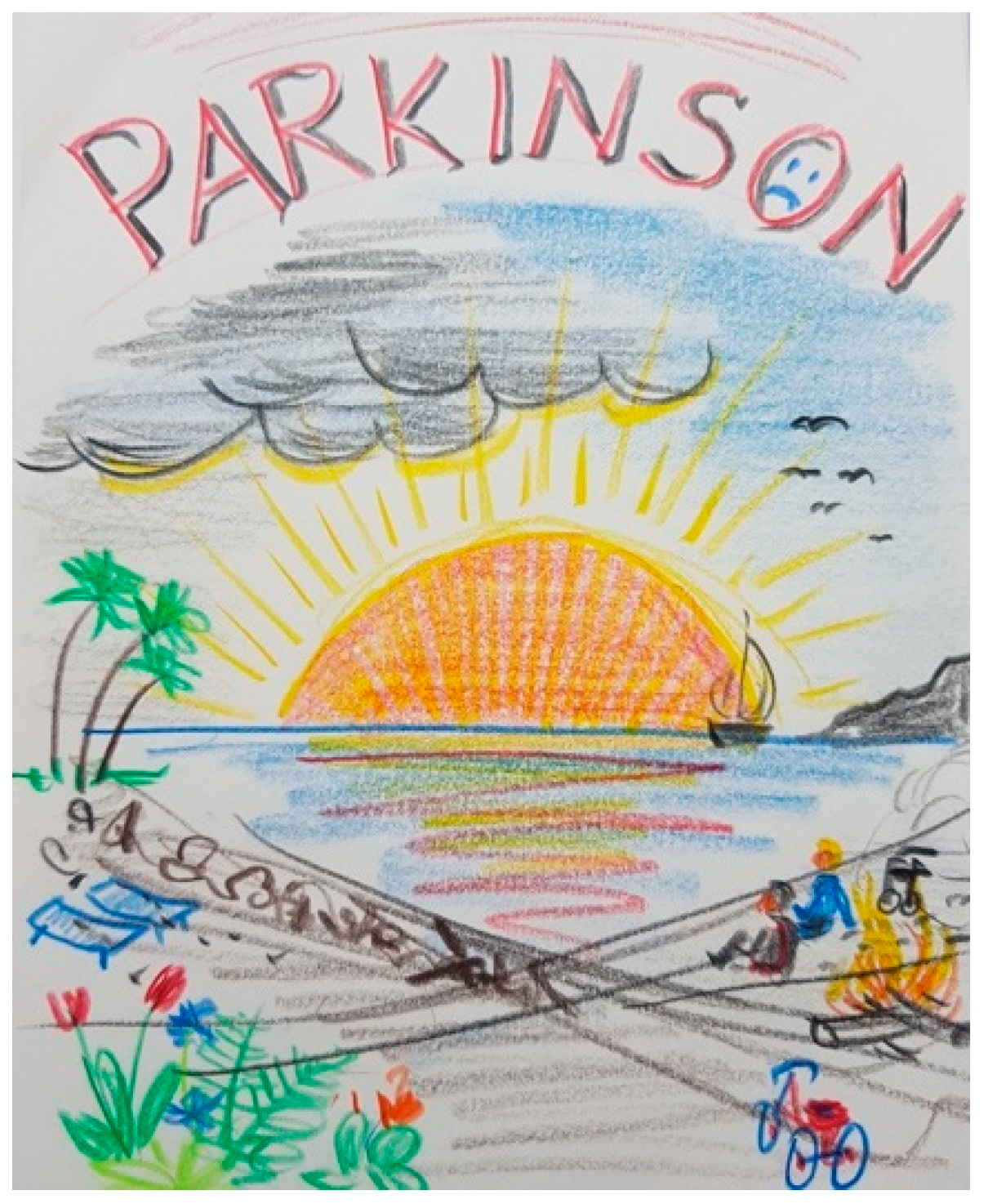
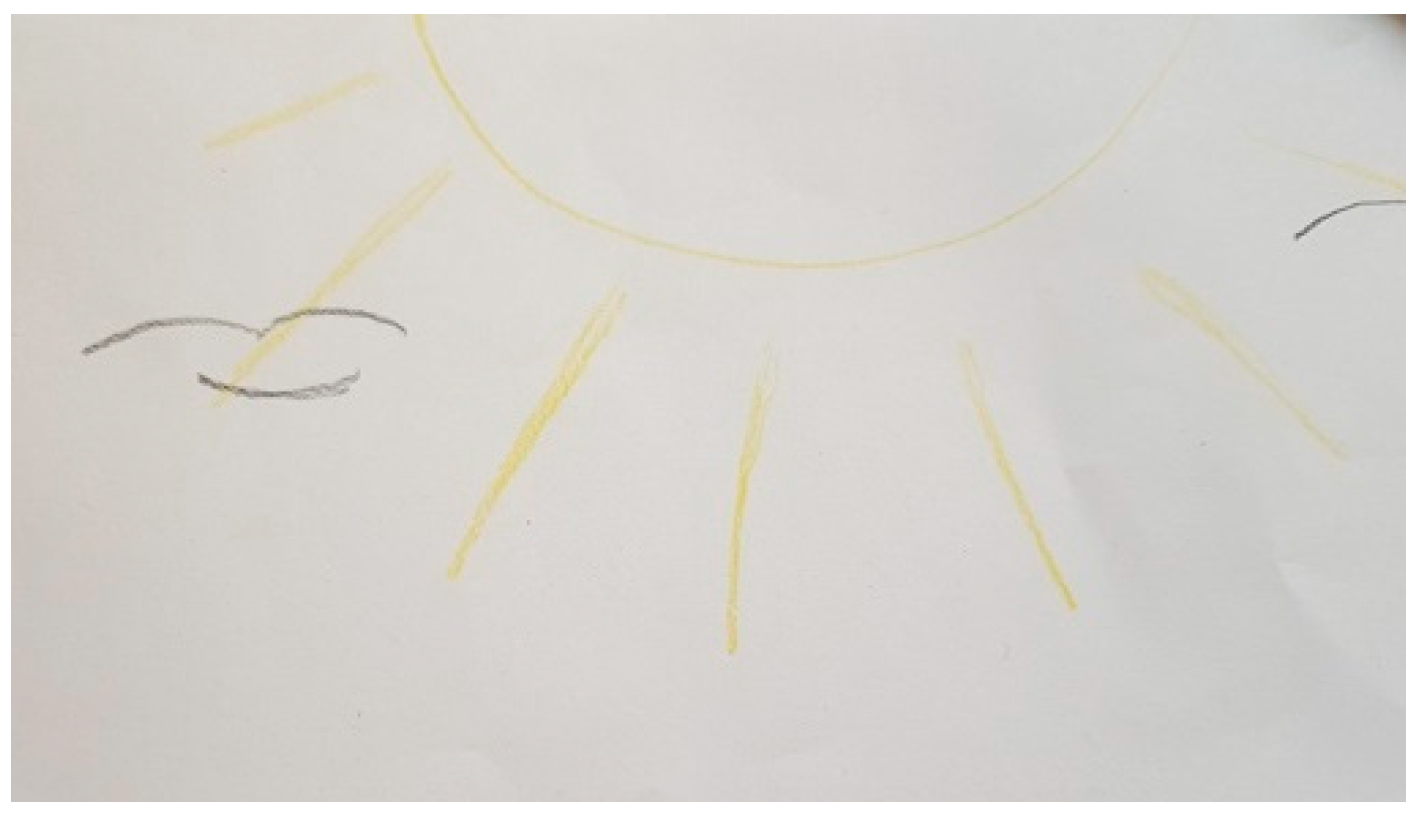
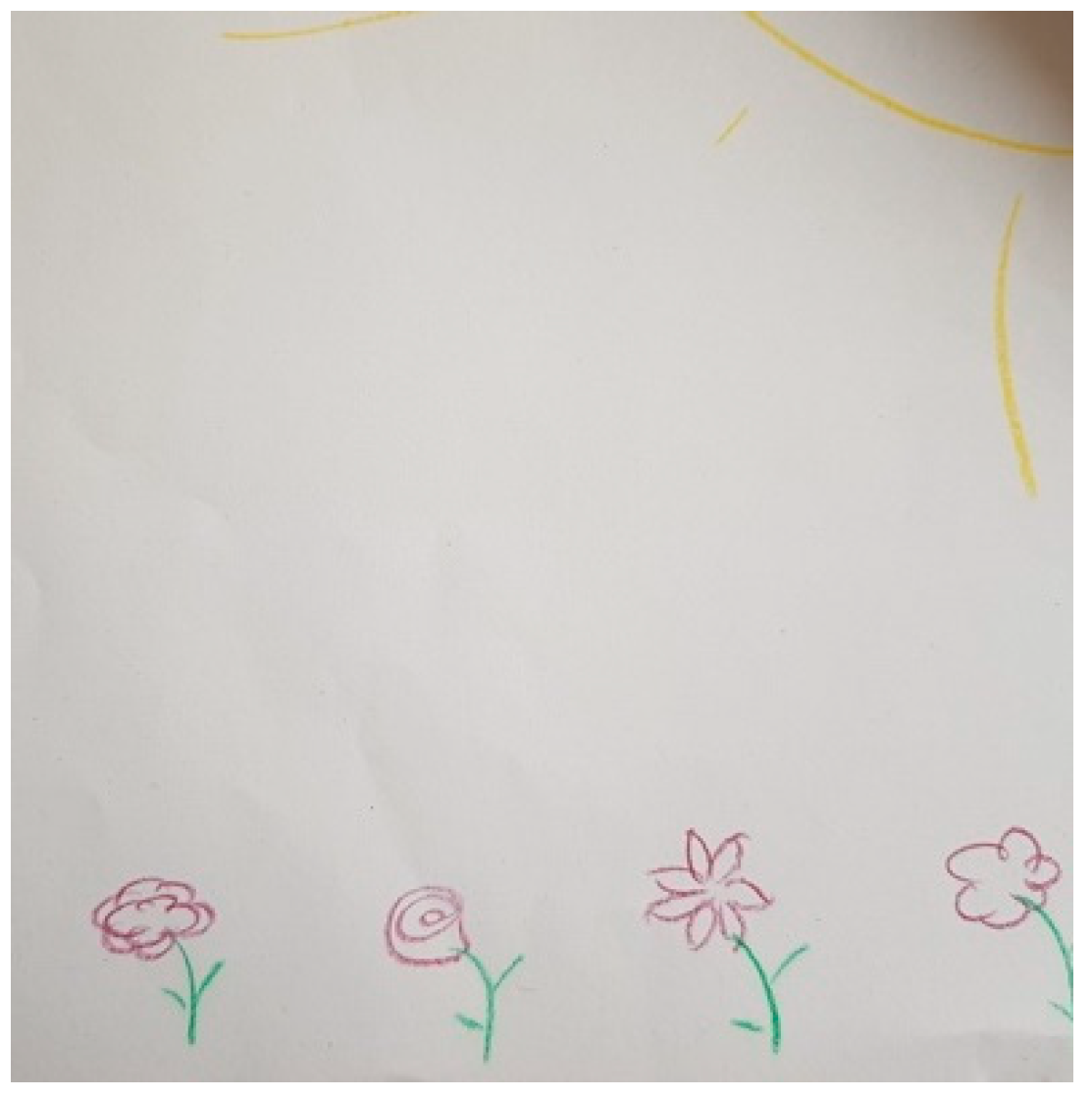
“It is a double-edged sword. Dark clouds and clear bright sky (…) I have painted a small campfire here, and my wife’s tricycle, with the walker standing next to it. We live with these handicaps, with these difficulties, but we always enjoy the sea and the view. We see a horizon (…) The ship disappears in the horizon to unknown places. We don’t see exactly where we are going but we are inside this ship and hope that it leads to a good destination towards the sun. The flowers at the beach indicate that we are also having a good time. We have experienced a lot of beautiful things, we were lying in the sun, here the chairs have become empty now, but we are still here (…). Seen from my point of view, it is a hopeful picture, which nevertheless has the shadows of everyday life, and it shows that there are also dark sides, stony paths, or you can be alone sometimes and still be together as a couple as long as it is possible. The fire is still burning, maybe a small one (…) Even our living together, our intimate life, that hasn’t been extinguished”.(FC26)
3.3. Changing as a Person during the Disease
“I have the feeling that my personality has been turned around a bit. I am not the same person I was before. I was so friendly and nice before. And today I am almost toxic. Sometimes I also give poisonous answer to my husband. I feel like that’s not very good. But I can’t help it” (…) (P28). “And you think this change has to do with the disease?” (R1). “Sure, 100 per cent yes, because it has come more now” (P28). “Since when?” (R1). “Since I could no longer walk. That was the worst thing for me”.(P28)
“That’s still a bit difficult for me now. Yes. In the past few years I had the feeling that he was somehow isolating himself and he is like in a cage with his illness. Somehow, I have the feeling that I can’t get close to him anymore as if there would be like a Parkinson’s wall between us”.(FC6)
“Before the illness, she was really energetic and always had to do something, and now with the illness, I almost have to force her to go somewhere, to the theatre or the cinema or somewhere. She has all the excuses she needs not to be around many people. And yes, how should I put it, um, because of the illness she has also become more selfish. So, she comes first and then again and then maybe the others. Sometimes I’ve also said, I’m not a domiciliary care provider. You pay him and you can give him orders, but I don’t get paid”.(FC29)
“He was so hyperactive, and I didn’t know if that was because he knew that he had a disease and he wanted to enjoy life (…) He was thinking more about himself, looking more for his own pleasure. He had no sense of time and he was looking for his pleasure. That was his first concern, to think of himself”.(FC2)
“On the one hand, you get emotional much more quickly. So, when there is an emotional situation, tears come immediately, even if I don’t want them to come. Both positively and negatively. The emotionality is actually much greater. But conversely, in the perception of happiness and unhappiness, one becomes somehow like a little more indifferent. Everything is always a little more or less good. It’s not extremely good and it’s not extremely bad either”.(P5)
3.4. DBS Improved My Life
“Since then, she can use her hand completely again. She doesn’t tremble. She can do different things by herself again. Before I had to cut the meat and everything for her, and today everything is back to normal”.(FC29)
“Well, there’s a kind of rebirth, yes, with a few clouds, because it’s not easy every day. But already much, much better than before”.(P40)
“And then after I drew spring, because the stimulation (DBS) is hope, renewal, and then it’s life that blooms again”.(FC41)
“If I hadn’t had the operation, I might be in a nursing home or something (…) If I hadn’t operated, I think it would probably be more difficult. Almost certainly. Anyway, my partner says that it has helped 100 per cent”.(P9)
“I’m alive now and if I wouldn’t have gone through it, I’d already be underground”.(P21)
