
Traumatic Distress of COVID-19 and Depression in the General Population: Exploring the Role of Resilience, Anxiety, and Hope



Abstract
1. Introduction
1.1. The Mediating Role of Resilience and Hope
1.2. The Present Study
2. Methods
2.1. Participants
2.2. Measures
2.2.1. Depression
2.2.2. Anxiety
2.2.3. Resilience
2.2.4. Hope
2.2.5. Traumatic Distress Related to COVID-19
2.3. Procedure
2.4. Data Analysis Overview
3. Results
3.1. Descriptive Statistics and Intercorrelations
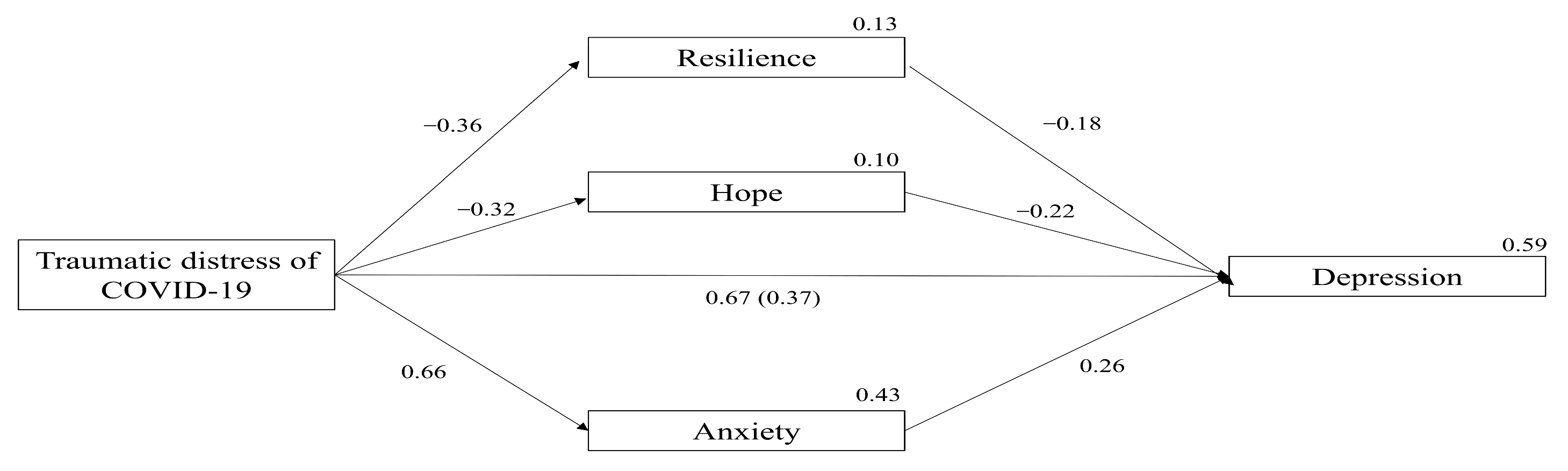
3.2. The Mediating Role of Anxiety, Hope and Resilience
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- WHO Listings of WHO’s Response to. Available online: https://www.who.int/news/item/29-06-2020-covidtimeline (accessed on 29 April 2021).
- Nicola, M.; Alsafi, Z.; Sohrabi, C.; Kerwan, A.; Al-Jabir, A.; Iosifidis, C.; Agha, M.; Agha, R. The Socio-Economic Implications of the Coronavirus Pandemic (COVID-19): A Review. Int. J. Surg. 2020, 78, 185–193. [Google Scholar] [CrossRef]
- Boserup, B.; McKenney, M.; Elkbuli, A. The Financial Strain Placed on America’s Hospitals in the Wake of the COVID-19 Pandemic. Am. J. Emerg. Med. 2020, 45, 530–531. [Google Scholar] [CrossRef] [PubMed]
- Davies, N.; Sweeney, S.; Torres-Rueda, S.; Bozzani, F.; Kitson, N.; Barasa, E.; Procter, S.R.; Quaife, M.; Eggo, R.M.; Vassall, A.; et al. The Impact of Coronavirus Disease 2019 (COVID-19) on Health Systems and Household Resources in Africa and South Asia. medRxiv 2020. [Google Scholar] [CrossRef]
- Serafini, G.; Parmigiani, B.; Amerio, A.; Aguglia, A.; Sher, L.; Amore, M. The Psychological Impact of COVID-19 on the Mental Health in the General Population. QJM 2020, 113, 229–235. [Google Scholar] [CrossRef] [PubMed]
- Krishnamoorthy, Y.; Nagarajan, R.; Saya, G.K.; Menon, V. Prevalence of Psychological Morbidities among General Population, Healthcare Workers and COVID-19 Patients amidst the COVID-19 Pandemic: A Systematic Review and Meta-Analysis. Psychiatry Res. 2020, 293, 113382. [Google Scholar] [CrossRef]
- Salari, N.; Hosseinian-Far, A.; Jalali, R.; Vaisi-Raygani, A.; Rasoulpoor, S.; Mohammadi, M.; Rasoulpoor, S.; Khaledi-Paveh, B. Prevalence of Stress, Anxiety, Depression among the General Population during the COVID-19 Pandemic: A Systematic Review and Meta-Analysis. Glob. Health 2020, 16, 1–11. [Google Scholar] [CrossRef] [PubMed]
- Xiong, J.; Lipsitz, O.; Nasri, F.; Lui, L.M.W.; Gill, H.; Phan, L.; Chen-Li, D.; Iacobucci, M.; Ho, R.; Majeed, A.; et al. Impact of COVID-19 Pandemic on Mental Health in the General Population: A Systematic Review. J. Affect. Disord. 2020, 277, 55–64. [Google Scholar] [CrossRef]
- Pfefferbaum, B.; North, C.S. Mental Health and the COVID-19 Pandemic. N. Engl. J. Med. 2020, 6, 510–512. [Google Scholar] [CrossRef] [PubMed]
- Pappa, S.; Ntella, V.; Giannakas, T.; Giannakoulis, V.G.; Papoutsi, E.; Katsaounou, P. Prevalence of Depression, Anxiety, and Insomnia among Healthcare Workers during the COVID-19 Pandemic: A Systematic Review and Meta-Analysis. Brain Behav. Immun. 2020, 88, 901–907. [Google Scholar] [CrossRef]
- Muller, A.E.; Hafstad, E.V.; Himmels, J.P.W.; Smedslund, G.; Flottorp, S.; Stensland, S.Ø.; Stroobants, S.; Van de Velde, S.; Vist, G.E. The Mental Health Impact of the COVID-19 Pandemic on Healthcare Workers, and Interventions to Help Them: A Rapid Systematic Review. Psychiatry Res. 2020, 293, 113441. [Google Scholar] [CrossRef]
