
New Growth Curves for Spanish Children (0–10 Years) in the Region of Extremadura



 ,
,  ,
,  and
and
Abstract
:1. Introduction
1.1. Objectives and Hypotheses
- Develop growth tables that reflect the somatometric variables of children in Extremadura.
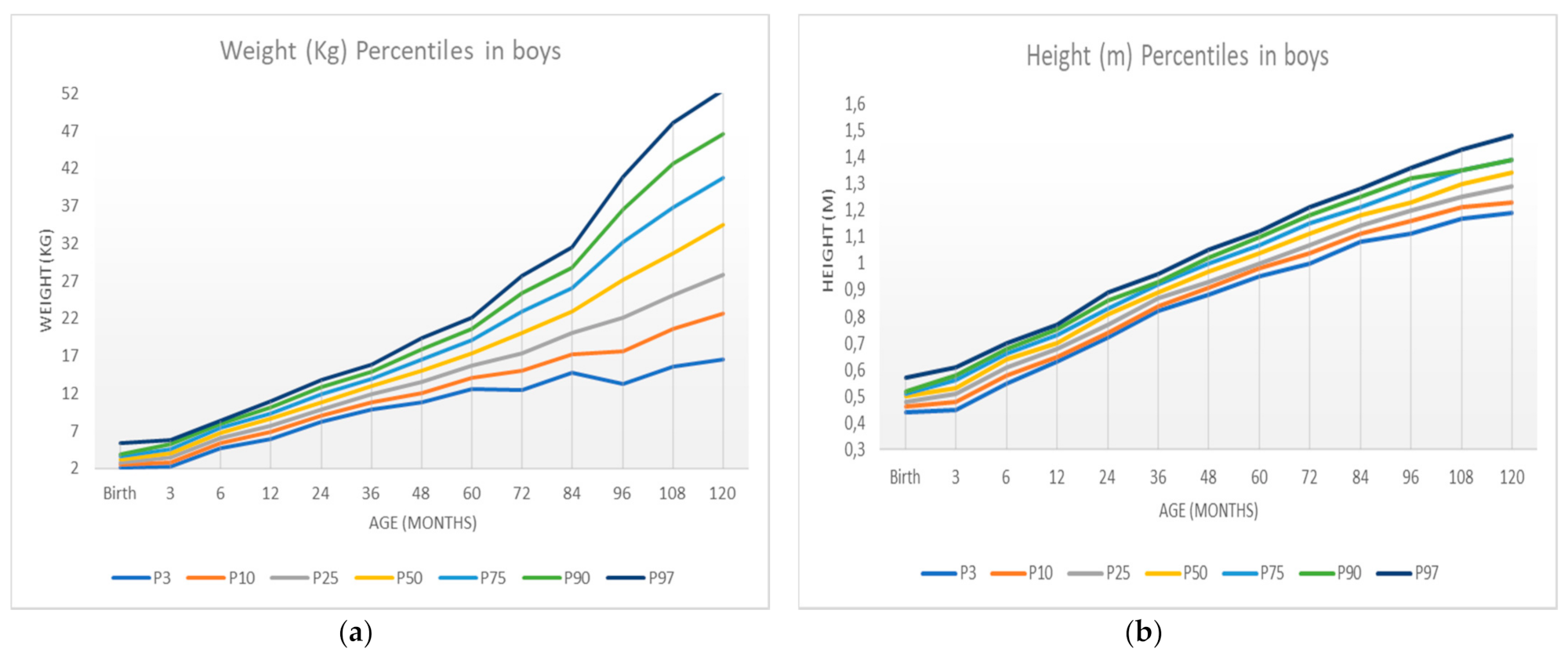
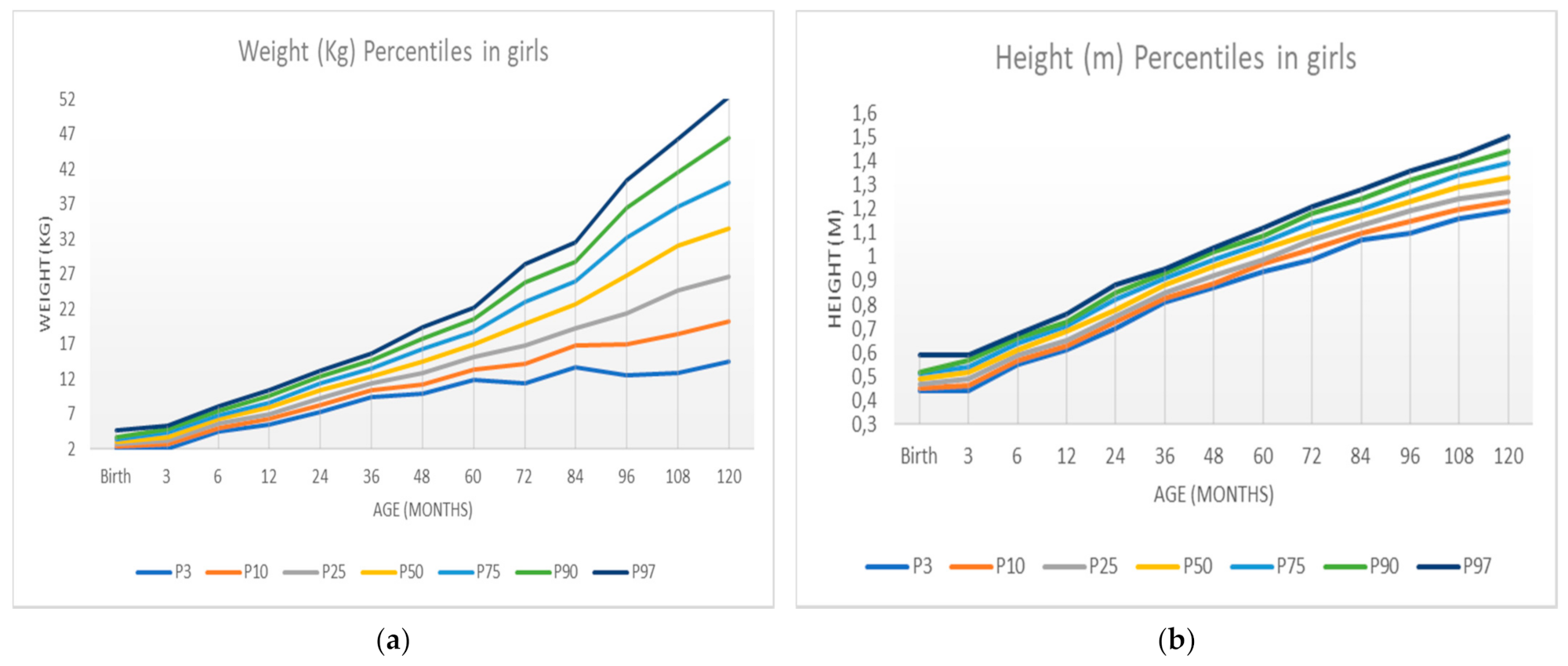
- Develop graphs that reflect the somatometric variables of children in Extremadura.