“Do you now feel that deep stimulation has changed your life?” (Researcher 1). “Yes, certainly, in the sense that I can do practically everything again. I have a perspective again, at least for the next ten years, a positive perspective. I can consciously plan things again that were previously written in the stars. I can now seriously plan them again. For example, going on a trip with my wife after retirement. We have so many plans that it makes a huge difference when you can plan again and assume that it will work out. We had all these uncertainties before. Before, I didn’t even know if I would be able to work until retirement. That is no longer a question. I’ve already agreed with my colleague that I’ll be available and able to work after retirement”.(P5)
“He is more at ease when speaking (…) He can stay standing or go with them [the neighbors] to see something. Whereas before he withdrew himself a little when he had so much dyskinesia. I do think that it’s better now for the contact and the neighborhood network”(FC39)
“Now it’s better after the deep brain stimulation. It is really better (…) The speaking part that is very important for me, that you can exchange and talk to each other. Of course, that became less. Parkinson’s patients also speak less, of course. That was also a huge problem for me. I like to talk about everything. I want to exchange ideas. That was no longer possible. That is better now”.(FC6)
“Now here I have the hope, partly after the deep brain stimulation, that even if it is a bit worse in between, it will get better again”.(FC6)
“One of my doctors described it [DBS effects], very well. He said that it’s like sitting in a cold room and making a fire. The fire goes up, down up, down, and you are cold and then warm, and cold and warm. And the stimulator is like you install a central heating system. So, it’s a continuous effect (…) Before [with oral treatment], it was high low high low, and the stimulation is straight. You have a constant effect with the stimulation”.(P1)
“It doesn’t always work out equally well, but as long as it is still possible to put the power up and then it works (…) Before, it was necessary to increase the meds, and now you can do the same much easier just using electricity”.(P27)
“Yes, I use it occasionally, so for control, but I don’t change it every day or much. I think I’m actually not badly adjusted. What I’m going to do, maybe this week, is to lower it a bit on the other side because I’m having more and more cramps in this upper arm, which are very painful and that can help”.(P12)
3.5. I Am Treated with DBS but I Still Have Parkinson’s
“The disease is progressing (…) It’s going to get worse and worse”(P44)
“It’s better, but you still live next to a sick person, and you sleep next to a sick person”(FC2)
“I have been given a new life. Another chance, so to speak. But this chance is now increasingly limited, of course, because I realize that I can’t do many things any more (…) It’s not a cure. That’s precisely the problem (…) Other people think you are healthy again. That is a consequence of the operation, that many people in the circle of friends then thought, now you have had the operation, now you are as you were before, capable of performing, able to work under pressure. And that is simply not true (…) The effect [of DBS] was like getting a new life, but now the illness is coming back stronger”.(P12)
“I would say that the little devil is still there, but at the moment he is sitting in a backpack and is not hindering me (…) I know that [PD] is not gone. That must always be clear. Maybe it’ll get out of the backpack again and lead back again. I don’t know. The doctors think I could expect the effect of deep brain stimulation for about ten years”.(P5)
“It is noticeable today that everything has become a little slower (…) The asking back and forth, that has increased. In the past she cooked, I had no problem, I ate what she made. Today I have to ask her, what would you like for dinner today? That has become our daily routine, three times a day, or, in the morning, I say, what would you like, bread, everything, at noon and in the evening. Yes, that has become my task, to think a bit more for my wife as well” (FC26). “More after the intervention than before?” (Researcher 1). “Yes, before I didn’t have to think for my wife anything. She organized everything herself and was independent in every way. She managed the household, but today we have to share everything”.(FC26)
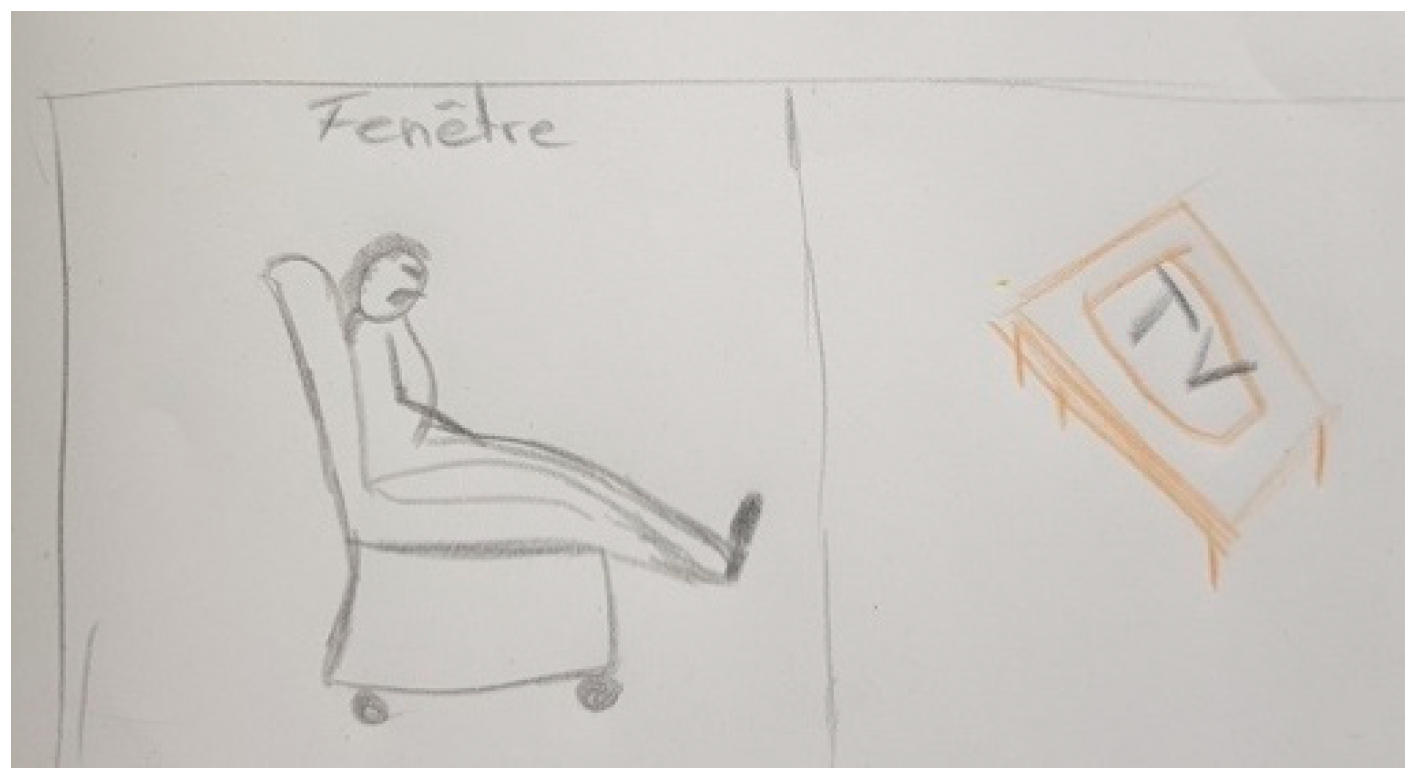
“It simply means that life in society is different. It means that he is often in a chair at home, uh, because of fatigue. Fatigue and then walking, eh walking, it has decreased a lot too”.(FC45)
