
Variation of Cancer Incidence between and within GRELL Countries

 ,
,  , ,
, , 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Incidence
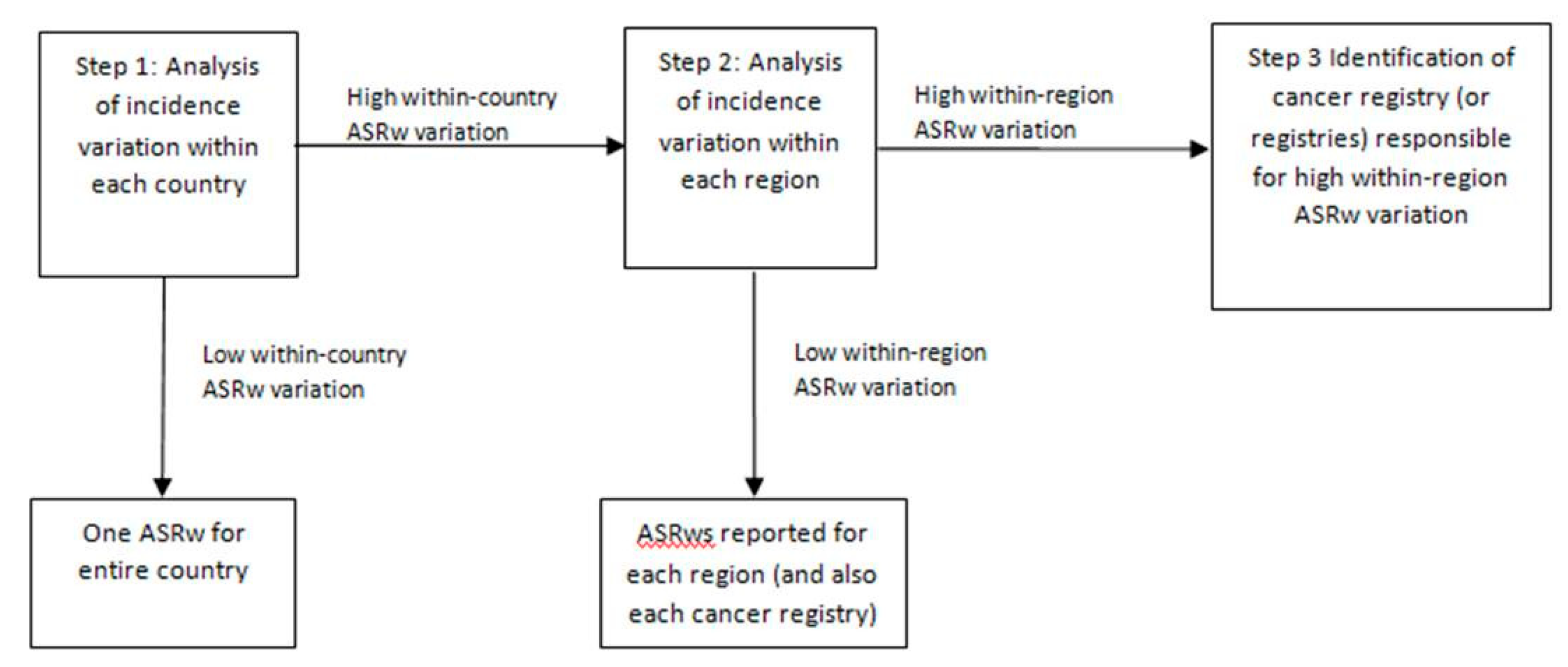
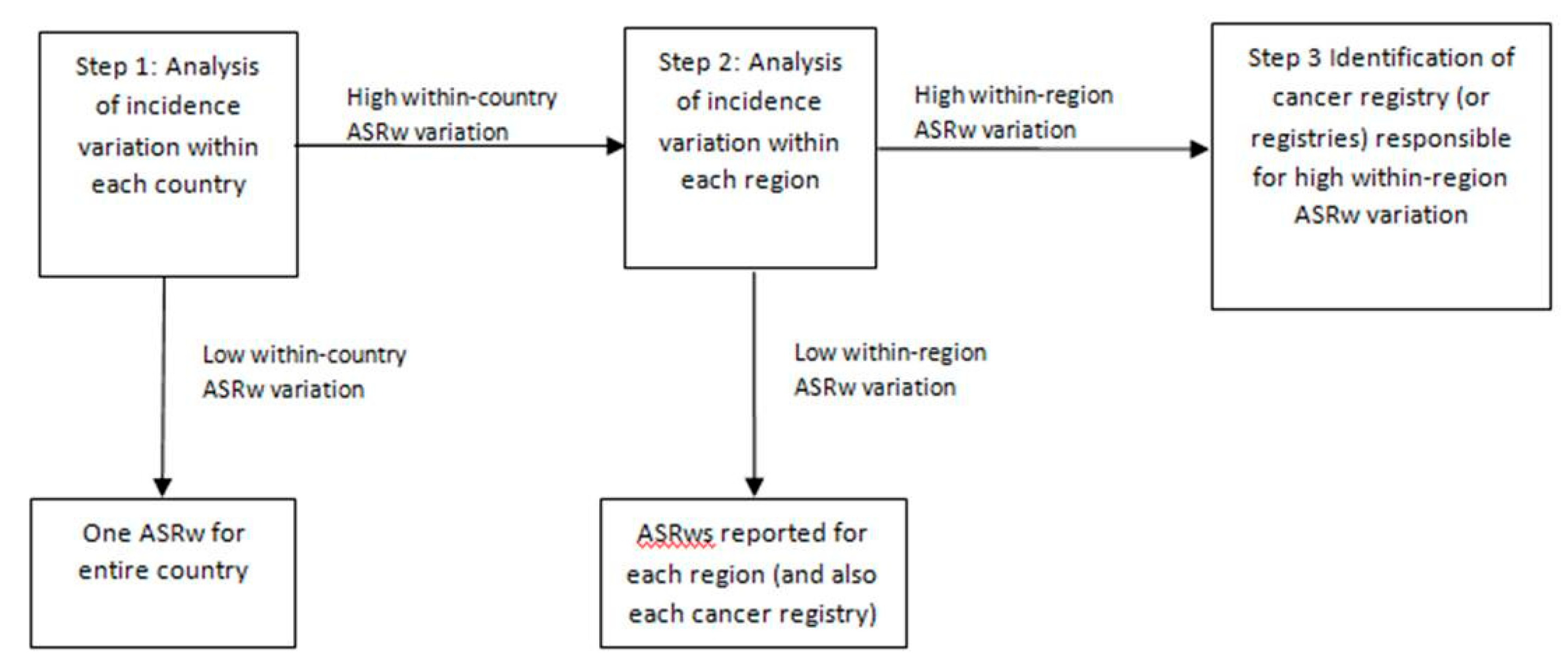
2.2. Within-Country Incidence Variation
3. Results
3.1. Breakdown of Countries into Regions According to r/R
3.2. Country and Regional Incidence Rates
3.2.1. Males
3.2.2. Females
3.2.3. Comparisons
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Global Cancer Observatory (IARC): Global Cancer Burden in 2020. Available online: https://infogram.com/globocan-2020-1h9j6qg7xdp8v4g?live (accessed on 26 August 2021).
- Group for Cancer Epidemiology and Registration in Latin Language Countries. Available online: https://www.grell-network.org (accessed on 26 August 2021).
- International Agency for the Research on Cancer, Global Cancer Observatory. Available online: https://gco.iarc.fr/causes/obesity (accessed on 26 August 2021).
- International Agency for the Research on Cancer, Global Cancer Observatory. Available online: https://gco.iarc.fr/causes/infections (accessed on 26 August 2021).
- International Agency for the Research on Cancer, Global Cancer Observatory. Available online: https://gco.iarc.fr/causes/uv (accessed on 26 August 2021).
- Van Donkelaar, A.; Martin, R.V.; Brauer, M.; Boys, B.L. Use of satellite observations for long-term exposure assessment of global concentrations of fine particulate matter. Environ. Health Perspect. 2015, 123, 135–143. [Google Scholar] [CrossRef] [Green Version]
