
Associations of Sedentary Time with Heart Rate and Heart Rate Variability in Adults: A Systematic Review and Meta-Analysis of Observational Studies

 , ,
, ,  , ,
, ,  ,
,  and
and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Data Sources and Search Strategy
2.2. Study Selection
2.3. Data Extraction and Quality Assessment
2.4. Data Synthesis
2.5. Data Analysis
3. Results
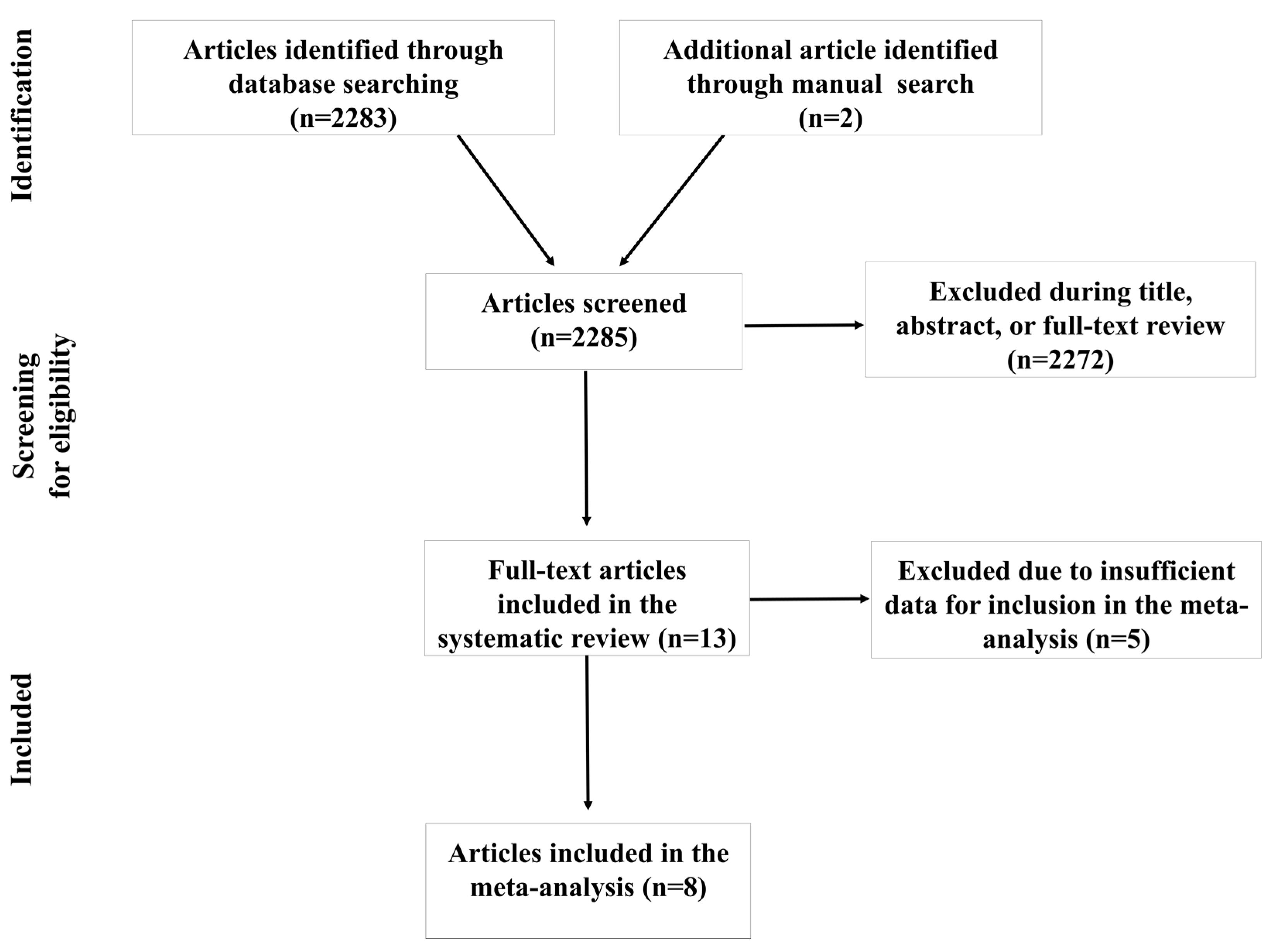
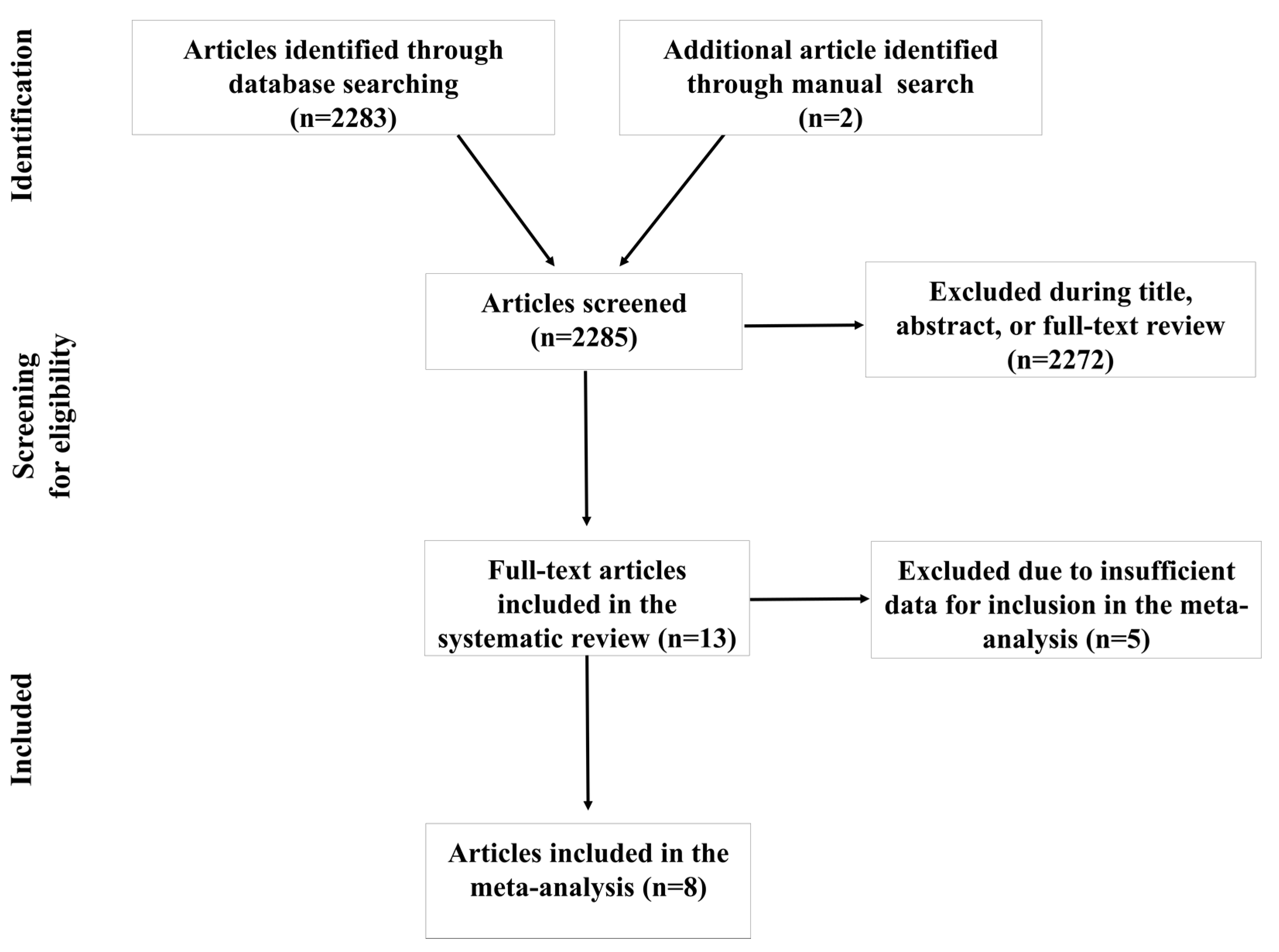
3.1. Literature Search and Trial Selection
3.2. Characteristics of Included Articles and Quality Assessment
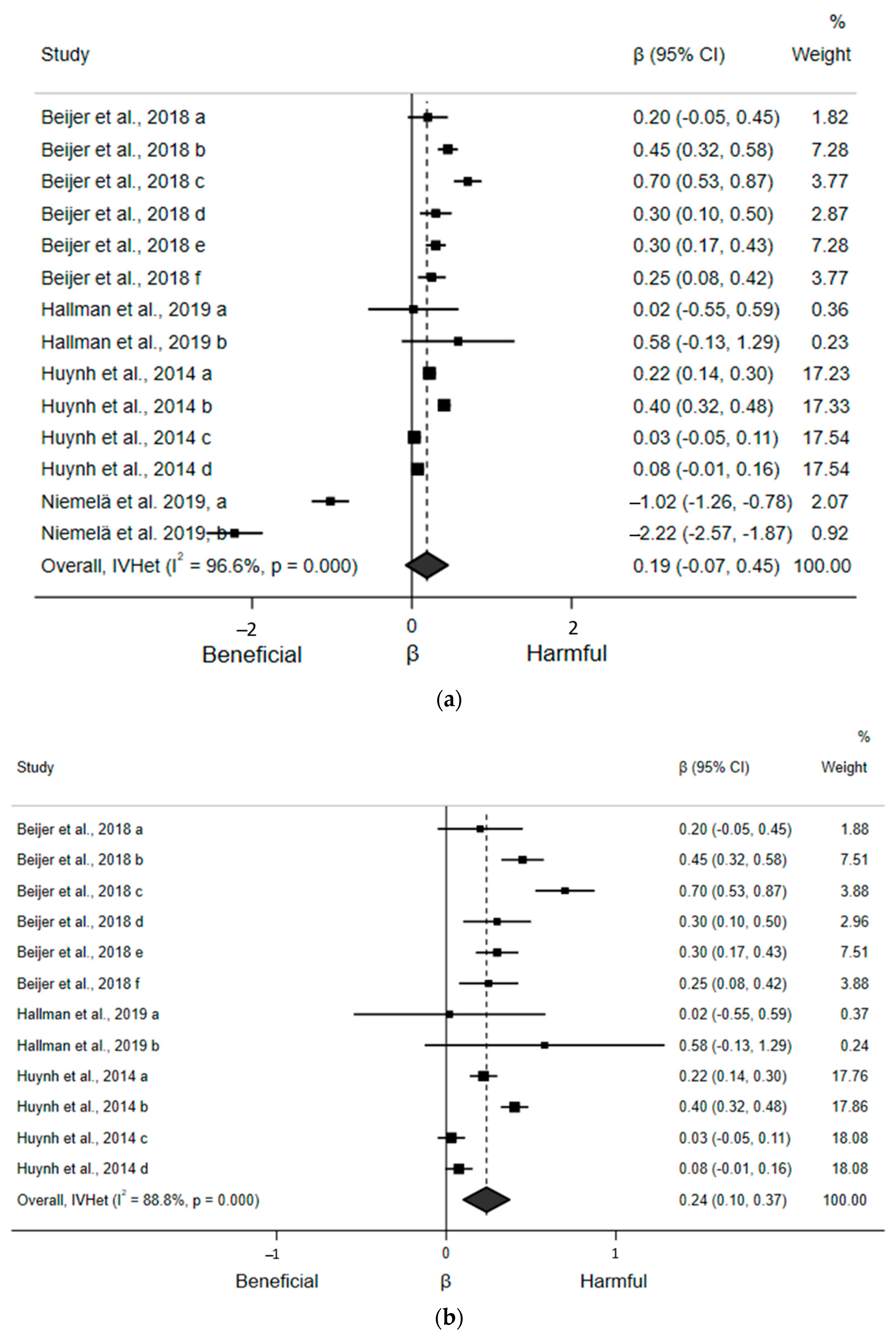
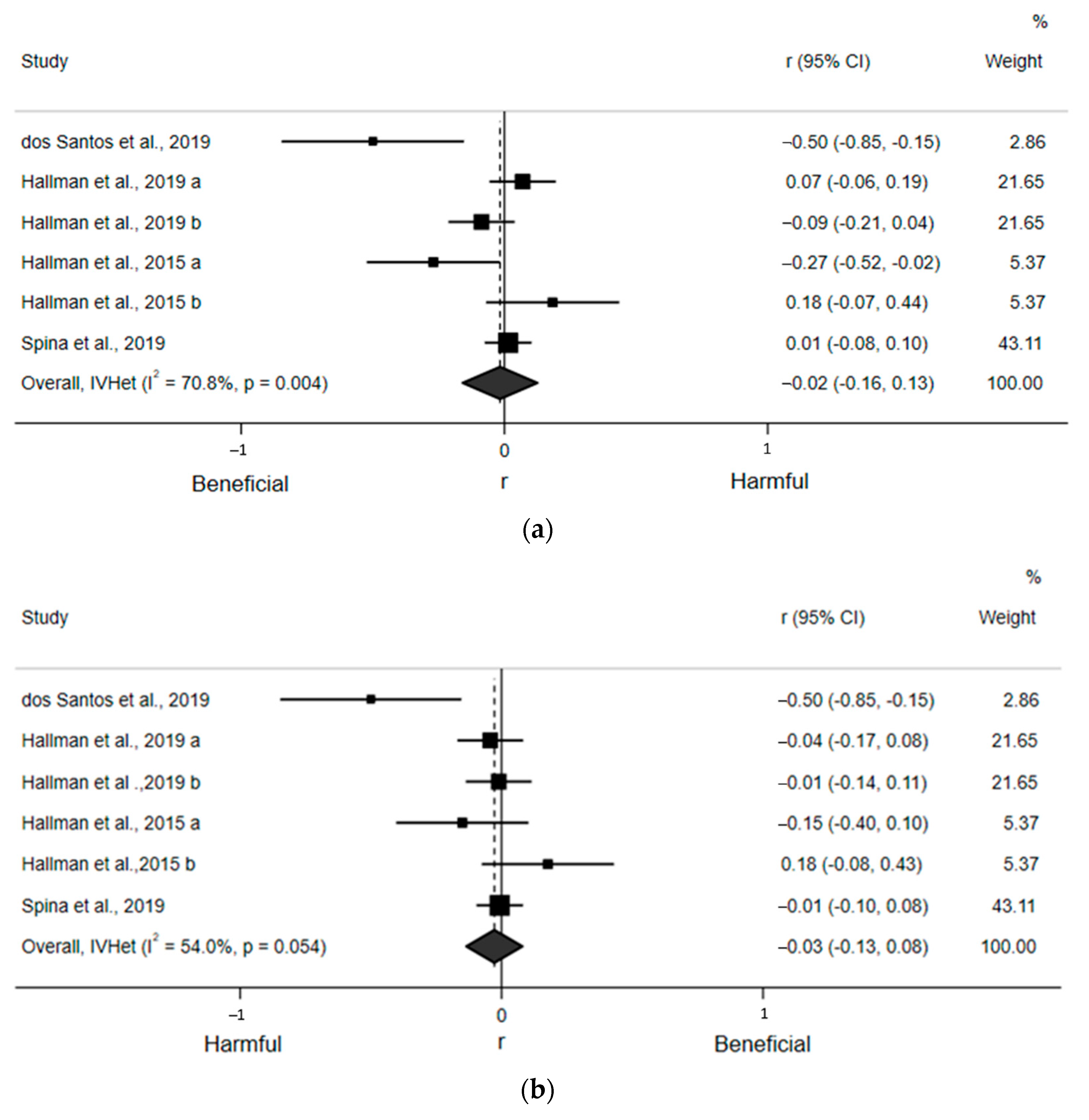
3.3. Association between Sedentary Time and Heart Rate