- Vizheh, M.; Qorbani, M.; Arzaghi, S.M.; Muhidin, S.; Javanmard, Z.; Esmaeili, M. The Mental Health of Healthcare Workers in the COVID-19 Pandemic: A Systematic Review. J. Diabetes Metab. Disord. 2020, 19, 1967–1978. [Google Scholar] [CrossRef] [PubMed]
- Romito, F.; Dellino, M.; Loseto, G.; Opinto, G.; Silvestris, E.; Cormio, C.; Guarini, A.; Minoia, C. Psychological Distress in Outpatients with Lymphoma During the COVID-19 Pandemic. Front. Oncol. 2020, 10, 1270. [Google Scholar] [CrossRef] [PubMed]
- Ng, K.Y.Y.; Zhou, S.; Tan, S.H.; Ishak, N.D.B.; Goh, Z.Z.S.; Chua, Z.Y.; Chia, J.M.X.; Chew, E.L.; Shwe, T.; Mok, J.K.Y.; et al. Understanding the Psychological Impact of COVID-19 Pandemic on Patients with Cancer, Their Caregivers, and Health Care Workers in Singapore. JCO Glob. Oncol. 2020, 6, 1494–1509. [Google Scholar] [CrossRef] [PubMed]
- Koppert, T.Y.; Jacobs, J.W.G.; Geenen, R. The Psychological Impact of the COVID-19 Pandemic on Dutch People with and without an Inflammatory Rheumatic Disease. Rheumatology 2020, 60, 3709–3715. [Google Scholar] [CrossRef] [PubMed]
- Addis, S.G.; Nega, A.D.; Miretu, D.G. Psychological Impact of COVID-19 Pandemic on Chronic Disease Patients in Dessie Town Government and Private Hospitals, Northeast Ethiopia. Diabetes Metab. Syndr. Clin. Res. Rev. 2021, 15, 129–135. [Google Scholar] [CrossRef]
- Amorim, R.; Catarino, S.; Miragaia, P.; Ferreras, C.; Viana, V.; Guardiano, M. The Impact of COVID-19 on Children with Autism Spectrum Disorder. Rev. Neurol. 2020, 71, 285–291. [Google Scholar] [CrossRef] [PubMed]
- Linehan, C.; Araten-Bergam, T.; Baumbusch, J.; Beadle-Brown, J.; Bigby, C.; Birkbeck, G.; Bradley, V.; Brown, M.; Bredewold, F.; Chirwa, M.; et al. COVID-19 IDD: A Global Survey Exploring Family Members’ and Paid Staff’s Perceptions of the Impact of COVID-19 on Individuals with Intellectual and Developmental Disabilities and Their Caregivers. HRB Open Res. 2020, 3, 39. [Google Scholar] [CrossRef]
- Solomou, I.; Constantinidou, F. Prevalence and Predictors of Anxiety and Depression Symptoms during the COVID-19 Pandemic and Compliance with Precautionary Measures: Age and Sex Matter. Int. J. Environ. Res. Public Health 2020, 17, 4924. [Google Scholar] [CrossRef]
- Pieh, C.; Budimir, S.; Probst, T. The Effect of Age, Gender, Income, Work, and Physical Activity on Mental Health during Coronavirus Disease (COVID-19) Lockdown in Austria. J. Psychosom. Res. 2020, 136, 110186. [Google Scholar] [CrossRef]
- Qiu, D.; Li, Y.; Li, L.; He, J.; Ouyang, F.; Xiao, S. Prevalence of Post-Traumatic Stress Symptoms among People Influenced by Coronavirus Disease 2019 Outbreak: A Meta-Analysis. Eur. Psychiatry 2021, 64, 1–42. [Google Scholar] [CrossRef]
- Özdin, S.; Bayrak Özdin, Ş. Levels and Predictors of Anxiety, Depression and Health Anxiety during COVID-19 Pandemic in Turkish Society: The Importance of Gender. Int. J. Soc. Psychiatry 2020, 66, 504–511. [Google Scholar] [CrossRef]
- Rogers, J.P.; Chesney, E.; Oliver, D.; Pollak, T.A.; McGuire, P.; Fusar-Poli, P.; Zandi, M.S.; Lewis, G.; David, A.S. Psychiatric and Neuropsychiatric Presentations Associated with Severe Coronavirus Infections: A Systematic Review and Meta-Analysis with Comparison to the COVID-19 Pandemic. Lancet Psychiatry 2020, 7, 611–627. [Google Scholar] [CrossRef]