“It is a picture full of confusion. You can see the brain and the lightning that works into the substantia nigra, those are the electronic currents. And that goes out again with these daily worries, with the medication, with the appointments you have, you always have to think about it, about all kinds of things. Time runs. It’s ringing again, that’s the alarm for the tablets intake that is at the center here. Today, it controls our everyday life quite strongly (…) The eyes are perhaps a little bit empty here (…). I would say they [the eyes] are hopeful for the future despite all the chaos, the lightning that comes at us every day, the question marks that surround everything here, DBS, the medications, yes, and so on”.(FC26)
3.6. DBS Is Not Perfect
“Does the medicine work right away? Doesn’t it work yet? Uh, a lot of things are happening at the same time. It’s very difficult and each person is very different”.(FC45)
“If he has to speak for a long time, usually his voice will diminish, he won’t be able to (…) He enjoys going to restaurants, eating, something he didn’t enjoy before. But on the other hand, he can’t express himself when he is in society and has to speak when there are a lot of people (…) So that’s one of the disadvantages”.(FC41)
“Walking is going down, but the doctor surgeon, neurologist said that deep stimulation does nothing for walking or very little. We had the impression that it was very difficult to adjust it, to make a fine adjustment”.(P39)
“I have to say, I expected more. I thought after the brain operation everything would be fine, yes, fine, the hope was there, now everything will be fine again. If I am stimulated every day afterwards it’ll be like before. But that wasn’t the case. That was only at the beginning. The shared joy (…) It’s only possible to adjust it so that it is optimal (…) And that ideal point, was not always ideal. At the beginning, they had to change it a bit up, a bit down, and then it is found wasn’t the best result. Ah, it’s the best possible, but not what we had hoped for”.(FC26)
“Yes, well my husband, he would rather go on holiday even more than I would. For me it’s always in a new place is already a bit stressful. So I notice that. I told you, I’m not so resilient anymore. So packing, that’s hard for me”.(P35)
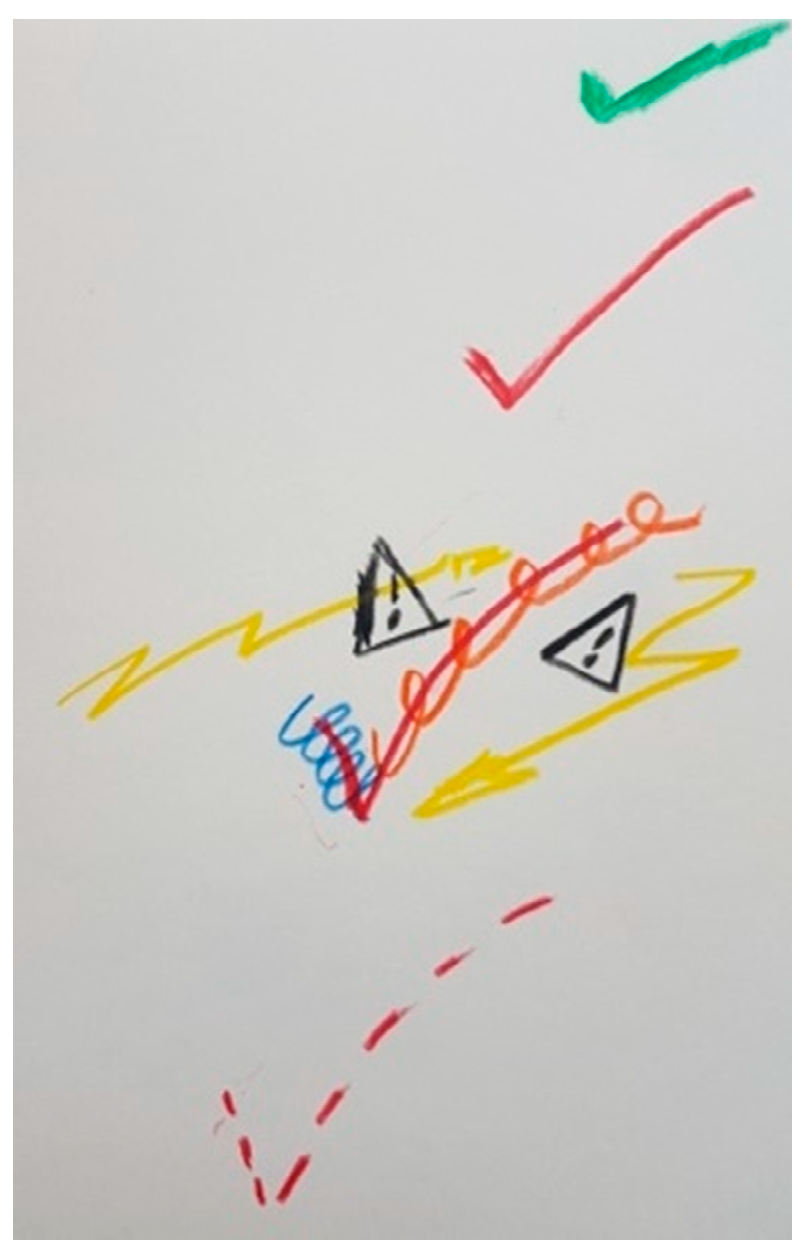
“This is at the beginning, and there is no signal, or few signals before the DBS is implanted, and afterwards there is a positive V. It’s a “big turn” but it is still fragile, and this is the infection [the triangles with the exclamation mark]. After the infection, it went well, but now, I have to say I always have the impression that in the depression, the stimulator is a very important element”.(P1)
3.7. Being Different after DBS
“He takes care of things he likes and doesn’t need to have a lot of people around him” (FC45). “And that was also like that before the operation?” (Researcher 2). “There was already a little bit like that before the operation, but it was really minimal. It didn’t happen daily or anything like that. (…) And then [after DBS intervention], he became much more sensitive. For example, if you watch a film and there are emotions involved in that film, he would cry straight away. You can see the tears. He was never like that”.(FC45)
“I was irritable, belligerent, and freaked out. I drove everyone crazy in the hospital” (P23). “And this was immediately after the operation?” (Researcher 1). “Immediately? Yes. Maybe three weeks later as well” (P23). “And now do you still feel different?” (Researcher 1). “Yeah. Still not good”.(P21)
“He really had a personality change for a short period of time and also a manic phase. He was completely different for a while” (FC37). “What do you mean by manic phase?” (Researcher 1). “Yes, after the operation he was really changed in his manner, that he for example/that he complimented me or hugged me when greeting me, as he never did before (…) He bought an expensive watch and booked holidays, big holidays, without discussing it with my mother. And also wanted to write a book. Yes, things like that”.(FC37)
“After DBS, she had a bit of trouble when I had so many ups and I made a lot of quick decisions. I invited people to our place and so on, and she didn’t appreciate that so much. Just because she also didn’t like it so much when it went down again after DBS. It wasn’t depression, but depressive moods”.(P27)