- Compare the average of these variables by sex.
- Determine if there are significant differences between boys and girls.
- Children born in different parts of the autonomous community of Extremadura between 2006 and 2016 were selected.
- It is assumed that we have a sufficiently representative sample of subjects to correctly elaborate the tables and growth curves. For this purpose, we used a convenience sample with a power of 95%.
- The weight and height of the subjects was obtained by their Primary Health Care Center.
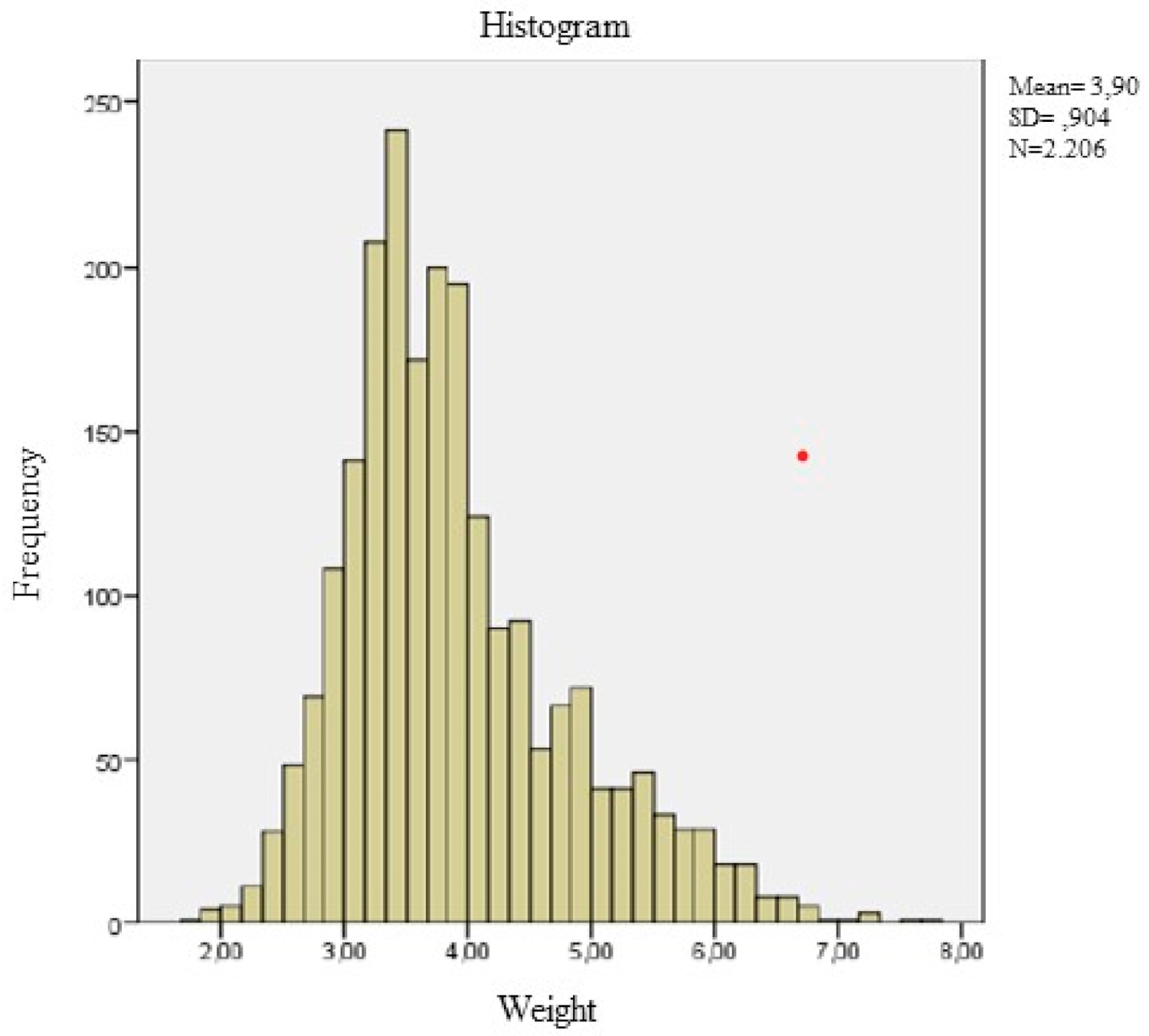
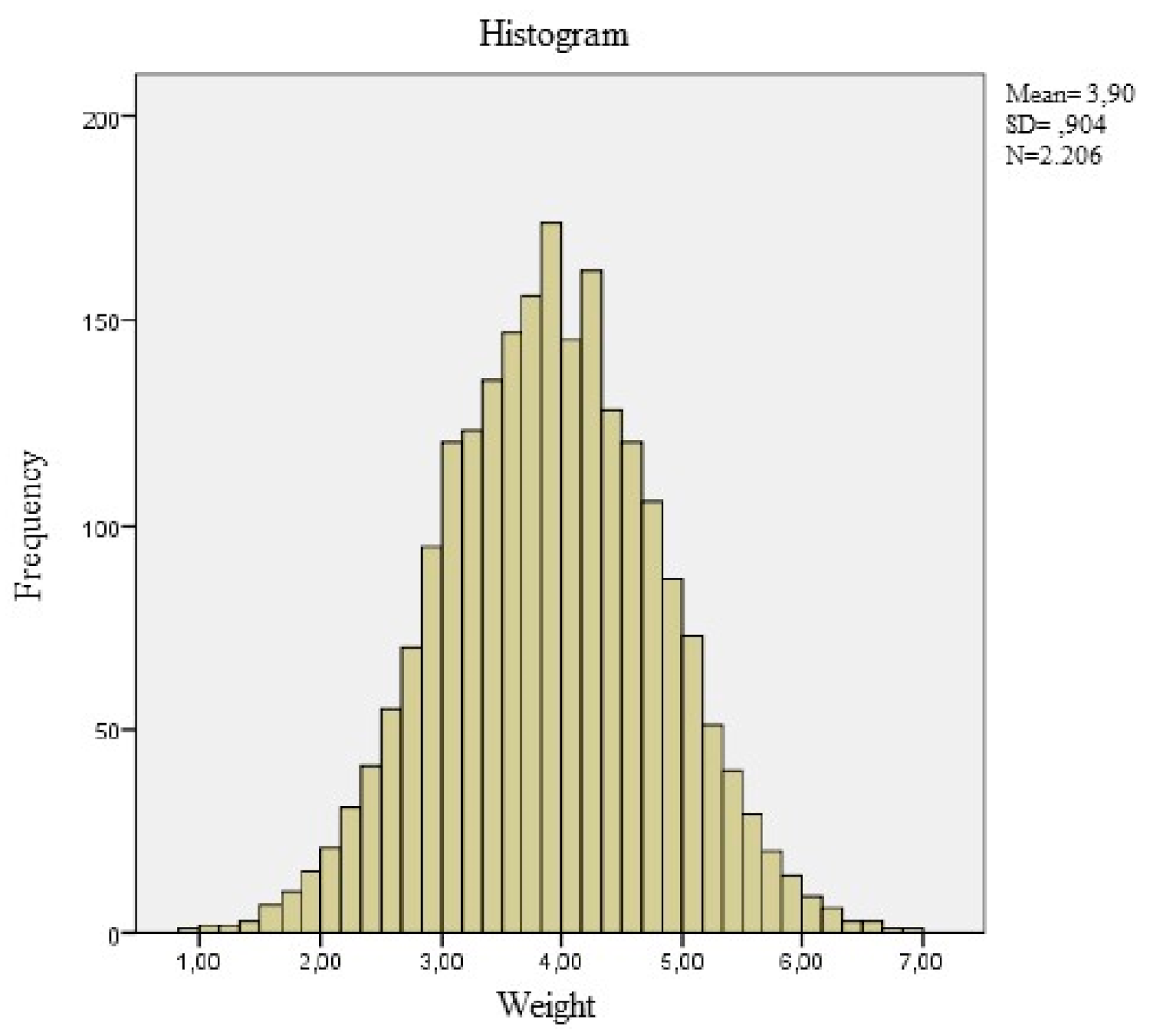
- The normality of the variables studied is verified. If this is not the case, we must correct the asymmetry of the variable by the Two-Step Transformation Procedure described below, with the help of the statistical software SPSS.