- Nearchou, F. Resilience Following Emotional Abuse by Teachers: Insights from a Cross-Sectional Study with Greek Students. Child Abus. Negl. 2018, 78, 96–106. [Google Scholar] [CrossRef]
- Ungar, M. Resilience across Cultures. Br. J. Soc. Work 2008, 38, 218–235. [Google Scholar] [CrossRef]
- Ungar, M. Systemic Resilience: Principles and Processes for a Science of Change in Contexts of Adversity. Ecol. Soc. 2018, 23. [Google Scholar] [CrossRef]
- Kukihara, H.; Yamawaki, N.; Uchiyama, K.; Arai, S.; Horikawa, E. Trauma, Depression, and Resilience of Earthquake/Tsunami/Nuclear Disaster Survivors of Hirono, Fukushima, Japan. Psychiatry Clin. Neurosci. 2014, 68, 524–533. [Google Scholar] [CrossRef] [PubMed]
- Lee, J.; Blackmon, B.J.; Cochran, D.M.; Kar, B.; Rehner, T.A.; Gunnell, M.S. Community Resilience, Psychological Resilience, and Depressive Symptoms: An Examination of the Mississippi Gulf Coast 10 Years after Hurricane Katrina and 5 Years after the Deepwater Horizon Oil Spill. Disaster Med. Public Health Prep. 2018, 12, 241–248. [Google Scholar] [CrossRef] [PubMed]
- Blackmon, B.J.; Lee, J.; Cochran, D.M.; Kar, B.; Rehner, T.A.; Baker, A.M. Adapting to Life after Hurricane Katrina and the Deepwater Horizon Oil Spill: An Examination of Psychological Resilience and Depression on the Mississippi Gulf Coast. Soc. Work Public Health 2017, 32, 65–76. [Google Scholar] [CrossRef] [PubMed]
- Song, S.; Yang, X.; Yang, H.; Zhou, P.; Ma, H.; Teng, C.; Chen, H.; Ou, H.; Li, J.; Mathews, C.A.; et al. Psychological Resilience as a Protective Factor for Depression and Anxiety among the Public during the Outbreak of COVID-19. Front. Psychol. 2021, 11, 618509. [Google Scholar] [CrossRef]
- Kimhi, S.; Eshel, Y.; Marciano, H.; Adini, B. Distress and Resilience in the Days of COVID-19: Comparing Two Ethnicities. Int. J. Environ. Res. Public Health 2020, 17, 3956. [Google Scholar] [CrossRef]
- Kimhi, S.; Marciano, H.; Eshel, Y.; Adini, B. Resilience and Demographic Characteristics Predicting Distress during the COVID-19 Crisis. Soc. Sci. Med. 2020, 265, 113389. [Google Scholar] [CrossRef]
- Ran, L.; Wang, W.; Ai, M.; Kong, Y.; Chen, J.; Kuang, L. Psychological Resilience, Depression, Anxiety, and Somatization Symptoms in Response to COVID-19: A Study of the General Population in China at the Peak of Its Epidemic. Soc. Sci. Med. 2020, 262, 113261. [Google Scholar] [CrossRef] [PubMed]
- Karaar, B.; Canli, D. Psychological Resilience and Depression during the COVID-19 Pandemic in Turkey. Psychiatr. Danub. 2020, 32, 273–279. [Google Scholar] [CrossRef]
- Chi, X.; Becker, B.; Yu, Q.; Willeit, P.; Jiao, C.; Huang, L.; Hossain, M.M.; Grabovac, I.; Yeung, A.; Lin, J.; et al. Prevalence and Psychosocial Correlates of Mental Health Outcomes Among Chinese College Students During the Coronavirus Disease (COVID-19) Pandemic. Front. Psychiatry 2020, 11, 803. [Google Scholar] [CrossRef] [PubMed]
- Barzilay, R.; Moore, T.M.; Greenberg, D.M.; DiDomenico, G.E.; Brown, L.A.; White, L.K.; Gur, R.C.; Gur, R.E. Resilience, COVID-19-Related Stress, Anxiety and Depression during the Pandemic in a Large Population Enriched for Healthcare Providers. Transl. Psychiatry 2020, 10, 1–8. [Google Scholar] [CrossRef] [PubMed]
- Snyder, C.R. Hope Theory: Rainbows in the Mind. Psychol. Inq. 2002, 13, 249–275. [Google Scholar] [CrossRef]