“And he had it again a fortnight ago. So, depression-like episodes (…) No one told me that could happen (…) He wasn’t told either. We talked about it recently. I told him, why don’t you ask that in the next consultation? I told him that when he has an examination in hospital, then he should ask whether this side effect is possible”.(FC17)
“My partner said, oh, you have to get an induction cooker. And then I immediately thought, magnetic fields. And then it was when I first googled that and it’s a topic in the media and that’s why I thought, I don’t want it. I don’t want that in ten years will be found out that it’s harmful for the brain or the battery. And those are moments that are different with my partner”.(P35)
“I don’t have the feeling that I’ve become a different person. I haven’t but at the same time I’m not the same. I’m much more anxious. (…) It [DBS intervention] was certainly a borderline experience. It’s a borderline experience like a birth. I also compare it to a new life that I got. Other people don’t have this borderline experience, and that creates often a distance to others”.(P12)
“I don’t have the feeling that there is something in there. I do notice it, of course it is a foreign body in my body, but I live with it now and not badly”.(P7)
“No, nothing bothers me about her, even that she has such a device above her chest that you can see and feel, that doesn’t bother me. (…) That belongs to my wife. Exactly. It’s not a foreign body from my point of view. I don’t perceive her as my wife, who has electronics in her brain. I just don’t think about it at all”.(FC26)
“I’ve always said I’m a so-called cyborg now. The funny thing was that I said this once to my neurologist that I would be a cyborg afterwards. Then he immediately objected and said, no, no, you are still a human being”.(P5)
4. Discussion
Strengths, Limitations, and Future Directions
- Firstly, our study was very comprehensive and did not focus specifically on one issue in relation to PD or DBS as other studies did. Therefore, some issues may have been missed during the interviews, such as the burden of normality, particularly in FCs. This particular topic should be investigated in more detail in the future as it is a very underrepresented topic in the medical literature.
- The participants were interviewed only after being treated with DBS and not before they started receiving this treatment. Although all participants were asked questions about their daily lives and how they were doing before treatment, those who have lived with PD and DBS for a longer period of time may have lost perspective on the before and after. This may have led to recall bias.
- Some patients who initially showed interest in the study finally decided not to participate because they were going through a difficult time with DBS side effects. Therefore, we missed some negative experiences with DBS due to the fact that people who have bad experiences are often more reluctant to share their experiences than those who have had positive experiences with the treatment.
- PD patients treated with DBS are a defined sub-cohort of PD and are not representative of the entire PD population. For example, patients within the first years after the first diagnosis (i.e., <5 years) are not represented, since DBS is usually not provided at this stage of the disease. Furthermore, patients experiencing moderate to severe dementia or with lack of physical or psychological resilience were excluded from the study. This means that the population of patients at a very advanced stage of the disease is not represented in our study either. We are aware that this exclusion may have led to inclusion bias. However, we could not include participants unable to hold a long conversation sharing stories over different time frames (e.g., before and after DBS), which is very difficult for patients with advanced PD. Therefore, we consider that despite the risk of inclusion bias, our study applied the best sampling strategy for the objectives of our study and its methodology.
- Only patients treated from 6 months to 10 years with DBS were included to have a broad spectrum of experiences with DBS at different stages. Further studies are needed to delve into the individual patients’ difficulties and needs at each stage of the treatment. Other issues need further elucidation, such as patient and FC experiences with the side-effects resulting from dopaminergic treatment or the impact of memories of DBS surgery.