- Miranda-Filho, A.; Piñeros, M.; Ferlay, J.; Soerjomataram, I.; Monnereau, A.; Bray, F. Global patterns and trends in the incidence of non- Hodgkin lymphoma. Cancer Causes Control 2019, 30, 489–499. [Google Scholar] [CrossRef]
- Miranda-Filho, A.; Piñeros, M.; Ferlay, J.; Soerjomataram, I.; Monnereau, A.; Bray, F. Epidemiological patterns of leukaemia in 184 countries: A population-based study. Lancet Haematol. 2018, 5, e14–e24. [Google Scholar] [CrossRef]
- Steliarova-Foucher, E.; Fidler, M.M.; Colombet, M.; Lacour, B.; Kaatsch, P.; Piñeros, M.; Soerjomataram, I.; Bray, F.; Coebergh, J.W.; Peris-Bonet, R.; et al. ACCIS contributors. Changing geographical patterns and trends in cancer incidence in children and adolescents in Europe, 1991-2010 (Automated Childhood Cancer Information System): A population-based study. Lancet Oncol. 2018, 19, 1159–1169. [Google Scholar] [CrossRef] [Green Version]
- Bell, J.S.; Koffie, R.M.; Rattani, A.; Dewan, M.C.; Baticulon, R.E.; Qureshi, M.M.; Wahjoepramono, E.J.; Rosseau, G.; Park, K.; Nahed, B.V. Global incidence of brain and spinal tumors by geographic region and income level based on cancer registry data. J. Clin. Neurosci. 2019, 66, 121–127. [Google Scholar] [CrossRef]
- Cancer Incidence in Five Continents. Vol XI. Available online: http://ci5.iarc.fr/CI5-XI/Default.aspx (accessed on 26 August 2021).