- Grewal, P.K.; Porter, J.E. Hope Theory: A Framework for Understanding Suicidal Action. Death Stud. 2007, 31, 131–154. [Google Scholar] [CrossRef] [PubMed]
- Suen, K.S.; Lai, Y.; Ho, S.M.Y.; Cheung, L.K.; Choi, W.S. A Longitudinal Evaluation of Psychosocial Changes throughout Orthognathic Surgery. PLoS ONE 2018, 13, e0203883. [Google Scholar] [CrossRef]
- Weinberg, M.; Besser, A.; Zeigler-Hill, V.; Neria, Y. Bidirectional Associations between Hope, Optimism and Social Support, and Trauma-Related Symptoms among Survivors of Terrorism and Their Spouses. J. Res. Personal. 2016, 62, 29–38. [Google Scholar] [CrossRef]
- Griggs, S. Hope and Mental Health in Young Adult College Students: An Integrative Review. J. Psychosoc. Nurs. Ment. Health Serv. 2017, 55, 28–35. [Google Scholar] [CrossRef] [PubMed]
- Riaz, H.; Riaz, M.N.; Batool, N. Positive Psychological Capital as Predictor of Internalizing Psychological Problems among Flood Victims. J. Indian Acad. Appl. Psychol. 2014, 40, 102. [Google Scholar]
- Brown, C.; Rempfer, M.; Hamera, E. Correlates of Insider and Outsider Conceptualizations of Recovery. Psychiatr. Rehabil. J. 2008, 32, 23–31. [Google Scholar] [CrossRef]
- Gilman, R.; Schumm, J.A.; Chard, K.M. Hope as a Change Mechanism in the Treatment of Posttraumatic Stress Disorder. Psychol. Trauma Theory Res. Pract. Policy 2012, 4, 270–277. [Google Scholar] [CrossRef]
- Madan, S.; Pakenham, K.I. The Stress-Buffering Effects of Hope on Adjustment to Multiple Sclerosis. Int. J. Behav. Med. 2014, 21, 877–890. [Google Scholar] [CrossRef] [PubMed]
- Mirhosseini, S.; Dadgari, A.; Basirinezhad, M.H.; Mohammadpourhodki, R.; Ebrahimi, H. The Role of Hope to Alleviate Anxiety in COVID-19 Outbreak among Community Dwellers: An Online Cross-Sectional Survey. Ann. Acad. Med. Singap. 2020, 49, 723–730. [Google Scholar] [CrossRef] [PubMed]
- Trzebiński, J.; Cabański, M.; Czarnecka, J.Z. Reaction to the COVID-19 Pandemic: The Influence of Meaning in Life, Life Satisfaction, and Assumptions on World Orderliness and Positivity. J. Loss Trauma 2020, 25, 544–557. [Google Scholar] [CrossRef]
- Ding, K.; Yang, J.; Chin, M.K.; Sullivan, L.; Demirhan, G.; Violant-Holz, V.; Uvinha, R.R.; Dai, J.; Xu, X.; Popeska, B.; et al. Article Mental Health among Adults during the COVID-19 Pandemic Lockdown: A Cross-Sectional Multi-Country Comparison. Int. J. Environ. Res. Public Health 2021, 18, 2686. [Google Scholar] [CrossRef]
- Long, L.J.; Bistricky, S.L.; Phillips, C.A.; D’Souza, J.M.; Richardson, A.L.; Lai, B.S.; Short, M.; Gallagher, M.W. The Potential Unique Impacts of Hope and Resilience on Mental Health and Well-Being in the Wake of Hurricane Harvey. J. Trauma. Stress 2020, 33, 962–972. [Google Scholar] [CrossRef]
- Wu, H.C. The Protective Effects of Resilience and Hope on Quality of Life of the Families Coping with the Criminal Traumatisation of One of Its Members. J. Clin. Nurs. 2011, 20, 1906–1915. [Google Scholar] [CrossRef]
- Shi, M.; Liu, L.; Wang, Z.Y.; Wang, L. Prevalence of Depressive Symptoms and Its Correlations with Positive Psychological Variables among Chinese Medical Students: An Exploratory Cross-Sectional Study. BMC Psychiatry 2016, 16, 3. [Google Scholar] [CrossRef]
- Alemi, Q.; Stempel, C.; Koga, P.M.; Montgomery, S.; Smith, V.; Sandhu, G.; Villegas, B.; Requejo, J. Risk and Protective Factors Associated with the Mental Health of Young Adults in Kabul, Afghanistan. BMC Psychiatry 2018, 18. [Google Scholar] [CrossRef] [PubMed]