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Appendix A


References
- Rizek, P.; Kumar, N.; Jog, M.S. An update on the diagnosis and treatment of Parkinson disease. Can. Med. Assoc. J. 2016, 188, 1157–1165. [Google Scholar] [CrossRef] [PubMed]
- Dorsey, E.R.; Sherer, T.; Okun, M.S.; Bloem, B.R. The Emerging Evidence of the Parkinson Pandemic. J. Park. Dis. 2018, 8, S3–S8. [Google Scholar] [CrossRef] [PubMed]
- Casacanditella, L.; Cosoli, G.; Ceravolo, M.; Tomasini, E. Non-contact measurement of tremor for the characterisation of Parkinsonian individuals: Comparison between Kinect and Laser Doppler vibrometer. J. Phys. Conf. Ser. 2017, 882, 012002. [Google Scholar] [CrossRef]
- Eeden, S.K.V.D.; Tanner, C.M.; Bernstein, A.L.; Fross, R.D.; Leimpeter, A.; Bloch, D.A.; Nelson, L.M. Incidence of Parkinson’s Disease: Variation by Age, Gender, and Race/Ethnicity. Am. J. Epidemiol. 2003, 157, 1015–1022. [Google Scholar] [CrossRef]
- Parkinson, J. An Essay on the Shaking Palsy. J. Neuropsychiatry Clin. Neurosci. 2002, 14, 223–236. [Google Scholar] [CrossRef]
- Charcot, J.M. Leçons du Mardi à la Salpêtrière: Policliniques 1887–1888; Publications du Progrès Médical: Paris, France, 1887. [Google Scholar]
- DeMaagd, G.; Philip, A. Parkinson’s disease and its management: Part 1: Disease entity, risk factors, pathophysiology, clinical presentation, and diagnosis. Pharm. Ther. 2015, 40, 504. [Google Scholar]
- Hawkes, C.H.; Del Tredici, K.; Braak, H. A timeline for Parkinson’s disease. Park. Relat. Disord. 2010, 16, 79–84. [Google Scholar] [CrossRef] [PubMed]
- Schrag, A.; Horsfall, L.; Walters, K.; Noyce, A.; Petersen, I. Prediagnostic presentations of Parkinson’s disease in primary care: A case-control study. Lancet Neurol. 2015, 14, 57–64. [Google Scholar] [CrossRef]
- Cronin-Golomb, A. Emergence of nonmotor symptoms as the focus of research and treatment of Parkinson’s disease: Introduction to the special section on nonmotor dysfunctions in Parkinson’s disease. Behav. Neurosci. 2013, 127, 135–138. [Google Scholar] [CrossRef][Green Version]
- Ortiz, K.Z.; Brabo, N.C.; Minett, T.S.C. Sensorimotor speech disorders in Parkinson’s disease: Programming and execution deficits. Dement. Neuropsychol. 2016, 10, 210–216. [Google Scholar] [CrossRef][Green Version]
- Smith, K.M.; Caplan, D.N. Communication impairment in Parkinson’s disease: Impact of motor and cognitive symptoms on speech and language. Brain Lang. 2018, 185, 38–46. [Google Scholar] [CrossRef]
- Soundy, A.; Stubbs, B.; Roskell, C. The Experience of Parkinson’s Disease: A Systematic Review and Meta-Ethnography. Sci. World J. 2014, 2014, 1–19. [Google Scholar] [CrossRef] [PubMed]
- Yang, W.; Hamilton, J.L.; Kopil, C.; Beck, J.C.; Tanner, C.M.; Albin, R.L.; Dorsey, E.R.; Dahodwala, N.; Cintina, I.; Hogan, P.; et al. Current and projected future economic burden of Parkinson’s disease in the U.S. NPJ Park. Dis. 2020, 6, 1–9. [Google Scholar] [CrossRef] [PubMed]
- Noyes, K.; Liu, H.; Li, Y.; Holloway, R.; Dick, A.W. Economic burden associated with Parkinson’s disease on elderly Medicare beneficiaries. Mov. Disord. 2005, 21, 362–372. [Google Scholar] [CrossRef]
- Nutt, J.G.; Woodward, W.R.; Hammerstad, J.P.; Carter, J.H.; Anderson, J.L. The “On–Off” Phenomenon in Parkinson’s Disease. N. Engl. J. Med. 1984, 310, 483–488. [Google Scholar] [CrossRef]
- Wood, L.D. Clinical Review and Treatment of Select Adverse Effects of Dopamine Receptor Agonists in Parkinson’s Disease. Drugs Aging 2010, 27, 295–310. [Google Scholar] [CrossRef] [PubMed]
- Groiss, S.; Wojtecki, L.; Südmeyer, M.; Schnitzler, A. Review: Deep brain stimulation in Parkinson’s disease. Ther. Adv. Neurol. Disord. 2009, 2, 379–391. [Google Scholar] [CrossRef]
- Weaver, F.M.; Follett, K.A.; Stern, M.B.; Luo, P.; Harris, C.L.; Hur, K.; Marks, W.J.; Rothlind, J.C.; Sagher, O.; Moy, C.S.; et al. Randomized trial of deep brain stimulation for Parkinson disease: Thirty-six-month outcomes. Neurology 2012, 79, 55–65. [Google Scholar] [CrossRef]
- Garcia-Ruiz, P.J. Impulse Control Disorders and Dopamine-Related Creativity: Pathogenesis and Mechanism, Short Review, and Hypothesis. Front. Neurol. 2018, 9, 1041. [Google Scholar] [CrossRef]
- Martinez-Ramirez, D.; Hu, W.; Bona, A.R.; Okun, M.; Shukla, A.W. Update on deep brain stimulation in Parkinson’s disease. Transl. Neurodegener. 2015, 4, 1–8. [Google Scholar] [CrossRef]
- Tekriwal, A.; Baltuch, G. Deep Brain Stimulation: Expanding Applications. Neurol. Med. Chir. 2015, 55, 861–877. [Google Scholar] [CrossRef] [PubMed]
- Sarem-Aslani, A.; Mullett, K. Industrial Perspective on Deep Brain Stimulation: History, Current State, and Future Developments. Front. Integr. Neurosci. 2011, 5, 46. [Google Scholar] [CrossRef] [PubMed]
- Martinez-Ramirez, D.; Jimenez-Shahed, J.; Leckman, J.F.; Porta, M.; Servello, D.; Meng, F.-G.; Kuhn, J.; Huys, D.; Baldermann, J.C.; Foltynie, T.; et al. Efficacy and Safety of Deep Brain Stimulation in Tourette Syndrome. JAMA Neurol. 2018, 75, 353–359. [Google Scholar] [CrossRef]
- Dandekar, M.P.; Fenoy, A.J.; Carvalho, A.F.; Soares, J.C.; Quevedo, J. Deep brain stimulation for treatment-resistant depression: An integrative review of preclinical and clinical findings and translational implications. Mol. Psychiatry 2018, 23, 1094–1112. [Google Scholar] [CrossRef]
- Youngerman, B.; Chan, A.K.; Mikell, C.B.; McKhann, G.M.; Sheth, S.A. A decade of emerging indications: Deep brain stimulation in the United States. J. Neurosurg. 2016, 125, 461–471. [Google Scholar] [CrossRef] [PubMed]
- Kahn, L.; Mathkour, M.; Lee, S.X.; Gouveia, E.E.; Hanna, J.A.; Garces, J.; Scullen, T.; McCormack, E.; Riffle, J.; Glynn, R.; et al. Long-term outcomes of deep brain stimulation in severe Parkinson’s disease utilizing UPDRS III and modified Hoehn and Yahr as a severity scale. Clin. Neurol. Neurosurg. 2019, 179, 67–73. [Google Scholar] [CrossRef] [PubMed]
- Lozano, A.M.; Lipsman, N.; Bergman, H.; Brown, P.; Chabardes, S.; Chang, J.W.; Matthews, K.; McIntyre, C.C.; Schlaepfer, T.E.; Schulder, M.; et al. Deep brain stimulation: Current challenges and future directions. Nat. Rev. Neurol. 2019, 15, 148–160. [Google Scholar] [CrossRef]
- Elliott, M.; Momin, S.; Fiddes, B.; Farooqi, F.; Sohaib, S.A. Pacemaker and Defibrillator Implantation and Programming in Patients with Deep Brain Stimulation. Arrhythmia Electrophysiol. Rev. 2019, 8, 138–142. [Google Scholar] [CrossRef]
- Baylis, F. “I Am Who I Am”: On the Perceived Threats to Personal Identity from Deep Brain Stimulation. Neuroethics 2011, 6, 513–526. [Google Scholar] [CrossRef] [PubMed]
- Gisquet, E. Cerebral implants and Parkinson’s disease: A unique form of biographical disruption? Soc. Sci. Med. 2008, 67, 1847–1851. [Google Scholar] [CrossRef] [PubMed]
- Kraemer, F. Me, Myself and My Brain Implant: Deep Brain Stimulation Raises Questions of Personal Authenticity and Alienation. Neuroethics 2011, 6, 483–497. [Google Scholar] [CrossRef] [PubMed]
- Gilbert, F.; Viaña, J.N.; Ineichen, C. Deflating the “DBS causes personality changes” bubble. Neuroethics 2018, 1–17. [Google Scholar] [CrossRef]
- Lhommée, E.; Boyer, F.; Wack, M.; Pélissier, P.; Klinger, H.; Schmitt, E.; Bichon, A.; Fraix, V.; Chabardès, S.; Mertens, P.; et al. Personality, dopamine, and Parkinson’s disease: Insights from subthalamic stimulation. Mov. Disord. 2017, 32, 1191–1200. [Google Scholar] [CrossRef]