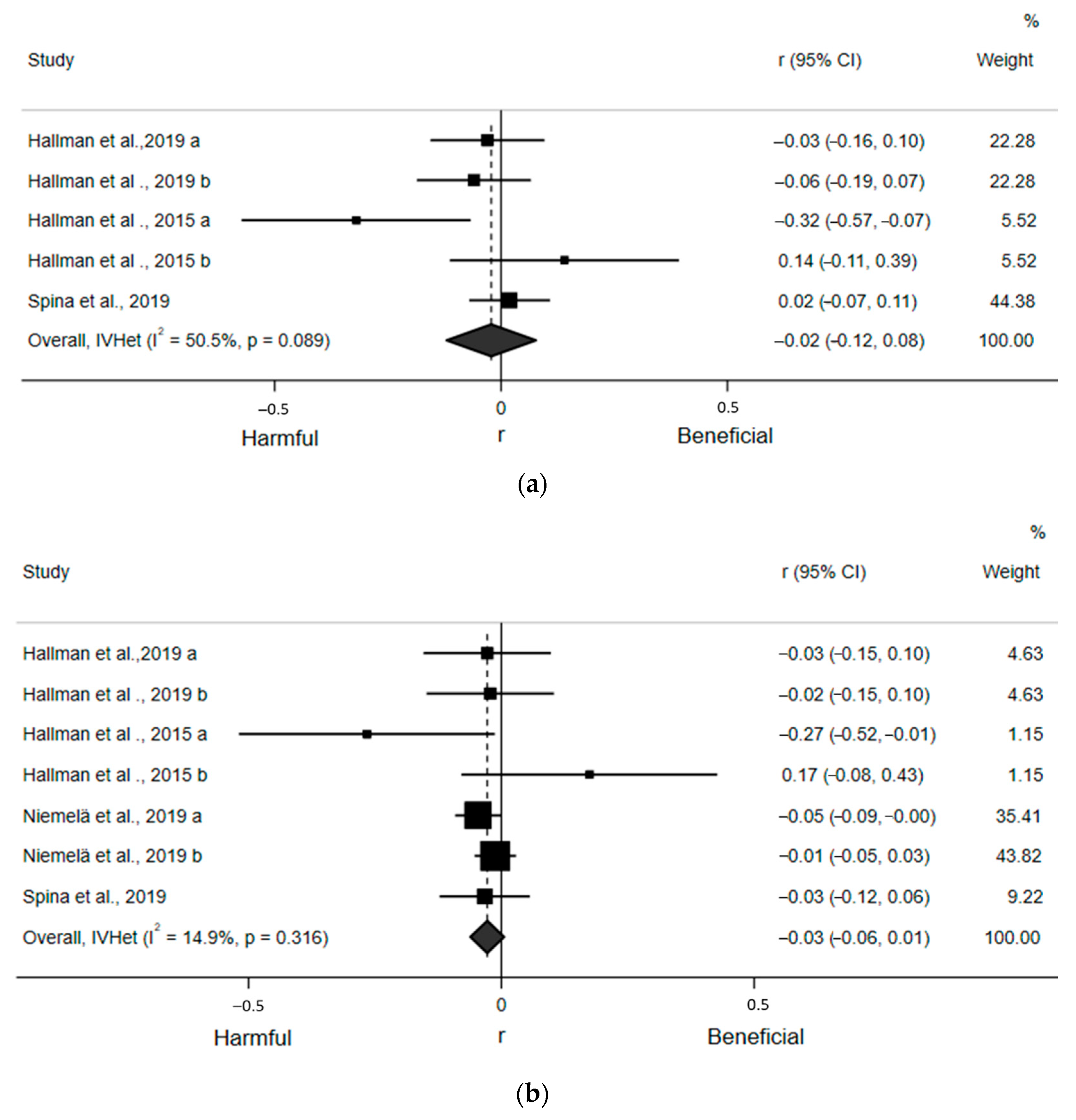
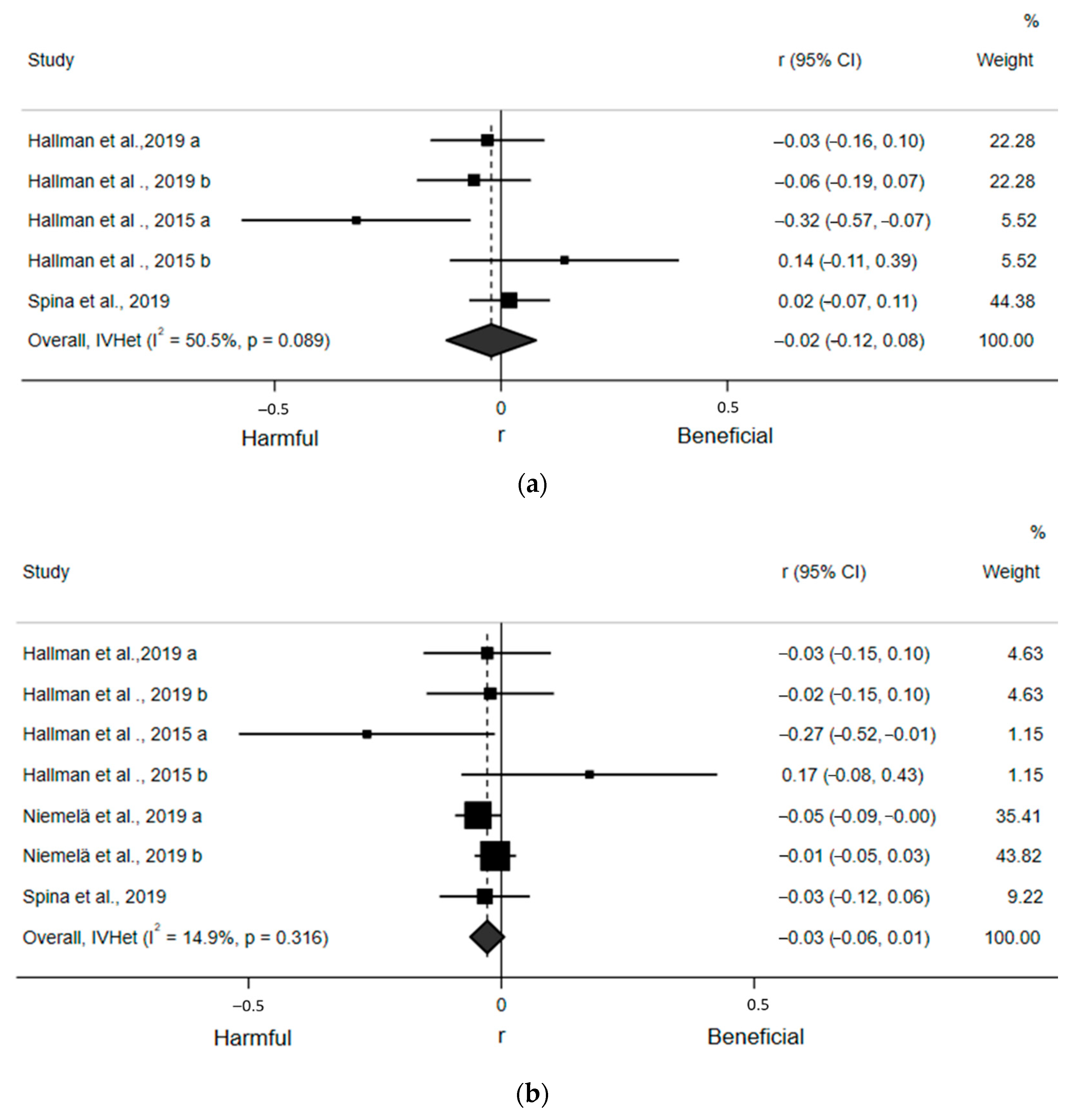
3.4. Association between Sedentary Time and Time Domain Indices of Heart Rate Variability
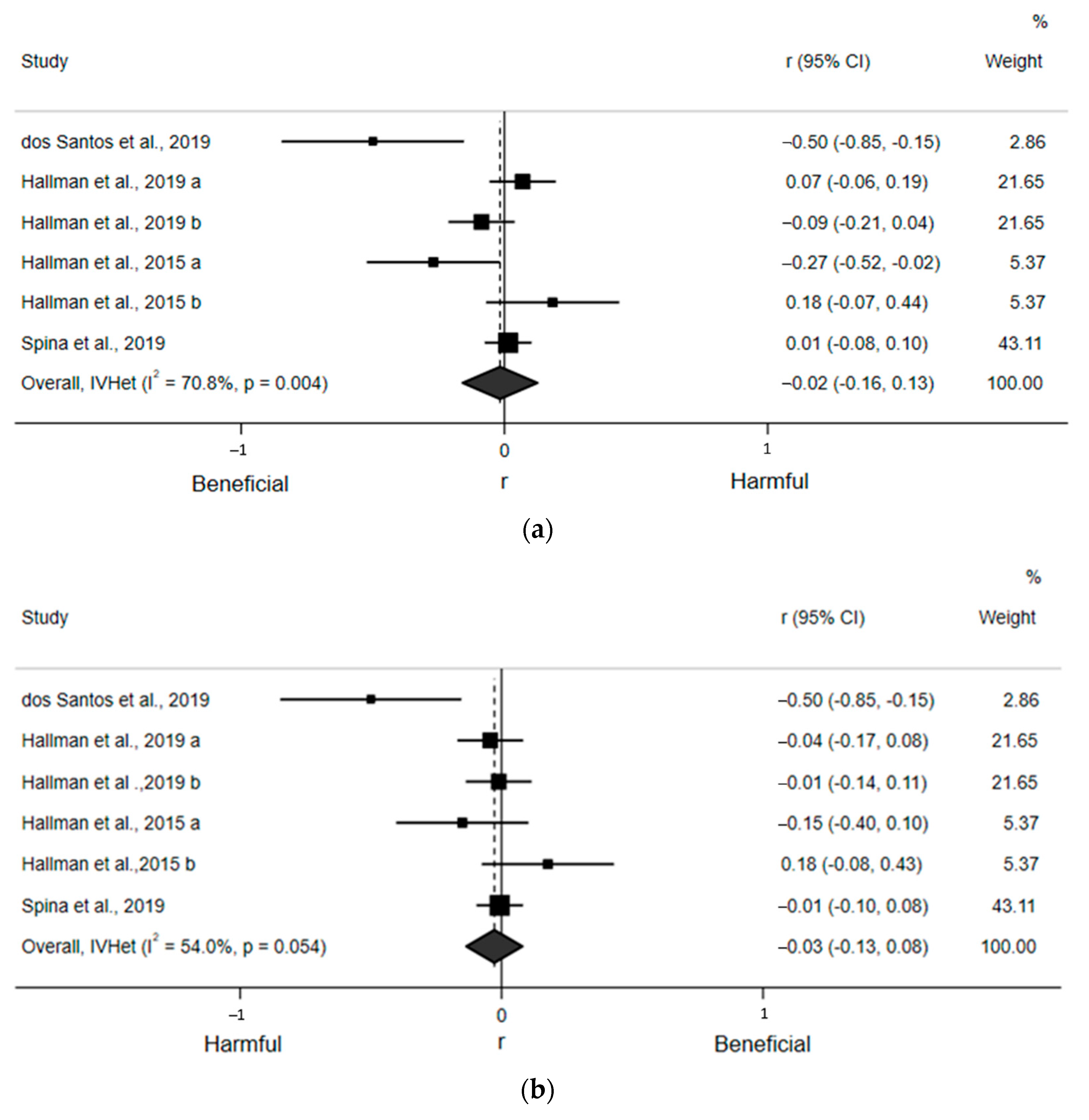
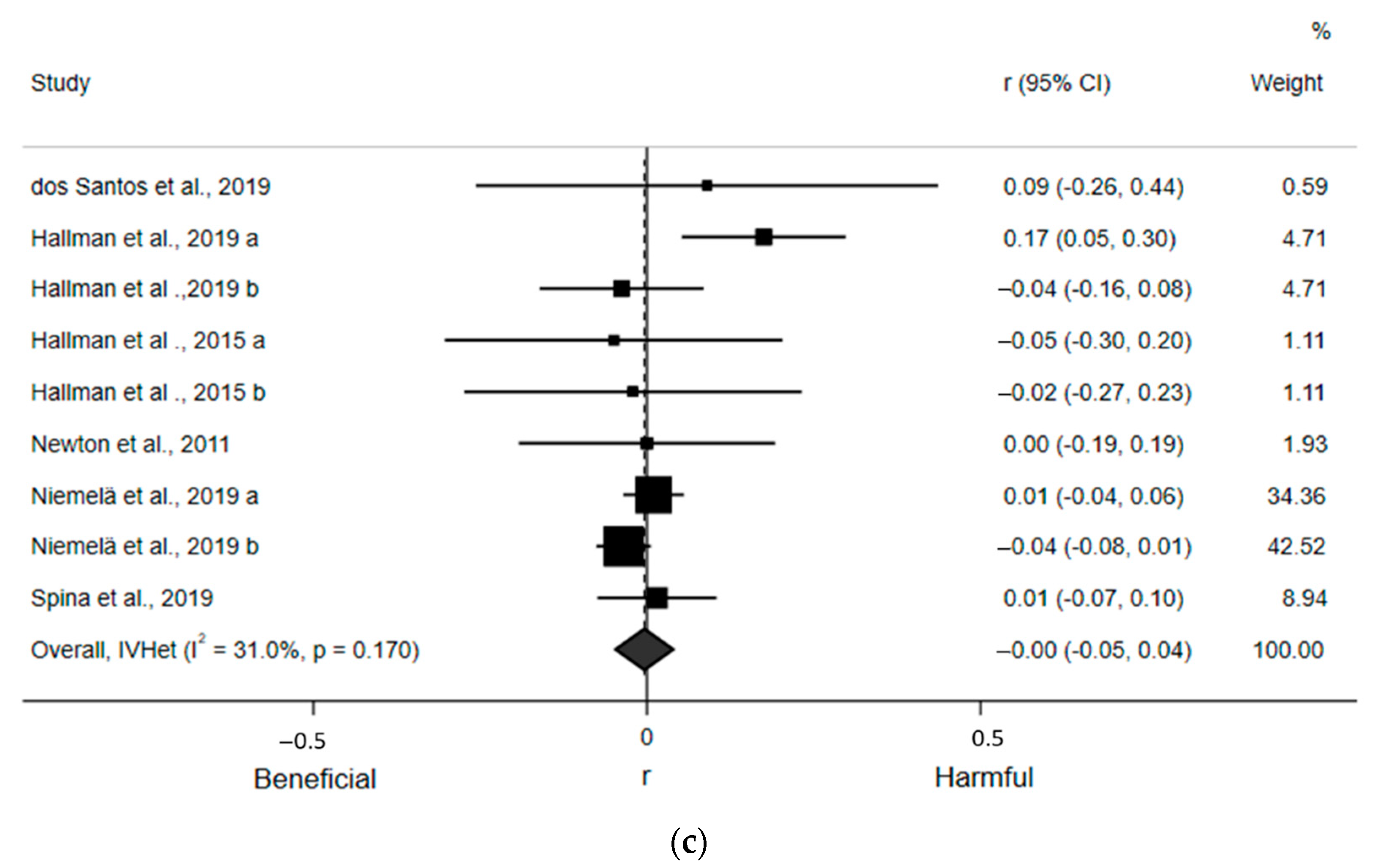
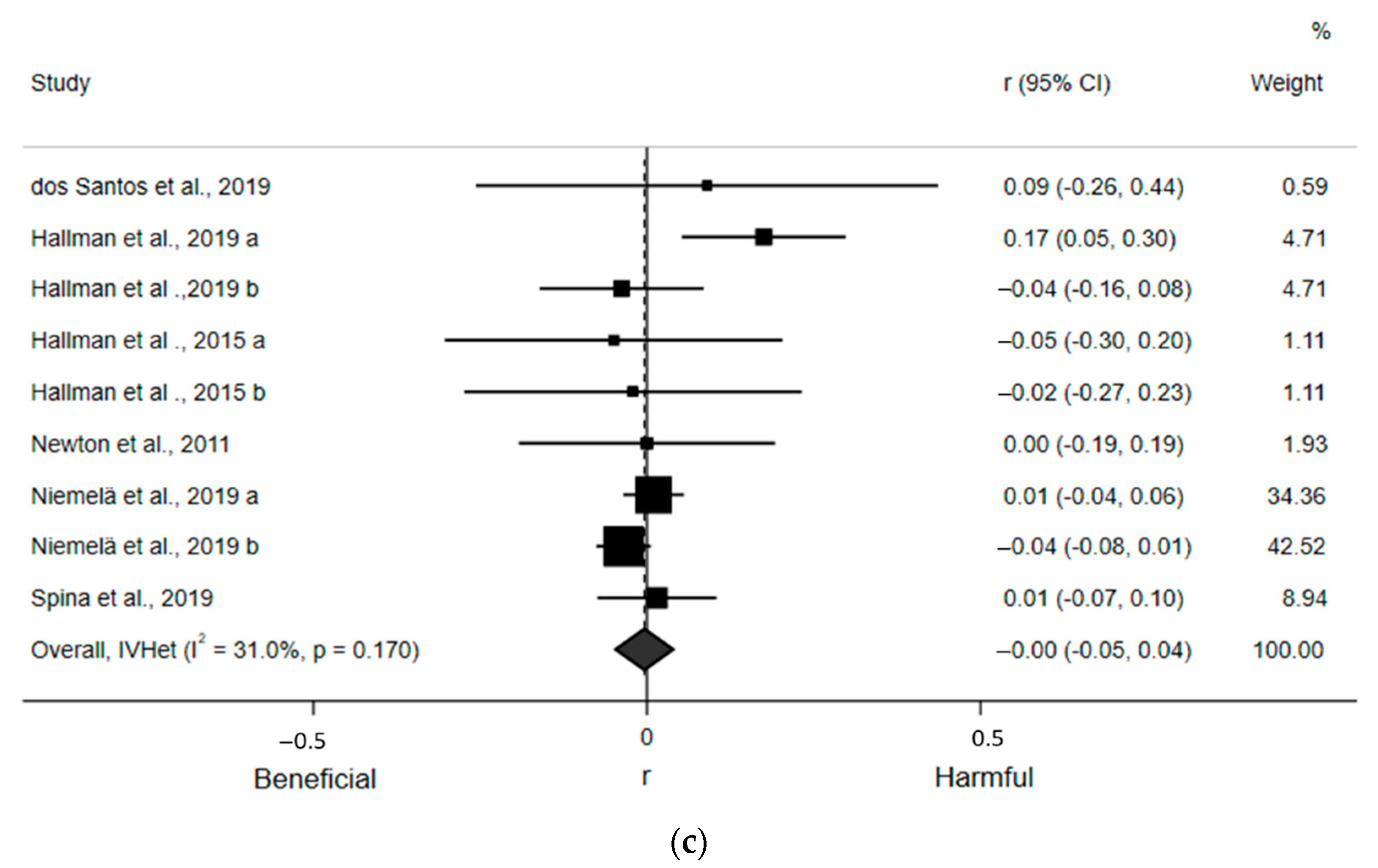
3.5. Association between Sedentary Time and Frequency Domain Indices of Heart Rate Variability
4. Discussion
4.1. Association between Sedentary Time and Heart Rate
4.2. Association between Sedentary Time and Heart Rate Variability
4.3. Hypothesized Physiological Mechanisms
4.4. Limitations
4.5. Implications and Future Directions
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Heidenreich, P.A.; Trogdon, J.G.; Khavjou, O.A.; Butler, J.; Dracup, K.; Ezekowitz, M.D.; Finkelstein, E.A.; Hong, Y.; Johnston, S.C.; Khera, A.; et