1.2. Methodology
2. Materials and Methods
2.1. Study Design
2.2. Participants
2.3. Measures and Procedures
2.4. Statistical Analysis
- Assign a fractional range to the variable and generate a new variable with this range assignment.
- Calculation of a new variable. This is acheived by selecting it in the function group panel GL Inverse and within this category “Idf. Normal”. This function requires three parameters: the variable generated in step 1, the mean, and standard deviation of the original variable.
Construction of a Percentile Table for the Variable Weight Using the GAMLSS Package in R
3. Results
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Longmuir, P.E.; Boyer, C.; Lloyd, M.; Borghese, M.M.; Knight, E.; Saunders, T.J. Tremblay canadian agility and movement skill assessment (camsa): Validity, objectivity, and reliability evidence for children 8–12 years of age. J. Sport Health Sci. 2000, 320, 6. [Google Scholar]
- Cole, T.J. The development of growth references and growth charts. Ann. Hum. Biol. 2012, 39, 382–394. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Perkins, J.M.; Subramanian, S.V.; Davey Smith, G.; Özaltin, E. Adult height, nutrition, and population health. Nutr. Rev. 2016, 74, 149–165. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Waterlow, J.C.; Buzina, R.; Keller, W.; Lane, J.M.; Nichaman, M.Z.; Tanner, J.M. The presentation and use of height and weight data for comparing the nutritional status of groups ot children under the age of 10 years. Bull. WHO 1977, 55, 489. [Google Scholar] [PubMed]
- Hernández, M.; Castellet, J.; Narvaiza, J.L.; Rincón, J.M.; Ruiz, E.; Sánchez, E.; Sobradillo, B.; Zurimendi, A. Curvas y Tablas de Crecimiento, 2nd ed.; Hernández Rodríguez, M., Orbegozo, F.F., Eds.; Instituto de Investigación Sobre Crecimiento y Desarrollo: Bilbao, Spain, 1988; ISBN 978-84-7391-177-1. [Google Scholar]
- Hernández Martínez, A.M.; Tebar Massó, F.J.; Serrano Corredor, S.; Alvarez Cantalapiedra, L.; Illán Gómez, F.; Valdés Chavarri, M. Estudio antropométrico de la población escolar de La Comunidad Autónoma de Murcia. Med. Clin. 1992, 98, 651–655. [Google Scholar]
- López-Siguero, J.P.; García, J.M.F.; de Dios, J.; Castillo, L.; Molina, J.A.M.; Cosano, C.R.; Ortiz, A.J. Cross-sectional study of height and weight in the population of Andalusia from age 3 to adulthood. BMC Endocr. Disord. 2008, 8, S1. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sobradillo, B.; Aguirre, A.; Aresti, U.; Bilbao, A.; Fernández-Ramos, C.; Lizárraga, A.; Lorenzo, H.; Madariaga, L.; Rica, I.; Ruiz, I.; et al. Curvas y Tablas de Crecimiento. Estudio Longitudinal y Transversal; Instituto de Investigación Sobre Crecimiento y Desarrollo: Bilbao, Spain, 2004. [Google Scholar]
- Ángel, M. Nivel de desarrollo humano en las Ciudades Autónomas españolas: Comparativos con las CC.AA. y Marruecos. Anal. ASEPUMA 2017, 25, 20. [Google Scholar]
- Indrayan, A. Demystifying LMS and BCPE methods of centile estimation for growth and other health parameters. Indian Pediatr. 2014, 51, 37–43. [Google Scholar] [CrossRef] [PubMed]
- García-Muñoz Rodrigo, F.; García-Alix Pérez, A.; Figueras Aloy, J.; Saavedra Santana, P. Nuevas curvas poblacionales de crecimiento en recién nacidos extremadamente prematuros españoles. An. Pediatr. 2014, 81, 107–114. [Google Scholar] [CrossRef] [PubMed]
- Templeton, G.F. A two-step approach for transforming continuous variables to normal: Implications and recommendations for is research. Commun. Assoc. Inf. Syst. 2011, 28, 4. [Google Scholar] [CrossRef] [Green Version]
- Stasinopoulos, D.M.; Rigby, R.A.; Akantziliotou, C. Instructions on How to Use the GAMLSS Package in R. 2008. Available online: http://www.gamlss.com/wp-content/uploads/2013/01/gamlss-manual.pdf (accessed on 23 August 2021).