- Bahmani, B.; Motamed Najjar, M.; Sayyah, M.; Shafi-Abadi, A.; Haddad Kashani, H. The Effectiveness of Cognitive-Existential Group Therapy on Increasing Hope and Decreasing Depression in Women-Treated with Haemodialysis. Glob. J. Health Sci. 2015, 8, 219–225. [Google Scholar] [CrossRef] [PubMed]
- Ho, S.M.Y.; Ho, J.W.C.; Pau, B.K.Y.; Hui, B.P.H.; Wong, R.S.M.; Chu, A.T.W. Hope-Based Intervention for Individuals Susceptible to Colorectal Cancer: A Pilot Study. Fam. Cancer 2012, 11, 545–551. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Hou, W.L.; Ko, N.Y.; Shu, B.C. Effects of a Strengths-Based Perspective Support Group among Taiwanese Women Who Left a Violent Intimate Partner Relationship. J. Clin. Nurs. 2016, 25, 543–554. [Google Scholar] [CrossRef]
- Kok, L.; Sep, M.S.; Veldhuijzen, D.S.; Cornelisse, S.; Nierich, A.P.; van der Maaten, J.; Rosseel, P.M.; Hofland, J.; Dieleman, J.M.; Vinkers, C.H.; et al. Trait Anxiety Mediates the Effect of Stress Exposure on Post-Traumatic Stress Disorder and Depression Risk in Cardiac Surgery Patients. J. Affect. Disord. 2016, 206, 216–223. [Google Scholar] [CrossRef]
- Place, P.J.; Ling, S.; Patihis, L. Full Statistical Mediation of the Relationship between Trauma and Depressive Symptoms. Int. J. Psychol. 2018, 53, 142–149. [Google Scholar] [CrossRef]
- Anyan, F.; Bizumic, B.; Hjemdal, O. Specificity in Mediated Pathways by Anxiety Symptoms Linking Adolescent Stress Profiles to Depressive Symptoms: Results of a Moderated Mediation Approach. J. Affect. Disord. 2018, 228, 109–117. [Google Scholar] [CrossRef]
- Anyan, F.; Worsley, L.; Hjemdal, O. Anxiety Symptoms Mediate the Relationship between Exposure to Stressful Negative Life Events and Depressive Symptoms: A Conditional Process Modelling of the Protective Effects of Resilience. Asian J. Psychiatry 2017, 29, 41–48. [Google Scholar] [CrossRef]
- Havnen, A.; Anyan, F.; Hjemdal, O.; Solem, S.; Riksfjord, M.G.; Hagen, K. Resilience Moderates Negative Outcome from Stress during the COVID-19 Pandemic: A Moderatedmediation Approach. Int. J. Environ. Res. Public Health 2020, 17, 6461. [Google Scholar] [CrossRef]
- Bryant, R.A.; O’Donnell, M.L.; Creamer, M.; McFarlane, A.C.; Clark, C.R.; Silove, D. The Psychiatric Sequelae of Traumatic Injury. Am. J. Psychiatry 2010, 167, 312–320. [Google Scholar] [CrossRef]
- Kessler, R.C.; Demler, O.; Frank, R.G.; Olfson, M.; Pincus, H.A.; Walters, E.E.; Wang, P.; Wells, K.B.; Zaslavsky, A.M. Prevalence and Treatment of Mental Disorders, 1990 to 2003. N. Engl. J. Med. 2005, 352, 2515–2523. [Google Scholar] [CrossRef]
- Gallagher, M.W.; Long, L.J.; Phillips, C.A. Hope, Optimism, Self-Efficacy, and Posttraumatic Stress Disorder: A Meta-Analytic Review of the Protective Effects of Positive Expectancies. J. Clin. Psychol. 2020, 76, 329–355. [Google Scholar] [CrossRef]
- Lovibond, S.H.; Lovibond, P.F. Manual for the Depression Anxiety and Stress Scales, 2nd ed.; Psychology Foundation: Sydney, Australia, 1995; Volume 33, ISBN 0005-7967. [Google Scholar]
- Resilience Research Centre. Child and Youth Resilience Measure (CYRM-R) & Adult Resilience Measure (ARM-R User Manual). Available online: http://www.resilienceresearch.org/2018 (accessed on 29 April 2021).