al. Forecasting the future of cardiovascular disease in the United States: A policy statement from the American Heart Association. Circulation 2011, 123, 933–944. [Google Scholar] [CrossRef] [Green Version]
- Perk, J.; De Backer, G.; Gohlke, H.; Graham, I.; Reiner, Ž.; Verschuren, M.; Albus, C.; Benlian, P.; Boysen, G.; Cifkova, R.; et al. European Guidelines on cardiovascular disease prevention in clinical practice (version 2012) The Fifth Joint Task Force of the European Society of Cardiology and Other Societies on Cardiovascular Disease Prevention in Clinical Practice (constituted by representatives of nine societies and by invited experts) Developed with the special contribution of the European Association for Cardiovascular Prevention & Rehabilitation (EACPR). Eur. Heart J. 2012, 33, 1635–1701. [Google Scholar]
- Tremblay, M.S.; Aubert, S.; Barnes, J.D.; Saunders, T.J.; Carson, V.; Latimer-Cheung, A.E.; Chastin, S.F.; Altenburg, T.M.; Chinapaw, M.J. Sedentary behavior research network (SBRN)–terminology consensus project process and outcome. Int. J. Behav. Nutr. Phys. Act. 2017, 14, 75. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ekelund, U.; Steene-Johannessen, J.; Brown, W.J.; Fagerland, M.W.; Owen, N.; Powell, K.E.; Bauman, A.; Lee, I.-M.; Series, L.P.A.; Lancet Sedentary Behaviour Working Group. Does physical activity attenuate, or even eliminate, the detrimental association of sitting time with mortality? A harmonised meta-analysis of data from more than 1 million men and women. Lancet 2016, 388, 1302–1310. [Google Scholar] [CrossRef] [Green Version]
- Pandey, A.; Salahuddin, U.; Garg, S.; Ayers, C.; Kulinski, J.; Anand, V.; Mayo, H.; Kumbhani, D.J.; de Lemos, J.; Berry, J.D. Continuous dose-response association between sedentary time and risk for cardiovascular disease: A meta-analysis. JAMA Cardiol. 2016, 1, 575–583. [Google Scholar] [CrossRef] [Green Version]
- US Department of Health and Human Services. 2018 Physical Activity Guidelines Advisory Committee Scientific Report; US Department of Health and Human Services: Washington, DC, USA, 2018.