- Rubén Quesada, M.; Rodríguez Chávez, L.E.; Esquivel Lauzurique, M.; Carmona, M.O. Experiencia en el uso de R para el ajuste de curvas de crecimiento. Rev. Cuba Info. Méd. 2011, 3, 9. [Google Scholar]
- Onis, M. WHO child growth standards based on length/height, weight and age: WHO child growth standards. Acta Paediatr. 2007, 95, 76–85. [Google Scholar] [CrossRef]
- Beatriz Oves Suárez, M.P.S.V.; Laura Escartín Madurga, M.; Luisa Álvarez, A. Tendencia secular del crecimiento durante la primera infancia en el norte de España. Nutr. Hosp. 2013, 28, 1985–1992. [Google Scholar] [CrossRef]
- Sánchez González, E.; Carrascosa Lezcano, A.; Fernández García, J.M.; Ferrández Longás, A.; López de Lara, D.; López-Siguero, J.P. Estudios españoles de crecimiento: Situación actual, utilidad y recomendaciones de uso. An. Pediatr. 2011, 74, 193.e1–1993.e16. [Google Scholar] [CrossRef] [PubMed]
- Bonthuis, M.; van Stralen, K.J.; Verrina, E.; Edefonti, A.; Molchanova, E.A.; Hokken-Koelega, A.C.S.; Schaefer, F.; Jager, K.J. Use of national and international growth charts for studying height in european children: Development of up-to-date european height-for-age charts. PLoS ONE 2012, 7, e42506. [Google Scholar] [CrossRef] [PubMed]
- WHO. Recommendations for Data Collection, Analysis and Reporting on Anthropometric Indicators in Children under 5 Years Old; Organización Mundial de la Salud y el Fondo de las Naciones Unidas para la Infancia (UNICEF): Geneva, Switzerland, 2019. [Google Scholar]
- Ogden, C.L. Prevalence of high body mass index in us children and adolescents, 2007–2008. JAMA 2010, 303, 242. [Google Scholar] [CrossRef] [PubMed] [Green Version]



{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variables | Differences | Birth | 3 | 6 | 12 | 24 | 36 | ||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Boys | Girl | Boys | Girls | Boys | Girls | Boys | Girls | Boys | Girls | Boys | Girls | ||
| Original Weight | p-value | 0.200 | 0.191 | 0.000 | 0.000 | 0.043 | 0.060 | 0.000 | 0.009 | 0.000 | 0.100 | 0.000 | 0.000 |
| Kurtosis | NA | NA | 0.588 | 0.728 | NA | NA | 8.248 | NA | 0.520 | NA | 3.829 | 4.298 | |
| Asymmetry | NA | NA | 0.892 | 0.834 | NA | NA | 0.040 | NA | 0.602 | NA | 1.209 | 1.388 | |
| Original Height | p-value | 0.000 | 0.000 | 0.000 | 0.000 | 0.000 | 0.000 | 0.000 | 0.000 | 0.000 | 0.000 | 0.000 | 0.000 |
| Kurtosis | NA | NA | 7.53 | −0.79 | 1.016 | −0.258 | 0.333 | 3.299 | 3.865 | 3.299 | 1.549 | 1.628 | |
| Asymmetry | NA | NA | 1.23 | −0.837 | −0.577 | −1.358 | 0.143 | −0.461 | −0.167 | −0.350 | 0.499 | 0.556 | |
| Treaty Weight | p-value | NA | NA | 0.200 | NA | NA | NA | 0.200 | NA | 0.009 | NA | 0.000 | 0.000 |
| Kurtosis | NA | NA | −0.77 | −0.79 | −0.175 | −0.258 | −0.164 | −0.076 | −0.104 | −0.127 | −0.009 | −0.013 | |
| Asymmetry | NA | NA | 0.011 | 0.001 | NA | NA | −0.143 | NA | 0.163 | NA | 0.008 | 0.020 | |
| Treaty Height | p-value | 0.000 | 0.000 | 0.000 | 0.000 | 0.000 | 0.006 | 0.005 | 0.013 | 0.000 | 0.001 | 0.000 | 0.000 |
| Kurtosis | NA | NA | −0.77 | −0.79 | −0.175 | −0.258 | −0.164 | −0.076 | −0.104 | −0.127 | −0.009 | −0.013 | |