- Snyder, C.R.; Harris, C.; Anderson, J.R.; Holleran, S.A.; Irving, L.M.; Sigmon, S.T.; Yoshinobu, L.; Gibb, J.; Langelle, C.; Harney, P. The Will and the Ways: Development and Validation of an Individual-Differences Measure of Hope. J. Personal. Soc. Psychol. 1991, 60, 570–585. [Google Scholar] [CrossRef]
- Edwards, L.M.; Rand, K.L.; Lopez, S.J.; Snyder, C.R. Understanding Hope: A Review of Measurement and Construct Validity Research. In Oxford Handbook of Methods in Positive Psychology; Ong, A.D., van Dulmen, M.H., Eds.; Oxford University Press: New York, NY, USA, 2007; pp. 83–95. ISBN 0-19-517218-3. [Google Scholar]
- Weiss, D.S.; Marmar, C.R. The impact of event scale—Revised. In Assessing Psychological Trauma and PTSD; Wilson, J.P., Keane, T.M., Eds.; Guilford Press: New York, NY, USA, 1997; pp. 399–411. [Google Scholar]
- Tee, M.L.; Tee, C.A.; Anlacan, J.P.; Aligam, K.J.G.; Reyes, P.W.C.; Kuruchittham, V.; Ho, R.C. Psychological Impact of COVID-19 Pandemic in the Philippines. J. Affect. Disord. 2020, 277, 379–391. [Google Scholar] [CrossRef]
- Wang, C.; Pan, R.; Wan, X.; Tan, Y.; Xu, L.; McIntyre, R.S.; Choo, F.N.; Tran, B.; Ho, R.; Sharma, V.K.; et al. A Longitudinal Study on the Mental Health of General Population during the COVID-19 Epidemic in China. Brain Behav. Immun. 2020, 87, 40–48. [Google Scholar] [CrossRef] [PubMed]
- Hao, F.; Tan, W.; Jiang, L.; Zhang, L.; Zhao, X.; Zou, Y.; Hu, Y.; Luo, X.; Jiang, X.; McIntyre, R.S.; et al. Do Psychiatric Patients Experience More Psychiatric Symptoms during COVID-19 Pandemic and Lockdown? A Case-Control Study with Service and Research Implications for Immunopsychiatry. Brain Behav. Immunity 2020, 87, 100–106. [Google Scholar] [CrossRef] [PubMed]
- Kline, R.B. Principles and Practice of Structural Equation Modeling, 3rd ed.; Guilford Press: New York, NY, USA, 2011. [Google Scholar]
- Peng, M.; Mo, B.; Liu, Y.; Xu, M.; Song, X.; Liu, L.; Fang, Y.; Guo, T.; Ye, J.; Yu, Z.; et al. Prevalence, Risk Factors and Clinical Correlates of Depression in Quarantined Population during the COVID-19 Outbreak. J. Affect. Disord. 2020, 275, 119–124. [Google Scholar] [CrossRef] [PubMed]
- Moreno-Agostino, D.; Wu, Y.T.; Daskalopoulou, C.; Hasan, M.T.; Huisman, M.; Prina, M. Global Trends in the Prevalence and Incidence of Depression:A Systematic Review and Meta-Analysis. J. Affect. Disord. 2021, 281, 235–243. [Google Scholar] [CrossRef] [PubMed]
- Liu, Q.; He, H.; Yang, J.; Feng, X.; Zhao, F.; Lyu, J. Changes in the Global Burden of Depression from 1990 to 2017: Findings from the Global Burden of Disease Study. J. Psychiatr. Res. 2020, 126, 134–140. [Google Scholar] [CrossRef] [PubMed]
- Price, M.; Legrand, A.C.; Brier, Z.M.F.; Hébert-Dufresne, L. The Symptoms at the Center: Examining the Comorbidity of Posttraumatic Stress Disorder, Generalized Anxiety Disorder, and Depression with Network Analysis. J. Psychiatr. Res. 2019, 109, 52–58. [Google Scholar] [CrossRef]
- Olfson, M.; Mojtabai, R.; Merikangas, K.R.; Compton, W.M.; Wang, S.; Grant, B.F.; Blanco, C. Reexamining Associations between Mania, Depression, Anxiety and Substance Use Disorders: Results from a Prospective National Cohort. Mol. Psychiatry 2017, 22, 235–241. [Google Scholar] [CrossRef] [PubMed]