- Bray, F.; Colombet, M.; Mery, L.; Piñeros, M.; Znaor, A.; Zanetti, R.; Ferlay, J. (Eds.) Cancer Incidence in Five Continents, Volume XI (Electronic Version); International Agency for Research on Cancer: Lyon, France, 2017; Available online: http://ci5.iarc.fr (accessed on 26 August 2021).
- Crocetti, E.; Giusti, F.; Martos, C.; Randi, G.; Dyba, T.; Bettio, M. Variability of cancer risk within an area: Time to complement the incidence rate. Eur. J. Cancer Prev. 2017, 26, 442–444. [Google Scholar] [CrossRef] [Green Version]
- Li, P.; Znaor, A.; Holcatova, I.; Fabianova, E.; Mates, D.; Wozniak, M.B.; Ferlay, J.; Scelo, G. Regional geographic variations in kidney cancer incidence rates in European countries. Eur. Urol. 2015, 67, 1134–1141. [Google Scholar] [CrossRef] [PubMed]
- GBD 2019 Respiratory Tract Cancers Collaborators. Global, regional, and national burden of respiratory tract cancers and associated risk factors from 1990 to 2019: A systematic analysis for the Global Burden of Disease Study 2019. Lancet Respir. Med. 2021, 16, S2213–S2600. [Google Scholar]
- Arnold, M.; Pandeya, N.; Byrnes, G.; Renehan, P.A.G.; Stevens, G.A.; Ezzati, P.M.; Ferlay, J.; Miranda, J.J.; Romieu, I.; Dikshit, R.; et al. Global burden of cancer attributable to high body-mass index in 2012: A population-based study. Lancet Oncol. 2015, 16, 36–46. [Google Scholar] [CrossRef]
- Giampaoli, S.; Krogh, V.; Grioni, S.; Palmieri, L.; Gulizia, M.M.; Stamler, J.; Vanuzzo, D. Gruppo di ricerca dell′Osservatorio epidemiologico cardiovascolare/Health Examination Survey. Comportamenti alimentari degli italiani: Risultati dell′Osservatorio epidemiologico cardiovascolare/Health Examination Survey [Eating behaviours of italian adults: Results of the Osservatorio epidemiologico cardiovascolare/Health Examination Survey]. Epidemiol. Prev. 2015, 39, 373–379. [Google Scholar] [PubMed]
- Available online: https://en.wikipedia.org/wiki/Florianópolis (accessed on 26 August 2021).