| Asymmetry | NA | NA | 0.006 | 0.005 | −0.020 | −0.035 | 0.002 | 0.055 | 0.000 | −0.001 | 0.007 | 0.007 | |
| Variables | Differences | 48 | 60 | 72 | 84 | 96 | 108 | 120 | |||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Boys | Girl | Boys | Girls | Boys | Girls | Boys | Girls | Boys | Girls | Boys | Girls | Boys | Girl | ||
| Original Weight | p-value | 0.000 | 0.000 | 0.000 | 0.000 | 0.000 | 0.000 | 0.000 | 0.000 | 0.000 | 0.000 | 0.000 | 0.000 | 0.000 | 0.000 |
| Kurtosis | 5.505 | 6.309 | 2.440 | 2.161 | 2.502 | 1.810 | 2.315 | 2.202 | 2.039 | 0.821 | 1.525 | 0.281 | 1.487 | 1.933 | |
| Asymmetry | 1.460 | 1.622 | 1.078 | 1.065 | 1.366 | 1.296 | 1.289 | 1.254 | 1.319 | 1.030 | 1.245 | 0.829 | 1.125 | 1.243 | |
| Original Height | p-value | 0.000 | 0.000 | 0.000 | 0.000 | 0.000 | 0.000 | 0.000 | 0.000 | 0.000 | 0.000 | 0.000 | 0.001 | 0.000 | 0.000 |
| Kurtosis | 1.871 | 2.792 | 0.789 | 1.182 | 0.200 | 0.056 | 0.871 | 2.059 | −0.055 | −0.138 | 0.595 | −0.038 | 24.693 | 31.104 | |
| Asymmetry | 0.493 | 0.672 | 0.130 | 0.296 | 0.134 | 0.088 | 0.239 | 0.401 | 0.009 | 0.107 | 0.059 | 0.001 | −2.273 | −2.616 | |
| Treaty Weight | p-value | 0.000 | 0.000 | 0.000 | 0.000 | 0.004 | 0.017 | 0.000 | 0.000 | 0.200 | 0.200 | 0.200 | 0.200 | 0.200 | 0.200 |
| Kurtosis | −0.002 | −0.025 | −0.001 | −0.002 | −0.045 | −0.046 | −0.014 | −0.017 | −0.056 | −0.058 | −0.078 | −0.015 | −0.127 | −0.128 | |
| Asymmetry | 0.007 | 0.000 | 0.003 | 0.004 | 0.000 | 0.000 | 0.001 | 0.000 | 0.001 | 0.000 | 0.001 | 0.027 | 0.002 | −0.001 | |
| Treaty Height | p-value | 0.000 | 0.000 | 0.000 | 0.000 | 0.000 | 0.000 | 0.000 | 0.000 | 0.000 | 0.000 | 0.001 | 0.005 | 0.015 | 0.200 |
| Kurtosis | 0.004 | −0.019 | 0.006 | −0.003 | −0.005 | −0.010 | −0.012 | −0.012 | −0.062 | −0.063 | −0.077 | 0.014 | −0.121 | −0.123 | |
| Asymmetry | 0.010 | 0.004 | 0.04 | 0.003 | 0.013 | 0.015 | 0.001 | 0.001 | 0.000 | 0.002 | 0.000 | 0.027 | −0.001 | −0.001 | |
| Height | |||||
|---|---|---|---|---|---|
| Age | Boys | Girls | p | ||
| n | Mean ± SD | n | Mean ± SD | ||
| Birth | 441 | 0.49 ± 0.27 | 376 | 0.48 ± 0.25 | <0.001 |
| 3 Months | 1176 | 0.53 ± 0.03 | 1031 | 0.52 ± 0.38 | <0.001 |
| 6 Months | 316 | 0.63 ± 0.03 | 234 | 0.61 ± 0.31 | <0.000 |
| 12 Months | 397 | 0.70 ± 0.03 | 335 | 0.68 ± 0.04 | <0.000 |
| 24 Months | 807 | 0.80 ± 0.44 | 627 | 0.79 ± 0.04 | <0.000 |
| 36 Months | 11,267 | 0.89 ± 0.37 | 9930 | 0.88 ± 0.38 | <0.000 |
| 48 Months | 8148 | 0.96 ± 0.04 | 7253 | 0.95± 0.04 | <0.000 |
| 60 Months | 22,461 | 1.04 ± 0.04 | 20,561 | 1.03 ± 0.04 | 0.000 |
| 72 Months | 3682 | 1.11 ± 0.05 | 3189 | 1.10 ± 0.05 | 0.000 |
| 84 Months | 15,593 | 1.17 ± 0.05 | 14,415 | 1.17 ± 0.05 | 0.000 |
| 96 Months | 2235 | 1.24 ± 0.06 | 2130 | 1.23 ± 0.06 | 0.000 |
| 108 Months | 1338 | 1.29 ± 0.07 | 1275 | 1.29 ± 0.07 | 0.005 |
| 120 Months | 656 | 1.34 ± 0.07 | 624 | 1.33 ± 0.08 | 0.159 |
| Weight | |||||
|---|---|---|---|---|---|
| Age | Boys | Girls | p | ||
| n | Mean ± SD | n | Mean ± SD | ||
| Birth | 441 | 3.2 ± 0.55 | 376 | 3.05 ± 0.25 | 0.000 |
| 3 Months | 1176 | 4.02 ± 0.92 | 1031 | 3.76 ± 0.86 | 0.000 |
| 6 Months | 316 | 6.71 ± 0.98 | 234 | 6.31 ± 0.95 | 0.000 |