- Kessler, R.C.; Sampson, N.A.; Berglund, P.; Gruber, M.J.; Al-Hamzawi, A.; Andrade, L.; Bunting, B.; Demyttenaere, K.; Florescu, S.; De Girolamo, G.; et al. Anxious and Non-Anxious Major Depressive Disorder in the World Health Organization World Mental Health Surveys. Epidemiol. Psychiatr. Sci. 2015, 24, 210–226. [Google Scholar] [CrossRef] [PubMed]
- Batista, P.; Duque, V.; Luzio-Vaz, A.; Pereira, A. Anxiety Impact during COVID-19: A Systematic Review. J. Infect. Dev. Ctries. 2021, 15, 320–325. [Google Scholar] [CrossRef]
- Wang, C.; Pan, R.; Wan, X.; Tan, Y.; Xu, L.; Ho, C.S.; Ho, R.C. Immediate Psychological Responses and Associated Factors during the Initial Stage of the 2019 Coronavirus Disease (COVID-19) Epidemic among the General Population in China. Int. J. Environ. Res. Public Health 2020, 17, 1729. [Google Scholar] [CrossRef]
- Bonichini, S.; Tremolada, M. Quality of Life and Symptoms of PTSD during the COVID-19 Lockdown in Italy. Int. J. Environ. Res. Public Health 2021, 18, 4385. [Google Scholar] [CrossRef]
- Zhou, M.; Guo, W. Subjective Distress about COVID-19 and Its Social Correlates: Empirical Evidence from Hubei Province of China. J. Affect. Disord. 2021, 289, 46–54. [Google Scholar] [CrossRef]
- Tyrer, P. COVID-19 Health Anxiety. World Psychiatry 2020, 19, 307. [Google Scholar] [CrossRef]
- Dennis, D.; Radnitz, C.; Wheaton, M.G. A Perfect Storm? Health Anxiety, Contamination Fears, and COVID-19: Lessons Learned from Past Pandemics and Current Challenges. Int. J. Cogn. Ther. 2021, 1–17. [Google Scholar] [CrossRef]
- Stewart, D.E.; Appelbaum, P.S. COVID-19 and Psychiatrists’ Responsibilities: A WPA Position Paper. World Psychiatry 2020, 19, 406. [Google Scholar] [CrossRef] [PubMed]
- Gloster, A.T.; Walder, N.; Levin, M.E.; Twohig, M.P.; Karekla, M. The Empirical Status of Acceptance and Commitment Therapy: A Review of Meta-Analyses. J. Contextual Behav. Sci. 2020, 18, 181–192. [Google Scholar] [CrossRef]
- Ma, Y.; She, Z.; Siu, A.F.Y.; Zeng, X.; Liu, X. Effectiveness of Online Mindfulness-Based Interventions on Psychological Distress and the Mediating Role of Emotion Regulation. Front. Psychol. 2018, 9, 2090. [Google Scholar] [CrossRef]
- Schultchen, D.; Küchler, A.M.; Schillings, C.; Weineck, F.; Karabatsiakis, A.; Ebert, D.D.; Baumeister, H.; Pollatos, O. Effectiveness of a Guided Online Mindfulness-Focused Intervention in a Student Population: Study Protocol for a Randomised Control Trial. BMJ Open 2020, 10, e032775. [Google Scholar] [CrossRef] [PubMed]
- Griffin, K.H.; Johnson, J.R.; Kitzmann, J.P.; Kolste, A.K.; Dusek, J.A. Outcomes of a Multimodal Resilience Training Program in an Outpatient Integrative Medicine Clinic. J. Altern. Complementary Med. 2015, 21, 628–637. [Google Scholar] [CrossRef] [PubMed]
- Hwang, W.J.; Lee, T.Y.; Lim, K.O.; Bae, D.; Kwak, S.; Park, H.Y.; Kwon, J.S. The Effects of Four Days of Intensive Mindfulness Meditation Training (Templestay Program) on Resilience to Stress: A Randomized Controlled Trial. Psychol. Health Med. 2018, 23, 497–504. [Google Scholar] [CrossRef]
- Sturgeon, J.A.; Darnall, B.D. Facilitating patient resilience: Mindfulness-based stress reduction, acceptance, and positive social and emotional interventions. In Psychological Approaches to Pain Management: A practitioner’s Handbook, 3rd ed.; Turk, D.C., Gatchel, R.J., Eds.; The Guildford Press: New York, NY, USA, 2018; pp. 250–263. [Google Scholar]