- Pham, U.; Solbakk, A.-K.; Skogseid, I.-M.; Toft, M.; Pripp, A.H.; Konglund, A.E.; Andersson, S.; Haraldsen, I.R.; Aarsland, D.; Dietrichs, E.; et al. Personality Changes after Deep Brain Stimulation in Parkinson’s Disease. Park. Dis. 2015, 2015, 1–7. [Google Scholar] [CrossRef]
- Kubu, C.S.; Ford, P.J.; Wilt, J.A.; Merner, A.R.; Montpetite, M.; Zeigler, J.; Racine, E. Pragmatism and the Importance of Interdisciplinary Teams in Investigating Personality Changes Following DBS. Neuroethics 2019, 2019, 1–11. [Google Scholar] [CrossRef]
- Thomson, C.J.; Segrave, R.A.; Racine, E.; Warren, N.; Thyagarajan, D.; Carter, A. “He’s Back so I’m Not Alone”: The Impact of Deep Brain Stimulation on Personality, Self, and Relationships in Parkinson’s Disease. Qual. Health Res. 2020, 30, 2217–2233. [Google Scholar] [CrossRef] [PubMed]
- Haahr, A.; Kirkevold, M.; Hall, E.O.; Østergaard, K. From miracle to reconciliation: A hermeneutic phenomenological study exploring the experience of living with Parkinson’s disease following Deep Brain Stimulation. Int. J. Nurs. Stud. 2010, 47, 1228–1236. [Google Scholar] [CrossRef]
- Chacón Gámez, Y.M. Deep brain stimulation and changes in personality and personal identity: The importance of qualitative studies. Neuroethics 2020, 6, 486–492. [Google Scholar]
- Armstrong, N.; Powell, J. Patient perspectives on health advice posted on Internet discussion boards: A qualitative study. Health Expect. 2009, 12, 313–320. [Google Scholar] [CrossRef] [PubMed]
- Jonasson, S.B.; Nilsson, M.H.; Lexell, J.; Carlsson, G. Experiences of fear of falling in persons with Parkinson’s disease—A qualitative study. BMC Geriatr. 2018, 18, 44. [Google Scholar] [CrossRef]
- Renouf, S.; Ffytche, D.; Pinto, R.; Murray, J.; Lawrence, V. Visual hallucinations in dementia and Parkinson’s disease: A qualitative exploration of patient and caregiver experiences. Int. J. Geriatr. Psychiatry 2018, 33, 1327–1334. [Google Scholar] [CrossRef] [PubMed]
- Cabrera, L.Y.; Kelly-Blake, K.; Sidiropoulos, C. Perspectives on Deep Brain Stimulation and Its Earlier Use for Parkinson’s Disease: A Qualitative Study of US Patients. Brain Sci. 2020, 10, 34. [Google Scholar] [CrossRef] [PubMed]
- De Haan, S.; Rietveld, E.; Stokhof, M.; Denys, D. Effects of Deep Brain Stimulation on the Lived Experience of Obsessive-Compulsive Disorder Patients: In-Depth Interviews with 18 Patients. PLoS ONE 2015, 10, e0135524. [Google Scholar] [CrossRef] [PubMed]
- Lewis, C.J.; Maier, F.; Horstkötter, N.; Zywczok, A.; Witt, K.; Eggers, C.; Meyer, T.D.; Dembek, T.A.; Maarouf, M.; Moro, E.; et al. Subjectively perceived personality and mood changes associated with subthalamic stimulation in patients with Parkinson’s disease. Psychol. Med. 2014, 45, 73–85. [Google Scholar] [CrossRef] [PubMed]
- Schupbach, M.; Gargiulo, M.; Welter, M.L.; Mallet, L.; Behar, C.; Houeto, J.L.; Maltete, D.; Mesnage, V.; Agid, Y. Neurosurgery in Parkinson disease: A distressed mind in a repaired body? Neurology 2006, 66, 1811–1816. [Google Scholar] [CrossRef]
- Liddle, J.; Phillips, J.; Gustafsson, L.; Silburn, P. Understanding the lived experiences of Parkinson’s disease and deep brain stimulation (DBS) through occupational changes. Aust. Occup. Ther. J. 2017, 65, 45–53. [Google Scholar] [CrossRef]
- Jewitt, C. The Routledge Handbook of Multimodal Analysis, 2nd ed.; First Published in Paperback; Routledge: London, UK; Taylor & Francis Group: New York, NY, USA, 2017. [Google Scholar]
- McLaughlin, D.; Hasson, F.; Kernohan, G.; Waldron, M.; McLaughlin, M.; Cochrane, B.; Chambers, H. Living and coping with Parkinson’s disease: Perceptions of informal carers. Palliat. Med. 2010, 25, 177–182. [Google Scholar] [CrossRef]
- Rastgardani, T.; Armstrong, M.J.; Marras, C.; Gagliardi, A.R. Improving patient-centred care for persons with Parkinson’s: Qualitative interviews with care partners about their engagement in discussions of “off” periods. Health Expect. 2019, 22, 555–564. [Google Scholar] [CrossRef]
- Hariz, G.-M.; Limousin, P.; Tisch, S.; Jahanshahi, M.; Fjellman-Wiklund, A. Patients’ perceptions of life shift after deep brain stimulation for primary dystonia-A qualitative study. Mov. Disord. 2011, 26, 2101–2106. [Google Scholar] [CrossRef]
- Chacón Gámez, Y.M.; Mouton Dorey, C.; Biller-Andorno, N. Exploring the experiences of Parkinson’s patients and their family caregivers with healthcare professionals: A qualitative assessment of unmet needs. PLoS ONE 2021, 14, e0226916. [Google Scholar]
- Gámez, Y.M.C.; Biller-Andorno, N. Living with Parkinson’s disease and connected to the duodopa pump: A qualitative study. Qual. Res. Med. Health 2021, 4. [Google Scholar] [CrossRef]
- ERG. Health Experiences Research Group, Researcher’s Handbook Health Talk Online & Youth Health Talk Modules; Deparment of Primary Health Care: Oxford, UK, 2018.
- Creswell, W.J. Qualitative Inquiry & Research Design. Choosing among Five Approaches, 3rd ed.; SAGE: London, UK, 2013. [Google Scholar]
- Ziebland, S.; McPherson, A. Making sense of qualitative data analysis: An introduction with illustrations from DIPEx (personal experiences of health and illness). Med. Educ. 2006, 40, 405–414. [Google Scholar] [CrossRef]
- Ziebland, S.; Herxheimer, A. How patients’ experiences contribute to decision making: Illustrations from DIPEx (personal experiences of health and illness). J. Nurs. Manag. 2008, 16, 433–439. [Google Scholar] [CrossRef]
- Adami, E. Multimodality; Routledge: London, UK, 2015. [Google Scholar] [CrossRef]
- Guillemin, M. Understanding Illness: Using Drawings as a Research Method. Qual. Health Res. 2004, 14, 272–289. [Google Scholar] [CrossRef]
- Eassey, D.; Reddel, H.K.; Ryan, K.; Smith, L. Living with severe asthma: The role of perceived competence and goal achievement. Chronic Illn. 2019. [Google Scholar] [CrossRef]
- Fereday, J.; Muir-Cochrane, E. Demonstrating Rigor Using Thematic Analysis: A Hybrid Approach of Inductive and Deductive Coding and Theme Development. Int. J. Qual. Methods 2006, 5, 80–92. [Google Scholar] [CrossRef]
- Costa, K. Systematic Guide to Qualitative Data Analysis within the C.O.S.T.A Postgraduate Research Model; OSF Preprints: Charlottesville, VA, USA, 2019. [Google Scholar] [CrossRef]
- Roberts, K.; Dowell, A.; Nie, J.-B. Attempting rigour and replicability in thematic analysis of qualitative research data; a case study of codebook development. BMC Med. Res. Methodol. 2019, 19, 66. [Google Scholar] [CrossRef] [PubMed]
- Nowell, L.S.; Norris, J.; White, D.E.; Moules, N.J. Thematic Analysis: Striving to meet the trustworthiness criteria. Int. J. Qual. Methods 2017, 16. [Google Scholar] [CrossRef]
- Cheung, M.M.Y.; Saini, B.; Smith, L. Using drawings to explore patients’ perceptions of their illness: A scoping review. J. Multidiscip. Health 2016, 9, 631–646. [Google Scholar] [CrossRef] [PubMed]
- Kirkham, J.A.; Smith, J.A.; Havsteen-Franklin, D. Painting pain: An interpretative phenomenological analysis of representations of living with chronic pain. Health Psychol. 2015, 34, 398–406. [Google Scholar] [CrossRef] [PubMed]