| 12 Months | 397 | 8.54 ± 1.27 | 335 | 7.92 ± 1.28 | 0.000 |
| 24 Months | 807 | 10.94 ± 1.44 | 627 | 10.33 ± 1.54 | 0.000 |
| 36 Months | 11,267 | 12.90 ± 1.61 | 9930 | 12.48 ± 1.59 | 0.000 |
| 48 Months | 8148 | 15.00 ± 2.27 | 7253 | 14.65 ± 2.43 | 0.000 |
| 60 Months | 22,461 | 17.40 ± 2.52 | 20,561 | 17.00 ± 2.72 | 0.000 |
| 72 Months | 3682 | 20.23 ± 4.09 | 3189 | 19.91 ± 4.50 | 0.255 |
| 84 Months | 15,593 | 23.06 ± 4.50 | 14,415 | 22.75 ± 4.66 | 0.000 |
| 96 Months | 2235 | 27.37 ± 7.02 | 2130 | 26.72 ± 7.54 | 0.003 |
| 108 Months | 1338 | 31.12 ± 8.65 | 1275 | 30.53 ± 8.82 | 0.084 |
| 120 Months | 656 | 34.31 ± 9.27 | 624 | 33.67 ± 9.94 | 0.240 |
| BMI | |||||
|---|---|---|---|---|---|
| Age | Boys | Girls | p | ||
| n | Mean ± SD | n | Mean ± SD | ||
| Birth | 441 | 13.04 ± 1.42 | 376 | 12.75 ± 1.39 | 0.003 |
| 3 Months | 1176 | 13.89 ± 1.86 | 1031 | 13.61 ± 1.94 | 0.001 |
| 6 Months | 316 | 16.66 ± 1.72 | 234 | 16.46 ± 1.75 | 0.179 |
| 12 Months | 397 | 17.15 ± 1.81 | 335 | 16.73 ± 2.00 | 0.003 |
| 24 Months | 807 | 16.79 ± 1.56 | 627 | 16.43 ± 1.72 | 0.000 |
| 36 Months | 11,267 | 16.06 ± 1.41 | 9930 | 15.85 ± 1.55 | 0.077 |
| 48 Months | 8148 | 15.96 ± 1.69 | 7253 | 15.81 ± 1.91 | 0.005 |
| 60 Months | 22,461 | 15.96 ± 1.65 | 20,561 | 15.84 ± 1.84 | 0.042 |
| 72 Months | 3682 | 16.24 ± 2.36 | 3189 | 16.13 ± 2.69 | 0.057 |
| 84 Months | 15,593 | 16.49 ± 2.39 | 14,415 | 16.43 ± 2.66 | 0.042 |
| 96 Months | 2235 | 17.52 ± 3.49 | 2130 | 17.31 ± 3.86 | 0.090 |
| 108 Months | 1338 | 18.18 ± 4.04 | 1275 | 18.09 ± 3.71 | 0.560 |
| 120 Months | 656 | 18.21 ± 4.03 | 624 | 18.41 ± 4.51 | 0.089 |
| Age (Months) | Variables | P3 | P10 | P25 | P50 | P75 | P90 | P97 | |||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Boys | Girls | Boys | Girls | Boys | Girls | Boys | Girls | Boys | Girls | Boys | Girls | Boys | Girls | ||
| Birth | Weight | 2.14 | 2.05 | 2.50 | 2.32 | 2.86 | 2.66 | 3.24 | 3.08 | 3.59 | 3.42 | 3.93 | 3.73 | 5.43 | 4.72 |
| Height | 0.44 | 0.44 | 0.46 | 0.45 | 0.48 | 0.47 | 0.50 | 0.49 | 0.51 | 0.51 | 0.52 | 3.73 | 0.57 | 0.59 | |
| 3 | Weight | 2.28 | 2.08 | 2.81 | 2.67 | 3.42 | 3.16 | 4.02 | 3.75 | 4.61 | 4.37 | 5.22 | 4.87 | 5.80 | 5.32 |
| Height | 0.45 | 0.44 | 0.48 | 0.46 | 0.51 | 0.49 | 0.53 | 0.52 | 0.56 | 0.54 | 0.58 | 0.57 | 0.61 | 0.59 | |
| 6 | Weight | 4.67 | 4.53 | 5.43 | 5.07 | 6.09 | 5.73 | 6.71 | 6.33 | 7.49 | 6.89 | 7.91 | 7.46 | 8.39 | 8.17 |
| Height | 0.55 | 0.55 | 0.58 | 0.57 | 0.61 | 0.59 | 0.64 | 0.61 | 0.66 | 0.64 | 0.68 | 0.66 | 0.70 | 0.68 | |
| 12 | Weight | 5.92 | 5.49 | 6.89 | 6.25 | 7.70 | 7.03 | 8.59 | 7.92 | 9.38 | 8.67 | 10.13 | 9.59 | 10.96 | 10.44 |
| Height | 0.63 | 0.61 | 0.65 | 0.63 | 0.68 | 0.65 | 0.70 | 0.69 | 0.73 | 0.71 | 0.75 | 0.73 | 0.77 | 0.76 | |
| 24 | Weight | 8.28 | 7.37 | 9.12 | 8.31 | 9.92 | 9.23 | 10.89 | 10.34 | 11.90 | 11.45 | 12.86 | 12.33 | 13.83 | 13.25 |
| Height | 0.72 | 0.70 | 0.74 | 0.73 | 0.77 | 0.75 | 0.81 | 0.78 | 0.83 | 0.82 | 0.86 | 0.85 | 0.89 | 0.88 | |
| 36 | Weight | 9.92 | 9.41 | 10.86 | 10.39 | 11.90 | 11.33 | 12.95 | 12.42 | 14.00 | 13.53 | 14.94 | 14.61 | 15.86 | 15.61 |