- Sierra, M.S.; Soerjomataram, I.; Antoni, S.; Laversanne, M.; Piñeros, M.; de Vries, E.; Forman, D. Cancer patterns and trends in Central and South America. Cancer Epidemiol. 2016, 44 (Suppl. 1), S23–S42. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pardo, C.; Bravo, L.E.; Uribe, C.; Lopez, G.; Yepez, M.C.; Navarro, E.; de Vries, E.; Pineros, M. Comprehensive assessment of population-based cancer registries: An experience in Colombia. J. Regist. Manag. 2014, 41, 128–134. [Google Scholar]
- Cendales, R.; Pardo, C.; Uribe, C.; López, G.; Yepez, M.C.; Bravo, L.E. Data quality at population-based cancer registries in Colombia. Biomedica 2012, 32, 536–544. [Google Scholar] [CrossRef]
- Vineis, P.; Wild, C.P. Global cancer patterns: Causes and prevention. Lancet 2014, 383, 549–555. [Google Scholar] [CrossRef]
- Plummer, M.; de Martel, C.; Vignat, J.; Ferlay, J.; Bray, F.; Franceschi, S. Global burden of cancers attributable to infections in 2012: A synthetic analysis. Lancet Glob. Health 2016, 4, e609–e616. [Google Scholar] [CrossRef] [Green Version]
- Prüss-Ustün, A.; Wolf, J.; Corvalán, C.; Neville, T.; Bos, R.; Neira, M. Diseases due to unhealthy environments: An updated estimate of the global burden of disease attributable to environmental determinants of health. J. Public Health 2017, 39, 464–475. [Google Scholar] [CrossRef] [PubMed]
- Raaschou-Nielsen, O.; Andersen, Z.J.; Beelen, R.; Samoli, E.; Stafoggia, M.; Weinmayr, G.; Hoffmann, B.; Fischer, P.; Nieuwenhuijsen, M.J.; Brunekreef, B.; et al. Air pollution and lung cancer incidence in 17 European cohorts: Prospective analyses from the European Study of Cohorts for Air Pollution Effects (ESCAPE). Lancet Oncol. 2013, 14, 813–822. [Google Scholar] [CrossRef]
- De Souza, J.A.; Hunt, B.; Asirwa, F.C.; Adebamowo, C.; Lopes, G. Global health equity: Cancer care outcome disparities in high-, middle-, and low-income countries. J. Clin. Oncol. 2016, 34, 6–13. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Vaccarella, S.; Lortet-Tieulent, J.; Saracci, R.; Fidler, M.M.; Conway, D.I.; Vilahur, N.; Sarfati, D.; Jemal, A.; Mackenbach, J.P.; Marmot, M.G.; et al. Reducing Social Inequalities in Cancer: Setting Priorities for Research. CA Cancer J. Clin. 2018, 68, 324–326. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Vaccarella, S.; De Vries, E.; Sierra, M.S.; Conway, D.I.; Mackenbach, J.P. Chapter 6: Social inequalities in cancer within countries. In Reducing Social Inequalities in Cancer: Evidence and Priorities for Research; Vaccarella, S., Lortet-Tieulent, J., Saracci, R., Conway, D.I., Straif, K., Wild, C.P., Eds.; IARC Scientific Publications: Lyon, France, 2019. [Google Scholar]
- Fidler, M.M.; Vaccarella, S.; Bray, F. Social inequalities in cancer between countries. In Reducing Social Inequalities in Cancer: Evidence and Priorities for Research; Vaccarella, S., Lortet-Tieulent, J., Saracci, R., Conway, D.I., Straif, K., Wild, C.P., Eds.; IARC Scientific Publications: Lyon, France, 2019. [Google Scholar]
- Goss, P.E.; Lee, B.L.; Badovinac-Crnjevic, T.; Strasser-Weippl, K.; Chavarri-Guerra, Y.; St Louis, J.; Villarreal-Garza, C.; Unger-Saldaña, K.; Ferreyra, M.; Debiasi, M.; et al. Planning cancer control in Latin America and the Caribbean. Lancet Oncol. 2013, 14, 391–436. [Google Scholar] [CrossRef] [PubMed]
- EPA (United States Environmental Protection Agency): Environmental Justice. Available online: https://www.epa.gov/environmentaljustice/learn-about-environmental-justice (accessed on 26 August 2021).
- Fairburn, J.; Schüle, S.A.; Dreger, S.; Karla Hilz, L.; Bolte, G. Social Inequalities in Exposure to Ambient Air Pollution: A Systematic Review in the WHO European Region. Int. J. Environ. Res. Public Health 2019, 16, 3127. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cancer Incidence in Five Continents. Chapter 5: Data Comparability and Quality. Available online: https://ci5.iarc.fr/CI5-XI/PDF/Chapter%205.pdf (accessed on 26 August 2021).
- ECIS—European Cancer Information System. Available online: https://ecis.jrc.ec.europa.eu/explorer.php (accessed on 26 August 2021).