- McGowan, L.; Luker, K.; Creed, F.; Chew-Graham, C.A. ‘How do you explain a pain that can’t be seen?’: The narratives of women with chronic pelvic pain and their disengagement with the diagnostic cycle. Br. J. Health Psychol. 2007, 12, 261–274. [Google Scholar] [CrossRef]
- Phillips, J.; Ogden, J.; Copland, C. Using drawings of pain-related images to understand the experience of chronic pain: A qualitative study. Br. J. Occup. Ther. 2015, 78, 404–411. [Google Scholar] [CrossRef]
- Haahr, A.; Kirkevold, M.; Hall, E.O.; Østergaard, K. ‘Being in it together’: Living with a partner receiving deep brain stimulation for advanced Parkinson’s disease—A hermeneutic phenomenological study. J. Adv. Nurs. 2012, 69, 338–347. [Google Scholar] [CrossRef] [PubMed]
- Theed, R.; Eccles, F.; Simpson, J. Experiences of caring for a family member with Parkinson’s disease: A meta-synthesis. Aging Ment. Health 2016, 21, 1007–1016. [Google Scholar] [CrossRef]
- Padovani, C.; Lopes, M.C.D.L.; Higahashi, I.H.; Pelloso, S.M.; Paiano, M.; Christophoro, R. Being caregiver of people with Parkinson’s Disease: Experienced situations. Rev. Bras. Enferm. 2018, 71, 2628–2634. [Google Scholar] [CrossRef] [PubMed]
- Martínez-Martín, P.; Forjaz, M.J.; Frades-Payo, B.; Rusiñol, A.B.; Fernández-García, J.M.; Benito-León, J.; Arillo, V.C.; Barberá, M.A.; Sordo, M.P.; Catalán, M.J. Caregiver burden in Parkinson’s disease. Mov. Disord. 2007, 22, 924–931. [Google Scholar] [CrossRef] [PubMed]
- Abendroth, M.; Greenblum, C.A.; Gray, J.A. The Value of Peer-Led Support Groups Among Caregivers of Persons With Parkinson’s Disease. Holist. Nurs. Pract. 2014, 28, 48–54. [Google Scholar] [CrossRef]
- Van Hienen, M.M.; Contarino, M.F.; Middelkoop, H.A.; Van Hilten, J.J.; Geraedts, V.J. Effect of deep brain stimulation on caregivers of patients with Parkinson’s disease: A systematic review. Park. Relat. Disord. 2020, 81, 20–27. [Google Scholar] [CrossRef] [PubMed]
- Joint, C.; Aziz, T.Z. Outcome After Deep Brain Stimulation Surgery of the Subthalamic Nucleus for Parkinson Disease: Do We Understand What Is Important to Our Patients? World Neurosurg. 2014, 82, 1035–1036. [Google Scholar] [CrossRef] [PubMed]
- Rossi, M.; Bruno, V.; Arena, J.; Cammarota, Á.; Merello, M. Challenges in PD Patient Management After DBS: A Pragmatic Review. Mov. Disord. Clin. Pract. 2018, 5, 246–254. [Google Scholar] [CrossRef]
- Müller, S.; Christen, M. Deep brain stimulation in parkinsonian patients—Ethical evaluation of cognitive, affective, and behavioral sequelae. AJOB Neurosci. 2011, 2, 3–13. [Google Scholar] [CrossRef]
- Witt, K.; Kuhn, J.; Timmermann, L.; Zurowski, M.; Woopen, C. Deep Brain Stimulation and the Search for Identity. Neuroethics 2011, 6, 499–511. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Hildt, E. Electrodes in the brain: Some anthropological and ethical aspects of deep brain stimulation. Int. Rev. Inf. Ethics 2006, 5, 33–38. [Google Scholar] [CrossRef]
- Schechtman, M. Philosophical reflections on narrative and deep brain stimulation. J. Clin. Ethics 2010, 21, 133–139. [Google Scholar]
- Voon, V.; Saint-Cyr, J.; Lozano, A.; Moro, E.; Poon, Y.Y.; Lang, A. Psychiatric symptoms in patients with Parkinson disease presenting for deep brain stimulation surgery. J. Neurosurg. 2005, 103, 246–251. [Google Scholar] [CrossRef] [PubMed]
- Radziunas, A.; Deltuva, V.P.; Tamasauskas, A.; Gleizniene, R.; Pranckeviciene, A.; Surkiene, D.; Bunevicius, A. Neuropsychiatric complications and neuroimaging characteristics after deep brain stimulation surgery for Parkinson’s disease. Brain Imaging Behav. 2018, 14, 62–71. [Google Scholar] [CrossRef]
- Zarzycki, M.Z.; Domitrz, I. Stimulation-induced side effects after deep brain stimulation—A systematic review. Acta Neuropsychiatr. 2019, 32, 57–64. [Google Scholar] [CrossRef] [PubMed]
- Christen, M.; Ineichen, C.; Bittlinger, M.; Bothe, H.-W.; Müller, S. Ethical Focal Points in the International Practice of Deep Brain Stimulation. AJOB Neurosci. 2014, 5, 65–80. [Google Scholar] [CrossRef]
- Mosley, P.; Marsh, R. The Psychiatric and Neuropsychiatric Symptoms after Subthalamic Stimulation for Parkinson’s Disease. J. Neuropsychiatry Clin. Neurosci. 2015, 27, 19–26. [Google Scholar] [CrossRef]
- Han, J.W.; Ahn, Y.D.; Kim, W.-S.; Shin, C.M.; Jeong, S.J.; Song, Y.S.; Bae, Y.J.; Kim, J.-M. Psychiatric Manifestation in Patients with Parkinson’s Disease. J. Korean Med. Sci. 2018, 33. [Google Scholar] [CrossRef]
- Leeman, R.F.; E Billingsley, B.; Potenza, M.N. Impulse control disorders in Parkinson’s disease: Background and update on prevention and management. Neurodegener. Dis. Manag. 2012, 2, 389–400. [Google Scholar] [CrossRef] [PubMed]
- Corvol, J.-C.; Artaud, F.; Cormier-Dequaire, F.; Rascol, O.; Durif, F.; Derkinderen, P.; Marques, A.-R.; Bourdain, F.; Brandel, J.-P.; Pico, F.; et al. Longitudinal analysis of impulse control disorders in Parkinson disease. Neurology 2018, 91, e189–e201. [Google Scholar] [CrossRef] [PubMed]
- Moore, T.J.; Glenmullen, J.; Mattison, D.R. Reports of Pathological Gambling, Hypersexuality, and Compulsive Shopping Associated With Dopamine Receptor Agonist Drugs. JAMA Intern. Med. 2014, 174, 1930–1933. [Google Scholar] [CrossRef] [PubMed]
- Klos, K.J.; Bower, J.H.; Josephs, K.A.; Matsumoto, J.Y.; Ahlskog, J.E. Pathological hypersexuality predominantly linked to adjuvant dopamine agonist therapy in Parkinson’s disease and multiple system atrophy. Park. Relat. Disord. 2005, 11, 381–386. [Google Scholar] [CrossRef] [PubMed]
- Tarakad, A.; Jankovic, J. Anosmia and Ageusia in Parkinson’s Disease. Int. Rev. Neurobiol. 2017, 133, 541–556. [Google Scholar] [CrossRef]
- Pandey, S.; Srivanitchapoom, P. Levodopa-induced Dyskinesia: Clinical Features, Pathophysiology, and Medical Management. Ann. Indian Acad. Neurol. 2017, 20, 190–198. [Google Scholar] [CrossRef]
- Glannon, W. Stimulating brains, altering minds. J. Med. Ethics 2009, 35, 289–292. [Google Scholar] [CrossRef]
- Gilbert, F. The burden of normality: From ‘chronically ill’ to ‘symptom free’. New ethical challenges for deep brain stimulation postoperative treatment. J. Med. Ethics 2012, 38, 408–412. [Google Scholar] [CrossRef]
- Gilbert, F.; Goddard, E.; Viaña, J.N.M.; Carter, A.; Horne, M. I Miss Being Me: Phenomenological Effects of Deep Brain Stimulation. AJOB Neurosci. 2017, 8, 96–109. [Google Scholar] [CrossRef]
- Costanza, A.; Radomska, M.; Bondolfi, G.; Zenga, F.; Amerio, A.; Aguglia, A.; Serafini, G.; Amore, M.; Berardelli, I.; Pompili, M.; et al. Suicidality Associated With Deep Brain Stimulation in Extrapyramidal Diseases: A Critical Review and Hypotheses on Neuroanatomical and Neuroimmune Mechanisms. Front. Integr. Neurosci. 2021, 15. [Google Scholar] [CrossRef]
- Bell, E.; Maxwell, B.; McAndrews, M.P.; Sadikot, A.F.; Racine, E. A Review of Social and Relational Aspects of Deep Brain Stimulation in Parkinson’s Disease Informed by Healthcare Provider Experiences. Park. Dis. 2011, 2011, 1–8. [Google Scholar] [CrossRef] [PubMed]
- Baertschi, M.; Favez, N.; Radomska, M.; Herrmann, F.; Burkhard, P.R.; Weber, K.; Canuto, A.; Dos Santos, J.F.A. An Empirical Study on the Application of the Burden of Normality to Patients Undergoing Deep Brain Stimulation for Parkinson’s Disease. J. Psychosoc. Rehabil. Ment. Health 2019, 6, 175–186. [Google Scholar] [CrossRef]