- Katzmarzyk, P.T.; Powell, K.E.; Jakicic, J.M.; Troiano, R.P.; Piercy, K.; Tennant, B.; 2018 Physical Activity Guidelines Committee. Sedentary behavior and health: Update from the 2018 Physical Activity Guidelines Advisory Committee. Med. Sci. Sports Exerc. 2019, 51, 1227–1241. [Google Scholar] [CrossRef]
- Young, H.A.; Benton, D. Heart-rate variability: A biomarker to study the influence of nutrition on physiological and psychological health? Behav. Pharmacol. 2018, 29, 140–151. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jensen, M.T.; Suadicani, P.; Hein, H.O.; Gyntelberg, F. Elevated resting heart rate, physical fitness and all-cause mortality: A 16-year follow-up in the Copenhagen Male Study. Heart 2013, 99, 882–887. [Google Scholar] [CrossRef] [PubMed]
- Palatini, P. Heart rate as an independent risk factor for cardiovascular disease. Drugs 2007, 67, 3–13. [Google Scholar] [CrossRef] [PubMed]
- Kleiger, R.E.; Miller, J.P.; Bigger, J.T., Jr.; Moss, A.J. Decreased heart rate variability and its association with increased mortality after acute myocardial infarction. Am. J. Cardiol. 1987, 59, 256–262. [Google Scholar] [CrossRef]
- Liao, D.; Carnethon, M.; Evans, G.W.; Cascio, W.E.; Heiss, G. Lower heart rate variability is associated with the development of coronary heart disease in individuals with diabetes: The atherosclerosis risk in communities (ARIC) study. Diabetes 2002, 51, 3524–3531. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Task Force of the European Society of Cardiology and the North American Society of Pacing Electrophysiology. Heart rate variability: Standards of measurement, physiological interpretation and clinical use. Circulation 1996, 93, 1043–1065. [Google Scholar] [CrossRef] [Green Version]
- Laborde, S.; Mosley, E.; Thayer, J.F. Heart rate variability and cardiac vagal tone in psychophysiological research–recommendations for experiment planning, data analysis, and data reporting. Front. Psychol. 2017, 8, 213. [Google Scholar] [CrossRef] [Green Version]
- Goldstein, D.S.; Bentho, O.; Park, M.Y.; Sharabi, Y. Low-frequency power of heart rate variability is not a measure of cardiac sympathetic tone but may be a measure of modulation of cardiac autonomic outflows by baroreflexes. Exp. Physiol. 2011, 96, 1255–1261. [Google Scholar] [CrossRef]
- Billman, G.E. The LF/HF ratio does not accurately measure cardiac sympatho-vagal balance. Front. Physiol. 2013, 4, 26. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shaffer, F.; McCraty, R.; Zerr, C.L. A healthy heart is not a metronome: An integrative review of the heart’s anatomy and heart rate variability. Front. Psychol. 2014, 5, 1040. [Google Scholar] [CrossRef] [Green Version]
- Beijer, K.; Lampa, E.; Sundström, J.; Nilsson, P.M.; Elmståhl, S.; Pedersen, N.L.; Lind, L. Physical activity may compensate for prolonged TV time regarding pulse rate—A cross-sectional study. Ups. J. Med Sci. 2018, 123, 247–254. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dempsey, P.C.; Matthews, C.E.; Dashti, S.G.; Doherty, A.R.; Bergouignan, A.; van Roekel, E.H.; Dunstan, D.W.; Wareham, N.J.; Yates, T.E.; Wijndaele, K.; et al. Sedentary behavior and chronic disease: Mechanisms and future directions. J. Phys. Act. Health 2020, 17, 52–61. [Google Scholar] [CrossRef]
- Hallman, D.M.; Sato, T.; Kristiansen, J.; Gupta, N.; Skotte, J.; Holtermann, A. Prolonged sitting is associated with attenuated heart rate variability during sleep in blue-collar workers. Int. J. Environ. Res. Public Health 2015, 12, 14811–14827. [Google Scholar] [CrossRef] [Green Version]
- Huynh, Q.L.; Blizzard, C.L.; Sharman, J.E.; Magnussen, C.G.; Dwyer, T.; Venn, A.J. The cross-sectional association of sitting time with carotid artery stiffness in young adults. BMJ Open 2014, 4, e004384. [Google Scholar] [CrossRef] [Green Version]
- Hallman, D.M.; Krause, N.; Jensen, M.T.; Gupta, N.; Birk Jørgensen, M.; Holtermann, A. Objectively measured sitting and standing in workers: Cross-sectional relationship with autonomic cardiac modulation. Int. J. Environ. Res. Public Health 2019, 16, 650. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Spina, G.; Gonze, B.; Barbosa, A.; Sperandio, E.; Dourado, V. Presence of age-and sex-related differences in heart rate variability despite the maintenance of a suitable level of accelerometer-based physical activity. Braz. J. Med Biol. Res. 2019, 52, e8088. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Newton, J.; Pairman, J.; Hallsworth, K.; Moore, S.; Plötz, T.; Trenell, M. Physical activity intensity but not sedentary activity is reduced in chronic fatigue syndrome and is associated with autonomic regulation. QJM 2011, 104, 681–687. [Google Scholar] [CrossRef] [Green Version]
- Niemelä, M.; Kiviniemi, A.; Kangas, M.; Farrahi, V.; Leinonen, A.M.; Ahola, R.; Tammelin, T.; Puukka, K.; Auvinen, J.; Korpelainen, R.; et al. Prolonged bouts of sedentary time and cardiac autonomic function in midlife. Transl. Sports Med. 2019, 2, 341–350. [Google Scholar] [CrossRef] [Green Version]
- dos Santos, R.R.; Rosa, E.C.; Rosa, T.; Ferreira, E.A.; Gris, E.F.; de Andrade, R.V.; Amato, A.A. Sedentary behavior: A key component in the interaction between an integrated lifestyle approach and cardiac autonomic function in active young men. Int. J. Environ. Res. Public Health 2019, 16, 2156. [Google Scholar] [CrossRef] [Green Version]
- Moher, D.; Shamseer, L.; Clarke, M.; Ghersi, D.; Liberati, A.; Petticrew, M.; Shekelle, P.; Stewart, L.A. Preferred reporting items for systematic review and meta-analysis protocols (PRISMA-P) 2015 statement. Syst. Rev. 2015, 4, 1. [Google Scholar] [CrossRef] [Green Version]
- National Heart, Lung, and Blood Institute. Quality Assessment Tool for Observational Cohort and Cross-Sectional Studies. Available online: https://www.nhlbi.nih.gov/health-topics/study-quality-assessment-tools (accessed on 3 June 2021).
- Brocklebank, L.A.; Falconer, C.L.; Page, A.S.; Perry, R.; Cooper, A.R. Accelerometer-measured sedentary time and cardiometabolic biomarkers: A systematic review. Prev. Med. 2015, 76, 92–102. [Google Scholar] [CrossRef] [Green Version]
- Stoner, L.; Rowlands, D.; Morrison, A.; Credeur, D.; Hamlin, M.; Gaffney, K.; Lambrick, D.; Matheson, A. Efficacy of exercise intervention for weight loss in overweight and obese adolescents: Meta-analysis and implications. Sports Med. 2016, 46, 1737–1751. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Higgins, J.; Thomas, J. Cochrane Handbook for Systematic Reviews of Interventions, Version 6.2. Available online: https://training.cochrane.org/handbook/current (accessed on 3 June 2021).