- Shechter, A.; Diaz, F.; Moise, N.; Anstey, D.E.; Ye, S.; Agarwal, S.; Birk, J.L.; Brodie, D.; Cannone, D.E.; Chang, B.; et al. Psychological Distress, Coping Behaviors, and Preferences for Support among New York Healthcare Workers during the COVID-19 Pandemic. Gen. Hosp. Psychiatry 2020, 66, 1–8. [Google Scholar] [CrossRef]
- Dominguez-Rodriguez, A.; de la Rosa-Gómez, A.; Jesús Hernández Jiménez, M.; Arenas-Landgrave, P.; Martínez-Luna, S.C.; Silva, J.A.; Hernández, J.E.G.; Arzola-Sánchez, C.; Guzmán, V.A. A Self-Administered Multicomponent Web-Based Mental Health Intervention for the Mexican Population during the COVID-19 Pandemic: Protocol for a Randomized Controlled Trial. JMIR Res. Protoc. 2020, 9, e23117. [Google Scholar] [CrossRef] [PubMed]
- Singh, A.B. What’s the Psychiatrist’s Role in the COVID-19 Outbreak? Aust. N. Z. J. Psychiatry 2020, 54, 759. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| n | % | |
|---|---|---|
| Gender | ||
| Males | 171 | 37.5% |
| Females | 284 | 62.3% |
| Not identify as female/male | 1 | 0.2% |
| Country of residence | ||
| Republic of Ireland/Northern Ireland | 197 | 43.2% |
| United States | 259 | 56.8% |
| Marital status | ||
| Single | 165 | 36.2% |
| Married/relationship | 255 | 56% |
| Separated/divorced/widowed | 36 | 7.8% |
| Living situation | ||
| Living on their own | 55 | 12.1% |
| Living with others (not family) | 21 | 4.6% |
| Living with family/partner | 380 | 83.2% |
| Normal (n) % | Mild (n) % | Moderate (n) % | Severe (n) % | Extremely Severe (n) % | |
|---|---|---|---|---|---|
| Traumatic distress | (346) 75.9% | (56) 12.3% | (19) 4.1% | (35) 7.7% | |
| Anxiety | (340) 74.6% | (27) 5.9% | (50) 11% | (20) 4.4% | (19) 4.2% |
| Depression | (287) 62.9% | (56) 12.3% | (71) 15.6% | (21) 4.6% | (21) 4.6% |
| Variables | M | SD | 1 | 2 | 3 | 4 |
|---|---|---|---|---|---|---|
| 1. Traumatic distress of COVID-19 | 14.8 | 14.5 | _ | |||
| 2. Resilience | 71.5 | 10.1 | −0.36 * | _ | ||
| 3. Anxiety | 4.89 | 6.44 | 0.66 * | −0.29 * | _ | |
| 4. Hope | 51.1 | 8.61 | −0.32 * | 0.59 * | −0.28 * | _ |
| 5. Depression | 8.33 | 8.71 | 0.67 * | −0.51 * | 0.61 * | −0.51 * |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Nearchou, F.; Douglas, E. Traumatic Distress of COVID-19 and Depression in the General Population: Exploring the Role of Resilience, Anxiety, and Hope. Int. J. Environ. Res. Public Health 2021, 18, 8485. https://doi.org/10.3390/ijerph18168485
Nearchou F, Douglas E. Traumatic Distress of COVID-19 and Depression in the General Population: Exploring the Role of Resilience, Anxiety, and Hope. International Journal of Environmental Research and Public Health. 2021; 18(16):8485. https://doi.org/10.3390/ijerph18168485
Chicago/Turabian StyleNearchou, Finiki, and Ellen Douglas. 2021. "Traumatic Distress of COVID-19 and Depression in the General Population: Exploring the Role of Resilience, Anxiety, and Hope" International Journal of Environmental Research and Public Health 18, no. 16: 8485. https://doi.org/10.3390/ijerph18168485
APA StyleNearchou, F., & Douglas, E. (2021). Traumatic Distress of COVID-19 and Depression in the General Population: Exploring the Role of Resilience, Anxiety, and Hope. International Journal of Environmental Research and Public Health, 18(16), 8485. https://doi.org/10.3390/ijerph18168485