{kind=link}
| 1A | 1B | ||
|---|---|---|---|
| Country | Incidence Males | Country | Incidence Females |
| Portugal (Azores) | 381.92 | Belgium * | 289.21 |
| France | 369.35 | Italy | 264.22 |
| Belgium * | 364.28 | Switzerland | 261.41 |
| Spain | 339.97 | France | 258.36 |
| Switzerland | 338.22 | Uruguay * | 216.77 |
| Italy | 331.81 | Spain | 210.56 |
| Uruguay * | 289.56 | Portugal (Azores) | 209.67 |
| Brazil | 272.58 | Argentina | 201.16 |
| Puerto Rico * | 258.28 | Brazil | 199.34 |
| Argentina | 215.22 | Puerto Rico * | 197.95 |
| Chile | 209.75 | Peru (Lima) | 187.51 |
| Peru (Lima) | 187.04 | Chile | 174.99 |
| Colombia | 179.15 | Colombia | 171.71 |
| Costa Rica * | 173.90 | Costa Rica * | 167.25 |
| Ecuador | 135.11 | Ecuador | 152.43 |
| Region | Incidence Males | Region | Incidence Females |
|---|---|---|---|
| Azores, Portugal | 381.92 | Florianopolis, Brazil * | 338.43 |
| Florianopolis, Brazil * | 380.33 | Belgium ** | 289.21 |
| Metropolitan France | 372.25 | North-east Italy | 281.59 |
| Belgium ** | 364.28 | Central Italy | 268.03 |
| North-east Spain | 357.91 | North-west Italy | 267.75 |
| North-east Italy | 346.53 | Metropolitan France | 262.20 |
| North-west Italy | 343.67 | Switzerland | 261.41 |
| Switzerland | 338.22 | South Italy | 240.80 |
| Central Italy | 324.55 | Islands of Italy | 237.76 |
| South Italy | 317.03 | Uruguay ** | 216.77 |
| South Spain | 308.34 | Spain | 210.56 |
| Overseas France | 304.79 | Azores, Portugal | 209.67 |
| Central Brazil | 301.67 | North-east Brazil | 208.57 |
| Islands of Italy | 292.27 | Central Argentina | 207.66 |
| Uruguay ** | 289.56 | South Ecuador | 206.51 |
| North-east Brazil | 281.88 | Central-north Ecuador | 199.11 |
| Puerto Rico ** | 258.28 | Puerto Rico ** | 197.95 |
| South Brazil | 235.58 | Central Brazil | 194.18 |
| Central Argentina | 222.12 | Lima (Peru) | 187.51 |
| Chile | 209.75 | Overseas France | 181.03 |
| Cali,* Colombia | 204.49 | South Brazil | 179.99 |
| Central-north Ecuador | 192.79 | Chile | 174.99 |
| North Argentina | 189.68 | North Argentina | 174.77 |
| Lima (Peru) | 187.04 | Costa Rica ** | 167.25 |
| Costa Rica ** | 173.90 | Colombia | 171.71 |
| South Argentina | 173.24 | South Argentina | 149.16 |
| South Ecuador | 168.50 | Central Ecuador | 144.88 |
| Rest of Colombia | 149.97 | Pacific Ecuador | 102.32 |
| Central Ecuador | 125.43 | ||
| Pacific Ecuador | 89.45 |
| Countries | Regions | Cancer Registries | |
|---|---|---|---|
| Males | 2.8 | 4.3 | 4.8 |
| Females | 1.9 | 3.3 | 3.3 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Contiero, P.; Tagliabue, G.; Gatta, G.; Galceran, J.; Bulliard, J.-L.; Bertoldi, M.; Scaburri, A.; Crocetti, E.; on behalf of the GRELL Geographic Analysis Working Group. Variation of Cancer Incidence between and within GRELL Countries. Int. J. Environ. Res. Public Health 2021, 18, 9262. https://doi.org/10.3390/ijerph18179262
Contiero P, Tagliabue G, Gatta G, Galceran J, Bulliard J-L, Bertoldi M, Scaburri A, Crocetti E, on behalf of the GRELL Geographic Analysis Working Group. Variation of Cancer Incidence between and within GRELL Countries. International Journal of Environmental Research and Public Health. 2021; 18(17):9262. https://doi.org/10.3390/ijerph18179262
Chicago/Turabian StyleContiero, Paolo, Giovanna Tagliabue, Gemma Gatta, Jaume Galceran, Jean-Luc Bulliard, Martina Bertoldi, Alessandra Scaburri, Emanuele Crocetti, and on behalf of the GRELL Geographic Analysis Working Group. 2021. "Variation of Cancer Incidence between and within GRELL Countries" International Journal of Environmental Research and Public Health 18, no. 17: 9262. https://doi.org/10.3390/ijerph18179262
APA StyleContiero, P., Tagliabue, G., Gatta, G., Galceran, J., Bulliard, J.-L., Bertoldi, M., Scaburri, A., Crocetti, E., & on behalf of the GRELL Geographic Analysis Working Group. (2021). Variation of Cancer Incidence between and within GRELL Countries. International Journal of Environmental Research and Public Health, 18(17), 9262. https://doi.org/10.3390/ijerph18179262