- Koenig, J.; Kemp, A.H.; Beauchaine, T.P.; Thayer, J.F.; Kaess, M. Depression and resting state heart rate variability in children and adolescents—A systematic review and meta-analysis. Clin. Psychol. Rev. 2016, 46, 136–150. [Google Scholar] [CrossRef]
- Peterson, R.A.; Brown, S.P. On the use of beta coefficients in meta-analysis. J. Appl. Psychol. 2005, 90, 175–181. [Google Scholar] [CrossRef] [Green Version]
- Doi, S.A.; Barendregt, J.J.; Khan, S.; Thalib, L.; Williams, G.M. Advances in the meta-analysis of heterogeneous clinical trials I: The inverse variance heterogeneity model. Contemp. Clin. Trials 2015, 45, 130–138. [Google Scholar] [CrossRef] [Green Version]
- Cohen, J. Statistical Power Analysis for the Behavioral Sciences, 2nd ed.; Lawrence Erlbaum Associates: Hillsdale, NJ, USA, 1988. [Google Scholar]
- Chalmers, J.A.; Quintana, D.S.; Abbott, M.J.; Kemp, A.H. Anxiety disorders are associated with reduced heart rate variability: A meta-analysis. Front. Psychiatry 2014, 5, 80. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sterne, J.A.; Sutton, A.J.; Ioannidis, J.P.; Terrin, N.; Jones, D.R.; Lau, J.; Carpenter, J.; Rücker, G.; Harbord, R.M.; Schmid, C.H.; et al. Recommendations for examining and interpreting funnel plot asymmetry in meta-analyses of randomised controlled trials. BMJ 2011, 343, d4002. [Google Scholar] [CrossRef] [Green Version]
- Egger, M.; Smith, G.D.; Schneider, M.; Minder, C. Bias in meta-analysis detected by a simple, graphical test. BMJ 1997, 315, 629–634. [Google Scholar] [CrossRef] [Green Version]
- Higgins, J.P.; Thompson, S.G.; Deeks, J.J.; Altman, D.G. Measuring inconsistency in meta-analyses. BMJ 2003, 327, 557–560. [Google Scholar] [CrossRef] [Green Version]
- Delfino, L.D.; Tebar, W.R.; Tebar, F.C.S.G.; de Souza, J.M.; Romanzini, M.; Fernandes, R.A.; Christofaro, D.G.D. Association between sedentary behavior, obesity and hypertension in public school teachers. Ind. Health 2020, 58, 345–353. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gerage, A.M.; Benedetti, T.R.; Farah, B.Q.; Santana, F.d.S.; Ohara, D.; Andersen, L.B.; Ritti-Dias, R.M. Sedentary behavior and light physical activity are associated with brachial and central blood pressure in hypertensive patients. PLoS ONE 2015, 10, e0146078. [Google Scholar]
- Oliveira, C.; Silveira, E.A.; Rosa, L.; Santos, A.; Rodrigues, A.P.; Mendonça, C.; Silva, L.; Gentil, P.; Rebelo, A.C. Risk factors associated with cardiac autonomic modulation in obese individuals. J. Obes. 2020, 2020, 7185249. [Google Scholar] [CrossRef]
- McGregor, D.E.; Carson, V.; Palarea-Albaladejo, J.; Dall, P.M.; Tremblay, M.S.; Chastin, S.F. Compositional analysis of the associations between 24-h movement behaviours and health indicators among adults and older adults from the Canadian health measure survey. Int. J. Environ. Res. Public Health 2018, 15, 1779. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Recio-Rodriguez, J.I.; Gomez-Marcos, M.A.; Patino-Alonso, M.C.; Romaguera-Bosch, M.; Grandes, G.; Menendez-Suarez, M.; Lema-Bartolome, J.; Gonzalez-Viejo, N.; Agudo-Conde, C.; Garcia-Ortiz, L.; et al. Association of television viewing time with central hemodynamic parameters and the radial augmentation index in adults. Am. J. Hypertens. 2013, 26, 488–494. [Google Scholar] [CrossRef] [Green Version]
- Zhang, D.; Shen, X.; Qi, X. Resting heart rate and all-cause and cardiovascular mortality in the general population: A meta-analysis. CMAJ 2016, 188, E53–E63. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dempsey, P.C.; Larsen, R.N.; Dunstan, D.W.; Owen, N.; Kingwell, B.A. Sitting less and moving more: Implications for hypertension. Hypertension 2018, 72, 1037–1046. [Google Scholar] [CrossRef] [PubMed]
- Koenig, J.; Thayer, J.F. Sex differences in healthy human heart rate variability: A meta-analysis. Neurosci. Biobehav. Rev. 2016, 64, 288–310. [Google Scholar] [CrossRef] [PubMed]
- Chastin, S.; Dontje, M.; Skelton, D.; Čukić, I.; Shaw, R.; Gill, J.; Greig, C.; Gale, C.; Deary, I.; Der, G.; et al. Systematic comparative validation of self-report measures of sedentary time against an objective measure of postural sitting (activPAL). Int. J. Behav. Nutr. Phys. Act. 2018, 15, 21. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Whitaker, K.M.; Buman, M.P.; Odegaard, A.O.; Carpenter, K.C.; Jacobs, D.R., Jr.; Sidney, S.; Pereira, M.A. Sedentary behaviors and cardiometabolic risk: An isotemporal substitution analysis. Am. J. Epidemiol. 2018, 187, 181–189. [Google Scholar] [CrossRef] [Green Version]
- Hallgren, M.; Dunstan, D.W.; Owen, N. Passive versus mentally active sedentary behaviors and depression. Exerc. Sport Sci. Rev. 2020, 48, 20–27. [Google Scholar] [CrossRef]
- Stanley, J.; Peake, J.M.; Buchheit, M. Cardiac parasympathetic reactivation following exercise: Implications for training prescription. Sports Med. 2013, 43, 1259–1277. [Google Scholar] [CrossRef]
- Gilbert, D.G.; Dibb, W.D.; Plath, L.C.; Hiyane, S.G. Effects of nicotine and caffeine, separately and in combination, on EEG topography, mood, heart rate, cortisol, and vigilance. Psychophysiology 2000, 37, 583–595. [Google Scholar] [CrossRef]
- Berntson, G.G.; Thomas Bigger Jr, J.; Eckberg, D.L.; Grossman, P.; Kaufmann, P.G.; Malik, M.; Nagaraja, H.N.; Porges, S.W.; Saul, J.P.; Stone, P.H. Heart rate variability: Origins, methods, and interpretive caveats. Psychophysiology 1997, 34, 623–648. [Google Scholar] [CrossRef]
- Shvartz, E.; Gaume, J.; White, R.; Reibold, R. Hemodynamic responses during prolonged sitting. J. Appl. Physiol. 1983, 54, 1673–1680. [Google Scholar] [CrossRef]
- Dempsey, P.C.; Sacre, J.W.; Larsen, R.N.; Straznicky, N.E.; Sethi, P.; Cohen, N.D.; Cerin, E.; Lambert, G.W.; Owen, N.; Kingwell, B.A.; et al. Interrupting prolonged sitting with brief bouts of light walking or simple resistance activities reduces resting blood pressure and plasma noradrenaline in type 2 diabetes. J. Hypertens. 2016, 34, 2376–2382. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- McManus, A.M.; Ainslie, P.N.; Green, D.J.; Simair, R.G.; Smith, K.; Lewis, N. Impact of prolonged sitting on vascular function in young girls. Exp. Physiol. 2015, 100, 1379–1387. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Horiuchi, M.; Takiguchi, C.; Kirihara, Y.; Horiuchi, Y. Impact of wearing graduated compression stockings on psychological and physiological responses during prolonged sitting. Int. J. Environ. Res. Public Health 2018, 15, 1710. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Horiuchi, M.; Thijssen, D.H. Ischemic preconditioning prevents impact of prolonged sitting on glucose tolerance and markers of cardiovascular health, but not cerebrovascular responses. Am. J. Physiol. Endocrinol. Metab. 2020, 319, E821–E826. [Google Scholar] [CrossRef]
- Thosar, S.S.; Johnson, B.D.; Johnston, J.D.; Wallace, J.P. Sitting and endothelial dysfunction: The role of shear stress. Med. Sci. Monit. 2012, 18, RA173. [Google Scholar] [CrossRef] [Green Version]
- Herring, N.; Paterson, D.J. Nitric oxide—cGMP pathway facilitates acetylcholine release and bradycardia during vagal nerve stimulation in the guinea—Pig in vitro. J. Physiol. 2001, 535, 507–518. [Google Scholar] [CrossRef]
- Edwardson, C.L.; Rowlands, A.V.; Bunnewell, S.; Sanders, J.P.; Esliger, D.W.; Gorely, T.; O’Connell, S.; Davies, M.J.; Khunti, K.; Yates, T.E. Accuracy of posture allocation algorithms for thigh-and waist-worn accelerometers. Med Sci Sports Exerc. 2016, 48, 1085–1090. [Google Scholar] [CrossRef] [Green Version]