| Height | 0.82 | 0.81 | 0.84 | 0.83 | 0.87 | 0.85 | 0.89 | 0.88 | 0.92 | 0.91 | 0.93 | 0.93 | 0.96 | 0.95 | |
| 48 | Weight | 10.82 | 10.01 | 12.09 | 11.32 | 13.49 | 12.80 | 15.07 | 14.53 | 16.47 | 16.27 | 17.92 | 17.83 | 19.36 | 19.36 |
| Height | 0.88 | 0.87 | 0.91 | 0.89 | 0.93 | 0.92 | 0.97 | 0.96 | 1.00 | 0.99 | 1.02 | 1.02 | 1.05 | 1.04 | |
| 60 | Weight | 12.66 | 11.92 | 14.11 | 13.40 | 15.67 | 15.11 | 17.35 | 16.97 | 19.06 | 18.83 | 20.60 | 20.53 | 22.12 | 22.23 |
| Height | 0.95 | 0.94 | 0.98 | 0.97 | 1.00 | 0.99 | 1.04 | 1.03 | 1.07 | 1.06 | 1.10 | 1.09 | 1.12 | 1.12 | |
| 72 | Weight | 12.41 | 11.44 | 15.05 | 14.24 | 17.30 | 16.88 | 20.10 | 19.89 | 22.95 | 23.08 | 25.43 | 25.90 | 27.73 | 28.43 |
| Height | 1.00 | 0.99 | 1.04 | 1.03 | 1.07 | 1.07 | 1.11 | 1.10 | 1.15 | 1.14 | 1.18 | 1.18 | 1.21 | 1.21 | |
| 84 | Weight | 14.71 | 13.75 | 17.17 | 16.80 | 20.03 | 19.34 | 22.92 | 22.66 | 26.00 | 26.00 | 28.77 | 28.76 | 31.47 | 31.54 |
| Height | 1.08 | 1.07 | 1.11 | 1.10 | 1.14 | 1.13 | 1.18 | 1.17 | 1.21 | 1.20 | 1.25 | 1.24 | 1.28, | 1.28 | |
| 96 | Weight | 13.34 | 12.62 | 17.64 | 16.92 | 22.11 | 21.44 | 27.21 | 26.84 | 32.17 | 32.14 | 36.54 | 36.53 | 40.95 | 40.41 |
| Height | 1.11 | 1.10 | 1.16 | 1.15 | 1.20 | 1.19 | 1.23 | 1.23 | 1.28 | 1.27 | 1.32 | 1.32 | 1.36 | 1.36 | |
| 108 | Weight | 15.60 | 12.92 | 20.60 | 18.44 | 25.16 | 24.70 | 30.71 | 31.03 | 36.83 | 36.62 | 42.66 | 41.60 | 48.15 | 46.35 |
| Height | 1.17 | 1.16 | 1.21 | 1.20 | 1.25 | 1.24 | 1.30 | 1.29 | 1.35 | 1.34 | 1.35 | 1.38 | 1.43 | 1.42 | |
| 120 | Weight | 16.55 | 14.46 | 22.69 | 20.32 | 27.78 | 26.66 | 34.46 | 33.57 | 40.79 | 40.15 | 46.65 | 46.48 | 52.48 | 52.45 |
| Height | 1.19 | 1.19 | 1.23 | 1.23 | 1.29 | 1.27 | 1.34 | 1.33 | 1.39 | 1.39 | 1.39 | 1.44 | 1.48 | 1.50 | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Pardo-Galán, L.; Pastor-Cisneros, R.; Collado-Mateo, D.; Adsuar, J.C.; García-Gordillo, M.Á.; Bautista-Bárcena, L. New Growth Curves for Spanish Children (0–10 Years) in the Region of Extremadura. Int. J. Environ. Res. Public Health 2021, 18, 8953. https://doi.org/10.3390/ijerph18178953
Pardo-Galán L, Pastor-Cisneros R, Collado-Mateo D, Adsuar JC, García-Gordillo MÁ, Bautista-Bárcena L. New Growth Curves for Spanish Children (0–10 Years) in the Region of Extremadura. International Journal of Environmental Research and Public Health. 2021; 18(17):8953. https://doi.org/10.3390/ijerph18178953
Chicago/Turabian StylePardo-Galán, Luis, Raquel Pastor-Cisneros, Daniel Collado-Mateo, José Carmelo Adsuar, Miguel Ángel García-Gordillo, and Lucía Bautista-Bárcena. 2021. "New Growth Curves for Spanish Children (0–10 Years) in the Region of Extremadura" International Journal of Environmental Research and Public Health 18, no. 17: 8953. https://doi.org/10.3390/ijerph18178953
APA StylePardo-Galán, L., Pastor-Cisneros, R., Collado-Mateo, D., Adsuar, J. C., García-Gordillo, M. Á., & Bautista-Bárcena, L. (2021). New Growth Curves for Spanish Children (0–10 Years) in the Region of Extremadura. International Journal of Environmental Research and Public Health, 18(17), 8953. https://doi.org/10.3390/ijerph18178953