- Baertschi, M.; Dos Santos, J.F.A.; Burkhard, P.; Weber, K.; Canuto, A.; Favez, N. The burden of normality as a model of psychosocial adjustment after deep brain stimulation for Parkinson’s disease: A systematic investigation. Neuropsychology 2019, 33, 178–194. [Google Scholar] [CrossRef]
- Accolla, E.A.; Pollo, C. Mood Effects after Deep Brain Stimulation for Parkinson’s Disease: An Update. Front. Neurol. 2019, 10, 617. [Google Scholar] [CrossRef] [PubMed]
- Mosley, P.E.; Robinson, K.; Coyne, T.; Silburn, P.; Breakspear, M.; Carter, A. ‘Woe Betides Anybody Who Tries to Turn me Down.’ A Qualitative Analysis of Neuropsychiatric Symptoms Following Subthalamic Deep Brain Stimulation for Parkinson’s Disease. Neuroethics 2019, 1–17. [Google Scholar] [CrossRef]
- Bogdan, I.D.; Van Laar, T.; Oterdoom, D.M.; Drost, G.; Van Dijk, J.M.C.; Beudel, M. Optimal Parameters of Deep Brain Stimulation in Essential Tremor: A Meta-Analysis and Novel Programming Strategy. J. Clin. Med. 2020, 9, 1855. [Google Scholar] [CrossRef]
- Brown, R.; Jahanshahi, M.; Quinn, N.; Marsden, C.D. Sexual function in patients with Parkinson’s disease and their partners. J. Neurol. Neurosurg. Psychiatry 1990, 53, 480–486. [Google Scholar] [CrossRef] [PubMed]
- MacKenzie, R. Who Should Hold the Remote for the New Me? Cognitive, Affective, and Behavioral Side Effects of DBS and Authentic Choices over Future Personalities. AJOB Neurosci. 2011, 2, 18–20. [Google Scholar] [CrossRef]
- MacKenzie, R. Must Family/Carers Look after Strangers? Post-DBS Identity Changes and Related Conflicts Of Interest. Front. Integr. Neurosci. 2011, 5, 12. [Google Scholar] [CrossRef]
- De Haan, S. Missing Oneself or Becoming Oneself? The Difficulty of What “Becoming a Different Person” Means. AJOB Neurosci. 2017, 8, 110–112. [Google Scholar] [CrossRef]
- Mecacci, G.; Haselager, P. Stimulating the Self: The Influence of Conceptual Frameworks on Reactions to Deep Brain Stimulation. AJOB Neurosci. 2014, 5, 30–39. [Google Scholar] [CrossRef]
- Gilbert, F. Deep Brain Stimulation: Inducing Self-Estrangement. Neuroethics 2017, 11, 157–165. [Google Scholar] [CrossRef]
- Pateraki, M. Τhe multiple temporalities of deep brain stimulation (DBS) in Greece. Med. Health Care Philos. 2018, 22, 353–362. [Google Scholar] [CrossRef]
- Tanner, C.M. A second honeymoon for Parkinson’s disease? N. Engl. J. Med. 2013, 368, 675–676. [Google Scholar] [CrossRef]
- Charmaz, K. Good Days, Bad Days: The Self in Chronic Illness and Time; Rutgers University Press: New Brunswick, NJ, USA, 1991. [Google Scholar]
- Vann-Ward, T.; Morse, J.M.; Charmaz, K. Preserving Self: Theorizing the Social and Psychological Processes of Living with Parkinson Disease. Qual. Health Res. 2017, 27, 964–982. [Google Scholar] [CrossRef]
- Pesantes, M.A.; Somerville, C.; Singh, S.B.; Perez-Leon, S.; Madede, T.; Suggs, S.; Beran, D. Disruption, changes, and adaptation: Experiences with chronic conditions in Mozambique, Nepal and Peru. Glob. Public Health 2019, 15, 372–383. [Google Scholar] [CrossRef]
- Bramley, N.; Eatough, V. The experience of living with Parkinson’s disease: An interpretative phenomenological analysis case study. Psychol. Health 2005, 20, 223–235. [Google Scholar] [CrossRef]
- Williams, S. Chronic illness as biographical disruption or biographical disruption as chronic illness? Reflections on a core concept. Sociol. Health Illn. 2000, 22, 40–67. [Google Scholar] [CrossRef]
- Barken, R. Caregivers’ Interpretations of Time and Biography. J. Contemp. Ethnogr. 2014, 43, 695–719. [Google Scholar] [CrossRef]
- Korstjens, I.; Moser, A. Series: Practical guidance to qualitative research. Part 4: Trustworthiness and publishing. Eur. J. Gen. Pract. 2017, 24, 120–124. [Google Scholar] [CrossRef]
- Danna, J.; Velay, J.-L.; Eusebio, A.; Véron-Delor, L.; Witjas, T.; Azulay, J.-P.; Pinto, S. Digitalized spiral drawing in Parkinson’s disease: A tool for evaluating beyond the written trace. Hum. Mov. Sci. 2019, 65, 80–88. [Google Scholar] [CrossRef] [PubMed]
- Shimura, H.; Tanaka, R.; Urabe, T.; Tanaka, S.; Hattori, N. Art and Parkinson’s disease: A dramatic change in an artist’s style as an initial symptom. J. Neurol. 2011, 259, 879–881. [Google Scholar] [CrossRef] [PubMed]
- Brailas, A. Using Drawings in Qualitative Interviews: An Introduction to the Practice. Qual. Rep. 2020, 25, 4447–4460. [Google Scholar] [CrossRef]
- Broadbent, E.; Petrie, K.J.; Ellis, C.J.; Ying, J.; Gamble, G. A picture of health—Myocardial infarction patients’ drawings of their hearts and subsequent disability. J. Psychosom. Res. 2004, 57, 583–587. [Google Scholar] [CrossRef]
- Thorpe, C.; Arbeau, K.J.; Budlong, B. ‘I drew the parts of my body in proportion to how much PCOS ruined them’: Experiences of polycystic ovary syndrome through drawings. Health Psychol. Open 2019, 6. [Google Scholar] [CrossRef]
- Broadbent, E.; Niederhoffer, K.; Hague, T.; Corter, A.; Reynolds, L. Headache sufferers’ drawings reflect distress, disability and illness perceptions. J. Psychosom. Res. 2009, 66, 465–470. [Google Scholar] [CrossRef] [PubMed]


















{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Group | Average Age at Diagnosis a | Number | Average Age at Interview a | Gender (F, M) | Average Years with DBS a |
|---|---|---|---|---|---|
| Patients | 37–71, 50.4, 50 | 19 | 54–75, 67.2, 71 | 6, 13 | 1–10, 4.7, 2 |
| FCs | 21–65, 48.7, 48 | 17 | 30–88, 64.2, 64 | 13, 4 | - |
| 1. Everyone’s Parkinson is different | 1.1. Different symptoms and disease duration 1.2. Different perception of the disease 1.3. Different reaction to drugs 1.4. Different difficulties and changes that led to different daily routines 1.5. Different impact on the family and couple relationships and on social life 1.6. Different coping strategies |
| 2. Changing through PD together | |
| 3. Changing as a person during the disease | |
| 4. DBS improved my life | |
| 5. I am treated with DBS, but I still have PD | |
| 6. DBS is not perfect | |
| 7. Being different after DBS |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Chacón Gámez, Y.M.; Brugger, F.; Biller-Andorno, N. Parkinson’s Disease and Deep Brain Stimulation Have an Impact on My Life: A Multimodal Study on the Experiences of Patients and Family Caregivers. Int. J. Environ. Res. Public Health 2021, 18, 9516. https://doi.org/10.3390/ijerph18189516
Chacón Gámez YM, Brugger F, Biller-Andorno N. Parkinson’s Disease and Deep Brain Stimulation Have an Impact on My Life: A Multimodal Study on the Experiences of Patients and Family Caregivers. International Journal of Environmental Research and Public Health. 2021; 18(18):9516. https://doi.org/10.3390/ijerph18189516
Chicago/Turabian StyleChacón Gámez, Yolanda María, Florian Brugger, and Nikola Biller-Andorno. 2021. "Parkinson’s Disease and Deep Brain Stimulation Have an Impact on My Life: A Multimodal Study on the Experiences of Patients and Family Caregivers" International Journal of Environmental Research and Public Health 18, no. 18: 9516. https://doi.org/10.3390/ijerph18189516
APA StyleChacón Gámez, Y. M., Brugger, F., & Biller-Andorno, N. (2021). Parkinson’s Disease and Deep Brain Stimulation Have an Impact on My Life: A Multimodal Study on the Experiences of Patients and Family Caregivers. International Journal of Environmental Research and Public Health, 18(18), 9516. https://doi.org/10.3390/ijerph18189516