- Suorsa, K.; Pulakka, A.; Leskinen, T.; Pentti, J.; Holtermann, A.; Heinonen, O.J.; Sunikka, J.; Vahtera, J.; Stenholm, S. Comparison of sedentary time between thigh-worn and wrist-worn accelerometers. J. Meas. Phys. Behav. 2020, 3, 234–243. [Google Scholar] [CrossRef]
- Malik, M.; Bigger, J.T.; Camm, A.J.; Kleiger, R.E.; Malliani, A.; Moss, A.J.; Schwartz, P.J. Heart rate variability: Standards of measurement, physiological interpretation, and clinical use. Eur. Heart J. 1996, 17, 354–381. [Google Scholar] [CrossRef] [Green Version]
- Shaffer, F.; Ginsberg, J. An overview of heart rate variability metrics and norms. Front. Public Health 2017, 5, 258. [Google Scholar] [CrossRef] [Green Version]
- Berntson, G.G.; Cacioppo, J.T.; Quigley, K.S. Respiratory sinus arrhythmia: Autonomic origins, physiological mechanisms, and psychophysiological implications. Psychophysiology 1993, 30, 183–196. [Google Scholar] [CrossRef] [PubMed]
- Ewing, D.; Neilson, J.; Shapiro, C.; Stewart, J.; Reid, W. Twenty four hour heart rate variability: Effects of posture, sleep, and time of day in healthy controls and comparison with bedside tests of autonomic function in diabetic patients. Heart 1991, 65, 239–244. [Google Scholar] [CrossRef] [Green Version]
- Kang, D.; Kim, Y.; Kim, J.; Hwang, Y.; Cho, B.; Hong, T.; Sung, B.; Lee, Y. Effects of high occupational physical activity, aging, and exercise on heart rate variability among male workers. Ann. Occup. Environ. Med. 2015, 27, 22. [Google Scholar] [CrossRef] [Green Version]
- Holtermann, A.; Coenen, P.; Krause, N. The paradoxical health effects of occupational versus leisure-time physical activity. In Handbook of Socioeconomic Determinants of Occupational Health: From Macro-Level to Micro-Level Evidence; Theorell, T., Ed.; Springer: Cham, Switzerland, 2020; pp. 241–267. [Google Scholar]
- Prince, S.A.; Rasmussen, C.L.; Biswas, A.; Holtermann, A.; Aulakh, T.; Merucci, K.; Coenen, P. The effect of leisure time physical activity and sedentary behaviour on the health of workers with different occupational physical activity demands: A systematic review. Int. J. Behav. Nutr. Phys. Act. 2021, 18, 100. [Google Scholar] [CrossRef] [PubMed]
- Massin, M.M.; Maeyns, K.; Withofs, N.; Ravet, F.; Gérard, P. Circadian rhythm of heart rate and heart rate variability. Arch. Dis. Child. 2000, 83, 179–182. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Barone Gibbs, B.; Kline, C.E.; Huber, K.A.; Paley, J.L.; Perera, S. COVID-19 shelter-at-home and work, lifestyle and well-being in desk workers. Occup. Med. 2021, 71, 86–94. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Reference | Country | Sample N (% Male); Mean Age | ST Measurement | Description of Estimates | Quality |
|---|---|---|---|---|---|
| Included in meta-analysis and systematic review | |||||
| Beijer et al., 2018 [18] | Sweden | 46,832 (41%); 47 yr | self-reported TV watching | age x sex subgroup estimates a (M; 26 y) b (M; 47 y) c (M; 68 y) d (F; 26 y) e (F; 47 y) f (F; 68 y) | 7 |
| dos Santos et al., 2019 [26] | Brazil | 35 (100%); NR | self-reported sitting time | single estimate | 6 |
| Hallman et al., 2019 [22] | Denmark | 490 (56%); 45 yr | thigh + trunk-mounted accelerometer | domain-specific estimates a (occupational sitting time) b (leisure sitting time) | 8 |
| Hallman et al., 2015 [20] | Denmark | 126 (55%); 46 yr | thigh + trunk-mounted accelerometer | domain-specific estimates a (occupational sitting time) b (leisure sitting time) | 9 |
| Huynh et al., 2014 [21] | Australia | 2328 (49%); 31 yr | self-reported sitting time | type of day × sex estimates a (M; weekday sitting time) b (M; weekend sitting time) c (F; weekday sitting time) d (F; weekend sitting time) | 6 |
| Newton et al., 2011 [24] | United Kingdom | 107 (NR); NR | multi-sensor armband | single estimate | 5 |
| Niemelä et al., 2019 [25] | Finland | 4150 (45%); 47 yr | wrist-worn accelerometer | sex subgroup estimates a (M) b (F) | 7 |
| Spina et al., 2019 [23] | Brazil | 485 (37%); 48 yr | waist-worn accelerometer | single estimate | 4 |
| Included in systematic review only | |||||
| Delfino et al., 2020 [40] | Brazil | 245 (24%); 45 yr | self-reported sitting time | 7 | |
| Gerage et al., 2015 [41] | Brazil | 87 (21%); 58 yr | hip-worn accelerometer | 5 | |
| McGregor et al., 2018 [43] | Canada | 7776 (50%); 47 yr | hip-worn accelerometer | 7 | |
| Oliveira et al., 2020 [42] | Brazil | 64 (14%); 39 yr | wrist-worn accelerometer | 5 | |
| Recio-Rodriguez et al., 2013 [44] | Spain | 732 (41%); 57 yr | self-reported TV watching | 6 | |
| Reference | Outcome(s) | HR or HRV Measurement Device | HR or HRV Measurement Duration, Posture, and Type |
|---|---|---|---|
| Included in meta-analysis and systematic review | |||
| Beijer et al., 2018 [18] | HR | oscillometer | N/A; seated; resting daytime |
| dos Santos et al., 2019 [26] | HRV (HF, LF, LF/HF) | HR monitor | 5 min; supine; afternoon |
| Hallman et al., 2019 [22] | HR; HRV (SDNN, RMSSD, HF, LF, LF/HF) | ECG | 3 × 5-min; supine; nocturnal |
| Hallman et al., 2015 [20] | HRV (SDNN, RMSSD, HF, LF, LF/HF) | ECG | 3 × 5-min; supine; nocturnal |
| Huynh et al., 2014 [21] | HR | NR | NR; seated; resting daytime |
| Newton et al., 2011 [24] | HRV (LF/HF) | ECG | 10 min; NR; daytime |
| Niemelä et al., 2019 [25] | HR; HRV (RMSSD, LF/HF) | HR monitor | 5 min; seated and standing; daytime |
| Spina et al., 2019 [23] | HRV (SDNN, RMSSD, HF, LF, LF/HF) | HR monitor | 5 min; supine; resting daytime |
| Included in systematic review only | |||
| Delfino et al., 2020 [40] | HR | oscillometer | N/A; seated; resting daytime |
| Gerage et al., 2015 [41] | HRV (HF, LF) | HR monitor | 5 min; supine; resting daytime |
| McGregor et al., 2018 [43] | HR | oscillometer | N/A; seated; resting daytime |
| Oliveira et al., 2020 [42] | HRV (LF, HF, LF/HF) | HR monitor | 10 min; supine; resting daytime |
| Recio-Rodriguez et al., 2013 [44] | HR | NR | NR; NR; daytime |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Alansare, A.B.; Bates, L.C.; Stoner, L.; Kline, C.E.; Nagle, E.; Jennings, J.R.; Hanson, E.D.; Faghy, M.A.; Gibbs, B.B. Associations of Sedentary Time with Heart Rate and Heart Rate Variability in Adults: A Systematic Review and Meta-Analysis of Observational Studies. Int. J. Environ. Res. Public Health 2021, 18, 8508. https://doi.org/10.3390/ijerph18168508
Alansare AB, Bates LC, Stoner L, Kline CE, Nagle E, Jennings JR, Hanson ED, Faghy MA, Gibbs BB. Associations of Sedentary Time with Heart Rate and Heart Rate Variability in Adults: A Systematic Review and Meta-Analysis of Observational Studies. International Journal of Environmental Research and Public Health. 2021; 18(16):8508. https://doi.org/10.3390/ijerph18168508
Chicago/Turabian StyleAlansare, Abdullah Bandar, Lauren C. Bates, Lee Stoner, Christopher E. Kline, Elizabeth Nagle, J. Richard Jennings, Erik D. Hanson, Mark A. Faghy, and Bethany Barone Gibbs. 2021. "Associations of Sedentary Time with Heart Rate and Heart Rate Variability in Adults: A Systematic Review and Meta-Analysis of Observational Studies" International Journal of Environmental Research and Public Health 18, no. 16: 8508. https://doi.org/10.3390/ijerph18168508
APA StyleAlansare, A. B., Bates, L. C., Stoner, L., Kline, C. E., Nagle, E., Jennings, J. R., Hanson, E. D., Faghy, M. A., & Gibbs, B. B. (2021). Associations of Sedentary Time with Heart Rate and Heart Rate Variability in Adults: A Systematic Review and Meta-Analysis of Observational Studies. International Journal of Environmental Research and Public Health, 18(16), 8508. https://doi.org/10.3390/ijerph18168508